
Submitted:
31 December 2025
Posted:
01 January 2026
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Although self-administered antigen tests are widely available, anatomical knowledge of nasal anatomy in the general population is limited. Cerebrospinal fluid leakage has been reported in multiple cases following damage to the roof of the nasal cavity due to accidental penetration of the cribriform plate of the ethmoid bone. Methods: Images of anatomical prosections used for teaching in the Dissection Room of the Faculty of Medicine of the University of Barcelona were obtained to illustrate the viable horizontal pathway to the nasopharynx through the inferior meatus, below the inferior turbinate. Screenshots from publicly available videos produced by the author demonstrating swab insertion were analyzed to measure the final insertion angle using 3D software. Publicly available instructions for patients included with authorized antigen tests in Spain were reviewed. Results: Antigen tests available in Spain in 2025 recommended a predominantly vertical swab insertion. However, successful horizontal insertion in the inferior meatus towards the nasopharynx can be achieved with a slight vertical angle of 7–9°. A schematic illustration for free use is provided. Conclusion: Swab instructions should be revised to emphasize an insertion perpendicular to the face in order to access the inferior meatus safely and reduce the risk of injury to the ethmoidal cells.
Keywords:
COVID-19 antigen test
; swab
; lamina cribrosa
1. Introduction
During the early stages of the pandemic, the technique for performing nasopharyngeal tests was clearly established [1,2]. However, as a significant number of instructional YouTube videos were found to be incorrect [3], our team prepared an illustrative video demonstrating the correct insertion into the inferior meatus [4]. This technique involves an initial perpendicular insertion of the swab in relation to the face, followed by a slight reorientation of approximately 7-9º cephalad, without cervical hyperextension.
The present communication aims to: 1) review the authorized antigen tests [5] and their corresponding patient instructions [6,7,8,9,10,11,12,13]; and 2) provide free open-access images and schema of the nasal cavity. These images are intended to aid in the proper introduction of the swab into the inferior meatus, minimizing damage to surrounding structures, in order to reliably reach the nasopharynx, the area with the highest viral load [14]. This is particularly relevant given that multiple cases of cerebrospinal fluid leakage have been reported following damage to the cribriform plate at the roof of the nasal cavity.
2. Materials and Methods
2.1. Prosections and illustrative graphic proposal.
Written consent for research and educational purposes is obtained from donors during their registration with the Body Donation Service of the Faculty of Medicine and Health Sciences at the University of Barcelona. Following their entry into the program, all ex vivo samples are fully anonymized.
Permission was granted by the Director of the Body Donation Service at the University of Barcelona to capture illustrative images from anonymized ex vivo nasal specimens used for teaching within the Faculty.
Coronal, sagittal, and parasagittal views of the nasal cavity were obtained, both with and without the nasal septum. In these images, key anatomical landmarks were outlined: the anterior, superior, and inferior boundaries of the nasal cavity, as well as the profiles of the inferior, middle, and superior turbinates. This was done to later create a graphical schema for potential use in patient instructions for antigen tests.
2.2. Introduction of the antigen test swab.
For illustrative purposes during the pandemic, a video was recorded demonstrating the introduction of a swab into the nasal cavity of one of the authors (seated, without cervical extension). This video was distributed to media outlets [4].
From this recording, screenshots were extracted to analyze the swab's orientation. Using Amira software, a horizontal reference line, perpendicular to the ground, was superimposed on the images. The facial axis was defined by a line connecting the superior orbital margin to the chin.
Two angles were then measured: 1) the angle between the facial axis and the horizontal reference line (perpendicular to the ground), and 2) the angle between this horizontal reference line and the swab itself (Figure 1)
2.3. Review of the instructions per patients of COVID antigen test
3. Results
3.1. Nasal cavity anatomical dissections.
Anatomical dissection images illustrating lateral (Figure 2A) and coronal (Figure 3) views of the nasal cavity were obtained. Notably, only a horizontal insertion angle (Figure 2B, green arrow) permits advancement along the inferior meatus—the narrow passage situated beneath the inferior turbinate (Figure 3).
3.2. Swab Insertion Technique
The facial axis was measured at an angle of 11º relative to the vertical plane. The optimal final insertion angle for the swab, which led to successful passage, was measured at 7–9º relative to the horizontal plane (Figure 1).
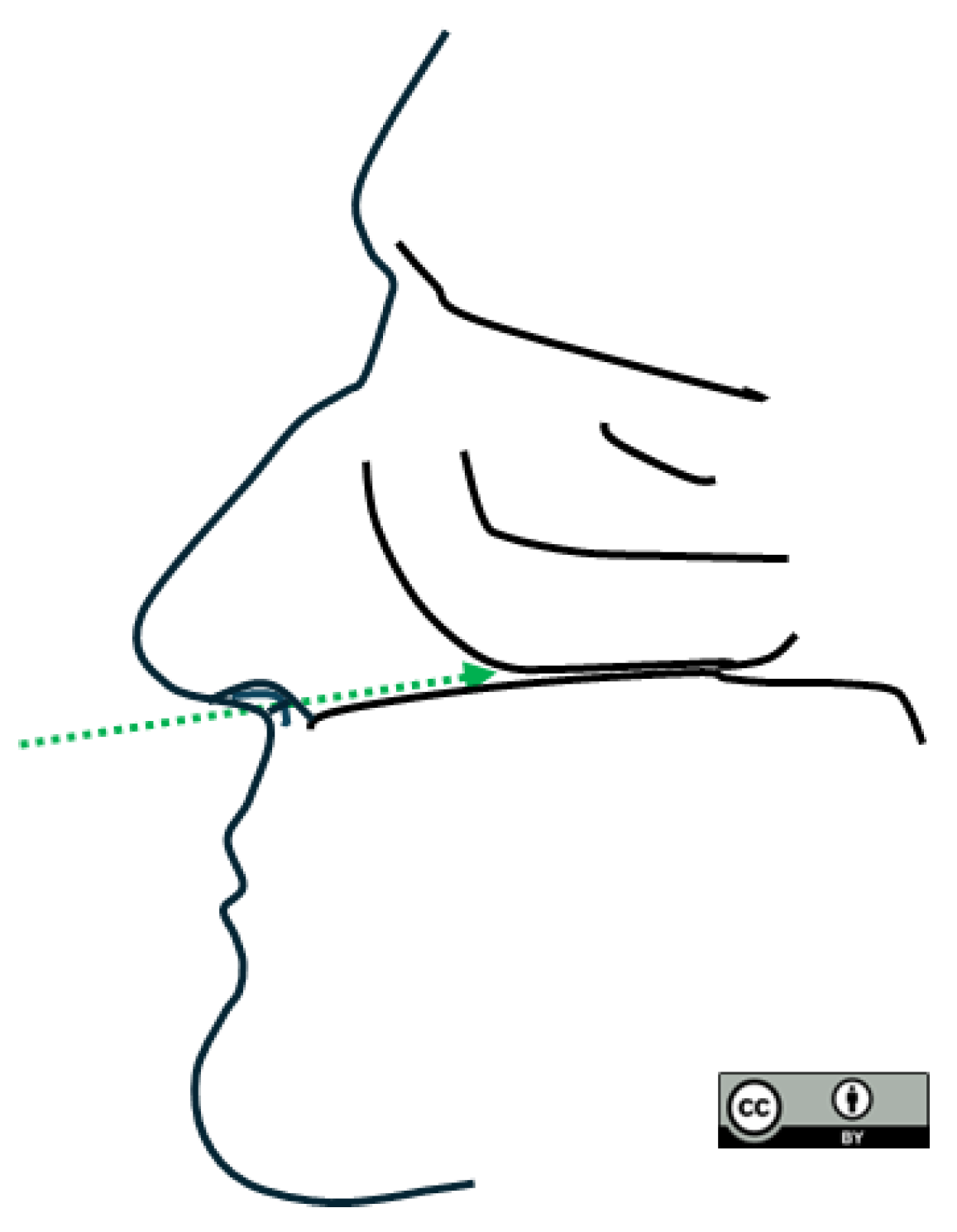
A composite schematic, created by outlining key anatomical features from the dissection images and video screenshot, is presented in Figure 4.
3.3. Review of the instructions for available antigen tests
4. Discussion
Early evidence from the pandemic indicated a higher viral load in nasal samples—specifically those taken from the middle turbinate and nasopharynx—compared to oral samples [14].
While antigen tests became widely available to the general public in 2020, their initial performance was highly variable. An early 2020 Cochrane systematic review reported an average sensitivity of only 56.2%, with a range of 34% to 91% depending on the brand [15]. More recent reviews (2022–2025) confirm that this wide range in sensitivity persists even when tests are used according to manufacturer instructions [16], becoming a public health threat if many false negatives become undiagnosed.
Nevertheless, patients have reported difficulties in sample collection [17] and severe side effects, including CSF rhinorrhea caused by violation of the bony skull base through the lamina cribrosa [18,19,20,21], as well as meningitis [22]; additional cases have been recently reviewed [23]. If the swab is inserted vertically, or horizontally in a patient with cervical spine extension, following the patient instructions included with antigen tests marketed between 2020 and 2025, the swab may be directed toward the roof of the nasal cavity, where the fragile lamina cribrosa could be damaged.
Samples obtained from the mid-turbinate show comparable sensitivity to nasopharyngeal samples in children [24], in whom fragile nasal walls could increase the risk of side effects. PCR or antigen testing performed using nasopharyngeal lavage with isotonic saline has also been described as an alternative method to avoid discomfort while maintaining high sensitivity rates [25].
5. Conclusions
We recommend inserting the swab primarily horizontally, with a slight upward angulation of about 8º, and with the patient seated without neck extension. In cases where this standard technique is not feasible, such as with uncooperative small children, alternative methods like nasal lavage with saline prior to antigen testing should be considered.
Freely available images are provided for use in the development of updated patient instructions for antigen testing.
Funding
This research received no external funding.
Institutional Review Board Statement
The use of atlas-like non identifiable images from ex-vivo samples used in the teaching of the medical school in which no interventions were made was conducted in accordance with the Declaration of Helsinki, and approved by the Head of the Donor Service of the Faculty of Medicine and Heatlh Sciences -campus Clínic- of the University of Barcelona.
Informed Consent Statement
Written consent for research and docent purposes is obtained from living donors when being registered in the Donor Service of the Faculty of Medicine and Health Sciences of the University of Barcelona. However, after their entry into the service, the ex-vivo sam-ples remain unidentifiable and no further specific consent is available.
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author(s).
Acknowledgments
The author thanks Professor of Anatomy of the University of Barcelona Alberto Prats-Galino for valuable discussion, the dissection room staff (Natalia Durán and Manuel Martín) for collaborating in the handling of the specimens and Pepa Montes Anglada for swab introduction in the video.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CG | Crista galli |
| EPL | Ethmoidal perpendicular lamina |
| EC | Ethmoidal cells |
| FS | Frontal sinus |
| IM | Inferior meatus |
| IT | Inferior turbinate |
| MM | Middle meatus |
| MT | Mid-turbinate |
| NC | Nasal cartilage |
| NPH | Nasopharynx |
| PB | Horizontal plate of palatine bone |
| ST | Superior turbinate |
| SS | Sphenoidal sinus |
| V | Vomer bone |
References
- Marty FM, Chen K, Verrill KA. How to Obtain a Nasopharyngeal Swab Specimen. N Engl J Med. 2020 May 28;382(22):e76.
- NEJM Group. https://youtu.be/DVJNWefmHjE?feature=shared [accessed September 21, 2025].
- Itamura K, Wu A, Illing E, Ting J, Higgins T. YouTube Videos Demonstrating the Nasopharyngeal Swab Technique for SARS-CoV-2 Specimen Collection: Content Analysis. JMIR Public Health Surveill. 2021 Jan 14;7(1):e24220. PMID: 33406478; PMCID: PMC7813578. [CrossRef]
- Ciència i Tecnologia. Demostració: com s'ha de col·locar el palet en un test d'antígens? https://www.regio7.cat/videos/ciencia-i-tecnologia/2021/12/23/demostracio-com-sha-collocar-palet-60978647.html [accessed December 21, 2025.
- https://www.aemps.gob.es/la-aemps/ultima-informacion-de-la-aemps-acerca-del-covid-19/informacion-general-sobre-tests-de-diagnostico-de-covid-19/?lang=en [accessed on December 21, 2025].
- https://www.assuretech-product.com/infectious-disease-tests/covid-19-tests/sars-cov-2-antigen-rapid-tests-for-self.html, minute 2:00, [accessed on December 21, 2025].
- https://farmaferoles.com/wp-content/uploads/2022/12/fluorecare_test_nasal_rapido_antigenos_covid19__gripe_a_b__vrs_instrucciones.pdf [accessed on December 21, 2025].
- https://www.medomics-dx.net/product/SARS-CoV-2--26-Influenza-AB--26-RSV-Antigen-Combo-Rapid-Test-Kit--LFIA--518.html [accessed on December 21, 2025].
- https://aidentiapreventix.com/wp-content/uploads/ES-IFU-Rapid-COVID-19-Antigen-Test-Colloidal-Gold-Nasal-Swab-V2.16.pdf [accessed on December 21, 2025].
- https://www.grupotristan.es/wp-content/uploads/2022/09/IFU-P213106-P213107-P213109-EZER-Flu-COVID-19-Antigen-Duo-ES.pdf [accessed on December 21, 2025].
- https://unahealth.co.uk/wp-content/uploads/146555702-ISIR-535-Beright-CE-EN-PI.pdf [accessed on December 21, 2025].
- https://cordx.com/wp-content/uploads/2022/07/CorDx-FluABCOVID-19RSV-4%E5%90%881-%E8%81%94%E5%8D%A1-210x285mm.pdf [accessed on December 21, 2025].
- https://www.certest.es/wp-content/uploads/2021/12/IU-SC80001P-Self-Test-ES-23.12.21.pdf [accessed on December 21, 2025].
- Zou L, Ruan F, Huang M, Liang L, Huang H, Hong Z, Yu J, Kang M, Song Y, Xia J, Guo Q, Song T, He J, Yen HL, Peiris M, Wu J. SARS-CoV-2 Viral Load in Upper Respiratory Specimens of Infected Patients. N Engl J Med. 2020 Mar 19;382(12):1177-1179. Epub 2020 Feb 19. PMID: 32074444; PMCID: PMC7121626. [CrossRef]
- Dinnes, J.; Deeks, J.J.; Berhane, S.; Taylor, M.; Adriano, A.; Davenport, C.; Dittrich, S.; Emperador, D.; Takwoingi, Y.; Cunningham, J.; et al. Cochrane COVID-19 Diagnostic Test Accuracy Group 2. Rapid point-of-care antigen and molecular-based tests for diagnosis of SARS-CoV-2 infection. Cochrane Database Syst. Rev. 2021, 3, CD013705.
- Dinnes J, Sharma P, Berhane S, van Wyk SS, Nyaaba N, Domen J, Taylor M, Cunningham J, Davenport C, Dittrich S, Emperador D, Hooft L, Leeflang MM, McInnes MD, Spijker R, Verbakel JY, Takwoingi Y, Taylor-Phillips S, Van den Bruel A, Deeks JJ; Cochrane COVID-19 Diagnostic Test Accuracy Group. Rapid, point-of-care antigen tests for diagnosis of SARS-CoV-2 infection. Cochrane Database Syst Rev. 2022 Jul 22;7(7):CD013705. Update in: Cochrane Database Syst Rev. 2025 Nov 28;11:CD013705. doi: 10.1002/14651858.CD013705.pub4. [CrossRef]
- Kohmer N, Eckermann L, Böddinghaus B, Götsch U, Berger A, Herrmann E, Kortenbusch M, Tinnemann P, Gottschalk R, Hoehl S, Ciesek S. Self-Collected Samples to Detect SARS-CoV-2: Direct Comparison of Saliva, Tongue Swab, Nasal Swab, Chewed Cotton Pads and Gargle Lavage. J Clin Med. 2021 Dec 8;10(24):5751. PMID: 34945047; PMCID: PMC8709431. [CrossRef]
- Paquin R, Ryan L, Vale FL, Rutkowski M, Byrd JK. CSF Leak After COVID-19 Nasopharyngeal Swab: A Case Report. Laryngoscope. 2021 Sep;131(9):1927-1929. Epub 2021 Feb 20. [CrossRef]
- Ku J, Chen CY, Ku J, Chang HK, Wu JC, Yen YS. Iatrogenic cerebrospinal fluid leak after repeated nasal swab tests for COVID-19: illustrative case. J Neurosurg Case Lessons. 2021 Oct 25;2(17):CASE21421. [CrossRef]
- Sullivan CB, Schwalje AT, Jensen M, Li L, Dlouhy BJ, Greenlee JD, Walsh JE. Cerebrospinal Fluid Leak After Nasal Swab Testing for Coronavirus Disease 2019. JAMA Otolaryngol Head Neck Surg. 2020 Dec 1;146(12):1179-1181. doi: 10.1001/jamaoto.2020.3579. Erratum in: JAMA Otolaryngol Head Neck Surg. 2020 Dec 1;146(12):1181. [CrossRef]
- Samadian M, Maroufi SF, Taheri MS, Jafari A. CSF rhinorrhea after nasopharyngeal swab testing for COVID-19: A case report and review of literature. Otolaryngol Case Rep. 2021 Nov;21:100370. [CrossRef]
- Alberola-Amores FJ, Valdeolivas-Urbelz E, Torregrosa-Ortiz M, Álvarez-Sauco M, Alom-Poveda J. Meningitis due to cerebrospinal fluid leak after nasal swab testing for COVID-19. Eur J Neurol. 2021 Nov;28(11):e91-e92. Epub 2021 Feb 12. [CrossRef]
- Samargandy SA, Fritz CG, Ahmadian D, Bhalla V, Lee JM, Le CH. Traumatic CSF rhinorrhea associated with COVID-19 testing: a case series and systematic review. Eur Arch Otorhinolaryngol. 2025 Jan;282(1):193-205. [CrossRef]
- Vos MB, Gonzalez MD, Stone C, Cleeton R, Figueroa J, Jerris R, Park SI, Heilman S, Nayee R, Chahroudi A, Schoof N, Mavigner M, Morris CR, Leong T, Grindle A, Westbrook A, Lam W, Rogers BB. Comparison of Mid-turbinate Nasal Swabs, Saliva, and Nasopharyngeal Swabs for SARS-CoV-2 Reverse Transcription-Polymerase Chain Reaction Testing in Pediatric Outpatients. Arch Pathol Lab Med. 2022 Sep 1;146(9):1056-1061. [CrossRef]
- Frezza D, Fabbris C, Franz L, Vian E, Rigoli R, De Siati R, Emanuelli E, Bertinato L, Boscolo-Rizzo P, Spinato G. A Severe Acute Respiratory Syndrome Coronavirus 2 detection method based on nasal and nasopharyngeal lavage fluid: A pilot feasibility study. Laryngoscope Investig Otolaryngol. 2021 Jul 27;6(4):646-649.
Figure 1.
Swab introduction. Rather than a vertical insertion, a horizontal approach with a slight vertical orientation (7-9º) allows a successful introduction of the swab into the inferior meatus to reach the nasopharynx. .
Figure 1.
Swab introduction. Rather than a vertical insertion, a horizontal approach with a slight vertical orientation (7-9º) allows a successful introduction of the swab into the inferior meatus to reach the nasopharynx. .
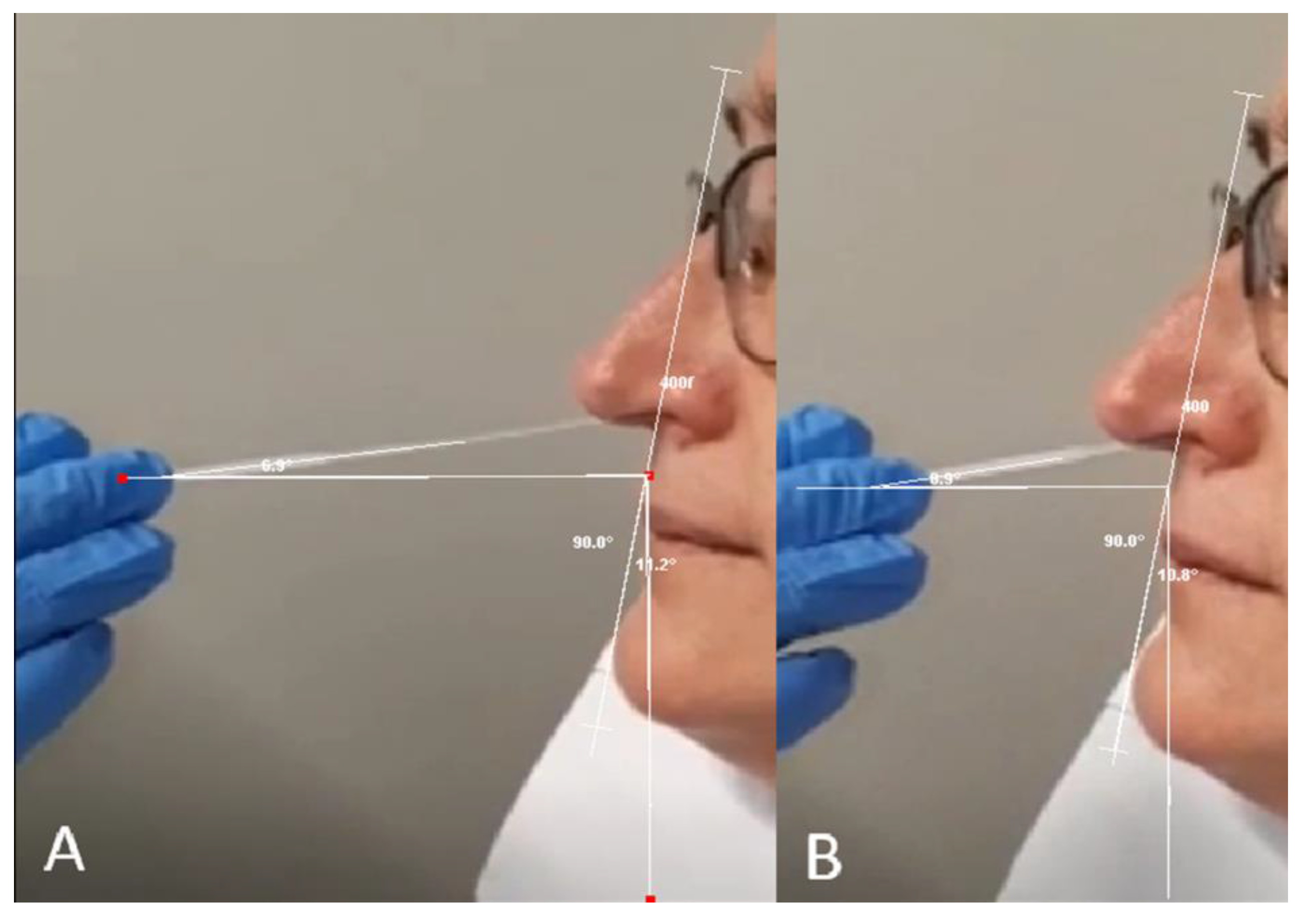
Figure 2.
A. Lateral view of the nasal septum is shown, comprising the nasal cartilage (nc), the vomer bone (v), and the perpendicular plate of the ethmoid bone (epl). Superiorly, the crista galli (cg) process is visible posterior to the frontal sinus (fs). The posterior boundary of the nasal cavity is formed by the sphenoidal sinus (ss) and the nasopharynx (nph). B. Lateral wall of the nasal cavity. The floor of the nasal cavity is formed by the maxillary bone (mb) and the horizontal plate of palatine bone (pb). The tongue (t) occupies the oral cavity inferiorly. The nasal septum has been removed to reveal the nasal mucosa covering the inferior, middle, and superior turbinates (it, mt, and st, respectively). Potential swab trajectories are illustrated. Only the green pathway follows the inferior meatus—the narrow passage beneath the inferior turbinate—which leads to the nasopharynx. Alternative trajectories contact the middle turbinate (yellow) or risk impinging upon the ethmoidal air cells (red), resulting in greater patient discomfort and a lower likelihood of obtaining a sample with high viral load.
Figure 2.
A. Lateral view of the nasal septum is shown, comprising the nasal cartilage (nc), the vomer bone (v), and the perpendicular plate of the ethmoid bone (epl). Superiorly, the crista galli (cg) process is visible posterior to the frontal sinus (fs). The posterior boundary of the nasal cavity is formed by the sphenoidal sinus (ss) and the nasopharynx (nph). B. Lateral wall of the nasal cavity. The floor of the nasal cavity is formed by the maxillary bone (mb) and the horizontal plate of palatine bone (pb). The tongue (t) occupies the oral cavity inferiorly. The nasal septum has been removed to reveal the nasal mucosa covering the inferior, middle, and superior turbinates (it, mt, and st, respectively). Potential swab trajectories are illustrated. Only the green pathway follows the inferior meatus—the narrow passage beneath the inferior turbinate—which leads to the nasopharynx. Alternative trajectories contact the middle turbinate (yellow) or risk impinging upon the ethmoidal air cells (red), resulting in greater patient discomfort and a lower likelihood of obtaining a sample with high viral load.
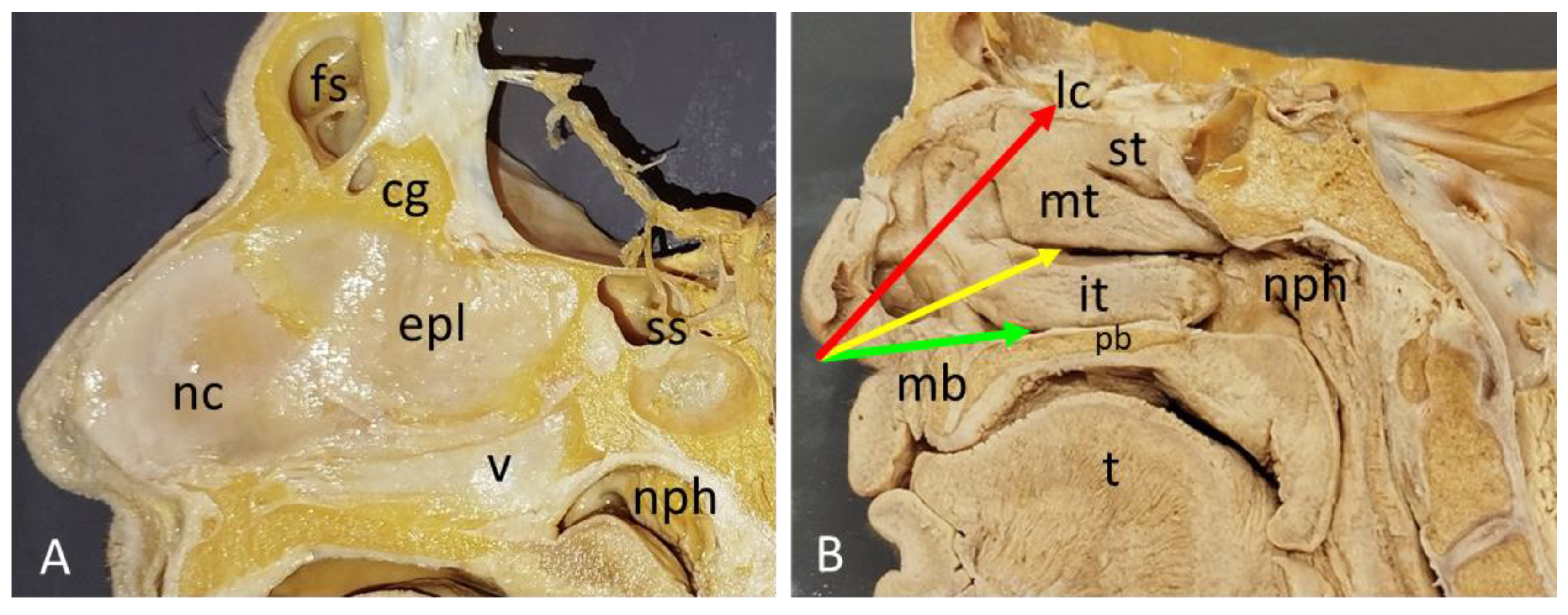
Figure 3.
Coronal view of the nasal cavity. Key anatomical structures are labeled from superior to inferior: cg (crista galli); ec (ethmoidal air cells); mt (middle turbinate); it (inferior turbinate); ns (nasal septum); ms (maxillary sinus); lp (lamina papiracea). The floor of the nasal cavity is formed by the palate. There, the hard palate is seen. The tongue (t) is visible in the oral cavity. The target for swab insertion, the inferior meatus (im, highlighted in green), is situated beneath the inferior turbinate. The middle meatus (mm) is also indicated.
Figure 3.
Coronal view of the nasal cavity. Key anatomical structures are labeled from superior to inferior: cg (crista galli); ec (ethmoidal air cells); mt (middle turbinate); it (inferior turbinate); ns (nasal septum); ms (maxillary sinus); lp (lamina papiracea). The floor of the nasal cavity is formed by the palate. There, the hard palate is seen. The tongue (t) is visible in the oral cavity. The target for swab insertion, the inferior meatus (im, highlighted in green), is situated beneath the inferior turbinate. The middle meatus (mm) is also indicated.
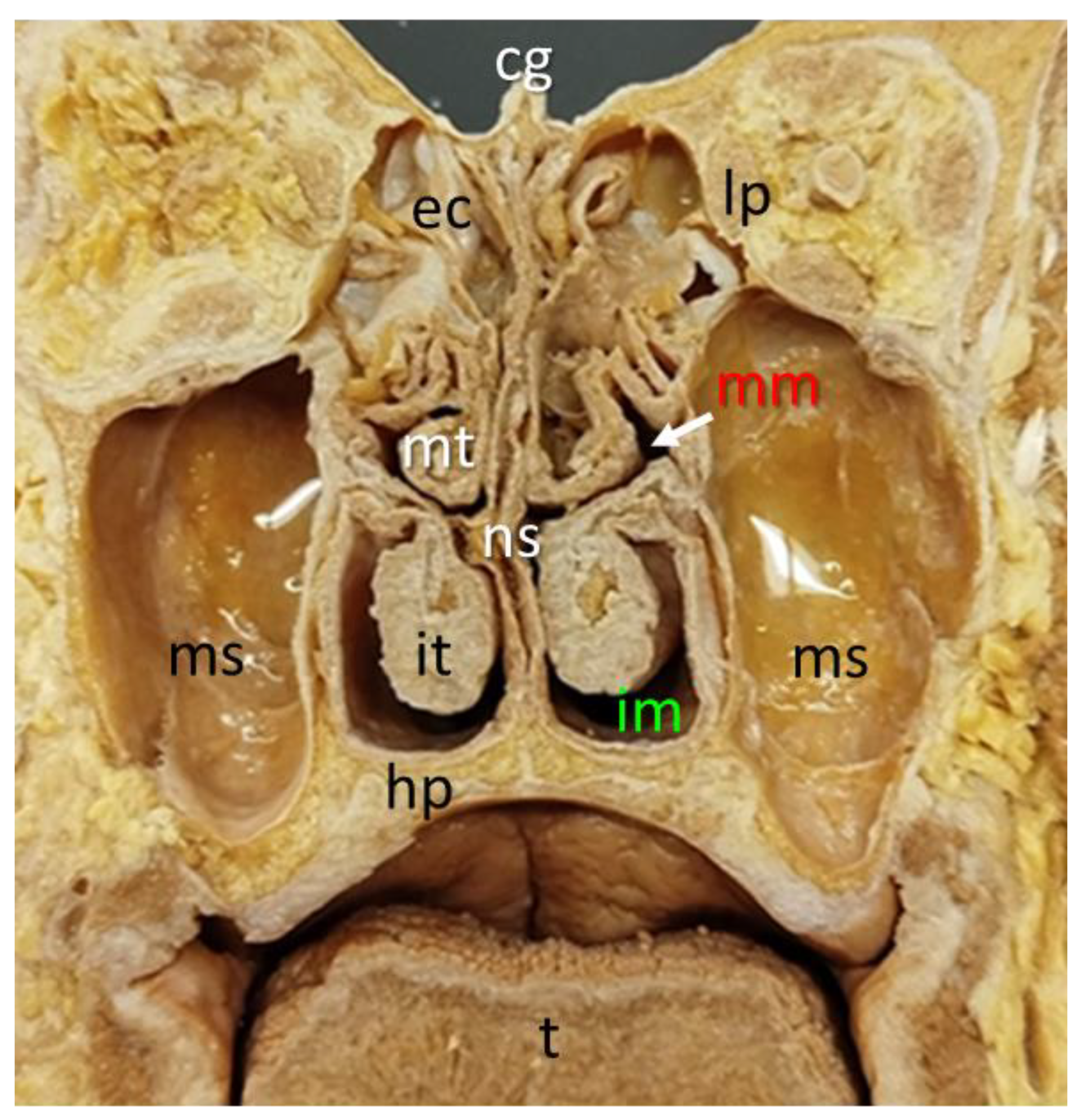
Figure 4.
Schematic illustration of the correct nasal swab insertion angle. This graphic is intended for use in patient instructions for self-administered antigen tests. It is released under a CC-BY 4.0 license, which permits free reuse and adaptation with proper attribution to the source.
Figure 4.
Schematic illustration of the correct nasal swab insertion angle. This graphic is intended for use in patient instructions for self-administered antigen tests. It is released under a CC-BY 4.0 license, which permits free reuse and adaptation with proper attribution to the source.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



