
Submitted:
25 December 2025
Posted:
26 December 2025
You are already at the latest version
Abstract
Background: Infective endocarditis (IE) is a rare yet serious condition affecting the heart valves and the endocardium. Notably, there has been a shift in the risk-factor profile from traditional factors such as rheumatic heart disease and poor dental health to more iatrogenic causes such as prosthetic heart valves, cardiac devices, foreign body implants, haemodialysis, and immunosuppression. Purpose: While IE has been extensively studied in the past, the evolving landscape prompts an epidemiological re-evaluation of vulnerable patient populations. Our primary objective is to examine the trends in microbiological and echocardiographic diagnostics over two decades and to compare them across native valve endocarditis (NVE), prosthetic valve endocarditis (PVE), and cardiac implantable electronic device-related IE (CIED-IE). Methods: We conducted a retrospective analysis of longitudinal data encompassing 912 patients admitted with either a possible or definite IE diagnosis between 2001 and 2023. Results: The incidence of IE increased over the study duration (p<0.01) with octogenarians most affected (21%). Iatrogenic risk factors were associated with nearly two-thirds (63%) of patients diagnosed with IE, while traditional risk factors were evident in almost one-eighth (13%). Blood culture-negative endocarditis increased over the study duration (19% versus 27%, p<0.01) and Staphylococcus aureus (29%, p<0.01) became the dominant pathogen over Viridans group streptococci (14%, p=0.001). Imaging with transthoracic (56% in 2004 versus 75% in 2023) and transoesophageal echocardiography (57% in 2004 versus 79% in 2023) had an increasing contribution in the diagnosis of IE over the two decades. The subgroup analysis suggested that PVE and CIED-IE were more likely to have negative blood cultures (OR=3.7, CI [1.2-6.8] & OR=4.9, CI [1.3-8]) compared to NVE (OR=0.04, CI [0.02-0.8]). PVE and CIED-IE were more likely to have inconclusive echocardiographic imaging (OR=3.7, CI [1.2-6.6] & OR=2.2, CI [0.07-7.8]) compared to NVE (OR=0.63, CI [0.3-3.2]). Conclusion: Our study underscores the evolving nature of IE, now predominantly a healthcare-related disease. Diagnostic challenges persist due to the heterogeneity of the disease, with the emergence of distinct entities such as PVE and CIED-IE.
Keywords:
infective endocarditis
; prosthetic valve endocarditis
; cardiac implantable electronic devices (CIED)
; blood culture-negative endocarditis
; transcatheter aortic valve replacement (TAVRs)
; transthoracic echocardiography
; trans-oesophageal echocardiography
; epidemiology
1. Introduction
Infective endocarditis (IE), a relatively rare disease involving the endocardium and heart valves, is still associated with significant morbidity and mortality despite advances in treatment [1]. First described in 1885 by William Osler, the subsequent clinical challenges of IE have followed distinct phases: the pre-antibiotic era when it remained universally fatal; the antibiotic era, post the introduction of penicillin and its derivates; and in the recent decades, advanced diagnostic, medical and surgical interventions [2]. Despite being well-studied in the past there has been an evolution in contemporary IE risk factors with increasing incidence of prosthetic valves and cardiac implantable electronic devices (CIED), as well as emerging risk groups [3,4].
Hence, this retrospective analysis aims to assess – (i): the demographic changes in IE over time; (ii) predisposing factors; (iii) trends in microbiology and echocardiographic imaging; and (iv) compare native valve endocarditis (NVE) with prosthetic valve endocarditis (PVE) and cardiac implantable electronic device IE (CIED-IE).
2. Materials and Methods
2.1. Definitions
The diagnosis of IE was based on the modified Duke criteria [2]. The major criterion involves microbiological and cardiac structural evidence in conjunction with minor criteria which include predisposing cardiac conditions, vascular and immunological phenomena, and the presence of fever [5]. Microbiological data encompassed blood culture results of the causative organism and antimicrobial resistance findings [6]. Blood culture-negative endocarditis (BCNE) was defined as endocarditis without known aetiology after three separate blood cultures with no growth after at least 48 hours [7]. Echocardiographic imaging included transthoracic echocardiography (TTE) most commonly, followed by transoesophageal echocardiography (TOE) if needed for further clarification or persisting suspicion [8]. Echocardiographic major criteria include vegetation, abscess, new dehiscence of a prosthetic valve or new regurgitation [9].
2.2. Study Design and Patient Selection
The study was a retrospective analysis of longitudinal data of hospitalisations between January 2001 and January 2023 at Flinders Medical Centre in South Australia. The data includes all adult patients admitted with a ‘possible’ or ‘definite’ diagnosis of IE identified from hospital discharge codes. In cases where patients presented more than once, subsequent presentations were recognised as re-admissions. All patients regardless of age, sex, or comorbidities were included. The main exclusion criteria were cases not meeting the possible or definite criteria for IE, or patients transferred to private health facilities.
2.3. Data Collection and Study Variables
The timeline in Figure 1 shows the study timeline and the data retrieved using the electronic medical record system through hospital electronic databases and ICD discharge code of I33.0 in ICD-10 or previous equivalents [6]. These dataset across timeframes are detailed in Figure 1. Our sub-group data analysis consisted of 151 patients which were further categorised in which 15 (10%) had CIED-IE, 38 (25%) had PVE and 98 (65%) had NVE.
2.4. Statistical Analysis
The temporal pattern of microbiology and echocardiography trends across two decades were analysed using linear regression. The risk factor correlation analysis was performed using the Pearson correlation coefficient test and co-morbidities with univariate analysis. For subgroup analysis, we compared NVE, PVE, and CIED-IE using logistic regression, charted on a forest plot across diagnostic, complication, and mortality parameters. For this, NVE was age-adjusted to a mean of 65 years, as PVE and CIED-IE were more prevalent in the elderly (see Figure 1). We conducted all statistical analyses using SPSS version 28 and State 18.
3. Results
3.1. Patient Characteristics
In our study of 912 adult patients with definite or possible infective endocarditis (IE), the male-to-female ratio was 1.7:1, with 572 males and 340 females. The incidence of IE increased over the years, with the highest occurrence in the 80-89 age group with the median at 70 years and the mean at 67 years (Figure 2). Left-sided IE accounted for 86% of cases, with 45% aortic valve and 41% mitral valve involvement, while 14% were right-sided, all attributed to the tricuspid valve. The average hospital stay was 30 days, and the all-cause mortality rate was 21% at 12 months and 29% over the study duration.
3.2. Blood Cultures
The rate of culture-positivity declined over the study duration as shown in Figure 3 (Appendix A.1) as BCNE comprised of 15% of all cases. The incidence of Viridans group streptococci declined over the study duration. In contrast, Staphylococcus aureus, Methicillin-resistant Staphylococcus aureus (MRSA), and Enterococcus faecalis increased in incidence. Other organisms had a negative co-efficient indicating a decline, but none reached statistical significance. Viridans group streptococci and S. aureus remained the dominant organisms as seen in Figure 3. However, from 2013 onwards the incidence of S. aureus increased, whereas Viridans Streptococcus decreased.
3.3. Echocardiography
Of 659 patients who underwent a TTE, 417 (63%) had features suggestive of IE. TOE was performed in 322 (48%) patients and found evidence for IE in an additional 33 (5%) patients with a previously negative TTE. Across the two decades, TTE showed imaging evidence in 53% (n=169) of patients diagnosed with IE during 2004-2013, which increased to 73% (n=248) in the most recent decade (Figure 4). Similarly, TOE contributed to the diagnosis of IE in 60% (n=104) of cases in 2004-2013, which increased to 75% (n=111) of cases in the recent decade (Figure 4). Abscess as imaging evidence for IE diagnosis also increased over the study duration both in TTE and TOE (Figure 4).
3.4. Sub-Group Analysis
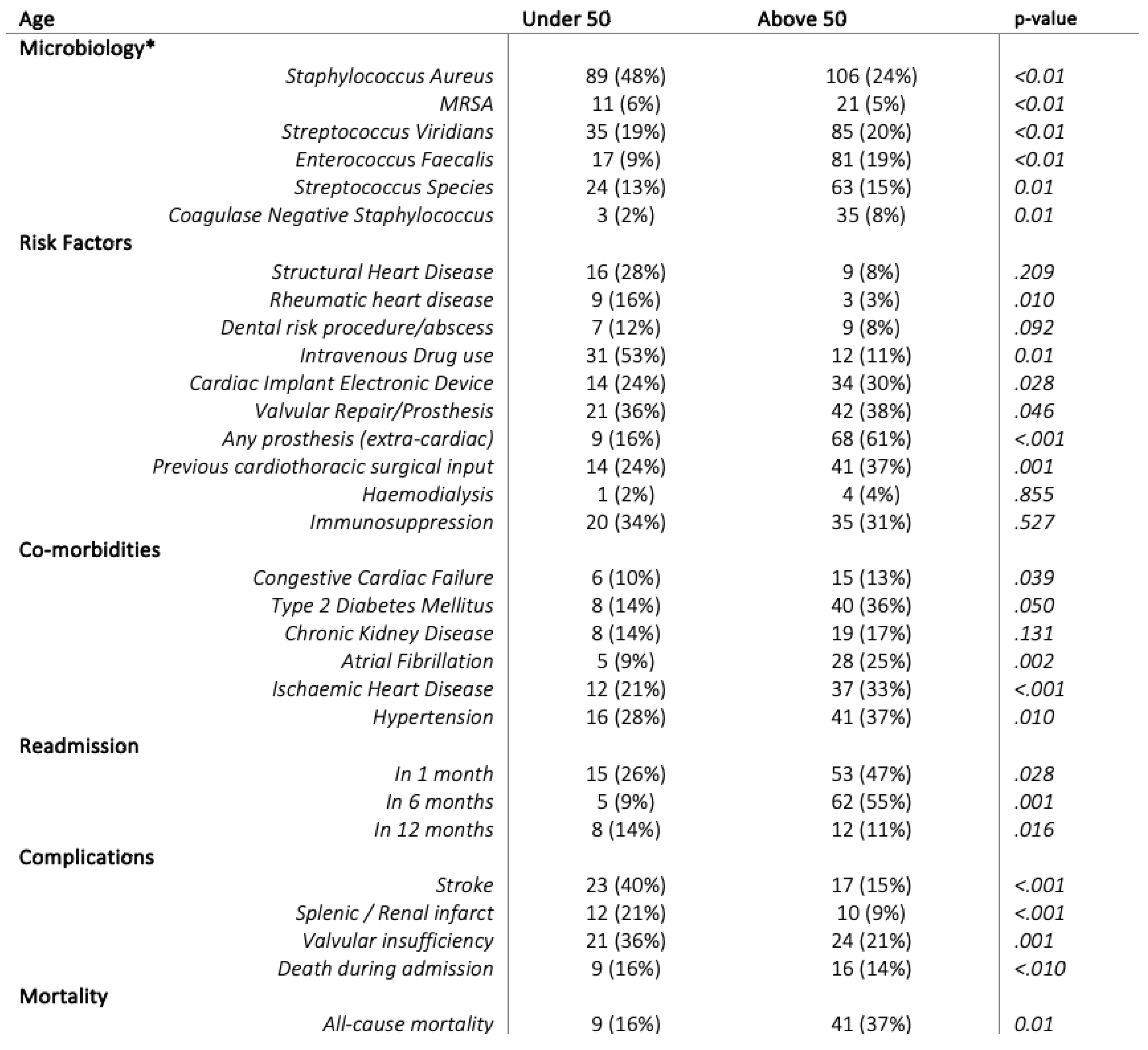
The older population (>50 years) had a widely distributed causative microbiology with S. aureus the leading pathogen as shown in Table 1 followed by Enterococcus faecalis, Streptococcus species, Coagulase-negative Staphylococcus, and MRSA. Comparatively, nearly half of the younger patients (<50 years) had bacteraemia with S. aureus.
Rheumatic heart disease showed an association with IE, although the number of affected cases was small. Structural heart disease, including congenital heart disease and bicuspid aortic valve, was more frequently identified in the younger cohort, while dental abscesses were more common in older patients; however, neither association reached statistical significance. Iatrogenic risk factors such as prior valve repair, prosthetic heart valves, cardiac implantable electronic devices, and extra-cardiac prosthetic material were markedly more prevalent than other risk factors, particularly among older adults. In contrast, more than half of patients with IE under the age of 50 were intravenous drug users.
Readmission within 1 month, 6 months, and 12 months was twice as high in the elderly compared to their younger counterparts. Stroke and valvular insufficiency remained high in both the younger and older groups, but fatal IE-related complications during hospital admission were significantly higher among older patients.
3.5. IE Compared Between NVE, PVE, and CIED-IE
PVE and CIED-IE were more likely to have BCNE (OR=3.7, CI [1.2-6.8] & OR=4.9, CI [1.3-8]), as seen in Figure 5. To allow more meaningful findings, our study tracked evidence for antibiotic use prior to culture, and this was found in 25 (26%) of NVE, 8 (21%) PVE and 5(33%) CIED-IE cases.
CIED-IE had higher odds for S. aureus as the causative pathogen (OR=1.5, CI [0.3-6.2]). Meanwhile, there was more likelihood of lack of echocardiography findings in both PVE and CIED-IE (OR=3.7, CI [1.2-6.6] & OR=2.2, CI [0.1-7.8]}) Similarly, abscess were more commonly found in CIED-IE and PVE (OR= 3.6, CI [1.5-10] and OR=1.7, CI [0.4-7]) Stroke was higher in PVE (OR=3.5, CI [0.89-10]), as was valvular insufficiency (OR=2.1, CI [0.6-4]). The 12-month mortality was no different across the entities (OR=0.3, CI [0.5-7.7] & OR=.49, CI [0.14-1.8] & OR=0.85, CI [0.3-2.4]).
4. Discussion
4.1. An Old Problem in Its New Forms
The new face of IE and the emergence of PVE and CIED-IE.
This study reveals that the complexity of IE is predominantly driven by This study reveals that the complexity of IE is predominantly driven by increasing medical interventions in the elderly while traditional risk factors for IE such as rheumatic heart disease, dental abscesses or procedures, and structural heart disease are now smaller contributors (Table 1). Instead, we are witnessing a growing correlation between IE and previous valvular repair, prosthetic heart valves, CIED, haemodialysis, and endovascular procedures (Table 1). IE is increasingly a healthcare-related disease, affecting immunosuppressed individuals (Table 1) [10]. This study further revealed that PVE and CIED-IE account for more than one-third of the IE disease burden (Figure 5). A decade ago, PVE was documented in less than 10%, and CIED-IE in less than 2% of IE cases respectively [10,11]. While no current literature indicates that NVE is decreasing per se, an increasing body of evidence suggests that IE is diversifying [6,7,8]. In the current era, with an ageing populace and longer life expectancies, we anticipate that CIED-IE and PVE will become major players in IE, particularly in the context of increasing numbers of minimally invasive cardiac structural interventions such as transcatheter aortic valve replacement (TAVR) and mitral transcatheter edge-to-edge repair (TEER) [6,8,10,12].
4.2. Microbiological Diagnosis
How has IE microbiology evolved?
The causative pathogens of IE have undergone a significant transformation, reflecting changes in predisposing risk factors and increased exposure to healthcare-related sources [4,13,14]. S. aureus has emerged as the predominant causative pathogen, primarily due to its correlation with IVDU, prosthetic valves, haemodialysis, diabetes, and CIED, all of which are now recognized as leading risk factors for IE (Figure 3) [1,14,15]. Conversely, we observed the prevalence of Viridans group streptococci had decreased likely due to a relative decline in oral sources of infection and rheumatic heart disease [16,17]. This shift is attributed to the effect of prophylactic antibiotics in reducing peri-operative or peri-procedural bacterial translocation, as well as targeted public health initiatives aimed at high-risk populations in Australia [17]. Meanwhile, Enterococcus faecalis has increased in the elderly cohort (Table 1) and is associated with haemodialysis, immunosuppression, diabetes, and TAVR [2,12,16]. Hence the last two decades have witnessed a transformation in the microbiology of IE, away from the conventional binary; subacute – Viridans Streptococcus and acute – S. aureus, towards a more diverse profile of organisms based on nuanced and novel risk factors [2,16].
Why is BCNE, is its rise a problem, and how are we mitigating it?
BCNE is a marker of poorer prognosis [13]. It prevents early diagnosis, reduces the likelihood of surgical intervention, and leads to sub-optimal medical management due to limitations in targeted antimicrobial regimens, their sensitivities, and resistance patterns [7,13,18,19]. Although we observed an increase in BCNE (Figure 3), global trends remain conflicting and highly variable from 7% to 66% [7]. This variation is attributed to how authors define BCNE and the differences in geographics, laboratory techniques, and local microbiological trends [7,20,21]. BCNE predominantly falls into two categories: BCNE due to antecedent antimicrobial therapy or inadequate growth despite the presence of an organism [7,20]. Our study found that 25% of our subgroup had antibiotics prior to cultures which comprised more than two-thirds of the BCNE cases. Of note is the higher BCNE in PVE and CIED-IE (Figure 5) remains unexplained, as the contamination with antibiotics remained statistically indifferent across the three IE entities. Hence, PVE and CIED-IE had an inherent propensity towards BCNE (Figure 5) compared to NVE. While a correlation between PVE & CIED-IE and BCNE does not imply causality, the authors of Caiati et al. (2019) found that introducing foreign leads causes endothelial damage and flow disruption. This forms micro-thrombosis on the endocardium, which in the presence of bacteraemia can lead to the formation of biofilms, especially in the elderly, diabetics and the immunocompromised [22]. Biofilms compromise immune defence mechanisms making eradication through medical therapy challenging, but also affect the efficacy of culturing [23]. Hence, the utility of blood cultures especially in patients with prosthetic heart valves and cardiac devices as a major diagnostic criterion is compromised [5,18,24].
New techniques to increase microbiological yield have emerged [7]. These include prolonging incubation periods for blood cultures, systemic serological assays for atypical and fastidious organisms, work-up for autoimmune diseases and specific plasma polymerase chain reaction (PCR) assays as per local microbiological trends [5,7]. The 2023 ESC guidelines found these diagnostic tools when employed in BCNE improved conventional cultural diagnostic methods in 30% of cases [25]. The recent update of the International Society for Cardiovascular Infectious Diseases (ISCVID) incorporated these techniques into the Duke criteria as it optimised the sensitivity and specificity for evidence of an infectious aetiology in the appropriate clinical situations, however its clinical application remains sub-optimally utilised and high costs remain a barrier to its wide-scale application [5,7].
4.3. Imaging Modalities
Evolving Utility of Echocardiography in IE Diagnostics
Echocardiography imaging modalities played an increasing role in IE diagnostics (Figure 4). Over the past decade, our study found that echocardiography both TTE and TOE had surpassed blood cultures in contributing to a ‘definite’ diagnosis (Figure 3 and Figure 4). In our analysis, imaging enabled reclassification from a ‘possible’ to a ‘definite’ diagnosis in 26% of later admissions, whereas only 6% of patients with an initial BCNE converted to seropositive cultures, consistent with recent reports [16,17,26,27]. Unlike blood culture analysis, which is routinely available, advanced echocardiographic imaging requires specialist interpretation and access to dedicated services; its availability and associated costs therefore make it a finite and clinically triaged resource [1,8,28].
Why Do We Need Advanced Imaging and the Future of Cardiac Imaging for IE?
Our study demonstrated that PVE and CIED-IE tended to lack diagnostic features for IE on echocardiography compared to NVE patients (age-adjusted) (Figure 5). A landmark meta-analysis by Kouijzer et al., in 2022 found TTE sensitivity reduced to 63% for PVE and 17% for CIED-IE, while TOE improved these figures to 80% for PVE and 67% for CIED [28]. Based on our single-centre experience and Mikail et al., (2022) the diagnostic challenges in interpreting PVE and CIED-IE imaging are attributed to acoustic shadowing, difficulties identifying perivalvular infection, artefacts from metal components and fibrinous deposition, and distinguishing normal-device-related anomalies or thrombus from active IE indicators [8,29].
The future of IE diagnosis lies in a multimodal imaging approach [2,8,29]. Emerging evidence for cardiac computed tomography (CCT) and 18-FDG-PET/CT led the 2023 ESC guidelines and the recent ISCVID update of the Duke criteria to incorporate these imaging modalities as major diagnostic criteria, resulting in improved sensitivities of PVE and CIED-IE ranging from 78% to 98%, aligning closer to NVE [5,25]. CCT provides superior spatial resolution, particularly with localising abscesses more frequently found in PVE and CIED-IE, however CCT cannot replace echocardiography as its independent sensitivity remains relatively low at 57% [5,8,29] with poor temporal resolution. Whilst 18-FDG-PET-CT allows a ‘definite’ diagnosis of PVE and CIED-IE, its sensitivity is much lower in NVE and exhibits significant false-positive rates in early post-surgical PVE, cardiac tumours, active thrombi, and atrial fibrillation [29,30]. Additionally, the use of antibiotics before imaging can impact the diagnostic performance and it remains prone to inter-observer variability and reporting [29,30]. Hence 18-FDG-PET/CT holds highest diagnostic utility in situations of suspected aortic root abscess or equivocal TOE features in patients with intracardiac prostheses. [30]. Though promising, 18-FDG-PET-CT is resource-intensive requiring expensive radiotracers, specialist nuclear medicine physicians for interpretation and access to state-of-the-art scanners only available in tertiary metropolitan centres [29,31].
Therefore, based on our disparities in diagnostics between NVE, PVE, and CIED-IE (Figure 5) tailoring individualised imaging workup based on the clinical context to balance sensitivity and specificity is paramount [8,29,32]. For instance, our findings highlight that a young culture-positive patient may suffice from a TTE or a secondary TOE if indicated to diagnose IE, but an elderly patient with comorbidities, cardiac devices, or prosthetic heart valves have a higher likelihood for BCNE and may warrant advanced imaging for the diagnosis [2,32].
4.4. The IE Mortality
Why Does IE Mortality Remain the Same as Several Decades Ago?
Our study highlights that mortality associated with IE remains a formidable clinical challenge with 21% at 12 months and 29% over the study duration. This echoes the enduring mortality rates documented in literature dating back to the 1970s [2,33]. A decade ago, López and colleagues performed an epidemiological analysis for IE and found the age group of 50 to 60 as bearing the highest IE disease burden [34]. However, our study and a 2022 European study observed octogenarians to be most affected by IE [35]. Hence, the disease burden has shifted to an elderly cohort with extensive cardiovascular comorbidities and iatrogenic risk factors, such as prosthetic valves, TAVR, and CIED (Table 1), which collectively confer higher risk of adverse outcomes [4,12,35]. Our research also reveals a notable increase in hospital stays, averaging nearly 30 days, compared to studies from the 1980s, where the mean admission duration was only 15 days, largely due to the rising complexity of comorbidities and again perhaps the diagnostic challenges, especially with PVE and CIED-IE [36]. Additionally, a shift towards aggressive nosocomial sources of bacteraemia such as S. aureus (Figure 3) and MRSA (Table 1), may also partly contribute to the mortality dilemma [1,6,21]. Thereby, the mortality remains high, perhaps as we treat an older, frailer, and more comorbid patient group that have a poorer baseline, and an inevitably limited window of prognostic benefit [1,4,32,35].
5. Limitations
This study has inherent limitations as an observational retrospective study. Selection bias was mitigated by including all patients admitted to Flinders Medical Centre with ‘definite’ or ‘possible’ IE. However, our findings may not be generalisable to different settings due to its single-centre design in a unique socioeconomic catchment area. The main diagnostic cardiac imaging modality analysed in this study is echocardiography because echocardiographic data was readily available throughout the study period. There is limited data for other advanced imaging modalities (CCT and 18-FDG-PET/CT) as these modalities were not routinely used, particularly earlier in the study period. Although we age-adjusted patients with NVE to compare with patients that had PVE and CIED-IE, there is potentially a small proportion with PVE and CIED-IE that may have been undiagnosed and assumed to be NVE due to frailty or clinical deterioration. Referral bias is possible as our centre serves as the state’s referral centre for CIED-IE explants. Data from 2001 to 2016 relied on automated extraction-based ICD discharge codes, which could introduce coding errors, however, our subgroup analysis from 2017 onwards had departmental database extraction.
6. Conclusion
Endocarditis in the contemporary era has emerged as a distinctly different clinical entity, characterized by changing microbiological patterns, evolving diagnostic techniques, and a shift toward an older patient population with multiple comorbidities. The increasing use of implantable medical devices has further contributed to its evolving epidemiology. This has resulted in increased complexity with challenges in diagnosis and management and remains a disease with significant morbidity and mortality.
Author Contributions
Conceptualization, A/Prof Majo Joseph. and Dr Sohel Modan.; methodology, A/Prof Majo Joseph.; software, Dr Sohel Modan.; validation, Dr James Gunton., Dr Kedar Madan. and Michael Hii.; formal analysis, Dr Sohel Modan. and Dr Kedar Madan.; investigation, A/Prof Majo Joseph.; resources, Dr Sohel Modan. and Dr Augustine Mugwagwa.; data curation, Dr Sohel Modan. and Dr Kedar Madan.; writing—original draft preparation, Dr Sohel Modan.; writing—review and editing, Dr Kedar Madan. and Dr Augustine Mugwagwa. and Dr James Gunton. and Dr Teddy Teo. and Dr Michael Hii. and A/Prof Majo Joseph.; visualization, Dr Sohel Modan.; supervision, A/Prof Majo Joseph. and Dr James Gunton.; project administration, A/Prof Majo Joseph.; funding acquisition, Nil. All authors have read and agreed to the published version of the manuscript. Sohel Modan contributed to the conception of the study, establishment of the infective endocarditis database, data extraction and analysis, and was primarily responsible for drafting and revising the manuscript.Associate Professor Majo Joseph served as the principal supervisor and senior investigator, providing overarching leadership, methodological oversight, and specialist expertise in cardiology imaging as Head of the Imaging Unit, and critically reviewed the manuscript.Dr James Gunton provided senior specialty input, contributed to the development of clinically relevant research questions, and assisted with manuscript drafting and intellectual refinement.Dr Augustine Mugwagwa contributed to the establishment and development of the infective endocarditis database and provided senior clinical input.Dr Teddy Teo, as an Infectious Diseases specialist, provided expert input regarding microbiological data interpretation and contributed to the infective endocarditis framework from a microbiological perspective.Dr Michael Hii and Dr Kedar Madan performed substantial transesophageal echocardiogram procedures, contributed to imaging interpretation, and assisted with manuscript preparation.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Southern Adelaide Local Health Network Office for Research according to the National Safety and Quality Health Service Standards (NSQHS) under the continuous improvement framework. The reference number of this project was 4465.
Informed Consent Statement
Informed consent was waived for all subjects involved in the study as it remained part of the continuous improvement framework by Southern Adelaide Local Health Network (SALHN) database of infective endocarditis. Given its retrospective nature and extraction of datapoints from an established infective endocarditis database, informed consent from each patient was deemed note required and waived as part of the ethics approval from the SALHN Office of Research. This is standard for retrospective studies with nil obvious individual patient identifiers.
Data Availability Statement
This data is available locally within the infective endocarditis database established at the Flinders Medical Centre at the Southern Adelaide Local Health Network. This was established in conjunction with the department of cardiology, department of infectious diseases, and department of cardiothoracic surgery. Unfortunately, there is no public data availability for this respecting the local privacy laws.
Acknowledgments
The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results”.
Abbreviations
The following abbreviations are used in this manuscript:
| ♦ IE: Infective endocarditis ♦ NVE: Native valve endocarditis ♦ PVE: Prosthetic valve endocarditis ♦ CIED-IE: Cardiac implant electronic device related to infective endocarditis. ♦ BCNE: Blood culture negative endocarditis ♦ TTE: Transthoracic echocardiography ♦ TOE: Transoesophageal echocardiography |
♦ ESC: European Society of Cardiology ♦ ISCVID: International Society for Cardiovascular Infectious Diseases ♦ IVDU: Intravenous Drug use ♦ CCT: Cardiac computed tomography ♦ 18-FDG-PET/CT: Fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography ♦ TAVR: transcatheter aortic valve replacement |
Appendix A
Appendix A.1

Table A1.
The linear regression data on blood cultures for all 912 patients. The co-efficient value indicates the direction and magnitude of change each year from 2001 to 2023. The standard error indicates the variability of a coefficient estimate to population value.
Table A1.
The linear regression data on blood cultures for all 912 patients. The co-efficient value indicates the direction and magnitude of change each year from 2001 to 2023. The standard error indicates the variability of a coefficient estimate to population value.
| Coefficient | Standard Error | p-value | |
| Positive Blood Culture | -0.453 | -0.739 | <0.01 |
| Staphylococcus Aureus | .479 | 0.088 | <0.01 |
| MRSA | .006 | 0.855 | <0.01 |
| Viridans Streptococci | -.540 | -.716 | <0.001 |
| E. faecalis | .001 | .125 | .006 |
| Streptococcus | -.108 | .138 | .440 |
| Coagulase negative S. | -.076 | -.161 | .473 |
| Fungal & Others | -.167 | -.351 | .109 |
| Gram-negatives | -.121 | .090 | .191 |
References
- Thuny, F; Grisoli, D; Collart, F; Habib, G; Raoult, D. Management of infective endocarditis: challenges and perspectives. The Lancet 2012, 379, 965–75. [Google Scholar] [CrossRef]
- Cahill, TJ; Baddour, LM; Habib, G; Hoen, B; Salaun, E; et al. Challenges in Infective Endocarditis. J Am Coll Cardiol 2017, 69, 325–44. [Google Scholar] [CrossRef]
- Bell, A; Adegboye, OA. The Epidemiology of Infective Endocarditis in New South Wales, Australia: A Retrospective Cross-Sectional Study From 2001 to 2020. Heart Lung Circ 2023, 32, 506–17. [Google Scholar] [CrossRef]
- Holland, DJ; Simos, PA; Yoon, J; Sivabalan, P; Ramnarain, J; Runnegar, NJ. Infective Endocarditis: A Contemporary Study of Microbiology, Echocardiography and Associated Clinical Outcomes at a Major Tertiary Referral Centre. Heart Lung Circ 2020, 29, 840–50. [Google Scholar] [CrossRef] [PubMed]
- Fowler, VG; Durack, DT; Selton-Suty, C; Athan, E; Bayer, AS; et al. The 2023 Duke-International Society for Cardiovascular Infectious Diseases Criteria for Infective Endocarditis: Updating the Modified Duke Criteria. Clinical Infectious Diseases 2023, ciad271. [Google Scholar] [CrossRef]
- Habib, G; Lancellotti, P; Antunes, MJ; Bongiorni, MG; Casalta, J-P; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC)Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). European Heart Journal 2015, 36, 3075–128. [Google Scholar] [PubMed]
- McHugh, J; Saleh, OA. Updates in Culture-Negative Endocarditis. Pathogens 2023, 12, 1027. [Google Scholar] [CrossRef] [PubMed]
- Silbiger, JJ; Rashed, E; Chen, H; Wiesenfeld, E; Robinson, SE; Cagliostro, M. Cardiac Imaging for Diagnosis and Management of Infective Endocarditis. Journal of the American Society of Echocardiography 2022, 8 35, 910–24. [Google Scholar] [CrossRef] [PubMed]
- Li, JS; Sexton, DJ; Mick, N; Nettles, R; Fowler, VG; et al. Proposed Modifications to the Duke Criteria for the Diagnosis of Infective Endocarditis. Clinical Infectious Diseases 2000, 30, 633–8. [Google Scholar] [CrossRef]
- Döring, M; Richter, S; Hindricks, G. The Diagnosis and Treatment of Pacemaker-Associated Infection. Dtsch Arztebl Int 2018, 10 115, 445–52. [Google Scholar] [CrossRef]
- Nagpal, A; Sohail, MR; Steckelberg, J. Prosthetic valve endocarditis: State of the heart. Clinical Investigation 2012, 2, 803–17. [Google Scholar]
- Zakhour, J; Allaw, F; Kalash, S; Wehbe, S; Kanj, SS. Infective Endocarditis after Transcatheter Aortic Valve Replacement: Challenges in the Diagnosis and Management. Pathogens 2023. [Google Scholar]
- Kong, WKF; Salsano, A; Giacobbe, DR; Popescu, BA; Laroche, C; et al. Outcomes of culture-negative vs. culture-positive infective endocarditis: the ESC-EORP EURO-ENDO registry. Eur Heart J 2022, 43, 2770–80. [Google Scholar]
- Tran, HM; Truong, VT; Ngo, TMN; Bui, QPV; Nguyen, HC; et al. Microbiological profile and risk factors for in-hospital mortality of infective endocarditis in tertiary care hospitals of south Vietnam. PLoS One 2017, 14 12, e0189421. [Google Scholar] [CrossRef]
- Poorzand, H; Hamidi, F; Sheybani, F; Ghaderi, F; Fazlinezhad, A; et al. Infective Endocarditis: Clinical Characteristics and Echocardiographic Findings. Frontiers in Cardiovascular Medicine 2022, 9. [Google Scholar] [CrossRef]
- Cimmino, G; Bottino, R; Formisano, T; Orlandi, M; Molinari, D; et al. Current Views on Infective Endocarditis: Changing Epidemiology, Improving Diagnostic Tools and Centering the Patient for Up-to-Date Management. Life 2023, 13, 377. [Google Scholar] [CrossRef] [PubMed]
- Mahony, M; Lean, D; Pham, L; Horvath, R; Suna, J; et al. Infective Endocarditis in Children in Queensland, Australia: Epidemiology, Clinical Features and Outcome. Pediatr Infect Dis J 2021, 40, 617–22. [Google Scholar]
- Meidrops, K; Zuravlova, A; Osipovs, JD; Kalejs, M; Groma, V; et al. Comparison of outcome between blood culture positive and negative infective endocarditis patients undergoing cardiac surgery. Journal of Cardiothoracic Surgery 2021, 16, 147. [Google Scholar] [CrossRef]
- Kang, D-H; Kim, Y-J; Kim, S-H; Sun, BJ; Kim, D-H; et al. Early Surgery versus Conventional Treatment for Infective Endocarditis. New England Journal of Medicine 2012, 19 366, 2466–73. [Google Scholar] [CrossRef]
- Godfrey, R; Curtis, S; Schilling, WH; James, PR. Blood culture negative endocarditis in the modern era of 16S rRNA sequencing. Clin Med (Lond) 2020, 20, 412–6. [Google Scholar] [CrossRef] [PubMed]
- Mutagaywa, RK; Vroon, JC; Fundikira, L; Wind, AM; Kunambi, P; et al. Infective endocarditis in developing countries: An update. Frontiers in Cardiovascular Medicine 2022, 9. [Google Scholar] [CrossRef]
- Caiati, C; Pollice, P; Lepera, ME; Favale, S. Pacemaker Lead Endocarditis Investigated with Intracardiac Echocardiography: Factors Modulating the Size of Vegetations and Larger Vegetation Embolic Risk during Lead Extraction. Antibiotics (Basel) 2019, 8. [Google Scholar]
- Anantha Narayanan, M; Mahfood Haddad, T; Kalil, AC; Kanmanthareddy, A; Suri, RM; et al. Early versus late surgical intervention or medical management for infective endocarditis: a systematic review and meta-analysis. Heart 2016, 102, 950–7. [Google Scholar] [CrossRef] [PubMed]
- Østergaard, L; Smerup, MH; Iversen, K; Jensen, AD; Dahl, A; et al. Differences in mortality in patients undergoing surgery for infective endocarditis according to age and valvular surgery. BMC Infect Dis 2020, 20, 705. [Google Scholar] [CrossRef] [PubMed]
- Delgado, V; Ajmone Marsan, N; de Waha, S; Bonaros, N; Brida, M; et al. 2023 ESC Guidelines for the management of endocarditis: Developed by the task force on the management of endocarditis of the European Society of Cardiology (ESC) Endorsed by the European Association for Cardio-Thoracic Surgery (EACTS) and the European Association of Nuclear Medicine (EANM). European Heart Journal 2023, ehad193. [Google Scholar]
- Williams, ML; Doyle, MP; McNamara, N; Tardo, D; Mathew, M; Robinson, B. Epidemiology of infective endocarditis before versus after change of international guidelines: a systematic review. Ther Adv Cardiovasc Dis 2021, 15, 17539447211002687. [Google Scholar]
- Chen, H; Zhan, Y; Zhang, K; Gao, Y; Chen, L; et al. The Global, Regional, and National Burden and Trends of Infective Endocarditis From 1990 to 2019: Results From the Global Burden of Disease Study 2019. Front Med (Lausanne) 2022, 9, 774224. [Google Scholar]
- Kouijzer, JJP; Noordermeer, DJ; van Leeuwen, WJ; Verkaik, NJ; Lattwein, KR. Native valve, prosthetic valve, and cardiac device-related infective endocarditis: A review and update on current innovative diagnostic and therapeutic strategies. Front Cell Dev Biol 2022, 10, 995508. [Google Scholar] [CrossRef]
- Mikail, N; Hyafil, F. Nuclear Imaging in Infective Endocarditis. Pharmaceuticals (Basel) 2021, 15. [Google Scholar] [CrossRef]
- Rojas-Moreno, C. Systematic Whole-body 18F-FDG PET/CT in Infective Endocarditis: Are We There Yet? Clinical Infectious Diseases 2021, 73, 404–5. [Google Scholar]
- Haq, IU; Haq, I; Griffin, B; Xu, B. Imaging to evaluate suspected infective endocarditis. Cleve Clin J Med 2021, 88, 163–72. [Google Scholar]
- Millar, BC; Habib, G; Moore, JE. New diagnostic approaches in infective endocarditis. Heart 2016, 102, 796–807. [Google Scholar] [CrossRef] [PubMed]
- Nomura, A; Omata, F; Furukawa, K. Risk factors of mid-term mortality of patients with infective endocarditis. European journal of clinical microbiology & infectious diseases: official publication of the European Society of Clinical Microbiology 2010, 29, 1355–60. [Google Scholar]
- López, J; Revilla, A; Vilacosta, I; Sevilla, T; Villacorta, E; et al. Age-dependent profile of left-sided infective endocarditis: a 3-center experience. Circulation 2010, 121, 892–7. [Google Scholar]
- Oliver, L; Lavoute, C; Giorgi, R; Salaun, E; Hubert, S; et al. Infective endocarditis in octogenarians. Heart 2017, 103, 1602–9. [Google Scholar] [CrossRef]
- Mansur, AJ; Grinberg, M; Bellotti, G; Jatene, A; Pileggi, F. Infective endocarditis in the 1980s: Experience at a heart hospital. Clinical cardiology (Mahwah, N.J.) 1990, 13, 623–30. [Google Scholar]
Figure 1.
Flowchart integrating the study timeline with all data categories, showing the respective collection periods for baseline, echocardiographic, and subgroup clinical variables.
Figure 1.
Flowchart integrating the study timeline with all data categories, showing the respective collection periods for baseline, echocardiographic, and subgroup clinical variables.
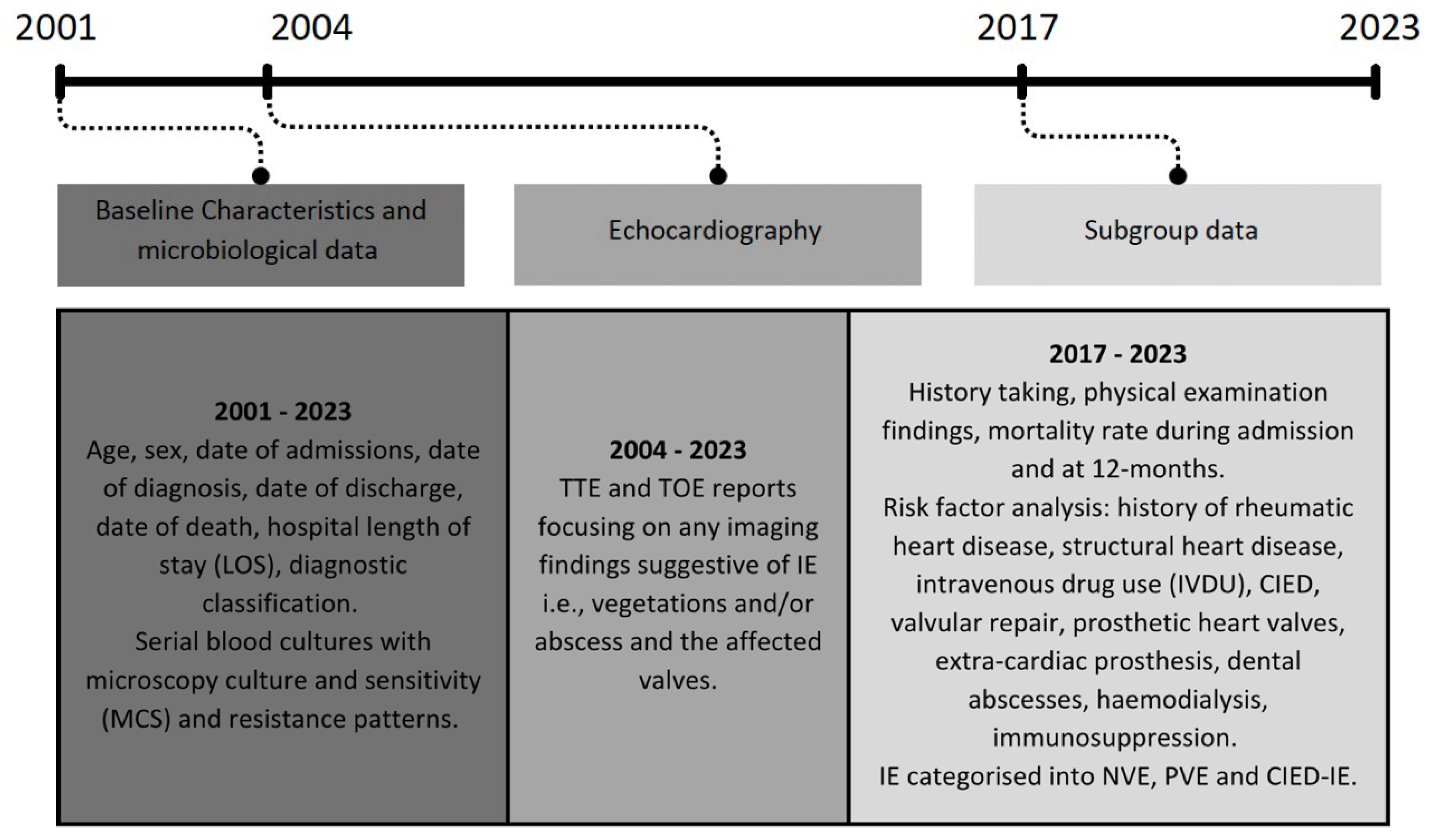
Figure 2.
Number of patients diagnosed over the 2001- 2023 with infective endocarditis and their age at the time stratified by 10-year age group.
Figure 2.
Number of patients diagnosed over the 2001- 2023 with infective endocarditis and their age at the time stratified by 10-year age group.
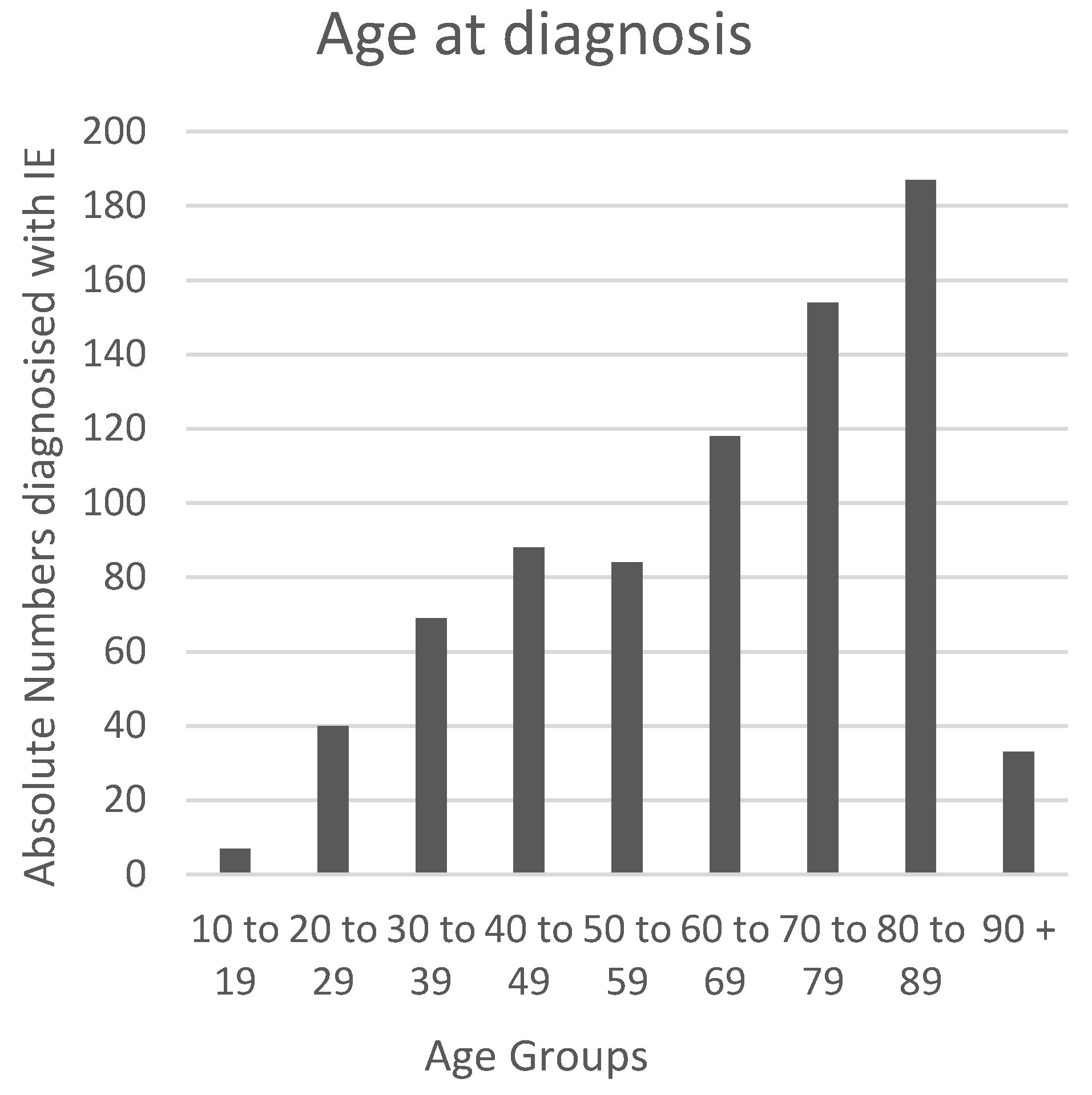
Figure 3.
Line graph showing the temporal trends of blood culture positivity and the common infective organism over the duration of this study.
Figure 3.
Line graph showing the temporal trends of blood culture positivity and the common infective organism over the duration of this study.
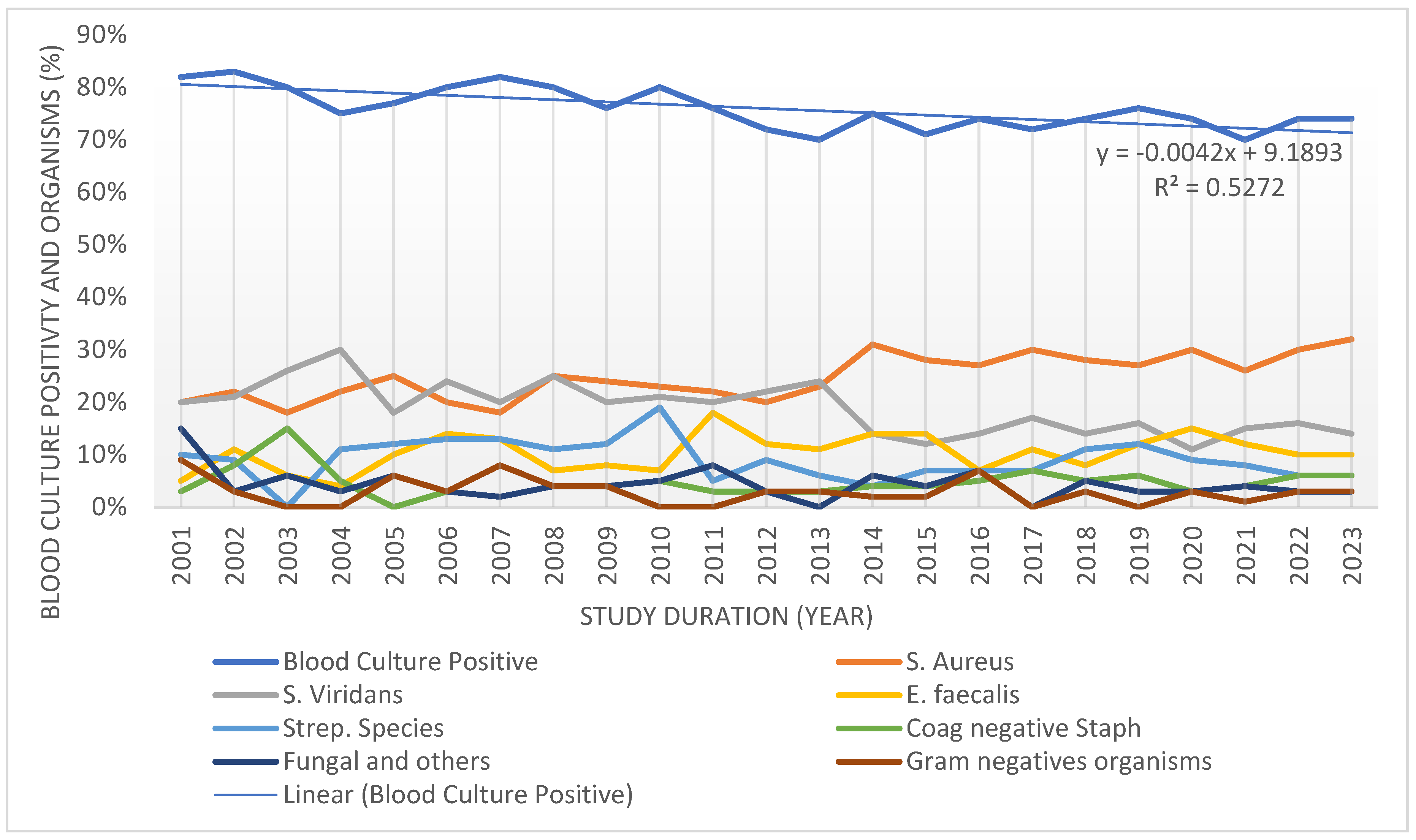
Figure 4.
Proportion of IE diagnosis based on major echocardiographic features, stratified by TTE and TOE over two decades (2004-2023). The line graphs represent the percentage of TTE (left) and TOE (right) that contributed to the diagnosis of IE with imaging evidence for vegetations, both presence of vegetations and abscesses and meeting major echocardiographic criteria.
Figure 4.
Proportion of IE diagnosis based on major echocardiographic features, stratified by TTE and TOE over two decades (2004-2023). The line graphs represent the percentage of TTE (left) and TOE (right) that contributed to the diagnosis of IE with imaging evidence for vegetations, both presence of vegetations and abscesses and meeting major echocardiographic criteria.
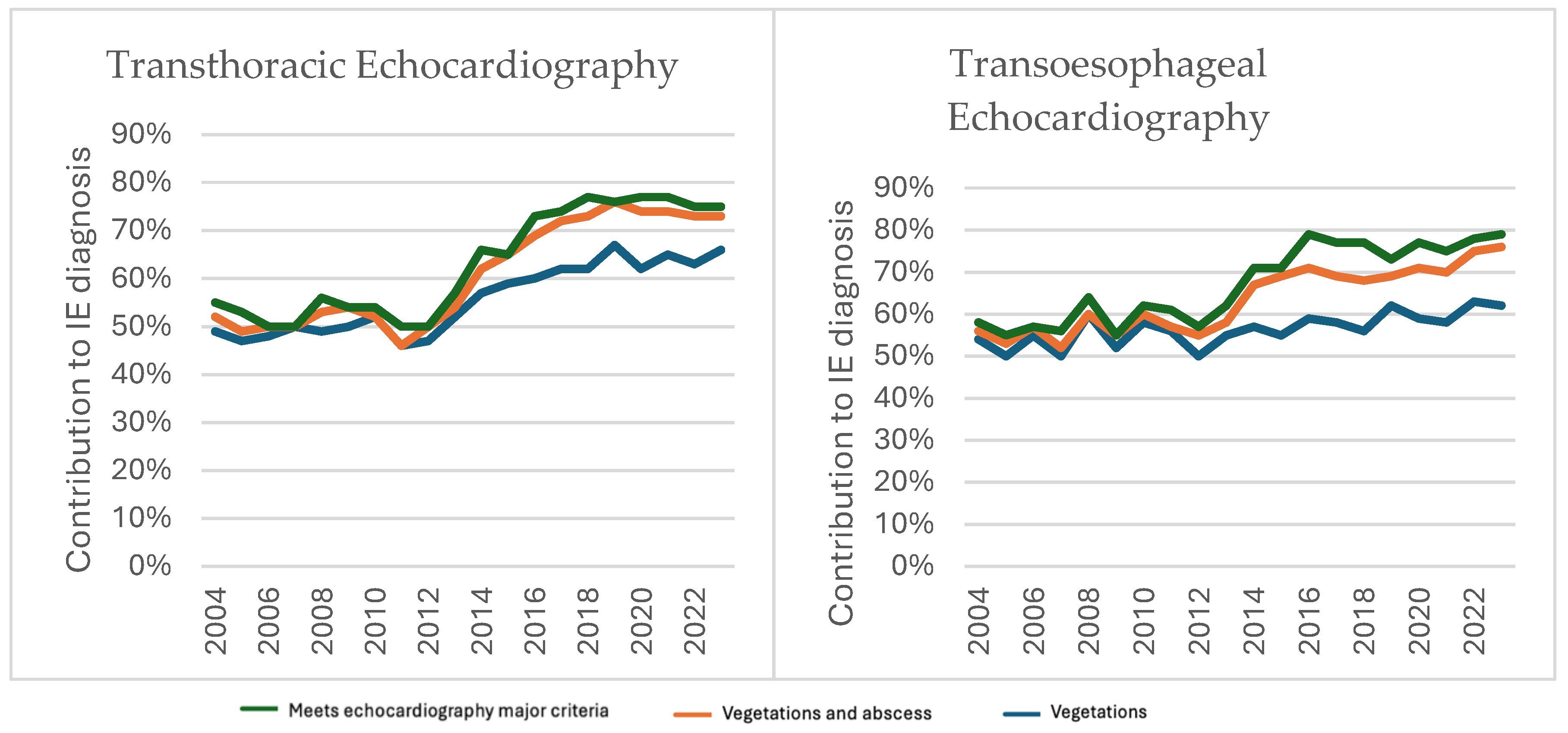
Figure 5.
Forest plot comparing CIED-IE (left), PVE (middle) & NVE (right)* (age adjusted) with odds ratio (OR) depicted as the diamond marked on the confidence intervals (CI) line. The vertical line across the columns indicates the odds ratio of 1 which indicates neither a higher nor lower odds. If the CI crosses the odds ratio of 1, it indicates inconclusive findings. The OR and CI both to the right of the line of no effect indicate a higher odd, whilst both on the left of the line of no effect indicate lower odds.
Figure 5.
Forest plot comparing CIED-IE (left), PVE (middle) & NVE (right)* (age adjusted) with odds ratio (OR) depicted as the diamond marked on the confidence intervals (CI) line. The vertical line across the columns indicates the odds ratio of 1 which indicates neither a higher nor lower odds. If the CI crosses the odds ratio of 1, it indicates inconclusive findings. The OR and CI both to the right of the line of no effect indicate a higher odd, whilst both on the left of the line of no effect indicate lower odds.
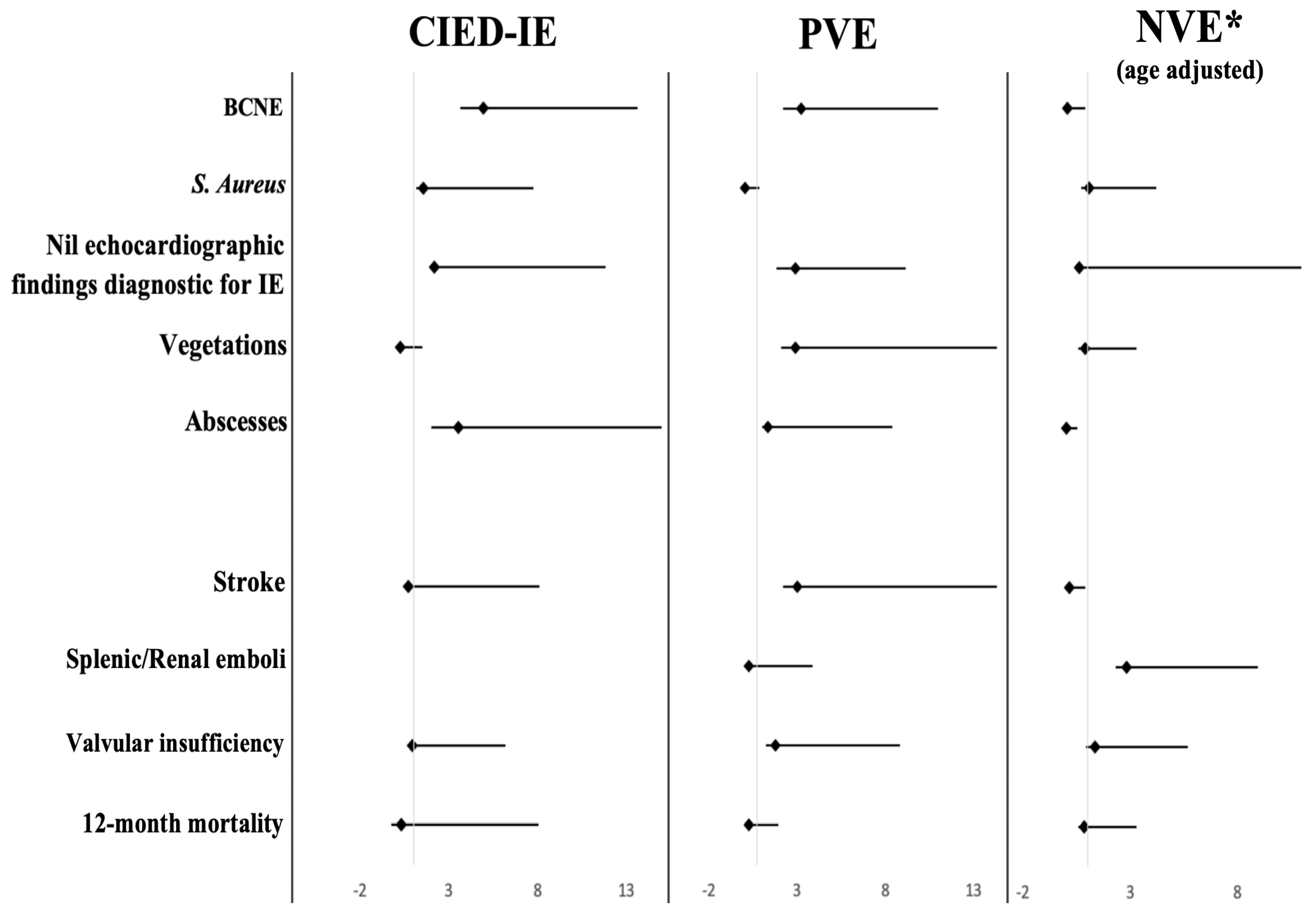
Table 1.
IE Patient characteristics stratified by age: microbiology, risk factors, co-morbidities, readmission, complications, and mortality.
Table 1.
IE Patient characteristics stratified by age: microbiology, risk factors, co-morbidities, readmission, complications, and mortality.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



