
Submitted:
25 December 2025
Posted:
26 December 2025
You are already at the latest version
Abstract
Diffusion tensor imaging (DTI) tractography is routinely employed in neurosurgical planning; however, the prognostic significance of quantitative DTI metrics for postoperative functional outcomes remains ambiguous. We conducted a PRISMA-informed systematic review of PubMed (January 2005–December 1, 2025), supplemented by additional indexed sources, to synthesize evidence on quantitative DTI measures associated with postoperative motor, language, and cognitive outcomes following intracranial surgery. Thirty-seven studies were included, primarily single-center and predominantly focused on glioma surgery. Motor outcomes exhibited the most consistent associations, with reduced corticospinal tract integrity and adverse postoperative diffusion changes correlating with weakness and poorer recovery. Recovery from supplementary motor area syndrome was associated with interhemispheric callosal connectivity, with greater disconnection predicting prolonged symptom duration. Language outcomes demonstrated reproducible structure–function relationships: higher preoperative integrity of dorsal language pathways was associated with milder postoperative aphasia and better recovery, whereas postoperative tract disruption and diffusivity changes predicted persistent naming and fluency deficits; ventral pathway alterations were specifically linked to lexico-semantic impairment. In epilepsy surgery, language performance correlated with contralateral and distributed network diffusion changes, consistent with reorganization. Evidence for cognition and gait outcomes was limited and mainly involved association, limbic, and callosal pathways. Overall, quantitative DTI provides clinically relevant markers of tract and network disruption and postoperative remodeling, but methodological heterogeneity and limited external validation currently preclude universal prognostic thresholds.
Keywords:
neurosurgery
; diffusion tensor imaging (DTI)
; fiber tracking
; fractional anisotropy (FA)
; corticospinal tract (CST)
; surgical outcome
1. Introduction
Diffusion magnetic resonance imaging (dMRI) has become an integral part of preoperative planning for intracranial surgery, particularly in patients with lesions close to eloquent white matter pathways [1]. In this setting, dMRI is especially useful, as proper sequences enable tractography, that is, the computational reconstruction of white matter fiber pathways [2]. This capability is crucial in neuro-oncology, where the goal is to maximize lesion removal while preserving the subcortical pathways that support motor, language, and cognitive functions [3]. However, tractography is only one of several applications of dMRI in this field. Another promising application is the investigation of apparently normal, non-pathological tissue microstructures. While several models have been developed over the years, diffusion tensor imaging (DTI) is the most commonly used in the scientific community with clinical applications, particularly because of the relative simplicity of the model and the complexity of the data required to perform this processing, other than historical reasons [4,5].
DTI relies on modeling water diffusion in each voxel as a tensor, that is, a 3×3 matrix decomposition of the diffusion coefficient along the three spatial axes, rather than a single scalar value. This matrix can be mathematically represented by an ellipsoid. The major and minor axes of the diffusion ellipsoid are defined by three orthogonal unit vectors (εi), known as eigenvectors, which describe the main directions of diffusion, and their lengths (λi), called eigenvalues, which are related to the diffusivity value in that direction [6]. Based on this framework, several scalar metrics interpreted as tissue microstructural characteristics can be derived. The DTI model defines a set of scalar quantities that locally describe the diffusion properties of the tissue based on eigenvalues λi. The first measure is the mean diffusivity (MD), which is the average eigenvalue. MD is related to the total amount of diffusion in a voxel, which is inversely related to the amount of water in the extracellular space. Connected measures are the axial (AD, equal to λ1) and radial (RD, equal to the average of λ2 and λ3) diffusivities, which describe the diffusivity along the main direction of diffusion and in the orthogonal plane, respectively. The second commonly used metric is the fractional anisotropy (FA), which measures the fraction of diffusion that is anisotropic (i.e., the existence of one preferential direction of diffusion opposed to the other axes) and can be interpreted as the difference between the diffusion ellipsoid and the perfect sphere along a single direction. An example of the voxel-wise parameter maps of MD, AD, RD, and FA is shown in Figure 1.
Additionally, microstructural modelling and tractography can be combined to perform along-tract analysis, that is, the investigation of voxel-wise parameter maps (such as FA and MD) along the course of a specific, tractography-reconstructed tract, rather than calculating the statistic over un-specific regions of interest [7].
Alterations in DTI metrics can result from axonal injury, demyelination, edema, increased cellularity, or tract displacement, making them sensitive, albeit not specific, indicators of microstructural changes [8]. Both experimental and clinical studies indicate that a decrease in FA, along with an increase in MD or RD, generally indicates axonal disorganization, edema, or demyelination rather than complete axonal loss [9]. However, interpreting these changes is complex, particularly when considered in isolation and without strong a priori hypotheses regarding the potential neurophysiological origins of the alterations, as they may be attributed to various factors [10].
In neurosurgical patients, tumors, cavernomas, hemorrhages, and hydrocephalus may infiltrate, compress, or disconnect key pathways, such as the corticospinal tract (CST), language-related association fibers, and commissural connections. Qualitative tractography is widely used to map these tracts, but quantitative DTI provides additional information on the microstructural burden and residual “reserve” of the affected pathways [11]. In the stroke literature, early reductions in CST FA and related metrics have been associated with poorer motor recovery, and DTI-based biomarkers have been evaluated as predictors of rehabilitation potential [12]. A similar prognostic role for DTI metrics has been suggested in neurosurgical cohorts; however, the evidence is scattered across small, heterogeneous studies and has not yet been comprehensively synthesized.
Understanding whether and how DTI metrics predict functional preservation and recovery after brain surgery is clinically relevant for several reasons, including the following. First, robust preoperative markers of tract vulnerability and neuroplastic potential could refine risk stratification, inform patient counseling, and guide the extent of resection and approach [13]. Second, early postoperative DTI may help differentiate transient deficits due to edema or temporary disconnection from permanent injury, thereby influencing the prognosis and rehabilitation planning [14]. Third, longitudinal DTI can serve as an imaging biomarker for structural reorganization and treatment response [15].
Therefore, this systematic review aimed to achieve three objectives.
- To summarize how quantitative DTI metrics have been used to characterize lesions and surgery-related white matter changes in patients undergoing brain surgery:
- To evaluate the evidence for DTI based prediction of motor, language, gait and cognitive outcomes across neurosurgical conditions; and
- To identify the methodological limitations and priorities for future research needed to establish DTI as a reliable prognostic biomarker in neurosurgical practice.
2. Materials and Methods
2.1. Study Design and Search Strategy
To ensure a robust and transparent approach to our literature search and analysis, this systematic review was designed in compliance with the PRISMA guidelines [16]. The search was conducted in MEDLINE (Medical Literature Analysis and Retrieval System Online; through the PubMed interface) from January 1990 to August 2025, using the following keywords: Diffusion Tensor Imaging (or diffusion tensor, DTI, tractography, fiber tracking) and functional outcome (or motor, motor recovery, language, aphasia, paresis, cortical reorganization, plasticity) and surgery (or resection, postoperative, craniotomy). To reduce publication bias and identify additional eligible studies, we queried the Elicit platform (Semantic Scholar and OpenAlex) [17] and screened the reference lists of the included articles and relevant reviews.
Studies were considered eligible if they involved adult patients who underwent intracranial surgery, such as tumor resection, epilepsy surgery, hematoma evacuation, or shunt placement. Methodological descriptions were required to provide comprehensive details on diffusion MRI acquisition, DTI processing methods (including preprocessing steps, tensor or higher-order modeling, and software used), and post-processing strategies (whole-brain, region-of-interest, or tractography). Studies were included only if they evaluated at least one DTI metric (FA, AD, RD, or MD), while those performing tractography without reporting DTI metrics were excluded from the study. Additionally, inclusion necessitated the reporting of quantifiable postoperative functional outcomes (motor, language, and cognitive), assessed at least once beyond the immediate perioperative period. Eligible designs encompassed original clinical investigations, including prospective or retrospective cohort studies, case series, and single-case reports, with full texts available in English. Reviews, meta-analyses, editorials, technical notes without patient data, and conference abstracts were excluded.
2.2. Study Selection and Data Extraction
All identified citations were imported into a reference management platform (Zotero version 7. x; open-source software; https://www.zotero.org). After removing duplicates, titles, and abstracts were screened by the first author to exclude records that were clearly unrelated to neurosurgery, did not perform quantitative diffusion MRI analysis, or did not report postoperative clinical data. Full texts were retrieved for studies deemed potentially relevant, and their eligibility was assessed in detail against the predefined criteria. The second author examined the equivocal cases and verified the final set of included studies.
The following information was retrieved from the manuscripts retained for the qualitative synthesis: study design and sample size, patient population and neurosurgical procedure, lesion type and location, regions of interest (ROIs) or tracts studied, quantitative DTI metrics, timing of imaging (preoperative, early postoperative, longitudinal follow-up), neurological outcomes (motor, language, cognition), and main reported associations between DTI metrics and clinical outcomes.
Owing to the marked heterogeneity in study designs, imaging protocols, and outcome measures, we did not attempt a meta-analysis. Instead, a qualitative synthesis was performed, grouping studies by their primary clinical domains (motor, language, cognition/gait).
3. Results
3.1. Search Results
The PubMed search identified 801 records published between 2005 and December 1, 2025. After title/abstract screening, 745 records were excluded, and 56 full texts were assessed for their eligibility. Nineteen studies met the inclusion criteria [18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36] and were included in the Twelve additional eligible studies were identified via the Elicit platform [34,37,38,39,40,41,42,43,44,45,46,47] and six via reference screening [48,49,50,51,52,53], yielding 37 studies included in the qualitative synthesis (Figure 2)
3.2. Characteristics of Included Studies
Table 1 summarizes the key characteristics of the 37 studies included in this systematic review. Most studies examined patients undergoing glioma resection [19,21,22,23,26,28,30,36,37,45,46,48,52,54], with additional studies investigating epilepsy surgery [40,47] and other conditions, including brainstem cavernoma [53], basal ganglia hemorrhage [43], moyamoya disease [41], and normal-pressure hydrocephalus [39]. The sample sizes ranged from 5 to 360 patients, with the majority being single-center retrospective or prospective cohort studies. The primary outcome domains included motor function [21,22,23,24,25,26,27,28,29,34,36,37,42,43,45,49,52,53], language function [18,19,20,31,38,40,44,46,47,50,55], and broader cognitive assessments [38,39,41].
3.3. DTI Metrics and Technical Approaches
Diffusion imaging was performed on 1.5T or 3T scanners using single-shot echo-planar sequences. The number of diffusion-encoding directions ranged from 6 to 64, with b values typically between 800 and 1,000 s/mm² and at least one b0 image. Preprocessing pipelines included correction for eddy currents and susceptibility-induced distortions, brain extraction, and tensor estimation. Most studies have utilized deterministic tractography algorithms with FA thresholds ranging from 0.1 to 0.2. The analysis software included FSL [18,19,20,25,41,46,47], Brainlab Elements [21,30,38], and DSI Studio [21,22,28].
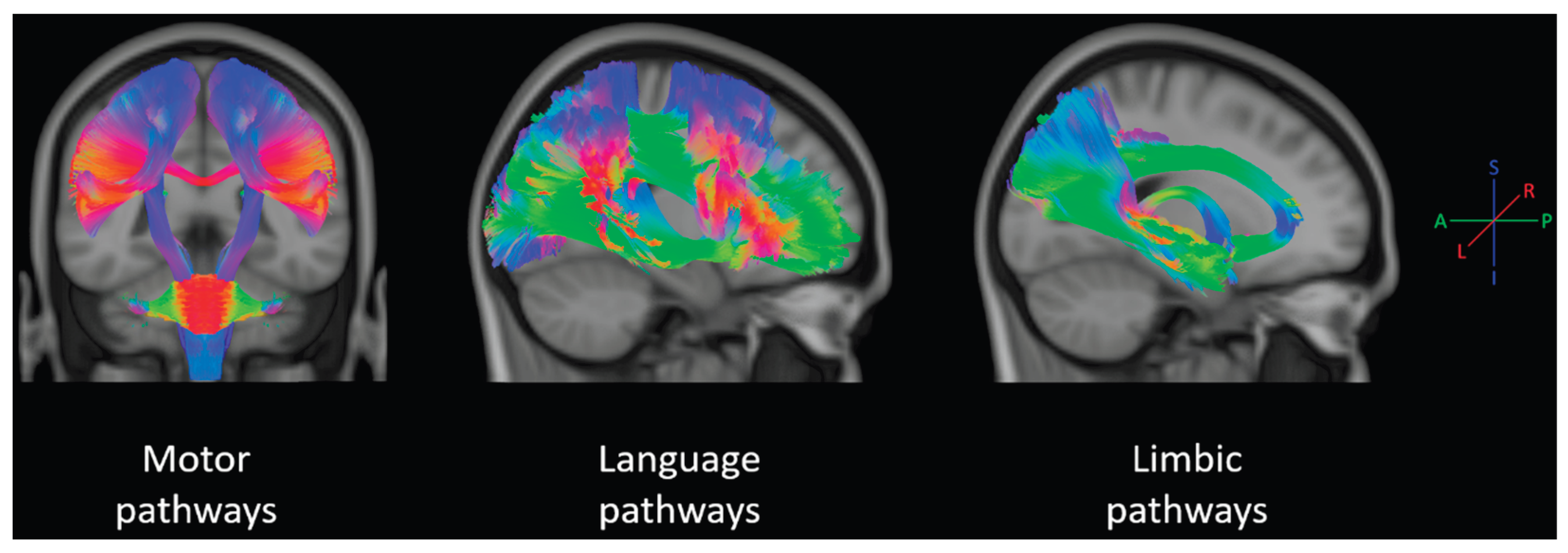
ROIs were defined manually in many studies, semi automatically using atlases in others, or post hoc from significant clusters in voxel wise analyses. The white matter pathways of interest, which are visually represented in Figure 2, included the following:
- Motor pathways: CST from the precentral gyrus through the corona radiata, posterior limb of the internal capsule, cerebral peduncle, pons, and medulla; frontal aslant tract (FAT); premotor and SMA connections, and corpus callosum segments connecting right and left SMAs. [21,22,23,24,25,26,27,28,29,35,37,42,43,45,48,49,51,53,54]
Figure 3.
Representation of the tractography-reconstructed main tracts supporting motor, language, and cognitive (within the limbic system) functions. The represented motor pathways included the cortico-spinal tract, cerebellar peduncles, frontal aslant tract, and motor corpus callosum; language pathways included the arcuate fasciculus, superior longitudinal fasciculus, inferior fronto occipital fasciculus, uncinate fasciculus, inferior longitudinal fasciculus, frontal aslant tract; and limbic pathways included the cingulum bundle, fornix, and middle temporal tract. Template tracts were selected from the KUL-FWT atlas [56]. The color encoding follows the typical tractography representation [57,58]: red for right-left streamlines, green for anterior-posterior, and blue for inferior-superior.
Figure 3.
Representation of the tractography-reconstructed main tracts supporting motor, language, and cognitive (within the limbic system) functions. The represented motor pathways included the cortico-spinal tract, cerebellar peduncles, frontal aslant tract, and motor corpus callosum; language pathways included the arcuate fasciculus, superior longitudinal fasciculus, inferior fronto occipital fasciculus, uncinate fasciculus, inferior longitudinal fasciculus, frontal aslant tract; and limbic pathways included the cingulum bundle, fornix, and middle temporal tract. Template tracts were selected from the KUL-FWT atlas [56]. The color encoding follows the typical tractography representation [57,58]: red for right-left streamlines, green for anterior-posterior, and blue for inferior-superior.
The quantitative measures reported fall into three broad categories:
3.4. Imaging Timepoints
Preoperative DTI was performed in all the studies. Early postoperative imaging, ranging from postoperative day 1 to approximately 6 weeks, is generally used to relate acute tract changes to new neurological deficits [21,24,43,44,47]. Longitudinal follow-up spanned from 3 months to over one year, particularly in glioma and temporal lobe epilepsy populations, and in iNPH cohorts assessed before and after shunting [39,41,46].
3.5. Predictive Value for Motor Function Outcomes
Motor outcomes represented the largest evidence base across the included studies. DTI-based approaches predominantly quantified corticospinal tract (CST) integrity using fractional anisotropy (FA) (often expressed as a side-to-side ratio), diffusivity measures (ADC/MD, RD, AD), and—in a smaller subset—DTI tractography–derived indices such as fiber/streamline-count metrics (e.g., NF index, NFidx) and tract “disconnection severity.” These measures were then related to (i) baseline motor status, (ii) early postoperative motor deficits and their persistence, or (iii) recovery trajectories, including recovery from supplementary motor area (SMA) syndrome.
3.5.1. Preoperative DTI-Derived CST Integrity Predicting Postoperative Motor Deficits
In a retrospective analysis by Ivren et al. (2023), a study of 203 patients with motor-eloquent gliomas examined the postoperative motor outcomes. Postoperatively, 57.1% of patients had no new deficits, 24.1% developed transient deficits, and 18.8% developed permanent deficits. Their diffusion analysis showed that lower FA values were linked to higher postoperative motor deterioration, with FA values associated with new transient (OR 3.0, 95% CI 1.5–6.0) and permanent (OR 7.4, 95% CI 2.8–19.5) deficits. Their predictive model reported an AUC of 0.79[26]. Ius et al. (2017) studied 37 LGG patients and introduced the NF index, calculated as (Hcst NF - Tcst NF)/Hcst NF, where NF represents CST fibers in healthy (H) and tumoral (T) hemispheres. In the ROC analysis, the NF index identified temporary postoperative motor deficits with an AUC of 0.92 (95% CI, 0.834–1.000). An NF index of <0.22 indicated an 87.5% probability of no early deficit, while ≥0.22 indicated an 81% probability of deficit. Compared to MEPs, the NF index showed fewer false negatives (13.3%) and high reliability (86.5%). The authors noted that tractography results depend on acquisition choices and should complement other decision tools [49].
3.5.2. Early Postoperative DTI Changes and Longitudinal Monitoring of Motor Recovery
Cepeda et al. (2021) investigated 11 patients with glioma and related early postoperative DTI changes to motor outcomes. They quantified CST/peritumoral DTI metrics bilaterally, focusing on the relative FA (rFA) (ipsilesional/contralesional). In group comparisons, rFA differed across outcome groups (Kruskal–Wallis H = 7.48, p = 0.024, effect size ε² = 0.75), with permanent deficit patients showing the lowest rFA values. For permanent deficit classification, all three patients with permanent motor deficit had rFA ≤ 0.8, achieving 100% sensitivity and 75% specificity. The ROC curve showed an AUC of 0.917. Cepeda et al. concluded that early postoperative DTI, especially rFA, marks persistent motor deficits, noting that postoperative DTI changes reflect surgical effects and microstructural alterations [21].
Figueredo et al. (2024) presented two illustrative cases involving the resection of gliomas in the primary motor area, with CST FA measurements taken preoperatively, immediately postoperatively, and at a 1-year follow-up. In Case 1, the FA values were 0.50, 0.47, and 0.42, whereas in Case 2, the values were 0.49, 0.44, and 0.44. The authors noted that, within this limited sample, changes in DTI-derived parameters, including FA, were not statistically significant at different time points. They positioned the report as a feasibility study and explicitly acknowledged the limitation of a very small sample size, which restricted inference and precluded robust statistical conclusions [22].
Horikawa et al. (2025) presented a detailed case study with serial DTI and functional assessments. They reported that rFA declined below 0.8 on postoperative day 12 and subsequently increased above 0.8 on days 29 and 134, paralleling clinical recovery in strength and dexterity, as documented in their longitudinal assessment. The authors’ conclusions were explicitly limited by the single-patient design and presented primarily as descriptive evidence supporting the need for continued rehabilitation [24].
Liao et al. (2025) compared 104 patients with minor basal ganglia hemorrhage managed with stereotactic surgery plus medical therapy (n = 52) versus medical therapy alone (n = 52). The DTI indices (FA, MD, RD, and AD) were sampled at the posterior limb of the internal capsule at 48 hours and 1 month, alongside motor impairment scores (Fugl–Meyer motor function) and 6 month disability (mRS). At 1 month, FA was higher in the surgery group (0.56 vs 0.51, p < 0.001) and RD was lower (0.42 vs 0.49, p < 0.001); MD was also lower (0.79 vs 0.86, p < 0.001), while AD did not differ significantly. Clinically, at 6 months, the distribution of disability differed between groups, with mRS 0–1 in 75.0% of the surgery group versus 42.3% of the medical group (p < 0.001) [43].
Non-tumor studies have also enriched the evidence-based literature on this topic. In the context of brainstem cavernoma surgery, Yao et al. (2015) identified quantitative correlations between corticospinal tract (CST) integrity and motor deficits in patients. Specifically, the preoperative mean fractional anisotropy (FA) was correlated with preoperative motor deficits (Spearman’s ρ = 0.63, p = 0.014) and postoperative motor outcomes (ρ = 0.69, p = 0.006). Additionally, preoperative apparent diffusion coefficient (ADC) values correlated with postoperative outcomes (ρ = −0.58, p = 0.027) [53]. Furthermore, following stereotactic evacuation of small basal ganglia hemorrhages, Liao et al. demonstrated that higher FA and better CST preservation at one month were associated with higher Fugl–Meyer scores and lower modified Rankin Scale scores at six months compared to patients receiving medical treatment. This suggests that early surgical decompression may provide measurable microstructural benefits detectable by diffusion tensor imaging (DTI) [43].
3.5.3. Supplementary Motor Area Syndrome: Interhemispheric DTI Metrics and Recovery
Oda et al. (2018) studied 11 brain tumor patients with postoperative SMA syndrome, all recovering within 5–30 days. Using DTI tractography, they extracted interhemispheric fibers "between contralateral SMA and ipsilateral primary motor cortex" and defined NFidx as the "number of tracts" connecting these regions. NFidx was higher in the early recovery group (8923.16 ± 1512.04 (early) vs. 4726.40 ± 1789.46 (late), p = 0.002). Tumor volume differed between groups (18.69 ± 12.11 cm³ vs. 47.10 ± 26.83 cm ³ in the early and late groups, respectively (p = 0.028). NFidx > 8000 occurred in 6/7 early recovery and 0/4 late-recovery patients; NFidx < 8000 occurred in 1/7 early recovery and 4/4 late-recovery patients (Fisher exact p = 0.0152). The authors noted the limitations of DTI tractography in tumor settings and described their results as preliminary evidence for DTT-derived indices predicting SMA syndrome recovery [51].
Tuncer et al. (2023) studied 56 patients; 39/56 (69.6%) developed acute SMA syndrome, recovering by 3 months, while 30/56 (54%) showed persistent fine motor deficits at 3 months. They computed tract "disconnection severity" using the HCP842 tractography atlas, defined as the percentage of streamlines intersecting the lesion mask. Robust regression showed that SMA–SMA fiber disconnection severity through the central corpus callosum correlated with longer acute symptom duration (unadjusted β = 1.73, robust SE 0.65, p = 0.01). LASSO logistic regression found M1–M1 fiber disconnection in midposterior corpus callosum associated with persistent deficits (OR 2.02, 95% CI 1.12–3.6, p = 0.02). They noted the limitations of atlas-based disconnection estimates, which may not fully represent individual tract anatomy variability [35].
3.6. Language Outcomes
In the reviewed literature, language-related endpoints were investigated through (i) cohort studies of tumor surgery, primarily glioma, utilizing tract-specific diffusion metrics and/or tractography-derived indices [18,20,36,46,50], and (ii) cohort studies of anterior temporal lobe resection (ATL) for temporal lobe epilepsy (TLE) employing voxelwise diffusion analyses correlated with language performance [44,47]. The most frequently examined pathways included the dorsal (arcuate fasciculus and closely related superior longitudinal fasciculus components) and ventral (inferior fronto-occipital, inferior longitudinal, and uncinate fasciculi) streams. The outcomes assessed encompassed global aphasia measures (e.g., the Western Aphasia Battery), naming, fluency, and sentence repetition.
3.6.1. Dorsal Stream Biomarkers (Arcuate Fasciculus / SLF)
Kinoshita et al. (2014) conducted a study on preoperative tensor-metric prediction of postoperative language recovery in 12 right-handed patients with left-hemisphere supratentorial tumors. This study quantified fractional anisotropy (FA) in the arcuate fasciculus (AF), including a relative FA metric, and evaluated language abilities using the Western Aphasia Battery (WAB) preoperatively and postoperatively. Results showed a positive correlation between preoperative relative AF FA and postoperative improvement in the total WAB score (r = 0.77, p = 0.0056), with significant associations in naming (p = 0.018), reading (p = 0.029), and writing (p = 0.012). Using K-means clustering, patients were categorized into high relative FA (n = 4) and low relative FA (n = 8) groups, with all patients in the high FA group showing improvement, while improvement in the low FA group was less consistent (4/8) [50].
Caverzasi et al. (2016) evaluated language outcomes following glioma surgery using preoperative diffusion imaging and postoperative assessments. Tract status was categorized using an altered fiber tractography density (AFTD) framework and dichotomized into "preserved" versus "affected" for predictive modeling. The arcuate fasciculus (AF) and temporoparietal component of the superior longitudinal fasciculus (SLF-tp) are the key dorsal pathways associated with language deficits. In patients without deficits, AF and SLF-tp were preserved in all cases. In patients with high-grade gliomas and language deficits at discharge, a logistic regression model using AF/SLF-tp tract status predicted persistent deficits at follow-up (p = 0.005), with a sensitivity and positive predictive value of 86% and a specificity and negative predictive value of 75% [18].
Single-case neurosurgical evidence shows the role of dorsal stream tractography in tracking the evolution of postoperative language. Chernoff et al. (2020) documented a case of a 26-year-old right-handed male with left inferior parietal glioma infiltrating the arcuate fasciculus (AF), who underwent awake craniotomy. Probabilistic tractography was used to quantify AF integrity compared to healthy controls using leave-one-out masking and normalized streamline counts. Postoperatively, the left AF streamline count decreased to 106, four standard deviations below the control mean (t51 = 3.79, p < .0004), while right-hemisphere counts remained within one standard deviation. The patient experienced severe postoperative aphasia that resolved within a week, leaving her with sentence repetition impairment. The sentence repetition accuracy was 94% preoperatively, 72.2% at 1 month, and 90% at 3.5 months, with a decrease at 1 month and an increase at 3.5 months. Methodological caveats included streamline count interpretation issues related to acquisition choices and confounding factors, such as edema [20].
3.6.2. Ventral Stream Biomarkers (IFOF / ILF / UF)
Tomasino et al. (2024) provided extensive cohort evidence linking diffusion metrics to postoperative language performance in 30 patients with left temporoinsular diffuse low-grade gliomas. Language assessments were conducted preoperatively, one week postoperatively, and four months postoperatively. The study evaluated inferior fronto-occipital fasciculus (IFOF) microstructural indices (FA, MD, AD, RD) and tractography indices. Postoperatively, many patients showed performance below normative cutoffs on language tasks (56% for noun naming and 64% for verb naming), with some impairments persisting at follow-up (24% and 44%, respectively). Changes in verb naming correlated with left IFOF voxel count (ρ = 0.541, p = 0.005) and right IFOF streamlines (ρ = 0.501, p = 0.011), as well as right IFOF AD (ρ = 0.631, p < 0.001) and MD (ρ = 0.414, p = 0.049). At follow-up, verb naming remained associated with left hemisphere indices and bilateral diffusivity metrics. Discriminative analysis showed that early postoperative streamline reduction above 79% identified patients with immediate lexico-semantic disorder (AUC: 0.875, sensitivity: 88.9%, specificity: 81.2%). The study found left-right IFOF asymmetries and differences based on radiological patterns, although tract-based measures depended on modeling choices [46].
Evidence regarding the inferior longitudinal fasciculus (ILF) and its impact on naming outcomes has been predominantly obtained from neurosurgical observations. Shinoura et al. (2010) documented a case in which diffusion tensor imaging (DTI) fiber tracking indicated an interruption of the left ILF, which was associated with a significant postoperative decline in object naming ability (with scores decreasing from 80 to 27), while other language functions remained unaffected. In the same study, longitudinal diffusion/tractography analysis of the ILF revealed a reduction in tract extent, quantified as a 35.4% decrease in the number of voxels within the tract, along with alterations in diffusion-derived properties, specifically increases in mean fractional anisotropy (FA) and axial diffusivity (AD) postoperatively for the remaining tract voxels.[31]
3.6.3. Diffusion Correlates of Fluency and Naming
Two cohort studies examining anterior temporal lobectomy (ATL) for temporal lobe epilepsy (TLE) linked postoperative language performance to diffusion tensor metrics using voxel-wise methods. Yogarajah et al. (2010) studied 46 ATL patients (26 left, 20 right) with pre-and postoperative diffusion imaging, using tract-based spatial statistics to identify diffusion changes and correlate them with neuropsychological assessments. In the left ATL cohort, they found an increased fractional anisotropy (FA) of 8% and parallel diffusivity of 6% in contralateral pathways, including the internal/external capsule and superior longitudinal fasciculus/corona radiata. These increases correlated with verbal fluency (FA: r = 0.48, p = 0.009; parallel diffusivity: r = 0.47, p = 0.009) and object naming (FA: r = 0.46, p = 0.027; parallel diffusivity: r = 0.52, p = 0.008) scores. The authors noted that postoperative diffusion changes cannot be attributed to a single biological process [47].
Pustina et al. (2014) studied diffusion and language outcomes in 26 anterior temporal lobectomy patients (11 left TLE, 15 right TLE) versus controls. Diffusion data were acquired at 3T with 32 directions (b = 850), analyzing fractional anisotropy (FA) across the preoperative and one-year postoperative periods. In left ATL patients, preoperative phonemic fluency correlated with FA values in postoperative FA-increase clusters in the left superior corona radiata (r = 0.73, p = 0.03), right superior longitudinal fasciculus (SLF) (r = 0.70, p = 0.02), and right uncinate fasciculus (r = 0.64, p = 0.05). Postoperative phonemic and semantic fluency correlated with FA in the right SLF cluster (r = 0.66, p = 0.04; r = 0.74, p = 0.02). The authors noted that the small sample size limited their ability to explain FA changes [44].
Chernoff et al. (2018) also offered diffusion-based quantification of the frontal aslant tract (FAT) in a glioma case that exhibited changes in speech production, such as a reduced mean length of utterance and altered timing measures. For the left FAT, the study presented pre/post tract diffusion metrics across various tract probability thresholds. While the mean FA showed no significant difference at several thresholds (e.g., threshold 5%: 0.55 ± 0.06 vs 0.56 ± 0.07; p = 0.26), there were significant decreases in mean diffusivity (e.g., 0.99 ± 0.13 vs 0.90 ± 0.11; p = 1.73E−16), radial diffusivity (0.66 ± 0.10 vs 0.57 ± 0.08; p = 1.73E−25), and axial diffusivity (1.66 ± 0.21 vs 1.57 ± 0.19; p = 2.42E−07) at the same threshold [19].
3.7. Higher Cognitive Function Outcomes
Three studies assessed higher cognitive functioning in relation to diffusion tensor imaging (DTI)-derived microstructural metrics, primarily focusing on FA and/or MD, across different neurosurgical populations, including glioma resection, moyamoya disease (MMD) revascularization, and shunt surgery for idiopathic normal-pressure hydrocephalus (iNPH). Across these studies, the pathways examined overlapped around fronto-parietal association tracts (SLF) and fronto-temporal/limbic pathways (e.g., uncinate/cingulate–cingulum and callosal regions), although there was considerable heterogeneity in the study design and endpoints.
In the glioma cohort (n=79), Andreoli et al. extracted the FA and streamline number of 13 bilateral tracts (AF segments, SLF I/II/III, CST, FAT, UF, ILF, IFOF, fornix, and cingulum) and explored tract–cognition relationships using extensive univariate regression modeling, followed by a second model set additionally adjusted for age, given the linear age-related decline in FA and cognition. A consistent pattern in the age-adjusted results showed that FA in long association tracts (particularly the IFOF, ILF, and SLF subcomponents) was linked to memory, visuospatial ability, processing speed, and executive language tasks. In contrast, CST, FAT, UF, and fornix showed no age-adjusted associations with neuropsychological tests in this dataset[38].
In a longitudinal revascularization cohort of adult MMD (n = 25), Kazumata et al. reported the results of multimodal MRI and neuropsychological assessments conducted at baseline and again 2–4 years postoperatively. Postoperative improvement was noted primarily in performance- and speed-related domains, alongside voxel-wise TBSS evidence of postoperative FA increases and MD decreases, including reported changes in the SLF (bilateral FA increases and MD decrease) and FA increases in the left IFOF [41].
Finally, in a prospective iNPH shunt cohort (n = 32; abstract-only), Bubeníková et al. (2025) examined whether DTI metrics tracked clinical improvement after shunt surgery. Within 1 year of shunt placement, improvements in memory and psychomotor speed were reported to correlate with DTI measures in the cingulate gyrus, uncinate fasciculus, superior longitudinal fasciculus (SLF), and corpus callosum, with FA and MD trending toward more physiological values [39].
4. Discussion
Across 37 heterogeneous studies spanning tumor, epilepsy, vascular, and hydrocephalus surgeries, quantitative diffusion tensor imaging (DTI) metrics were consistently associated with postoperative neurological deficits and recovery trajectories. A unifying concept across indications is that diffusion-derived measures act as proxies for tract and network "structural reserve": lower preoperative integrity and greater perioperative disruption generally track with higher functional vulnerability [29,34,38,42,45,48,49,54], whereas longitudinal changes reflect a mixture of injury, decompression, and neuroplastic reorganization [21,23,24,41]. At the same time, the available evidence is dominated by single-center observational cohorts with substantial variation in acquisition, processing, tract definition, and outcome ascertainment, which limits the portability of any single numeric cutoff and supports the interpretation of DTI metrics as risk markers to be integrated with clinical and mapping data rather than as stand-alone decision rules.
4.1. Summary of Findings
Motor outcomes provide the largest and most coherent evidence. In cohorts of patients with glioma, hemorrhage, and brainstem surgery, lower preoperative corticospinal tract (CST) fractional anisotropy (FA) (often expressed as an ipsilesional-to-contralesional ratio) and higher diffusivity were repeatedly associated with a higher probability of new postoperative weakness and reduced likelihood of complete recovery. Several studies have additionally reported promising discrimination using tractography-derived indices (e.g., fiber/streamline reduction metrics), with good-to-excellent AUC values in selected cohorts; however, these measures are intrinsically sensitive to tracking parameters and perilesional signal changes [21,22,24,29,42,43,49]. For supplementary motor area (SMA) syndrome, the limited available data suggest that interhemispheric motor connectivity (callosal SMA-SMA and M1-M1 fibers) influences both symptom duration and the persistence of fine motor deficits, aligning with a network-disconnection framework rather than a single-tract model [35,51].
For language, the evidence is smaller and more varied, yet it similarly supports a tract-reserve interpretation: outcomes frequently implicate the dorsal stream (AF/SLF), and across different cohorts and cases, tract integrity/status is associated with postoperative aphasia severity and recovery. Notably, several studies caution that postoperative diffusion changes cannot be solely attributed to a single biological process, which limits mechanistic inference, even when clinical correlations are observed [18,20,50].
For higher cognition, the evidence remains sparse, but the available studies point toward long association and limbic pathways (e.g., SLF, IFOF/ILF, cingulum, and callosal segments), and in some datasets, network-level measures as candidate prognostic targets. This is biologically plausible: unlike motor function, many cognitive outcomes are distributed, and tract-level metrics may need to be contextualized within the connectome organization and preoperative cognitive reserve [60,61,62]. Importantly, the current literature in these domains is insufficient to define which diffusion features add independent value beyond age, lesion burden, and baseline neuropsychological performance [38,41].
4.2. Comparison with Stroke Literature
When compared with the stroke DTI biomarker literature, the conceptual parallels are strong (especially for CST-based motor prognostication); however, neurosurgical translation is not straightforward. Neurosurgical cohorts combine chronic, often infiltrative pathology with planned tissue disruption, perioperative edema, resection cavities, and susceptibility artifacts that can bias both tensor metrics and tractography. Moreover, functional mapping and surgical strategy are themselves determinants of outcome, introducing confounding factors. [1]. The most transferable lesson from stroke is methodological rather than biological: prognostic utility increases when diffusion features are prespecified, combined with clinical predictors in multivariable models, and tested with external validation and calibration rather than being reported as isolated correlations or center-specific cut-off points [12].
4.3. Methodological Factors Explaining Heterogeneity
Several methodological factors likely explain the wide range of reported thresholds and effect sizes. Diffusion acquisition varied markedly (field strength, number of directions, b-values, and availability of distortion-correction data), and preprocessing was inconsistently described. Because perilesional and postoperative tissues are particularly vulnerable to motion, susceptibility, and partial volume effects, differences in correction strategies (eddy current, susceptibility and bias-field correction, and brain extraction) can materially influence FA and diffusivity estimates [1,12,21,38,63,64].
Heterogeneity in tract definition is an equally important source of non-portability of DTI. Many studies have relied on manual or semi-manual region-of-interest placement and deterministic tracking with low FA cutoffs, which can inflate the apparent disruption in edematous or infiltrated tissue [65]. Conversely, aggressive thresholds can prematurely terminate the streamlines and underestimate the residual fibers. Tractography-derived metrics, such as streamline count or tract volume, are intuitive, but they are not direct quantitative measures of axon number and are strongly algorithm- and parameter-dependent [66]. Across studies, relative or within-subject metrics (e.g., hemispheric ratios, along-tract sampling, or change-from-baseline) appear more robust than absolute values and may be better candidates for harmonization than absolute values.
Finally, clinical and statistical heterogeneity was substantial. Outcome definitions ranged from bedside motor grading to detailed neuropsychological batteries, and follow-up windows varied from discharge to more than one year. Many reports were underpowered, relied on univariate testing, and seldom evaluated whether DTI features added incremental prognostic value beyond established predictors (baseline deficit, tumor grade, lesion volume, distance-to-tract, and intraoperative mapping or neurophysiology). External validation is rare, raising the likelihood that some published cutoffs represent optimistic and sample-specific estimates.
4.4. Strengths and Limitations of the Current Evidence
The main strength of this review is the cross-indication synthesis, which shows that tract- and network-level diffusion features repeatedly map onto clinically meaningful postoperative phenotypes, supporting biological plausibility and clinical relevance. In addition, the literature increasingly includes early postoperative and longitudinal imaging, which is essential for distinguishing pre-existing vulnerability from perioperative changes and recovery-related remodeling.
However, the evidence base has some notable limitations. Most studies were single-center and heavily weighted toward glioma surgery, with comparatively few epilepsy, vascular, and cerebrospinal fluid disorder cohorts, limiting generalizability to epilepsy surgery populations and minimally invasive approaches. Imaging and analysis pipelines were heterogeneous and frequently incompletely reported, and formal risk-of-bias assessment and publication-bias evaluation were challenging in this setting. These factors, together with the narrative synthesis necessitated by heterogeneity, mean that the present conclusions should be viewed as hypothesis-shaping and clinically suggestive rather than definitive for patient-level decision making.
4.5. Implications for Clinical Practice and Future Directions
From a clinical standpoint, quantitative DTI can be positioned as a complementary tool with three practical roles. First, preoperative tract integrity metrics (especially CST ratios for motor and AF/IFOF integrity for language) may help stratify functional risk, prioritize patients for awake mapping or more extensive intraoperative monitoring, and frame counseling regarding the likelihood and expected time course of recovery. Second, when new deficits occur, early postoperative diffusion changes, interpreted cautiously and ideally in relation to preoperative baselines and the contralateral hemisphere, may support a differential prognosis between transient perioperative effects and more severe structural injury. Third, longitudinal diffusion measures and connectomics can provide objective markers of structural reorganization that can be integrated with rehabilitation planning, including in epilepsy surgery patients with language or memory concerns.
To move from association to clinically deployable prognostication, future work should prioritize (i) harmonized acquisition with distortion correction and transparent quality control; (ii) standardized, anatomically explicit tract definitions or tractometry pipelines with reproducible parameters; (iii) common outcome sets with prespecified time points (e.g., early postoperative and 3- to 6-month follow-up); (iv) multivariable prediction modeling that tests incremental value over clinical and mapping data; (v) external validation across centers and scanners with calibration and clinical-utility analyses; and (vi) reporting aligned with established prediction-model and imaging-biomarker guidance. Multicenter prospective studies that include epilepsy surgery cohorts and leverage modern diffusion methods (while maintaining compatibility with DTI-derived metrics) will be particularly important for defining which biomarkers are robust enough to inform patient-specific counseling in the future. With these steps, quantitative diffusion metrics can evolve from descriptive adjuncts to reliable components of individualized surgical planning and postoperative care.
5. Conclusions
In conclusion, across diverse neurosurgical indications, quantitative DTI provides clinically meaningful markers of white matter integrity that are consistently associated with postoperative motor and language outcomes and show promise for cognitive and gait domains. The strongest and most reproducible evidence supports CST-based FA and diffusivity asymmetry as correlates of postoperative weakness and recovery, while language outcomes appear to depend on the integrity of the dorsal (AF/SLF) and ventral (IFOF/ILF/UF) pathways and on distributed network reorganization after resection, including in ATL cohorts for temporal lobe epilepsy. At present, heterogeneity in acquisition, tract definition, outcome ascertainment, and statistical validation precludes universal thresholds and argues against stand-alone prognostic use. Progress toward clinical translation will require harmonized pipelines, rigorous prospective multicenter validation, and integrated models that combine diffusion features with clinical variables, lesion characteristics, and functional mapping or neurophysiology. Such efforts would clarify the role of diffusion biomarkers in epilepsy and neurosurgical practice, enabling more accurate risk counseling and better-targeted rehabilitation.
Author Contributions
Conceptualization, N.B.D.; methodology, N.B.D.; validation, G. S., V.R.; formal analysis, N.B.D.; investigation, N.B.D. and G.S.; resources, N.B.D.; data curation, N.B.D.; writing—original draft preparation, N.B.D.; review and editing, G.S., V.R.; visualization, G.G, F.F. S.C.; supervision, A.C., C.T., R.L.; project administration, A.C. All authors have read and agreed to the published version of this manuscript.
Funding
This research received no external funding.
Declaration of generative AI and AI-assisted technologies in the manuscript preparation process
During the preparation of this work, the author used Open-Paperpal for grammar and spell-checking. After using this tool, the author reviewed and edited the content as needed and took full responsibility for the content of published articles.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries should be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript.
| Abbreviation | Full term | |
| AD | Axial diffusivity | |
| ADC | Apparent diffusion coefficient | |
| AF | Arcuate fasciculus | |
| AFTD | Altered fiber tractography density | |
| ATL | Anterior temporal lobectomy | |
| AUC | Area under the curve | |
| CI | Confidence interval | |
| CST | Corticospinal tract | |
| dMRI | Diffusion magnetic resonance imaging | |
| DSI | Diffusion spectrum imaging | |
| DTI | Diffusion tensor imaging | |
| FA | Fractional anisotropy | |
| FAT | Frontal aslant tract | |
| FLAIR | Fluid-attenuated inversion recovery | |
| FSL | FMRIB Software Library | |
| HCP | Human Connectome Project | |
| IFOF | Inferior fronto-occipital fasciculus | |
| ILF | Inferior longitudinal fasciculus | |
| iNPH | Idiopathic normal-pressure hydrocephalus | |
| LGG | Low-grade glioma | |
| MD | Mean diffusivity | |
| MEP | Motor evoked potential | |
| MMD | Moyamoya disease | |
| MRI | Magnetic resonance imaging | |
| mRS | Modified Rankin Scale | |
| NF | Number of fibers | |
| NFidx | Fiber number index | |
| OR | Odds ratio | |
| RD | Radial diffusivity | |
| ROC | Receiver operating characteristic | |
| ROI | Region of interest | |
| rFA | Relative fractional anisotropy | |
| SLF | Superior longitudinal fasciculus | |
| SMA | Supplementary motor area | |
| TBSS | Tract-based spatial statistics | |
| TLE | Temporal lobe epilepsy | |
| UF | Uncinate fasciculus | |
| WAB | Western Aphasia Battery | |
| WHO | World Health Organization | |
References
- Wende, T.; Hoffmann, K.-T.; Meixensberger, J. Tractography in Neurosurgery: A Systematic Review of Current Applications. J Neurol Surg A Cent Eur Neurosurg 2020, 81, 442–455. [Google Scholar] [CrossRef]
- Jeurissen, B.; Descoteaux, M.; Mori, S.; Leemans, A. Diffusion MRI Fiber Tractography of the Brain. NMR in Biomedicine 2019, 32, e3785. [Google Scholar] [CrossRef]
- Alstott, J.; Breakspear, M.; Hagmann, P.; Cammoun, L.; Sporns, O. Modeling the Impact of Lesions in the Human Brain. PLoS Comput Biol 2009, 5, e1000408. [Google Scholar] [CrossRef]
- Mukherjee, P.; Berman, J.I.; Chung, S.W.; Hess, C.P.; Henry, R.G. Diffusion Tensor MR Imaging and Fiber Tractography: Theoretic Underpinnings. AJNR Am J Neuroradiol 2008, 29, 632–641. [Google Scholar] [CrossRef] [PubMed]
- Alexander, A.L.; Lee, J.E.; Lazar, M.; Field, A.S. Diffusion Tensor Imaging of the Brain. Neurotherapeutics 2007, 4, 316–329. [Google Scholar] [CrossRef]
- O’Donnell, L.J.; Westin, C.-F. An Introduction to Diffusion Tensor Image Analysis. Neurosurgery Clinics of North America 2011, 22, 185–196. [Google Scholar] [CrossRef] [PubMed]
- Colby, J.B.; Soderberg, L.; Lebel, C.; Dinov, I.D.; Thompson, P.M.; Sowell, E.R. Along-Tract Statistics Allow for Enhanced Tractography Analysis. NeuroImage 2012, 59, 3227–3242. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, L.J.; Westin, C.-F. An Introduction to Diffusion Tensor Image Analysis. Neurosurgery Clinics of North America 2011, 22, 185–196. [Google Scholar] [CrossRef]
- Harris, N.G.; Verley, D.R.; Gutman, B.A.; Sutton, R.L. Bi-Directional Changes in Fractional Anisotropy after Experiment TBI: Disorganization and Reorganization? NeuroImage 2016, 133, 129–143. [Google Scholar] [CrossRef]
- Jones, D.K.; Knösche, T.R.; Turner, R. White Matter Integrity, Fiber Count, and Other Fallacies: The Do’s and Don’ts of Diffusion MRI. Neuroimage 2013, 73, 239–254. [Google Scholar] [CrossRef]
- Manan, A.A.; Yahya, N.A.; Taib, N.H.M.; Idris, Z.; Manan, H.A. The Assessment of White Matter Integrity Alteration Pattern in Patients with Brain Tumor Utilizing Diffusion Tensor Imaging: A Systematic Review. Cancers 2023, 15, 3326. [Google Scholar] [CrossRef]
- Moura, L.M.; Luccas, R.; Paiva, J.P.Q.D.; Amaro, E.; Leemans, A.; Leite, C.D.C.; Otaduy, M.C.G.; Conforto, A.B. Diffusion Tensor Imaging Biomarkers to Predict Motor Outcomes in Stroke: A Narrative Review. Front. Neurol. 2019, 10, 445. [Google Scholar] [CrossRef]
- Ng, S.; Duffau, H. Brain Plasticity Profiling as a Key Support to Therapeutic Decision-Making in Low-Grade Glioma Oncological Strategies. Cancers 2023, 15, 3698. [Google Scholar] [CrossRef]
- Costabile, J.D.; Alaswad, E.; D’Souza, S.; Thompson, J.A.; Ormond, D.R. Current Applications of Diffusion Tensor Imaging and Tractography in Intracranial Tumor Resection. Front. Oncol. 2019, 9, 426. [Google Scholar] [CrossRef]
- Manan, A.A.; Yahya, N.; Idris, Z.; Manan, H.A. The Utilization of Diffusion Tensor Imaging as an Image-Guided Tool in Brain Tumor Resection Surgery: A Systematic Review. Cancers 2022, 14, 2466. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 Explanation and Elaboration: Updated Guidance and Exemplars for Reporting Systematic Reviews. BMJ 2021, n160. [Google Scholar] [CrossRef]
- Kung, J. Elicit (Product Review). J Can Health Libr Assoc 2023, 44. [Google Scholar] [CrossRef]
- Caverzasi, E.; Hervey-Jumper, S.L.; Jordan, K.M.; Lobach, I.V.; Li, J.; Panara, V.; Racine, C.A.; Sankaranarayanan, V.; Amirbekian, B.; Papinutto, N.; et al. Identifying Preoperative Language Tracts and Predicting Postoperative Functional Recovery Using HARDI Q-Ball Fiber Tractography in Patients with Gliomas. J Neurosurg 2016, 125, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Chernoff, B.L.; Teghipco, A.; Garcea, F.E.; Sims, M.H.; Paul, D.A.; Tivarus, M.E.; Smith, S.O.; Pilcher, W.H.; Mahon, B.Z. A Role for the Frontal Aslant Tract in Speech Planning: A Neurosurgical Case Study. J Cogn Neurosci 2018, 30, 752–769. [Google Scholar] [CrossRef]
- Chernoff, B.L.; Teghipco, A.; Garcea, F.E.; Belkhir, R.; Sims, M.H.; Paul, D.A.; Tivarus, M.E.; Smith, S.O.; Hintz, E.; Pilcher, W.H.; et al. Reorganized Language Network Connectivity after Left Arcuate Fasciculus Resection: A Case Study. Cortex 2020, 123, 173–184. [Google Scholar] [CrossRef] [PubMed]
- Cepeda, S.; García-García, S.; Arrese, I.; Velasco-Casares, M.; Sarabia, R. Acute Changes in Diffusion Tensor-Derived Metrics and Its Correlation with the Motor Outcome in Gliomas Adjacent to the Corticospinal Tract. Surgical Neurology International 2021, 12, 51. [Google Scholar] [CrossRef]
- Figueredo, L.F.; Mejía-Cordovez, J.A.; Gomez-Amarillo, D.A.; Hakim, F.; Pimienta-Redondo, H.D.; Almeida, J.P.; Kehayov, I.; Angelova, P.; Apostolov, G.; Luzzi, S.; et al. Differential Tractography and Whole Brain Connectometry in Primary Motor Area Gliomas Resection: A Feasibility Study. Clinical Neurology and Neurosurgery 2024, 241, 108305. [Google Scholar] [CrossRef] [PubMed]
- Gong, Z.; Zhang, H.; Grziwotz, M.; Krieg, S.; Ille, S. Adaptive Motor Cortex Reorganization Following Surgical Intervention in Tumor-Related Upper Limb Regions. Brain and Spine 2025, 5, 105145. [Google Scholar] [CrossRef]
- Horikawa, Y.; Yuri, T.; Umaba, C.; Yamawaki, R.; Nankaku, M.; Ikeguchi, R.; Arakawa, Y. Motor Recovery in Glioma Patients After Craniotomy: A Case Study of Continuous Rehabilitation Assessed With Diffusion Tensor Imaging. Cureus 2025, 17, e82747. [Google Scholar] [CrossRef]
- Hou, Z.; Cai, X.; Li, H.; Zeng, C.; Wang, J.; Gao, Z.; Zhang, M.; Dou, W.; Zhang, N.; Zhang, L.; et al. Quantitative Assessment of Invasion of High-Grade Gliomas Using Diffusion Tensor Magnetic Resonance Imaging. World Neurosurg 2018, 113, e561–e567. [Google Scholar] [CrossRef]
- Ivren, M.; Grittner, U.; Khakhar, R.; Belotti, F.; Schneider, H.; Pöser, P.; D’Agata, F.; Spena, G.; Vajkoczy, P.; Picht, T.; et al. Comparison of Anatomical-Based vs. nTMS-Based Risk Stratification Model for Predicting Postoperative Motor Outcome and Extent of Resection in Brain Tumor Surgery. Neuroimage Clin 2023, 38, 103436. [Google Scholar] [CrossRef]
- Laundre, B.J.; Jellison, B.J.; Badie, B.; Alexander, A.L.; Field, A.S. Diffusion Tensor Imaging of the Corticospinal Tract before and after Mass Resection as Correlated with Clinical Motor Findings: Preliminary Data. AJNR Am J Neuroradiol 2005, 26, 791–796. [Google Scholar]
- Liu, X.; Zeng, S.; Tao, T.; Yang, Z.; Wu, X.; Zhao, J.; Zhang, N. A Comparative Study of Diffusion Kurtosis Imaging and Diffusion Tensor Imaging in Detecting Corticospinal Tract Impairment in Diffuse Glioma Patients. Neuroradiology 2024, 66, 785–796. [Google Scholar] [CrossRef]
- Martino, J.; Caballero, H.; DE Lucas, E.M.; DA Silva-Freitas, R.; Velasquez, C.; Gomez, E.; Vazquez-Bourgon, J.; Vázquez-Barquero, A. Recovery of Long-Term Paresis Following Resection of WHO Grade II Gliomas Infiltrating the Pyramidal Pathway. J Neurosurg Sci 2017, 61, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Muir, M.; Prinsloo, S.; Michener, H.; Traylor, J.I.; Patel, R.; Gadot, R.; de Almeida Bastos, D.C.; Kumar, V.A.; Ferguson, S.; Prabhu, S.S. TMS Seeded Diffusion Tensor Imaging Tractography Predicts Permanent Neurological Deficits. Cancers (Basel) 2022, 14, 340. [Google Scholar] [CrossRef] [PubMed]
- Shinoura, N.; Suzuki, Y.; Tsukada, M.; Yoshida, M.; Yamada, R.; Tabei, Y.; Saito, K.; Koizumi, T.; Yagi, K. Deficits in the Left Inferior Longitudinal Fasciculus Results in Impairments in Object Naming. Neurocase 2010, 16, 135–139. [Google Scholar] [CrossRef]
- Sierpowska, J.; Gabarrós, A.; Fernandez-Coello, A.; Camins, À.; Castañer, S.; Juncadella, M.; de Diego-Balaguer, R.; Rodríguez-Fornells, A. Morphological Derivation Overflow as a Result of Disruption of the Left Frontal Aslant White Matter Tract. Brain Lang 2015, 142, 54–64. [Google Scholar] [CrossRef]
- Sollmann, N.; Negwer, C.; Ille, S.; Maurer, S.; Hauck, T.; Kirschke, J.S.; Ringel, F.; Meyer, B.; Krieg, S.M. Feasibility of nTMS-Based DTI Fiber Tracking of Language Pathways in Neurosurgical Patients Using a Fractional Anisotropy Threshold. Journal of Neuroscience Methods 2016, 267, 45–54. [Google Scholar] [CrossRef]
- Sollmann, N.; Negwer, C.; Tussis, L.; Hauck, T.; Ille, S.; Maurer, S.; Giglhuber, K.; Bauer, J.S.; Ringel, F.; Meyer, B.; et al. Interhemispheric Connectivity Revealed by Diffusion Tensor Imaging Fiber Tracking Derived from Navigated Transcranial Magnetic Stimulation Maps as a Sign of Language Function at Risk in Patients with Brain Tumors. J Neurosurg 2017, 126, 222–233. [Google Scholar] [CrossRef] [PubMed]
- Tuncer, M.S.; Fekonja, L.S.; Ott, S.; Pfnür, A.; Karbe, A.-G.; Engelhardt, M.; Faust, K.; Picht, T.; Coburger, J.; Dührsen, L.; et al. Role of Interhemispheric Connectivity in Recovery from Postoperative Supplementary Motor Area Syndrome in Glioma Patients. J Neurosurg 2023, 139, 324–333. [Google Scholar] [CrossRef]
- Shinoura, N.; Midorikawa, A.; Onodera, T.; Yamada, R.; Tabei, Y.; Onda, Y.; Itoi, C.; Saito, S.; Yagi, K. The Left Superior Longitudinal Fasciculus within the Primary Sensory Area of Inferior Parietal Lobe Plays a Role in Dysgraphia of Kana Omission within Sentences. Behav Neurol 2012, 25, 363–368. [Google Scholar] [CrossRef]
- Shinoura, N.; Suzuki, Y.; Yamada, R.; Kodama, T.; Takahashi, M.; Yagi, K. Restored Activation of Primary Motor Area from Motor Reorganization and Improved Motor Function after Brain Tumor Resection. AJNR Am J Neuroradiol 2006, 27, 1275–1282. [Google Scholar]
- Andreoli, M.; Mackie, M.-A.; Aaby, D.; Tate, M.C. White Matter Tracts Contribute Selectively to Cognitive Functioning in Patients with Glioma. Front. Oncol. 2023, 13, 1221753. [Google Scholar] [CrossRef] [PubMed]
- Bubeníková, A.; Sedlák, V.; Skalický, P.; Rýdlo, O.; Haratek, K.; Vlasák, A.; Leško, R.; Netuka, D.; Beneš, V.; Beneš, V.; et al. Clinical Improvement after Shunt Surgery in Patients with Idiopathic Normal Pressure Hydrocephalus Can Be Quantified by Diffusion Tensor Imaging. AJNR Am J Neuroradiol 2025, 46, 766–773. [Google Scholar] [CrossRef]
- Drane, D.; Glasser, M.; Voets, N.; Ojemann, J.; Saindane, A.; Loring, D.; Price, M.; Ivanisevic, M.; Phatak, V.; Willie, J.; et al. Key Pathways for Visual Naming and Object Recognition Revealed by Diffusion Tensor Imaging Probabilistic Tractography in Epilepsy Surgery Patients (S43.008). Neurology 2014, 82. [Google Scholar] [CrossRef]
- Kazumata, K.; Tha, K.K.; Tokairin, K.; Ito, M.; Uchino, H.; Kawabori, M.; Sugiyama, T. Brain Structure, Connectivity, and Cognitive Changes Following Revascularization Surgery in Adult Moyamoya Disease. Neurosurg. 2019, 85, E943–E952. [Google Scholar] [CrossRef]
- Khan, K.A.; Jain, S.K.; Sinha, V.D.; Sinha, J. Preoperative Diffusion Tensor Imaging: A Landmark Modality for Predicting the Outcome and Characterization of Supratentorial Intra-Axial Brain Tumors. World Neurosurgery 2019, 124, e540–e551. [Google Scholar] [CrossRef]
- Liao, C.; Lu, Z.; Pan, G.; Ye, J.; Nong, S.; Nordin, R.B.; Liang, J.; Fazel, M.F.; Baharin, N.H.Z. Diffusion Tensor Imaging Assessments to Investigate Motor Impairment Recovery after Minor Basal Ganglia Hemorrhage Post-Stereotactic Surgery. Front. Neurosci. 2025, 19, 1526910. [Google Scholar] [CrossRef] [PubMed]
- Pustina, D.; Doucet, G.; Evans, J.; Sharan, A.; Sperling, M.; Skidmore, C.; Tracy, J. Distinct Types of White Matter Changes Are Observed after Anterior Temporal Lobectomy in Epilepsy. PLoS ONE 2014, 9, e104211. [Google Scholar] [CrossRef] [PubMed]
- Roth, A.; Buttrick, S.S.; Cajigas, I.; Jagid, J.R.; Ivan, M.E. Accuracy of Frame-Based and Frameless Systems for Deep Brain Stimulati on: A Meta-Analysis. Journal of Clinical Neuroscience 2018, 57, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Tomasino, B.; Baiano, C.; Ricciardi, G.K.; Maieron, M.; Romano, A.; Guarracino, I.; Isola, M.; De Martino, M.; D’Agostini, S.; Bagatto, D.; et al. A Longitudinal Multimodal Imaging Study in Patients with Temporo-Insular Diffuse Low-Grade Tumors: How the Inferior Fronto-Occipital Fasciculus Provides Information on Cognitive Outcomes. Current Oncology 2024, 31, 8075–8093. [Google Scholar] [CrossRef]
- Yogarajah, M.; Focke, N.K.; Bonelli, S.B.; Thompson, P.; Vollmar, C.; McEvoy, A.W.; Alexander, D.C.; Symms, M.R.; Koepp, M.J.; Duncan, J.S. The Structural Plasticity of White Matter Networks Following Anterior Temporal Lobe Resection. Brain 2010, 133, 2348–2364. [Google Scholar] [CrossRef]
- Gao, B.; Shen, X.; Shiroishi, M.S.; Pang, M.; Li, Z.; Yu, B.; Shen, G. A Pilot Study of Pre-Operative Motor Dysfunction from Gliomas in the Region of Corticospinal Tract: Evaluation with Diffusion Tensor Imaging. PLoS One 2017, 12, e0182795. [Google Scholar] [CrossRef]
- Ius, T.; Turella, L.; Pauletto, G.; Isola, M.; Maieron, M.; Sciacca, G.; Budai, R.; D’Agostini, S.; Eleopra, R.; Skrap, M. Quantitative Diffusion Tensor Imaging Analysis of Low-Grade Gliomas: From Preclinical Application to Patient Care. World Neurosurg 2017, 97, 333–343. [Google Scholar] [CrossRef]
- Kinoshita, M.; Nakada, M.; Okita, H.; Hamada, J.-I.; Hayashi, Y. Predictive Value of Fractional Anisotropy of the Arcuate Fasciculus for the Functional Recovery of Language after Brain Tumor Resection: A Preliminary Study. Clin Neurol Neurosurg 2014, 117, 45–50. [Google Scholar] [CrossRef]
- Oda, K.; Yamaguchi, F.; Enomoto, H.; Higuchi, T.; Morita, A. Prediction of Recovery from Supplementary Motor Area Syndrome after Brain Tumor Surgery: Preoperative Diffusion Tensor Tractography Analysis and Postoperative Neurological Clinical Course. Neurosurg Focus 2018, 44, E3. [Google Scholar] [CrossRef]
- Stadlbauer, A.; Nimsky, C.; Gruber, S.; Moser, E.; Hammen, T.; Engelhorn, T.; Buchfelder, M.; Ganslandt, O. Changes in Fiber Integrity, Diffusivity, and Metabolism of the Pyramidal Tract Adjacent to Gliomas: A Quantitative Diffusion Tensor Fiber Tracking and MR Spectroscopic Imaging Study. AJNR Am J Neuroradiol 2007, 28, 462–469. [Google Scholar]
- Yao, Y.; Ulrich, N.H.; Guggenberger, R.; Alzarhani, Y.A.; Bertalanffy, H.; Kollias, S.S. Quantification of Corticospinal Tracts with Diffusion Tensor Imaging in Brainstem Surgery: Prognostic Value in 14 Consecutive Cases at 3T Magnetic Resonance Imaging. World Neurosurgery 2015, 83, 1006–1014. [Google Scholar] [CrossRef] [PubMed]
- Sollmann, N.; Wildschuetz, N.; Kelm, A.; Conway, N.; Moser, T.; Bulubas, L.; Kirschke, J.S.; Meyer, B.; Krieg, S.M. Associations between Clinical Outcome and Navigated Transcranial Magnetic Stimulation Characteristics in Patients with Motor-Eloquent Brain Lesions: A Combined Navigated Transcranial Magnetic Stimulation-Diffusion Tensor Imaging Fiber Tracking Approach. J Neurosurg 2018, 128, 800–810. [Google Scholar] [CrossRef]
- Stasenko, A.; Kaestner, E.; Arienzo, D.; Schadler, A.J.; Helm, J.L.; Shih, J.J.; Ben-Haim, S.; McDonald, C.R. Preoperative White Matter Network Organization and Memory Decline after Epilepsy Surgery. Journal of Neurosurgery 2023, 139, 1576–1587. [Google Scholar] [CrossRef] [PubMed]
- Radwan, A.M.; Sunaert, S.; Schilling, K.; Descoteaux, M.; Landman, B.A.; Vandenbulcke, M.; Theys, T.; Dupont, P.; Emsell, L. An Atlas of White Matter Anatomy, Its Variability, and Reproducibility Based on Constrained Spherical Deconvolution of Diffusion MRI. NeuroImage 2022, 254, 119029. [Google Scholar] [CrossRef]
- Sandgaard, A.D.; Shemesh, N.; Østergaard, L.; Kiselev, V.G.; Jespersen, S.N. The Larmor Frequency Shift of a White Matter Magnetic Microstructure Model with Multiple Sources. NMR in Biomedicine 2024, 37, e5150. [Google Scholar] [CrossRef]
- Eriksson, S.; Lasič, S.; Nilsson, M.; Westin, C.-F.; Topgaard, D. NMR Diffusion-Encoding with Axial Symmetry and Variable Anisotropy: Distinguishing between Prolate and Oblate Microscopic Diffusion Tensors with Unknown Orientation Distribution. The Journal of Chemical Physics 2015, 142, 104201. [Google Scholar] [CrossRef]
- Jeong, J.; Asano, E.; Juhász, C.; Behen, M.E.; Chugani, H.T. Postoperative Axonal Changes in the Contralateral Hemisphere in Children with Medically Refractory Epilepsy: A Longitudinal Diffusion Tensor Imaging Connectome Analysis. Human Brain Mapping 2016, 37, 3946–3956. [Google Scholar] [CrossRef] [PubMed]
- Sarwar, T.; Tian, Y.; Yeo, B.T.T.; Ramamohanarao, K.; Zalesky, A. Structure-Function Coupling in the Human Connectome: A Machine Learning Approach. NeuroImage 2020, 226, 117609. [Google Scholar] [CrossRef]
- Corriveau, A.; Chun, M.M.; Rosenberg, M.D.; Yoo, K.; Kwon, Y.H. Functional Connectome Stability and Optimality Are Markers of Cognitive Performance. Cerebral Cortex 2022, 33, 5025–5041. [Google Scholar] [CrossRef] [PubMed]
- Amico, E.; Arenas, A.; Goñi, J. Centralized and Distributed Cognitive Task Processing in the Human Connectome. Network Neuroscience 2019, 3, 455–474. [Google Scholar] [CrossRef] [PubMed]
- A., S.; C., N.; S., G.; E., M.; T., H.; T., E.; M., B.; O., G. Changes in Fiber Integrity, Diffusivity, and Metabolism of the Pyramidal Tract Adjacent to Gliomas: A Quantitative Diffusion Tensor Fiber Tracking and MR Spectroscopic Imaging Study. AJNR. American journal of neuroradiology 2007. [Google Scholar]
- Curran, K.M.; Emsell, L.; Leemans, A. Quantitative DTI Measures. In Diffusion Tensor Imaging; Van Hecke, W., Emsell, L., Sunaert, S., Eds.; Springer New York: New York, NY, 2016; pp. 65–87. ISBN 978-1-4939-3117-0. [Google Scholar]
- Van Westen, D.; Lätt, J.; Englund, E.; Brockstedt, S.; Larsson, E.-M. Tumor Extension in High-Grade Gliomas Assessed with Diffusion Magnetic Resonance Imaging: Values and Lesion-to-Brain Ratios of Apparent Diffusion Coefficient and Fractional Anisotropy. Acta Radiol 2006, 47, 311–319. [Google Scholar] [CrossRef]
- Jordan, K.M.; Amirbekian, B.; Keshavan, A.; Henry, R.G. Cluster Confidence Index: A Streamline-Wise Pathway Reproducibility Metric for Diffusion-Weighted MRI Tractography. Journal of Neuroimaging 2018, 28, 64–69. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Example of whole-brain voxel-wise maps of diffusion tensor imaging metrics. MD, mean diffusivity; AD, axial diffusivity; RD, radial diffusivity; FA, fractional anisotropy.
Figure 1.
Example of whole-brain voxel-wise maps of diffusion tensor imaging metrics. MD, mean diffusivity; AD, axial diffusivity; RD, radial diffusivity; FA, fractional anisotropy.
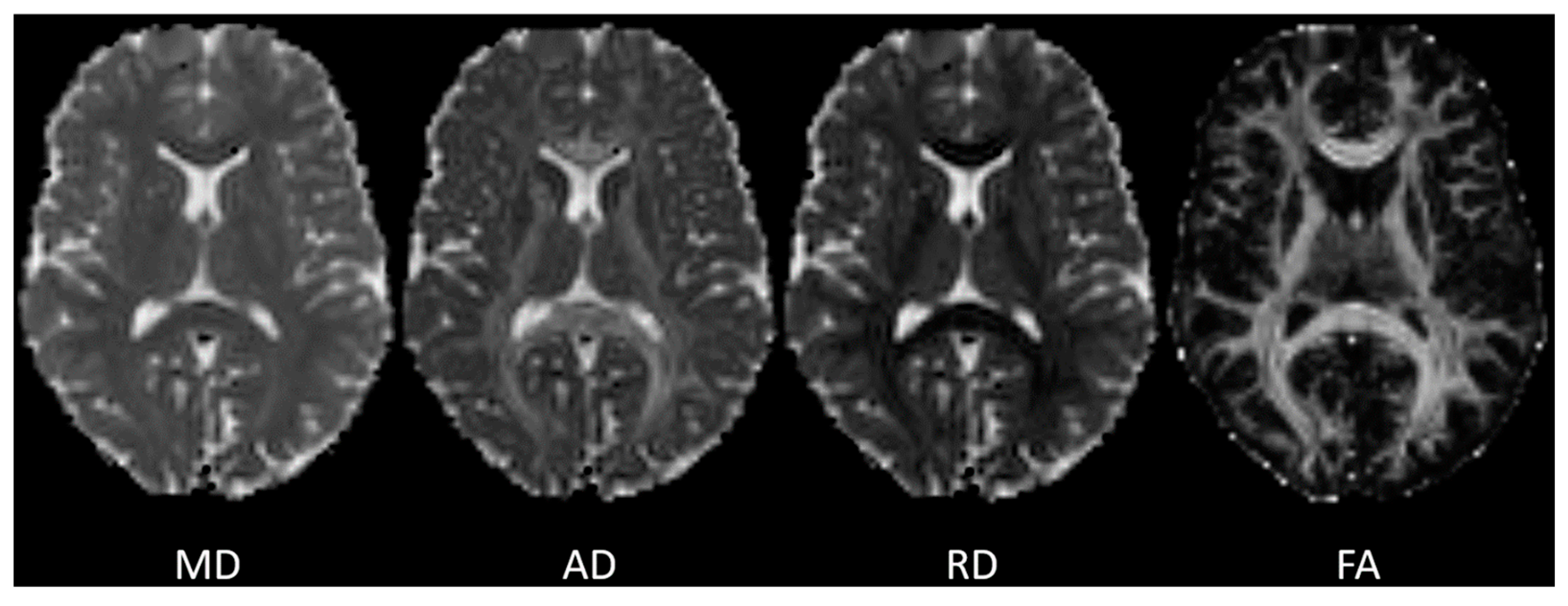
Figure 2.
PRISMA flow diagram of the literature search and selection of relevant studies.
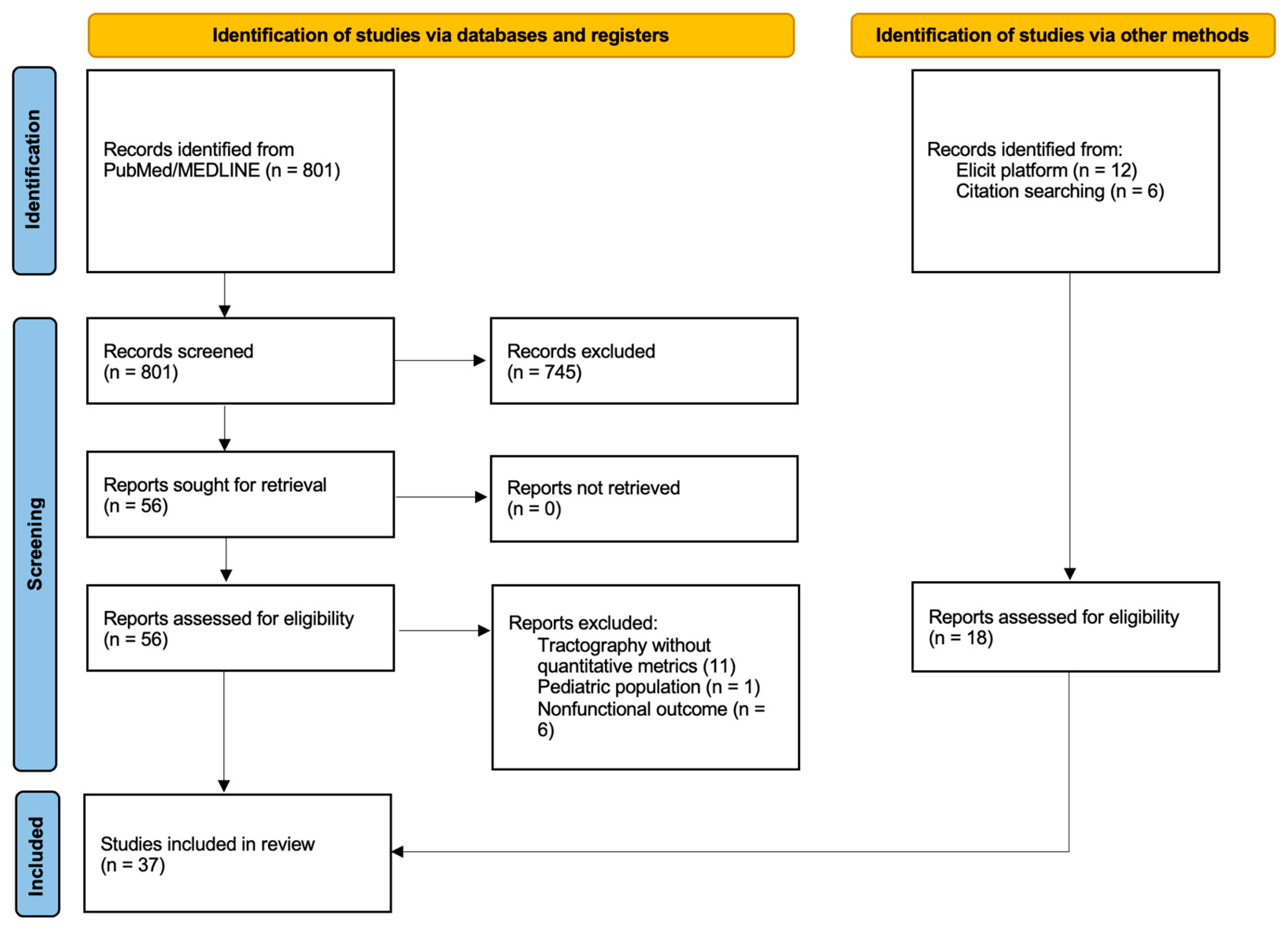

Table 1.
General characteristics of the 37 included studies.
| Study (year) | Condition / surgery type | Primary functional domain |
|---|---|---|
| Gong et al. (2025) | Motor-eloquent gliomas | Motor |
| Horikawa et al. (2025) | Recurrent glioma patient | Motor |
| Roth et al. (2025) | Gliomas near CST | Motor |
| Figueredo et al. (2024) | Primary motor-area gliomas | Motor |
| Liu et al. (2024) | WHO II/IV gliomas near CST | Motor |
| Ivren et al. (2023) | Motor-area gliomas | Motor |
| Tuncer et al. (2023) | SMA gliomas | Motor |
| Muir et al. (2022) | Motor-eloquent gliomas | Motor |
| Cepeda et al. (2021) | Gliomas ≤2 cm from CST | Motor |
| Laundre et al. (2005) | Mass lesions incl. glioma | Motor |
| Khan et al. (2019) | Mixed supratentorial intra-axial tumors | Motor |
| Oda et al. (2018) | SMA tumors | Motor |
| Sollmann et al. (2018) | Motor-eloquent gliomas | Motor |
| Gao et al. (2017) | Gliomas near CST | Motor |
| Martino et al. (2017) | LGG with long-term paresis | Motor |
| Sollmann et al. (2017) | Eloquent brain tumors (mixed) | Motor |
| Ius et al. (2016) | LGGs involving the CST | Motor |
| Hou et al. (2015) | Gliomas adjacent to PT | Motor |
| Liao et al. (2025) | Basal ganglia hemorrhage surgery | Motor |
| Shinoura et al. (2006) | Metastatic brain tumor resection | Motor |
| Stadlbauer et al. (2007) | Gliomas near CST | Motor |
| Yao et al. (2015) | Brainstem surgery | Motor |
| Shinoura et al. (motor) (2006) | Gliomas near M1 | Motor |
| Drane et al. (2014) | Temporal lobe epilepsy surgery | Language |
| Chernoff et al. (2020) | Left parietal glioma | Language |
| Tomasino (2020) | Glioma near AF | Language |
| Chernoff et al. (2018) | Frontal glioma resection | Language |
| Caverzasi et al. (2016) | Language-eloquent gliomas | Language |
| Sollmann et al. (language) (2016) | Perisylvian gliomas | Language |
| Sierpowska et al. (2015) | Left frontal glioma | Language |
| Pustina et al. (2014) | Adult ATL for TLE | Language |
| Kinoshitaa et al. (2014) | Language recovery after tumor resection | Language |
| Shinoura et al. (language) (2009) | Temporal glioma | Language |
| Yogarajah et al. (2010) | Adult ATL for temporal lobe epilepsy | Language |
| Andreoli et al. (2023) | Glioma patients | Cognitive |
| Kazumata et al. (2019) | Adult Moyamoya revascularization | Cognitive |
| Bubeníková et al. (2025) | Idiopathic NPH shunt surgery | Cognition/gait |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



