
Submitted:
02 January 2026
Posted:
05 January 2026
You are already at the latest version
Abstract
Background: Childhood cancer is the leading cause of natural death among children in high-income countries, despite treatment improvements. The Spanish Registry of Childhood Tumours (RETI-SEHOP) systematically records all cases treated within the network of SEHOP units. Using RETI-SEHOP data, we evaluated survival trends to assess progress in patient care, both overall and by tumour. Methods: 20,534 childhood cancer cases (0-14 years) were recorded across the period 1999-2021. 1-, 3- and 5-year overall survival (OS) were estimated using the Kaplan-Meier method, applying the cohort approach for 1999-2018 and the period approach for 2019-2022. OS by age and sex was analysed in the recent 2009-2018 incidence cohort. Age-adjusted OS time trends were examined using joinpoint Cox models for 1999-2022. Results: For all tumours combined, 5-year OS increased from 75.4% to 84.6% between 1999-2003 and 2019-2022. While positive trends were identified for all haematological malignancies examined, a more varied scenario was in evidence for solid tumours: ependymomas improved fastest (1.51 points annually), and sarcomas, except rhabdomyosarcoma, remained stagnant. Conclusion: Our results reflect a period characterised by a combination of new therapeutic developments, improved diagnostics and more refined risk stratification, which has ultimately led to a reduction in disease-related mortality.
Keywords:
childhood cancer
; survival
; cancer registries
; trends
; epidemiology
1. Introduction
Childhood cancer is a heterogeneous group of rare neoplasms which jointly account for fewer than 1% of all cancer cases in Europe. Nonetheless, childhood cancer remains the leading cause of natural death among children and adolescents in high-income countries (HIC), despite substantial reductions in mortality [1]. In Southern Europe, age-standardised incidence of cancer in children (<15 years) was estimated at 170.9 cases per million across the period 2001-2010 [2]. Currently, approximately 1,000 cancer cases <15 years are expected annually in Spain, and more than 96% are diagnosed and managed at paediatric oncology or haematology units [3].
In Europe, 5-year survival among children with cancer exceeded 80% roughly a decade ago [4] and may now be approaching 85% in highly developed European countries [5,6,7]. These improvements have largely resulted from the co-ordinated efforts of international collaborative groups and consortia, leading to refined risk stratification, the optimisation of chemotherapy regimens, the development of immunotherapy, and the integration of molecular marker data [8,9]. While advances in surgical techniques have improved the safety and completeness of tumour resections [10,11,12], modern imaging technologies allow for earlier detection of metastatic disease [13]. In the context of high survival rates in HIC, childhood cancer care is increasingly focusing on preventing late effects and preserving organ function [14,15,16].
Cancer registries are essential instruments for documenting and monitoring the burden of cancer through the surveillance of incidence, mortality, survival and prevalence [17]. In Spain, the Spanish Registry of Childhood Tumours (RETI-SEHOP) functions as a central hospital-based registry that systematically records all childhood cancer cases (<15 years) managed at paediatric oncology and haematology units. One of RETI-SEHOP chief goals is to evaluate progress in the care of childhood cancer patients by analysing survival patterns and their evolution over time.
This study had two main aims: firstly, to provide an up-to-date description of childhood cancer survival in Spain for the 1999-2022 period, both overall and for a broad range of diagnostic entities; and secondly, to analyse time trends in survival, as an indirect means of assessing progress in the management of these diseases. A secondary aim was to document any survival differences by age and sex in the recent cohort (2009-2018), for comparison with existing literature. Our results indicate that the period 1999-2022 was marked by general improvements in childhood cancer outcomes in Spain, and we discuss how these changes relate to the implementation of new protocols and other developments in clinical practice.
2. Materials and Methods
2.1. Case Registration
RETI-SEHOP is a central hospital-based cancer registry that coordinates a nationwide network of all paediatric oncology and haematology (SEHOP) units in Spain (44 centres as of 2025) [3,18]. New cases are actively reported by these units to the RETI-SEHOP. Follow-up data up to 5 years from diagnosis are provided by each unit upon request from the registry, at 3 and 5 years. All data received are checked and coded before registration. Any queries arising during these case-by-case reviews, mainly with regard to tumour morphology, primary site, date inconsistencies or patients’ usual residence at the time of diagnosis, are referred to the reporting centres for clarification prior to registration.
All cases included in this study were coded according to the International Classification of Diseases for Oncology, 3rd Edition (ICD-O-3.1) [19] and tumours were classified into diagnostic groups, subgroups and further divisions as per the latest version of the International Childhood Cancer Classification (ICCC-3-2017) [20]. Date of diagnosis was defined as the earliest of either the true diagnosis date or the date of first suspicion of cancer, corresponding to the first consultation with a paediatric oncology unit.
Additionally, quality checks of registered cases are routinely performed, including the use of ENCR Quality Check Software (QCS) for this purpose. Follow-up information is cross-checked with the Spanish National Death Index (INDEF) as a complementary source. Death certificates are not used as a source of new case registration.
2.2. Study Population
The study population comprised all childhood cancer cases managed by SEHOP units and registered in the RETI-SEHOP, provided that they: i) had been diagnosed between 1 January 1999 and 31 December 2021; ii) were under 15 years of age at the time of diagnosis; iii) had a tumour classified in any valid category of the ICCC-3-2017; and iv) had their usual place of residence in Spain at the date of diagnosis, as defined by Regulation no. 763/2008 of the European Commission [21]. Cases of myelodysplastic syndrome and other myeloproliferative diseases (Id) and miscellaneous lymphoreticular neoplasms (IId) were excluded from all analyses [22]. Follow-up information up to 5 years after diagnosis was available for the incidence period 1999-2018. Cases diagnosed during 2019-2021 were followed up until 31 December 2022.
2.3. Statistical Analysis
Overall survival (OS) at 1, 3 and 5 years after diagnosis was estimated using the Kaplan-Meier method. For each set of cases, OS refers to absolute survival from all causes of death. For childhood cancer cases, absolute survival is almost equivalent to tumour cause-specific survival, especially in HIC [4]. The cohort approach was applied to cases diagnosed during the years 1999-2018, whereas the period approach was used for 2019-2022. The period method is used when follow-up for a recent cohort is not yet complete, as it provides the most up-to-date observed survival estimates available for that calendar period [23]. This method evaluates the survival experience of patients during the defined period, using data from those diagnosed both within the period itself and up to 5 years earlier. In the case of the period 2019-2022, follow-up data from cases diagnosed between 2014 and 2021 were used. Cases diagnosed in 2022 did not yet have follow-up data available and were therefore excluded, though the year 2022 was kept as a year of follow-up [24].
OS estimates were obtained by incidence cohort, age and sex. The 1999-2018 period was divided into four 5-year cohorts, while a single estimate was obtained for the 2019-2022 period. Survival by age (<1 year, 1-4, 5-9 and 10-14 years) and sex (female/male) was analysed for the recent 2009-2018 incidence cohort. For some tumours, the <1 year and 1-4-year groups were pooled into a single 0-4-year group when either of the former contained fewer than 15 cases. Survival differences between sexes and age groups were assessed using log-rank tests. Survival estimates based on fewer than 15 cases are not reported in the tables.
Age-standardised survival estimates (<15 years) were calculated to account for demographic changes across the study period, allowing for more robust comparisons over time. For each tumour, age-specific weights were obtained from the case pool from the incidence period 1999-2021 (Table S1). Generally, age-standardisation considered three age groups: 0-4, 5-9 and 10-14 years. However, adjacent age groups were combined (0-9 years or 5-14 years) when any group in a cohort contained fewer than 15 cases [25]. Even so, for retinoblastomas, hepatic tumours, extracranial and extragonadal germ cell tumours (GCT) and thyroid carcinomas, age-standardisation was not performed because the minimum number of cases per age group was not met.
For a subset of clinically relevant tumours, survival trends were analysed with Cox proportional hazards models modified to accommodate joinpoints [26]. All cases diagnosed from 1999 to 2021 were included, with follow-up right-truncated at 5 years after diagnosis. For each tumour type, the number and location of joinpoints were determined by minimising the Bayesian information criterion (BIC). All models included year of incidence as the explanatory variable and, where possible, stratification by age groups was introduced to allow for computation of model-adjusted age-standardised survival estimates. Adjusted survival estimates were first calculated for each age group, and the overall age-standardised estimate and its standard error were subsequently derived using the corresponding weights (Table S1).
The absolute change in survival (AACS) represents the average yearly change in survival over a defined period, expressed in percentage points. AACS was used to quantify the magnitude of trends in the time series of adjusted 5-year survival estimates. Statistical significance of AACS was assessed through bootstrap resampling: for each tumour, the dataset was resampled 500 times, and the AACS was calculated for each bootstrap iteration using the selected model. Reported AACS values and their 95% confidence intervals (CI) correspond to the median and the 2.5th and 97.5th percentiles of the bootstrap distributions. Although cases diagnosed in 2022 were not included in the models, the adjusted survival time series were extended to 2022 by means of modelled prediction, to match and compare them with the full study period.
All analyses were performed in R v4.4.1 (https://www.r-project.org/). Period survival estimates were obtained using the periodR package [27]. An ad hoc script was developed to fit age-stratified Cox models with up to two joinpoints to estimate age-standardised survival curves from individual case datasets (https://github.com/palf98/CoxJP).
3. Results
3.1. Brief Data Description
In the 1999-2021 diagnostic period, 20,534 cases with tumours classified under valid ICCC-3-2017 categories (Table S1) were registered in the RETI-SEHOP, with 8,077 haematological neoplasms (39.3%) and 12,457 solid tumours (60.7%). Among the 5,074 recorded central nervous system (CNS) tumours, 1,637 were non-malignant (32.7%), though this proportion increased slightly across the study period, going from 31.7% in 1999-2010 to 33.4% in 2011-2021. This increase reached statistical significance (p = 0.037) in a linear model that tested the effect of diagnosis year on the proportion of non-malignant CNS cases. Second tumours accounted for 123 (0.6%) of all cases, and only 2 third tumours were registered during the 1999-2021 period for children aged 0-14 years. Our data complied with the IARC quality indicators for childhood cancer registries [28] (Table 1).
3.2. Observed Survival
Follow-up at 5 years ranged from 96% to 98% for all tumours across the entire study period. In the 2019-2022 follow-up period, fewer than 3% of contributing cases were lost to follow-up before 5 years or the period’s closure date.
During the study period, OS at 5 years increased by 9 percentage points for all tumours (ICCC-3-2017 groups I-XII) and all malignant tumours, reaching 84.6% and 83.1% in 2019-2022, respectively (Table 2, Figure 1). In 2019-2022, 5-year OS appears to have consolidated above 90% for Hodgkin lymphomas (HL), Burkitt lymphomas (BL), retinoblastomas, renal tumours and GCT. In contrast, survival remained comparatively low for intracranial and intraspinal embryonal tumours, other gliomas (a category formed by non-ependymoma, non-astrocytoma gliomas), and malignant bone tumours. A more detailed overview of tabulated survival results, including the number of cases, follow-up percentages at 5 years, and OS at 1 and 3 years by diagnostic group is shown in Tables S2-S6.
Remarkable survival improvements were observed for cases of haematological malignancies between 1999-2003 and 2019-2022. Comparing the first and the last estimates of the series, 5-year risk of death decreased by 45% for leukaemias and 59% for lymphomas (Table 2). For BL specifically, 5-year risk of death declined by approximately 80%. Conversely, progress in acute myeloid leukaemia (AML) has been comparatively modest within haematological neoplasms, leaving substantial room for further improvement.
For solid tumours, the picture is more heterogeneous. At one end of the spectrum, 5-year risk of death fell close to 0 in astrocytomas (non-malignant), retinoblastomas and gonadal GCT, all of which already had high survival rates at the beginning of the study period. At the other end, little or no improvement was observed for other gliomas and malignant bone tumours, which started with some of the lowest survival rates among the tumours studied.
For all cancers combined, OS up to 5 years differed significantly across age groups (Table 3). In general, observed survival was highest for children aged 1-4 years and lowest among those aged 10-14 years. By specific diagnostics, significant differences by age group were identified for lymphoid leukaemias (LL), CNS tumours, neuroblastomas, hepatoblastomas and epithelial neoplasms. For CNS tumours, differences disappeared when analysing non-malignant cases. The number of cases by age group used to obtain the calculations in Table 3 is shown in Table S7.
In general, survival rates were homogeneous between males and females (Table S8). Among the 38 tumour categories studied a statistically significant difference in survival by sex was observed solely for non-Hodgkin lymphomas (NHL) (except Burkitt). Males, who accounted for almost 70% of these cases, had a 5-year OS rate of 90.5% in the 2009-2018 cohort as compared to 81.9% in females.Table 2. Observed 5-year survival and 95% confidence interval by diagnostic groups, 0-14 years.
3.3. Survival Trends
Age standardisation of survival was tailored to each tumour type according to its age distribution at diagnosis. For most tumours, three five-year age groups (0-4, 5-9 and 10-14 years) were used, allowing for a more sensitive capture of demographic variation. The 0-9 and 10-14 year groups were applied to tumours typically diagnosed at older ages, such as HL, bone sarcomas, intracranial/intraspinal and gonadal GCT, and epithelial neoplasms. Conversely, standardisation based on 0-4 and 5-14 year groups was used for ependymomas, medulloblastomas, neuroblastomas and nephroblastomas. Due either to their scarcity or to their incidence being concentrated within narrow age ranges, or to both, age standardisation was not performed for some tumours. This was the case of retinoblastomas, hepatoblastomas, extracranial/extragonadal GCT, and thyroid carcinomas. Age-standardised survival rates are shown by cohort and tumour type in Table S9, including the 2019-2022 follow-up period. Since case population weights are used for the standardisations, estimates can be interpreted on the scale of observed 5-year survival for all ages (0-14 years).
In general, fitted models did not identify change points in the 5-year survival trend over the study period (Figure 2, Figure 3, Figure 4 and Figure 5). A single change point was only identified for non-malignant astrocytomas (Figure 3), retinoblastomas (Figure 4), GCT and intracranial/intraspinal GCT in particular, and epithelial tumours (Figure 5), but in no case did the models that minimised BIC identify more than one joinpoint.
For all tumours with malignant behaviour combined, the fitted model identified a significant increase in age-standardised survival between 1999 and 2022 (Figure 2a), achieving an increase of approximately one percentage point every two years on average. Given the large number of cases included and the nearly linear progression of the observed annual hazard estimates, the model seems to correctly capture survival variation throughout the period.
All analysed subgroups of haematological malignancies experienced statistically significant upward trends across the study period (Figure 2b-f). Fitted 5-year survival estimates for LL (Figure 2b) and non-Burkitt NHL (Figure 2e) surpassed 90% in about 2019. AML experienced the highest AACS among haematological neoplasms over the study period, but their survival still lags well behind that of the other subgroups (Figure 2c). Age-standardised 5-year survival in BL increased to almost 100% by 2022, with an estimated AACS of 0.65 over the series of 24 years, which is exceptionally high given that fitted survival was already around 84% at the start of the series (Figure 2f).
In contrast to the relatively homogeneous trends seen in haematological malignancies, survival patterns among solid tumours, including brain tumours, were more diverse (Figure 3, Figure 4 and Figure 5). Among all tumours studied, ependymomas registered the lowest fitted 5-year survival rates at the beginning of the study period (Figure 3a). However, they experienced the steepest absolute increase in 5-year survival, by more than one percentage point every year. Throughout the period, approximately 7% of ependymomas were non-malignant, with this proportion remaining relatively stable. For malignant astrocytomas, no statistically significant improvement in survival could be established, as the 95% CI of the AACS included zero (Figure 3b). In contrast, non-malignant astrocytomas showed significant improvement from 2007 onwards, with fitted 5-year survival rates remaining nearly at 100% after 2015, consistent with the observed values (Figure 3c). For medulloblastomas, observed annual estimates showed substantial variability, but the model was able to identify a significantly positive AACS, estimated at around 0.71 (Figure 3d).
Overall, extracranial embryonal tumours displayed positive trends. Both fitted and observed data show a consistent increase in survival for neuroblastoma cases throughout the period (Figure 3e). Like non-malignant astrocytomas, retinoblastomas registered a phase of significant survival improvement beginning after 2012, following an earlier period of stagnation (Figure 3f). For nephroblastomas, the fitted model identified a modest, albeit significant, upward trend in 5-year survival, with survival exceeding 90% after 2008 (Figure 4a). Unlike the rest of analysed embryonal tumours, no significant improvements in survival were found for hepatoblastomas, possibly due to the number of cases being insufficient to detect a slight increase (Figure 4b).
Among the analysed sarcomas, only rhabdomyosarcomas (RMS) exhibited a significant increase in fitted age-standardised 5-year survival (Figure 4e), as opposed to osteosarcomas (Figure 4c), Ewing sarcomas of bone (Figure 4d) and non-RMS soft tissue sarcomas (STS) (Figure 4f). The fitted model for RMS indicated an annual increase of 0.62 percentage points in age-standardised 5-year survival, though the proximity of the lower end of the 95% CI to zero suggests that this improvement should be interpreted with caution. In the case of osteosarcomas, though not statistically significant, the model fitted a slightly negative survival trend between 1999 and 2022.
For all GCT combined, the model identified a significant decline in age-standardised 5-year survival during the early years of the study period (1999-2002), followed by a positive trend that eventually recovered and surpassed the initial loss in survival (Figure 5a). This change point was located near the beginning of the series, leaving only three years prior to it, which was the minimum allowed. The negative trend in these early years appeared to be mostly influenced by extragonadal GCT (Figure 5b-c). In the case of intracranial/intraspinal GCT, the same change point was identified, with a very steep decrease in survival between 1999 and 2002 (Figure 5b). However, this negative trend was not statistically significant due to the low number of cases included in this subgroup. For extracranial/extragonadal GCT, no statistically significant trends were identified (Figure 5c). A mild improvement was observed in gonadal GCT, with 5-year survival slowly approaching 100% by the end of the period (Figure 5d).
For epithelial neoplasms, a significant decrease in survival was identified between 1999 and 2007, followed by a period of non-significant improvement (Figure 5e). Notably, the number of registered epithelial tumour cases, i.e., the number of patients attending SEHOP units, rose substantially over the study period (Table S6). This broader inclusion of cases, potentially involving patients with different prognostic profiles, may partly explain the initial decline in survival. Since no deaths were observed for thyroid carcinomas during the study period, no trends could be analysed (Figure 5f).
4. Discussion
This study analyses survival outcomes and time trends based in more than 20,000 children (0-14 years) treated at SEHOP units, which provides nationwide coverage. The 24-year study period offers a sufficiently long time frame to combine historical and recent data, allowing for analysis of long-term survival trends. We used the period approach to estimate 5-year survival rates up to 2022, with the aim of providing the most up-to-date observed survival results possible [29].
On average, approximately 3% of cases were lost to follow-up at 5 years. This finding was applicable to most diagnostic groups except epithelial tumours, for which the proportion of cases lost to follow-up ranged from 10 to 23%. For these tumours in particular, survival results should be interpreted with caution, since censoring might have been associated with prognostic differences. Among the main reasons for loss to follow-up is that notifying units may lose contact with patients after cure or transfer to non-paediatric units.
In Spain, the vast majority of children with cancer are treated at SEHOP units, especially in recent years. These units handled roughly 80% of incident cases during 1999-2009 and more than 90% after 2009 [3]. A proportion of childhood cancer cases continues to be managed in non-paediatric units, such as general surgery, haematology and dermatology departments: this is especially true of haematological neoplasms and epithelial tumours. In the Spanish context, collaborative efforts between regional population-based cancer registries and RETI-SEHOP are being made to achieve the most representative datasets possible for such areas through record linkage.
Among SEHOP units, 5-year OS for all tumours exceeded 80% in the 2009-2013 cohort, and is nearing 85% in the period 2019-2022 for children aged 0-14 years. These figures fit comparatively well with published results from other HIC. In EUROCARE-6, 5-year survival in 2010-2014 for the pool of all participating European registries was estimated at 81.3% (period approach) [4]. The nationwide Italian hospital-based childhood cancer registry reported 5-year survival of up to 84% in 2009-2017 (period approach) [7]. In the Netherlands, childhood cancer survival stood at 83.7% in 2010-2015, and at 81.1% for tumours of malignant behaviour only [30]. In France, 5-year survival increased from 80.8% in 2004-2008 to 84.6% in 2010-2016 [31]. England’s National Health Service (NHS) published a series of annual survival estimates for childhood cancer in 2002-2020, surpassing the 80% mark after 2006 and the 85% mark after 2016 (period approach: 2017-2020) [32]. It should be noted that the most up-to-date survival estimates provided by cancer registries are often released on their institutional websites well in advance of publications from international collaborative projects, such as EUROCARE. However, this mode of dissemination may limit long-term accessibility if such results are not published in public repositories or peer-reviewed journals.
In our 2009-2018 cohort, survival was broadly similar between males and females, with a significant difference observed only for NHL (except Burkitt), where males registered higher 5-year survival than did females (90.5% vs. 81.9%). Other studies have reported sex-related differences in several tumour types [33] but most of these differences disappeared when adjusting for age, histology, site and stage, except in the case of ependymomas [34]. Overall, sex appears to have a limited influence on childhood cancer survival, and any observed effects are likely small and may diminish over time as therapeutic approaches improve for disease subtypes that differ in prevalence between the sexes.
In contrast, age at diagnosis showed a clear association with survival, which was especially stark for some tumours. Three distinct age-related survival patterns were observed: i) survival peaking at 1-4 years (LL, malignant astrocytomas, hepatic tumours); ii) survival increasing with age (ependymomas and choroid plexus tumour, CNS embryonal tumours, epithelial tumours); and iii) survival decreasing with age (other gliomas, neuroblastomas). These results are in line with the findings for the French 2000-2008 cohort [33].
Among LL, age disparities have persisted over time due to a lack of progress in infant disease, which presents unique biological and clinical challenges, such as KMT2A rearrangement mutations and increased treatment toxicity [35,36]. Furthermore, survival decreased slightly for children over 9 years old, replicating the pattern observed in CONCORD-2 [37]. For malignant astrocytomas, glioblastoma represented the morphology with the poorest outcomes in our cohort, comprising <10% of cases among children aged 1-4 years but around 20% in other groups. Conversely, malignant gliomas of optic nerve, a histology with excellent survival, were the most prevalent among cases 1-4 years old (>40%).
Complete resection for ependymomas below 3 years of age is known to be challenging, which is partly responsible for the poorer outcomes in this age bracket. Treatment regimens for intracranial ependymoma in this age group are characterised by avoidance or delay of radiotherapy to reduce the risk of cognitive sequelae and secondary tumours [38,39]. For neuroblastomas, older age at diagnosis correlates with advanced disease, but survival differences persist even after adjustment for stage [40]. On the whole, survival variations by age probably reflect a combination of biological heterogeneity, treatment tolerance and surgical feasibility. These findings highlight the need for continued biologically-based stratification in paediatric oncology research.
Overall, fitted trends in age-standardised survival between 1999 and 2022 were predominantly linear for Spain, with no change points for the most part. In a study analysing paediatric cancer survival trends with SEER data by main diagnostic groups, no joinpoints were identified after 1999 [41], which suggests that progress over recent decades has generally advanced at a steady pace.
Remarkable progress has been made in paediatric haematological neoplasms during the study period. Observed trends closely resembled those published recently for a selection of Spanish regions in a population-based study (2000-2016) [42]. This similarity supports the contention that, to a greater or lesser degree, their results, covering almost 65% of the Spanish paediatric population, can be extrapolated to the national level.
Survival trends for LL indicated steady improvement across the study period, which was characterised by a succession of two branches of national protocols that were unified in 2013: SHOP/ALL-99 (1999-2005), SHOP/ALL-05 (2005-2013), PETHEMA ALL-IR 96 (1996-2013), PETHEMA ALL-LR 2001 (2001-2013) and PETHEMA ALL-HR 2005 (2005-2013). In 2013, LAL-SEHOP-PETHEMA-2013 unified national protocols, thereby integrating the experience of the SHOP and PETHEMA groups. These protocols have achieved a reduction in deaths and relapses in all risk strata of non-infant LL. In the case of infants, even though Spain did not participate in the European INTERFANT-06 trial (EudraCT 2005-004599-19), most units nevertheless adopted its scheme from 2007 onwards. However, results of the INTERFANT-06 Phase III trial showed no significant improvements with respect to the previous INTERFANT-99 protocol [43]. Recently, the incorporation of blinatumomab into the INTERFANT-06 backbone showed potential to enhance outcomes for infants with ALL [44]. Despite overall progress in LL management in Spain, 5-year survival has yet to surpass 90%, whereas other European countries reached this threshold years ago [4,6,45]. This gap prompted the SEHOP to prioritise first-line treatment in prospective clinical trials conducted by European cooperative study groups, rather than rely solely on guideline-based therapeutic protocols.
In the case of AML, treatment regimens during the study period specialised in Down syndrome (DS) cases, acute promyelocytic leukaemias (APL) and non-DS-AML cases. DS cases were treated following their BFM-98 protocol branch until 2007, when the strategy of the ML-DS-2006 trial (EudraCT 2007-006219-2) was adopted. However, the ML-DS-2006 trial did not report an increase in survival for DS cases, which was already high [46]. For APL, specific national protocols were used throughout the study period (PETHEMA-LPA-96/2005/2012/2017), optimising risk-adapted strategies based on the use of ATRA [47]. PETHEMA-LPA-2017 sought to improve outcomes by introducing ATO+ATRA therapy for low and intermediate-risk cases. In 2017, Spanish centres began participating in the NOPHO-DBH-AML-2012 phase III trial (EudraCT 2012-002934-35) for non-DS AML cases [48], though some units had already started to adhere to their protocol several years earlier. In all likelihood, improved risk stratification, novel therapies, and advances in supportive care and haematopoietic stem cell transplantation contributed to rising cure rates, consolidating 5-year OS above 70%, in line with other European countries. [6,7,49]. Looking ahead, further improvements for AML will depend on the cooperation of international collaborative groups, enabling the design of large prospective trials, the integration of biology-driven risk stratification, and the incorporation of targeted therapeutic approaches [50].
The 1999-2022 period proved to be very positive for lymphomas, with only NHL remaining below 90% 5-year OS. HL showed excellent survival from the start of the period, yet some improvements were still observed, especially around 2008, as shown by the OS estimates by cohort. About this time, Spanish centres shifted from national protocols to EuroNET-PHL-C1 (EudraCT 2006-000995-33), which omitted radiotherapy for early-stage cases with good response to chemotherapy, ultimately reducing toxicity [51]. This change might partly explain the observed increase in survival. Spain has actively participated in both EuroNET-PHL-C1 and EuroNET-PHL-C2 (EudraCT 2012-004053-88), the latter covering the most recent years of our cohort since 2016.
Given the marked biological and therapeutic heterogeneity of NHL, trends observed likely reflect a composite of different changes in clinical practice. Major NHL subtypes comprise mature B-cell lymphoma, lymphoblastic lymphoma (LBL) and anaplastic large cell lymphoma (ALCL). In general, a major milestone in our country was joining the European Inter-Group for Childhood Non-Hodgkin Lymphoma (eicnhl) in the late 1990s, enabling active participation in international protocols and cooperative clinical trials incorporating new biomarkers, risk-stratification strategies, and novel therapies, all contributing to improved survival outcomes.
Regarding B-mature NHL, including BL, Spain adopted LMB-89 [52] dose-dense treatment strategy in the early 2000s, achieving better outcomes than earlier national protocols. Subsequent participation in the phase III INTER-NHL-B-2010 trial (NCT01516580) demonstrated that adding rituximab to LMB chemotherapy significantly improved survival in high-risk patients, becoming the standard of care in many HIC [53]. Although Spain did not participate in Euro-LB-02 (NCT00275106) [54], its control arm was adopted as the national standard for LBL, avoiding CNS irradiation but yielding lower event-free survival than earlier BFM studies [55]. Since 2020, Spain has participated in the LBL2018 trial (NCT04043494), which incorporates molecular risk stratification (NOTCH1/FBXW7). For ALCL, Spanish centres did not participate in the ALCL99 trial (NCT00006455), but adopted its protocol as the national standard of care in the early 2000s, as it represented the option with the lowest treatment-intensity among the available regimens. Given the strong prognostic value of NPM1-ALK-based biomarkers in ALCL [56], Spain has recently incorporated centralised assessment into routine practice to refine risk stratification and guide treatment intensity, particularly in the context of emerging targeted therapies.
Despite excellent survival for NHL overall, outcomes in relapsed/refractory (r/r) cases remain poor [57]. Only one clinical trial within the eicnhl addressed r/r NHL from 1999 to 2021: the ALCL Relapse trial (NCT00317408) [58], whose recommendations were followed by Spanish centres until targeted therapies became available after 2022. For r/r B-NHL, rituximab combined with ICE followed by autologous SCT has been the standard of care, with limited success in some entities [59]. At the time of writing this manuscript, the Glo-B-NHL study (EudraCT 2021-004283-10), a prospective, risk-adapted, cooperative clinical trial focusing on r/r B-NHL, is open for recruitment [60].
We performed separate analyses for malignant and non-malignant CNS tumours to avoid bias, since the proportion of registered non-malignant cases increased during the study period. A previous study covering the period 1991-2005 reported that survival for childhood CNS tumours in Spain and its major subtypes was stagnant and below that of Europe [61]. In this study, we report that ependymomas, non-malignant astrocytomas, and medulloblastomas, registered positive trends in the 1999-2022 period, narrowing the gap with Europe. 5-year OS for malignant CNS tumours reached 63.7% in 2014-2018 and is expected to reach 66.2% or more in the 2019-2022 cohort, which compares relatively well with the 66% reported for Germany in 2011-2016 [6].
Between 1999 and 2005, CNS cases under 3 years of age were treated with a single national protocol. At the same time, ependymomas over 3 years were managed following the SIOP Ependymoma I protocol, which emphasised total resection and validated the effectiveness of VEC chemotherapy in residual tumours [62]. In parallel, it became increasingly clear that post-operative radiotherapy in cases under 3 years of age enhanced disease control [63]. From 2015 onwards, most ependymomas regardless of age followed the SIOP Ependymoma II protocol (EudraCT 2013-002766-39), which was widely adopted in Spanish centres. This protocol avoided radiotherapy in children below 1 year of age, planning for delays and temporary control with chemotherapy to prevent cognitive sequelae. Further improvements can be expected after 2022, driven by the COG ACNS0121 phase III (NCT00027846) and SIOP Epend II phase II/III trials. In addition, new European guidelines now stratify treatment using specific molecular markers [39].
Our study identified a period of stable survival for non-malignant astrocytomas from 1999 to 2007, followed by a rising trend up to 2022. The joinpoint occurs in a year with an abnormally low 5-year survival, which may have exaggerated the AACS in the second segment. Nonetheless, an improvement is evident in the second half of the period, coinciding with a more exhaustive capture of non-malignant CNS cases. Non-malignant astrocytomas were treated with the SIOP-LGG-1995 and SIOP-LGG-2004 protocols. The SIOP-LGG-2004 trial (EudraCT 2005-005377-29) recruited patients, including Spanish cases, to test the addition of etoposide to classic vincristine+carboplatin induction [64]. We suggest that this new protocol, together with surgical refinements contributed to the increase in survival, which approached 100% after 2010. Conversely, we report no significant progress in outcomes for malignant astrocytomas. German HIT-GBM-D and HIT-HGG-2007 (EudraCT 2007-000128-42) protocols were sporadically used in Spanish units. From 2011 to 2016, the HERBY trial (EudraCT 2010-022189-28) recruited high-grade gliomas to test the addition of bevacizumab to the radiotherapy+temozolomide treatment but was halted due to high toxicity, with no added benefit [65]. High-grade gliomas continue to lag behind in survival progress, and broader collaborative efforts may be needed to advance in this field.
Medulloblastomas displayed the second most marked survival improvement among brain tumours in terms of AACS. PNET-SIOP-3, PNET-SIOP-4 and PNET-SIOP-5 (EudraCT 2011-004868-30) were the most frequent protocols in our cohort. Since 2009, high-risk cases under 4 years have generally been treated following the HEAD-START-I, II and III protocols, which have likely contributed to improve outcomes and reduce late effects, using brief and intensive chemotherapy [66,67]. Since 2017, a non-negligible proportion of high-risk cases over 3 years has been treated following COG ACNS-0332/0334 strategies (NCT00392327/NCT00336024), which similarly achieved better outcomes by combining radiotherapy and carboplatin treatment [68]. Nevertheless, survival remains limited, and long-term quality of life has still to be improved.
There was significant progress in outcomes for all embryonal tumours, except hepatoblastomas. Turning to neuroblastoma, a recent Spanish study (2000-2017) suggested positive effects of the HR-NBL-1 (EudraCT 2006-001489-17) and LINES (NCT01728155) trials and highlighted that improvements were mostly concentrated among locoregional cases [69]. Our data indicate that progress continued through 2022, reaching a 5-year OS of 85%. For retinoblastomas, survival consistently approached 100% after the joinpoint in 2012. In Spain, retinoblastomas were managed in five highly specialised ophthalmology services throughout the study period. Key developments around 2012 included the use of intraarterial chemotherapy as first-line treatment and intravitreous/intracameral chemotherapy to eliminate residual disease, enabling a shift from systemic to eye-directed chemotherapies. Paired with the avoidance of enucleation, these techniques improved both survival and vision-preservation rates [70]. In the case of nephroblastomas, steady improvement occurred from 1999 to 2022, a period with strong adherence of SEHOP units to SIOP protocols (SIOP-93, SIOP-01 and UMBRELLA SIOP-RTSG 2016). SIOP-93/01 trials highlighted the importance of preoperative chemotherapy and proper postoperative risk stratification in the management of non-metastatic cases [71]. Nevertheless, a small subset of high-risk nephroblastomas remained refractory. The UMBRELLA protocol (EudraCT 2016-004180-39) unifies management of nephroblastomas and other renal tumours by performing centralised diagnostic evaluation, which determines risk stratification and directs the recommended treatment [72]. With respect to hepatoblastomas, Spanish cases were treated by successively following the European SIOPEL-3, -4 and -6 protocols. While SIOPEL-3 and -4 introduced significant progress in outcomes for high-risk patients by intensifying preoperative chemotherapy with cisplatin [73,74], SIOPEL-6 (EudraCT 2007-002402-21) focused on reducing cisplatin-induced ototoxicity in standard-risk patients with sodium thiosulfate [75]. The PHITT trial (NCT03017326) protocol, adopted in Spain around 2018, employs the CHIC risk stratification system based on PRETEXT staging [76,77,78] but its implementation is too recent to evaluate with our cohort. Due to their rarity, the positive trend modelled for hepatoblastomas in our study has a wide CI, but we suggest that this positive trend may consolidate in the coming years.
As in other recent cancer registry studies, we report no significant progress for bone sarcomas [6,7,30,41]. During the period 1999-2022, Spanish osteosarcoma cases were treated according to national protocols (SEOP-SO-95/2001/2010). Spain did not participate in the EURAMOS-1 trial (NCT00134030), which ultimately did not significantly improve outcomes [79]. Since 2014, non-metastatic extremity cases enrolled in the GEIS-33 national trial (NCT04383288), which sought to identify molecular markers for biological stratification [80]. The use of mifamurtide in adjuvant chemotherapy has recently shown promising results for localised ABCB1/P-glycoprotein-positive cases [81]. Yet despite the availability of this drug in Spain since 2010, we found no significant impact on population-level outcomes. With regard to Ewing sarcomas, national protocols predominated until the introduction of EuroEwing-2012 (EudraCT 2012-002107-17). Most cases in the 1999-2015 period were treated according to Ewing-SEOP-95/99/01. EuroEwing-2012 became predominant after 2016, with some overlap with the national GEIS-21 trial (NCT01696669). GEIS-21 explored the use of gemcitabine+docetaxel cycles in high-risk patients [82]. EuroEwing-2012 subsequently introduced VDC+IE, which demonstrated survival advantages in children under 14 years [83]. Even so, our cohort reflects no clear progress between 1999 and 2022.
RMS and other STS were managed under SIOPE protocols throughout the study period. RMS were treated with MMT-95 (until 2005), EpSSG-RMS-2005 (2005-2021; EudraCT 2005-000217-35) and FaR-RMS (EudraCT 2018-000515-24), which was first used in 2021. These successive cooperative trials progressively refined risk-adapted multimodal treatment, reducing the chemotherapy burden where possible [84,85]. Survival of RMS cases in Spain increased significantly over time and is on par with other European countries [4]. Non-metastatic non-RMS STS, except for Ewing and Askin tumours, were treated largely under the EpSSG-NRSTS-2005 protocol (EudraCT 2005-001139-31) for most of the study period. This protocol unified treatment across Europe and improved risk stratification. Progress remains limited, however, partly due to the heterogeneity and poor chemosensitivity of these tumours [86]. Regarding metastatic cases, no major breakthroughs were introduced during the study period [87]. The positive but not significant trend in our findings highlights the need for further advancements in non-RMS STS management, including subtype-focused research and careful adaptation of adult trial findings to paediatric patients.
Overall, GCT displayed favourable trends. Children with CNS GCT in Spain were generally managed according to SIOP-CNS-GCT-96 until 2010, and thereafter with SIOP-CNS-GCT-II (EudraCT 2009-018072-33). Throughout the study period, craniospinal irradiation remained the standard for germinomas, while non-germinomatous GCT require multimodal therapy, as demonstrated by the SIOP-CNS-96 trial [88,89]. The SIOP-CNS-GCT-II trial sought to adjust the radiotherapy dose for germinomas to maintain already excellent outcomes and to improve survival in high-risk non-germinomatous GCT by chemotherapy dose escalation, which may partly explain the positive trend observed after 2007. Survival for gonadal GCT approached 100%, with no deaths registered for cases diagnosed after 2015. Although we observed no significant changes in survival for extracranial/extragonadal GCT cases, it is difficult to ascertain the accuracy of this, given that this subgroup had fewer than 10 cases annually. Moreover, not performing age-standardisation for this rare subgroup may have led to an underestimation of the trend, as infants not only show higher survival but also became a lower proportion of all children after 2010.
In the case of epithelial tumours, the identified negative trend in 1999-2007 most likely reflects an artifact of insufficient follow-up completeness and the increase in coverage by paediatric oncologists, which probably affected the composition of diagnostics analysed over time. Currently, epithelial tumours make up the main ICCC-3 group with lowest registration completeness in RETI-SEHOP [3], suggesting that many are still being managed by other services, especially thyroid carcinomas and localised malignant melanomas.
In recent decades, improving quality of life has become a major priority for clinicians, especially in the case of tumours for which survival is already high or excellent. There is also a need to evaluate survivorship in the growing population of childhood cancer survivors [90]. However, most cancer registries currently lack the capacity to record such data systematically, given the multidimensional nature of quality of life, although long-term excess mortality might serve as a reasonable provisional proxy [91]. Our findings underscore the importance of incorporating such data into HIC cancer registries, in order to keep monitoring progress, especially for tumours already approaching 100% long-term disease-related survival.
As for the strengths of our study, we analysed survival over a 24-year long period for all children with cancer attended by paediatric oncologists and haematologists in Spain, providing up-to-date estimates through the period approach. We studied survival trends using Cox-joinpoint models, which yielded meaningful results overall. These models captured trends consistently across the entire period, since residuals by diagnosis year were relatively homogeneous. Additionally, we modelled age-standardised survival to minimise any bias introduced by demographic changes.
With respect to limitations, survival figures for 2019-2022 can be expected to be slightly underestimated, as has been shown to happen for period estimates in a context of continuous progress of care [29]. Joinpoints identify trend changes well but fail to identify abrupt additive changes, as can occur with therapeutic breakthroughs. Regarding registration, non-malignant CNS and epithelial tumours registration completeness increased across the study period, hindering longitudinal analysis. Furthermore, coding changes can be expected to occur in long-term series but did not appear to introduce major deviations. Though a primary benchmark, 5-year survival cannot suffice to describe long-term survival and is even less informative for assessing survivors’ quality of life. Additionally, we could not obtain event-free survival, a preferred metric for outcome evaluation in some diagnostics, because relapse information was not available.
5. Conclusions
Childhood cancer 5-year survival in Spain is currently approaching 85%, in line with other European countries. Our retrospective analysis of the SEHOP network of paediatric oncology and haematology units across the period 1999-2022 reveals substantial survival improvements for most childhood cancer diagnostics. Survival increases have been generally steady, reflecting a cumulative effect of advances in clinical practice. More precise diagnostics and better-tailored risk-adapted treatments are likely responsible for much of this progress. However, there are still several tumours with unfavourable outcomes which did not show significant improvements, such as malignant astrocytomas and bone sarcomas. Addressing tumours with persistently poor survival and reducing late effects remain key challenges for Spanish paediatric oncology in the coming years.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprint.org. Table S1. Age-specific case population weights sampled from the study case pool, 1999-2021. Table S2. Survival results by incidence cohort for all tumours, 0-14 years. Table S3. Survival results by incidence cohort for haematological neoplasms, 0-14 years. Table S4. Survival results by incidence cohort for central nervous system tumours, 0-14 years. Table S5. Survival results by incidence cohort for embryonal and germ cell tumours, 0-14 years. Table S6. Survival results by incidence cohort for sarcomas and epithelial tumours, 0-14 years. Table S7. Number of registered cases by age group in the 2009-2018 incidence cohort by diagnostic group. Table S8. Observed survival at 5 years by sex and diagnostic group in the 2009-2018 incidence cohort, 0-14 years. Table S9. Age-standardised overall survival rates (StOS) by diagnostic group and incidence cohort.
Author Contributions
Conceptualisation, P.AC., A.C., Á.BR.; methodology, P.AC., Á. BR.; software, P.AC., Á. BR.; validation, A.C., Á.BR., JL.DD., S.R., JM.FN., J.VA.; formal analysis, P.AC., Á.BR.; writing—original draft preparation, P.AC.; writing—review and editing, A.C., Á.BR., JL.DD., S.R., JM.FN., J.VA.; visualisation, P.AC.; supervision, A.C., Á.BR. All authors have read and agreed to the published version of the manuscript.
Funding
The Spanish Registry of Childhood Tumours (RETI-SEHOP) has the support of the Ministry of Health of Spain, the University of Valencia and the SEHOP, as well as the collaboration of the Enriqueta Villavecchia Foundation. The funding sources had no role in study conception or design, data collection, data analysis, data interpretation, writing of the paper or in the decision to submit for publication.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee (CEIM) of the La Fe University and Polytechnic Hospital (Hospital Universitario y Politécnico La Fe), Valencia, Spain (Approval no. 2025-0723-1; initial approval 30/07/2025, amendment approved 08/10/2025).
Informed Consent Statement
Informed consent was obtained from the parents or legal guardians of all patients prior to their registration in the RETI-SEHOP. The use of these data for the present study is legitimate, as the consent forms explicitly included authorisation for future use in epidemiological studies aimed at advancing knowledge of childhood cancer.
Data Availability Statement
The datasets generated and/or analysed during the current study are not publicly available due to privacy restrictions, but aggregated tables, as well as the R code used for the analysis, can be made available from the corresponding authors on reasonable request.
Acknowledgments
The Spanish Childhood Cancer Registry (RETI-SEHOP) is supported by collaboration between Spain’s Ministry of Health, the Spanish Society of Paediatric Haematology and Oncology (SEHOP), and the University of Valencia, for whose support we are most grateful. We would also like to thank the Enriqueta Villavecchia Foundation for their support. We are also grateful for the continuous support of the SEOP and SEHOP executive boards over the years. Finally, we further acknowledge the collaboration of the SEHOP unit co-ordinators responsible for reporting to the RETI-SEHOP.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AACS | Absolute annual change in survival |
| ALCL | Anaplastic large cell lymphoma |
| AML | Acute myeloid leukaemia |
| BIC | Bayesian information criterion |
| BL | Burkitt lymphoma |
| CI | Confidence interval |
| CNS | Central nervous system |
| GCT | Germ cell tumours |
| HIC | High-income countries |
| HL | Hodgkin lymphoma |
| ICCC | International Childhood Cancer Classification |
| ICD-O | International Classification of Diseases for Oncology |
| LBL | Lymphoblastic lymphoma |
| LL | Lymphoid leukaemias |
| NHL | Non-Hodgkin lymphomas |
| OS | Overall survival |
| RETI-SEHOP | Spanish Registry of Childhood Tumours |
| SEHOP | Spanish Society of Paediatric Haematology and Oncology |
Appendix A
Members of the RETI-SEHOP Survival Working Group are disclosed in Appendix A.
References
- Pritchard-Jones, K; Pieters, R; Reaman, GH; Hjorth, L; Downie, P; Calaminus, G; Naafs-Wilstra, MC; Steliarova-Foucher, E. Sustaining innovation and improvement in the treatment of childhood cancer: lessons from high-income countries. Lancet Oncol. 2013, 14(3), e95–e103. [Google Scholar] [CrossRef] [PubMed]
- Steliarova-Foucher, E; Colombet, M; Ries, LAG; Moreno, F; Dolya, A; Bray, F; Hesseling, P; Shin, HY; Stiller, CA. IICC-3 contributors. International incidence of childhood cancer, 2001-10: a population-based registry study. Lancet Oncol. Erratum in: Lancet Oncol. 2017 Jun;18(6):e301. doi: 10.1016/S1470-2045(17)30369-8. 2017, 18(6), 719–731. [Google Scholar] [CrossRef]
- Cañete Nieto, A; Pardo Romaguera, E; Alfonso Comos, P; Valero Poveda, S; Porta Cebolla, S; Peris Bonet, R. 45 años de Estadísticas del Cáncer infantil en España. Universidad de Valencia; Valencia, 2025. Available online: https://hdl.handle.net/10550/112145.
- Botta, L; Gatta, G; Capocaccia, R; Stiller, C; Cañete, A; Dal Maso, L; Innos, K; Mihor, A; Erdmann, F; Spix, C; Lacour, B; Marcos-Gragera, R; Murray, D; Rossi, S; EUROCARE-6 Working Group. Long-term survival and cure fraction estimates for childhood cancer in Europe (EUROCARE-6): results from a population-based study. Lancet Oncol. 2022, 23(12), 1525–1536. [Google Scholar] [CrossRef] [PubMed]
- Cromie, KJ; Hughes, NF; Milner, S; Crump, P; Grinfeld, J; Jenkins, A; Norman, PD; Picton, SV; Stiller, CA; Yeomanson, D; Glaser, AW; Feltbower, RG. Socio-economic and ethnic disparities in childhood cancer survival, Yorkshire, UK. Br J Cancer 2023, 128(9), 1710–1722. [Google Scholar] [CrossRef]
- Wellbrock, M; Spix, C; Ronckers, CM; Grabow, D; Filbert, AL; Borkhardt, A; Wollschläger, D; Erdmann, F. Temporal patterns of childhood cancer survival 1991 to 2016: A nationwide register-study based on data from the German Childhood Cancer Registry. Int J Cancer 2023, 153(4), 742–755. [Google Scholar] [CrossRef]
- Pession, A; Quarello, P; Zecca, M; Mosso, ML; Rondelli, R; Milani, L; De Rosa, M; Rosso, T; Maule, M; Fagioli, F. Survival rates and extra-regional migration patterns of children and adolescents with cancer in Italy: The 30-year experience of the Italian Association of Pediatric Hematology and Oncology (AIEOP) with the Italian hospital-based registry of pediatric cancer (Mod. 1.01). Int J Cancer 2024, 155(10), 1741–1750. [Google Scholar] [CrossRef]
- Ehrlich, PF. The impact of cooperative group studies on childhood cancer: Improving outcomes and quality and international collaboration. Semin Pediatr Surg. 2019, 28(6), 150857. [Google Scholar] [CrossRef] [PubMed]
- Gore, L; O’Brien, MM. Only the beginning: 50 years of progress toward curing childhood cancer. Cell 2024, 187(7), 1584–1588. [Google Scholar] [CrossRef]
- Fischer, J; Pohl, A; Volland, R; Hero, B; Dübbers, M; Cernaianu, G; Berthold, F; von Schweinitz, D; Simon, T. Complete surgical resection improves outcome in INRG high-risk patients with localized neuroblastoma older than 18 months. BMC Cancer 2017, 17(1), 520. [Google Scholar] [CrossRef]
- Gow, KW; Lautz, TB; Malek, MM; Cost, NG; Newman, EA; Dasgupta, R; Christison-Lagay, ER; Tiao, GM; Davidoff, AM. COG Surgery Discipline Committee. Children’s Oncology Group’s 2023 blueprint for research: Surgery. Pediatr Blood Cancer 2024, 71(3), e30766. [Google Scholar] [CrossRef]
- Jacobson, JC; Scrushy, MG; Gillory, LA; Pandya, SR. Utilization of robotics in pediatric surgical oncology. Semin Pediatr Surg 2023, 32(1), 151263. [Google Scholar] [CrossRef]
- Rogers, W; Thulasi Seetha, S; Refaee, TAG; Lieverse, RIY; Granzier, RWY; Ibrahim, A; Keek, SA; Sanduleanu, S; Primakov, SP; Beuque, MPL; Marcus, D; van der Wiel, AMA; Zerka, F; Oberije, CJG; van Timmeren, JE; Woodruff, HC; Lambin, P. Radiomics: from qualitative to quantitative imaging. Br J Radiol 2020, 93(1108), 20190948. [Google Scholar] [CrossRef] [PubMed]
- Izurieta-Pacheco, AC; Ramaswamy, V; Tsang, DS; Rutka, J; Wasserman, J; Guger, S; Weidman, DR; Nathan, PC; Scheinemann, K; Bennett, J. Late Effects in Survivors of Pediatric Medulloblastoma: A Comprehensive Review. Pediatr Blood Cancer 2025, e32132. [Google Scholar] [CrossRef]
- Wang, K; Chen, Y; Ahn, S; Zheng, M; Landoni, E; Dotti, G; Savoldo, B; Han, Z. GD2-specific CAR T cells encapsulated in an injectable hydrogel control retinoblastoma and preserve vision. Nat Cancer 2020, 1(10), 990–997. [Google Scholar] [CrossRef]
- Kaneuchi, Y; Yoshida, S; Fujiwara, T; Evans, S; Abudu, A. Limb salvage surgery has a higher complication rate than amputation but is still beneficial for patients younger than 10 years old with osteosarcoma of an extremity. J Pediatr Surg. 2022, 57(11), 702–709. [Google Scholar] [CrossRef]
- Parkin, DM. The role of cancer registries in cancer control. Int J Clin Oncol. 2008, 13(2), 102–11. [Google Scholar] [CrossRef]
- Navarro, C; Martos, C; Ardanaz, E; Galceran, J; Izarzugaza, I; Peris-Bonet, R; Martínez, C; Spanish Cancer Registries Working Group. Population-based cancer registries in Spain and their role in cancer control. Ann Oncol. 2010, 21 Suppl 3, iii3–13. [Google Scholar] [CrossRef]
- Fritz, A; Percy, C; Jack, A; Shanmugartnam, K; Sobin, L; Parkin, DM; Author 1, A.; Author 2, B.; International Classification of Diseases for Oncology. 3rd ed; 1st revision. Title of the chapter. In Book Title, 2nd ed.; Editor 1, A., Editor 2, B., Eds.; WHO: Geneva; Publisher: Publisher Location, Country, 2013; Volume 3, pp. 154–196. [Google Scholar]
- Steliarova-Foucher, E; Colombet, M; Ries, LAG; Rous, B; Stiller, CA. Classification of tumours. In International Incidence of Childhood Cancer, Vol. III (electronic version); Steliarova-Foucher, E, Colombet, M, Ries, LAG, Moreno, F, Dolya, A, Shin, HY, Hesseling, P, Stiller, CA, Eds.; IARC: Lyon, France, 2017; Available online: https://iicc.iarc.fr/classification/.
- European Parliament and Council of the European Union. Regulation (EC) No 763/2008 of the European Parliament and of the Council of 9 July 2008 on population and housing censuses. Off J Eur Union 2008, L218, 14–20. Available online: https://eur-lex.europa.eu/eli/reg/2008/763/oj (accessed on December 2025).
- Vincent, TJ; Bayne, AM; Brownbill, PA; Stiller, CA; Stiller, C. Methods. In Childhood Cancer in Britain: Incidence, Survival, Mortality.; Oxford University Press: Oxford, 2007; pp. 8–21. [Google Scholar] [CrossRef]
- Brenner, H; Gefeller, O. An alternative approach to monitoring cancer patient survival. Cancer 1996, 78(9), 2004–10. [Google Scholar] [CrossRef] [PubMed]
- Cronin, K; Mariotto, A; Scoppa, S; Green, D; Clegg, L. Differences between Brenner et al. and NCI Methods for calculating period survival. Technical report 2003-02-A; Statistical Research and Application Branch, National Cancer Institute: Bethesda, 2003. [Google Scholar]
- Girardi, F; Di Carlo, V; Stiller, C; Gatta, G; Woods, RR; Visser, O; Lacour, B; Tucker, TC; Coleman, MP; Allemani, C; CONCORD Working Group. Global survival trends for brain tumors, by histology: Analysis of individual records for 67,776 children diagnosed in 61 countries during 2000-2014 (CONCORD-3). Neuro Oncol. 2023, 25(3), 593–606. [Google Scholar] [CrossRef]
- Mariotto, AB; Zhang, F; Buckman, DW; Miller, D; Cho, H; Feuer, EJ. Characterizing Trends in Cancer Patients’ Survival Using the JPSurv Software. Cancer Epidemiol Biomarkers Prev. 2021, 30(11), 2001–2009. [Google Scholar] [CrossRef]
- Holleczek, B; Brenner, H. Model based period analysis of absolute and relative survival with R: data preparation, model fitting and derivation of survival estimates. Comput Methods Programs Biomed. 2013, 110(2), 192–202. [Google Scholar] [CrossRef]
- Steliarova-Foucher, E; Colombet, M; Ries, LAG; Rous, B; Stiller, CA. Indicators of data quality. In International Incidence of Childhood Cancer, Vol. III (electronic version); Steliarova-Foucher, E, Colombet, M, Ries, LAG, Moreno, F, Dolya, A, Shin, HY, Hesseling, P, Stiller, CA, Eds.; IARC: Lyon, France, 2017; Available online: https://iicc.iarc.who.int/results/introduction/qualityindicators.pdf.
- Brenner, H; Gefeller, O; Hakulinen, T. Period analysis for ‘up-to-date’ cancer survival data: theory, empirical evaluation, computational realisation and applications. Eur J Cancer 2004, 40(3), 326–35. [Google Scholar] [CrossRef] [PubMed]
- Peirelinck, H; Schulpen, M; Hoogendijk, R; Van Damme, A; Pieters, R; Henau, K; Van Damme, N; Karim-Kos, HE. Incidence, survival, and mortality of cancer in children and young adolescents in Belgium and the Netherlands in 2004-2015: A comparative population-based study. Int J Cancer 2024, 155(2), 226–239. [Google Scholar] [CrossRef]
- Registre National des Cancers de l’Enfant. Les chiffres: statistiques de survie [Internet]. Paris (France): Registre National des Cancers de l’Enfant. Available online: https://rnce.inserm.fr/rnce/les-chiffres/ (accessed on December 2025).
- Digital, NHS. Cancer survival in England, cancers diagnosed 2016 to 2020, followed up to 2021 [Internet]. Leeds (England): NHS Digital, 2023. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/cancer-survival-in-england/cancers-diagnosed-2016-to-2020-followed-up-to-2021 (accessed on December 2025).
- Lacour, B; Goujon, S; Guissou, S; Guyot-Goubin, A; Desmée, S; Désandes, E; Clavel, J. Childhood cancer survival in France, 2000-2008. Eur J Cancer Prev. 2014, 23(5), 449–57. [Google Scholar] [CrossRef]
- Williams, LA; Spector, LG. Survival Differences Between Males and Females Diagnosed With Childhood Cancer. JNCI Cancer Spectr 2019, 3(2), pkz032. [Google Scholar] [CrossRef]
- Duguid, A; Mattiucci, D; Ottersbach, K. Infant leukaemia—faithful models, cell of origin and the niche. Dis Model Mech. 2021, 14(10), dmm049189. [Google Scholar] [CrossRef] [PubMed]
- Balduzzi, A; Buechner, J; Ifversen, M; Dalle, JH; Colita, AM; Bierings, M. Acute Lymphoblastic Leukaemia in the Youngest: Haematopoietic Stem Cell Transplantation and Beyond. Front Pediatr 2022, 10, 807992. [Google Scholar] [CrossRef]
- Bonaventure, A; Harewood, R; Stiller, CA; Gatta, G; Clavel, J; Stefan, DC; Carreira, H; Spika, D; Marcos-Gragera, R; Peris-Bonet, R; Piñeros, M; Sant, M; Kuehni, CE; Murphy, MFG; Coleman, MP; Allemani, C. CONCORD Working Group. Worldwide comparison of survival from childhood leukaemia for 1995-2009, by subtype, age, and sex (CONCORD-2): a population-based study of individual data for 89 828 children from 198 registries in 53 countries. Lancet Haematol Erratum in: Lancet Haematol. 2017 May;4(5):e201. doi: 10.1016/S2352-3026(17)30067-4. 2017, 4(5), e202–e217. [Google Scholar] [CrossRef] [PubMed]
- Howe, GN; Edmonston, DY; Dirks, GC; Boop, FA; Merchant, TE. Conformal Radiation Therapy for Ependymoma at Age ≤3 Years: A 25-Year Experience. Int J Radiat Oncol Biol Phys. 2023, 116(4), 869–877. [Google Scholar] [CrossRef]
- Rubio-San-Simón, A; Ritzmann, TA; Obrecht-Sturm, D; Benesch, M; Timmermann, B; Leblond, P; Kilday, JP; Poggi, G; Thorp, N; Massimino, M; van Veelen, ML; Schuhmann, M; Thomale, UW; Tippelt, S; Schüller, U; Rutkowski, S; Grundy, RG; Bolle, S; Fernández-Teijeiro, A; Pajtler, KW. European standard clinical practice recommendations for newly diagnosed ependymoma of childhood and adolescence. EJC Paediatr Oncol. 2025, 5, 100227. [Google Scholar] [CrossRef]
- Cheung, NK; Zhang, J; Lu, C; Parker, M; Bahrami, A; Tickoo, SK; Heguy, A; Pappo, AS; Federico, S; Dalton, J; Cheung, IY; Ding, L; Fulton, R; Wang, J; Chen, X; Becksfort, J; Wu, J; Billups, CA; Ellison, D; Mardis, ER; Wilson, RK; Downing, JR; Dyer, MA; St Jude Children’s Research Hospital–Washington University Pediatric Cancer Genome Project. Association of age at diagnosis and genetic mutations in patients with neuroblastoma. JAMA 2012, 307(10), 1062–71. [Google Scholar] [CrossRef]
- Sultan, I; Alfaar, AS; Sultan, Y; Salman, Z; Qaddoumi, I. Trends in childhood cancer: Incidence and survival analysis over 45 years of SEER data. PLoS One 2025, 20(1), e0314592. [Google Scholar] [CrossRef] [PubMed]
- Trallero, J; Sanvisens, A; Almela Vich, F; Jeghalef El Karoni, N; Saez Lloret, I; Díaz-Del-Campo, C; Marcos-Navarro, AI; Aizpurua Atxega, A; Sancho Uriarte, P; De-la-Cruz Ortega, M; Sánchez, MJ; Perucha, J; Franch, P; Chirlaque, MD; Guevara, M; Ameijide, A; Galceran, J; Ramírez, C; Camblor, MR; Alemán, MA; Gutiérrez, P; Marcos-Gragera, R; REDECAN. Incidence and time trends of childhood hematological neoplasms: a 36-year population-based study in the southern European context, 1983-2018. Front Oncol. 2023, 13, 1197850. [Google Scholar] [CrossRef]
- Pieters, R; De Lorenzo, P; Ancliffe, P; Aversa, LA; Brethon, B; Biondi, A; Campbell, M; Escherich, G; Ferster, A; Gardner, RA; Kotecha, RS; Lausen, B; Li, CK; Locatelli, F; Attarbaschi, A; Peters, C; Rubnitz, JE; Silverman, LB; Stary, J; Szczepanski, T; Vora, A; Schrappe, M; Valsecchi, MG. Outcome of Infants Younger Than 1 Year With Acute Lymphoblastic Leukemia Treated With the Interfant-06 Protocol: Results From an International Phase III Randomized Study. J Clin Oncol. 2019, 37(25), 2246–2256. [Google Scholar] [CrossRef] [PubMed]
- van der Sluis, IM; de Lorenzo, P; Kotecha, RS; Attarbaschi, A; Escherich, G; Nysom, K; Stary, J; Ferster, A; Brethon, B; Locatelli, F; Schrappe, M; Scholte-van Houtem, PE; Valsecchi, MG; Pieters, R. Blinatumomab Added to Chemotherapy in Infant Lymphoblastic Leukemia. N Engl J Med. 2023, 388(17), 1572–1581. [Google Scholar] [CrossRef]
- Ssenyonga, N; Stiller, C; Nakata, K; Shalkow, J; Redmond, S; Bulliard, JL; Girardi, F; Fowler, C; Marcos-Gragera, R; Bonaventure, A; Saint-Jacques, N; Minicozzi, P; De, P; Rodríguez-Barranco, M; Larønningen, S; Di Carlo, V; Mägi, M; Valkov, M; Seppä, K; Wyn Huws, D; Coleman, MP; Allemani, C; CONCORD Working Group. Worldwide trends in population-based survival for children, adolescents, and young adults diagnosed with leukaemia, by subtype, during 2000-14 (CONCORD-3): analysis of individual data from 258 cancer registries in 61 countries. Lancet Child Adolesc Health Erratum in: Lancet Child Adolesc Health. 2022;6(7):e21. doi: 10.1016/S2352-4642(22)00165-1. 2022, 6(6), 409–431. [Google Scholar] [CrossRef]
- Uffmann, M; Rasche, M; Zimmermann, M; von Neuhoff, C; Creutzig, U; Dworzak, M; Scheffers, L; Hasle, H; Zwaan, CM; Reinhardt, D; Klusmann, JH. Therapy reduction in patients with Down syndrome and myeloid leukemia: the international ML-DS 2006 trial. Blood 2017, 129(25), 3314–3321. [Google Scholar] [CrossRef] [PubMed]
- Sanz, MA; Montesinos, P; Kim, HT; Ruiz-Argüelles, GJ; Undurraga, MS; Uriarte, MR; Martínez, L; Jacomo, RH; Gutiérrez-Aguirre, H; Melo, RA; Bittencourt, R; Pasquini, R; Pagnano, K; Fagundes, EM; Vellenga, E; Holowiecka, A; González-Huerta, AJ; Fernández, P; De la Serna, J; Brunet, S; De Lisa, E; González-Campos, J; Ribera, JM; Krsnik, I; Ganser, A; Berliner, N; Ribeiro, RC; Lo-Coco, F; Löwenberg, B; Rego, EM. IC-APL and PETHEMA and HOVON Groups. All-trans retinoic acid with daunorubicin or idarubicin for risk-adapted treatment of acute promyelocytic leukaemia: a matched-pair analysis of the PETHEMA LPA-2005 and IC-APL studies. Ann Hematol. 2015, 94(8), 1347–56. [Google Scholar] [CrossRef]
- Tierens, A; Arad-Cohen, N; Cheuk, D; De Moerloose, B; Fernandez Navarro, JM; Hasle, H; Jahnukainen, K; Juul-Dam, KL; Kaspers, G; Kovalova, Z; Lausen, B; Norén-Nyström, U; Palle, J; Pasauliene, R; Jan Pronk, C; Saks, K; Zeller, B; Abrahamsson, J. Mitoxantrone Versus Liposomal Daunorubicin in Induction of Pediatric AML With Risk Stratification Based on Flow Cytometry Measurement of Residual Disease. J Clin Oncol. 2024, 42(18), 2174–2185. [Google Scholar] [CrossRef]
- Schulpen, M; Goemans, BF; Kaspers, GJL; Raaijmakers, MHGP; Zwaan, CM; Karim-Kos, HE. Increased survival disparities among children and adolescents & young adults with acute myeloid leukemia: A Dutch population-based study. Int J Cancer 2022, 150(7), 1101–1112. [Google Scholar] [CrossRef] [PubMed]
- Zwaan, CM; Kolb, EA; Reinhardt, D; Abrahamsson, J; Adachi, S; Aplenc, R; De Bont, ES; De Moerloose, B; Dworzak, M; Gibson, BE; Hasle, H; Leverger, G; Locatelli, F; Ragu, C; Ribeiro, RC; Rizzari, C; Rubnitz, JE; Smith, OP; Sung, L; Tomizawa, D; van den Heuvel-Eibrink, MM; Creutzig, U; Kaspers, GJ. Collaborative Efforts Driving Progress in Pediatric Acute Myeloid Leukemia. J Clin Oncol. 2015, 33(27), 2949–62. [Google Scholar] [CrossRef] [PubMed]
- Mauz-Körholz, C; Landman-Parker, J; Fernández-Teijeiro, A; Attarbaschi, A; Balwierz, W; Bartelt, JM; Beishuizen, A; Boudjemaa, S; Cepelova, M; Ceppi, F; Claviez, A; Daw, S; Dieckmann, K; Fosså, A; Gattenlöhner, S; Georgi, T; Hjalgrim, LL; Hraskova, A; Karlén, J; Kurch, L; Leblanc, T; Mann, G; Montravers, F; Pears, J; Pelz, T; Rajić, V; Ramsay, AD; Stoevesandt, D; Uyttebroeck, A; Vordermark, D; Körholz, D; Hasenclever, D; Wallace, WH; Kluge, R. Response-adapted omission of radiotherapy in children and adolescents with early-stage classical Hodgkin lymphoma and an adequate response to vincristine, etoposide, prednisone, and doxorubicin (EuroNet-PHL-C1): a titration study. Lancet Oncol. 2023, 24(3), 252–261. [Google Scholar] [CrossRef]
- Patte, C; Auperin, A; Michon, J; Behrendt, H; Leverger, G; Frappaz, D; Lutz, P; Coze, C; Perel, Y; Raphaël, M; Terrier-Lacombe, MJ; Société Française d’Oncologie Pédiatrique. The Société Française d’Oncologie Pédiatrique LMB89 protocol: highly effective multiagent chemotherapy tailored to the tumor burden and initial response in 561 unselected children with B-cell lymphomas and L3 leukemia. Blood 2001, 97(11), 3370–9. [Google Scholar] [CrossRef]
- Minard-Colin, V; Aupérin, A; Pillon, M; Burke, GAA; Barkauskas, DA; Wheatley, K; Delgado, RF; Alexander, S; Uyttebroeck, A; Bollard, CM; Zsiros, J; Csoka, M; Kazanowska, B; Chiang, AK; Miles, RR; Wotherspoon, A; Adamson, PC; Vassal, G; Patte, C; Gross, TG. European Intergroup for Childhood Non-Hodgkin Lymphoma; Children’s Oncology Group. Rituximab for High-Risk, Mature B-Cell Non-Hodgkin’s Lymphoma in Children. N Engl J Med. 2020, 382(23), 2207–2219. [Google Scholar] [CrossRef]
- Landmann, E; Burkhardt, B; Zimmermann, M; Meyer, U; Woessmann, W; Klapper, W; Wrobel, G; Rosolen, A; Pillon, M; Escherich, G; Attarbaschi, A; Beishuizen, A; Mellgren, K; Wynn, R; Ratei, R; Plesa, A; Schrappe, M; Reiter, A; Bergeron, C; Patte, C; Bertrand, Y. Results and conclusions of the European Intergroup EURO-LB02 trial in children and adolescents with lymphoblastic lymphoma. Haematologica 2017, 102(12), 2086–2096. [Google Scholar] [CrossRef]
- Reiter, A; Schrappe, M; Ludwig, WD; Tiemann, M; Parwaresch, R; Zimmermann, M; Schirg, E; Henze, G; Schellong, G; Gadner, H; Riehm, H. Intensive ALL-type therapy without local radiotherapy provides a 90% event-free survival for children with T-cell lymphoblastic lymphoma: a BFM group report. Blood 2000, 95(2), 416–21. [Google Scholar] [CrossRef]
- Damm-Welk, C; Mussolin, L; Zimmermann, M; Pillon, M; Klapper, W; Oschlies, I; d’Amore, ES; Reiter, A; Woessmann, W; Rosolen, A. Early assessment of minimal residual disease identifies patients at very high relapse risk in NPM-ALK-positive anaplastic large-cell lymphoma. Blood 2014, 123(3), 334–7. [Google Scholar] [CrossRef]
- Burkhardt, B; Taj, M; Garnier, N; Minard-Colin, V; Hazar, V; Mellgren, K; Osumi, T; Fedorova, A; Myakova, N; Verdu-Amoros, J; Andres, M; Kabickova, E; Attarbaschi, A; Chiang, AKS; Bubanska, E; Donska, S; Hjalgrim, LL; Wachowiak, J; Pieczonka, A; Uyttebroeck, A; Lazic, J; Loeffen, J; Buechner, J; Niggli, F; Csoka, M; Krivan, G; Palma, J; Burke, GAA; Beishuizen, A; Koeppen, K; Mueller, S; Herbrueggen, H; Woessmann, W; Zimmermann, M; Balduzzi, A; Pillon, M. Treatment and Outcome Analysis of 639 Relapsed Non-Hodgkin Lymphomas in Children and Adolescents and Resulting Treatment Recommendations. Cancers (Basel) 2021, 13(9), 2075. [Google Scholar] [CrossRef]
- Knörr, F; Brugières, L; Pillon, M; Zimmermann, M; Ruf, S; Attarbaschi, A; Mellgren, K; Burke, GAA; Uyttebroeck, A; Wróbel, G; Beishuizen, A; Aladjidi, N; Reiter, A; Woessmann, W. European Inter-Group for Childhood Non-Hodgkin Lymphoma. Stem Cell Transplantation and Vinblastine Monotherapy for Relapsed Pediatric Anaplastic Large Cell Lymphoma: Results of the International, Prospective ALCL-Relapse Trial. J Clin Oncol. 2020, 38(34), 3999–4009. [Google Scholar] [CrossRef] [PubMed]
- Mato, S; Castrejón-de-Anta, N; Colmenero, A; Carità, L; Salmerón-Villalobos, J; Ramis-Zaldivar, JE; Nadeu, F; Garcia, N; Wang, L; Verdú-Amorós, J; Andrés, M; Conde, N; Celis, V; Ortega, MJ; Galera, A; Astigarraga, I; Perez-Alonso, V; Quiroga, E; Jiang, A; Scott, DW; Campo, E; Balagué, O; Salaverria, I. MYC-rearranged mature B-cell lymphomas in children and young adults are molecularly Burkitt Lymphoma. Blood Cancer J 2024, 14(1), 171. [Google Scholar] [CrossRef] [PubMed]
- Seaford, E; Maycock, S; Alexander, S; Beishuizen, A; Wistinghausen, B; Minard-Colin, V; Rigaud, C; Phillips, CA; Ford, JB; Kearns, PR; Lawson, A; Williams, E; Ahmed, Z; Muzaffar, M; Parsons, R; Gore, L; Scobie, N; Buenger, V; Allen, C; Mellgren, K; Bollard, CM; Auperin, A; Billingham, L; Burke, GAA. A global study of novel agents in paediatric and adolescent relapsed and refractory B-cell non-Hodgkin lymphoma (Glo-BNHL). Blood 2023, 142 Suppl 1, 3097. [Google Scholar] [CrossRef]
- Chirlaque MD, Peris-Bonet R, Sánchez A, Cruz O, Marcos-Gragera R, Gutiérrez-Ávila G, Quirós-García JR, Almela-Vich F, López de Munain A, Sánchez MJ, Franch-Sureda P, Ardanaz E, Galceran J, Martos C, Salmerón D, Gatta G, Botta L, Cañete A, The Spanish Childhood Cancer Epidemiology Working Group. Childhood and Adolescent Central Nervous System Tumours in Spain: Incidence and Survival over 20 Years: A Historical Baseline for Current Assessment. Cancers (Basel). 2023;15, 5889. https://doi.org/10.3390/cancers15245889.
- Ritzmann TA, Chapman RJ, Kilday JP, Thorp N, Modena P, Dineen RA, Macarthur D, Mallucci C, Jaspan T, Pajtler KW, Giagnacovo M, Jacques TS, Paine SML, Ellison DW, Bouffet E, Grundy RG. SIOP Ependymoma I: Final results, long-term follow-up, and molecular analysis of the trial cohort-A BIOMECA Consortium Study. Neuro Oncol. 2022;24, 936-948. https://doi.org/10.1093/neuonc/noac012.
- Merchant TE, Bendel AE, Sabin ND, Burger PC, Shaw DW, Chang E, Wu S, Zhou T, Eisenstat DD, Foreman NK, Fuller CE, Anderson ET, Hukin J, Lau CC, Pollack IF, Laningham FH, Lustig RH, Armstrong FD, Handler MH, Williams-Hughes C, Kessel S, Kocak M, Ellison DW, Ramaswamy V. Conformal Radiation Therapy for Pediatric Ependymoma, Chemotherapy for Incompletely Resected Ependymoma, and Observation for Completely Resected, Supratentorial Ependymoma. J Clin Oncol. 2019;37, 974-983. https://doi.org/10.1200/JCO.18.01765.
- Gnekow AK, Walker DA, Kandels D, Picton S, Giorgio Perilongo, Grill J, Stokland T, Sandstrom PE, Warmuth-Metz M, Pietsch T, Giangaspero F, Schmidt R, Faldum A, Kilmartin D, De Paoli A, De Salvo GL; of the Low Grade Glioma Consortium and the participating centers. A European randomised controlled trial of the addition of etoposide to standard vincristine and carboplatin induction as part of an 18-month treatment programme for childhood (≤16 years) low grade glioma—A final report. Eur J Cancer. 2017;81:206-225. https://doi.org/10.1016/j.ejca.2017.04.019. Erratum in: Eur J Cancer. 2018;90:156-157. https://doi.org/10.1016/j.ejca.2017.11.017.
- Grill J, Massimino M, Bouffet E, Azizi AA, McCowage G, Cañete A, Saran F, Le Deley MC, Varlet P, Morgan PS, Jaspan T, Jones C, Giangaspero F, Smith H, Garcia J, Elze MC, Rousseau RF, Abrey L, Hargrave D, Vassal G. Phase II, Open-Label, Randomized, Multicenter Trial (HERBY) of Bevacizumab in Pediatric Patients With Newly Diagnosed High-Grade Glioma. J Clin Oncol. 2018;36, 951-958. https://doi.org/10.1200/JCO.2017.76.0611.
- Dhall G, Grodman H, Ji L, Sands S, Gardner S, Dunkel IJ, McCowage GB, Diez B, Allen JC, Gopalan A, Cornelius AS, Termuhlen A, Abromowitch M, Sposto R, Finlay JL. Outcome of children less than three years old at diagnosis with non-metastatic medulloblastoma treated with chemotherapy on the “Head Start” I and II protocols. Pediatr Blood Cancer. 2008;50, 1169–1175. https://doi.org/10.1002/pbc.21525.
- Dhall G, O’Neil SH, Ji L, Haley K, Whitaker AM, Nelson MD, Gilles F, Gardner SL, Allen JC, Cornelius AS, Pradhan K, Garvin JH, Olshefski RS, Hukin J, Comito M, Goldman S, Atlas MP, Walter AW, Sands S, Sposto R, Finlay JL. Excellent outcome of young children with nodular desmoplastic medulloblastoma treated on “Head Start” III: a multi-institutional, prospective clinical trial. Neuro Oncol. 2020;22, 1862-1872. https://doi.org/10.1093/neuonc/noaa102.
- Leary SES, Packer RJ, Li Y, Billups CA, Smith KS, Jaju A, Heier L, Burger P, Walsh K, Han Y, Embry L, Hadley J, Kumar R, Michalski J, Hwang E, Gajjar A, Pollack IF, Fouladi M, Northcott PA, Olson JM. Efficacy of Carboplatin and Isotretinoin in Children With High-risk Medulloblastoma: A Randomized Clinical Trial From the Children’s Oncology Group. JAMA Oncol. 2021;7, 1313-1321. https://doi.org/10.1001/jamaoncol.2021.2224.
- Alfonso-Comos P, Cañete A, Briz-Redón Á, Romaguera EP, Segura V, Ramal D, Martínez de Las Heras B, Fernández-Teijeiro A; Spanish Neuroblastoma Working Group. Incidence and survival among children with neuroblastoma in Spain over 22 years. BMC Cancer. 2025;25, 1548. https://doi.org/10.1186/s12885-025-14877-4.
- Schaiquevich P, Francis JH, Cancela MB, Carcaboso AM, Chantada GL, Abramson DH. Treatment of Retinoblastoma: What Is the Latest and What Is the Future. Front Oncol. 2022;12:822330. https://doi.org/10.3389/fonc.2022.822330.
- Ora I, van Tinteren H, Bergeron C, de Kraker J; SIOP Nephroblastoma Study Committee. Progression of localised Wilms’ tumour during preoperative chemotherapy is an independent prognostic factor: a report from the SIOP 93-01 nephroblastoma trial and study. Eur J Cancer. 2007 Jan;43, 131–136. https://doi.org/10.1016/j.ejca.2006.08.033. Epub 2006 Nov 2. PMID: 17084075.
- van den Heuvel-Eibrink MM, Hol JA, Pritchard-Jones K, van Tinteren H, Furtwängler R, Verschuur AC, Vujanic GM, Leuschner I, Brok J, Rübe C, Smets AM, Janssens GO, Godzinski J, Ramírez-Villar GL, de Camargo B, Segers H, Collini P, Gessler M, Bergeron C, Spreafico F, Graf N; International Society of Paediatric Oncology — Renal Tumour Study Group (SIOP–RTSG). Position paper: Rationale for the treatment of Wilms tumour in the UMBRELLA SIOP-RTSG 2016 protocol. Nat Rev Urol. 2017;14, 743-752. https://doi.org/10.1038/nrurol.2017.163.
- Zsíros J, Maibach R, Shafford E, Brugieres L, Brock P, Czauderna P, Roebuck D, Childs M, Zimmermann A, Laithier V, Otte JB, de Camargo B, MacKinlay G, Scopinaro M, Aronson D, Plaschkes J, Perilongo G. Successful treatment of childhood high-risk hepatoblastoma with dose-intensive multiagent chemotherapy and surgery: final results of the SIOPEL-3HR study. J Clin Oncol. 2010;28, 2584–2590. https://doi.org/10.1200/JCO.2009.22.4857.
- Zsiros J, Brugieres L, Brock P, Roebuck D, Maibach R, Zimmermann A, Childs M, Pariente D, Laithier V, Otte JB, Branchereau S, Aronson D, Rangaswami A, Ronghe M, Casanova M, Sullivan M, Morland B, Czauderna P, Perilongo G; International Childhood Liver Tumours Strategy Group (SIOPEL). Dose-dense cisplatin-based chemotherapy and surgery for children with high-risk hepatoblastoma (SIOPEL-4): a prospective, single-arm, feasibility study. Lancet Oncol. 2013;14, 834–842. https://doi.org/10.1016/S1470-2045(13)70272-9.
- Brock PR, Maibach R, Childs M, Rajput K, Roebuck D, Sullivan MJ, Laithier V, Ronghe M, Dall’Igna P, Hiyama E, Brichard B, Skeen J, Mateos ME, Capra M, Rangaswami AA, Ansari M, Rechnitzer C, Veal GJ, Covezzoli A, Brugières L, Perilongo G, Czauderna P, Morland B, Neuwelt EA. Sodium Thiosulfate for Protection from Cisplatin-Induced Hearing Loss. N Engl J Med. 2018;378, 2376-2385. https://doi.org/10.1056/NEJMoa1801109.
- Meyers RL, Maibach R, Hiyama E, Häberle B, Krailo M, Rangaswami A, Aronson DC, Malogolowkin MH, Perilongo G, von Schweinitz D, Ansari M, Lopez-Terrada D, Tanaka Y, Alaggio R, Leuschner I, Hishiki T, Schmid I, Watanabe K, Yoshimura K, Feng Y, Rinaldi E, Saraceno D, Derosa M, Czauderna P. Risk-stratified staging in paediatric hepatoblastoma: a unified analysis from the Children’s Hepatic tumors International Collaboration. Lancet Oncol. 2017;18, 122-131. https://doi.org/10.1016/S1470-2045(16)30598-8.
- Rangaswami AA, Trobaugh-Lotrario AD, Maibach R, O’Neill AF, Aronson DC, Meyers RL, Krailo MD, Piao J, Hiyama E, Hishiki T, Ansari M, Lopez-Terrada D, Czauderna P, Malogolowkin M, Häberle B. Validation of the stratification for newly diagnosed hepatoblastoma: An analysis from the Children’s Hepatic tumors International Collaboration (CHIC) database. EJC Paediatric Oncology. 2025 ;5:100206. https://doi.org/10.1016/j.ejcped.2024.100206.
- Schmid I, O’Neill AF, Watanabe K, Aerts I, Branchereau S, Brock PR, Dandapani M, Fresneau B, Geller J, Hishiki T, Ingham D, Kraal K, Ronghe M, Tiao G, Trobaugh-Lotrario A, Rangaswami A, Sullivan MJ, Zsiros J, Hiyama E, Malogolowkin M, Ansari M. Global consensus from the PHITT consortium surrounding an interim chemotherapy guidance for the treatment of children with hepatoblastoma, hepatocellular neoplasm—not otherwise specified (HCN-NOS), hepatocellular carcinoma and fibrolamellar carcinoma after trial closure. EJC Paediatric Oncology. 2025;5:100235. https://doi.org/10.1016/j.ejcped.2025.100235.
- Smeland S, Bielack SS, Whelan J, Bernstein M, Hogendoorn P, Krailo MD, Gorlick R, Janeway KA, Ingleby FC, Anninga J, Antal I, Arndt C, Brown KLB, Butterfass-Bahloul T, Calaminus G, Capra M, Dhooge C, Eriksson M, Flanagan AM, Friedel G, Gebhardt MC, Gelderblom H, Goldsby R, Grier HE, Grimer R, Hawkins DS, Hecker-Nolting S, Sundby Hall K, Isakoff MS, Jovic G, Kühne T, Kager L, von Kalle T, Kabickova E, Lang S, Lau CC, Leavey PJ, Lessnick SL, Mascarenhas L, Mayer-Steinacker R, Meyers PA, Nagarajan R, Randall RL, Reichardt P, Renard M, Rechnitzer C, Schwartz CL, Strauss S, Teot L, Timmermann B, Sydes MR, Marina N. Survival and prognosis with osteosarcoma: outcomes in more than 2000 patients in the EURAMOS-1 (European and American Osteosarcoma Study) cohort. Eur J Cancer. 2019;109:36-50. https://doi.org/10.1016/j.ejca.2018.11.027.
- Salazar J, Arranz MJ, Martin-Broto J, Bautista F, Martínez-García J, Martínez-Trufero J, Vidal-Insua Y, Echebarria-Barona A, Díaz-Beveridge R, Valverde C, Luna P, Vaz-Salgado MA, Blay P, Álvarez R, Sebio A. Pharmacogenetics of Neoadjuvant MAP Chemotherapy in Localized Osteosarcoma: A Study Based on Data from the GEIS-33 Protocol. Pharmaceutics. 2024 Dec 12;16, 1585. https://doi.org/10.3390/pharmaceutics16121585.
- Palmerini E, Meazza C, Tamburini A, Márquez-Vega C, Bisogno G, Fagioli F, Ferraresi V, Milano GM, Coccoli L, Rubio-San-Simón A, Gallego O, Llinares Riestra ME, Manzitti C, Mora J, Vaz-Salgado MÁ, Luksch R, Mata C, Pierini M, Carretta E, Cesari M, Paioli A, Marrari A, Scotlandi K, Serra M, Asaftei SD, Gambarotti M, Picci P, Ferrari S, Valverde C, Ibrahim T, Broto JM. Is There a Role for Mifamurtide in Nonmetastatic High-Grade Osteosarcoma? Results From the Italian Sarcoma Group (ISG/OS-2) and Spanish Sarcoma Group (GEIS-33) Trials. J Clin Oncol. 2025;43, 3113-3122. https://doi.org/10.1200/JCO-25-00210.
- Mora J, Castañeda A, Perez-Jaume S, Lopez-Pousa A, Maradiegue E, Valverde C, Martin-Broto J, Garcia Del Muro X, Cruz O, Cruz J, Martinez-Trufero J, Maurel J, Vaz MA, de Alava E, de Torres C. GEIS-21: a multicentric phase II study of intensive chemotherapy including gemcitabine and docetaxel for the treatment of Ewing sarcoma of children and adults: a report from the Spanish sarcoma group (GEIS). Br J Cancer. 2017;117, 767-774. https://doi.org/10.1038/bjc.2017.252.
- Brennan B, Kirton L, Marec-Bérard P, Gaspar N, Laurence V, Martín-Broto J, Sastre A, Gelderblom H, Owens C, Fenwick N, Strauss S, Moroz V, Whelan J, Wheatley K. Comparison of two chemotherapy regimens in patients with newly diagnosed Ewing sarcoma (EE2012): an open-label, randomised, phase 3 trial. Lancet. 2022;400, 1513-1521. https://doi.org/10.1016/S0140-6736(22)01790-1.
- Oberlin O, Rey A, Sanchez de Toledo J, Martelli H, Jenney ME, Scopinaro M, Bergeron C, Merks JH, Bouvet N, Ellershaw C, Kelsey A, Spooner D, Stevens MC. Randomized comparison of intensified six-drug versus standard three-drug chemotherapy for high-risk nonmetastatic rhabdomyosarcoma and other chemotherapy-sensitive childhood soft tissue sarcomas: long-term results from the International Society of Pediatric Oncology MMT95 study. J Clin Oncol. 2012;30, 2457–2465. https://doi.org/10.1200/JCO.2011.40.3287. Erratum in: J Clin Oncol. 2025;43, 1398. https://doi.org/10.1200/JCO-25-00440.
- Bergeron C, Jenney M, De Corti F, Gallego S, Merks H, Glosli H, Ferrari A, Ranchère-Vince D, De Salvo GL, Zanetti I, Chisholm J, Minard-Colin V, Rogers T, Bisogno G; European paediatric Soft tissue sarcoma Study Group (EpSSG). Embryonal rhabdomyosarcoma completely resected at diagnosis: The European paediatric Soft tissue sarcoma Study Group RMS2005 experience. Eur J Cancer. 2021;146:21-29. https://doi.org/10.1016/j.ejca.2020.12.025.
- Ferrari A, Brennan B, Casanova M, Corradini N, Berlanga P, Schoot RA, Ramirez-Villar GL, Safwat A, Guillen Burrieza G, Dall’Igna P, Alaggio R, Lyngsie Hjalgrim L, Gatz SA, Orbach D, van Noesel MM. Pediatric Non-Rhabdomyosarcoma Soft Tissue Sarcomas: Standard of Care and Treatment Recommendations from the European Paediatric Soft Tissue Sarcoma Study Group (EpSSG). Cancer Manag Res. 2022;14:2885-2902. https://doi.org/10.2147/CMAR.S368381.
- Ferrari A, Merks JHM, Chisholm JC, Orbach D, Brennan B, Gallego S, van Noesel MM, McHugh K, van Rijn RR, Gaze MN, Martelli H, Bergeron C, Corradini N, Minard-Colin V, Bisogno G, Geoerger B, Caron HN, De Salvo GL, Casanova M. Outcomes of metastatic non-rhabdomyosarcoma soft tissue sarcomas (NRSTS) treated within the BERNIE study: a randomised, phase II study evaluating the addition of bevacizumab to chemotherapy. Eur J Cancer. 2020;130:72-80. https://doi.org/10.1016/j.ejca.2020.01.029.
- Calaminus G, Frappaz D, Kortmann RD, Krefeld B, Saran F, Pietsch T, Vasiljevic A, Garre ML, Ricardi U, Mann JR, Göbel U, Alapetite C, Murray MJ, Nicholson JC. Outcome of patients with intracranial non-germinomatous germ cell tumors-lessons from the SIOP-CNS-GCT-96 trial. Neuro Oncol. 2017;19, 1661-1672. https://doi.org/10.1093/neuonc/nox122.
- Calaminus G, Kortmann R, Worch J, Nicholson JC, Alapetite C, Garrè ML, Patte C, Ricardi U, Saran F, Frappaz D. SIOP CNS GCT 96: final report of outcome of a prospective, multinational nonrandomized trial for children and adults with intracranial germinoma, comparing craniospinal irradiation alone with chemotherapy followed by focal primary site irradiation for patients with localized disease. Neuro Oncol. 2013 Jun;15, 788–796. https://doi.org/10.1093/neuonc/not019.
- Phillips SM, Padgett LS, Leisenring WM, Stratton KK, Bishop K, Krull KR, Alfano CM, Gibson TM, de Moor JS, Hartigan DB, Armstrong GT, Robison LL, Rowland JH, Oeffinger KC, Mariotto AB. Survivors of childhood cancer in the United States: prevalence and burden of morbidity. Cancer Epidemiol Biomarkers Prev. 2015;24, 653–663. https://doi.org/10.1158/1055-9965.EPI-14-1418.
- Williams, AM; Liu, Q; Bhakta, N; Krull, KR; Hudson, MM; Robison, LL; Yasui, Y. Rethinking Success in Pediatric Oncology: Beyond 5-Year Survival. J Clin Oncol. Erratum in: J Clin Oncol. 2022;40(20):2283. doi: 10.1200/JCO.22.01230. 2021, 39(20), 2227–2231. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Observed survival curves for all tumours with malignant behaviour by cohort of diagnosis, 0-14 years. Period survival estimates are provided for the 2019-2022 cohort.
Figure 1.
Observed survival curves for all tumours with malignant behaviour by cohort of diagnosis, 0-14 years. Period survival estimates are provided for the 2019-2022 cohort.
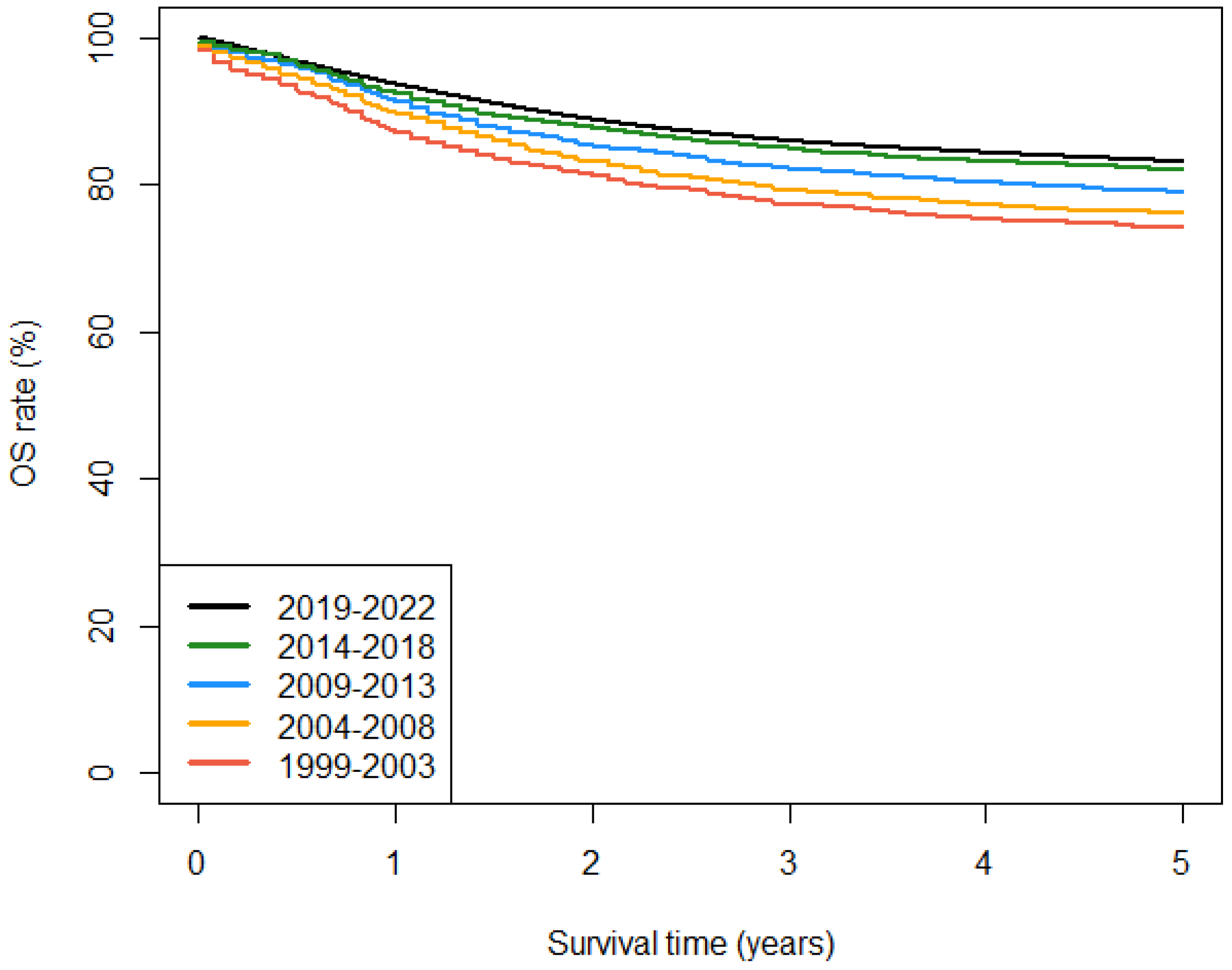
Figure 2.
Fitted trends in age-standardised 5-year survival for (a) all tumours and (b-f) haematological malignancies diagnosed in Spain, 1999-2022, 0-14 years. Black dots correspond to annual cohort estimates, while grey dots correspond to annual period estimates. Shaded areas represent 95% confidence bands around the fitted curves. AACS [95% CI]: average absolute change in survival.
Figure 2.
Fitted trends in age-standardised 5-year survival for (a) all tumours and (b-f) haematological malignancies diagnosed in Spain, 1999-2022, 0-14 years. Black dots correspond to annual cohort estimates, while grey dots correspond to annual period estimates. Shaded areas represent 95% confidence bands around the fitted curves. AACS [95% CI]: average absolute change in survival.
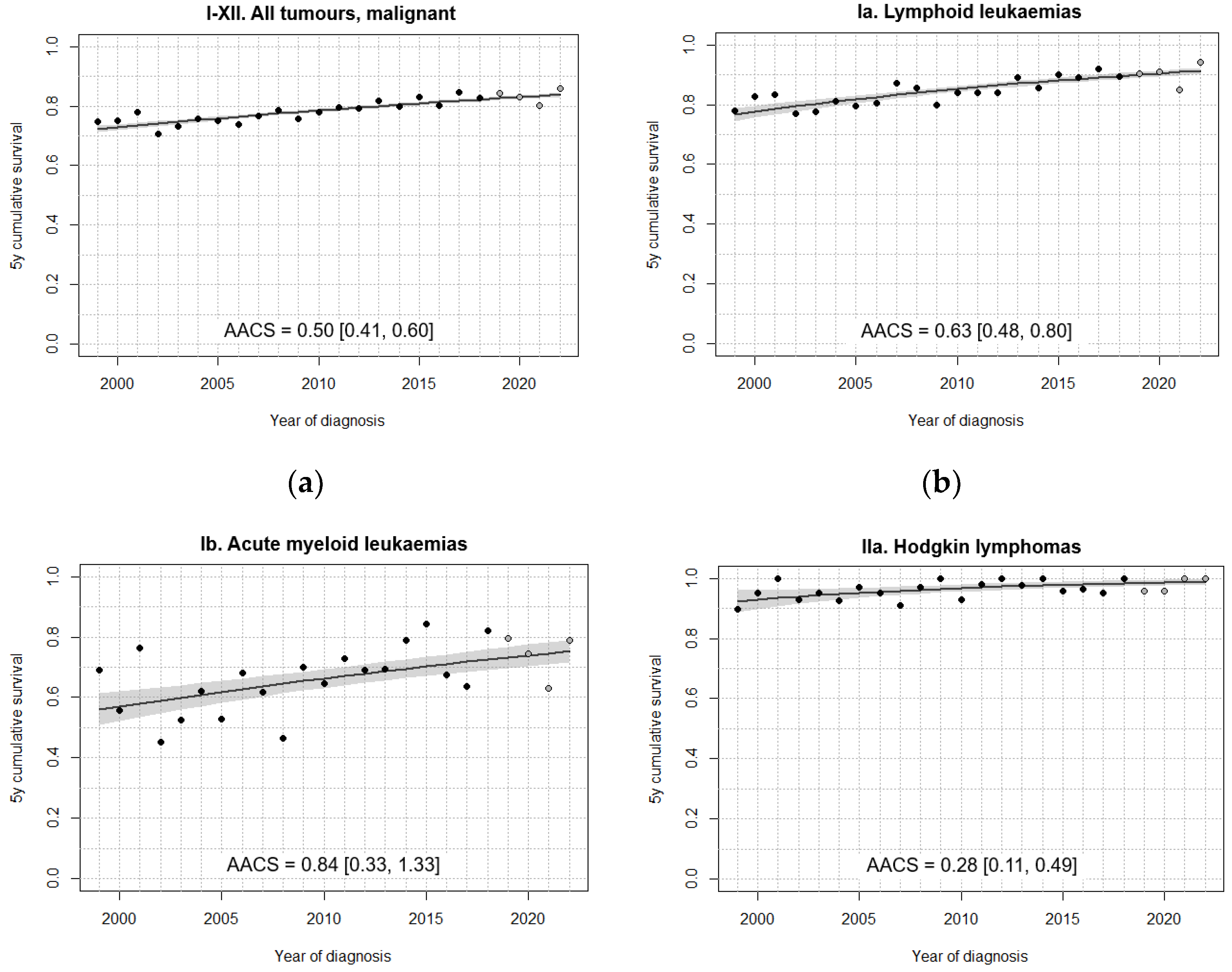
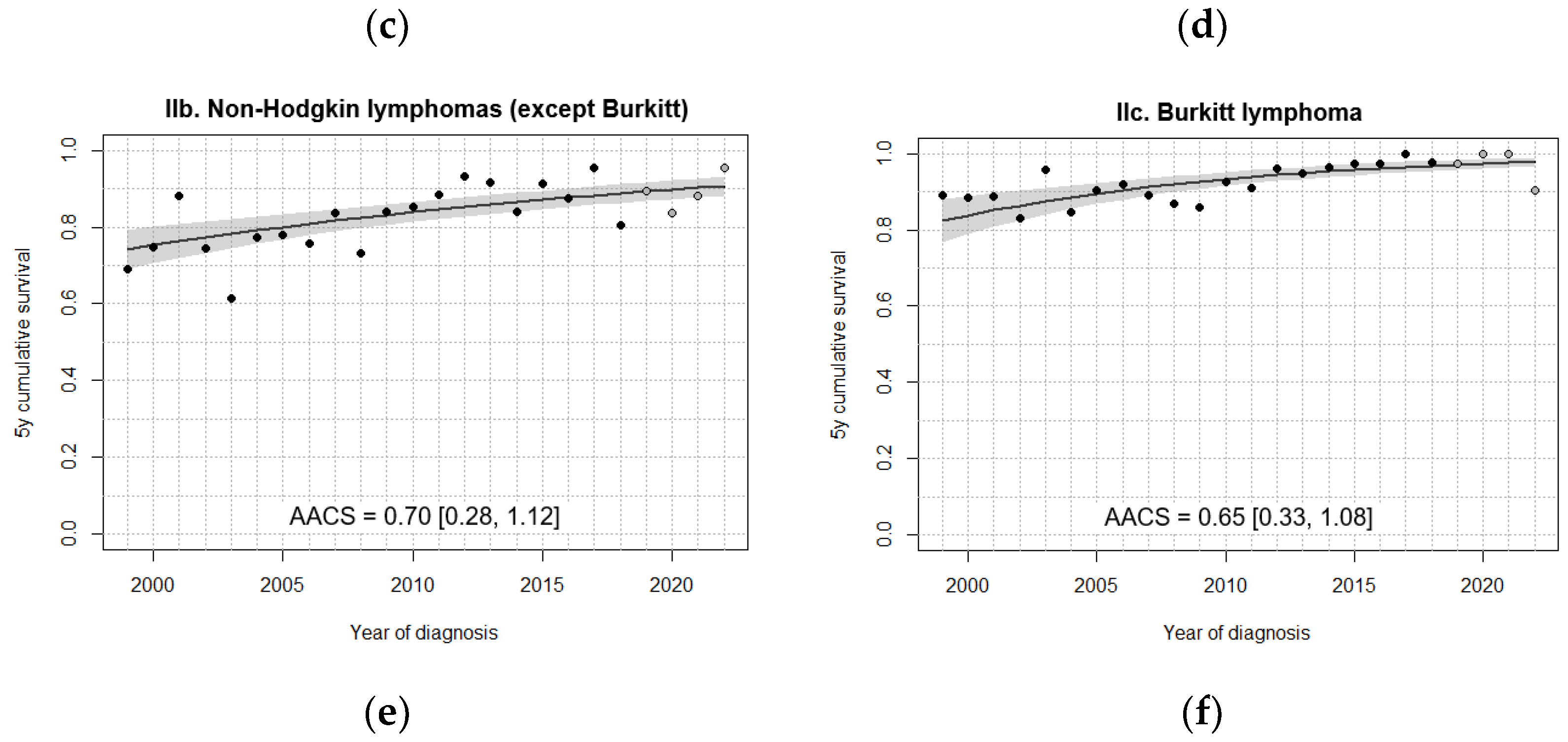
Figure 3.
Fitted trends in 5-year survival for (a-d) selected brain tumours, (e) neuroblastomas and (f) retinoblastomas diagnosed in Spain, 1999-2022, 0-14 years. Age standardisation was performed in all cases except for (f) retinoblastomas. Black dots correspond to annual cohort estimates, while grey dots correspond to annual period estimates. Shaded areas represent 95% confidence bands around the fitted curves. AACS [95% CI]: average absolute change in survival.
Figure 3.
Fitted trends in 5-year survival for (a-d) selected brain tumours, (e) neuroblastomas and (f) retinoblastomas diagnosed in Spain, 1999-2022, 0-14 years. Age standardisation was performed in all cases except for (f) retinoblastomas. Black dots correspond to annual cohort estimates, while grey dots correspond to annual period estimates. Shaded areas represent 95% confidence bands around the fitted curves. AACS [95% CI]: average absolute change in survival.
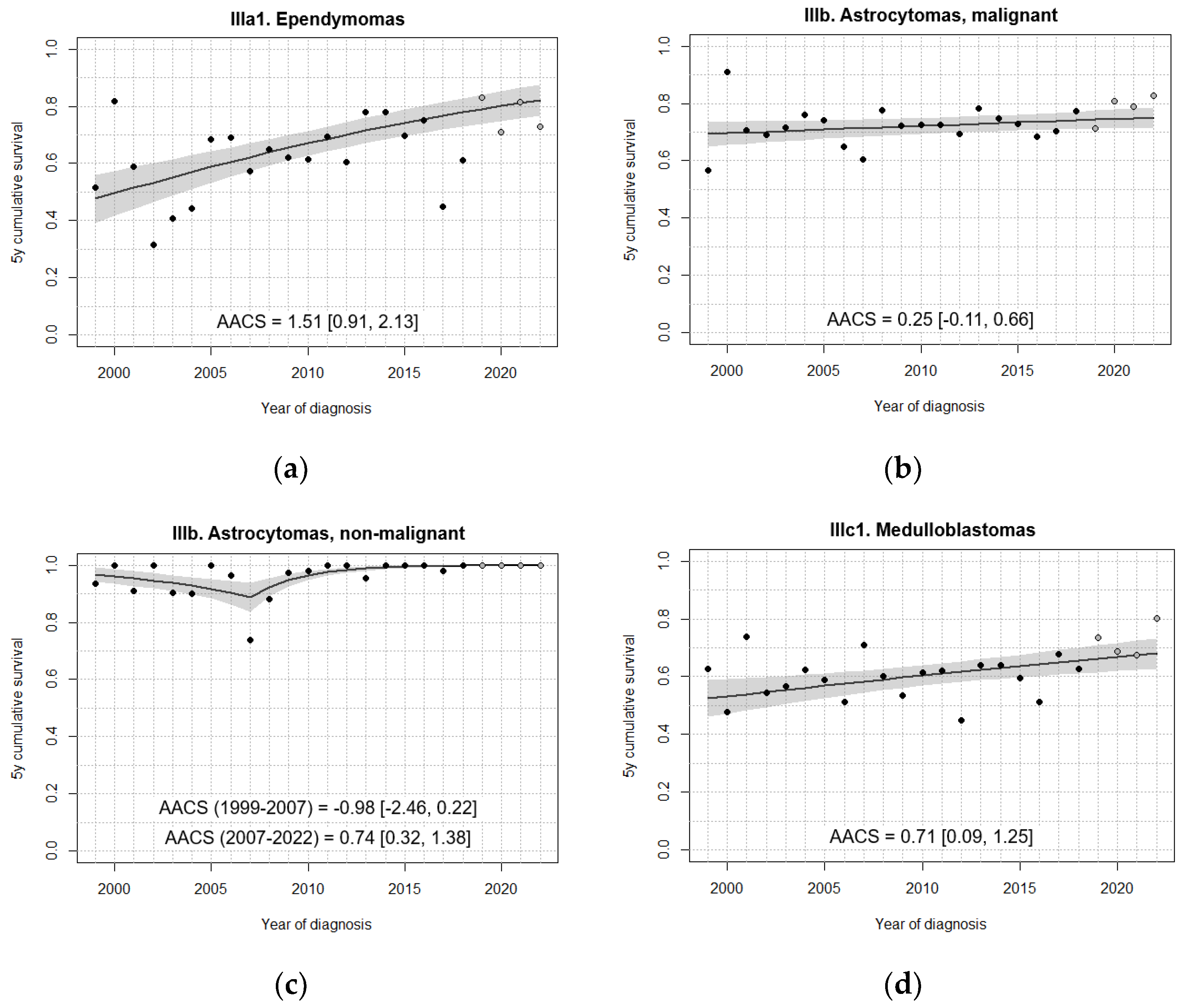
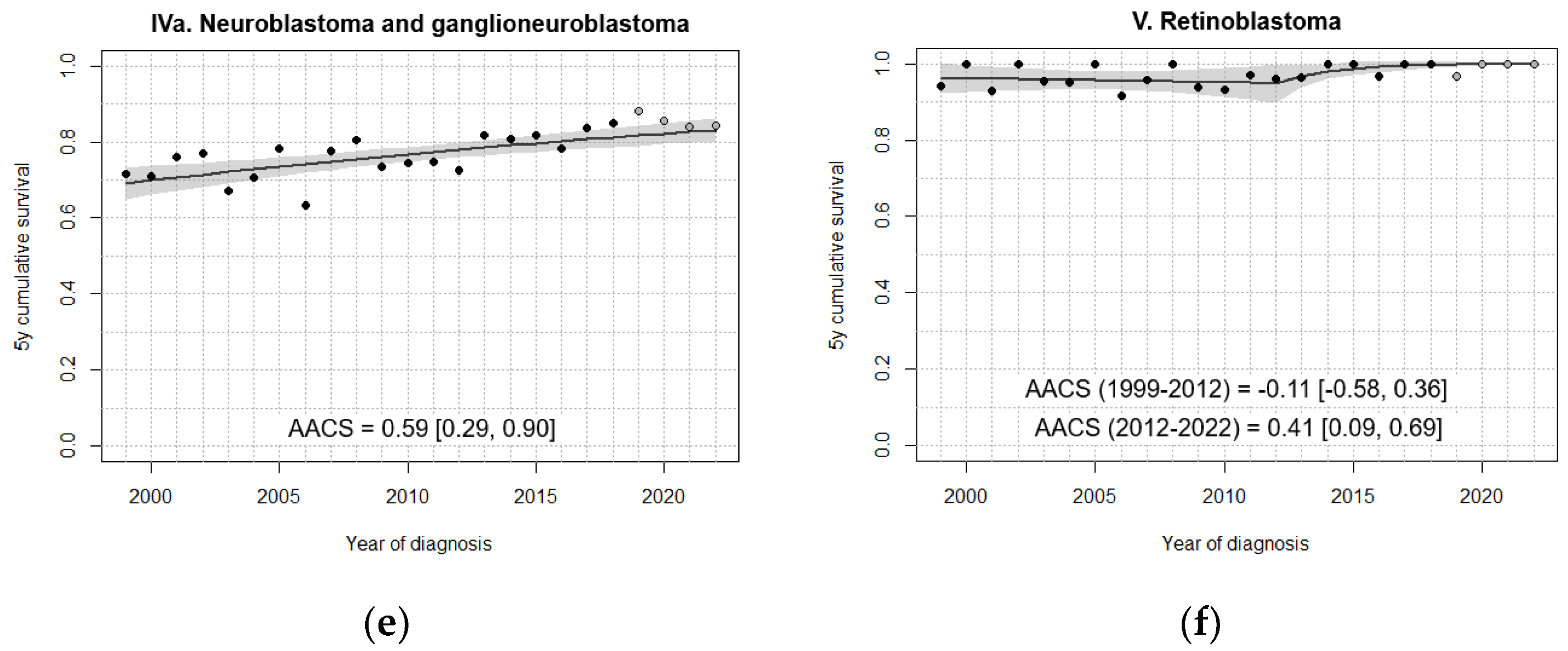
Figure 4.
Fitted trends in 5-year survival for (a) nephroblastoma, (b) hepatoblastoma, (c-d) bone tumours and (e-f) soft tissue sarcomas diagnosed in Spain, 1999-2022, 0-14 years. Age standardisation was performed in all cases except for (b) hepatoblastomas. Black dots correspond to annual cohort estimates, while grey dots correspond to annual period estimates. Shaded areas represent 95% confidence bands around the fitted curves. AACS [95% CI]: average absolute change in survival.
Figure 4.
Fitted trends in 5-year survival for (a) nephroblastoma, (b) hepatoblastoma, (c-d) bone tumours and (e-f) soft tissue sarcomas diagnosed in Spain, 1999-2022, 0-14 years. Age standardisation was performed in all cases except for (b) hepatoblastomas. Black dots correspond to annual cohort estimates, while grey dots correspond to annual period estimates. Shaded areas represent 95% confidence bands around the fitted curves. AACS [95% CI]: average absolute change in survival.

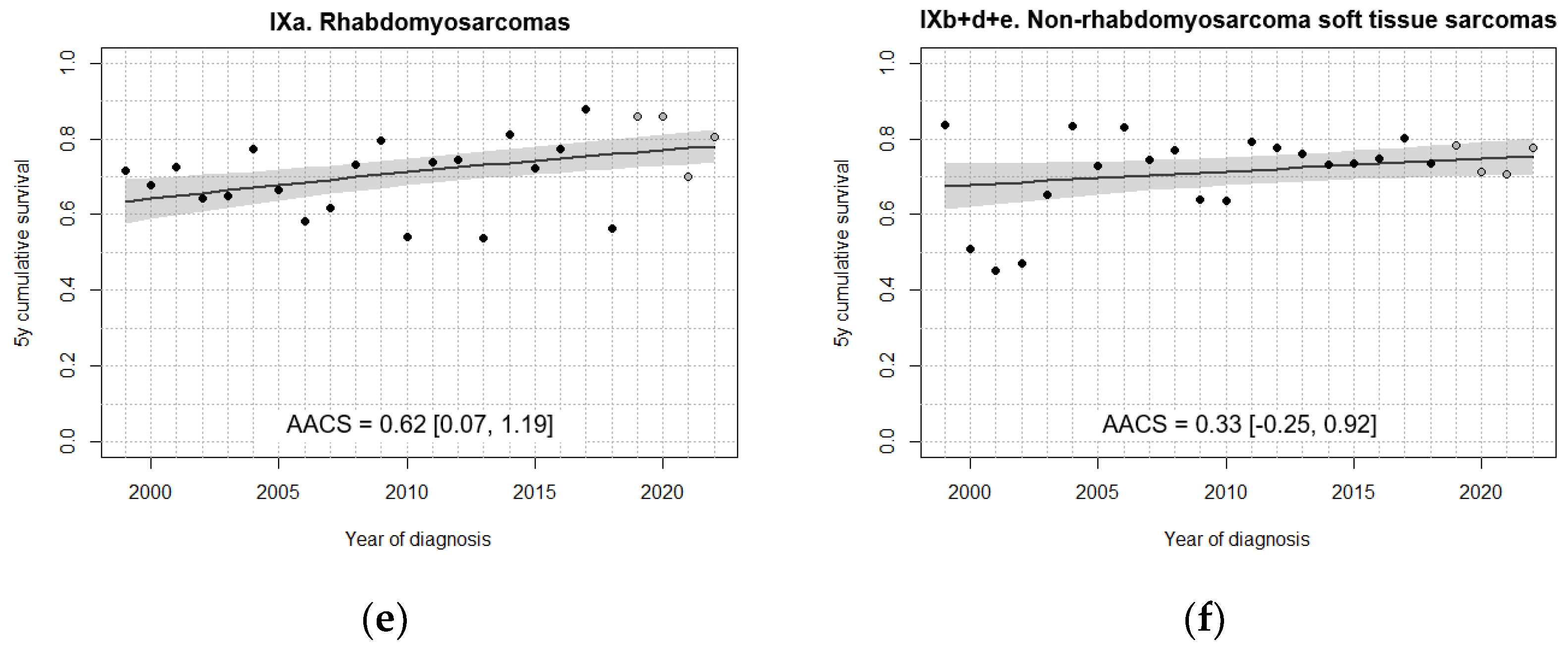
Figure 5.
Fitted trends in 5-year survival for (a-d) germ cell tumours and (e-f) epithelial neoplasms diagnosed in Spain, 1999-2022, 0-14 years. Age standardisation was not performed for (c) extracranial/extragonadal germ cell tumours and (f) thyroid carcinomas. Black dots correspond to annual cohort estimates, while grey dots correspond to annual period estimates. Shaded areas represent 95% confidence bands around the fitted curves. AACS [95% CI]: average absolute change in survival.
Figure 5.
Fitted trends in 5-year survival for (a-d) germ cell tumours and (e-f) epithelial neoplasms diagnosed in Spain, 1999-2022, 0-14 years. Age standardisation was not performed for (c) extracranial/extragonadal germ cell tumours and (f) thyroid carcinomas. Black dots correspond to annual cohort estimates, while grey dots correspond to annual period estimates. Shaded areas represent 95% confidence bands around the fitted curves. AACS [95% CI]: average absolute change in survival.
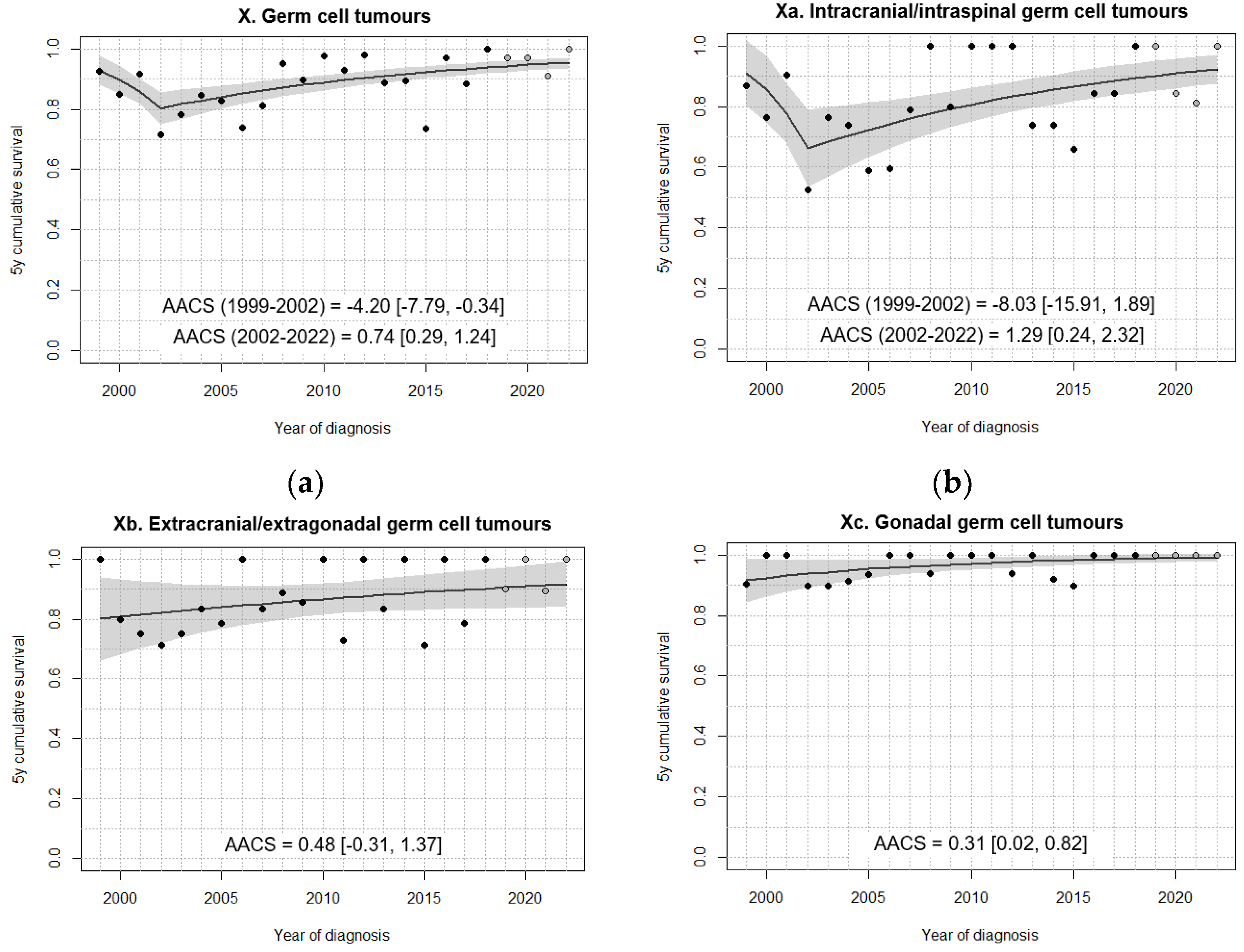
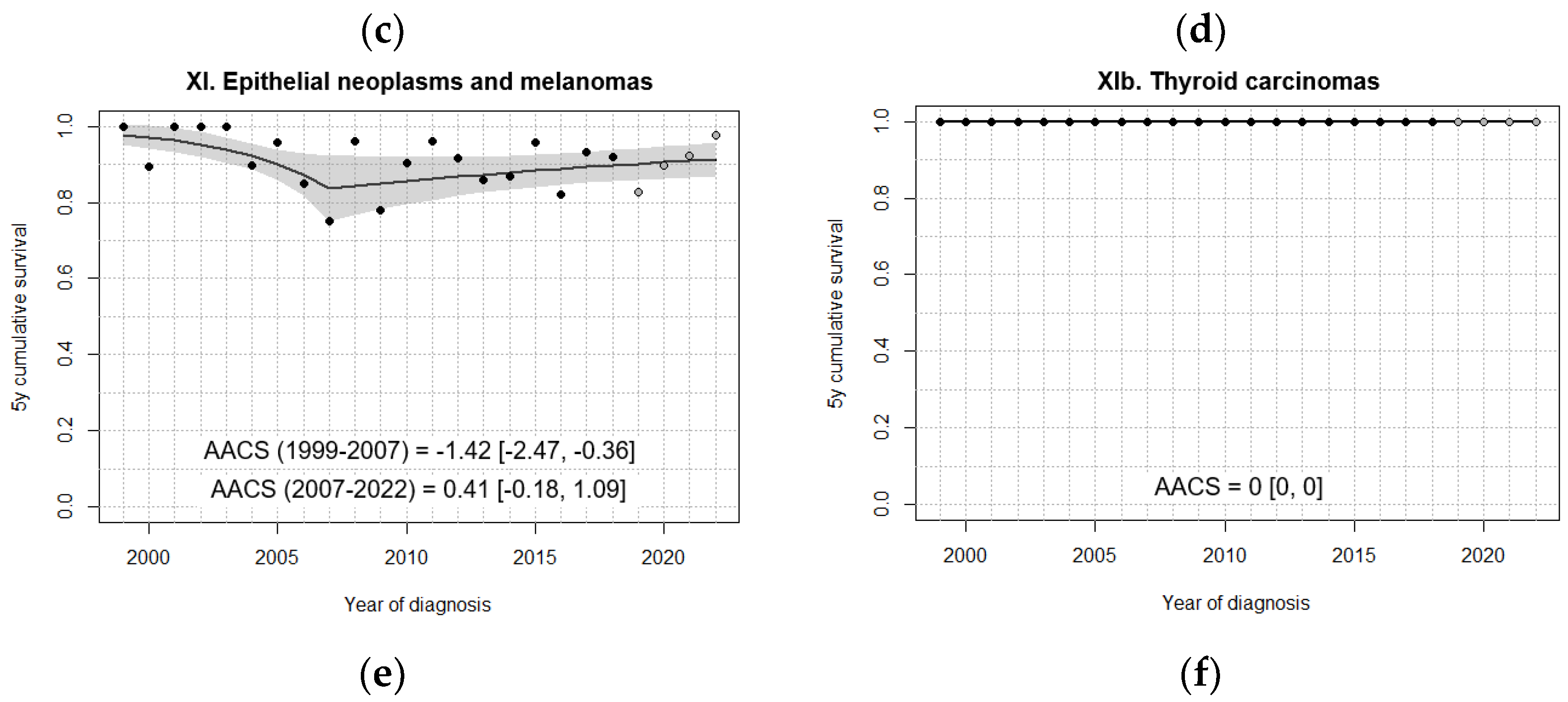

Table 1.
Compliance of RETI-SEHOP registration with IARC quality standards for childhood cancer registries, 1999-2021.
Table 1.
Compliance of RETI-SEHOP registration with IARC quality standards for childhood cancer registries, 1999-2021.
| IARC Quality Indicators | Recommended values | RETI-SEHOP, 1999-2021 |
|---|---|---|
| Microscopically verified cases (%) | 85-98 | 89.5 |
| Cases ascertained from death certificate only (%) | <5 | - |
| Proportion of unspecified cases (NOS %) * | <10 | 2.1 |
| Cases aged 0 years (%) | 5-15 | 10.9 |
| Non-malignant CNS cases (%)† | 20-40 | 32.7 |
Table 2.
Observed 5-year survival and 95% confidence interval by diagnostic groups, 0-14 years.
| Diagnostic group | 5-year OS rate (%) [95% CI] | ||||
|---|---|---|---|---|---|
| 1999-2003 | 2004-2008 | 2009-2013 | 2014-2018 | 2019-2022* | |
| I-XII. All tumours | 75.4 [73.9, 76.9] | 76.6 [75.3, 77.9] | 80.1 [79.0, 81.2] | 83.5 [82.5, 84.5] | 84.6 [83.4, 85.7] |
| I-XII. All tumours, malignant | 74.1 [72.6, 75.7] | 76.1 [74.8, 77.5] | 78.9 [77.7, 80.1] | 82.0 [80.9, 83.1] | 83.1 [81.8, 84.3] |
| I. Leukaemias | 75.8 [72.8, 78.7] | 77.8 [75.4, 80.2] | 82.1 [80.0, 84.1] | 86.7 [85.0, 88.5] | 86.6 [84.6, 88.7] |
| Ia. Lymphoid leukaemias | 79.9 [76.8, 82.9] | 83.0 [80.6, 85.5] | 84.7 [82.6, 86.8] | 89.2 [87.4, 91.0] | 89.8 [87.8, 91.9] |
| Ib. Acute myeloid leukaemias | 59.5 [51.5, 67.5] | 59.3 [52.8, 65.8] | 67.6 [61.3, 73.9] | 75.0 [69.3, 80.6] | 72.5 [65.6, 79.5] |
| II. Lymphomas | 86.4 [83.2, 89.6] | 87.7 [84.8, 90.6] | 93.1 [91.0, 95.2] | 94.0 [92.0, 95.9] | 94.4 [92.2, 96.5] |
| IIa. Hodgkin lymphomas | 94.6 [91.3, 97.8] | 94.0 [90.5, 97.4] | 97.6 [95.5, 99.7] | 97.3 [95.1, 99.4] | 97.8 [95.6, 99.9] |
| IIb. Non-Hodgkin lymphomas (except Burkitt) | 75.7 [68.6, 82.7] | 78.4 [72.0, 84.7] | 88.7 [84.2, 93.3] | 87.0 [82.2, 91.7] | 87.7 [82.4, 93.0] |
| IIc. Burkitt lymphoma | 86.7 [80.6, 92.8] | 90.0 [85.4, 94.7] | 92.4 [88.4, 96.4] | 97.6 [95.3, 99.9] | 97.4 [94.5, 100] |
| III. CNS | 66.6 [63.1, 70.2] | 66.6 [63.5, 69.7] | 70.7 [68.1, 73.3] | 76.0 [73.6, 78.3] | 78.2 [75.6, 80.9] |
| III. CNS, malignant | 54.2 [49.6, 58.8] | 58.6 [54.7, 62.5] | 59.6 [56.2, 63.0] | 63.7 [60.4, 67.1] | 66.2 [62.5, 69.9] |
| III. CNS, non-malignant | 92.3 [88.7, 95.8] | 82.9 [78.7, 87.2] | 94.0 [91.7, 96.4] | 99.1 [98.2, 100] | 99.4 [98.6, 100] |
| IIIa. Ependymomas and choroid plexus tumour | 62.4 [52.3, 72.6] | 62.2 [53.1, 71.3] | 69.8 [61.9, 77.7] | 74.9 [67.6, 82.2] | 78.6 [70.6, 86.5] |
| IIIa. Ependymomas and choroid plexus tumour, malignant | 53.5 [41.9, 65.1] | 57.1 [47.0, 67.2] | 65.3 [56.3, 74.2] | 66.9 [57.6, 76.1] | 72.1 [61.9, 82.3] |
| IIIb. Astrocytomas | 79.9 [75.1, 84.7] | 78.4 [73.8, 82.9] | 85.3 [82.1, 88.6] | 84.7 [81.7, 87.8] | 88.5 [85.3, 91.7] |
| IIIb. Astrocytomas, malignant | 68.9 [61.6, 76.2] | 69.9 [63.3, 76.6] | 74.1 [68.5, 79.6] | 73.2 [68.2, 78.2] | 77.0 [71.1, 83.0] |
| IIIb. Astrocytomas, non-malignant | 94.7 [90.6, 98.8] | 89.7 [84.5, 94.8] | 98.1 [96.3, 99.9] | 99.6 [98.7, 100] | 100 |
| IIIc. Intracranial and intraspinal embryonal tumours | 47.5 [39.6, 55.5] | 54.4 [47.7, 61.0] | 49.5 [43.7, 55.3] | 52.9 [46.3, 59.5] | 63.6 [56.1, 71.1] |
| IIId. Other gliomas | 44.5 [31.3, 57.8] | 50.0 [40.7, 59.3] | 53.8 [45.8, 61.7] | 60.4 [53.1, 67.7] | 50.1 [42.2, 57.9] |
| IV. Peripheral nervous cell tumours | 72.2 [67.5, 76.9] | 73.6 [69.3, 78.0] | 75.7 [71.6, 79.8] | 82.3 [78.6, 86.1] | 85.1 [80.9, 89.3] |
| IVa. Neuroblastoma and ganglioneuroblastoma | 72.1 [67.4, 76.8] | 73.6 [69.3, 78.0] | 75.5 [71.4, 79.7] | 82.0 [78.2, 85.8] | 84.9 [80.6, 89.2] |
| V. Retinoblastoma | 96.9 [93.4, 100] | 96.9 [93.9, 99.9] | 95.4 [92.0, 98.7] | 99.3 [98.0, 100] | 99.0 [97.2, 100] |
| VI. Renal tumours | 87.1 [81.6, 92.5] | 89.2 [85.3, 93.0] | 91.9 [88.7, 95.2] | 93.9 [90.9, 96.9] | 92.5 [88.8, 96.3] |
| VIa. Nephroblastoma | 86.7 [81.1, 92.3] | 89.0 [85.1, 92.9] | 91.8 [88.5, 95.1] | 93.7 [90.6, 96.8] | 92.8 [89.0, 96.6] |
| VII. Hepatic tumours | 69.2 [55.8, 82.7] | 75.1 [64.5, 85.7] | 86.1 [78.1, 94.1] | 74.8 [64.5, 85.2] | 79.8 [68.6, 91.0] |
| VIIa. Hepatoblastoma | 74.4 [60.7, 88.1] | 79.7 [69.4, 89.9] | 86.8 [78.8, 94.9] | 76.6 [65.5, 87.7] | 81.1 [69.3, 92.9] |
| VIII. Malignant bone tumours | 70.8 [65.0, 76.6] | 62.0 [56.1, 67.8] | 71.0 [65.8, 76.2] | 67.9 [62.8, 72.9] | 69.1 [63.4, 74.8] |
| VIIIa. Osteosarcomas | 72.8 [64.2, 81.4] | 63.0 [53.9, 72.0] | 69.8 [61.7, 77.8] | 65.8 [58.1, 73.5] | 69.0 [60.4, 77.7] |
| VIIIc. Ewing tumour and related sarcomas of bone | 68.2 [60.2, 76.3] | 61.8 [54.0, 69.6] | 70.5 [63.4, 77.6] | 67.2 [60.0, 74.5] | 66.2 [58.1, 74.3] |
| IX. Soft tissue sarcomas and other extraosseous sarcomas | 64.0 [57.6, 70.4] | 72.6 [67.1, 78.1] | 69.0 [63.8, 74.3] | 75.9 [71.1, 80.6] | 77.5 [72.2, 82.8] |
| IXa. Rhabdomyosarcomas | 66.5 [58.2, 74.8] | 67.9 [60.1, 75.6] | 67.3 [60.0, 74.7] | 77.5 [70.8, 84.3] | 78.8 [71.3, 86.4] |
| IXb+d+e. Non-rhabdomyosarcoma soft tissue sarcomas | 60.5 [50.4, 70.5] | 78.3 [70.8, 85.9] | 70.7 [63.2, 78.1] | 73.9 [67.1, 80.7] | 75.8 [68.1, 83.4] |
| X. Germ cell tumours | 84.1 [77.3, 90.8] | 86.4 [80.8, 91.9] | 93.4 [89.5, 97.4] | 89.8 [85.3, 94.3] | 96.3 [93.0, 99.5] |
| Xa. Intracranial and intraspinal germ cell tumours | 75.7 [61.9, 89.5] | 73.3 [60.4, 86.3] | 93.8 [86.9, 100] | 81.0 [71.3, 90.7] | 92.7 [84.7, 100] |
| Xb. Extracranial and extragonadal germ cell tumours | 80.0 [65.7, 94.3] | 86.5 [75.4, 97.5] | 86.7 [75.8, 97.6] | 90.2 [81.0, 99.3] | 93.9 [85.8, 100] |
| Xc. Gonadal germ cell tumours | 93.3 [86.1, 100] | 95.3 [90.1, 100] | 98.4 [95.3, 100] | 97.2 [93.3, 100] | 100 |
| XI. Epithelial neoplasms and melanomas | 98.3 [94.8, 100] | 90.6 [84.8, 96.5] | 88.1 [82.0, 94.2] | 90.7 [85.9, 95.5] | 89.8 [84.1, 95.5] |
| XIb. Thyroid carcinomas | 100 | 100 | 100 | 100 | 100 |
* Survival estimates for 2019-2022 were obtained using the period approach, with cases diagnosed across the period 2014-2021. Note: Number of cases by diagnosis cohort: 3,236 in 1999-2003; 4,218 in 2004-2008; 4,959 in 2009-2013; 5,098 in 2014-2018; 3,023 in 2019-2021.
Table 3.
Observed 5-year survival by age group, 2009-2018.
| Diagnostic group | 5-year OS rate (%) [95% CI] | P log-rank |
|||
|---|---|---|---|---|---|
| <1 year | 1-4 years | 5-9 years | 10-14 years | ||
| I-XII. All tumours | 81.4 [79.1, 83.7] | 83.4 [82.1, 84.6] | 81.3 [79.9, 82.8] | 80.5 [79.0, 82.0] | 0.02 |
| I-XII. All tumours, malignant | 80.7 [78.3, 83.1] | 82.4 [81.1, 83.7] | 79.5 [77.9, 81.1] | 78.8 [77.2, 80.5] | 0.005 |
| I. Leukaemias | 60.0 [52.2, 67.8] | 89.7 [88.0, 91.4] | 86.3 [83.9, 88.7] | 77.4 [74.1, 80.7] | <0.0001 |
| Ia. Lymphoid leukaemias | 55.8 [44.8, 66.9] | 91.6 [89.9, 93.2] | 88.5 [86.1, 90.9] | 78.8 [75.0, 82.7] | <0.0001 |
| Ib. Acute myeloid leukaemias | 61.1 [48.9, 73.3] | 74.8 [67.5, 82.2] | 74.2 [66.2, 82.1] | 70.3 [62.4, 78.2] | 0.2 |
| II. Lymphomas | 93.5 [90.0, 97.1] | 94.7 [92.5, 96.8] | 92.7 [90.6, 94.9] | 0.5 | |
| IIa. Hodgkin lymphomas | - | 98.2 [95.8, 100] | 97.0 [95.1, 98.9] | - | |
| IIb. Non-Hodgkin lymphomas (except Burkitt) | 88.1 [81.2, 95.0] | 92.3 [87.9, 96.7] | 83.5 [77.6, 89.4] | 0.06 | |
| IIc. Burkitt lymphoma | 97.7 [94.6, 100] | 94.3 [90.7, 97.9] | 93.6 [88.7, 98.6] | 0.4 | |
| III. CNS | 63.4 [56.0, 70.8] | 74.0 [71.0, 77.0] | 71.1 [68.1, 74.1] | 79.0 [75.6, 82.4] | <0.0001 |
| III. CNS, malignant | 47.7 [38.3, 57.1] | 65.5 [61.7, 69.3] | 58.1 [54.0, 62.1] | 65.6 [60.4, 70.8] | <0.0001 |
| III. CNS, non-malignant | 94.6 [88.5, 100] | 96.9 [94.6, 99.2] | 96.1 [93.9, 98.2] | 97.8 [96.0, 99.7] | 0.5 |
| IIIa. Ependymomas and choroid plexus tumour | 51.5 [34.5, 68.6] | 67.2 [58.7, 75.8] | 81.0 [71.3, 90.7] | 86.7 [77.5, 95.9] | 0.0003 |
| IIIa. Ependymomas and choroid plexus tumour, malignant | 31.8 [12.4, 51.3] | 63.4 [54.1, 72.7] | 76.5 [64.8, 88.1] | 81.3 [67.7, 94.8] | <0.0001 |
| IIIb. Astrocytomas | 81.1 [70.6, 91.7] | 92.1 [89.3, 95.0] | 81.9 [77.9, 85.8] | 80.0 [74.6, 85.3] | 0.0001 |
| IIIb. Astrocytomas, malignant | 72.7 [57.5, 87.9] | 87.7 [83.2, 92.2] | 65.8 [59.1, 72.5] | 61.0 [51.9, 70.1] | <0.0001 |
| IIIb. Astrocytomas, non-malignant | 95.0 [85.5, 100] | 98.6 [96.6, 100] | 98.9 [97.4, 100] | 100 | 0.3 |
| IIIc. Intracr/intrasp embryonal tumours | 27.5 [13.7, 41.3] | 44.4 [37.4, 51.3] | 56.9 [49.7, 64.1] | 64.8 [54.5, 75.2] | <0.0001 |
| IIId. Other gliomas | 72.1 [63.0, 81.2] | 41.5 [33.2, 49.7] | 65.5 [55.9, 75.0] | <0.0001 | |
| IV. Peripheral nervous cell tumours | 92.3 [89.6, 95.0] | 68.1 [63.3, 73.0] | 63.2 [52.0, 74.5] | 86.4 [72.0, 100] | <0.0001 |
| IVa. Neuroblastoma/ganglioneuroblastoma | 92.3 [89.5, 95.0] | 68.0 [63.1, 72.8] | 62.1 [50.7, 73.6] | 82.4 [64.2, 100] | <0.0001 |
| V. Retinoblastoma | 97.6 [94.8, 100] | 97.0 [94.3, 99.6] | - | - | - |
| VI. Renal tumours | 89.5 [83.0, 96.0] | 94.7 [92.1, 97.3] | 91.4 [86.6, 96.3] | 91.3 [79.8, 100] | 0.3 |
| VIa. Nephroblastoma | 89.5 [83.0, 96.0] | 94.6 [92.0, 97.3] | 91.0 [85.9, 96.1] | 88.2 [72.9, 100] | 0.2 |
| VII. Hepatic tumours | 78.7 [66.3, 91.1] | 93.5 [87.3, 99.7] | 72.2 [51.5, 92.9] | 47.1 [23.3, 70.8] | 0.0002 |
| VIIa. Hepatoblastoma | 77.6 [64.7, 90.5] | 93.2 [86.7, 99.6] | 75.0 [53.8, 96.2] | - | - |
| VIII. Malignant bone tumours | 65.0 [50.2, 79.8] | 75.0 [68.8, 81.2] | 67.1 [62.4, 71.8] | 0.2 | |
| VIIIa. Osteosarcomas | - | 70.0 [59.8, 80.3] | 67.5 [60.8, 74.2] | - | |
| VIIIc. Ewing tumour and related sarcomas of bone | 66.7 [49.8, 83.5] | 76.6 [68.4, 84.8] | 64.9 [58.1, 71.7] | 0.1 | |
| IX. Soft tissue sarcomas and other extraosseous sarcomas | 68.3 [57.1, 79.5] | 74.2 [67.8, 80.6] | 76.5 [69.9, 83.0] | 69.3 [63.0, 75.6] | 0.3 |
| IXa. Rhabdomyosarcomas | 80.0 [62.5, 97.5] | 74.4 [66.8, 82.1] | 73.6 [64.6, 82.7] | 64.1 [52.7, 75.6] | 0.3 |
| IXb+d+e. Non-rhabdomyosarcoma STS | 63.3 [49.4, 77.2] | 72.0 [59.6, 84.5] | 80.1 [70.7, 89.4] | 71.6 [64.1, 79.2] | 0.1 |
| X. Germ cell tumours | 89.4 [81.4, 97.4] | 86.8 [78.2, 95.3] | 91.6 [85.6, 97.5] | 94.5 [90.5, 98.5] | 0.3 |
| Xa. Intracr/intrasp germ cell tumours | - | 89.4 [80.6, 98.2] | 90.5 [82.5, 98.4] | - | |
| Xb. Extracranial and extragonadal germ cell tumours | 89.1 [79.0, 99.2] | 82.0 [67.6, 96.3] | - | - | - |
| Xc. Gonadal germ cell tumours | 100 | 100 | 92.9 [83.3, 100] | 98.5 [95.5, 100] | 0.2 |
| XI. Epithelial neoplasms and melanomas | 70.4 [51.9, 88.8] | 89.2 [82.0, 96.3] | 92.8 [88.7, 96.9] | 0.003 | |
| XIb. Thyroid carcinomas | - | 100 | 100 | - | |
Note: cases younger than 5 years were pooled into a single group when either age group (0 or 1-4 years) did not reach 15 cases in the 2009-2018 cohort.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



