
Submitted:
25 December 2025
Posted:
25 December 2025
You are already at the latest version
Abstract
Background: Anterior cruciate ligament (ACL) reconstruction is a common orthopedic procedure, but graft failure remains a significant complication, particularly in young and active individuals. Understanding the multifactorial etiology of failure and optimizing revision strategies are crucial for improving outcomes. Methods: A structured narrative review of the literature was conducted, including studies published from January 2000 to May 2024. Databases searched included PubMed/MEDLINE, Embase, and Google Scholar. Eligible studies addressed definitions, etiology, classification, and surgical management of ACL reconstruction failure. Data were synthesized qualitatively, integrating evidence on technical, biological, and traumatic causes, as well as neuromuscular and psychosocial factors influencing functional outcomes. Results: ACL reconstruction failure is primarily caused by technical errors, particularly tunnel malposition (60–70% of cases), followed by traumatic (15–25%) and biological (10–15%) mechanisms. Failure timing provides diagnostic clues: early (< 3 months) failures often relate to fixation or infection, mid-term (3–12 months) to technical errors, and late (>12 months) to trauma or degeneration. Revision strategies include individualized graft selection, anatomical tunnel placement, repair of associated lesions, and consideration of biomechanical abnormalities. Overall success rates of revision procedures average 70–75%, with lower outcomes in adolescents and high-demand athletes. Emerging techniques, including lateral extra-articular tenodesis and biologic augmentation, may enhance revision outcomes, although long-term evidence remains limited. Conclusions: ACL reconstruction failure is a multifactorial event requiring thorough preoperative assessment, precise surgical planning, and individualized management. Addressing technical, biological, and neuromuscular factors, alongside patient-specific considerations, is essential to optimize functional outcomes and reduce failure rates. Future research should focus on standardized reporting, multicenter prospective studies, and advanced surgical planning tools to further improve revision success.
Keywords:
ACL reconstruction
; graft failure
; revision surgery
; tunnel malposition
; biomechanical factors
; neuromuscular control
; functional outcomes
1. Introduction
Anterior cruciate ligament (ACL) rupture is one of the most frequent injuries in young athletes, accounting for up to 50% of all ligamentous knee injuries and leading to significant socioeconomic impact due to time loss from sport and work [1]. ACL reconstruction has become a routine and highly standardized procedure in orthopedic sports medicine, with over 200,000 surgeries performed annually in the United States alone [2]. Despite advances in surgical techniques and rehabilitation protocols, graft failure remains a challenging complication, affecting between 1.8% and 16.7% of patients depending on follow-up duration and population characteristics [3].
Anterior cruciate ligament (ACL) reconstruction is a widely performed procedure in orthopedic sports medicine, particularly in young and physically active patients [4]. Despite generally positive outcomes, graft failure is a notable complication, with rates ranging from 1.8% to 16.7% depending on follow-up duration. Failure manifests through a combination of objective signs, such as positive Lachman and pivot-shift tests, instrumented laxity >3 mm, and reduced knee range of motion, and subjective symptoms including pain, instability, or functional impairment [5]. Traditional definitions of failure focusing solely on mechanical instability are limited. Studies show that a significant portion of patients with positive laxity tests report satisfactory subjective outcomes, while others experience symptoms despite normal objective findings [6]. The 2022 ESSKA consensus defines ACL failure as abnormal knee function due to graft insufficiency or failure to restore expected knee stability, caused by trauma, microtrauma, technical errors, biological factors, or untreated associated lesions [7]. This broadened definition underscores that ACL reconstruction outcomes are multifactorial, involving both mechanical and biological determinants of stability.
Beyond mechanical stability, recent literature emphasizes the concept of functional knee stability, which depends not only on passive structures such as the graft and capsule, but also on neuromuscular control and proprioceptive feedback mechanisms. Disruption of this sensorimotor integration may lead to subjective instability even when objective graft integrity is preserved, highlighting the complex interaction between biomechanical and neurophysiological recovery following ACL reconstruction.
Emerging evidence suggests that neuromuscular retraining and proprioceptive rehabilitation are essential to restore dynamic joint control and prevent recurrent instability [8].
In addition, the biopsychosocial dimension of postoperative recovery has gained increasing attention. Psychological readiness, fear of re-injury, and patient expectations have been shown to significantly influence subjective perception of function and return-to-sport rates [9]. These factors contribute to discrepancies between clinical tests and patient-reported outcomes, underscoring the need for a holistic assessment of surgical success.
Revision surgery success rates average around 75%, though outcomes vary by patient subgroup. Adolescents show higher failure rates (9%–21%) and reduced return to pre-injury sport levels (27%–68%). Primary ACL reconstruction failures typically range from 5% to 10% [10]. Recent large-scale registries and meta-analyses have confirmed that revision ACL reconstruction outcomes are consistently inferior to primary procedures, with higher rates of graft re-rupture and persistent instability [11]. These findings highlight the importance of preventing failure through meticulous surgical planning and comprehensive rehabilitation.
Etiologically, failure stems from recurrent instability (most common), postoperative complications (e.g., stiffness, infection), and patient factors (muscle dysfunction, arthritis). Technical errors, especially tunnel malposition, account for up to 80% of femoral and 37% of tibial tunnel-related failures. Biological failure involves inadequate graft integration, and traumatic failures often occur within the first postoperative year when biological incorporation is incomplete [12].
Failure timing offers diagnostic clues: early (<3 months) failures relate to fixation or infection, mid-term (3–12 months) to technical issues or aggressive rehab, and late (>12 months) to new trauma or degeneration. Infections are rare (<1%) but serious, requiring infection eradication before revision [13].
Late failures are increasingly recognized as multifactorial, often involving degenerative joint changes, secondary meniscal tears, or altered kinematics due to chronic instability [14].
Revision ACL reconstruction represents a growing clinical and research challenge. Despite numerous studies, consensus on optimal revision strategies remains limited, and current trends emphasize individualized approaches based on patient age, activity level, graft type, and associated injuries [15].
This review aims to provide an overview of ACL reconstruction failure classifications, causes, and current revision strategies, integrating recent perspectives on neuromuscular, biological, and psychosocial determinants of postoperative outcomes.
2. Materials and Methods
This work was designed as a narrative review conducted in accordance with the principles of the PRISMA 2020 (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines to ensure transparency, reproducibility, and methodological rigor [16]. The review protocol was prospectively registered in the PROSPERO database (registration number: 1170825). A comprehensive literature search was carried out across the PubMed/MEDLINE, Embase, and Google Scholar databases to identify relevant publications from January 2000 to May 2024. The search strategy combined the following terms and Boolean operators: “anterior cruciate ligament reconstruction” OR “ACL reconstruction” AND “failure” OR “graft failure” OR “revision” OR “instability” OR “technical error” OR “tunnel malposition” OR “biological failure” OR “revision outcomes.” This strategy was designed to maximize sensitivity while maintaining specificity. In addition, the reference lists of the included studies and relevant reviews were manually screened to identify further eligible papers not retrieved during the initial database search.
Only articles published in English were considered eligible. Studies were included if they addressed at least one of the following topics: definitions and classifications of anterior cruciate ligament (ACL) reconstruction failure, etiological factors such as technical, biological, or traumatic causes, or clinical and surgical management of revision ACL reconstruction. Eligible study designs included original research, systematic and narrative reviews, consensus statements, and large multicenter cohort studies, with particular attention to contributions from the Multicenter ACL Revision Study (MARS) group. Exclusion criteria comprised case reports, letters, editorials, conference abstracts, and studies not directly related to ACL reconstruction failure.
Two reviewers (G.C. and R.S.) independently screened all retrieved titles and abstracts, followed by full-text assessment of potentially relevant studies. Disagreements were resolved through discussion with a senior author (R.V.) to ensure consensus and consistency. For each included study, data were extracted regarding study design, population characteristics, mechanisms and classifications of failure, surgical techniques, graft selection, and clinical outcomes following revision procedures.
Given the narrative nature of the review, no formal quantitative synthesis or meta-analysis was performed. However, the methodological quality of each study was qualitatively assessed based on clarity of design, adequacy of clinical data, and relevance to the review’s objectives. The extracted evidence was synthesized thematically, focusing on the etiology, classification, and management of ACL reconstruction failure.
The final synthesis integrated evidence-based data, expert consensus, and clinical experience to provide a comprehensive overview of current knowledge in the field of ACL reconstruction failure and revision surgery. The process of study selection is summarized in the PRISMA flow diagram (Figure 1), while the inclusion and exclusion criteria are presented in Table 1.
3. Results
3.1. Etiology of ACL Reconstruction Failure
ACL reconstruction failure is a multifactorial event involving technical, biological, and traumatic mechanisms. Among these, technical errors remain predominant, representing approximately 60%–70% of all failures [Table 2].
The most common technical issue is femoral tunnel malposition, which is reported in up to 80% of failed reconstructions, typically due to an excessively anterior tunnel compromising graft isometry and tension balance. Posterior malpositioning of the tibial tunnel occurs in approximately 37% of cases and can lead to impingement and loss of stability. Other frequent causes include inappropriate graft selection, improper fixation or tensioning, and unaddressed concomitant lesions, such as meniscal ramp tears, anterolateral ligament (ALL) or posterolateral corner (PLC) injuries, that compromise rotational control and predispose to residual instability [Table 2].Traumatic causes, responsible for about 15–25% of failures, often involve high-energy injuries during the first postoperative year, when biological incorporation is still incomplete. However, secondary traumatic ruptures may also occur years later due to new pivoting injuries or return to contact sports.Biological failure, reported in 10–15% of cases, remains less clearly understood. It involves insufficient graft osteointegration, delayed revascularization, or incomplete ligamentization, often presenting without a distinct traumatic episode or technical fault. MRI and second-look arthroscopy studies have demonstrated variable graft remodeling and vascular ingrowth within the first 12–24 months postoperatively, with incomplete maturation associated with inferior mechanical strength and higher re-tear risk.Postoperative complications, such as infection (<1%), hematoma, and arthrofibrosis, may further compromise outcomes. Moreover, patient-related factors (smoking, diabetes, low quadriceps strength, high BMI, or premature return to sport) have been identified as independent predictors of revision surgery [Table 3].
3.2. Classification of Failure
ACL reconstruction failures can be classified according to their etiology (technical, biological, or traumatic) or timing (early, mid-term, or late), as illustrated in Table 4.
Early failures (< 3 months) are typically linked to fixation loss, infection, or acute trauma; mid-term failures (3–12 months) are commonly associated with technical errors, tunnel widening, or overly aggressive rehabilitation; and late failures (> 12 months) often result from new trauma, progressive graft elongation, or degenerative changes.
More refined classification systems, such as the Pittsburgh group or MARS criteria, integrate both failure mode and timing, aiding surgical planning by correlating the cause of failure with the most appropriate revision approach. In addition, the concept of “functional failure” has emerged to describe cases with persistent instability despite anatomically correct reconstruction, highlighting the influence of neuromuscular and sensorimotor deficits on knee kinematics .
3.3. Treatment and Surgical Strategies
Revision ACL reconstruction requires a personalized, stepwise approach based on the etiology of failure, tunnel condition, graft choice, and presence of associated lesions. Overall, the success rate after revision surgery averages 70–80%, though outcomes remain inferior to primary reconstructions, particularly in adolescents, where failure rates can reach 35% and return-to-sport rates remain below 65% [Table 3].Preoperative assessment should include 3D imaging (CT or MRI) to evaluate tunnel position, enlargement, and bone stock. Significant tunnel widening (> 13 mm femoral or > 16 mm tibial) generally necessitates a two-stage revision, with bone grafting and subsequent healing verification (typically 20–24 weeks post-grafting). Graft selection is a key determinant of outcome [Table 5].
Bone–patellar tendon–bone (BPTB) autografts remain the gold standard due to reliable bone-to-bone healing and fixation strength, especially when reusing previous tunnels, quadriceps tendon grafts have gained popularity for their low donor-site morbidity and consistent cross-sectional area, offering versatility in complex revisions. Hamstring autografts, though strong, show higher elongation rates when tunnels are dilated or fixation is suboptimal. Allografts may be considered in older or low-demand patients but carry higher failure rates in young, active individuals, up to three times greater according to MARS data.Fixation and tensioning are critical: optimal tension ranges between 20–40 N, with the knee positioned at 20–30° of flexion to ensure balanced anterior–posterior and rotational stability. Anatomical tunnel placement is guided by the Bernard–Hertel quadrant method (femur) and Tsukada’s landmarks (tibia). When anatomical constraints preclude standard positioning, alternative techniques such as out-in femoral drilling, over-the-top reconstructions, or lateral extra-articular tenodesis (LET) may be indicated to restore rotational stability.Addressing associated lesions is paramount: unrecognized ALL injuries, PLC insufficiency, or meniscal ramp tears are implicated in up to 25–30% of revision cases and should be systematically repaired. Furthermore, biomechanical abnormalities such as an increased posterior tibial slope (>12°) significantly elevate anterior tibial translation forces and may justify a corrective osteotomy to reduce graft stress.
Recent literature has also emphasized the potential benefit of augmented reconstructions, including the use of synthetic internal braces or biological adjuncts (platelet-rich plasma, stem-cell scaffolds) to enhance graft maturation and reduce re-tear risk, though long-term data remain limited.
4. Discussion
Revision anterior cruciate ligament (ACL) reconstruction represents a complex surgical challenge, markedly different from primary reconstruction in terms of planning, technical execution, and prognosis [17]. The results of this review confirm that technical errors, particularly tunnel malposition, remain the leading and largely preventable cause of graft failure, accounting for approximately 60–70% of cases [18]. Anterior malpositioning of the femoral tunnel increases graft tension, predisposing to rupture, whereas posterior malposition of the tibial tunnel compromises joint kinematics and rotational stability. When tunnels are inadequately positioned or overlapping, two-stage revision procedures with bone grafting are often required, which prolong rehabilitation and increase patient morbidity [19].The selection of an appropriate graft is central to surgical success. BPTB autografts provide reliable bone-to-bone healing and strong fixation, particularly advantageous when reusing previous tunnels [20]. Quadriceps tendon grafts offer versatility and low donor-site morbidity, while hamstring autografts may show weaker fixation, especially in the presence of tunnel enlargement [21,22]. Allografts, although convenient, carry higher failure rates in young, active patients, consistent with data from multicenter cohorts such as the MARS study [23]. Recent evidence further supports the use of quadriceps tendon autografts as a reliable alternative in revision settings, with comparable biomechanical strength to BPTB and superior patient-reported outcomes in some studies [24]. In contrast, the use of synthetic grafts has shown inconsistent results and remains controversial due to higher elongation rates and inflammatory complications [25].Associated lesions, including meniscal ramp tears, anterolateral ligament (ALL), and posterolateral corner (PLC) injuries, are frequently underestimated but significantly impact rotational stability and revision outcomes [26]. Addressing these concomitant injuries is crucial to restore functional knee stability, as persistent neuromuscular deficits or uncorrected ligamentous insufficiency may result in subjective instability despite anatomically correct graft placement [27]. Moreover, biomechanical abnormalities such as increased posterior tibial slope or coronal malalignment may necessitate corrective osteotomy to optimize long-term outcomes [28]. Several recent studies have confirmed that combined procedures, such as LET or ALL reconstruction, can significantly reduce rotational laxity and improve graft survivorship, particularly in high-risk populations such as young pivoting athletes [29,30]. A growing body of evidence also highlights the importance of individualized rehabilitation protocols emphasizing neuromuscular control, proprioception, and psychological readiness to return to sport [31,32].Technological advancements, including 3D computed tomography (CT), virtual surgical planning, and the adoption of techniques such as out-in femoral tunnels, over-the-top reconstructions, and selective double-bundle augmentation, have enhanced the precision of revision procedures, allowing tailored approaches for complex anatomical scenarios [33,34]. Additionally, emerging strategies, such as lateral extra-articular tenodesis (LET) and biologic augmentation with platelet-rich plasma or stem cells, may further reduce re-rupture risk, although long-term evidence remains limited [35].Furthermore, recent developments in intraoperative navigation, augmented reality (AR), and robotic-assisted drilling have shown promising potential in improving tunnel placement accuracy and reducing technical variability among surgeons [36]. Although these technologies are not yet widely adopted, they represent an important direction for future refinement of revision ACL surgery.Despite these innovations, long-term outcomes after revision ACL reconstruction remain inferior to primary procedures, with success rates averaging 70–75% and reduced rates of return to pre-injury sport, particularly in adolescents or high-demand athletes. This underscores the multifactorial nature of failure, in which technical, biological, traumatic, and patient-specific factors interact to influence prognosis. Meta-analyses confirm that psychological readiness, persistent muscle weakness, and residual instability are key determinants of unsuccessful return to sport [37]. Future research should focus on standardized definitions of failure, integration of patient-reported outcome measures (PROMs), and exploration of biological adjuvants to enhance graft integration and healing. Moreover, multidisciplinary approaches combining orthopedic, biomechanical, and psychological expertise are increasingly advocated to improve overall functional recovery and patient satisfaction.
4.1. Study Limitations
This narrative review has inherent limitations typical of its methodology. The absence of a systematic protocol or quantitative meta-analysis limits the ability to precisely estimate effect sizes and may introduce selection or publication bias. The included studies are heterogeneous in design, patient populations, follow-up duration, and definitions of failure, which constrains direct comparability. Furthermore, the scarcity of longitudinal, prospective, randomized trials in the field hampers the development of universally applicable recommendations. Finally, the exclusive inclusion of English-language publications may have excluded relevant studies from other regions.Despite these limitations, this review provides a comprehensive synthesis of current evidence on ACL reconstruction failure, highlighting key factors influencing revision outcomes and identifying gaps in knowledge. These findings reinforce the need for standardized reporting protocols, multicenter prospective studies, and integrated assessment of technical, biological, and neuromuscular factors to optimize surgical strategies and long-term functional outcomes.
5. Conclusions
ACL reconstruction failure is a multifactorial event that requires comprehensive assessment and individualized surgical planning. Successful revision surgery depends on technical precision in tunnel placement, appropriate graft selection, and thorough management of associated lesions, including meniscal, anterolateral, and posterolateral structures.The inherent complexity of revision ACL procedures necessitates meticulous preoperative evaluation, supported by advanced imaging, detailed anatomical assessment, and careful consideration of patient-specific risk factors such as age, activity level, comorbidities, and neuromuscular status. Although revision outcomes are generally favorable, they remain inferior to primary reconstructions, with lower rates of return to pre-injury sport and increased risk of graft re-rupture.
Future advancements in this field will rely on the implementation of sophisticated surgical planning tools, precision-guided graft placement, and enhanced patient stratification. Moreover, ongoing clinical research, including longitudinal and multicenter studies, is essential to refine surgical strategies, improve graft integration, and optimize long-term functional outcomes, ultimately reducing failure rates in both primary and revision ACL reconstructions.
Author Contributions
All authors have contributed to the conception and design of this study, acquisition of data, in drafting the article, in its revision, and all the authors approved the final draft of the submitted article.
Funding
This research received no external funding. None of the authors received any funds or has any financial interests to disclose.
Institutional Review Board Statement
The study was conducted according to the principles expressed in the Declaration of Helsinki and its later amendments. The research protocol was approved by the Institutional Review Board of Fondazione Policlinico Universitario “A Gemelli” IRCCS – Rome.
Data Availability Statement
All the data we analysed and tables we compiled are available for any clarification.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| ACL | Anterior Cruciate Ligament |
| ALL | Anterolateral Ligament |
| BPTB | Bone–Patellar Tendon–Bone |
| CT | Computed Tomography |
| LET | Lateral Extra-articular Tenodesis |
| MRI | Magnetic Resonance Imaging |
| MARS | Multicenter ACL Revision Study |
| PLC | Posterolateral Corner |
| ROM | Range of Motion |
| ESSKA | European Society of Sports Traumatology, Knee Surgery & Arthroscopy |
| BMI | Body Mass Index |
References
- Domnick, C.; Raschke, M.J.; Herbort, M. Biomechanics of the anterior cruciate ligament: Physiology, rupture and reconstruction techniques. World J Orthop. 2016, 7, 82–93. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Brinlee, A.W.; Dickenson, S.B.; Hunter-Giordano, A.; Snyder-Mackler, L. ACL Reconstruction Rehabilitation: Clinical Data, Biologic Healing, and Criterion-Based Milestones to Inform a Return-to-Sport Guideline. Sports Health 2022, 14, 770–779. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yao, S.; Fu, B.S.; Yung, P.S. Graft healing after anterior cruciate ligament reconstruction (ACLR) https://doi.org/10.1016/j.asmart.2021.03.003. Asia Pac J Sports Med Arthrosc Rehabil Technol. Erratum in: Asia Pac J Sports Med Arthrosc Rehabil Technol. 2021 Aug 13, 26, 58. https://doi.org/10.1016/j.asmart.2021.08.001. PMID: 34094881; PMCID: PMC8134949. 2021, 25, 8–15. [Google Scholar] [PubMed]
- Gerami, M.H.; Haghi, F.; Pelarak, F.; Mousavibaygei, S.R. Anterior cruciate ligament (ACL) injuries: A review on the newest reconstruction techniques. J Family Med Prim Care 2022, 11, 852–856. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Samitier, G.; Marcano, A.I.; Alentorn-Geli, E.; Cugat, R.; Farmer, K.W.; Moser, M.W. Failure of Anterior Cruciate Ligament Reconstruction. Arch Bone Jt Surg. 2015, 3, 220–240. [Google Scholar] [PubMed] [PubMed Central]
- Aldag, L.; Dallman, J.; Henkelman, E.; Herda, A.; Randall, J.; Tarakemeh, A.; Morey, T.; Vopat, B.G. Various Definitions of Failure Are Used in Studies of Patients Who Underwent Anterior Cruciate Ligament Reconstruction. Arthrosc Sports Med Rehabil. 2023, 5, 100801. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tischer, T.; Andriolo, L.; Beaufils, P.; Ahmad, S.S.; Bait, C.; Bonomo, M.; Cavaignac, E.; Cristiani, R.; Feucht, M.J.; Fiodorovas, M.; Grassi, A.; Helmerhorst, G.; Hoser, C.; Karahan, M.; Komnos, G.; Lagae, K.C.; Madonna, V.; Monaco, E.; Monllau, J.C.; Ollivier, M.; Ovaska, M.; Petersen, W.; Piontek, T.; Robinson, J.; Samuelsson, K.; Scheffler, S.; Sonnery-Cottet, B.; Filardo, G.; Condello, V. Management of anterior cruciate ligament revision in adults: the 2022 ESSKA consensus part III-indications for different clinical scenarios using the RAND/UCLA appropriateness method. Knee Surg Sports Traumatol Arthrosc. 2023, 31, 4662–4672. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kakarlapudi, T.K.; Bickerstaff, D.R. Knee instability: isolated and complex. West J Med. 2001, 174, 266–272. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nedder, V.J.; Raju, A.G.; Moyal, A.J.; Calcei, J.G.; Voos, J.E. Impact of Psychological Factors on Rehabilitation After Anterior Cruciate Ligament Reconstruction: A Systematic Review. Sports Health 2025, 17, 291–298. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tátrai, M.; Halasi, T.; Tállay, A.; Tátrai, A.; Karácsony, A.F.; Papp, E.; Pavlik, A. Higher revision and secondary surgery rates after ACL reconstruction in athletes under 16 compared to those over 16: a case-control study. J Orthop Surg Res. 2025, 20, 597. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wilde, J.; Bedi, A.; Altchek, D.W. Revision anterior cruciate ligament reconstruction. Sports Health 2014, 6, 504–518. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Diquattro, E.; Jahnke, S.; Traina, F.; Perdisa, F.; Becker, R.; Kopf, S. ACL surgery: reasons for failure and management. EFORT Open Rev. 2023, 8, 319–330. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Roethke, L.C.; Braaten, J.A.; Rodriguez, A.N.; LaPrade, R.F. Revision Anterior Cruciate Ligament Reconstruction (ACLR): Causes and How to Minimize Primary ACLR Failure. Arch Bone Jt Surg. 2023, 11, 80–93. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Belkhelladi, M.; Cierson, T.; Martineau, P.A. Biomechanical Risk Factors for Increased Anterior Cruciate Ligament Loading and Injury: A Systematic Review. Orthop J Sports Med. 2025, 13, 23259671241312681. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kemler, B.; Coladonato, C.; Perez, A.; Erickson, B.J.; Tjoumakaris, F.P.; Freedman, K.B. Considerations for revision anterior cruciate ligament reconstruction: A review of the current literature. J Orthop. 2024, 56, 57–62. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; Chou, R.; Glanville, J.; Grimshaw, J.M.; Hróbjartsson, A.; Lalu, M.M.; Li, T.; Loder, E.W.; Mayo-Wilson, E.; McDonald, S.; McGuinness, L.A.; Stewart, L.A.; Thomas, J.; Tricco, A.C.; Welch, V.A.; Whiting, P.; Moher, D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yan, X.; Yang, X.G.; Feng, J.T.; Liu, B.; Hu, Y.C. Does Revision Anterior Cruciate Ligament (ACL) Reconstruction Provide Similar Clinical Outcomes to Primary ACL Reconstruction? A Systematic Review and Meta-Analysis. Orthop Surg. 2020, 12, 1534–1546. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Li, X.; Yan, L.; Li, D.; Fan, Z.; Liu, H.; Wang, G.; Jiu, J.; Yang, Z.; Li, J.J.; Wang, B. Failure modes after anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Int Orthop. 2023, 47, 719–734. [Google Scholar] [CrossRef] [PubMed]
- Burnham, J.M.; Malempati, C.S.; Carpiaux, A.; Ireland, M.L.; Johnson, D.L. Anatomic Femoral and Tibial Tunnel Placement During Anterior Cruciate Ligament Reconstruction: Anteromedial Portal All-Inside and Outside-In Techniques. Arthrosc Tech. 2017, 6, e275–e282. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ostojic, M.; Indelli, P.F.; Lovrekovic, B.; Volcarenghi, J.; Juric, D.; Hakam, H.T.; Salzmann, M.; Ramadanov, N.; Królikowska, A.; Becker, R.; Prill, R. Graft Selection in Anterior Cruciate Ligament Reconstruction: A Comprehensive Review of Current Trends. Medicina (Kaunas) 2024, 60, 2090. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Runer, A.; Suter, A.; Roberti di Sarsina, T.; Jucho, L.; Gföller, P.; Csapo, R.; Hoser, C.; Fink, C. Quadriceps tendon autograft for primary anterior cruciate ligament reconstruction show comparable clinical, functional, and patient-reported outcome measures, but lower donor-site morbidity compared with hamstring tendon autograft: A matched-pairs study with a mean follow-up of 6.5 years. J ISAKOS 2023, 8, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Albishi, W.; Baltow, B.; Albusayes, N.; Sayed, A.A.; Alrabai, H.M. Hamstring autograft utilization in reconstructing anterior cruciate ligament: Review of harvesting techniques, graft preparation, and different fixation methods. World J Orthop. 2022, 13, 876–890. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Spindler, K.P. The Multicenter ACL Revision Study (MARS): a prospective longitudinal cohort to define outcomes and independent predictors of outcomes for revision anterior cruciate ligament reconstruction. J Knee Surg. 2007, 20, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Cohen, D.; Slawaska-Eng, D.; Almasri, M.; Sheean, A.; de Sa, D. Quadricep ACL Reconstruction Techniques and Outcomes: an Updated Scoping Review of the Quadricep Tendon. Curr Rev Musculoskelet Med. 2021, 14, 462–474. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Moretti, L.; Garofalo, R.; Cassano, G.D.; Geronimo, A.; Reggente, N.; Piacquadio, F.; Bizzoca, D.; Solarino, G. Anterior Cruciate Ligament Reconstruction with LARS Synthetic Ligament: Outcomes and Failures. J Clin Med. 2024, 14, 32. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Stranger, N.; Kaulfersch, C.; Mattiassich, G.; Mandl, J.; Hausbrandt, P.A.; Szolar, D.; Schöllnast, H.; Tillich, M. Frequency of anterolateral ligament tears and ramp lesions in patients with anterior cruciate ligament tears and associated injuries indicative for these lesions-a retrospective MRI analysis. Eur Radiol. 2023, 33, 4833–4841. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dadgostar, H.; Zarrini, M.; Hoveidaei, A.H.; Sattarpour, R.; Razi, S.; Arasteh, P.; Razi, M. Two-Year Functional Outcomes of Nonsurgical Treatment in Concomitant Anterior Cruciate Ligament and Medial Collateral Ligament Injuries: A Case-Control Study. J Knee Surg. 2024, 37, 730–735. [Google Scholar] [CrossRef] [PubMed]
- Nazzal, E.M.; Zsidai, B.; Pujol, O.; Kaarre, J.; Curley, A.J.; Musahl, V. Considerations of the Posterior Tibial Slope in Anterior Cruciate Ligament Reconstruction: a Scoping Review. Curr Rev Musculoskelet Med. 2022, 15, 291–299. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Madhan, A.S.; Ganley, T.J.; McKay, S.D.; Pandya, N.K.; Patel, N.M. Trends in Anterolateral Ligament Reconstruction and Lateral Extra-articular Tenodesis With ACL Reconstruction in Children and Adolescents. Orthop J Sports Med. 2022, 10, 23259671221088049. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Guarino, A.; Farinelli, L.; Iacono, V.; Screpis, D.; Piovan, G.; Rizzo, M.; Mariconda, M.; Zorzi, C. Lateral extra-articular tenodesis and anterior cruciate ligament reconstruction in young patients: clinical results and return to sport. Orthop Rev (Pavia) 2022, 14, 33696. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zampolini, M; Selb, M; Boldrini, P; Branco, CA; Golyk, V; Hu, X; Kiekens, C; Negrini, S; Nulle, A; Oral, A; Sgantzos, M; Shmonin, A; Treger, I; Stucki, G. UEMS-PRM Section and Board. The Individual Rehabilitation Project as the core of person-centered rehabilitation: the Physical and Rehabilitation Medicine Section and Board of the European Union of Medical Specialists Framework for Rehabilitation in Europe. Eur J Phys Rehabil Med. 2022, 58, 503–510. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Comodo, R. M.; Grassa, D.; Motassime, A. E.; Bocchino, G.; Totti, R.; De Fazio, A.; Meschini, C.; Capece, G.; Maccauro, G.; Vitiello, R. Telerehabilitation in Hip and Knee Arthroplasty: A Narrative Review of Clinical Outcomes, Patient-Reported Measures, and Implementation Challenges. Journal of Functional Morphology and Kinesiology 2025, 10, 370. [Google Scholar] [CrossRef]
- Yang, G.; Liu, D.; Zhou, G.; Wang, Q.; Zhang, X. Robot-assisted anterior cruciate ligament reconstruction based on three-dimensional images. J Orthop Surg Res. 2024, 19, 246. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Capece, G.; Andriollo, L.; Sangaletti, R.; Righini, R.; Benazzo, F.; Rossi, S.M.P. Advancements and Strategies in Robotic Planning for Knee Arthroplasty in Patients with Minor Deformities. Life (Basel) 2024, 14, 1528. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Migliorini, F.; Lucenti, L.; Mok, Y.R.; Bardazzi, T.; D'Ambrosi, R.; De Carli, A.; Paolicelli, D.; Maffulli, N. Anterior Cruciate Ligament Reconstruction Using Lateral Extra-Articular Procedures: A Systematic Review. Medicina (Kaunas) 2025, 61, 294. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bian, D.; Lin, Z.; Lu, H.; Zhong, Q.; Wang, K.; Tang, X.; Zang, J. The application of extended reality technology-assisted intraoperative navigation in orthopedic surgery. Front Surg. 2024, 11, 1336703. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Xiao, M.; van Niekerk, M.; Trivedi, N.N.; Hwang, C.E.; Sherman, S.L.; Safran, M.R.; Abrams, G.D. Patients Who Return to Sport After Primary Anterior Cruciate Ligament Reconstruction Have Significantly Higher Psychological Readiness: A Systematic Review and Meta-analysis of 3744 Patients. Am J Sports Med. 2023, 51, 2774–2783. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA 2020 Flow Diagram.
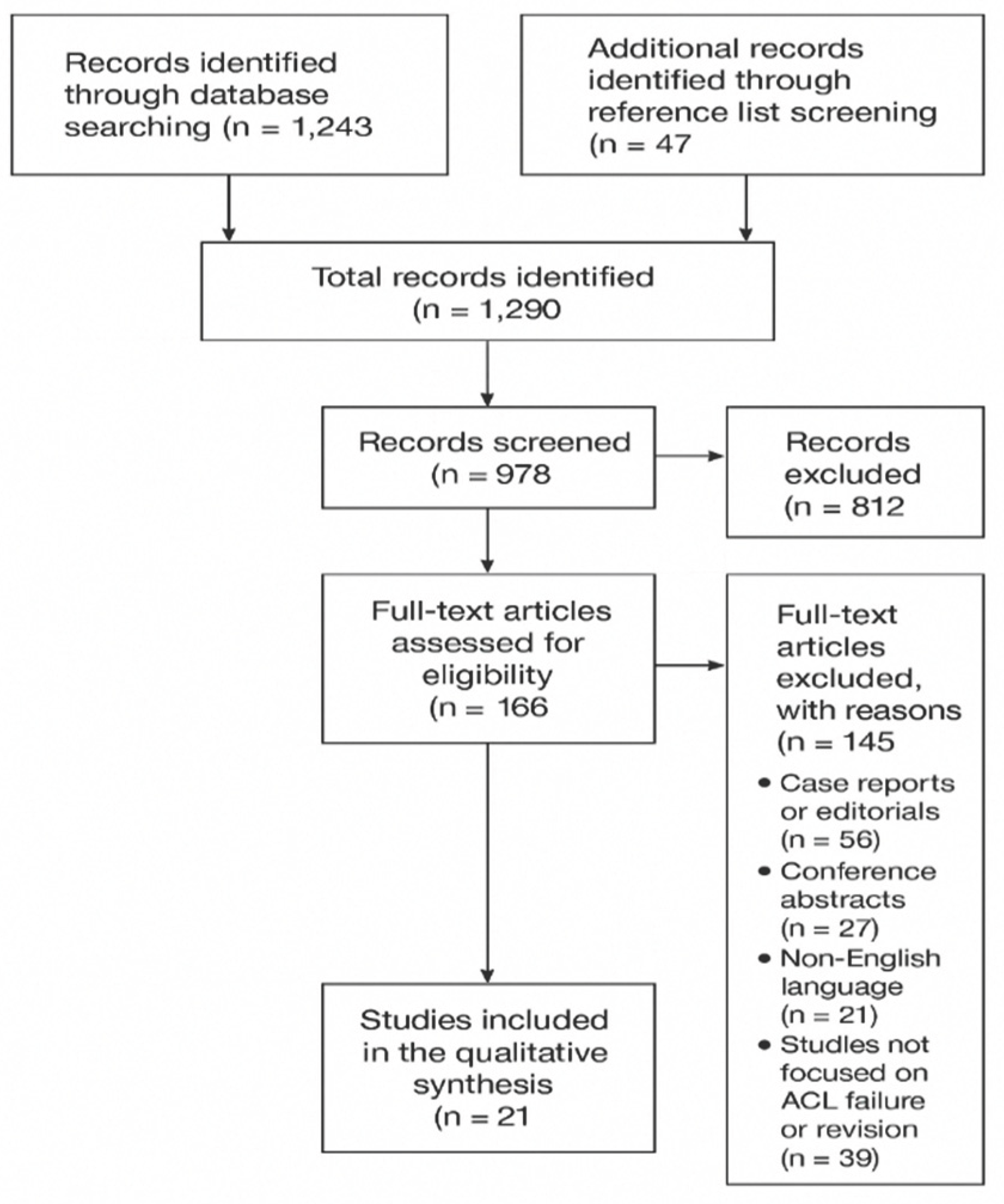

Table 1.
Inclusion and Exclusion Criteria.
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Original research, narrative/systematic reviews, consensus statements, and multicenter studies on ACL reconstruction failure | Case reports, editorials, letters, conference abstracts |
| Studies addressing definitions, etiology (technical, biological, or traumatic), or surgical management of ACL failure | Studies not directly related to ACL reconstruction or revision |
| English-language publications (2000–2024) | Non-English publications |
Table 2.
Etiology of ACL Reconstruction Failure.
| Etiology | Description | Approximate Frequency |
| Technical causes | Tunnel malposition (femoral anterior, tibial posterior), poor graft choice, fixation errors | 60 % – 70 % |
| Traumatic causes | High-energy trauma, especially within first postoperative year | 15 % – 25 % |
| Biological causes | Poor graft osteointegration, revascularization or ligamentization | 10 % – 15 % |
Table 3.
Incidence and Risk Factors of ACL Reconstruction Failure.
| Factor | Incidence / Rate | Notes |
|---|---|---|
| Overall failure rate | 4 % – 25 % | Varies by demographics and activity level |
| Female patients (< 20 or > 40 years) | Higher incidence | Hormonal and biomechanical influences |
| Adolescents (< 20 years) | Up to 35 % failure | Highest risk subgroup; early return to sport |
| Revision surgery success rate | ~ 75 % | Lower in adolescents and high-level athletes |
| Early return to sport (< 9 months) | ↑ failure risk | Associated with incomplete graft maturation |
Table 4.
Timing-Based Classification of ACL Failure.
| Time from Surgery | Common Causes | Clinical Considerations |
|---|---|---|
| Early (< 3 months) | Fixation failure, infection | Requires urgent management |
| Mid-term (3–12 months) | Technical errors, aggressive rehab, missed lesions | Surgical re-evaluation critical |
| Late (> 12 months) | New trauma, graft elongation, degenerative widening | Assess for secondary instability |
Table 5.
Graft Options and Considerations in Revision ACL Reconstruction.
| Graft Type | Advantages | Disadvantages | Indications |
|---|---|---|---|
| Bone–Patellar Tendon–Bone (BPTB) | Strong bone-to-bone healing, rigid fixation | Anterior knee pain, donor-site morbidity | Reuse of previous tunnels, high-demand athletes |
| Quadriceps Tendon | Versatile, low donor-site morbidity, large cross-section | Less widespread familiarity | Complex or revision cases |
| Hamstring Tendon | Good strength, minimal anterior knee pain | Weaker fixation in enlarged tunnels | Primary or single-stage revisions |
| Allograft | No donor morbidity, shorter operative time | Higher re-rupture rate in young patients | Older or low-demand individuals |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



