
Submitted:
29 December 2025
Posted:
30 December 2025
You are already at the latest version
Abstract
Objective: To compare oral health-related quality of life (OHRQoL) between patients undergoing root canal treatment (RCT) and tooth extraction in Malaysia. Methods: A cross-sectional study was conducted among 484 adult patients (243 RCT, 241 extrac-tion) attending public restorative dental clinics in Selangor and Kuala Lumpur. Par-ticipants completed the validated 14-item Malaysian Oral Health Impact Profile (S-OHIP(M)). Independent t-tests and chi-square tests were applied (p < 0.05). Results: The RCT group reported significantly lower mean OHIP-14 scores (12.9 ± 8.4) com-pared to the extraction group (18.5 ± 10.5), indicating better OHRQoL. Across all OHIP-14 domains, RCT patients experienced fewer functional limitations, less pain, reduced psychological discomfort, and lower social handicap. Sociodemographic dif-ferences were observed in age, gender, and education, but not ethnicity. Conclusion: RCT is associated with better OHRQoL outcomes than extraction, supporting its role as a tooth-preserving, cost-effective option. Findings highlight the importance of inte-grating patient-centred outcomes into oral health policy and clinical decision-making.
Keywords:
oral health-related quality of life
; root canal treatment
; tooth extraction
; OHIP-14
; Malaysia
; restorative dentistry
1. Introduction
In 2022, the World Health Organization reported that almost 3.5 billion people worldwide suffered from oral diseases [1]. Dental caries, periodontal disease, and tooth loss remain highly prevalent across all age groups in the Southeast Asia region. This region recorded more than 900 million cases on untreated dental caries of deciduous teeth with an estimated prevalence of 43.8%, untreated caries of permanent teeth with 28.7% of estimated cases and edentulism with 4.1% of prevalence. This region has the highest oral cancer incidence and mortality among all WHO regions [2].
In Malaysia, national oral health surveys reported an improvement with decreases in tooth extraction and improved retention of functional teeth among adults [3]. Root Canal Treatment (RCT) is a major advantage as it preserves the natural tooth, maintaining the normal chewing function, occlusion and aesthetics. While with tooth extraction, the bone remodelling and resorption usually follows with a more pronounced buccal plate area. However, RCT might be complex, and it requires careful cleaning, disinfection, shaping of the root canal system and sealing. Failure to do so might lead to infection or surgical treatment [4]. In terms of cost, RCT is more expensive ($689.10) as compared to simple extraction ($280.10) among Swedish adults [5]. However, if the extracted tooth was replaced, the cost was even higher ($1245.50). This study also indicates no differences in the QALYs for both groups.
Nonetheless, disparities persist especially among elderly and lower income groups [6]. Malaysia had a revised set of Oral Health Goals 2010 adapting to current challenges, recent evidence and changing health priorities parallel to Malaysia’s population [2]. The objective is to improve health status and quality of life caused by oral conditions. This was mainly set to achieve through lifelong wellness, reducing levels of morbidity and mortality caused by oral conditions. Targets were set at 76.9% and 23.9% of 35-44 and 60-70 age groups respectively having at least 20 functional teeth.
The Oral Health Related Quality of Life (OHRQoL) captures functional, psychological and social impacts of oral health. It goes beyond clinical indicators but reflects how an individual's oral condition influences the person’s ability to eat, speak and interact socially [7]. Oral Health Impact Profile (OHIP) is a standardized tool developed by Slade & Spencer used to measure OHRQoL [8]. The initial 49 statements described the consequences of oral disorders (OHIP-49). In 1997, Slade developed OHIP-14, with good reliability, validity and precision. This version was widely used with language modifications and regional concerns [9].
The OHIP-14 Malaysia has been a cultural adaptation, linguistic and validated for the Malaysian population [10]. It has been adapted to represent and capture the language and cultural interpretation pertaining to pains or discomfort, cultural norms on aesthetics and the differences in health-seeking behaviour [10]. It is widely used in cross sectional studies investigating ranges of OHRQoL of Malaysian population from periodontitis, decayed, missing or filled teeth or basic periodontal services [11,12,13]. S-OHIP(M) is used for general oral health impact assessment and can also be used for condition-specific assessment with its own specific version [14]. Research involving tools has shown that oral conditions like periodontitis affect specific domains of OHRQoL especially on psychological domains and physical pain. Studies also indicate that observable differences can be seen across ethnicity and socioeconomic status [15,16]. These studies showed consistent cultural adaptation using S-OHIP (M) with broad application across populations of specific clinical groups. This tool also reflects its versatility across oral health impact from basic examination and diseases.
Evidence indicated positive impact on OHRQoL among root canal treatment patients as opposed to tooth extraction among adults and children’s patients [17,18]. Local studies also have been focusing on naval officers and athletes [19,20]. However, lack of local study demonstrates the difference of OHRQoL between RCT and tooth extraction among adults in Malaysia. Thus, this study aimed to understand an adult patient’s perspective by evaluating the effect of root canal treatment quality of life as with patients who underwent tooth extraction in daily life.
2. Materials and Methods
Study Design
This cross-sectional study was carried out involving patients attending selected Restorative Dental Clinics in Malaysia. The selection of the clinics was done purposively based on the level of willingness of the specialists in participation of this study.
Sample Size Calculation
Sample size was calculated based on Dhand & Khatkar (2014) considering an expected population standard deviation (SD) of 10.9 to estimate a mean with 95% confidence and a precision of 1.5. The expected number of participants is 206 individuals per group [21].
Data Collection
The data collection period was from January to December 2023 (twelve months). A total of 484 participants were recruited at 10 different Restorative Clinics in the study from Selangor and Wilayah Persekutuan Kuala Lumpur. For the RCT group, a total of 243 participants were recruited and 241 participants recruited for the Tooth Extraction group. The inclusion criteria were patients aged 18 years old and above, patients that were referred from endodontic treatment at a restorative dental clinic and patients presented with clinical evidence of pulp or periapical tissue problems indicating a need for root canal treatment. The exclusion criteria were patients exhibited with uncontrolled periodontal disease, patients with serious medical conditions that required hospitalisations in the past and patients that required physician consultation before dental treatment. Disability patients and patients with communication disabilities were also excluded. The study protocol was registered with NMRR-17-3485-37374 S2 R2 and approved by Medical Research Ethics Committee (MREC), Ministry of Health Malaysia.
Patients attending the study sites were screened for eligibility during the clinic visits. The selection was done using convenience sampling. The patients were personally invited to join this study. For the RCT group, participants were invited to the study after they completed their RCT treatment while participants in the Tooth Extraction group were invited prior to their consultation session at the clinic. The purpose of this study was explained to the patients and informed consent was obtained. The questionnaires were answered by the patients and collected upon completion.
Instrument
The study used a modified 14-item Oral Health Impact Profile (Malaysia) S-OHIP (M)[10], which had been validated for use in the Malay and English language. The questionnaire comprises three sections. Section A consists of 14 items. It has domains of physical pain (questions A6 – A12), oral functional limitations (questions A1- A5, A13), and psychological discomfort (question A14). Section B has three questions on general self-perception on oral health status; section C consists of 4 questions on tooth condition and finally section D has 4 questions on the patient's social demographic and economic background.
Patients were asked to complete the survey. A five-point Likert scale was used to assess patients’ oral impacts throughout the previous 12 months. The scale ranges from ‘0’ for ‘never’, ‘1’ for ‘hardly ever’, ‘2’ for ‘occasionally’, ‘3’ for ‘fairly often’ and ‘4’ for ‘very often’. The total ordinal response indicates the severity of the individual patients’ impact. The mean severity score is equal to the mean OHIP score, and the severity impact can range from 0 to 56. Poorer OHRQoL is indicated by a higher OHIP score. The prevalence of impact, or the proportion of participants who answered "fairly often" or "very often" to one or more items, was also ascertained.
Data management and Analysis
Data entered and managed using IBM (SPSS Statistics) version 25.0. Data were initially tabulated using frequency and percentages. Descriptive statistics are used to describe sociodemographic characteristics. Chi-square test and student t-test was used to compare the differences between the root canal treatment and Tooth Extraction groups [20].
3. Results
A total of 484 participants completed the questionnaires on their visit. A total of 243 participants (50.2%) represent the RCT group and 241 (49.8%) for the Tooth Extraction group as in Table 1.
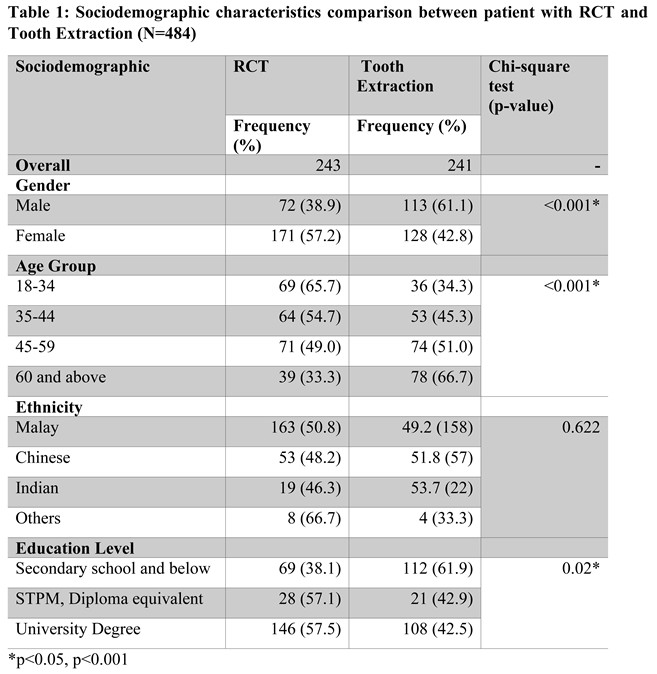
Comparing the two groups by socio-demographic characteristics showed significant differences except for ethnicity (Table 1). Male participants showed a higher proportion in the Tooth Extraction group (61.1%) as compared to female participants (57.2%) in the RCT group. Participants aged 60 years old and above were in a higher proportion in the Tooth Extraction group (66.7%) while participants aged 18 to 34 years old showed a higher proportion of having RCT (65.7%) than other age groups. Patients with secondary school and below education showed a higher proportion in the Tooth Extraction (61.9%) as compared to the RCT group (38.1%).
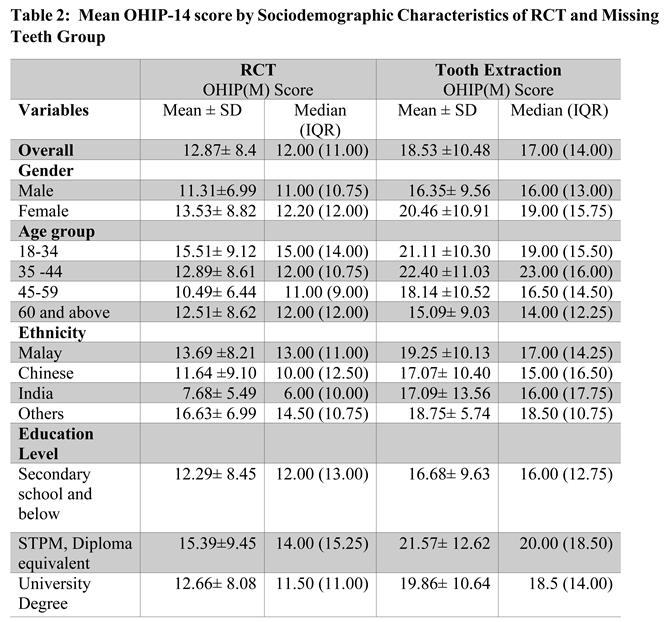
The mean and median values for both RCT and Tooth Extraction were comparable, indicating an acceptable skewness. The overall mean OHIP-14 score for the RCT group is 12.87±8.37 and Tooth Extraction group is 18.53±10.48 (Table 2). Compared by gender, females have higher mean OHIP scores as compared to male across both RCT and Tooth Extraction. However, the difference between male and female respondents are bigger in the Tooth Extraction group (male =16.35± 9.56, female=20.46 ±10.91) compared to the RCT (male =11.31±6.99, female=13.53± 8.82) group. Between age groups, in the RCT group, the mean OHIP score was lower among 45-59 age groups (10.49± 6.44). While for the Tooth Extraction group, the oldest age category has the lowest mean OHIP score (15.09± 9.03). By ethnicity, in the RCT group, Indians with the lowest mean OHIP score (7.68± 5.49) compared to other ethnicities. In the Tooth Extraction group, Chinese reported the lowest mean OHIP score (17.07± 10.40). Compared by education level, secondary and below level have the lowest mean OHIP score for both RCT and Tooth Extraction group (RCT=12.29± 8.45, Tooth Extraction=16.68± 9.63).
Analysis of the mean of OHIP-14 domains showed significant differences in all 7 domains. Across all domains (functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability, handicap), RCT groups have a lower mean OHIP score compared to Tooth Extraction group (Table 3). The highest mean OHIP score across domains were for psychological discomfort with an average of 3.06±1.83 in the RCT group and an average of 3.70±2.09 for Tooth Extraction group. While the lowest mean OHIP scores were for the social disability domain with an average of 0.72±1.18 for RCT group and an average of 1.30±1.78 for Tooth Extraction group.
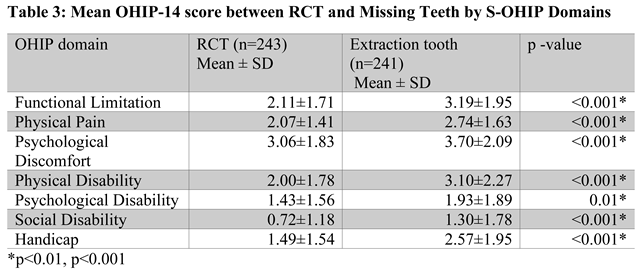
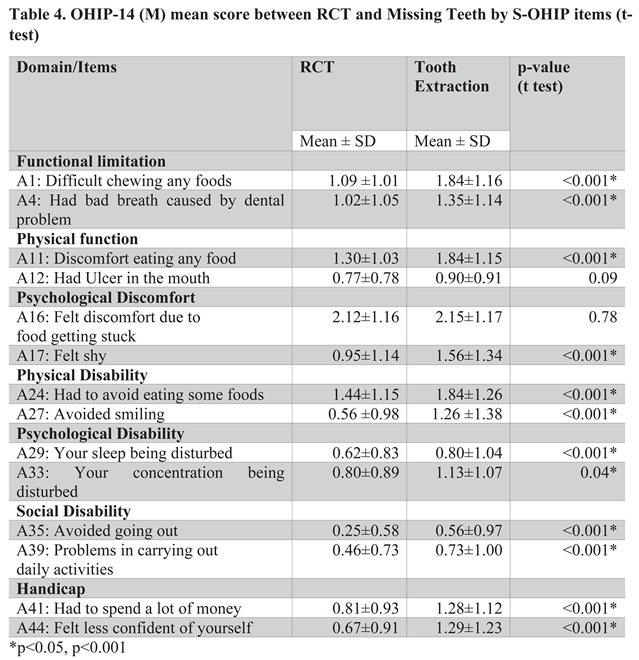
Figure 14. items in Table 4 showed significant differences between RCT and Tooth Extraction. Across all items signify statistically significant differences in the mean of OHIP-14 score, except in item A12: Ulcer in the mouth (p=0.09) and item A16: Felt discomfort due to food getting stuck (p=0.78). Across all items, the lowest mean OHIP-14 score was 0.25±0.58 for the item Avoiding Going Out among RCT participants and 0.56±0.97 among Tooth Extraction participants. While the highest mean OHIP-14 score was for item, Had to Avoid Eating Some Foods with an average of 1.44±1.15 among RCT participants and an average of 1.84±1.26 among Tooth Extraction participants.
4. Discussion
This study highlights the significant sociodemographic differences of patients attending the restorative clinics. In terms of gender, most of RCT patients were female, as this aligned with local studies indicating women that are generally health conscious, actively seeking dental care and showed more concern for aesthetics and tooth preservation [22,23]. Younger adults (18-34 years) were more likely to receive RCT reflecting their literacy to maintain natural dentition during working and socially active years [24]. While in contrast, the older age exhibits significantly higher tooth loss, often presented with tooth carries or periodontal reasons which required tooth extraction which reflects the cumulative effects of old age and access to restorative care [25]. In terms of ethnicity, this study showed no significant association between ethnicities and RCT or Tooth Extraction group. While other local studies indicate differences across ethnicities in Malaysia [26].
Adults choose RCT or tooth extraction procedure based on the perceived value of the tooth. Local study by Razak and colleagues showed that a higher proportion of adults preferred RCT to preserve teeth [27]. While previous studies indicated the lower cost associated with tooth extraction as compared to RCT [28,29]. This reason being one of the deciding factors in choosing either RCT or tooth extraction. While the perception of pain and anxiety influences patients to choose tooth extraction as compared to RCT [30]. However, reviews stress on the usability of value-based payment approaches with the utilisation of OHRQoL as the outcome of interest [31,32]. The superiority of using OHRQoL as it captures the perceptions of adults comparing both treatment options.
This study reports oral health-related impact on quality of life among patients seen in restorative dental clinics using a standardized questionnaire. The study showed significant mean differences of OHRQoL domains of patients with RCT and tooth extraction. Systematic review indicates improvements of OHRQoL of RCT among cross-sectional studies but no significant association in longitudinal studies. Previous study also found significant improvements in OHRQoL significantly associated with the method of root canal treatment [33].
In this study, the mean OHIP-14 score across domains indicates that social disability was least likely to affect the OHRQoL among adults in Malaysia. These findings align with other studies [20,34] indicating that oral health impacts are less immediately perceived by everyday Malaysians as compared to physical or psychological domains. Malaysians may perceive socially accepted with a minor oral function or aesthetic problem. This reflects cultural adaptation towards social norms among the Malaysian community [34]. By contrast, the highest mean OHIP-14 score in the psychological domain reflects that symptoms may interfere with daily function, mastication and emotional well-being of Malaysian adults [35]. This is a similar finding in other countries as oral issues caused significant physical as well as psychological affect [36,37].
The OHRQoL concept evolved as more evidence grew of the impact of oral disease on social roles. Patients reporting pain will negatively impact quality of life including oral function, psychological discomfort and disability [30]. Evidence of effective endodontic treatment or RCT and successful treatment being mainly considered as clinical outcome, and lack of information from patients' perspectives. The study showed no significant differences between the two groups in getting ulcers, food stuck, disturbed sleep and concentration in daily life. Endodontic treatment in the elderly is very challenging as pulp becomes necrotic and other pathological changes [38]. The lack of information from preoperative radiographs can create uncertainty and guesswork during access. Medical conditions such as hearing loss and cognitive impairments may cause communication difficulties and as consequence, they receive limited services, in suboptimal care such as extractions and removable prostheses despite age-related declines in orofacial sensorimotor [39]. The RCT group has similar OHRQoL compared to other individual treatments except preventive controls.
RCT is highly cost-effective as first line intervention [40]. Orthograde and even surgical re-treatment is also cost-effective compared to fixed partial dentures or implant supported crowns. Study on catastrophic spending also showed huge spending in the Tooth Extraction group, where replacement of teeth is costly compared to saving the tooth by RCT [5].
This study strength lies in the diverse adult population OHRQoL perceptions. It can capture young adults, working adults as well as older adults. However, the differences with RCT and Tooth Extraction needed to be interpreted with caution as the differences between groups might be attributed by the demographic and contextual differences in the study design. Future study might be looking at adjusted analysis.
5. Conclusions
In conclusion, this study adds knowledge to the differences of OHRQoL of RCT and Tooth Extraction patients. Significant differences between the two groups in response to OHRQoL domains. The outcome from this study can be used as an input for future reference to dental fraternity services especially the dental restorative specialties. This can further provide input in patients counselling and referral. The knowledge gained to develop strategies and activities in promoting Root Canal treatment nationwide.
Author Contributions
Balkis G – Principal Investigator (PI) of the research project. Email: balkishazmi@yahoo.com Nurul Salwana AB – Overall write-up of the manuscript. Email: salwana.ab@moh.gov.my Roshima MS – PI at research site and acquisition of data. Email: roshima@moh.gov.my Kamarul Hisham K – PI at research site and acquisition of data. Email: drkamarul@ moh.gov.my Intan Azimah A – PI at research site and acquisition of data. Email: intanazimahazman@ gmail.com Ithnaniah AW – PI at research site and acquisition of data. Email: ithnaniah01@yahoo.com Rohani M – PI at research site and acquisition of data. Email: rohanimahmood@gmail.com Aswani CA – PI at research site and acquisition of data. Email: aswaniahmad@gmail.com Nik Fareedah M – PI at research site and acquisition of data. Email: nikfareedah@gmail.com Saripah S – PI at research site and acquisition of data. Email: ssaud67@yahoo.com Nor Ziana I – PI at research site and acquisition of data. Email: ziana71@yahoo.co.uk Zulkarnain AK – Research methodology and data analysis. Email: zulkarnain.ak@moh.gov.my.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Medical Research Ethics Committee of the Ministry of Health Malaysia (protocol code NMRR-17-3485-37374 S2 R2 and date of approval on 2nd October 2019).”.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data supporting reported results can be requested from the corresponding author.
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author’s contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments). Where GenAI has been used for purposes such as generating text, data, or graphics, or for study design, data collection, analysis, or interpretation of data, please add “During the preparation of this manuscript/study, the author(s) used [tool name, version information] for the purposes of [description of use]. The authors have reviewed and edited the output and take full responsibility for the content of this publication.”.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| OHIP | Oral Health Impact Profile |
| OHRQoL | Oral Health Related Quality of Life |
| RCT | Root Canal Treatment |
| S-OHIP | Short-form - Oral Health Impact Profile |
References
- WHO. Action Plan for Oral Health in South-East Asia 2022–2030. 2022. Available online: https://www.who.int/publications/i/item/9789290210061.
- Oral Health Programme. 2022. National Oral Health Strategic Plan 2022-2030 NATIONAL_ORAL_HEALTH_STRATEGIC_PLAN_2022-2030_Edaran (1).
- Najihah, Lokman; et al. Caries-Free Prevalence among Schoolchildren In. Children 2023, 10(264), 1–11. [Google Scholar] [CrossRef] [PubMed]
- Gulabivala; Kishor; Yuan, Ling; Ng. Factors that affect the outcomes of root canal treatment and retreatment- A reframing of the principles. International Endodontic Journal 2023, (56), 82–115. [Google Scholar] [CrossRef] [PubMed]
- Wigsten, Emma; Kvist, Thomas; Husberg, Magnus; Davidson, Thomas. Cost-Effectiveness of Root Canal Treatment Compared with Tooth Extraction in a Swedish Public Dental Service: A Prospective Controlled Cohort Study. Clinical and Experimental Dental Research 2023, 9(4), 661–69. [Google Scholar] [CrossRef] [PubMed]
- Tan, Yeung R’ong; et al. Demographic and Socioeconomic Inequalities in Oral Healthcare Utilisation in Malaysia: Evidence from a National Survey. BMC Oral Health 2021, 21(1), 34. [Google Scholar] [CrossRef]
- Sischo, L.; Broder, H. L. Oral Health-Related Quality of Life: What, Why, How, and Future Implications. Journal of Dental Research 2011, 90(11), 1264–70. [Google Scholar] [CrossRef]
- Slade, G D; Spencer, A J. Development and Evaluation of the Oral Health Impact Profile. Community dental health 1994, 11(1), 3–11. [Google Scholar]
- Husain, Fuad Akbar; Tatengkeng, Fransiske. Oral Health-Related Quality of Life Appraised by OHIP-14 Between Urban and Rural Areas in Kutai Kartanegara Regency, Indonesia: Pilot Pathfinder Survey. The Open Dentistry Journal 2017, 11(1), 557–64. [Google Scholar] [CrossRef]
- Saub, Roslan; Locker, David; Allison, Paul. Derivation and Validation of the Short Version of the Malaysian Oral Health Impact Profile. Community Dentistry and Oral Epidemiology 2005, 33(5), 378–83. [Google Scholar] [CrossRef]
- Saub, Roslan; Locker, D. The Impact of Oral Conditions on the Quality of Life of the Malaysian Adult Population: Preliminary Results. Medical Journal of Malaysia 2006, 61(4), 438–46. [Google Scholar]
- Vollset, Stein Emil; et al. Burden of Disease Scenarios for 204 Countries and Territories, 2022–2050: A Forecasting Analysis for the Global Burden of Disease Study 2021. The Lancet 2024, 403(10440), 2204–56. [Google Scholar] [CrossRef]
- Yusof, Zamros Y.M.; Jaafar, Nasruddin. A Malay Version of the Child Oral Impacts on Daily Performances (Child-OIDP) Index: Assessing Validity and Reliability. Health and Quality of Life Outcomes 2012, 10, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ching, Lim Ching; Mohamad, Wan Majdiah Wan; Saddki, Norkhafizah; Ghazali, Wan Syamimee Wan. Perceived Oral Health Status and Its Association with Oral Health-Related Quality of Life of Patients with Rheumatoid Arthritis - A Pilot Study. Sains Malaysiana 2019, 48(12), 2709–15. [Google Scholar] [CrossRef]
- Husain, Juzaily binti; Mohd, Farah Natasha; Said, Abdul Hadi; Yaacob, Munirah. Oral Health Related Quality of Life Among Adult Patients Attending Periodontal Clinic in Kuliyyah of Dentistry IIUM Kuantan. IIUM Medical Journal Malaysia 2020, 18(2), 2019. [Google Scholar] [CrossRef]
- Jaafar, M. A.; et al. Oral Health Impact among Periodontal Patients at Supportive Periodontal Care: A Cross-Sectional Study. Journal of the University of Malaya Medical Centre (JUMMEC) 2025, 28(1), Article 14. [Google Scholar]
- Abanto, Jenny; et al. Impact of Pulpectomy versus Tooth Extraction in Children’s Oral Health-Related Quality of Life: A Randomized Clinical Trial. Community Dentistry and Oral Epidemiology 2024, 52(1), 13–23. [Google Scholar] [CrossRef]
- Wigsten, Emma; et al. Comparing Quality of Life of Patients Undergoing Root Canal Treatment or Tooth Extraction. Journal of Endodontics 2020, 46(1), 19–28.e1. [Google Scholar] [CrossRef]
- Mohd Shaharuddin; Izzati; et al. Prevalence of Dental Caries and Their Relation to Oral Health Impact Profile (OHIP-14) among National Contact Sports Athletes: A Cross-Sectional Study. Journal of International Oral Health 2021, 13(6), 593–600. [Google Scholar] [CrossRef]
- Azis, Nik; Madihah, Nik; Abdullah, Raja Noreihan Raja; Ayub, Mohamad Nur Adzmi Mohamad; Baharin, Badiah. Oral Health Status, Behavior and Impact Profile among Naval Personnel in the Malaysian Naval Armed Forces. BMC Oral Health 2025, 25(1). [Google Scholar] [CrossRef]
- Dhand, N. K.; Khatkar, M. S. Statulator: An Online Statistical Calculator. Sample Size Calculator for Comparing Two Paired Proportions. 2014. Available online: http://statulator.com/SampleSize/ss2PP.html.
- Lipsky, Martin S.; Su, Sharon; Crespo, Carlos J.; Hung, Man. Men and Oral Health: A Review of Sex and Gender Differences. American Journal of Men’s Health 2021, 15(3). [Google Scholar] [CrossRef]
- Sfeatcu, Ruxandra; et al. Gender Differences in Oral Health: Self-Reported Attitudes, Values, Behaviours and Literacy among Romanian Adults. Journal of Personalized Medicine 2022, 12(10). [Google Scholar] [CrossRef]
- Klarić Puđa, Iva; et al. A Cohort Study on the Impact of Oral Health on the Quality of Life of Adolescents and Young Adults. Clinics and Practice 2025, 15(4), 1–16. [Google Scholar] [CrossRef] [PubMed]
- Kayash, J; et al. Oral Health and Oral Health-related Quality of Life Among Geriatric Population- A Narrative Review Jagreeti. Journal of Pharmacy and Bioallied Science 2024, 7(10), S3105–7. [Google Scholar] [CrossRef] [PubMed]
- Lim, Fei Yee; Goo, Chui Ling; Leung, Wai Keung; Goh, Victor. Validation of the Malay Oral Impacts on Daily Performances and Evaluation of Oral Health-Related Quality of Life in a Multi-Ethnic Urban Malaysian Population: A Cross-Sectional Study. International Journal of Environmental Research and Public Health 2022, 19(24). [Google Scholar] [CrossRef] [PubMed]
- Razak, I A; Jaafar, N; Jalalludin, R L; Esa, R. Patients’ Preference for Exodontia versus Preservation in Malaysia. Community dentistry and oral epidemiology 1990, 18(3), 131–32. [Google Scholar] [CrossRef]
- Kharel; Smriti; et al. Reasons for Patients Preferring Extraction over Root Canal Treatment in a Tertiary Care Hospital. Nepal Journal of Health Sciences 2024, 4(1), 9–14. [Google Scholar] [CrossRef]
- Sadasiva, Kadandale; et al. Analyzing the Reasons for Patients Opting-out from Root Canal Treatment and Preferring Extraction in South Indian Population—Prospective Study. International Journal of Prosthodontics and Restorative Dentistry 2018, 8(4), 108–13. [Google Scholar] [CrossRef]
- Alroomy, Riyadh; et al. Factors Influencing Pain and Anxiety Before Endodontic Treatment: A Cross-Sectional Study Amongst American Individuals. European endodontic journal 2020, 5(3), 199–204. [Google Scholar] [CrossRef]
- Elangovan, Satheesh; Allareddy, Veerasathpurush. Value-Based Payment Approaches. The Journal of the American Dental Association 2019, 150(6), 485. Available online: https://www.sciencedirect.com/science/article/pii/S0002817719302661. [CrossRef]
- Tatari, Pourya; Rezayatmand, Reza; Nilchian, Firoozeh. Costs in Dental Care: A Scoping Review of Methodologies and Trends. BMC oral health 2025, 25(1), 1571. [Google Scholar] [CrossRef]
- Neelakantan, Prasanna; Liu, Pei; Dummer, Paul M.H.; McGrath, Colman. Oral Health–Related Quality of Life (OHRQoL) before and after Endodontic Treatment: A Systematic Review. Clinical Oral Investigations 2020, 24(1), 25–36. [Google Scholar] [CrossRef]
- Saub, R; Locker, D; Allison, P; Disman, M. Cross-Cultural Adaptation of the Oral Health Impact Profile (OHIP) for the Malaysian Adult Population. Community dental health 2007, 24(3), 166–75. [Google Scholar]
- Abdullah, N.S.; Radzali, N.F.M.; Saub, R.; Vaithilingam, R.D. Oral Health Related Quality of Life and Periodontal Status of a Selected Malaysian Adult Population: A Pilot Study. Annals of Dentistry 2013, 20(2), 16–23. [Google Scholar] [CrossRef]
- James, Anju; et al. Impact of Oral Conditions on Oral Health-Related Quality of Life among Indians- a Systematic Review and Meta-Analysis. Health and Quality of Life Outcomes 2023, 21(1), 1–18. [Google Scholar] [CrossRef]
- Roberto, Paulo; et al. O r a l H e a l t h -R e l a t e d Q u a l i t y of Life and Associated Factors i n B r a z i l i a n A d o l e s c e n t S. Brazilian Dental Journal 2017, 28(1), 113–20. [Google Scholar] [CrossRef]
- Alrahabi, Mothanna K. Root Canal Treatment in Elderly Patients: A Review and Clinical Considerations. Saudi Medical Journal 2019, 40(3), 217–23. [Google Scholar] [CrossRef]
- Huang, Dingming; et al. Expert Consensus on Difficulty Assessment of Endodontic Therapy. International Journal of Oral Science 2024, 16(1). [Google Scholar] [CrossRef]
- Zang, Hai Ling; et al. Cost-Effectiveness Analysis: Nonsurgical Root Canal Treatment versus Single-Tooth Implant. BMC Oral Health 2023, 23(1), 1–8. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



