
Submitted:
30 December 2025
Posted:
31 December 2025
You are already at the latest version
Abstract
Congenital erythropoietic porphyria (CEP), also known as Günther disease, is a rare autosomal recessive porphyria caused by deficiency of uroporphyrinogen III synthase, leading to accumulation of phototoxic type I porphyrins. CEP classically presents in infancy with severe photosensitivity, blistering, scarring, and hemolytic anemia; however, significant phenotypic variability has increasingly been recognized. We report 32-year-old women diagnosed with CEP in early infancy who demonstrated persistently and profoundly elevated erythrocyte porphyrin levels over more than a decade yet followed a relatively non-mutilating clinical course. Genetic testing identified a low penetrance intronic UROS variant typically associated with erythropoietic protoporphyria, underscoring diagnostic challenges and genotype-phenotype discordance. The patient experienced marked improvement in photosensitivity and burning pain after initiation of afamelanotide, without need for transfusion therapy or stem cell transplantation. This case highlights the heterogeneity of CEP, the importance of long-term biochemical follow up, and the potential role of afamelanotide in improving quality of life for selected patients with CEP.
Keywords:
congenital erythropoietic porphyria
; Günther disease
; erythrocyte porphyrins
; photosensitivity
; afamelanotide
; UROS mutations
1. Introduction and Clinical Significance
Congenital erythropoietic porphyria (CEP), also known as Günther disease, is a rare autosomal recessive disease of heme biosynthesis caused by deficient activity of uroporphyrinogen III synthase (UROS) [1]. CEP belongs to the group of erythropoietic porphyrias and is characterized by the accumulation of non-physiologic type I porphyrins, predominantly uroporphyrin I and coproporphyrin I, within erythroid cells, plasma, skin, and other tissues [1,2,3]. These phototoxic porphyrins lead to severe cutaneous photosensitivity and variable hematologic manifestations, making CEP one of the most clinically debilitating porphyrias.
CEP most commonly presents in early infancy with dark or reddish urine, blistering and erosions of sun exposed skin, hypertrichosis, erythrodontia, and chronic hemolytic anemia [12]. The cutaneous manifestations are driven by porphyrin activation by visible light, particularly wavelengths in the Soret band (400-410 nm), resulting in oxidative tissue injury [7,13]. Repeated phototoxic damage often leads to scarring, deformity, and mutilation of exposed areas such as the hands, face, and ears [1,2,3]. Historically, CEP has been regarded as a severe and relentlessly progressive disease with significant morbidity and reduced quality of life.
Despite this classic description, increasing evidence suggests that CEP exhibits substantial phenotypic heterogeneity. Reports of milder disease, delayed presentation, and even adult-onset CEP challenge the traditional view of CEP as universally devastating [4,5,6]. Adult-onset CEP cases have been described with attenuated cutaneous findings, hematologic abnormalities, or atypical presentations, highlighting the importance of maintaining diagnostic suspicion even outside infancy [5,6]. This variability is attributed to differences in residual UROS activity, genetic modifiers, iron metabolism, and environmental exposures [6,7,8,9].
Diagnosis of CEP relies on a combination of clinical features, markedly elevated erythrocyte and urinary porphyrins with a predominance of type I isomers, and molecular confirmation of pathogenic UROS variants [1,3,8]. However, genotype-phenotype correlations are imperfect, and low penetrance or intronic variants may complicate interpretation, particularly in patients with atypical presentations [6,8]. As a result, biochemical evaluation remains central to diagnosis and disease classification.
Management of CEP is challenging due to its rarity and the absence of standardized treatment guidelines. Traditional management strategies include lifelong photoprotection, wound care, treatment of hemolytic anemia, and supportive management of complications [2,7,11]. In severe cases, transfusion therapy, splenectomy, or hematopoietic stem cell transplantation (HSCT) have been employed, with HSCT representing the only curative option to date [15,16]. However, these interventions carry significant risk and are typically reserved for patients with severe or progressive disease.
Advances in the understanding of erythropoietic porphyrias have led to the exploration of therapies initially developed for erythropoietic protoporphyria (EPP), including afamelanotide, a melanocortin analogue that increases eumelanin production and improves tolerance to visible light exposure [12,14]. While approved for EPP, its role in CEP remains limited to anecdotal and emerging evidence, warranting further investigation.
Here, we present the case of a women with CEP diagnosed in early infancy who demonstrated persistently severe biochemical abnormalities over more than a decade yet followed a relatively non-mutilating clinical course and experienced symptomatic improvement with afamelanotide. This case highlights the phenotypic variability of CEP, the importance of long term biochemical monitoring, and the potential applicability of newer therapeutic approaches in selected patients.
2. Case Presentation
The patient is a 32-year-old female with a past medical history significant for congenital erythropoietic porphyria, psoriasis, anxiety/depression, and severe intolerance to intravenous iron, who presented to the Hematology-Oncology clinic for routine follow up. She was diagnosed with CEP at 2 weeks of age following extensive evaluation, including bone marrow testing. During infancy and childhood, she experienced severe photosensitivity with recurrent second- and third-degree burn injuries following sun exposure, resulting in residual scarring of the dorsal hands and forearms. Early management included beta-carotene supplementation, topical burn therapy, antihistamines, and strict photoprotection.
Approximately five years prior to presentation, she was referred to a porphyria specialist for further evaluation after markedly elevated erythrocyte porphyrin levels were identified (2048 µg/dL; Figure 1). Genetic testing showed a pathogenic low penetrance intronic UROS variant (c.315-48T>C), which is the most prevalent variant associated with autosomal recessive erythropoietic protoporphyria (EPP). Bone marrow testing was deferred in light of confirmatory genetic and biochemical findings. She was subsequently initiated on afamelanotide therapy four years prior to the current visit, with reported improvement in photosensitivity despite persistently elevated erythrocyte porphyrin levels (Table 1).
On examination, the patient demonstrated cutaneous changes consistent with chronic photosensitivity involving multiple sun-exposed areas. Clinical photographs illustrate sharply demarcated phototoxic injury of the forefoot, scarring of the dorsal hand, patterned sunborn of the upper back corresponding to clothing exposure, and residual facial scarring involving the nose and chin, without evidence of mutilation or tissue loss (Figure 2). The patient remains stable on afamelanotide therapy and continues to practice strict photoprotection, reporting decreased frequency and severity of burn injuries since treatment initiation.
- (A)
- The forefoot showing a sharply demarcated band of sunburn measuring approximately 6-8 cm in width across the dorsal aspect, consistent with phototoxic injury.
- (B)
- The dorsal hand demonstrating residual scarring, most prominent along the thumb, from prior photosensitivity-related injury.
- (C)
- The upper back showing a geometric area of sunburn corresponding to the lower border of clothing, with greater exposure and erythema of the uncovered upper back.
- (D)
- The face demonstrating residual scarring involving the nose and chin with associated cheilitis. No evidence of mutilation, tissue loss, or auto-amputation is observed.
3. Discussion
Congenital erythropoietic porphyria (CEP) is an exceptionally rare autosomal recessive porphyria caused by deficiency of uroporphyrinogen III synthase (UROS), resulting in accumulation of type I porphyrins and severe photosensitivity. Although classically described as a devastating, mutilating disorder of infancy, CEP is now recognized as a disease with broad phenotypic variability [1]. The present case exemplifies this spectrum: despite a biochemical profile showing persistently extreme erythrocyte porphyrin elevations for more than a decade, the patient’s clinical course has remained non-mutilating, relatively stable, and significantly improved with afamelanotide therapy.
3.1. Phenotypic Spectrum of CEP
Classic CEP typically presents during infancy with severe photosensitivity, vesicles, bullae, erosions, and mutilating scarring of sun-exposed areas, including hands, ears, and face [2,3]. Patients often develop erythrodontia, hypertrichosis, splenomegaly, and hemolytic anemia [1]. However, more recent reports describe mild, attenuated, or non-mutilating variants in which patients exhibit lifelong photosensitivity but do not develop progressive disfigurement [4,5,6].
The current patient represents this non-mutilating phenotype, despite decades of markedly elevated erythrocyte porphyrins (>1,500-2500 µg/dL). Her early childhood blistering decreased over time, and she did not develop the severe scarring or deformity characteristics of classic CEP. This is consistent with published cases documenting milder disease presentations, sometimes without scarring or hemolysis, and occasionally with later onset [4,5,7]. Such cases underscore that porphyrin levels alone do not predict severity, and that genotype, residual enzyme activity, iron metabolism, and other modifying influences significantly shape disease expression [6,7,8,9,10].
This case is particularly valuable because longitudinal biochemical data extending over a decade are rarely reported. The persistently extreme porphyrin elevation, despite relatively stable clinical manifestations, provides insight into the natural history of non-mutilating CEP.
3.2. Molecular and Pathophysiologic Considerations
CEP results from biallelic pathogenic variations in UROS leading to impaired conversion of hydroxymethylbilane into uroporphyrinogen III. The deficiency causes spontaneous formation of type I porphyrin isomers, which cannot enter downstream heme synthesis and instead accumulate in tissues where they generate phototoxic injury [1].
Genotype-phenotype correlation in CEP is complex. Some variants such as well-studied C73R allele, produce nearly absent UROS activity and aggressive disease [8]. Other mutations allow partial activity, explaining milder phenotypes. Furthermore, modifying factors such as iron status, erythropoietic rate, and additional genetic modifiers influence the severity of cutaneous and hematologic manifestations [6,9,10].
The identification of the c.315-48T>C intronic variant, a low-penetrance allele more commonly associated with erythropoietic protoporphyria (EPP), adds complexity to this case. Although the biochemical pattern clearly indicates CEP rather than EPP, this finding highlights the overlap between erythropoietic porphyrias, the imperfect nature of genotype-only diagnosis, and the importance of integrating biochemical, clinical, and molecular findings [6,11]. Such overlap has been observed in other reports demonstrating unexpected genotype-phenotype mismatches, supporting the concept of a continuum of erythropoietic porphyrias.
3.3. Diagnostic Considerations
Diagnosis of CEP typically relies on:
This patient’s biochemical profile, with persistently extreme erythrocyte porphyrin levels, strongly supports CEP. Erythrocyte porphyrins remain chronically elevated because porphyrins are tightly bound within circulating red cells [13]. This contrasts with EPP, where protoporphyrin levels may fluctuates alongside environmental triggers and erythropoietic activity [11].
One diagnostic challenge illustrated by this case is the potential for misclassification when genetic variants associated with EPP or low-penetrance alleles are detected. The biochemical profile remains the most reliable discriminator in such scenarios [11].
3.4. Management Strategies and Therapeutic Lessons
3.1. Photoprotection
Photoprotection remains the cornerstone of management for all photosensitive porphyrias. Avoidance of visible-light wavelengths around the Soret band (400-410 nm) is essential. Patients often require lifelong environmental modification and protective clothing [7].
3.2. Afamelanotide
A significant finding in this case is the patient’s meaningful symptom improvement after initiation of afamelanotide, a melanocortin analogue FDA-approved for EPP. Leaf et al. describes how afamelanotide increases eumelanin density, thereby extending pain-free light exposure time in erythropoietic porphyrias [11]. Although off label for CEP, the biologic rationale is applicable because both CEP and EPP involve phototoxic activation of porphyrins by visible light. The positive outcome observed reinforces the potential benefit of afamelanotide as an adjunctive therapy in selected CEP patients, particularly those seeking improved quality of life.
3.3. Iron Modulation
Iron influences heme biosynthesis and may modify porphyrin production. Studies suggest that inducing mild iron deficiency can reduce erythropoietic drive and porphyrin accumulation, while excess iron may worsen photosensitivity [6,11]. The patient’s intolerance to IV iron and chronic nausea highlights the importance of individualized iron management.
3.4. Transfusion Support and Splenectomy
3.5. Hematopoietic Stem Cell Transplantation (HSCT)
HSCT remains the only curative therapy for CEP. Successful transplants show complete normalization of UROS activity, resolution of hemolytic anemia, and dramatic improvement in skin disease [16]. However, due to significant risks, HSCT is reserved for severe, progressive, or mutilating cases, criteria that this patient does not meet.
3.6. Emerging Therapies
3.5. Systemic Symptoms and Quality of Life Considerations
Patients with erythropoietic porphyrias frequently report systemic manifestations during phototoxic episodes, including fatigue, malaise, dehydration, and gastrointestinal distress [14]. These symptoms are believed to result from cytokine release triggered by porphyrin activation. This patient’s chronic nausea, abdominal pain, and fatigue may reflect these mechanisms, compounded by the psychosocial burden of lifelong photoprotection.
4. Conclusions
This patient exemplifies the expanding phenotypic spectrum of CEP, demonstrating that extremely elevated porphyrin levels do not necessarily predict mutilating disease. Her positive therapeutic response to afamelanotide provides valuable evidence supporting broader consideration of melanocortin analogues in CEP management. By combining decades-long biochemical data, atypical genotyping, and detailed clinical evolution, this case strengthens understanding of CEP heterogeneity and highlights opportunities for improved personalized care and future therapuetic innovation.
Author Contributions
Conceptualization, S.P. and K.S.K.; methodology, S.P., K.S.K., E.T..; validation, S.P., B.R., S.K.U. and K.S.K.; formal analysis, S.P., K.S.K., and E.T.; investigation, S.P., K.S.K, E.T., B.R., S.K.U., P.K.G.; resources, S.P., K.S.K., E.T., B.R., S.K.U., and P.K.G.; data curation, S.P., K.S.K, E.T., B.R., S.K.U., and P.K.G.; writing—original draft preparation, S.P., K.S.K, E.T., B.R., S.K.U., and P.K.G.; writing—review and editing, S.P., K.S.K, E.T., B.R., S.K.U., and P.K.G.; visualization, S.P., K.S.K., E.T., and S.S.; supervision, S.P. and S.S.; project administration, S.P. and S.S.; funding acquisition, S.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Sakshi Singal.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Erwin A, Balwani M, Desnick RJ; Porphyrias Consortium of the NIH-Sponsored Rare Diseases Clinical Research Network. Congenital Erythropoietic Porphyria. 2013 Sep 12 [Updated 2021 Apr 15]. In: Adam MP, Bick S, Mirzaa GM, et al., editors. GeneReviews®® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2025.
- Fritsch, C.; Bolsen, K.; Ruzicka, T.; Goerz, G. Congenital erythropoietic porphyria. J. Am. Acad. Dermatol. 1997, 36, 594–610. [Google Scholar] [CrossRef] [PubMed]
- Puy, H.; Gouya, L.; Deybach, J.-C. Porphyrias. Lancet 2010, 375, 924–937. [Google Scholar] [CrossRef] [PubMed]
- Saikrishna, P.; Palaniswamy, G.; Doddareddy, N.P.; Ishfaq, L.; Zargar, M.N.; Eranhikkal, F.W.; Sahu, S. Congenital Erythropoietic Porphyria: A Rare Inherited Disorder. Cureus 2024, 16, e55558. [Google Scholar] [CrossRef] [PubMed]
- Murphy, A; Gibson, G; Elder, GH; Otridge, BA; Murphy, GM. Adult-onset congenital erythropoietic porphyria (Günther’s disease) presenting with thrombocytopenia. J R Soc Med 1995, 88(6), 357P–358P. [Google Scholar] [PubMed] [PubMed Central]
- To-Figueras, J; Erwin, AL; Aguilera, P; Millet, O; Desnick, RJ. Congenital erythropoietic porphyria. Liver Int. 2024, 44, 1842–1855. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, P.; Schwarz, T. Photodermatoses. Dtsch. Aerzteblatt Online 2011, 108, 135–41. [Google Scholar] [CrossRef] [PubMed]
- Desnick, R.J.; Glass, I.A.; Xu, W.; Solis, C.; Astrin, K.H. Molecular Genetics of Congenital Erythropoietic Porphyria. Semin. Liver Dis. 1998, 18, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Balwani, M.; Desnick, R.J. The porphyrias: advances in diagnosis and treatment. Blood 2012, 120, 4496–4504. [Google Scholar] [CrossRef] [PubMed]
- Cappellini, M.D. Coagulation in the Pathophysiology of Hemolytic Anemias. Hematol. 2007, 2007, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Tintle, S.; Alikhan, A.; Horner, M.E.; Hand, J.L.; Davis, D.M.R. Cutaneous porphyrias part II: treatment strategies. Int. J. Dermatol. 2013, 53, 3–24. [Google Scholar] [CrossRef] [PubMed]
- Lecha, M.; Puy, H.; Deybach, J.-C. Erythropoietic protoporphyria. Orphanet J. Rare Dis. 2009, 4, 19–19. [Google Scholar] [CrossRef] [PubMed]
- Poh-Fitzpatrick, M.B. Porphyrin-sensitized cutaneous photosensitivity. Clin. Dermatol. 1985, 3, 41–82. [Google Scholar] [CrossRef] [PubMed]
- Leaf, R.K.; Dickey, A.K. How I treat erythropoietic protoporphyria and X-linked protoporphyria. Blood 2023, 141, 2921–2931. [Google Scholar] [CrossRef] [PubMed]
- Shetty, A. K.; Ode, D.; Galen, W. K.; Warrier, R. P. Successful splenectomy for congenital erythropoietic porphyria (Gunther’s disease). Journal of Investigative Medicine 1999, 47(2), 161A. [Google Scholar]
- Besnard, C.; Schmitt, C.; Galmiche-Rolland, L.; Debray, D.; Fabre, M.; Molina, T.; Gouya, L.; Ged, C.; Castelle, M.; Cavazzana, M.; et al. Bone Marrow Transplantation in Congenital Erythropoietic Porphyria: Sustained Efficacy but Unexpected Liver Dysfunction. Biol. Blood Marrow Transplant. 2020, 26, 704–711. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Serial erythrocyte porphyrin measurements over time in a patient with congenital erythropoietic porphyria. Values remained markedly elevated and consistently exceeded the upper limit of normal over more than four years, despite a relatively non-mutilating clinical course and symptomatic improvement following afamelanotide therapy.
Figure 1.
Serial erythrocyte porphyrin measurements over time in a patient with congenital erythropoietic porphyria. Values remained markedly elevated and consistently exceeded the upper limit of normal over more than four years, despite a relatively non-mutilating clinical course and symptomatic improvement following afamelanotide therapy.
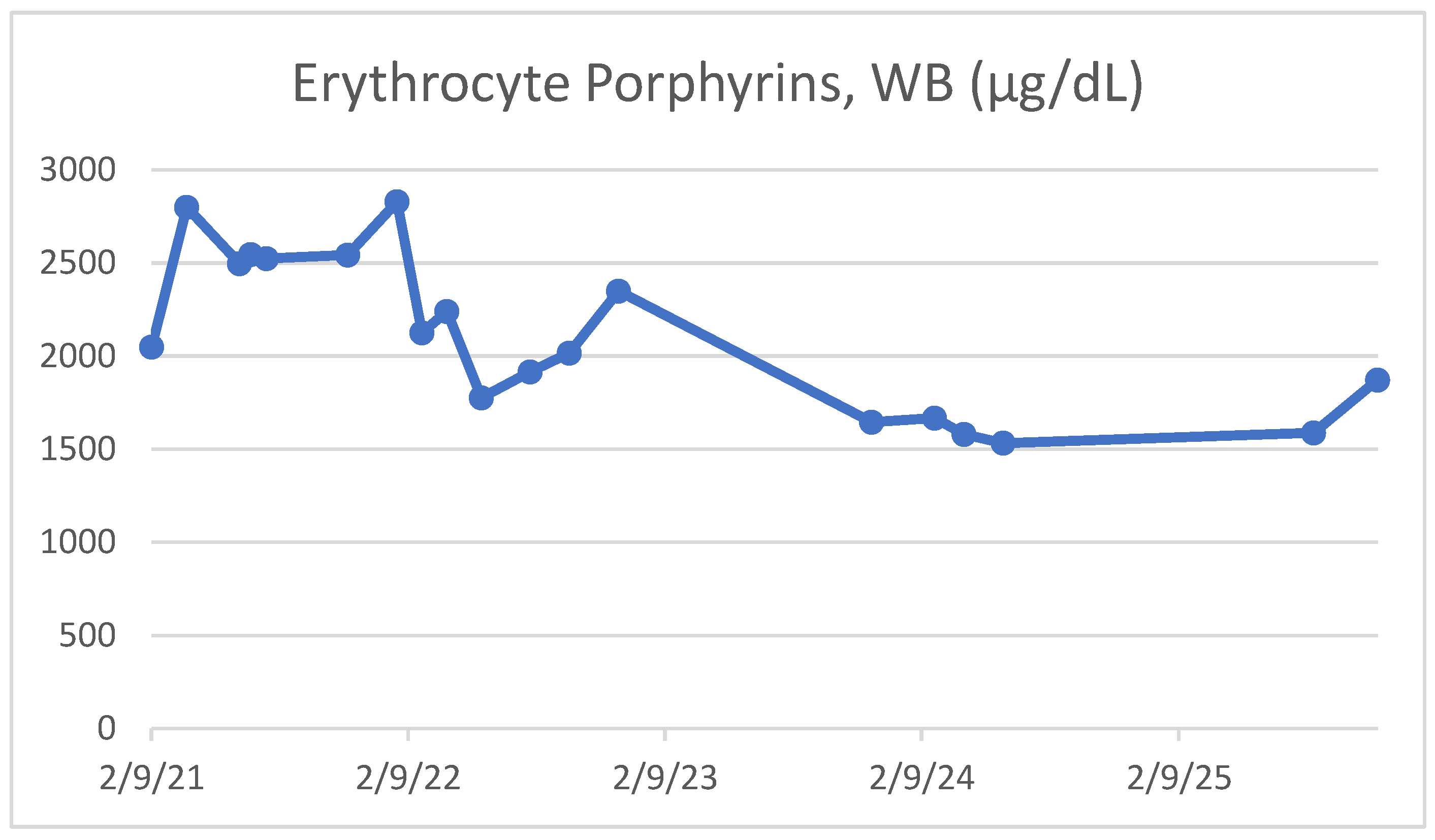
Figure 2.
Clinical photographs demonstrating photosensitivity-related cutaneous findings in a patient with congenital erythropoietic porphyria.
Figure 2.
Clinical photographs demonstrating photosensitivity-related cutaneous findings in a patient with congenital erythropoietic porphyria.


Table 1.
Longitudinal erythrocyte porphyrin measurements in a patient with congenital erythropoietic porphyria demonstrating persistently severe biochemical abnormalities over more than four years. Despite sustained porphyrin levels exceeding 50-fold the upper limit of normal, the patient followed a relatively non-mutilating clinical course with symptomatic improvement following afamelanotide therapy.
Table 1.
Longitudinal erythrocyte porphyrin measurements in a patient with congenital erythropoietic porphyria demonstrating persistently severe biochemical abnormalities over more than four years. Despite sustained porphyrin levels exceeding 50-fold the upper limit of normal, the patient followed a relatively non-mutilating clinical course with symptomatic improvement following afamelanotide therapy.
| Date | Erythrocyte Porphyrins, WB (µg/dL) | Interpretation |
|---|---|---|
| 02/09/2021 | 2048 | Markedly elevated |
| 03/31/2021 | 2800 | Markedly elevated |
| 06/14/2021 | 2495 | Markedly elevated |
| 06/30/2021 | 2545 | Markedly elevated |
| 07/22/2021 | 2524 | Markedly elevated |
| 11/15/2021 | 2544 | Markedly elevated |
| 01/24/2022 | 2828 | Markedly elevated |
| 02/28/2022 | 2124 | Markedly elevated |
| 04/05/2022 | 2240 | Markedly elevated |
| 05/24/2022 | 1776 | Markedly elevated |
| 08/01/2022 | 1915 | Markedly elevated |
| 09/26/2022 | 2016 | Markedly elevated |
| 12/05/2022 | 2350 | Markedly elevated |
| 11/30/2023 | 1645 | Markedly elevated |
| 02/27/2024 | 1668 | Markedly elevated |
| 04/09/2024 | 1580 | Markedly elevated |
| 06/04/2024 | 1532 | Markedly elevated |
| 08/19/2025 | 1588 | Markedly elevated |
| 11/18/2025 | 1872 | Markedly elevated |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



