
Submitted:
24 December 2025
Posted:
25 December 2025
You are already at the latest version
Abstract
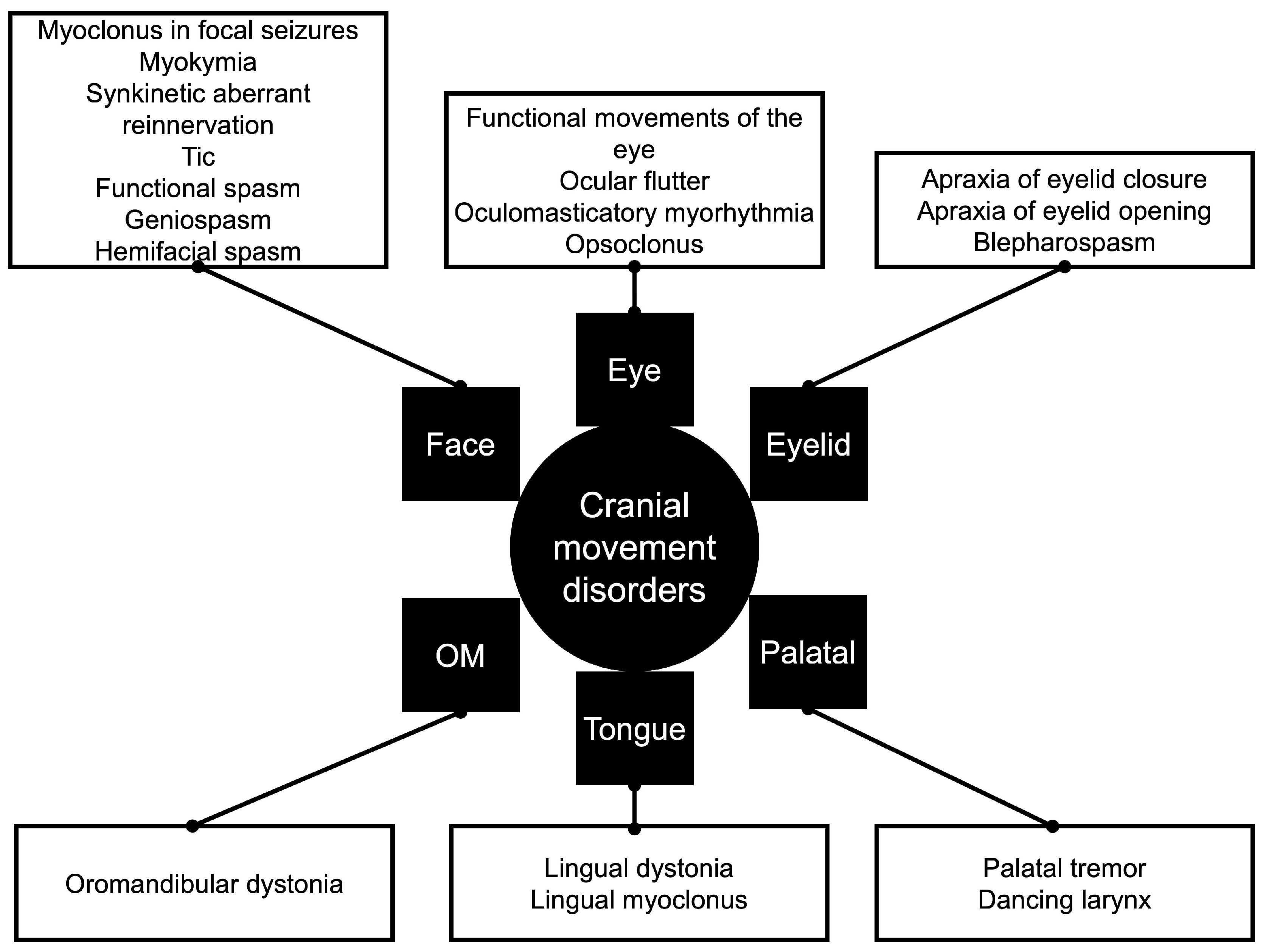
Craniofacial or cranial movement disorders are commonly seen in clinical practice. However, they are usually underdiagnosed or even misdiagnosed, leading to significant impairment in the quality of life of patients affected by these disorders. They are traditionally defined as movement disorders involving the face, jaw, tongue, and palate; but, it is possible to include the eye and ear based on the literature available. The current study aims to generally describe the phenomenology related to these abnormal movements for the general neurologist and practitioner. The most frequent are hemifacial spasm, blepharospasm, and myokymia. Other less commonly discussed are rabbit syndrome, apraxia of the eyelid opening/closing, tardive dyskinesia, chorea, tics, myorhythmia, dystonia, and tremor. Also, there are locations for the development of movement dis-orders, such as the ears (ear dyskinesia and ear myoclonus), chin (geniospasm), and tongue (lingual dystonia and lingual myoclonus) that are rarely discussed. Craniofacial movements are also seen in patients with autoimmune conditions, and the different features of these movements led to new terms like dystonic or dyskinetic stereotypies due to the dynamic change of the phenomenology. Another fact is that up to ten percent of patients with functional movement disorder will have craniofacial movement disorders.
Keywords:
1. Introduction
2. Craniofacial Movement Disorders
2.1. Hemifacial Spasm
2.2. Tardive Dyskinesia
2.3. Rabbit Syndrome
2.4. Chorea
2.5. Tics And Stereotyped Movements
2.6. Myorhythmia
2.7. Dystonia
2.7.1. Tongue Dystonia
2.7.2. Cervical Dystonia
2.7.3. Trismus
2.8. Tremor
2.8.1. Palatal Tremor
2.8.2. Tongue, Jaw, And Head Tremor
2.9. Facial Myokymia and Facial Myoclonus
2.10. Ear
2.11. Autoimmune Encephalitis
2.12. Ataxia-Telangiectasia
3. Functional Craniofacial Movement Disorders
4. Future Directions and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yi, M.; Li, J.; Liu, G.; Ou, Z.; Liu, Y.; Li, J.; Chen, Y.; Guo, Y.; Wang, Y.; Zhang, W.; et al. Mental Health and Quality of Life in Patients with Craniofacial Movement Disorders: A Cross-Sectional Study. Front Neurol 2022, 13, 938632. [CrossRef]
- Yaltho, T.C.; Jankovic, J. The Many Faces of Hemifacial Spasm: Differential Diagnosis of Unilateral Facial Spasms. Mov Disord 2011, 26, 1582–1592. [CrossRef]
- Aghazadeh, K.; Rahmaty, B.; Kouhi, A.; Dabiri, S.; Sohrabpour, S.; Mohammadzadeh, M.; Jafari, N. Bilateral Facial Nerve Schwannoma: A Case Report and Review of the Literature. An International Journal of Otorhinolaryngology Clinics 2021, 13, 47–52.
- Anusa, A.M.; Thavarajah, R.; Nayak, D.; Joshua, E.; Rao, U.K.; Ranganathan, K. A Study on Drug-Induced Tardive Dyskinesia: Orofacial Musculature Involvement and Patient’s Awareness. J Orofac Sci 2018, 10, 86–95.
- Ondo, W.G.; Adam, O.R.; Jankovic, J.; Chinnery, P.F. Dramatic Response of Facial Stereotype/Tic to Tetrabenazine in the First Reported Cases of Neuroferritinopathy in the United States. Mov Disord 2010, 25, 2470–2472. [CrossRef]
- Baizabal-Carvallo, J.F.; Ondo, W.G. Stereotypies as a Manifestation of Acute Hyperglycemia without Ketosis. J Neurol Sci 2012, 315, 176–177. [CrossRef]
- Rissardo, J.P.; Kherajani, K.; Vora, N.M.; Yatakarla, V.; Fornari Caprara, A.L.; Ratliff, J.; Caroff, S.N. A Systematic Review of Oral Vertical Dyskinesia (“Rabbit” Syndrome). Medicina (Kaunas) 2024, 60. [CrossRef]
- Fekete, R.; Jankovic, J. Upper Facial Chorea in Huntington Disease. J Clin Mov Disord 2014, 1, 7. [CrossRef]
- Danek, A.; Tison, F.; Rubio, J.; Oechsner, M.; Kalckreuth, W.; Monaco, A.P. The Chorea of McLeod Syndrome. Mov Disord 2001, 16, 882–889. [CrossRef]
- Koller, W.C. Edentulous Orodyskinesia. Ann Neurol 1983, 13, 97–99. [CrossRef]
- Evidente, V.G.; Adler, C.H. Hemifacial Spasm and Other Craniofacial Movement Disorders. Mayo Clin Proc 1998, 73, 67–71. [CrossRef]
- Baizabal-Carvallo, J.F.; Alonso-Juarez, M.; Jankovic, J. Oromandibular Tics Associated with Tourette Syndrome. J Neurol 2023, 270, 2591–2596. [CrossRef]
- Baizabal-Carvallo, J.F.; Jankovic, J. The Clinical Phenomenology and Correlations of Oculogyric Tics. Acta Neurol Belg 2022, 122, 925–930. [CrossRef]
- Baizabal-Carvallo, J.F.; Alonso-Juarez, M.; Jankovic, J. Dystonic Motor and Phonic Tics in Tourette Syndrome. J Neurol 2022, 269, 5312–5318. [CrossRef]
- Baizabal-Carvallo, J.F.; Cardoso, F.; Jankovic, J. Myorhythmia: Phenomenology, Etiology, and Treatment. Mov Disord 2015, 30, 171–179. [CrossRef]
- Leal-Ortega, R.; Baizabal-Carvallo, J.F. Orolingual Myorhythmia, the “Frog Sac” Sign. Acta Neurol Belg 2025. [CrossRef]
- Nakashima, K.; Kusumi, M.; Inoue, Y.; Takahashi, K. Prevalence of Focal Dystonias in the Western Area of Tottori Prefecture in Japan. Mov Disord 1995, 10, 440–443. [CrossRef]
- Nutt, J.G.; Muenter, M.D.; Aronson, A.; Kurland, L.T.; Melton, L.J. 3rd Epidemiology of Focal and Generalized Dystonia in Rochester, Minnesota. Mov Disord 1988, 3, 188–194. [CrossRef]
- Duffey, P.O.; Butler, A.G.; Hawthorne, M.R.; Barnes, M.P. The Epidemiology of the Primary Dystonias in the North of England. Adv Neurol 1998, 78, 121–125.
- Epidemiological Study of Dystonia in Europe (ESDE) Collaborative Group A Prevalence Study of Primary Dystonia in Eight European Countries. J Neurol 2000, 247, 787–792. [CrossRef]
- Defazio, G.; Abbruzzese, G.; Livrea, P.; Berardelli, A. Epidemiology of Primary Dystonia. Lancet Neurol 2004, 3, 673–678. [CrossRef]
- Hallett, M. Blepharospasm: Recent Advances. Neurology 2002, 59, 1306–1312. [CrossRef]
- Cimmino, A.T.; Vitali, F.; Iorio, R. Teaching Video NeuroImage: Bilateral Eyelid Opening Apraxia in a Patient With Top of the Basilar Syndrome. Neurology 2023, 100, 734–735. [CrossRef]
- Verghese, J.; Milling, C.; Rosenbaum, D.M. Ptosis, Blepharospasm, and Apraxia of Eyelid Opening Secondary to Putaminal Hemorrhage. Neurology 1999, 53, 652. [CrossRef]
- Miranda, M.; Millar, A. Blepharospasm Associated with Bilateral Infarcts Confined to the Thalamus: Case Report. Mov Disord 1998, 13, 616–617. [CrossRef]
- Kulisevsky, J.; Avila, A.; Roig, C.; Escartín, A. Unilateral Blepharospasm Stemming from a Thalamomesencephalic Lesion. Mov Disord 1993, 8, 239–240. [CrossRef]
- Singer, C.; Schatz, N.J.; Bowen, B.; Eidelberg, D.; Kazumata, K.; Sternau, L.; Shulman, L.M.; Weiner, W.J. Asymmetric Predominantly Ipsilateral Blepharospasm and Contralateral Parkinsonism in an Elderly Patient with a Right Mesencephalic Cyst. Mov Disord 1998, 13, 135–139. [CrossRef]
- Saeedi, Y.; Kazemi, F.; Habibi, S.A.H.; Tafakhori, A.; Chitsaz, A.; Fasano, A.; Lang, A.E.; Rohani, M. Tongue Protrusion Dystonia in Pantothenate Kinase-Associated Neurodegeneration. Pediatr Neurol 2020, 103, 76–78. [CrossRef]
- Stephen, C.D.; Dy-Hollins, M.; Gusmao, C.M.D.; Qahtani, X.A.; Sharma, N. Dystonias: Clinical Recognition and the Role of Additional Diagnostic Testing. Semin Neurol 2023, 43, 17–34. [CrossRef]
- Yoshida, K. Coronoidotomy as Treatment for Trismus Due to Jaw-Closing Oromandibular Dystonia. Mov Disord 2006, 21, 1028–1031. [CrossRef]
- Chronic Clicking Tinnitus Due to Palatal Tremor: Essential or Secondary?; England, 2021; Vol. 397;
- Schrag, A.; Bhatia, K.P.; Quinn, N.P.; Marsden, C.D. The Dancing Larynx--a Variant of Palatal Tremor? Mov Disord 1999, 14, 882–883. [CrossRef]
- Shoeibi, A.; Litvan, I. Prominent Tongue and Jaw Tremor in a Patient with Probable Progressive Supranuclear Palsy. Mov Disord Clin Pract 2018, 5, 99–100. [CrossRef]
- Olfati, N.; Dickson, D.W.; Shoeibi, A.; Haubenberger, D.; Litvan, I. Isolated Jaw and Tongue Tremor in a Definite Case of Progressive Supranuclear Palsy. Mov Disord Clin Pract 2023, 10, 348–349. [CrossRef]
- Chung, S.J.; Im, J.-H.; Lee, J.-H.; Cho, A.-H.; Kwon, M.; Lee, M.C. Isolated Tongue Tremor after Gamma Knife Radiosurgery for Acoustic Schwannoma. Mov Disord 2005, 20, 108–111. [CrossRef]
- Kim, S.J.; Lee, W.Y.; Kim, B.J.; Kim, J.-Y.; Hong, S.B.; Tae, W.S.; Seo, D.-W. Isolated Tongue Tremor after Removal of Cerebellar Pilocytic Astrocytoma: Functional Analysis with SPECT Study. Mov Disord 2007, 22, 1825–1828. [CrossRef]
- Saka, E.; Ozkaynak, S.; Tuncer, R. Tongue Tremor in Brainstem Pilocytic Astrocytoma. J Clin Neurosci 2006, 13, 503–506. [CrossRef]
- Thakolwiboon, S.; Ruthirago, D.; Laengvejkal, P.; Wilms, H. Mystery Case: Symptomatic Isolated Tongue Tremor of Cortical Origin Due to Stroke. Neurology 2020, 94, 591–592. [CrossRef]
- Salari, M.; Rezaei, K.; Mirdehghan, A.; Behzadi, A.; Etemadifar, M. Focal Epilepsy Presenting as Tongue Tremor: A Case Report. Clin Case Rep 2022, 10, e05478. [CrossRef]
- Louis, E.D.; Rios, E.; Applegate, L.M.; Hernandez, N.C.; Andrews, H.F. Jaw Tremor: Prevalence and Clinical Correlates in Three Essential Tremor Case Samples. Mov Disord 2006, 21, 1872–1878. [CrossRef]
- Robakis, D.; Louis, E.D. Head Tremor in Essential Tremor: “Yes-Yes”, “No-No”, or “Round and Round”? Parkinsonism Relat Disord 2016, 22, 98–101. [CrossRef]
- Sulica, L.; Louis, E.D. Clinical Characteristics of Essential Voice Tremor: A Study of 34 Cases. Laryngoscope 2010, 120, 516–528. [CrossRef]
- Lynch, M.C.; Cohen, J.A. A Primer on Electrophysiologic Studies in Myopathy. Rheum Dis Clin North Am 2011, 37, 253–268, vii. [CrossRef]
- Gobernado, J.M.; Galarreta, M.; De Blas, G.; Jimenez-Escrig, A.; Hernandez, A. Isolated Continuous Rhythmic Lingual Myoclonus. Mov Disord 1992, 7, 367–369. [CrossRef]
- Carluer, L.; Schupp, C.; Defer, G.-L. Ear Dyskinesia. J Neurol Neurosurg Psychiatry 2006, 77, 802–803. [CrossRef]
- Kirk, A.; Heilman, K.M. Auricular Myoclonus. Can J Neurol Sci 1991, 18, 503–504. [CrossRef]
- Rizvi, I.; Garg, R.K.; Malhotra, H.S.; Kumar, N.; Uniyal, R. Severe Lingual and Orofacial Dyskinesias in Anti-NMDA Receptor Encephalitis: A Case Report and Review of Indian Literature. Neurol India 2020, 68, 225–229. [CrossRef]
- Dineen, R.A.; Whitehouse, W.P. Ataxia Telangiectasia. In Essentials of Cerebellum and Cerebellar Disorders: A Primer For Graduate Students; Gruol, D.L., Koibuchi, N., Manto, M., Molinari, M., Schmahmann, J.D., Shen, Y., Eds.; Springer International Publishing: Cham, 2023; pp. 621–630 ISBN 978-3-031-15070-8.
- Mishra, A.; Pandey, S. Cranial Functional Movement Disorders: A Case Series with Literature Review. Tremor Other Hyperkinet Mov (N Y) 2020, 10, 33. [CrossRef]
- Fasano, A.; Valadas, A.; Bhatia, K.P.; Prashanth, L.K.; Lang, A.E.; Munhoz, R.P.; Morgante, F.; Tarsy, D.; Duker, A.P.; Girlanda, P.; et al. Psychogenic Facial Movement Disorders: Clinical Features and Associated Conditions. Mov Disord 2012, 27, 1544–1551. [CrossRef]
- Baizabal-Carvallo, J.F.; Jankovic, J. Distinguishing Features of Psychogenic (Functional) versus Organic Hemifacial Spasm. J Neurol 2017, 264, 359–363. [CrossRef]
- Baizabal-Carvallo, J.F.; Jankovic, J. Examiner Manoeuvres “sensory Tricks” in Functional (Psychogenic) Movement Disorders. J Neurol Neurosurg Psychiatry 2017, 88, 453–455. [CrossRef]
- Aniello, M.S.; Altomare, S.; Difazio, P.; Giorelli, M. Functional Rabbit Syndrome: A Case Report. Tremor Other Hyperkinet Mov (N Y) 2021, 11, 56. [CrossRef]
- Baizabal-Carvallo, J.F.; Jankovic, J. The Clinical Features of Psychogenic Movement Disorders Resembling Tics. J Neurol Neurosurg Psychiatry 2014, 85, 573–575. [CrossRef]
- Baizabal-Carvallo, J.F.; Jankovic, J. Functional (Psychogenic) Saccadic Oscillations and Oculogyric Crises. Lancet Neurol 2016, 15, 791. [CrossRef]
- McLoughlin, C.; McWhirter, L.; Pisegna, K.; Tijssen, M.A.J.; Tak, L.M.; Carson, A.; Stone, J. Stigma in Functional Neurological Disorder (FND) - A Systematic Review. Clin Psychol Rev 2024, 112, 102460. [CrossRef]
- Baydar, C.; Yevgi, R.; Karataş, Ö. Assessment of Depression and Anxiety After Botulinum Toxin Injection Treatment in Patients with Hemifacial Spasm and Blepharospasm. IAMR 2024, 16, 1–10. [CrossRef]
- Dong, H.; Fan, S.; Luo, Y.; Peng, B. Botulinum Toxin Relieves Anxiety and Depression in Patients with Hemifacial Spasm and Blepharospasm. Neuropsychiatr Dis Treat 2019, 15, 33–36. [CrossRef]
- Berardelli, I.; Pasquini, M.; Roselli, V.; Biondi, M.; Berardelli, A.; Fabbrini, G. Cognitive Behavioral Therapy in Movement Disorders: A Review. Mov Disord Clin Pract 2015, 2, 107–115. [CrossRef]

| Movement Disorder | Note |
| Apraxia of eyelid closure | Impaired voluntary eyelid closure despite normal reflex blinking. |
| Apraxia of eyelid opening | Difficulty initiating voluntary eyelid elevation despite normal levator muscle function. |
| Blepharospasm | It is a focal dystonia involving involuntary, bilateral eyelid contractions caused by orbicularis oculi hyperactivity. |
| Facial myoclonus in focal seizures | Jerking movements of facial muscles, resulting from abnormal electrical activity in the contralateral motor cortex or brainstem regions. |
| Facial myokymia/ neuromyotonia/ superior oblique myokymia and facial fasciculation | Continuous, fine, rippling muscle contractions involving the facial muscles, often without voluntary control. Unlike simple fasciculations, myokymia produces persistent wave-like movements that may spread across muscle groups. Neuromyotonia is more severe than myokymia and involves delayed relaxation and stiffness of the affected muscles. |
| Facial nerve palsy with synkinetic aberrant reinnervation | Improper regeneration of facial nerve fibers, causing involuntary muscle contractions and uncoordinated facial movements, often seen as simultaneous eye and mouth muscle activity. |
| Facial tic | Repetitive muscle movement or vocalization affecting the face, often linked to conditions like Tourette syndrome, exacerbated by stress or anxiety. |
| Functional facial spasm | Episodic facial muscle contractions without underlying neurological pathology, often triggered by stress or emotional factors. Unlike dystonias, functional facial spasms may resolve with relaxation or psychological interventions, and they lack the persistent or repetitive nature seen in other movement disorders. |
| Functional movement disorders of the eye | Convergence spasm, convergence paralysis, gaze limitation, functional and voluntary nystagmus and oscillopsia. |
| Geniospasm | Involuntary contraction of the mentalis muscle, causing chin tightening or protrusion. |
| Hemifacial spasm | Unilateral contractions of facial muscles, often due to irritation of the facial nerve, typically resulting from vascular compression or nerve lesions. |
| Hemimasticatory spasm | Sustained contractions of unilateral chewing muscles (masseter, temporalis), causing jaw clenching and difficulty opening the mouth. |
| Lingual dystonia | Sustained contractions of the tongue muscles, leading to abnormal tongue postures, difficulty speaking or swallowing. |
| Lingual myoclonus | Jerking movements of the tongue, often due to brainstem or basal ganglia lesions. |
| Myotonia | Delayed muscle relaxation in the face after contraction, causing stiffness or difficulty with facial expressions. It is often associated with myotonic dystrophy. |
| Ocular flutter | Rapid, uncontrolled, repetitive horizontal eye movements. |
| Oculomasticatory myorhythmia | Convergent-divergent nystagmus, concurrent contractions of the masticatory muscles. |
| Opsoclonus | Rapid, multidirectional eye movements, without slow-phase. |
| Oromandibular dystonia | Contractions of the jaw, lips, and tongue muscles, leading to difficulty speaking, chewing, or swallowing |
| Palatal Tremor | Rhythmic, involuntary contractions of the soft palate muscles |
| Variable | Essential palatal tremor | Psychogenic palatal tremor | Secondary palatal tremor |
| Etiology | Unknown | Psychiatric disorder | Brainstem, cerebellar, and basal ganglia |
| Muscle involved | Tensor veli palatini | Levator veli palatini and tensor veli palatini | Levator veli palatini |
| Nerve Innervated | Trigeminal nerve | Trigeminal, glossopharyngeal, and vagus cranial nerves | Glossopharyngeal and vagus cranial nerves |
| Side | Bilateral | Variable, mainly bilateral | Monolateral |
| Voluntary control | Rarely | Yes | No |
| Ear clicks (tensor veli palatini) | Frequent | Frequent | Absent |
| Persistence during sleep | Absence | Absence | Presence |
| Olivary autonomous oscillator | Unknown | No | Evidence |
| Course | Disappear spontaneously | Variable | Continuous |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



