
Submitted:
25 December 2025
Posted:
30 December 2025
You are already at the latest version
Abstract
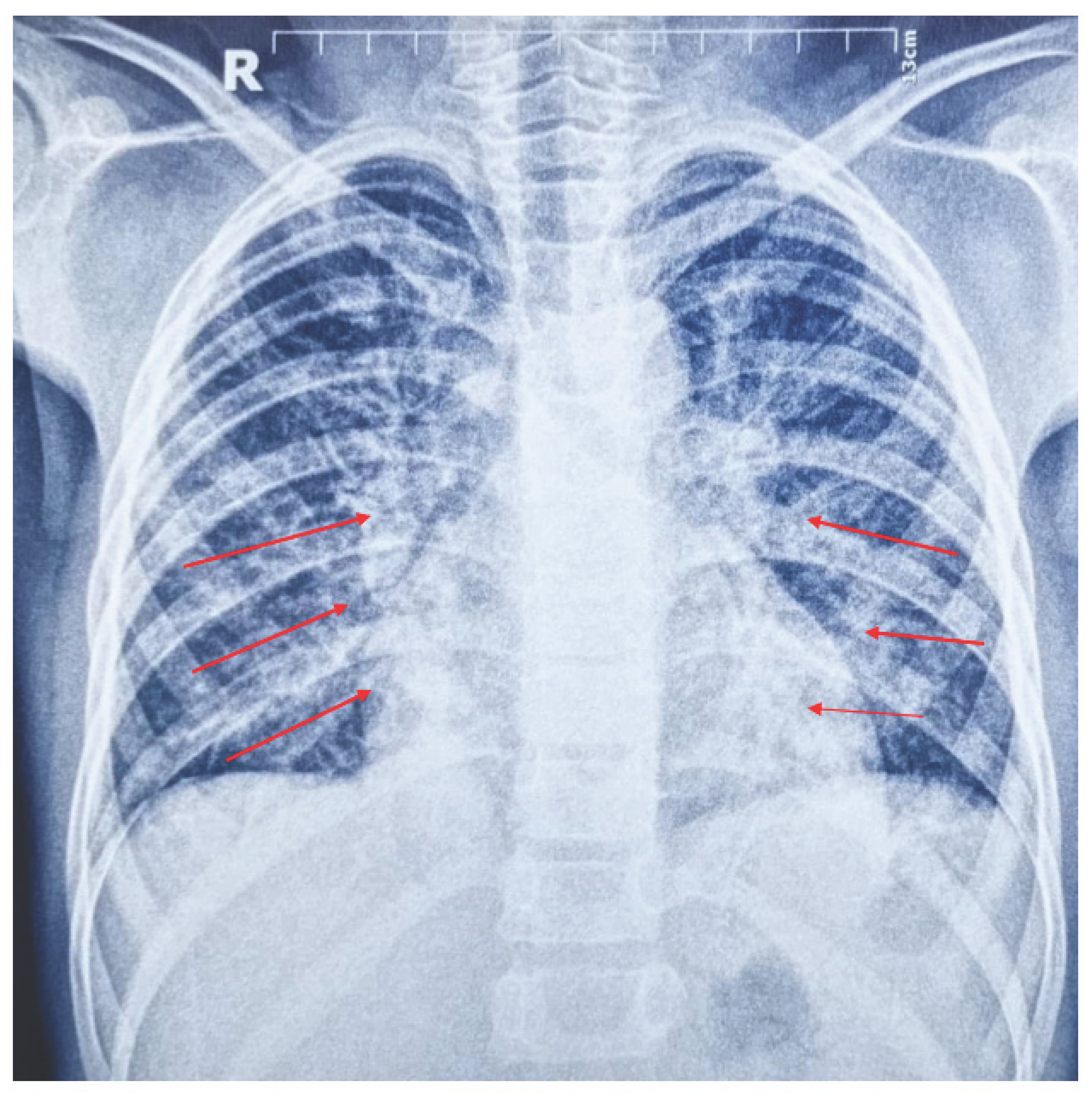
Background: Post-streptococcal glomerulonephritis (PSGN) is a common cause of acute nephritic syndrome in children. Rarely, it may result in life-threatening complications, including acute pulmonary edema and critical hyperkalemia. Case Presentation: We report a 10-year-old Yemeni girl (25 kg) presenting with severe respiratory distress, irritability, and generalized pitting edema. Laboratory tests confirmed PSGN with markedly reduced complement C3 (42.2 mg/dL) and nephritic urine sediment containing numerous red blood cells and casts. The patient developed critical hyperkalemia (7.0 mmol/L) and acute pulmonary edema, requiring urgent intubation and mechanical ventilation using pressure-controlled mandatory ventilation (P-CMV). Management: Aggressive fluid mobilization and electrolyte stabilization were initiated. High-dose intravenous furosemide (4 mg/kg/day), renal-dose dopamine (5 μg/kg/min), and potassium-lowering interventions were applied. Morphine sedation (0.1 mg/kg/dose) was administered every 4 hours during the first 24 hours, then every 8 hours for 12 additional hours, followed by withdrawal prior to extubation. Morphine effectively controlled irritability and optimized patient–ventilator synchronization. The patient produced 1700 mL urine in 17 hours, demonstrating a strong diuretic response. Conclusion: Early recognition of severe extra-renal complications in PSGN is critical. Intensive supportive care—including mechanical ventilation, meticulous fluid and electrolyte management, and appropriate sedation—is essential for survival in cases of acute pulmonary edema and critical hyperkalemia.
Keywords:
1. Introduction
2. Case Presentation
Initial Assessment
Diagnostic Investigations
Management and Clinical Course
- Diuretics: High-dose IV furosemide (4 mg/kg/day)
- Renal support: Renal-dose dopamine (5 μg/kg/min)
- Electrolyte management: Salbutamol nebulization and strict potassium restriction
- Fluid balance: Input calculated including insensible losses (400 mL/m²) plus prior urine output
- Antimicrobials: IV ampicillin/sulbactam (100 mg/kg), followed by oral azithromycin
3. Discussion
Sedation and Ventilatory Support
Renal Hemodynamics and Diuresis
Electrolyte Management
Diagnostic Reliability and Prognosis
4. Conclusion
5. Limitations
6. Acknowledgments
7. Author Contributions
- Mansoor Khalid Mansoor Ayish: Conceptualization, clinical data collection, primary manuscript drafting
- Hussein Mussa Muafa: Manuscript revision and critical review
- Ali Abdu Abdelbaky Mohamed: Clinical supervision, final manuscript approval
8. Declarations
Funding
References
- Hassanein, M; Gudsoorkar, P; Padala, SA; et al. Infection-Related Glomerulonephritis. [Updated 2025 Dec 13]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island (FL), Jan 2025; Available online: https://www.ncbi.nlm.nih.gov/books/NBK538255/.
- Rodriguez-Iturbe, B; Haas, M. Post-Streptococcal Glomerulonephritis. In Streptococcus pyogenes: Basic Biology to Clinical Manifestations [Internet]; Ferretti, JJ, Stevens, DL, Fischetti, VA, Eds.; University of Oklahoma Health Sciences Center: Oklahoma City (OK), 10 Feb 2016. [Google Scholar] [PubMed]
- Alhamoud, MA; Salloot, IZ; Mohiuddin, SS; AlHarbi, TM; Batouq, F; Alfrayyan, NY; Alhashem, AI; Alaskar, M. A Comprehensive Review Study on Glomerulonephritis Associated With Post-streptococcal Infection. Cureus 2021, 13(12), e20212. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Munif, MR; Hart, RA; Rafeek, RAM; Mallawaarachchi, AC; Anderson, L; McMillan, DJ; Sriprakash, KS; Ketheesan, N. Mechanisms that potentially contribute to the development of post-streptococcal glomerulonephritis. Pathog Dis. 2024, 82, ftae024. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Geetha, Duvuru. Poststreptococcal Glomerulonephritis. Medscape. Updated 2023 sep 25. Available online: https://emedicine.medscape.com/article/240337-overview (accessed on 21 December 2025).
- Chiu, CY; Huang, YC; Wong, KS; Hsia, SH; Lin, CJ; Lin, TY. Poststreptococcal glomerulonephritis with pulmonary edema presenting as respiratory distress. Pediatr Nephrol 2004, 19(11), 1237–40. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



