
Submitted:
26 December 2025
Posted:
29 December 2025
You are already at the latest version
Abstract
Background. Emotional implications of childhood dental encounters are very important on the long run. The aim of the study was to assess parents’ childhood dental memories and potential impact upon current attitudes towards dental treatment, and the perceived usefulness of an educational material on efficient psychological management of child’s dental visit. Method: An educational booklet was produced. Parents were encouraged to read it and subsequently fill a brief questionnaire. Answers were analyzed using IBM SPSS Statistics 25. Results: During the first month, 142 parents (88% moms) filled the questionnaire; 44.4% reported negative childhood dental experiences (mothers ss more, p< 0.001); 18.3% had shared these experiences with their children. Dental encoun-ters-related emotional discomfort of various degrees was reported by 61.3% (38.7% a little, 5.6% some, 13.4 % pretty much, 3.5% a lot). The self-reported level of dental anxiety was ss correlated to childhood negative experiences (p< 0.001). Parents’ level of education influenced criteria for choosing a dentist for their children: parents with higher education were ss more likely to choose a certified pedodontist rather than a closer-to-home dentist (p=0.002). Most respondents (97.9%) felt the provided educational material will, to var-iable extent, help them manage their children’s dental visits better in the future (28.2% very much; 44.4% a lot) and 91.6% would share it with other parents /families. Conclu-sions. Childhood dental fear does not necessarily fade away with time. Parents need and appreciate initiatives that enable them manage their children’s dental encounters in a positive supportive way, thus avoiding early onset of dental fear/anxiety.
Keywords:
dental fear and anxiety
; children
; parental education
1. Introduction
Dental fear and anxiety (DFA) are very frequent findings in children and adolescents worldwide, with higher prevalence in preschool children and schoolchildren [1]. DFA however often remains underestimated in terms of occurrence, causes and – more important - long-term consequences. When DFA occurs in early years, it does not necessarily fade away with time, and negative perceptions regarding dental care risk to negatively impact oral health throughout life, as individuals with DFA shall tend to postpone or even avoid dental visits [2,3]. In consequence, children with DFA have higher caries experience, more untreated caries lesions and poorer oral health-related quality of life than children without dental anxiety [4,5,6].
There are two main categories of people that can, through their ways of managing the child’s dental visit from their own respective perspectives, influence children’s perception and attitude regarding oral care: Family and the Dental Team. Educating families and dental professionals in this respect thus appears crucial for growing new generations with healthy teeth and positive attitudes towards oral health.
Dental professionals may get, through under- and/or post-graduate programs, some training in behavior guidance (BG) techniques. BG teaching varies widely across various countries and is also subject to cultural influences and particularities. In the attempt to encourage evidence-based practice in all fields of medicine and dentistry, during the last decades, the subject has gained increased attention from researchers and international pediatric dentistry (PD) forums. The International Association of Paediatric Dentistry (IAPD), American Academy of Pediatric Dentistry (AAPD) and European Academy of Paediatric Dentistry (EAPD) provide, on their respective websites, scientifically based information for dental practitioners on this topic [7,8,9], and this tendency is being undertaken by national professional organizations as well.
While BG tools are being made available for dental practitioners, families do not necessarily have this kind of information at hand. With parents being, naturally, their children’s very first models in life since very young ages, their approaches towards all aspects of being shall consistently impact their children’s attitudes.
Parenting styles have evolved a lot with time, constantly adjusting to changes in society. Public accessibility to information – be that scientifically sustained or not – has hugely increased and it is our professional responsibility, as dental professionals, to help families pick up and use the correct information in an appropriate manner, to the highest long-term benefit of children’s health. This traditionally applies to the prevention of oral disease, but, for all the previously mentioned reasons, when it comes to prevention in dentistry, DFA should also be taken into account.
Parental engagement in friendly, stress-free relationship between child and dental team is very important on the long term. However, mere encouragement of parental engagement may not be enough. Shaping parents’ involvement by teaching them how to efficiently manage the child’s dental visit can be useful in many cases, and initiatives in this respect need to be developed.
Pre-appointment parental counselling is already demonstrated to be very effective. When parents are informed about the procedures their child will undergo and about the ways they should talk to their children about these procedures, using explanations, demonstration videos, drawings etc., pediatric dental patients have lower levels of dental anxiety and fear, giving rise to more cooperative behavior during dental treatment [10,11].
Erasmus+ PaFein+ project aims to help grow generations of children with healthy teeth and positive attitudes towards oral care by fostering positive dental encounters, minimizing the early onset of DFA and reducing the need for dental sedation and general anesthesia, with a positive impact upon the environment as a natural consequence. Given the already mentioned considerations, providing parents and families with the appropriate information as to enable them to prepare and handle the dental visit of their children in a positively supportive way and reduce stress associated with pediatric dental visits for all involved – child, family, dental team – was identified as an important step towards more efficient prevention in dentistry on the long run. A dedicated Parents’ section of PaFein+ project was thus created. The present study is part of the research carried out within this section.
The aim of this study was to assess parents’ childhood dental experience and potential implications upon their current perception towards dental treatment and attitudes towards children’s dental treatment, as well as to test the usefulness of information provided by a targeted educational initiative within the project.
2. Materials and Methods
The Parents’ section of PaFein+ started as a pilot in 2025 in Romania. In the initial stage of the initiative, a booklet (Figure 1) with advice on how to efficiently prepare and handle the child’s dental encounter was conceived by an interdisciplinary team of pediatric dentists and trained psychologists. The material provides information on how to handle and support the child before, during and after the dental visit in a manner that would naturally include such events in current, everyday living, thus minimizing potential stress for all involved – child, family, dental team.
Easy-to-understand language was used and examples with appropriate/unrecommended words to use were given in order to make communication more effective (Figure 2).
The material was shared through social media (digital version) and directly (brochures), in the Pedodontics Clinic of Carol Davila University, Bucharest (Romania). Parents were subsequently encouraged to complete a feedback questionnaire. The questionnaire had 4 sections. Section 1 contained demographic data; section 2 comprised 3 questions on personal childhood experience and present dental attitude; section 3 had 7 questions on attitudes towards children’s dental treatment; section 4 had 2 questions on the usefulness of the educational material provided. Average time for questionnaire completion was estimated to 4-5 minutes.
Parents’ answers were collected. Data was analyzed using IBM SPSS Statistics 25 and illustrated using Microsoft Office Excel/Word 2024. Quantitative variables were tested for normal distribution using the Shapiro-Wilk Test and were written as averages with standard deviations or medians with interquartile ranges. Quantitative variables with non-parametric distribution were tested between groups using the Mann-Whitney U Test/Kruskal-Wallis H Test. Qualitative variables were written as counts or percentages and were tested between groups using Fisher’s Exact Test. Z-tests with Bonferroni correction were used to further detail the results obtained in the contingency tables. The threshold considered for the significance level for all tests was considered to be α = 0.05.
Depending on the results of this pilot study, the PaFein+ educational initiative targeting parents is to be extended in terms of both contents and geography, not only to the other countries participating in the project, but also to any interested regions.
3. Results
During the first month after the start of the pilot initiative, the material reached an estimate of roughly 7700 Romanian families, out of which 142 parents filled the feedback form. The characteristics of the analyzed participants are shown in Table 1.
3.1. Demographic Data
Most of the participating parents (88%) were mothers. The age range of the respondents was 18 to over 55 years, with 52.1% of them in the 36-45 years age group. The age of their children at the time of their first dental visit ranged between 5 and 11 years, with a mean age of 8.4 years [SD 5.17]. Main reported reason for dental visit was check-up (54.5%), followed by noticed cavity (24.2%).
3.2. Own Childhood Dental Experience
Negative childhood dental experiences were remembered and reported by 44.4% of the parents. Z-tests with Bonferroni correction pointed out that mothers were ss more likely to remember negative childhood experiences (p<0.001), and 18.3% had already shared these experiences with their children. A proportion of 38.7% of the respondents stated they felt no unease related to dental encounters, while the other 61.3% admitted they feel emotional discomfort of various degrees (38.7% a little, 5.6% some, 13.4% pretty much, 3.5% a lot). The self-reported level of anxiety was ss correlated to negative childhood dental experiences (Fisher’s exact test, p < 0.001) (Figure 3).
3.3. Attitudes Towards Children’s Dental Treatment
Most of the parents (73.2%) preferred their children to be treated by a trained pediatric dentist. Differences of opinion in choosing a dentist for their child were significantly influenced by parents’ level of education: parents with no academic studies were ss more likely to make their choice taking into account the geographic criteria rather than the dental professional’s specialization, preferring a dentist situated closer to their home (20.8% vs. 0.8%, p=0.002) (Figure 4).
A great majority of the responding parents (85.2%) stated they prepared their kids for dental visits. Most respondents (66.9%) considered that it is normal for a child to feel some pain during dental treatment, fathers being significantly more inclined to agree to that than mothers (p = 0.001), while 14.1% felt that general anesthesia should be the golden standard for stress and pain-free pediatric dental treatments. This latter finding is however not correlated with parents’ dental anxiety (Table 2). Similarly, parents’ tendency to tell their kids stories about their own negative childhood dental experiences is not correlated with their self-reported degree of dental anxiety (Table 2).
3.4. Perceived Usefulness of Provided Info
The great majority of the respondents (97.9%) felt the provided educational material will, to variable extents, help them better manage their children’s dental visits in the future (44.4% a lot; 28.2% very much); 91.6% stated they would share it with other parents/families (54.2% very high level of agreement, 37.3% high level of agreement) (Table 3).
4. Discussion
The calculated mean age of the respondents’ children at the time of their first dental visit is rather high from the prevention point of view. This finding is in line with previous reports [12]. Similar ages at first visit were previously reported [13] despite the recommendations of international professional organisations for children to have their first dental visit by the age of 12 months, in order to establish a “Dental Home” (DH) at the earliest possible time [14,15]. The advantages of the DH system are well known and proven in time, both for healthy children and for children with special healthcare needs [15,16]. The absence of dental fear can be cited among the most important positive characteristics of this care model.
A tendency to agree for some degree of pain in association with their children’s dental treatment was obvious in two thirds of the subjects (66.9%). This rather surprising perception could be due to a cultural background that “traditionally” links dental treatment to suffering, as well as to parents’ own childhood experiences, given that many parents were children in a time when Romania was still under a communist regime, with much lesser access to advanced means of pain avoidance during dental treatment. The fact that fathers were significantly more prone to this perception than mothers may be regarded as an expression of fathers’ greater tendency to show some harshness in handling and educating children. In contrast with our findings, a recent systematic review on parents’ perception regarding dental interventions performed on their children pointed practitioner’s abilities in alleviating pain and fear as important elements for treatment acceptance [17].
Studies show that children psychologically prepared for their dental encounters beforehand are less anxious [10,18,19]. Psychological preparation can address children either directly, in the waiting room [18,19], or indirectly, using parents as vectors [10,20]. A controlled trial conducted by Fox & Newton (2006) demonstrated that positive images of dentistry showed to the children prior to their appointment promotes a positive relationship with the dentist by short-term reductions in anticipatory anxiety in children. In their study, anticipatory anxiety was not correlated to age and gender [18].
Another option is to train parents (by booklets, videos, smartphone application etc.) on how to efficiently prepare the child before the dental visit [10,20]. A study performed by Bagattoni et al. (2022) analyzed the efficacy of this method. Before the child’s first dental appointment, parents received by e-mail a booklet with suggestions on how to prepare the child for this visit. The importance of the first dental visit in developing a positive attitude towards dental team was also explained. During the first visit, visual examination of the oral cavity was performed using a dental mirror and a dental probe, without any operative or invasive procedures. The results of this study demonstrated that children whose parents used the advice from the booklet reported less pain and assessed this visit as more enjoyable than children whose parents did not receive the booklet [10]. It is important that this psychological preparation occurs in a safe environment and is made by an affectively relevant person for the child [10].
Mittal et al (2025) conducted a randomized controlled trial aiming to evaluate the impact of a specially designed dentistry modelling story on dental anxiety and managing behavior among 6-8-year-old children. They compared a group of children who received a booklet describing the various aspects of the dental visit, dental team, instruments etc. aiming to familiarize children with the dental visit with another group of children who received a folk story. Children in both the groups showed a significant reduction in anxiety after storytelling, and differences in the anxiety and behavior of the children between the two groups were not statistically significant. Dentistry modelling story was preferred by the parents. [21].
All these interventions (comic strips, booklets etc.), designed to give details about the dental treatment and preparing the child for dental visit, are relatively inexpensive, easy to administer, and generate a positive behaviour [10,22,23,24].
In order to be more effective, advice for parents how to prepare the child for dental visits should mainly address parents of young children, without prior dental experience. It was demonstrated that children who had negative experience in the first dental visit have a higher risk of developing DFA than children who had a potentially painful experience after a few positive dental visits [10].
In our study, a great majority (more than 85%) of the parents taking part in this section of PaFein+ project stated that they prepared their kids for dental visits beforehand. Almost all respondents (97.9%) considered that the provided material would help them manage their kids’ dental encounters better in the future and many (over 90%) would share the info with peers.
These findings were considered encouraging by the project team, therefore educational materials for families are subsequently being diversified and developed in accordance to feedback. As previous studies emphasized that parents tend to find storytelling videos relatable and reflective of real-life experiences [17], an original video on appropriate versus improper ways to support children before, during and after their dental encounters was produced. The material depicts a real-life inspired 5-year old’s first visit to the dentist, from entering the waiting room to treatment completion. It is structured is 5 distinct chapters, each of which contains “do’s” and “don’t’s”. The video is freely available (in two languages, English and Romanian) on youtube: https://www.youtube.com/watch?v=SBTjpmGo5k0 (EN), https://www.youtube.com/watch?v=QgCeQBw470M (RO)
More activities are planned and involvement of new potential partners (e.g. national PD societies, universities, parents’ groups and associations, technology providers) is sought and encouraged in order to further develop project contents and increase project impact.
This study has some limitations. Research has a cross-sectional design and cannot assess the long-term impact on the children behavior and cooperation in the dental setting. Further longitudinal studies are necessary to analyze the long-term efficacy of the educational materials for parents.
Feedback was exclusively collected from parents, while the actual ultimate beneficiaries of such initiatives are the children. Objective measurements are also needed to evaluate the effects of parental involvement on their children behavior.
Difficulties in collecting answers to feedback forms were encountered, especially when parents accessed the info through media channels. Larger number of respondents would give more accurate feedback.
5. Conclusions
Childhood dental fear does not necessarily fade away with time. Parents need and appreciate initiatives that enable them manage their children’s dental encounters in a positive supportive way, thus avoiding early onset of dental fear/anxiety, with long-term beneficial effects upon oral health.
Targeted booklets and videos with psychologic advice for parents are useful and can be easily shared online or in public and private dental clinics.
Author Contributions
Conceptualization, AV, AM, OOK, SP; Data Curation, IAC; Formal analysis, IAC; Funding acquisition, OOK; Investigation, AV, AM, MT; Methodology, AM, AV, AP, AGB; Project administration, BK; Resources, AM, RS, MT; Supervision, AG, BK; Validation, RS, MT, AG,AGB, OOK, SP; Visualization, AV; Writing-original draft: AV and AM; Writing-review & editing, AM, AV, AP . All authors have read and agreed to the published version of the manuscript.
Funding
This research was partially supported by Erasmus+ 2023-1-TR01-KA220-HED-000155608 PaFein+ Project.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Carol Deavila University Bucharest, Romania (approval no.11580/30.04.2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study and the information booklet are available on request from the corresponding authors.
Acknowledgments
The authors are grateful to parents participating in this study for agreeing to give their feedback and help PaFein+ Project progression.
Conflicts of Interest
The authors declare no conflicts of interest. The funder had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| PD | Pediatric Dentistry |
| BG | Behavior Guidance |
References
- Grisolia, B.M.; Dos Santos, A.P.P.; Dhyppolito, I.M.; Buchanan, H.; Hill, K.; Oliveira, B.H. Prevalence of dental anxiety in children and adolescents globally: a systematic review with meta-analyses. Int J Paediatr Dent 2021, 31, 168–183. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, M.A.; Vale, M.P.; Bendo, C.B.; Paiva, S.M.; Serra-Negra, J.M. Influence of negative dental experiences in childhood on the development of dental fear in adulthood: a case-control study. J Oral Rehabil 2017, 44, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Dahlander, A.; Soares, F.; Grindefijord, M.; Dahllöf, G. Factors associated with dental fear and anxiety in children aged 7 to 9 years. Dent. J 2019, 7, 68. [Google Scholar] [CrossRef] [PubMed]
- Raadal, M.; Strand, G.V.; Amarante, E.C.; Kvale, G. Relationship between caries prevalence at 5 years of age and dental anxiety at 10. Eur J Paediatr Dent 2002, 3, 22–26. [Google Scholar]
- Porritt, J.; Buchanan, H.; Hall, M.; Gilchrist, F.; Marshman, Z. Assessing children’s dental anxiety: a systematic review of current measures. Community Dent Oral Epidemiol 2013, 41, 130–142. [Google Scholar] [CrossRef]
- Marshman, Z.; Rodd, H.; Fairhurst, C.; Porritt, J.; Dawett, B.; Day, P.; Innes, N.; Vernazza, C; Newton, T; Ronaldson, S; Cross, L; Ross, J; Baker, SR; Hewitt, C; Torgerson, D; Ainsworth, H. The CALM trial protocol: a randomised controlled trial of a guided self-help cognitive behavioural therapy intervention to reduce dental anxiety in children. Trials 2023, 24, 15. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- IAPD Foundational Articles and Consensus Recommendations: Behaviour Guidance in Paediatric Dental Patients, 2022. Available online: http://www.iapdworld.org/2022_06_behaviour-guidance-in-paediatric-dental-patients (accessed on 18 December 2025).
- American Academy of Pediatric Dentistry. Behavior guidance for the pediatric dental patient. In The Reference Manual of Pediatric Dentistry; American Academy of Pediatric Dentistry: Chicago, IL, 2025; pp. 379–399. [Google Scholar]
- Roberts, J.F.; Curzon, M.E.J.; Koch, G.; Martens, L.C. Review: Behavior Management Techniques in Pediatric Dentistry. Eur Arch Paediatr Dent 2010, 11, 166–174. [Google Scholar] [CrossRef]
- Bagattoni, S.; Nascimben, F.; Biondi, E.; Fitzgibbon, R.; Lardani, L.; Gatto, M.R.; Piana, G.; Mattarozzi, K. Preparing Children for Their First Dental Visit: A Guide for Parents. Healthcare 2022, 10, 2321. [Google Scholar] [CrossRef]
- Ramesh, R.; Sathyaprasad, S.; Nandan, S.; Havaldar, K.S.; Antony, A. Assessment of Preappointment Parental Counseling on Dental Fear and Anxiety in Children in Pedodontic Dental Operatory: A Randomized Controlled Trial. Int J Clin Pediatr Dent 2024, 17, 346–351. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Besiroglu-Turgut, E.; Kayaalti-Yuksek, S.; Bulut, M. Evaluation of the relationship between dental anxiety and oral health status of mothers and their children. BMC Oral Health 2024, 24, 749. [Google Scholar] [CrossRef]
- Padung, N.; Singh, S.; Awasthi, N. First Dental Visit: Age Reasons Oral Health Status and Dental Treatment Needs among Children Aged 1 Month to 14 Years. Int J Clin Pediatr Dent 2022, 15, 394–397. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- American Academy of Pediatric Dentistry: guideline on infant oral health care. Pediatr Dent 2014, 36, 1141–1145.
- Nowak, A.J.; Casamassimo, P.S. The dental home: a primary care oral health concept. J Am Dent Assoc 2002, 133, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://oscarpd.ro/ (accessed on 18 December 2025).
- Dalsochio, L.; Montagner, A.F.; Tedesco, T.K.; Maske, T.T.; van de Sande, F.H. Experiences and Parents' Perceptions Regarding Dental Interventions Performed on Their Children: A Qualitative Systematic Review. Int J Paediatr Dent 2025, 35, 1029–1045. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fox, C.; Newton, J.T. A controlled trial of the impact of exposure to positive images of dentistry on anticipatory dental fear in children. Community Dent Oral Epidemiol 2006, 34, 455–459. [Google Scholar] [CrossRef] [PubMed]
- Freeman, R. Viewing positive images of dentistry reduces anticipatory anxiety in children. Evid Based Dent 2007, 8, 47. [Google Scholar] [CrossRef] [PubMed]
- Porritt, J.; Rodd, H.; Morgan, A.; Williams, C.; Gupta, E.; Kirby, J.; Creswell, C.; Newton, T.; Stevens, K.; Baker, S.; et al. Development and Testing of a Cognitive Behavioral Therapy Resource for Children’s Dental Anxiety. JDR Clin Transl Res 2016, 2, 23–37. [Google Scholar] [CrossRef]
- Mittal, M.; Chopra, R.; Malhotra, D.; Dharmasya, T.; Gupta, N.; Lokade, A.; Atri, M. Impact of dentistry modeling story on dental anxiety in 6–8-year-old children of industrial workers: A randomized controlled trial. J Indian Soc Pedod Prev Dent 2025, 43, 95–103. [Google Scholar] [CrossRef]
- Deshpande, A.; Jain, A.; Shah, Y.; Jaiswal, V.; Wadhwa, M. Effectiveness of self-designed dental storybook as behaviour modification technique in 5-7 year- old children: A randomized controlled study. J Indian Soc Pedod Prev Dent 2002, 40, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Murshid, E.Z. Effectiveness of a preparatory aid in facilitating oral assessment in a group of Saudi children with autism spectrum disorders in Central Saudi Arabia. Saudi Med J 2017, 38, 533–40. [Google Scholar] [CrossRef]
- Meshki, R.; Basir, L.; Alidadi, F.; Behbudi, A.; Rakhshan, V. Effects of pretreatment exposure to dental practice using a smartphone dental simulation game on children’s dental anxiety: A preliminary duble-blind randomized clinical trial. J Dental 2018, 15, 251–258. [Google Scholar]
Figure 1.
Brochure with advice for parents.

Figure 2.
– Sample advice from the brochure.
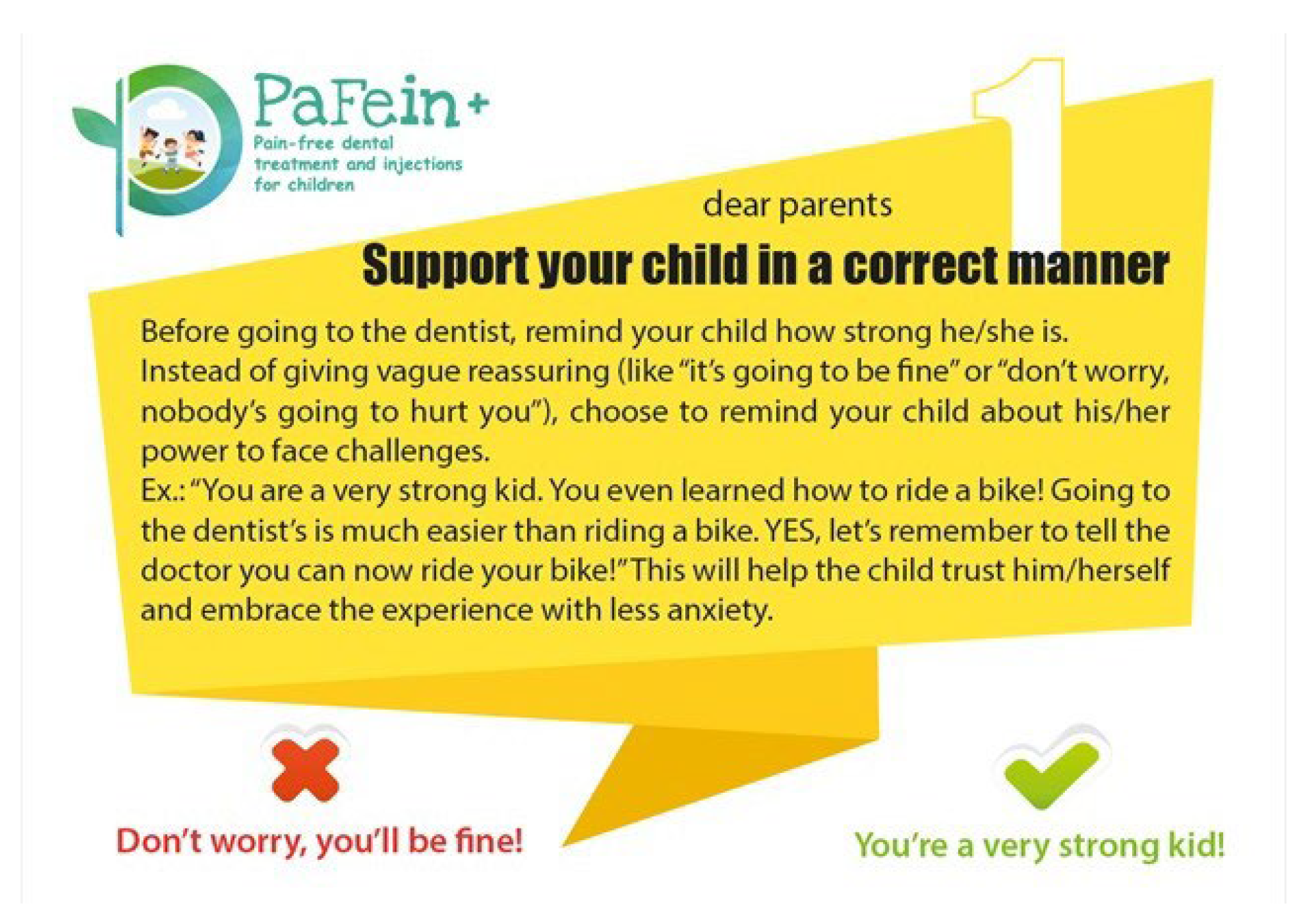
Figure 3.
Distribution of the participants according to the existence of negative childhood experiences in parents and dentist anxiety.
Figure 3.
Distribution of the participants according to the existence of negative childhood experiences in parents and dentist anxiety.
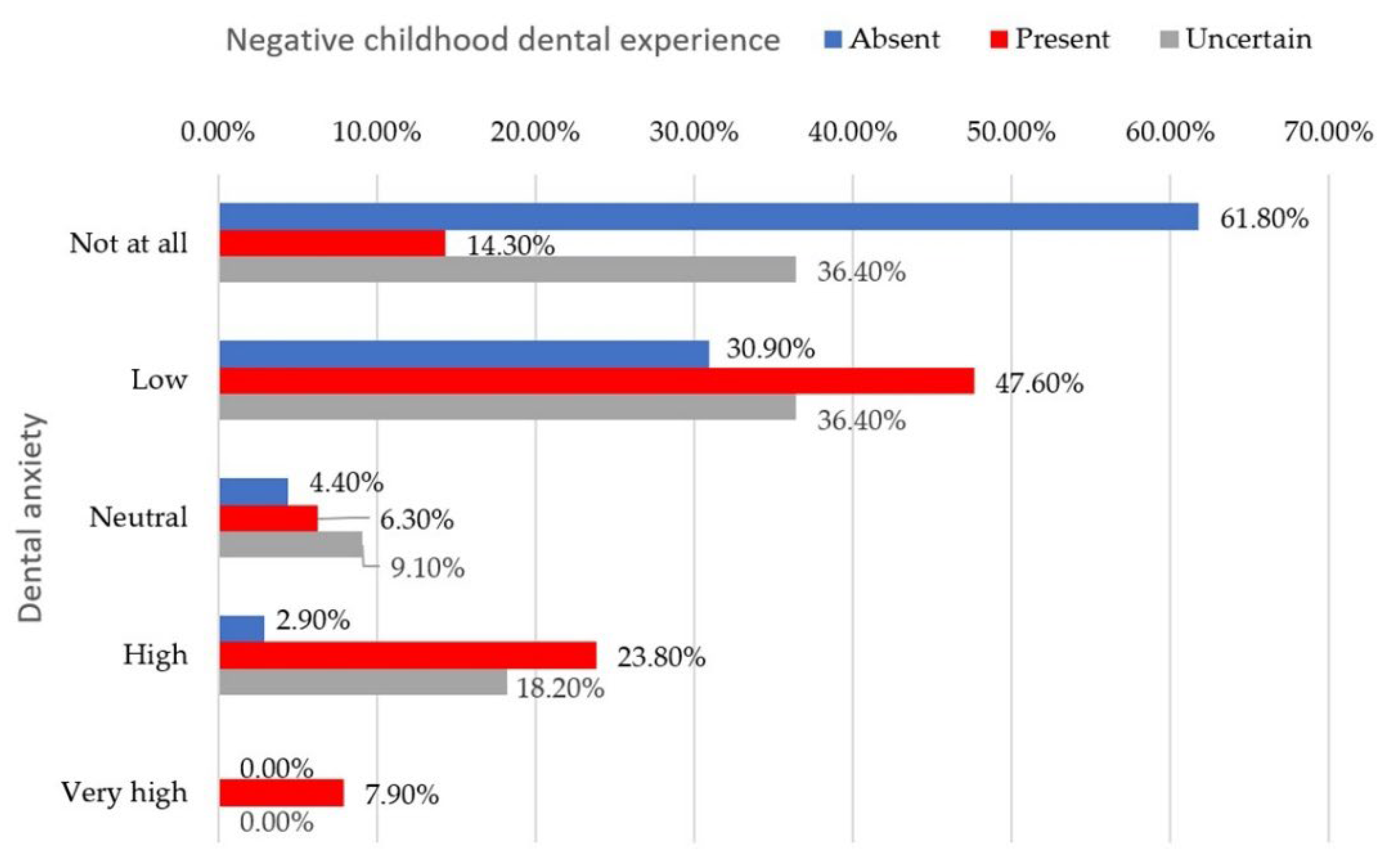
Figure 4.
Distribution of the participants according to parents’ level of education and opinions in choosing child’s dentist.
Figure 4.
Distribution of the participants according to parents’ level of education and opinions in choosing child’s dentist.
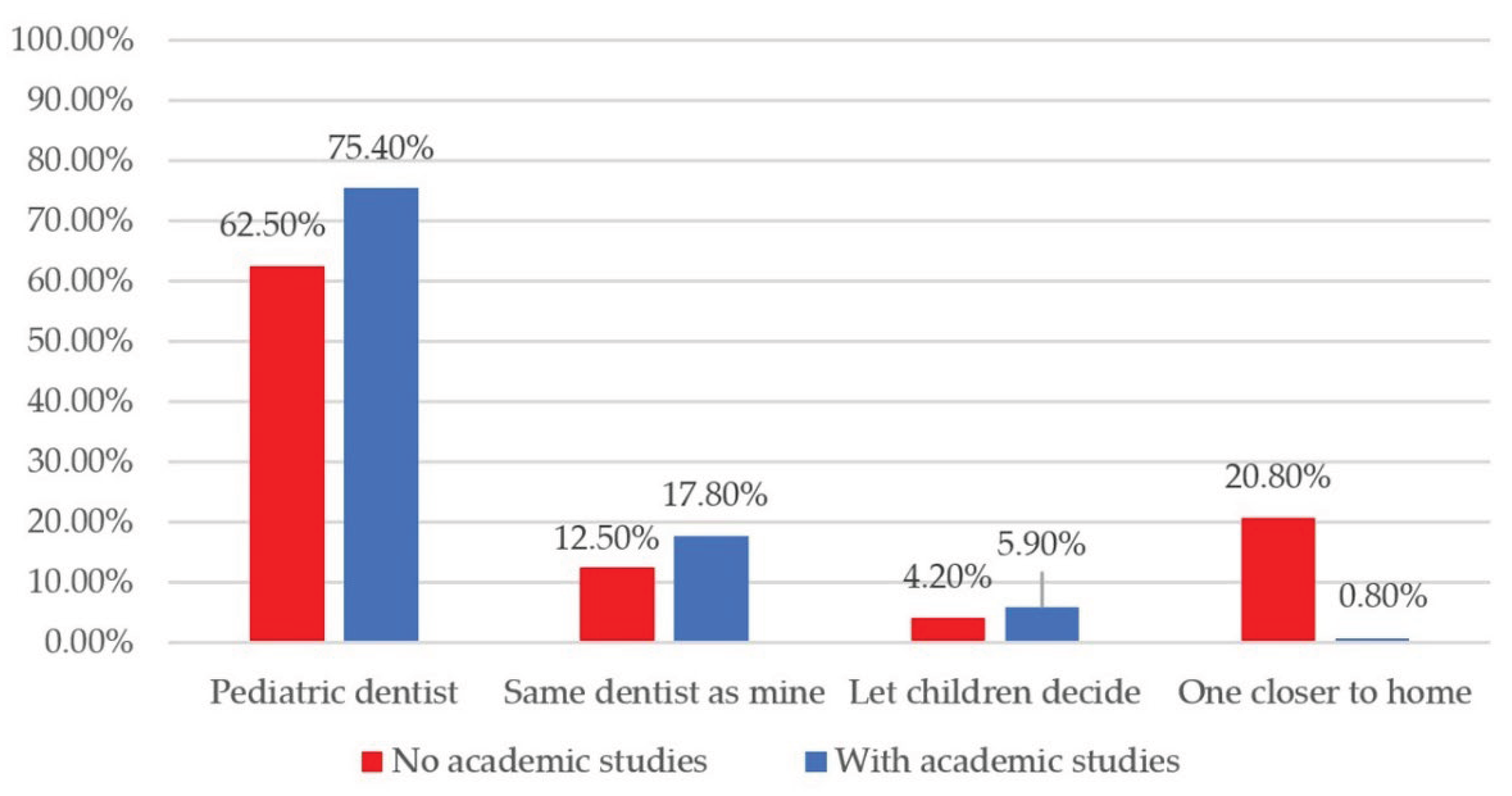

Table 1.
Characteristics of the analyzed participants
| Parameter | Value |
|---|---|
| Parent – Gender (Female) (Nr., %) | 125 (88%) |
| Parent – Age (Nr., %) | |
| 18-25 years | 3 (2.1%) |
| 26-35 years | 20 (14.1%) |
| 36-45 years | 74 (52.1%) |
| 46-55 years | 42 (29.6%) |
| > 55 years | 3 (2.1%) |
| Number of children (Nr., %) | |
| One | 62 (43.7%) |
| Two | 74 (52.1%) |
| Three | 6 (4.2%) |
| Child – Age (Mean ± SD, Median (IQR)) | 8.4 ± 5.17, 8 (5-11) |
| Parent education (Nr., %) | |
| Lower secondary | 2 (1.4%) |
| Secondary | 12 (8.5%) |
| Post-secondary | 10 (7%) |
| Tertiary | 118 (83.1%) |
| Negative childhood experiences (Nr., %) | |
| Absent | 68 (47.9%) |
| Present | 63 (44.4%) |
| Don’t remember | 11 (7.7%) |
| Narration to children (Nr., %) | |
| Absent | 41 (65.1%) |
| Present | 18 (28.6%) |
| Don’t remember | 4 (6.3%) |
| Dentist anxiety (Nr., %) | |
| Not at all | 55 (38.7%) |
| Low | 55 (38.7%) |
| Neutral | 8 (5.6%) |
| High | 19 (13.4%) |
| Very high | 5 (3.5%) |
| Dentist visit with children (Nr., %) | 134 (94.4%) |
| Child – Age - Visit (Mean ± SD, Median (IQR)) | 4.45 ± 2.3, 4 (3-6) |
| Dentist visit – Reason (Nr., %) | |
| Pain | 8 (6.1%) |
| Check-up | 72 (54.5%) |
| Cavity | 32 (24.2%) |
| Other | 20 (15.2%) |
| Child – Negative experiences (Nr., %) | 12 (8.5%) |
| Informing children before visit (Nr., %) | 121 (85.2%) |
| Preferred dentist (Nr., %) | |
| Pediatric dentist | 104 (73.2%) |
| Same dentist as parents’ | 24 (16.9%) |
| Let children decide | 8 (5.6%) |
| One closer to home | 6 (4.2%) |
| Child pain tolerance during treatment – normal (Nr., %) | 95 (66.9%) |
| General anesthesia – ideal for pain control (Nr., %) | |
| Highly disagree | 56 (39.4%) |
| Disagree | 29 (20.4%) |
| Neutral | 34 (23.9%) |
| Agree | 20 (14.1%) |
| Highly agree | 3 (2.1%) |
Table 2.
Comparison of participants’ characteristics according to reported dentist anxiety.
| Anxiety/Children narration (No., %) | Very low | Low | Neutral | High | Very high | p* |
| Absent | 8 (88.9) | 19 (63.3) | 4 (100) | 7 (46.7) | 3 (60) | 0.307 |
| Present | 1 (11.1) | 10 (33.3) | 0 (0) | 5 (33.3) | 2 (40) | |
| Don’t remember | 0 (0) | 1 (3.3) | 0 (0) | 3 (20) | 0 (0) | |
| Anxiety/General anesthesia – Ideal (No., %) | Very low | Low | Neutral | High | Very high | p* |
| Highly disagree | 23 (41.8) | 25 (45.5) | 4 (50) | 4 (21.1) | 0 (0) | 0.124 |
| Disagree | 9 (16.4) | 10 (18.2) | 1 (12.5) | 8 (42.1) | 1 (20) | |
| Neutral | 11 (20) | 14 (25.5) | 3 (37.5) | 5 (26.3) | 1 (20) | |
| Agree | 9 (16.4) | 6 (10.9) | 0 (0) | 2 (10.5) | 3 (60) | |
| Highly agree | 3 (5.5) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
* Fisher’s Exact Test.
Table 3.
Table 3. Perceived usefulness of information booklet.
| No. | % | ||
|---|---|---|---|
| Utility of information booklet | Not at all | 3 | 2.1% |
| Low | 13 | 9.2% | |
| Neutral | 23 | 16.2% | |
| High | 63 | 44.4% | |
| Very high | 40 | 28.2% | |
| Recommendation to other parents | Highly disagree | 0 | 0% |
| Disagree | 7 | 4.9% | |
| Neutral | 5 | 3.5% | |
| Agree | 53 | 37.3% | |
| Highly agree | 77 | 54.2% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



