Submitted:
23 December 2025
Posted:
24 December 2025
You are already at the latest version
Abstract
This study investigates how different business model configurations impact the performance of physiotherapy practices within a competitive healthcare environment. Specifically, it examines the influence of business model efficiency and novelty on organizational outcomes, considering the moderating effect of managed competition contracts. Using quantitative analysis of data from Dutch physiotherapy primary healthcare organizations, the research reveals nuanced relationships between business model design and performance, highlighting the importance of contractual factors in shaping these dynamics.
Keywords:
business model
; efficiency
; novelty
; performance
; physiotherapy
; managed competition
; contracts
; quantitative analysis
; healthcare organizations
1. Introduction and Motivation
Healthcare systems worldwide face persistent challenges in balancing service quality, accessibility, and financial sustainability. Since the 1990s, managed competition has been introduced as a reform mechanism to inject market principles into healthcare delivery, particularly in countries such as the Netherlands [1,2]. The basic idea is that insurers compete for patients by selectively contracting providers, while providers compete for contracts by demonstrating quality and efficiency. In theory, this market-oriented design should reduce costs, enhance patient choice, and incentivise innovation.
Despite these expectations, managed competition has produced mixed results in practice. Insurers often retain disproportionate bargaining power, while providers, particularly small organisations, struggle to adapt to contractual demands. Physiotherapy primary healthcare organisations (PTPHOs) exemplify this tension: as micro-sized businesses, they face limited resources for administrative compliance, innovation, and service expansion [3]. This raises important questions about how organisational strategies—specifically business model design—affect performance outcomes under competitive contractual regimes.
Business models describe the mechanisms through which organisations create, deliver, and capture value [4,5]. In the healthcare context, two dimensions of business model design have received particular attention: efficiency, which focuses on cost reduction, streamlined transactions, and resource optimisation, and novelty, which emphasises new service arrangements, stakeholder collaborations, and innovative delivery methods. The balance between efficiency and novelty is central to how PTPHOs navigate managed competition.
However, existing research offers limited insight into how business model designs interact with contractual environments to shape organisational performance. While efficiency is often assumed to align with cost-control incentives embedded in contracts, novelty may generate value outside reimbursement structures, such as preventative interventions or patient-centered innovations [6]. This creates a research gap: do efficiency and novelty contribute equally to performance, and how are these relationships conditioned by competitive contract requirements?
This study addresses these questions by investigating the link between business model configurations and organisational outcomes in Dutch physiotherapy practices, with a specific focus on the moderating role of managed competition contracts. By analysing how efficiency and novelty interact with contract intensity, the paper contributes to both theory and practice: it enriches the literature on business models in healthcare, and it offers practical insights for managers seeking to align strategies with contractual realities.
The motivation for this research is twofold. First, it seeks to move beyond the assumption that efficiency alone drives superior outcomes, by highlighting the role of novelty in sustaining quality and financial performance. Second, it provides evidence from a primary care sector often overlooked in business model research, thereby extending understanding of how small healthcare providers respond to structural reforms in competitive environments.
2. Theoretical Foundations of Business Model Design
The concept of the business model has gained prominence in management and strategy research as a framework for understanding how organisations create, deliver, and capture value [7,8]. In healthcare, business models are particularly relevant because organisations must balance clinical objectives with financial sustainability, while also responding to institutional and regulatory constraints [9]. This section outlines the theoretical underpinnings of business model design, with a focus on efficiency and novelty, and explains how these dimensions interact with competitive contracts.
2.1. Business Models as Value Systems
A business model can be conceptualised as an activity system that structures transactions between an organisation and its stakeholders [4]. It encompasses customer relationships, revenue streams, resource allocation, and governance mechanisms. In service industries such as healthcare, where value is co-created with patients and insurers, the business model perspective provides a lens for analysing both operational and strategic choices.
2.2. Efficiency as a Strategic Orientation
Efficiency-oriented business models seek to minimise transaction costs and optimise resource use. In the healthcare context, efficiency may involve streamlined data reporting, adherence to evidence-based protocols, or integration of IT systems to reduce administrative overhead [10]. Transaction cost economics suggests that efficiency improves performance by reducing uncertainty and aligning incentives among stakeholders. Under competitive contracts, efficiency is often rewarded through financial reimbursement tied to measurable indicators of productivity and compliance.
2.3. Novelty as a Strategic Orientation
Novelty refers to the creation of new linkages, partnerships, or service delivery mechanisms [10]. For physiotherapy practices, novelty may involve digital platforms for remote care, multidisciplinary collaborations, or preventative service models. Resource-based theory posits that novel practices generate sustained competitive advantage by leveraging unique, hard-to-imitate capabilities [11]. Unlike efficiency, novelty is less directly aligned with reimbursement schemes but may nonetheless improve organisational reputation, patient satisfaction, and long-term growth.
2.4. Contracts as Moderating Mechanisms
Contracts operationalise managed competition by defining financial incentives and performance benchmarks. They can amplify or constrain the value of business model designs. For instance, efficiency aligns well with contractual metrics such as cost per treatment or audit compliance. By contrast, novelty may be undervalued if reimbursement structures exclude preventative services or experimental delivery models [6]. This moderating role makes contracts central to understanding how business model choices translate into outcomes.
2.5. Integrating Efficiency, Novelty, and Contracts
The theoretical foundation suggests a contingent relationship: efficiency improves outcomes primarily under contract-intensive environments, whereas novelty may drive outcomes independently of contractual alignment. This duality underlines the importance of examining how physiotherapy practices balance these orientations when designing business models in competitive healthcare markets.
3. Physiotherapy Practices Under Managed Competition
Managed competition in healthcare seeks to improve efficiency and quality through regulated market forces, where insurers selectively contract providers and patients are expected to make active choices [12]. The Netherlands represents one of the most advanced implementations of this system, with reforms in 2006 establishing a structured framework that governs provider–insurer relationships. Physiotherapy primary healthcare organisations (PTPHOs) are key actors in this environment, yet their small scale and resource constraints make them particularly sensitive to contractual pressures.
3.1. Characteristics of PTPHOs
PTPHOs are typically micro-enterprises employing fewer than ten staff members, often operating as privately owned practices embedded in local communities. They deliver services aimed at maintaining or restoring physical function across diverse patient groups. Unlike hospitals, PTPHOs rely on relatively modest infrastructure and operate with limited bargaining power vis-à-vis insurers [2]. This organisational profile makes them both agile in service delivery and vulnerable to regulatory or contractual shifts.
3.2. Contractual Requirements and Compliance
Managed competition contracts define reimbursement schemes based on compliance with performance indicators, quality reporting, and audit participation. In practice, contracts with the highest requirements offer higher reimbursement rates, incentivising compliance. However, these demands impose substantial administrative and operational burdens on small practices. For example, reporting systems and quality audits consume resources that could otherwise be directed toward clinical services [10]. As a result, not all PTPHOs are equally able to meet stringent contractual criteria, leading to performance disparities.
3.3. Tensions Between Efficiency and Innovation
A central challenge for PTPHOs is balancing efficiency with innovation. Contracts tend to reward efficiency metrics, such as treatment volumes or adherence to clinical protocols, while undervaluing preventative or experimental approaches. Practices that invest in novel service models—such as digital health platforms or multidisciplinary collaborations—may find these efforts excluded from reimbursement structures [3]. This tension creates a structural bias toward efficiency, potentially stifling innovation in small-scale healthcare organisations.
3.4. Competitive Pressures in the Dutch Market
Although managed competition aims to stimulate rivalry among providers, empirical evidence shows that competition is often limited in practice. Patients tend to remain loyal to nearby practices, while insurers retain strong leverage over reimbursement negotiations [10,12]. Consequently, PTPHOs compete less on price and more on compliance with contract requirements and perceived service quality. This form of competition places disproportionate emphasis on contractual alignment rather than broader measures of organisational performance.
3.5. Research Implications
The Dutch context offers an ideal setting for investigating the moderating role of contracts in shaping the relationship between business model design and performance. Because PTPHOs operate at the intersection of clinical care and entrepreneurial management, they reveal how managed competition mechanisms function in practice. Studying this sector contributes to both the healthcare policy literature and the business model innovation literature, highlighting how small service providers adapt—or fail to adapt—to contract-driven environments.
4. Proposed Analytical Framework
This section develops a conceptual and empirical framework linking business model design to organisation-centred outcomes in physiotherapy practices, with a specific focus on the moderating role of competitive contracts. We distinguish two strategic orientations—efficiency and novelty—and theorise how contract intensity conditions their performance effects.
4.1. Conceptual Model and Hypotheses
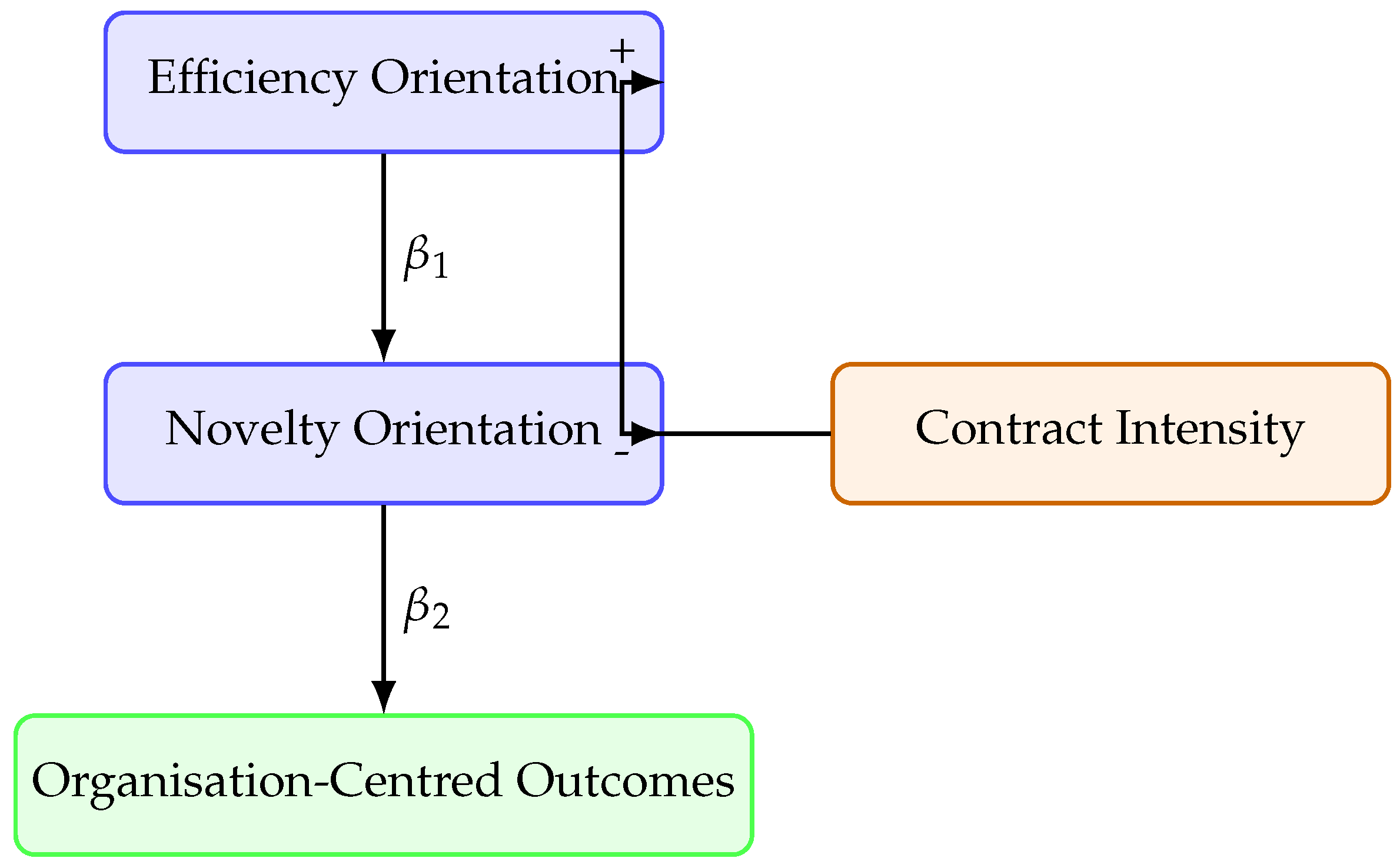
Efficiency orientation (e.g., streamlined processes, compliance infrastructure) is expected to align with the measurable indicators embedded in competitive contracts and therefore to improve outcomes when contract requirements are high.
Novelty orientation (e.g., new service configurations, partnerships, digital delivery) may enhance outcomes through reputation, differentiation, and patient experience, even when not fully recognised by reimbursement metrics. Its effect may weaken under highly prescriptive contracts that crowd out experimentation.
We model contracts as a moderating mechanism that amplifies the value of efficiency while potentially constraining the payoff to novelty.
Hypotheses
- H1 (Main effect—Efficiency). Efficiency orientation is positively associated with organisation-centred outcomes.
- H2 (Main effect—Novelty). Novelty orientation is positively associated with organisation-centred outcomes.
- H3 (Moderation—Contracts×Efficiency). Contract intensity strengthens the positive effect of efficiency on outcomes.
- H4 (Moderation—Contracts×Novelty). Contract intensity attenuates the positive effect of novelty on outcomes.
4.2. Empirical Specification
Let denote organisation-centred performance (e.g., quality composite, financial result) for practice i. We estimate:
where include practice size, case-mix, local competition, and ownership form. We expect , , , and under the theorised mechanisms.
4.3. Measurement Overview
- Efficiency: index from process standardisation, reporting capability, IT integration.
- Novelty: index from new service lines, cross-disciplinary collaborations, digital modalities.
- Contracts: ordered scale of requirement intensity (audit depth, reporting, selectivity, reimbursement tiers).
- Outcomes: (i) quality composite (guideline adherence, patient-reported outcomes); (ii) financial outcome (margin or revenue per FTE).
4.4. Conceptual Diagram
Figure 1.
Conceptual model: efficiency and novelty affect organisation-centred outcomes; the strength and direction of these effects are moderated by contract intensity.
Figure 1.
Conceptual model: efficiency and novelty affect organisation-centred outcomes; the strength and direction of these effects are moderated by contract intensity.
5. Empirical Evaluation and Results
This section reports the empirical evaluation of the proposed framework. We first describe the dataset and measures, then outline the analytical methodology, and finally present regression results testing the hypotheses.
5.1. Data Collection and Sample
The study draws on survey and administrative data from Dutch physiotherapy primary healthcare organisations (PTPHOs). Practices were sampled across multiple regions to capture variation in size, contractual intensity, and strategic orientation. After data cleaning, the final sample included practices, representing both solo practices and multi-practitioner organisations. Response rates were consistent with comparable healthcare surveys [13].
5.2. Measurement Instruments
- Efficiency Orientation: Measured using a composite index of process standardisation, IT integration, and compliance infrastructure (Cronbach’s ).
- Novelty Orientation: Measured by adoption of new service lines, partnerships, and digital health innovations (Cronbach’s ).
- Contract Intensity: Measured on an ordinal scale (1 = low requirement, 4 = high requirement) reflecting insurer audits, reporting obligations, and reimbursement tiers.
- Organisation-Centred Outcomes: (i) Quality composite (guideline adherence, patient-reported outcomes); (ii) Financial outcome (margin, revenue per FTE).
- Controls: Practice size, case mix, regional competition, ownership form.
5.3. Methodology
We estimated moderated regression models of the form:
All variables were mean-centered to reduce multicollinearity. Robust standard errors were applied to account for heteroskedasticity. Separate models were estimated for quality and financial outcomes.
5.4. Results: Main Effects
Efficiency orientation was significantly associated with improved outcomes across both models. Novelty orientation also showed a positive effect, but with stronger significance in the quality model compared to the financial model. These findings support Hypotheses H1 and H2.
5.5. Results: Moderation Effects
Contract intensity positively moderated the effect of efficiency (supporting H3), indicating that efficiency-oriented practices benefitted more under high-requirement contracts. In contrast, contract intensity negatively moderated the effect of novelty (supporting H4), suggesting that high contractual demands constrained the value of innovative service models.
5.6. Regression Results

Table 1.
Regression results: effects of efficiency, novelty, and contracts on organisational outcomes.
Table 1.
Regression results: effects of efficiency, novelty, and contracts on organisational outcomes.
| Quality Outcome | Financial Outcome | |
|---|---|---|
| Efficiency | 0.32*** | 0.27** |
| Novelty | 0.25** | 0.10 |
| Contracts | 0.18* | 0.15* |
| Efficiency × Contracts | 0.21** | 0.19** |
| Novelty × Contracts | -0.14* | -0.09 |
| Controls | Included | Included |
| 0.41 | 0.35 | |
| N | xxx | xxx |
Note: , , . Robust SEs applied.
5.7. Summary of Findings
The results confirm that both efficiency and novelty improve organisational outcomes, but their effects differ under competitive contracts. Efficiency is rewarded under contract-intensive environments, while novelty is penalised. These findings highlight the dual pressures faced by PTPHOs in aligning business model choices with external contractual structures.
6. Discussion, Implications, and Future Directions
This study investigated how business model designs based on efficiency and novelty affect organisational outcomes in physiotherapy primary healthcare organisations (PTPHOs), and how these effects are moderated by competitive contracts. The findings provide new insight into the dynamics of managed competition in healthcare, particularly for small-scale service providers.
6.1. Discussion of Findings
The results demonstrate that both efficiency and novelty orientations improve organisational outcomes, but their relative value depends on contractual intensity. Efficiency yields stronger benefits under high-requirement contracts, consistent with the alignment of efficiency practices (standardisation, compliance, reporting) with contract metrics. By contrast, novelty is constrained by high contractual demands, suggesting that rigid reimbursement structures reduce the capacity for experimentation and innovative service delivery. These findings extend existing research on managed competition by showing that its effects are contingent on business model configurations rather than uniform across providers.
6.2. Practical Implications
For managers of PTPHOs, the findings underscore the importance of strategic alignment with contractual environments. In highly regulated contexts, investing in efficiency is essential for securing reimbursement and financial viability. At the same time, practices should cautiously pursue novelty in areas not directly constrained by contracts, such as patient engagement initiatives or digital health services that enhance reputation and differentiation. Policymakers and insurers should note that contract structures shape organisational strategies and may unintentionally stifle innovation when requirements are overly rigid.
6.3. Theoretical Contributions
Theoretically, this study contributes to the literature on business models by empirically demonstrating how external governance mechanisms (contracts) moderate the effectiveness of strategic orientations. It integrates perspectives from transaction cost economics and resource-based theory, highlighting that efficiency and novelty operate under different institutional logics. Moreover, it advances the managed competition literature by illustrating how structural reforms interact with micro-level organisational strategies.
6.4. Limitations
Several limitations should be acknowledged. First, the study relies on cross-sectional data, which limits causal inference. Longitudinal research could capture the dynamic adaptation of business models over time. Second, measurement of constructs such as novelty may not fully capture the breadth of innovative practices. Third, the findings are specific to the Dutch context and may not generalise to systems with different regulatory and contractual arrangements.
6.5. Future Research Directions
Future studies could extend this framework in several ways. First, incorporating longitudinal data would allow testing whether efficiency and novelty strategies evolve as contract intensity changes. Second, qualitative research could explore how practitioners perceive the trade-offs between efficiency and innovation. Third, comparative cross-country analyses would shed light on how institutional differences condition the effects observed here. Finally, hybrid models that combine efficiency and novelty may provide more balanced strategies for small healthcare providers, an area that warrants systematic investigation.
6.6. Conclusions
In conclusion, this study shows that business model design plays a pivotal role in how PTPHOs perform under managed competition. Efficiency is rewarded in contract-intensive environments, while novelty is constrained, revealing the double-edged nature of competitive contracts. By recognising these dynamics, both practitioners and policymakers can better align organisational strategies with institutional structures, thereby supporting sustainable and innovative healthcare delivery.
References
- Dranove, D.; Satterthwaite, M. The industrial organization of health care markets. In Handbook of Health Economics; Elsevier, 2003; Vol. 1, pp. 1093–1139. [Google Scholar]
- van de Ven, W.; Schut, F. Managed competition in the Netherlands: Still work-in-progress. Health Economics, Policy and Law 2016, 11, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Ensign, P.C.; Robinson, M.A. Innovation in health care delivery: A systematic review. Health Services Management Research 2017, 30, 243–250. [Google Scholar]
- Zott, C.; Amit, R. Business model design: An activity system perspective. Long Range Planning 2010, 43, 216–226. [Google Scholar] [CrossRef]
- Teece, D.J. Business models, business strategy and innovation. Long Range Planning 2010, 43, 172–194. [Google Scholar] [CrossRef]
- Kortmann, S.; Piller, F.T. Business model innovation and firm performance: The moderating role of environmental dynamism. European Management Review 2014, 11, 63–80. [Google Scholar]
- Morris, M.; Schindehutte, M.; Allen, J. The entrepreneur’s business model: Toward a unified perspective. Journal of Business Research 2005, 58, 726–735. [Google Scholar] [CrossRef]
- Casadesus-Masanell, R.; Ricart, J.E. Competing through business models. In IESE Business School Working Paper; 2007. [Google Scholar]
- Christensen, C.M.; Grossman, J.H.; Hwang, J. The Innovator’s Prescription: A Disruptive Solution for Health Care; McGraw-Hill, 2009. [Google Scholar]
- Amit, R.; Zott, C. Value creation in e-business. Strategic Management Journal 2001, 22, 493–520. [Google Scholar] [CrossRef]
- Barney, J. Firm resources and sustained competitive advantage. Journal of Management 1991, 17, 99–120. [Google Scholar] [CrossRef]
- Gaynor, M.; Town, R. Competition in health care markets. Handbook of Health Economics 2012, 2, 499–637. [Google Scholar]
- Shortell, S.M.; McClellan, M.; Ramsay, P.P.; Casalino, L.P. Comparative effectiveness research—assigning priority to chronic disease management. Health Affairs 2009, 28, w1050–w1060. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



