
Submitted:
29 December 2025
Posted:
30 December 2025
You are already at the latest version
Abstract
Background: Persistent pain following orthopaedic trauma is common, often disproportionate to structural healing, and increasingly attributed to central sensitisation (CS). However, the mechanisms, clinical features, diagnostic approaches, prognostic indicators, and management strategies relevant to trauma-related CS remain poorly understood. Objective: To map and synthesise existing evidence on CS following orthopaedic trauma, addressing mechanistic pathways, clinical manifestations, epidemiology, assessment methods, management approaches, and health system implications. Methods: A scoping review was conducted in accordance with PRISMA-ScR. Twenty-one studies met the eligibility criteria, comprising nine primary trauma cohorts and 12 contextual mechanistic or review studies relevant to trauma-associated CS. Data were charted across six prespecified domains of mechanistic processes, clinical presentation and diagnostic features, epidemiology and prognosis, assessment tools and outcome measures, interventions, and health system and care delivery considerations. Results: Mechanistic studies demonstrated trauma-induced neuroimmune activation, altered cortical and spinal excitability, and molecular pathways consistent with sensitisation. Clinical studies have identified neuropathic features, widespread pain, and heightened sensory responsiveness following fractures and other injuries. Neurophysiological evidence has indicated early cortical disinhibition following upper limb trauma, whereas epidemiological cohorts have reported persistent pain and disability years after major trauma. Measurement studies have highlighted the limited reliability and specificity of current tools in trauma populations, including quantitative sensory testing and self-report instruments. Early predictors of adverse trajectories include severe acute pain, neuropathic descriptors, psychological distress, and opioid-dominant analgesia. Evidence regarding early intervention, rehabilitation strategies, and system-level screening pathways remains limited. Conclusions: CS after orthopaedic trauma is supported by convergent mechanistic, neurophysiological, and clinical findings. However, trauma-specific diagnostic criteria, prognostic models, and management frameworks remain underdeveloped. High-quality longitudinal research is needed to clarify early trajectories, refine assessment methods, and establish targeted interventions to reduce long-term pain and disability.
Keywords:
central sensitisation
; orthopaedic trauma
; chronic post-traumatic pain
; neuropathic pain
; pain chronification
; psychological distress
; widespread pain
; functional disability
; scoping review
1. Introduction
Orthopaedic trauma remains a leading cause of long-term pain and disability, and a substantial proportion of patients continue to experience symptoms that cannot be explained by ongoing tissue injury or structural pathology [1,2]. Persistent posttraumatic pain often presents with sensory amplification, disproportionate symptom intensity, and diffuse hypersensitivity, which are increasingly attributed to central sensitisation (CS). CS describes a state of heightened central nervous system responsiveness to sensory input, underpinned by an altered inhibitory–excitatory balance, neuroimmune activation, and synaptic plasticity [3,4,5]. Although CS is well characterised in chronic musculoskeletal pain, its development, presentation, measurement, and management in trauma populations remain incompletely understood.
Traumatic musculoskeletal injuries differ fundamentally from controlled surgical trauma. High-energy mechanisms, crush forces, open fractures, and concomitant soft tissue damage generate intense, prolonged nociceptive signalling that differs in magnitude and quality from operative injury [3,6]. Elective surgery involves predictable tissue handling and uniform inflammatory response. In contrast, trauma triggers heterogeneous inflammatory cascades, including chemokine signalling, microglial activation, glial proliferation, and cytokine release, which are implicated in sustained pain hypersensitivity [4,5]. Clinical evidence supports early central involvement after trauma; motor cortex intracortical inhibition is disrupted within 14 days following fracture [7], and severe acute pain is strongly associated with later persistent pain [8].
Despite these biological insights, identifying CS in the trauma population remains challenging. Patients with trauma present with overlapping nociceptive, neuropathic, and nociceptive features. Pain may be influenced by immobilisation, nerve irritation, surgical revision, psychological distress, and social factors, making it difficult to attribute to CS difficult [2,9,10]. Diagnostic tools such as the Central Sensitisation Inventory (CSI), Quantitative Sensory Testing (QST) based measures, PainDETECT, and Douleur Neuropathique (DN4) have been studied for musculoskeletal pain, but their measurement properties have been inconsistent in trauma cohorts [11,12]. The QST demonstrates variable reliability, limited construct validity, and uncertain prognostic value outside chronic pain conditions [11], whereas widespread pain, often used as a surrogate marker of central amplification, may reflect psychological distress as much as biological sensitisation [9,13].
Epidemiological evidence suggests that a substantial subgroup of patients with trauma progress to chronic pain with CS-like features. Neuropathic descriptors are reported in up to one-third of patients following major lower-limb trauma and are associated with greater disability and worse quality of life [2]. Longitudinal studies have shown that trauma exposure increases the risk of new-onset widespread pain [13], and chronic posttraumatic pain is common even when structural healing is satisfactory [10]. Early predictors, such as severe acute pain, high opioid exposure without multimodal strategies, catastrophising, sleep disturbance, and PTSD symptoms, have been associated with poor long-term trajectories [6,8,9]. However, the mechanisms that link these early factors to CS-driven chronic pain remain unclear.
Management strategies targeting central mechanisms have been inconsistently applied to trauma practices. Multimodal analgesia can reduce nociceptive input and attenuate early sensitisation; however, its integration into acute trauma care remains variable [6,14]. Psychological distress and PTSD, which are common in trauma populations, can exacerbate central amplification; however, trauma pathways rarely include structured screening or interventions to address these factors [9]. Rehabilitation strategies intended to promote loading and movement may inadvertently exacerbate sensitisation if not tailored to patients with hyperexcitability or fear-avoidant responses [6]. System-level gaps include a lack of CS recognition in trauma clinics, the absence of consensus outcome measures, and limited integration of CS assessment into fracture pathways.
Collectively, these uncertainties highlight the need for a comprehensive synthesis of mechanistic, clinical, diagnostic, epidemiological, and management-related evidence specific to central sensitisation after orthopaedic trauma.
Accordingly, this scoping review aims to
- Clarify how CS is conceptualised within orthopaedic trauma literature and identify areas of definitional inconsistency.
- Describe how CS-related symptoms, diagnostic tools, and early risk indicators are applied to or interpreted in injured populations.
- We mapped the current evidence on assessment approaches, prognostic patterns, management strategies, and system-level implications relevant to CS after orthopaedic trauma.
- Examining the extent to which existing evidence supports the hypothesis that early identification of central sensitisation after orthopaedic trauma might reduce chronic pain, unnecessary reoperations, and morbidity while explicitly acknowledging where direct data are lacking.
2. Materials and Methods
2.1. Protocol and Registration
This review followed the methodological framework for scoping reviews and was reported in accordance with the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) guidelines. This scoping review protocol was prospectively registered on the Open Science Framework (OSF; Registration DOI: 10.17605/OSF.IO/A4NEP)
2.2. Eligibility Criteria
Eligibility criteria were established to capture evidence of central sensitisation (CS), specifically within the context of orthopaedic trauma, including the mechanistic, neurophysiological, clinical, epidemiological, assessment-related, psychological, and management domains of the disease.
Inclusion Criteria
- Population: Adults or adolescents with orthopaedic trauma, including fractures, dislocations, high-energy limb injuries, crush injuries, soft tissue injuries, or polytrauma.
- Concept: Studies were eligible if they assessed constructs consistent with central sensitisation (e.g., neuropathic pain, widespread pain, pain chronification, cortical disinhibition, or psychological amplification), even if the term ‘central sensitisation’ was not explicitly used after orthopaedic trauma.
- Context: Acute, subacute, or chronic post-traumatic phases; inpatient, outpatient, surgical, or rehabilitation settings.
- Study designs: Mechanistic laboratory studies, neurophysiology studies, observational cohorts, prospective studies, clinical prediction studies, systematic reviews, and thematic or narrative reviews.
- Outcomes: Any outcome related to pain, sensory testing, neurophysiology, functional disability, psychological features, or long-term morbidity.
Exclusion Criteria
- Studies focusing solely on chronic non-traumatic pain
- Elective orthopaedic surgery without a trauma cohort, unless directly comparing traumatic vs. surgical mechanisms
- Animal studies
- Non–peer reviewed literature (conference abstracts, dissertations).
2.3. Information Sources
A comprehensive search was performed in the following electronic databases:
- MEDLINE (via PubMed)
- EMBASE
- CINAHL
- Scopus
- Cochrane Library
2.4. Search Strategy
The search strategy combined controlled vocabulary (e.g., MeSH terms) with free-text keywords related to
- central sensitisation, nociplastic pain, pain modulation, widespread pain, quantitative sensory testing, cortical excitability, temporal summation, conditioned pain modulation, combined with
- trauma, fracture, orthopaedic trauma, musculoskeletal injury, post-traumatic, post-surgical, lower limb fracture, upper limb fracture.
An example MEDLINE search string is as follows: (fracture* OR “musculoskeletal injury” OR “orthopaedic trauma” OR trauma* OR polytrauma) AND (“central sensitization” OR “central sensitisation” OR nociplastic OR hyperalgesia OR allodynia OR “cortical excitability”) AND (pain OR neuropathic OR persistent OR chronic).
2.5. Selection of Sources of Evidence
The search results were imported into a citation management system and duplicates were removed. Screening was performed in two stages: 1. Title and abstract screening was also performed. 2. Full-text eligibility assessment.
Two reviewers independently screened the abstracts and full texts. Disagreements were resolved by discussion. The PRISMA flow diagram illustrates the screening and selection process.
Twenty-one sources of evidence were included, comprising nine primary trauma cohorts and 12 contextual mechanistic or review studies.
2.6. Data Charting Process
A structured data-charting form was developed to extract the following information.
- Study design, sample, population characteristics
- Nature and mechanism of injury
- Mechanistic findings
- Neurophysiological markers
- Clinical features and pain phenotypes
- Psychological correlates
- QST or measurement outcomes
- Treatment or analgesic findings
- Prognostic outcomes and trajectory findings
Data were charted independently by two reviewers and compared for accuracy. Systematic, narrative, and mechanistic reviews were included to provide contextual interpretation of central sensitisation mechanisms, but were not used to estimate prevalence, effect sizes, or prognostic associations.
2.7. Synthesis of Results
Given the heterogeneity of the study designs, populations, and outcome measures, narrative thematic synthesis was performed. A meta-analysis was not performed because of the substantial clinical, methodological, and conceptual heterogeneity across trauma types, CS constructs, outcome measures, and follow-up durations. The findings were organised according to the six domains defined a priori:
- Mechanistic & Pathophysiological Processes
- Clinical Manifestation & Diagnostic Features
- Epidemiology & Prognosis
- Assessment & Measurement
- Intervention & Management
- Health-System and Outcomes
3. Results
3.1. Study Selection
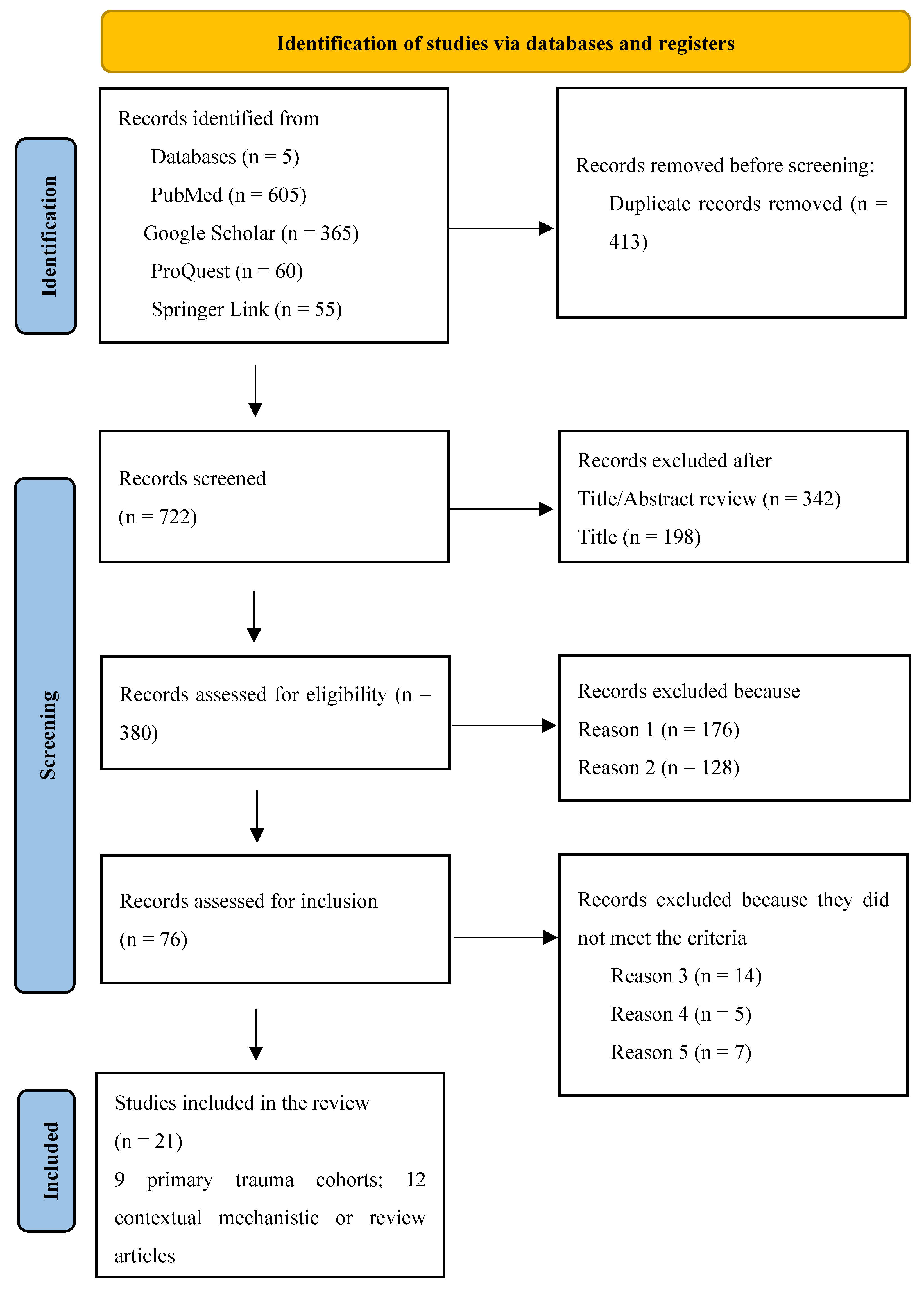
The literature search and screening process identified studies examining pain outcomes, sensory phenotypes, and central pain mechanisms following orthopaedic and musculoskeletal trauma. After removing duplicates and applying predefined inclusion and exclusion criteria, 21 studies were retained for the qualitative synthesis. Of these, nine were primary clinical studies of trauma-exposed populations, while the remaining 12 were systematic reviews, narrative reviews, and methodological or mechanistic papers. The latter provided a contextual interpretation of central sensitisation but was excluded from the PRISMA-ScR evidence map.
The nine primary studies included prospective cohort studies, retrospective follow-up cohorts, neurophysiological experiments, and multicentre trauma trial datasets [1,2,7,8,13,16,17,18,19]. These studies involved patients with fractures of the upper and lower limbs, pelvic injuries, postoperative orthopaedic trauma, major blunt trauma, and motor vehicle collision–related musculoskeletal injuries, with follow-up durations ranging from days to over six years.
The 12 non-primary sources included systematic and narrative reviews, as well as conceptual or methodological papers addressing central sensitisation, quantitative sensory testing, pain modulation, and trauma-related pain mechanisms [3,4,6,9,10,11,12,14,20,21,22,23]. These were retained to provide mechanistic and interpretive contexts but were not used to estimate prevalence or effect sizes, in line with the PRISMA-ScR guidance.
This approach enabled the scoping review to map the extent and nature of empirical evidence on central sensitisation after orthopaedic trauma while integrating high-level mechanistic literature to explain clinical patterns.
Figure 1.
PRISMA-ScR flow diagram of the search and selection process for sources of evidence in this scoping review. Note: Reason 1: Sources not addressing central sensitisation (CS) mechanisms, prevalence, or impacts post-orthopaedic trauma (e.g., general chronic pain without trauma focus); Reason 2: Non-adult populations (< 18 years) or non-orthopaedic contexts (e.g., neuropathic pain only); Reason 3: Articles with full-text not retrievable (e.g., paywalled/no open access); Reason 4: Publication date before 2000 or non-English language; Reason 5: Duplicate or non-peer-reviewed sources (e.g., conference abstracts without full data).
Figure 1.
PRISMA-ScR flow diagram of the search and selection process for sources of evidence in this scoping review. Note: Reason 1: Sources not addressing central sensitisation (CS) mechanisms, prevalence, or impacts post-orthopaedic trauma (e.g., general chronic pain without trauma focus); Reason 2: Non-adult populations (< 18 years) or non-orthopaedic contexts (e.g., neuropathic pain only); Reason 3: Articles with full-text not retrievable (e.g., paywalled/no open access); Reason 4: Publication date before 2000 or non-English language; Reason 5: Duplicate or non-peer-reviewed sources (e.g., conference abstracts without full data).
3.2. Characteristics of Included Trauma Cohorts
Large multicenter datasets included the UK WHiST trial cohort of surgically treated lower limb fractures [2] and a US multicenter extremity fracture randomised controlled trial [19]. Single-centre or regional cohorts, including fracture osteosynthesis [16], pelvic trauma [17], unstable ankle fractures [18], major blunt trauma [1], and acute isolated fractures studied neurophysiologically [7]. A national UK insurance cohort captured post-collision (MVC) musculoskeletal pain trajectories [13].
None of the included trauma cohorts applied a formal diagnosis of central sensitisation; CS-consistent constructs were inferred from neuropathic pain, neurophysiological changes, pain persistence, and psychological amplification [2,7,8,16,17]. Detailed study-level data extraction is provided in Supplementary Table S1, and a concise summary of the nine primary trauma cohorts is presented in Table 1.
3.3. Epidemiology and Prognostic Patterns
3.3.1. Prevalence of CS-Related Symptoms After Trauma
Persistent pain and neuropathic pain features were common across all included trauma cohorts, with prevalence varying by injury type, severity, and duration of follow-up.
In the UK WHiST multicenter cohort of surgically treated lower-limb fractures, approximately one-third of the patients reported neuropathic pain characteristics at both three and six months post-injury, measured using validated descriptors of neuropathic pain [2]. Importantly, some patients develop neuropathic features over time, indicating that neuropathic and centrally mediated pain phenotypes may emerge during recovery rather than being present only in the immediate post-injury phase [2].
Similar findings were observed in a German fracture osteosynthesis cohort, in which chronic post-traumatic or postsurgical pain was prevalent at both three and 12 months. Among those with chronic pain, a substantial subset met the criteria for neuropathic pain using the DN4 interview and painDETECT screening tools, confirming that neuropathic symptomatology is a frequent component of persistent fracture pain [16].
Long-term follow-up studies have demonstrated that pain frequently persists beyond the tissue healing period. In pelvic fracture survivors, 64% reported ongoing pelvic pain at a median of 52 months after injury, with many meeting higher grades of chronicity on the Mainz Pain Staging System, indicating clinically significant and persistent pain syndromes [17]. In a cohort of unstable ankle fractures treated operatively, persistent pain was reported at a mean of 5.8 years, with 23% of patients fulfilling the criteria for neuropathic pain, demonstrating that neuropathic features remain detectable for many years after injury [18].
Similarly, in a multicenter major blunt trauma cohort followed for six years, nearly half of the patients reported chronic pain, with severity ranging from intermittent moderate pain to persistent severe pain interfering with daily activities. Injury severity was the strongest predictor of long-term pain in this cohort [1].
Motor-vehicle collision–related musculoskeletal injuries also show persistent long-term pain. In a national UK insurance cohort, a substantial proportion of patients continued to report pain and functional limitations months to years after collision, confirming that even non-fracture musculoskeletal trauma can result in prolonged pain trajectories [13].
Neuropathic pain features, pain persistence, and functional interference were consistently observed across these diverse trauma populations, indicating that a large proportion of patients develop pain phenotypes that extend beyond the expected peripheral tissue recovery following orthopaedic trauma.
3.3.2. Objective Evidence of Central Nervous System Change After Orthopaedic Trauma
Only one of the included trauma studies directly measured the central nervous system function using neurophysiological methods.
Jodoin et al. [7] examined motor cortex excitability using transcranial magnetic stimulation (TMS) in patients with acute upper limb fractures within the first two weeks following injury. Patients reporting moderate to severe pain (numerical rating scale ≥4) demonstrated significant reductions in short interval intracortical inhibition (SICI) and intracortical facilitation (ICF) compared to healthy controls and trauma patients reporting lower pain intensity. These findings indicate an early disruption of the normal inhibitory–excitatory balance within the primary motor cortex, which is consistent with cortical disinhibition and central hyperexcitability.
Importantly, these neurophysiological abnormalities were observed during the acute post-injury period, prior to chronic pain development. The magnitude of cortical disinhibition was proportional to the reported pain intensity, supporting a dose–response relationship between nociceptive load and central nervous system adaptation.
This study provides only direct objective evidence in the trauma literature that orthopaedic injury is associated with early central nervous system dysregulation, linking acute pain exposure to altered cortical processing. Although derived from a single cohort, these findings provide a mechanistic link between acute traumatic nociception and the later emergence of persistent neuropathic pain phenotypes observed in long-term trauma studies.
3.3.3. Psychological and Behavioural Modifiers of Pain Persistence After Orthopaedic Trauma
Psychological distress and maladaptive cognitive-affective responses are consistently associated with more severe acute pain and poorer short- to medium-term outcomes after orthopaedic trauma.
In an orthopaedic trauma surgery cohort, Edgley et al. [8] reported that higher perioperative pain catastrophising and psychological distress were associated with greater acute pain severity and increased risk of persistent postsurgical pain with pain-related disability at follow-up. These associations remained evident even after accounting for clinical and surgical factors, indicating that cognitive and affective vulnerability meaningfully contribute to pain persistence and functional interference following trauma surgery.
In a fracture osteosynthesis cohort, Aulenkamp et al. [16] found that patients who developed chronic post-traumatic or post-surgical pain, particularly those with neuropathic pain features, demonstrated higher levels of anxiety and depressive symptoms at follow-up. The clustering of persistent pain with affective distress supports an interaction between psychological vulnerability and pain chronification trajectory after fracture management.
Evidence from motor–vehicle collision-related musculoskeletal injuries similarly indicates that recovery trajectories are heterogeneous and influenced by non-structural factors. In the national UK insurance cohort, persistent pain and functional limitations following collision were not solely explained by the apparent extent of musculoskeletal injury, supporting the relevance of behavioural and psychosocial modifiers in post-traumatic pain outcomes [13].
Collectively, these findings indicate that psychological and behavioural factors are closely linked to pain persistence and disability following orthopaedic trauma and that affective distress and catastrophising identify subgroups at a higher risk of developing ongoing, disruptive pain states after injury.
3.4. Prognostic Factors Associated with Persistent and Neuropathic Pain After Orthopaedic Trauma
Across the included trauma cohorts, the prognostic patterns were broadly consistent; greater injury severity, neural involvement, higher early pain burden, and psychological vulnerability were associated with worse long-term pain and functional outcomes. Although none of the primary studies applied a formal diagnosis of central sensitisation, these predictors repeatedly characterised patients who developed persistent pain with neuropathic features and disability.
3.4.1. Injury Severity and Trauma Burden
In a major blunt trauma cohort with a six-year follow-up, the injury severity score (ISS) was the strongest predictor of chronic pain, independent of demographic factors. This indicates that a higher trauma burden is associated with a greater risk of long-term pain persistence [1]. In multicenter extremity fracture trial datasets, a substantial persistent pain burden was also observed across patients with severe limb injuries, supporting the relevance of injury magnitude and complexity as determinants of longer-term outcomes [19].
3.4.2. Neural Involvement and Nerve Injury
Clinically documented nerve injury in pelvic fracture survivors is associated with more advanced pain chronicity stages and more severe persistent pain syndromes, suggesting that neural insults contribute to pain persistence and symptom severity beyond skeletal healing [17]. In unstable ankle fracture survivors, neuropathic pain at long-term follow-up occurs in a defined subset of patients, supporting the notion that peripheral neural disruption, late complications, and adverse recovery trajectories may contribute to neuropathic and persistent pain [18].
3.4.3. Early Pain Intensity and Early Sensory Disturbance
Markers of early pain burden are repeatedly associated with persistent pain. In the WHiST lower-limb fracture cohort, higher early pain was associated with neuropathic pain characteristics and worse disability at three and six months [2]. Among patients with fracture osteosynthesis, those who later met the criteria for chronic post-traumatic or post-surgical pain, particularly neuropathic pain, demonstrated higher early pain intensity and evidence of early neuropathic symptomatology, indicating that sensory disturbance may precede pain chronification [16].
3.4.4. Psychological Vulnerability
Psychological factors modify risk across cohorts. In patients undergoing orthopaedic trauma surgery, higher pain catastrophising and psychological distress are associated with more severe acute pain and an increased likelihood of persistent pain with disability at follow-up [8]. In fracture osteosynthesis cohorts, anxiety and depressive symptoms were more prominent in patients with chronic and neuropathic pain phenotypes, reinforcing the consistent association between affective distress and adverse pain outcomes [16].
Overall, prognostic evidence indicates a multifactorial model of post-traumatic pain persistence, in which trauma severity, neural involvement, early pain burden, and psychological vulnerability jointly identify patients at a higher risk of developing persistent pain with neuropathic features and clinically meaningful disability.
3.5. Long-Term Outcome Burden and Functional Impact After Orthopaedic Trauma
Across primary trauma cohorts, persistent pain was consistently associated with clinically meaningful disability and reduced health-related quality of life, often extending several years beyond index injuries. In a major blunt trauma cohort followed up for six years, chronic pain was common and frequently disruptive, ranging from intermittent moderate pain to persistent severe pain that interfered with daily activities. Notably, long-term pain is not confined to patients with an obvious ongoing structural pathology, indicating that persistent pain and functional limitations can remain prominent even after the completion of standard trauma care [1].
In pelvic fracture survivors assessed at a median of 52 months post-injury, 64% of the patients reported ongoing pelvic pain, which was accompanied by substantial disability. Higher pain chronicity stages were correlated with worse functional outcomes, including poorer disability and reduced physical quality of life, indicating that persistent pelvic pain translates into sustained impairment of mobility and activities of daily living. [17].
Long-term disability was also evident after the less severe injuries. In unstable ankle fracture survivors assessed at a mean of 5.8 years, a substantial proportion reported persistent pain, and those with neuropathic pain features experienced greater interference with daily activities and worse quality of life, demonstrating that enduring pain-related disability can follow apparently localised orthopaedic injuries [18].
At the intermediate follow-up, similar patterns were observed in the large fracture cohorts. In the WHiST lower-limb fracture cohort, patients with neuropathic pain characteristics at three and six months reported significantly worse disability and lower health-related quality of life than those without neuropathic features, indicating that early neuropathic phenotypes are associated with delayed functional recovery [2]. In patients who underwent fracture osteosynthesis, chronic post-traumatic or post-surgical pain at 12 months was associated with higher pain interference and poorer quality-of-life scores, confirming that pain persistence is closely coupled with impaired rehabilitation and reduced patient-reported health status [16].
Collectively, these cohorts demonstrate that persistent and neuropathic pain phenotypes after orthopaedic trauma are associated with sustained disability and reduced health-related quality of life, with meaningful impacts measurable from early recovery through a multi-year follow-up.
3.6. Health-System and Outcome Implications
Although none of the included trauma studies directly measured healthcare utilisation or costs, persistent pain and neuropathic phenotypes were consistently associated with prolonged functional impairment and reduced quality of life across all cohorts. In major blunt trauma, pelvic fracture, ankle fracture, and lower limb fracture populations, patients with chronic or neuropathic pain demonstrated greater disability, poorer physical function, and ongoing interference with daily activities at intermediate and long-term follow-ups [1,2,16,17,18]. These findings imply that a substantial subgroup of trauma patients follows a prolonged and clinically burdensome recovery trajectory, with likely increased rehabilitation needs and ongoing healthcare engagement after the completion of standard orthopaedic treatment.
4. Discussion
4.1. Principal Findings
This scoping review demonstrates that persistent pain after orthopaedic trauma is common and frequently exhibits features consistent with central sensitisation (CS). Across diverse trauma populations—including fracture surgery, pelvic injury, ankle fractures, and major blunt trauma—a substantial proportion of patients develop neuropathic pain features, psychological amplification, and long-term disability, often persisting well beyond the expected biological recovery [1,2,3,16,17,18]. Although direct experimental measurement of CS is uncommon in orthopaedic trauma cohorts, the convergence of sensory, neurophysiological, psychological, and functional findings supports the presence of centrally mediated pain mechanisms in a clinically important subset of patients.
Importantly, this evidence does not support a model in which persistent post-traumatic pain is solely driven by residual tissue damage. Instead, pain trajectories appear heterogeneous and dynamic, with some patients developing neuropathic and centrally mediated phenotypes over time, even as fractures unite and rehabilitation is completed, highlighting a transition from peripherally dominated pain to more complex pain states in vulnerable individuals [2,16].
4.2. Burden and Trajectories of Sensitisation-Consistent Pain After Orthopaedic Trauma
Epidemiological evidence demonstrates that long-term pain following orthopaedic trauma is common and frequently persists. In a large cohort of major trauma survivors, nearly half of the patients reported chronic pain at six years, with a substantial proportion experiencing moderate to severe symptoms that interfered with daily activities [1]. Similarly, in postoperative lower-limb fracture cohorts, approximately one-third of patients reported neuropathic pain characteristics at three and six months after injury, indicating that pain with central features frequently emerges during the recovery period [2].
The long-term pain burden is not confined to high-energy trauma. In patients with pelvic fractures, more than half reported ongoing pelvic pain several years after the injury, with higher pain chronicity associated with worse physical function and a reduced quality of life [17]. Persistent pain is also common after unstable ankle fractures, with a clinically important subset developing neuropathic pain during long-term follow-up [18]. At the population level, exposure to physical trauma is associated with an increased risk of new-onset widespread pain, suggesting that traumatic injury can alter long-term pain vulnerability beyond the site of local tissue damage [13].
Together, these data indicate that sensitisation-consistent pain phenotypes are prevalent and sustained after orthopaedic trauma, frequently persisting well beyond fracture union and standard rehabilitation pathways.
4.3. Mechanistic and Pathophysiological Interpretation
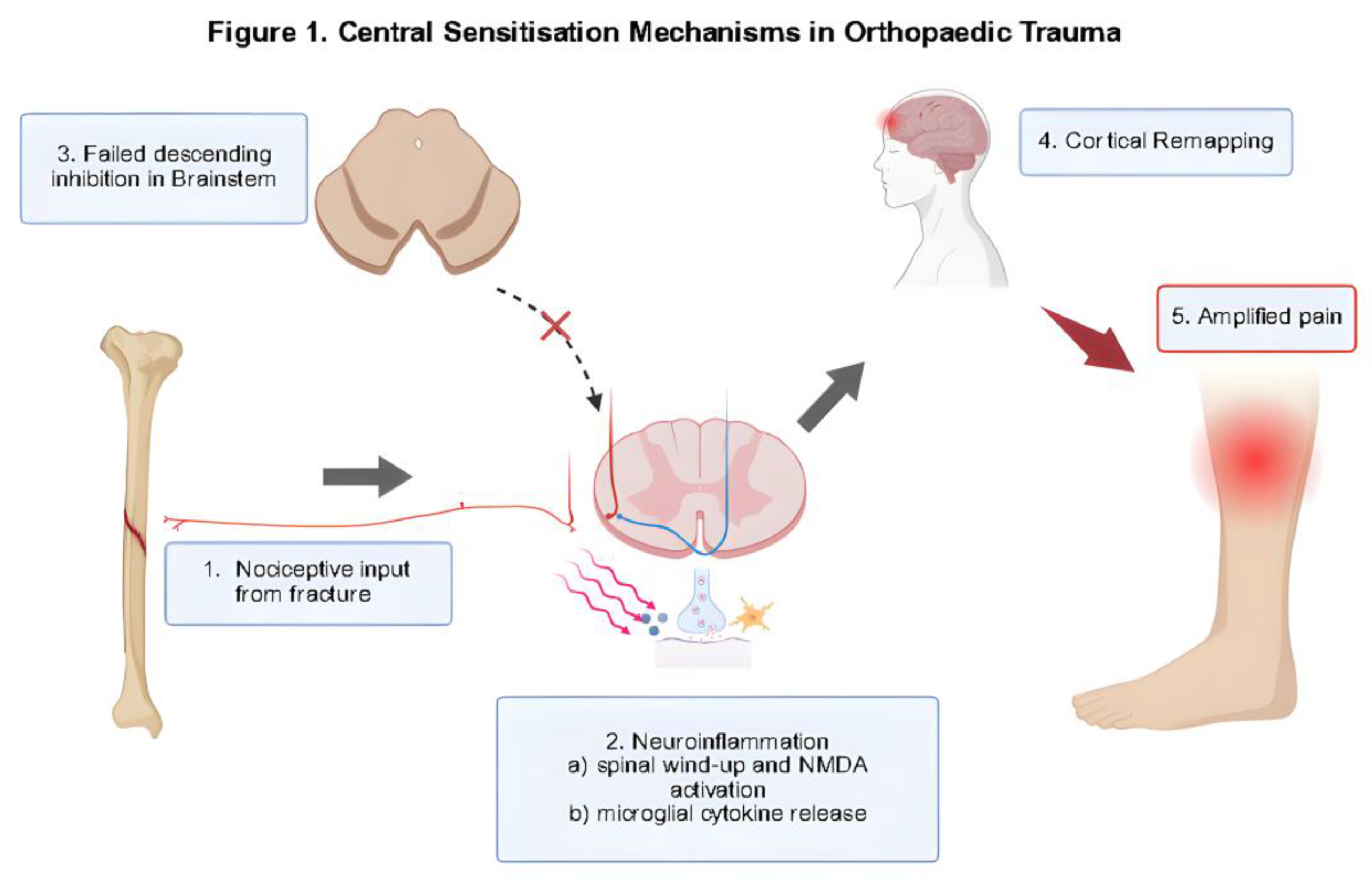
Traumatic injury is a potent trigger of central nervous system plasticity. Acute fractures and soft tissue injuries generate intense and prolonged nociceptive inputs capable of inducing spinal and supraspinal hyperexcitability, altering inhibitory control, and reorganising pain networks. Direct human evidence of this process in patients with orthopaedic trauma was provided by Jodoin et al. [7], who demonstrated early cortical disinhibition on transcranial magnetic stimulation in patients with acute fracture pain. x
These findings are consistent with the experimental and clinical pain literature synthesised by Arendt-Nielsen et al. [20], which showed that sustained deep-tissue nociception facilitates temporal summation, receptive field expansion, referred pain, and widespread hyperalgesia. Trauma, particularly when combined with surgery, prolonged inflammation, and immobilisation, is the biological condition required to trigger this cascade. Neurophysiological studies have demonstrated reduced intracortical inhibition and facilitation within 14 days of fracture, especially in patients with higher acute pain intensity, which is consistent with early cortical disinhibition [7]. Similar alterations in GABAergic and Glutamatergic Circuits are Recognised as Features of Central Sensitisation in chronic pain states [15,24,25].
Preclinical fracture models further reinforce this biological trajectory from tissue injury to sustained central hyperexcitability. Trauma produces substantial and prolonged nociceptive inputs that facilitate dorsal horn and supraspinal sensitisation [26,27]. Chemokine-mediated microglial activation, caspase-dependent synaptic plasticity, and changes in excitatory neurotransmission have been identified as the drivers of persistent fracture-related hyperalgesia [5,28,29]. These mechanisms mirror those observed in established nociplastic pain conditions, supporting the concept that trauma can induce central nervous system adaptations that sustain pain beyond peripheral tissue healing [30,31]. Trauma-specific reviews further indicate that these neuroimmune cascades are more chaotic and heterogeneous than those following elective surgery, in which tissue handling and inflammatory responses are more controlled [32,33].
Clinical trauma data support this mechanistic framework. High rates of neuropathic pain, persistent pain, and disability at 3 to 12 months and at multi-year follow-up suggest that early central changes may persist or evolve into sustained sensitisation in vulnerable individuals [1,2,3,16,17,18]. Together, these findings indicate that central sensitisation can emerge early after trauma and contribute to long-term pain maintenance, particularly in the presence of high nociceptive load, nerve injury, or psychological stress. However, clinical variability also indicates that central sensitisation is not universal and that persistent pain must be interpreted in the context of ongoing tissue pathology, mechanical complications, and peripheral nerve injury. Figure 1 demonstrates the CS mechanisms after Orthopaedic trauma.
4.4. Trauma Versus Elective Surgery
Orthopaedic trauma differs fundamentally from elective surgery in terms of its biological and mechanical characteristics. Trauma is characterised by uncontrolled tissue destruction, high-energy mechanical loading, and variable degrees of nerve and soft-tissue injury, whereas elective surgery involves controlled and predictable operative insult. Mechanistic reviews indicate that the inflammatory and neuroimmune signatures of trauma are substantially more dysregulated than those observed after planned operative injury, with greater cytokine release and wider neuroimmune activation [4,6].
Chunduri et al. [14] further emphasised that perioperative pain trajectories following elective surgery are biologically narrower and more modifiable through analgesic and anaesthetic strategies. In contrast, the heterogeneous and often severe inflammatory and nociceptive environment created by traumatic injury is more likely to overwhelm endogenous inhibitory systems and promote maladaptive central plasticity. This distinction supports the concept that orthopaedic trauma represents a uniquely high-risk context for the development of central sensitisation compared with routine elective orthopaedic procedures.
4.5. Clinical Phenotypes and Diagnostic Features
Clinical manifestations of orthopaedic trauma are heterogeneous and rarely reflect a single pain mechanism. Across trauma cohorts, many patients report persistent or disproportionate pain, sensory amplification, and functional intolerance that cannot be fully explained by tissue status or radiological healing alone [1,2,10]. Widespread hyperalgesia and allodynia have also been reported after injury, consistent with the features of central sensitisation described in broader musculoskeletal pain populations [34,35].
The timing of symptom emergence supports the early contribution of central mechanisms. Neurophysiological evidence shows that disruption of intracortical inhibition and facilitation can occur within 14 days of fracture in patients with moderate-to-severe acute pain, indicating early cortical disinhibition [7]. Clinical trauma data mirror this pattern: severe postoperative pain shortly after orthopaedic trauma surgery is a strong predictor of persistent pain at 12 months, suggesting that sensitisation trajectories are established during the acute recovery phase [8].
Post-traumatic pain typically reflects a mixture of nociceptive, neuropathic, and nociplastic processes rather than a discrete mechanism. Symptoms commonly fluctuate with physical load, sleep quality, emotional distress, and fear avoidance, reflecting the dynamic interactions between peripheral inputs and central modulation [36,37]. Persistent pain after trauma is frequently accompanied by impaired mobility, delayed return to activity, and reduced participation in rehabilitation, particularly in patients with neuropathic features [1,2]. Together, these findings indicate that trauma-related central sensitisation presents as a combined sensory, functional, and behavioural syndrome rather than isolated hyperalgesia.
4.6. Neuropathic Pain as a Practical Clinical Marker of Central Sensitisation
Given the clinical heterogeneity of post-traumatic pain, neuropathic pain features provide a useful and clinically accessible marker for centrally mediated pain states after orthopaedic injury. Across lower limb fracture surgery, pelvic trauma, unstable ankle fractures, and fracture osteosynthesis cohorts, approximately 20–40% of patients meet the screening criteria for neuropathic pain using instruments such as DN4 or painDETECT [2,16,17,18]. These patients consistently reported greater pain severity, worse functional impairment, and poorer health-related quality of life than those without neuropathic features.
Importantly, neuropathic pain in this context does not necessarily reflect isolated peripheral nerve injury. Neuropathic-like symptoms may arise from altered central processing, particularly when they emerge or worsen over time, rather than immediately after trauma [15,24,25,38]. This interpretation is supported by longitudinal data from the WHiST cohort, in which some patients developed neuropathic features between three and six months after fracture surgery, a period during which tissue healing is expected to have progressed substantially [2].
Mechanistic pain research indicates that central sensitisation can generate neuropathic sensory experiences through spinal and supraspinal hyperexcitability, impaired inhibition, and altered somatosensory integration [12,20]. The convergence of these mechanistic insights with trauma cohort data supports the view that neuropathic pain after orthopaedic injury frequently reflects a centrally mediated pain state rather than a persistent peripheral pathology alone.
4.7. Measurement and Diagnostic Limitations
Accurate identification of central sensitisation after orthopaedic trauma remains difficult because no validated trauma-specific diagnostic standards exist. Most tools currently used to infer central pain mechanisms have been developed for chronic musculoskeletal pain populations and show inconsistent performance when applied to trauma cohorts.
Methodological reviews have demonstrated substantial limitations in commonly used measures. Middlebrook et al. [11] reported wide measurement errors and limited reliability across more than 30 CS-related tools, including quantitative sensory testing (QST), temporal summation, and the Central Sensitisation Inventory (CSI). Similarly, Georgopoulos et al. [12] found that although QST can detect sensory hypersensitivity, its ability to predict outcomes or discriminate between central and peripheral mechanisms is variable, limiting its clinical utility in heterogeneous musculoskeletal populations.
In trauma cohorts, neuropathic pain screening tools such as DN4 and painDETECT have been used to identify CS-consistent pain phenotypes. However, these measures overlap substantially with centrally mediated symptoms, complicating their interpretation [2,16]. Widespread pain has also been used as a proxy for central sensitisation; however, population studies indicate that widespread pain is more strongly predicted by baseline psychological distress and somatic symptoms than by trauma exposure, reducing its specificity as a marker of central mechanisms [29].
Neurophysiological measures may offer greater mechanistic specificity than behavioural measures. TMS-derived indices, such as short-interval intracortical inhibition and intracortical facilitation, can detect cortical disinhibition and altered excitability during the acute post-traumatic phase [7]. However, these techniques are resource intensive and lack normative trauma benchmarks. The broader musculoskeletal literature suggests that wearable sensors and ecological momentary assessment may provide complementary insights into pain hypersensitivity and movement avoidance over time [25], although these approaches remain largely untested in trauma populations.
Overall, the absence of a gold-standard diagnostic framework and the limited validity of existing tools constrain both research synthesis and clinical identification of central sensitisation after orthopaedic trauma, contributing to the under-recognition of centrally mediated pain in routine trauma care.
4.8. Implications for Early Diagnosis, Reoperations, and Morbidity
Although no included trauma study directly evaluated whether early identification of central sensitisation reduces reoperation rates or morbidity, several clinically important patterns emerged from trauma evidence. Across cohorts, persistent post-traumatic pain and neuropathic features frequently occurred despite radiographic healing and completion of standard orthopaedic care, indicating that a proportion of patients develop pain states that are not driven by ongoing structural pathology [1,2,16,17,18].
In such patients, continued pain may prompt repeated imaging, injections, or surgical consultations to provide a mechanical explanation. However, trauma cohort data have demonstrated that neuropathic pain features, high early pain burden, and psychological vulnerability are associated with an increased risk of persistent pain and disability [2,8,16]. In the absence of structured screening for centrally mediated pain mechanisms, these individuals may be misclassified as having unresolved tissue pathology, which increases the likelihood of unnecessary or low-yield surgical interventions with potential implications for iatrogenic harm, prolonged recovery, and healthcare utilisation.
Early recognition of CS-consistent phenotypes using neuropathic pain screening, pain trajectories, and psychological risk markers could allow clinicians to redirect patients toward nonsurgical management pathways, including neuropathic pain pharmacotherapy, psychologically informed physiotherapy, graded activity exposure, and pain education. Although prospective trials are required, this represents a biologically and clinically plausible strategy to reduce avoidable reoperations, limit morbidity, and improve long-term outcomes following orthopaedic trauma.
4.9. Interventions and Management Implications
The trauma literature indicates that the early post-injury period represents a critical window during which central sensitisation trajectories may be initiated or modified. Severe acute pain after orthopaedic trauma surgery predicts persistent pain and disability at three months [8], and neurophysiological evidence shows that patients with moderate-to-severe acute fracture pain exhibit early cortical disinhibition within days of injury [7]. Historical trauma cohorts have relied heavily on opioid-based analgesia, and opioid-induced hyperalgesia, together with the limited use of multimodal strategies, has been proposed as a contributor to chronic pain risk [1].
Therefore, perioperative pain frameworks emphasise pre-emptive, opioid-sparing multimodal analgesia [14] with the integration of biological, psychological, and rehabilitative strategies within early trauma pathways [6]. Evidence from reviews of fracture pain further suggests that NSAIDs and COX-2 inhibitors can reduce opioid requirements without impairing healing in specific populations. Together, these findings support the early identification of patients at risk for central sensitisation to guide targeted multimodal analgesia and potentially limit the development of persistent pain.
No trauma cohort directly evaluated treatments that specifically targeted trauma-related central sensitisation. However, narrative evidence supports the use of neuromodulatory pharmacotherapy, such as duloxetine and pregabalin, combined with psychologically informed rehabilitation, graded exposure, and desensitisation-based approaches for patients with CS-consistent pain phenotypes [6,14].
Psychological factors strongly influence treatment response. Catastrophising and perioperative psychological distress are associated with higher acute pain, persistent post-surgical pain, and greater disability at three months [8]. In patients undergoing fracture osteosynthesis, anxiety and depression were significantly higher among those with chronic and neuropathic pain phenotypes [16]. In motor vehicle collision cohorts, the association between trauma exposure and widespread pain was substantially attenuated after adjusting for psychological distress and somatic symptoms [29,39]. PTSD symptoms and psychological distress are also associated with CS-like features, and trauma-exposed chronic pain cohorts demonstrate dose–response relationships between trauma severity and widespread pain, disability, sleep disturbance, anxiety, depression, and somatisation [9,40]. Reviews of chronic post-traumatic pain further emphasise bidirectional interactions between neurobiological sensitisation, stress systems, and psychosocial factors, indicating that rehabilitation should be adapted for hypersensitivity and fear avoidance, with load progression aligned with symptom behaviour [6].
4.10. Clinical Implications
The findings of this scoping review indicate that a substantial proportion of patients develop centrally mediated pain after orthopaedic trauma, characterised by neuropathic features, psychological amplification, and long-term disability that cannot be explained by residual structural pathology alone [1,2,3,16,17,18]. Early identification of patients with high acute pain, neuropathic symptoms, psychological distress, or widespread pain may help clinicians recognise those at risk for central sensitisation [7,8]. In such patients, repeated imaging, revision surgery, or prolonged opioid therapy is unlikely to be effective and may expose them to unnecessary harm.
Instead, a mechanism-based approach incorporating neuromodulatory pharmacotherapy, psychologically informed rehabilitation, pain education, and multidisciplinary care is more appropriate for patients with CS-consistent phenotypes [6,23]. Incorporating a central sensitisation framework into trauma follow-up and fracture clinics could improve patient stratification, guide treatment selection, and reduce progression to long-term pain-related disability after orthopaedic injury.
4.11. Strengths, Limitations, and Future Research Priorities
This scoping review integrates evidence from diverse orthopaedic trauma populations, including fracture surgery, pelvic injury, unstable ankle fractures, and major trauma cohorts, and synthesises clinical, neurophysiological, and psychosocial data to map features consistent with central sensitisation after injury [1,2,3,16,17,18]. A key strength of this study is its focus on primary trauma cohorts rather than extrapolation from elective surgery or non-traumatic musculoskeletal conditions, thus providing clinically relevant insights for trauma care.
This study had several limitations. Direct experimental assessments of central sensitisation, such as quantitative sensory testing or conditioned pain modulation, have rarely been applied, with most studies relying on proxy indicators, including neuropathic pain questionnaires, psychological measures, or disability scores [11,12,38]. Outcome measures were heterogeneous, follow-up durations varied widely, and confounding factors such as injury severity, comorbidity, and baseline pain were inconsistently addressed, limiting causal inference. In addition, the predominance of observational study designs restricts conclusions regarding mechanisms and treatment effects.
These limitations define priorities for future research. There is a need for validated trauma-specific tools to identify central sensitisation and prospective longitudinal studies mapping neurobiological, sensory, and psychological changes from the acute post-injury period through recovery. Importantly, randomised trials are required to test whether early mechanism-based interventions such as multimodal analgesia, pain neuroscience education, psychologically informed rehabilitation, or neuromodulatory therapies can prevent or attenuate the development of centrally mediated pain. Finally, translation into clinical practice will require integration of central sensitisation screening and management frameworks into routine trauma pathways, fracture clinics, and rehabilitation services.
5. Conclusions
This scoping review demonstrates that persistent pain after orthopaedic trauma is common and frequently exhibits features consistent with central sensitisation, including neuropathic pain, psychological amplification, early central nervous system disinhibition, and long-term functional impairment. Across diverse trauma cohorts, pain often persists well beyond structural healing, indicating that ongoing nociception alone does not fully explain post-traumatic pain outcomes. Although direct experimental assessment of central sensitisation remains limited in trauma research, the convergence of clinical, neurophysiological, and psychosocial evidence supports the central role of pain amplification mechanisms in a substantial subgroup of patients. Failure to recognise these mechanisms risks misdirected investigations and ineffective interventions. Future trauma research should prioritise the early identification of central sensitisation using standardised measures and evaluate mechanism-based, multidisciplinary interventions aimed at preventing long-term disability. Recognising central sensitisation as a key contributor to post-traumatic pain represents an important step towards more precise, effective, and patient-centred orthopaedic trauma care.
Supplementary Materials
following supporting information can be downloaded at the website of this paper posted on Preprint.org. Table S1: Detailed characteristics and data extraction for all included sources of evidence.
Author Contributions
Conceptualization, A.S. and A.C.; methodology, A.S.;formal analysis, A.S.; investigation, A.S. and A.C.; resources, A.A. and U.H.; data curation, A.S.; writing—original draft preparation, A.S.; writing—review and editing, A.S., A.C., A.A., A.N., and U.H.; visualization, A.S.; supervision, A.C.; project administration, A.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable. This study is a scoping review of published literature and did not involve the collection or analysis of individual-level patient data.
Informed Consent Statement
Not applicable. This study did not involve the direct participation of human subjects.
Data Availability Statement
No new data was created or analysed in this study. All data supporting the findings of this scoping review are derived from publicly available published sources, which are cited within the manuscript and listed in the reference section.
Acknowledgments
The authors thank their respective NHS Trusts for institutional support and protected academic times.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
ACR—American College of Rheumatology; BPI—Brief Pain InventoryCPGQ—Chronic Pain Grading Questionnaire; CPSP—Chronic Post-Surgical Pain; CS—Central Sensitisation; CSI—Central Sensitisation InventoryDASH—Disabilities of the Arm, Shoulder and Hand; DN4—Douleur Neuropathique 4 Questions; DN4i—DN4 interview; DRI—Disability Rating Index; EQ-5D—EuroQol-5 Dimensions; EQ-5D-3L—EuroQol-5 Dimensions, three-level version; EQ-5D-5L—EuroQol-5 Dimensions, five-level version; GHQ—General Health Questionnaire; HADS—Hospital Anxiety and Depression Scale; HADS-A—Hospital Anxiety Scale; HADS-D—Hospital Depression Scale; ICF—Intracortical Facilitation; ISS—Injury Severity Score; K10—Kessler Psychological Distress Scale; LICI—Long-Interval Intracortical Inhibition; MPQ—McGill Pain Questionnaire; MPSS—Mainz Pain Staging System; MPOPS—Multidimensional Post-operative Pain Scale; MVC—Motor-Vehicle Collision; NRS—Numerical Rating Scale; ORIF—Open Reduction and Internal Fixation; PACU—Post-Anesthesia Care Unit; PCS—Pain Catastrophizing Scale; PCL—PTSD Checklist; PHQ-9—Patient Health Questionnaire-9; PPP—Post-traumatic Pelvic Pain; PRISMA-ScR—Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews; QST—Quantitative Sensory Testing; rMT—Resting Motor Threshold; RR—Relative Risk; SES—Subjective Experience of Sensation; SF-8—Short Form-8 Health Survey; SF-12—Short Form-12 Health Survey; SICI—Short-Interval Intracortical Inhibition; SMFA—Short Musculoskeletal Function Assessment; SSC—Somatic Symptoms Checklist; TMS—Transcranial Magnetic Stimulation; VAS—Visual Analogue Scale; VR-12—Veterans RAND 12-Item Health Survey; WHODAS—World Health Organisation Disability Assessment Schedule; WHiST—Wound Healing in Surgical Trauma Trial; WP—Widespread Pain Appendix A
References
- Kolstadbraaten, K.M.; Spreng, U.J.; WisloeffAase, K.; Gaarder, C.; Naess, P.A.; Raeder, J. Incidence of Chronic Pain 6 y after Major Trauma. Acta Anaesthesiologica Scandinavica 2019, 63, 1074–1078. [Google Scholar] [CrossRef] [PubMed]
- Keene, D.J.; Knight, R.; Bruce, J.; Dutton, S.J.; Tutton, E.; Achten, J.; Costa, M.L. Chronic Pain with Neuropathic Characteristics after Surgery for Major Trauma to the Lower Limb: Prevalence, Predictors, and Association with Pain Severity, Disability, and Quality of Life in the UK WHiST Trial. The Bone & Joint Journal 2021, 103-B, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, H.; Layne, J.; Yamaura, K.; Marcucio, R.; Morioka, K.; Basbaum, A.I.; Weinrich, J.A.P.; Bahney, C.S. A Bad Break: Mechanisms and Assessment of Acute and Chronic Pain after Bone Fracture. Pain 2025, 166, e491–e505. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Zhang, H.; Li, N.; Li, J.; Zhang, L. Chronic Pain after Bone Fracture: Current Insights into Molecular Mechanisms and Therapeutic Strategies. Brain Sciences 2022, 12. [Google Scholar] [CrossRef]
- Harte, S.; Harris, R.; Clauw, D. The Neurobiology of Central Sensitization. Journal of Applied Biobehavioral Research 2018. [Google Scholar] [CrossRef]
- Hartman Budnik, J.V.; Higgins, T.F.; Malfait, A.-M.; Weinrich, J.A.P.; Basbaum, A.I.; Hsu, J.R.; Morshed, S.; Bahney, C.S. New Paradigms in Pain Management after Skeletal Trauma: Orthopaedic Trauma Association’s 2023 Basic Science Focus Forum Symposium. OTA International 2025, 8. [Google Scholar] [CrossRef]
- Jodoin, M.; Rouleau, D.M.; Bellemare, A.; Provost, C.; Larson-Dupuis, C.; Sandman, E.; Laflamme, G.-Y.; Benoit, B.; Leduc, S.; Levesque, M.; et al. Moderate to Severe Acute Pain Disturbs Motor Cortex Intracortical Inhibition and Facilitation in Orthopaedic Trauma Patients: A TMS Study. PLOS ONE 2020, 15, e0226452. [Google Scholar] [CrossRef]
- Edgley, C.; Hogg, M.; De Silva, A.; Braat, S.; Bucknill, A.; Leslie, K. Severe Acute Pain and Persistent Post-Surgical Pain in Orthopaedic Trauma Patients: A Cohort Study. British Journal of Anaesthesia 2019, 123, 350–359. [Google Scholar] [CrossRef]
- Manuel, J.; Rudolph, L.; Beissner, F.; Neubert, T.-A.; Dusch, M.; Karst, M. Traumatic Events, Post-traumatic Stress Disorder, and Central Sensitization in Chronic Pain Patients of a German University Outpatient Pain Clinic. Psychosomatic Medicine 2023, 85, 351–357. [Google Scholar] [CrossRef]
- Karateev, A.; Nesterenko, V.; Makarov, M.; Lila, A. Chronic Post-traumatic Pain: Rheumatological and Orthopaedic Aspects. Rheumatology Science and Practice 2022. [Google Scholar] [CrossRef]
- Middlebrook, N.; Rushton, A.; Abichandani, D.; Kuithan, P.; Heneghan, N.; Falla, D. Measures of Central Sensitization and Their Measurement Properties in Musculoskeletal Trauma: A Systematic Review. European Journal of Pain 2020, 25, 71–87. [Google Scholar] [CrossRef]
- Georgopoulos, V.; Akin-Akinyosoye, K.; Zhang, W.; McWilliams, D.; Hendrick, P.; Walsh, D. Quantitative Sensory Testing and Predicting Outcomes for Musculoskeletal Pain, Disability, and Negative Affect: A Systematic Review and Meta-Analysis. Pain 2019. [Google Scholar] [CrossRef] [PubMed]
- Wynne-Jones, G.; Macfarlane, G.J.; Silman, A.J.; Jones, G.T. Does Physical Trauma Lead to an Increase in the Risk of New Onset Widespread Pain? Annals of the Rheumatic Diseases 2006, 65, 391–393. [Google Scholar] [CrossRef] [PubMed]
- Chunduri, A.; Aggarwal, A.K. Multimodal Pain Management in Orthopaedic Surgery. Journal of Clinical Medicine 2022, 11, 6386. [Google Scholar] [CrossRef] [PubMed]
- Nijs, J.; Goubert, D.; Ickmans, K. Recognition and Treatment of Central Sensitization in Chronic Pain Patients: Not Limited to Specialized Care. Journal of Orthopaedic & Sports Physical Therapy 2016, 46, 1024–1028. [Google Scholar] [CrossRef]
- Aulenkamp, J.L.; Malewicz, N.M.; Brauckhoff, J.D.; Zahn, P.K.; Ebel, M.; Schnitzler, R.; Clever, J.; Geßmann, J.; Bauer, M.; Meyer-Frießem, C.H. Chronic Pain Following Fracture-Related Surgery: Post-traumatic Rather Than Postsurgical Origin Promotes Chronification—A Prospective OOrthopaedical Study With 1-Year Follow-Up. Anesthesia & Analgesia 2022, 134, 974–986. [Google Scholar] [CrossRef]
- Gerbershagen, H.J.; Dagtekin, O.; Isenberg, J.; Martens, N.; Özgür, E.; Krep, H.; Sabatowski, R.; Petzke, F. Chronic Pain and Disability After Pelvic and Acetabular Fractures—Assessment With the Mainz Pain Staging System. Journal of Trauma: Injury, Infection & Critical Care 2010, 69, 128–136. [Google Scholar] [CrossRef]
- Rbia, N.; Van Der Vlies, C.H.; Cleffken, B.I.; Selles, R.W.; Hovius, S.E.R.; Nijhuis, T.H.J. High Prevalence of Chronic Pain With Neuropathic Characteristics After Open Reduction and Internal Fixation of Ankle Fractures. Foot Ankle Int. 2017, 38, 987–996. [Google Scholar] [CrossRef]
- Castillo, R.C.; Raja, S.N.; Frey, K.P.; Vallier, H.A.; Tornetta, P.; Jaeblon, T.; Goff, B.J.; Gottschalk, A.; Scharfstein, D.O.; O’Toole, R.V.; et al. Improving Pain Management and Long-Term Outcomes Following High-Energy Orthopaedic Trauma (Pain Study). Journal of Orthopaedic Trauma 2017, 31, S71–S77. [Google Scholar] [CrossRef]
- Arendt-Nielsen, L.; Fernández-de-las-Peñas, C.; Graven-Nielsen, T. Basic Aspects of Musculoskeletal Pain: From Acute to Chronic Pain. Journal of Manual & Manipulative Therapy 2011, 19, 186–193. [Google Scholar] [CrossRef]
- Langeveld, M.; Raasveld, F.V.; Hundepool, C.A.; Hagenaars, T.; Spijkerman, D.C.M.; Eberlin, K.R.; Zuidam, J.M. Neuropathic Pain after Major Limb Amputation: A Cross-Sectional Study. Plastic & Reconstructive Surgery 2025, 155, 419e–427e. [Google Scholar] [CrossRef]
- Alkassabi, O.; Voogt, L.; Andrews, P.; Alhowimel, A.; Nijs, J.; Alsobayel, H. Risk Factors to Persistent Pain Following Musculoskeletal Injuries: A Systematic Literature Review. IJERPH 2022, 19, 9318. [Google Scholar] [CrossRef] [PubMed]
- Rosenbloom, B.; Khan; McCartney; Katz, J. Systematic Review of Persistent Pain and Psychological Outcomes Following Traumatic Musculoskeletal Injury. JPR 2013, 39. [Google Scholar] [CrossRef] [PubMed]
- Nijs, J.; George, S.Z.; Clauw, D.J.; Fernández-de-las-Peñas, C.; Kosek, E.; Ickmans, K.; Fernández-Carnero, J.; Polli, A.; Kapreli, E.; Huysmans, E.; et al. Central Sensitisation in Chronic Pain Conditions: Latest Discoveries and Their Potential for Precision Medicine. The Lancet Rheumatology 2021, 3, e383–e392. [Google Scholar] [CrossRef]
- Watson, J.A.; Ryan, C.G.; Cooper, L.; Ellington, D.; Whittle, R.; Lavender, M.; Dixon, J.; Atkinson, G.; Cooper, K.; Martin, D.J. Pain Neuroscience Education for Adults With Chronic Musculoskeletal Pain: A Mixed-Methods Systematic Review and Meta-Analysis. The Journal of Pain 2019, 20, 1140.e1–1140.e22. [Google Scholar] [CrossRef]
- Carlton, S.; Du, J.; Tan, H.; Nesic, O.; Hargett, G.; Bopp, A.; Yamani, A.; Lin, Q.; Willis, W.; Hulsebosch, C. Peripheral and Central Sensitization in Remote Spinal Cord Regions Contribute to Central Neuropathic Pain after Spinal Cord Injury. PAIN® 2009, 147, 265–276. [Google Scholar] [CrossRef]
- Winkelstein, B. Mechanisms of Central Sensitization, Neuroimmunology & Injury Biomechanics in Persistent Pain: Implications for Musculoskeletal Disorders. Journal of electromyography and kinesiology: Official journal of the International Society of Electrophysiological Kinesiology 2004, 14 1, 87–93. [Google Scholar] [CrossRef]
- Ji, R.; Nackley, A.; Huh, Y.; Terrando, N.; Maixner, W. Neuroinflammation and Central Sensitization in Chronic and Widespread Pain. Anesthesiology 2018, 129 2, 343–366. [Google Scholar] [CrossRef]
- Donnelly, C.; Andriessen, A.; Chen, G.; Wang, K.; Jiang, C.; Maixner, W.; Ji, R. Central Nervous System Targets: Glial Cell Mechanisms in Chronic Pain. Neurotherapeutics 2020, 17, 846–860. [Google Scholar] [CrossRef]
- Tanaka, K.; Murata, S.; Nishigami, T.; Mibu, A.; Manfuku, M.; Shinohara, Y.; Tanabe, A.; Ono, R. The Central Sensitization Inventory Predicts Painrelated Disability for Musculoskeletal Disorders in the Primary Care Setting. European Journal of Pain 2019, 23, 1640–1648. [Google Scholar] [CrossRef]
- Wang, H.-Q.; Varrassi, G. Emerging Basic and Clinical Studies on Musculoskeletal Pain and Management. Pain Research and Management 2020, 2020, 1–2. [Google Scholar] [CrossRef]
- Richeb\’ e, P.; Capdevila, X.; Rivat, C. Persistent Postsurgical Pain: Pathophysiology and Preventative Pharmacologic Considerations. Anesthesiology 2018, 129, 590. [Google Scholar] [CrossRef]
- Reddi, D.; Curran, N. Chronic Pain after Surgery: Pathophysiology, Risk Factors and Prevention. Postgraduate Medical Journal 2014, 90, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Rold\’ an-Jim\’ enez, C.; P\’ erez-Cruzado, D.; Neblett, R.; Gatchel, R.; Cuesta-Vargas, A. Central Sensitization in Chronic Musculoskeletal Pain Disorders in Different Populations: A Cross-Sectional Study. Pain Medicine 2020, 21, 2958–2963. [Google Scholar] [CrossRef] [PubMed]
- Van Griensven, H.; Schmid, A.; Trendafilova, T.; Low, M. Central Sensitization in Musculoskeletal Pain: Lost in Translation? The Journal of orthopaedic and sports physical therapy 2020, 50 11, 592–596. [Google Scholar] [CrossRef] [PubMed]
- Louw, A.; Zimney, K.; Puentedura, E.J.; Diener, I. The Efficacy of Pain Neuroscience Education on Musculoskeletal Pain: A Systematic Review of the Literature. Physiotherapy Theory and Practice 2016, 32, 332–355. [Google Scholar] [CrossRef]
- Yücel, F.N.; Sanal-Toprak, C. Central Sensitization-Related Symptoms and Their Relationship to Disability in Prevalent Chronic Musculoskeletal Pain: A Cross-Sectional Study. Musculoskeletal Science and Practice 2024, 73, 103147. [Google Scholar] [CrossRef]
- Nijs, J.; Van Houdenhove, B.; Oostendorp, R.A.B. Recognition of Central Sensitization in Patients with Musculoskeletal Pain: Application of Pain Neurophysiology in Manual Therapy Practice. Manual Therapy 2010, 15, 135–141. [Google Scholar] [CrossRef]
- Lütolf, R.; Rosner, J.; Curt, A.; Hubli, M. Indicators of Central Sensitization in Chronic Neuropathic Pain after Spinal Cord Injury. European Journal of Pain (London, England) 2022, 26, 2162–2175. [Google Scholar] [CrossRef]
- McKernan, L.; Johnson, B.; Crofford, L.; Lumley, M.; Bruehl, S.; Cheavens, J. Post-traumatic Stress Symptoms Mediate the Effects of Trauma Exposure on Clinical Indicators of Central Sensitization in Patients With Chronic Pain. The Clinical Journal of Pain 2019, 35, 385. [Google Scholar] [CrossRef]

Table 1.
Characteristics of Included Trauma Cohorts.
| Study | Country | Design | n | Trauma | Follow-up | CS Construct | CS Measures | Pain Outcomes | Function/QoL | Psych | Adjusted Analyses |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Keene 2021 [2] | UK | Multicentre RCT secondary analysis | 1,547 (DN4 933) | Lower-limb fractures | 3, 6 m | Neuropathic phenotype | DN4, NRS | Neuropathic pain; NRS | DRI; EQ-5D-5L | – | ISS, baseline pain, age, sex |
| Aulenkamp 2022 [16] | Germany | Prospective cohort | 82 | Fracture osteosynthesis | Pre-op–12 m | CPSP/neuropathic | DN4i; painDETECT | CPSP; NP | BPI; EQ-5D | HADS | Not stated |
| Kolstadbraaten 2019 [1] | Norway | Retrospective cohort | 68 | Major blunt trauma | 6 y | Acute sensitisation (conceptual) | Custom | Chronic pain | – | – | ISS-adjusted logistic |
| Gerbershagen 2010 [17] | Germany | Cross-sectional follow-up | 69 | Pelvic fractures | 52 m | Pain chronicity | MPSS; painDETECT | PPP; NRS; CPGQ | ODI; Majeed; SF-12 | HADS | Nerve injury vs. MPSS |
| Rbia 2017 [18] | Netherlands | Retrospective survey | 271 | Ankle ORIF | 5.8 y | Neuropathic pain | DN4; MPQ | Persistent pain; NP | QoL/work | – | Multivariable |
| Castillo 2017 [19] | USA | Multicentre RCT | 495 | Extremity fractures | 3–12 m | Persistent pain risk | painDETECT; BPI | Acute & chronic pain | SMFA; VR-12 | PHQ-9; PCL | ITT; centre-adjusted |
| Edgley 2019 [8] | Australia | Prospective cohort | 229 | Trauma surgery | 3 m | Psych–pain vulnerability | NRS; PCS; WHODAS | PPSP | WHODAS | K10; PCS | Multivariable |
| Jodoin 2020 [7] | Canada | Case–control neurophysiology | 56 + 28 | Upper-limb fractures | ≤14 d | Cortical disinhibition | TMS (SICI; ICF) | NRS ≥4 | DASH | – | Pain→SICI |
| Wynne-Jones 2006 [13] | UK | Prospective cohort | 490 | MVC | 6 m | Widespread pain | Body manikin | New WP | SF-8 | GHQ; SSC | Poisson-adjusted |
Abbreviations: CS = central sensitisation; RCT = randomised controlled trial; DN4 = Douleur Neuropathique en 4 questions; NRS = numerical rating scale; DRI = Disability Rating Index; EQ-5D = EuroQol-5 Dimension; CPSP = chronic postsurgical pain; NP = neuropathic pain; BPI = Brief Pain Inventory; HADS = Hospital Anxiety and Depression Scale; ISS = Injury Severity Score; MPSS = Mainz Pain Staging System; PPP = post-traumatic pelvic pain; CPGQ = Chronic Pain Grade Questionnaire; ODI = Oswestry Disability Index; MPQ = McGill Pain Questionnaire; ORIF = open reduction and internal fixation; SMFA = Short Musculoskeletal Function Assessment; VR-12 = Veterans RAND 12-Item Health Survey; PHQ-9 = Patient Health Questionnaire-9; PCL = PTSD Checklist; PCS = Pain Catastrophizing Scale; WHODAS = World Health Organization Disability Assessment Schedule; K10 = Kessler Psychological Distress Scale; TMS = transcranial magnetic stimulation; SICI = short-interval intracortical inhibition; ICF = intracortical facilitation; DASH = Disabilities of the Arm, Shoulder and Hand; SF-8 = Short-Form-8; GHQ = General Health Questionnaire; SSC = Somatic Symptoms Checklist; MVC = motor vehicle collision; ITT = intention-to-treat.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



