
Submitted:
23 December 2025
Posted:
24 December 2025
You are already at the latest version
Abstract
Background:
Diabetes is a growing public health concern worldwide, with an estimated 537 million people affected in 2021. This number is projected to increase by 46% over the next 25 years. In the Americas, the prevalence of diabetes is expected to rise from 84 million in 2021 to 112 million by 2045. Indigenous populations may face unique risk factors, yet there is limited consolidated data on diabetes prevalence within these communities. This systematic review examines the prevalence of diabetes among Indigenous populations in the Americas.
Methods:
Following PRISMA-ScR guidelines, a systematic search was conducted in Scopus and PubMed. Studies were included if they reported population-based surveys on diabetes prevalence among Indigenous and mestizo adults in the Americas. Data extraction focused on study location, population characteristics, diagnostic criteria, and reported prevalence.
Results:
A total of 60 documents, representing 73 studies, met the inclusion criteria and covered 45,503 individuals from 16 countries between 1975 and 2025. Mexico contributed the largest number of studies (17), followed by the United States (15), Brazil (10), Canada (7), Chile (6), and Guatemala (5). Most participants were from North America (29,093), followed by Central America (8,144) and South America (6,911). No eligible reports were identified from Caribbean nations, Peru, or Guyana. In total, 111 Indigenous groups were represented. The most frequently used diagnostic method was fasting blood glucose (FBG), applied in 50 studies (75%), followed by the oral glucose tolerance test (OGTT) in 41 studies (61%). The combined prevalence of diabetes among Indigenous and mestizo populations was 12% overall (17% among women and 14% among men). Mean diabetes prevalence was highest in North America (17%), followed by Central America (8.9%) and South America (4.9%). Notably, five studies—from Brazil, Chile, Colombia, Mexico, and Paraguay—reported no cases of diabetes.
Conclusions:
The prevalence of diabetes among Indigenous populations in the Americas is highly heterogeneous, with considerably higher rates reported in North America compared with Central and South America. Although genetic predisposition may play an important role, environmental and lifestyle factors likely contribute substantially to these differences. The decline in published studies in recent years suggests a reduction in research focus on this topic. Further investigation into modifiable risk factors—such as diet, physical activity, and socioeconomic conditions—is essential to better understand the epidemiology of diabetes, clarify how these determinants interact, and support the development of targeted interventions to reduce risk and address health disparities among Indigenous populations across the region.
Keywords: Diabetes, Indigenous populations, Americas, epidemiology, public health, prevalence, systematic review.
Keywords:
indigenous populations
; native Americans
; diabetes prevalence
; health disparities
; population heterogeneity
; personalized medicine
; precision public health
; ethnic diversity
; Americas
; scoping review
; epidemiology
Introduction
The global prevalence of diabetes was estimated at 589 million people between the ages of 20 and 79 years, in 2024 and this number is projected to increase by 46% over the next 25 years. In the Americas, approximately 92 million people were living with diabetes in 2024, with forecasts predicting an increase to 120 million by 2050.
Diabetes manifests in two primary clinical forms, and although its exact cause remains unknown, each type has distinct risk factors. The rising global prevalence of diabetes is largely driven by the increasing incidence of type 2 diabetes, which is associated with both modifiable and non-modifiable risk factors. Modifiable risk factors include overweight or obesity, physical inactivity, and poor nutrition, while non-modifiable factors primarily involve age and genetic predisposition.
Before Europeans came to America, the Indigenous population was estimated to have ranged from 43–60 million people in conservative reconstructions to 90–110 million in high-end demographic models[1,2]. They were organized into thousands of distinct peoples, speaking more than 1,000 Indigenous languages [3,4]. This period represented one of the richest concentrations of linguistic diversity in the world. The demographic collapse that followed the 16th century—driven by epidemics, warfare, forced labor, and displacement—reduced many nations to fragments of their former size, with entire language families disappearing [1,2,5,6].
Historically, an increased prevalence of diabetes has been documented among Native populations in North America. One of the highest recorded rates has been observed in the Pima Indians of Arizona [7,8]. For years, research has emphasized the critical contribution of genetic susceptibility to type 2 diabetes, especially when compounded by adverse environmental conditions [9].
Understanding the scope, trends, and risk factors of diabetes in the Indigenous populations of the Americas is crucial for identifying research gaps and guiding future studies. By summarizing existing data, this systematic review aims to provide an evidence-based foundation to improve health outcomes and reduce disparities. The objective of this study is to identify reports on the prevalence of diabetes in adult Indigenous populations across the Americas.
Materials & Methods
Registration: Registered with the Open Science Framework (OSF): https://osf.io/jwshk/?view_only=faa24d3d587346f0bbf705ff1da61db0.
This systematic review was designed to address the following research question: What is the prevalence of diagnosed and undiagnosed diabetes among the adult Indigenous populations of the Americas?
The search strategy adheres to PRISMA guidelines for systematic reviews [10]. Specifically, this study follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR). In accordance with these guidelines, the study protocol was prospectively registered with the Open Science Framework (OSF): https://osf.io/jwshk/?view_only=faa24d3d587346f0bbf705ff1da61db0.
Search strategy
The literature search was conducted using PubMed and Scopus with the following keywords:
(TITLE-ABS-KEY(indigenous) OR TITLE-ABS-KEY(aboriginal) OR TITLE-ABS-KEY(indian) AND TITLE-ABS-KEY(diabetes prevalence) AND TITLE-ABS-KEY(america) OR TITLE-ABS-KEY(mexico) OR TITLE-ABS-KEY(belize) OR TITLE-ABS-KEY(guatemala) OR TITLE-ABS-KEY(el AND salvador) OR TITLE-ABS-KEY(honduras) OR TITLE-ABS-KEY(nicaragua) OR TITLE-ABS-KEY(costa AND rica) OR TITLE-ABS-KEY(panama) OR TITLE-ABS-KEY(colombia) OR TITLE-ABS-KEY(venezuela) OR TITLE-ABS-KEY(peru) OR TITLE-ABS-KEY(bolivia) OR TITLE-ABS-KEY(ecuador) OR TITLE-ABS-KEY(chile) OR TITLE-ABS-KEY(paraguay) OR TITLE-ABS-KEY(argentina) OR TITLE-ABS-KEY(uruguay) OR TITLE-ABS-KEY(brazil) OR TITLE-ABS-KEY(guyana) OR TITLE-ABS-KEY(suriname) OR TITLE-ABS-KEY (united states) OR TITLE-ABS-KEY (canada) OR TITLE-ABS-KEY (puerto rico) OR TITLE-ABS-KEY (cuba) OR TITLE-ABS-KEY (dominican) OR TITLE-ABS-KEY (dominicana) OR TITLE-ABS-KEY (haiti) OR TITLE-ABS-KEY (jamaica) OR TITLE-ABS-KEY (trinidad) OR TITLE-ABS-KEY (grenada))
In addition, we conducted an internet search for relevant gray literature, including documents from governmental and academic institutions. We also reviewed citations from the retrieved documents to identify additional reports meeting the inclusion criteria that may have been overlooked in the systematic review. Furthermore, articles that met the inclusion criteria and were identified in a previous search [11] were also included.

Table 1.
World Health Organization criteria for the diagnosis of diabetes mellitus, 1985, 2003-2006 and 2011.
Table 1.
World Health Organization criteria for the diagnosis of diabetes mellitus, 1985, 2003-2006 and 2011.
| Test | 1985 WHO Criteria[12] | 1999 WHO Criteria [13] | 2003, 2006 WHO Criteria [14,15] | 2011 WHO Criteria [16] |
| Fasting Blood Glucose (FBG) | ≥ 140 mg/dl (7.8 mmol/l) | ≥ 126 mg/dl (7.0 mmol/l) | ≥ 126 mg/dl (7.0 mmol/l) | ≥ 126 mg/dl (7.0 mmol/l) |
| Oral Glucose Tolerance Test (OGTT) | ≥200 mg/dl (11.1 mm/l | ≥200 mg/dl (11.1 mm/l) | ≥200 mg/dl (11.1 mm/l) | ≥200 mg/dl (11.1 mm/l) |
| HbA1c | - | - | - | ≥6.5% |
Article Selection
A comprehensive search was conducted for relevant documents from all countries in the Americas, restricted to publications from 1975 through 2025. The search was completed in July 2025. The inclusion criteria required original documents that:
(a) described a population-based survey of diabetes prevalence among adult native, indigenous, or mestizo populations of both genders (or a subpopulation);
(b) employed an unbiased, adequate population-based sampling procedure (probabilistic sample, cluster sample, or census);
(c) reported prevalence rates in percentage;
(d) included total diabetes prevalence (diagnosed plus newly identified cases) using international diagnostic blood glucose standards and tests available at the time of the study (as shown in Figure 1); and
(e) were published in English, Spanish, French, or Portuguese between 1975 and 2025.
Studies were excluded if they exhibited any source of selection bias, such as non-random samples or clinical series. All retrieved articles were independently reviewed by three reviewers.
Data Extraction
Data were independently extracted using a predefined template by the two reviewers (ES, FC, RWM, NCB). Discrepancies were resolved by a third reviewer (AB) before finalizing the dataset. Extracted data points included country, author, study site, year of study, year of publication, ethnic group, age, sample size, diagnostic test, diagnostic method and values, and prevalence rate.
Data Analysis
The extracted data on the prevalence of diabetes among indigenous populations in the Americas were analyzed descriptively. Prevalence rates were compared by study year (or publication year if the study year was unavailable), country, subregion, diagnostic test, diagnostic criteria and values, and gender.
To address measurement heterogeneity, all summaries were stratified by diagnostic test Fasting Blood Glucose (FBG), Oral Glucose Tolerance Test (OGTT), Casual (or random) Glucose Test (CGT) or Hemoglobin A1c (HbA1c) and diagnostic criteria (WHO 1985/1999/2003–06/2011).
Primary Effect Measure
The primary effect measure in this review was the prevalence of diabetes mellitus, expressed as the percentage of participants with diabetes in each included study population (diagnosed and undiagnosed combined). Where available, we reported sex-specific prevalence (men, women, both), as well as 95% confidence intervals provided in the original studies. We did not calculate pooled effect sizes because of substantial heterogeneity across populations, diagnostic tests, and time periods. Instead, we present prevalence estimates descriptively and stratify by country, region, sex, diagnostic test, and diagnostic criteria.
Results
Ascertainment
The search across Scopus, PubMed, and additional sources identified 2,267 documents. After screening and eligibility assessment to identify valid population-based surveys reporting both diagnosed and undiagnosed diabetes among Indigenous and mestizo populations in the Americas, 60 documents—representing 73 distinct studies—met the inclusion criteria (Figure 1).
Articles published between 1975 and 2025 were included. Although studies predating 1975 were reviewed, they were excluded because standardized blood glucose thresholds aligned with the 1979 American Diabetes Data Group (ADDG) and 1985 WHO diagnostic criteria were not systematically applied before the mid-1970s.
As summarized in Table 2, Mexico contributed the largest number of studies (n=16), followed by the United States (n=15), Brazil (n=10), Canada (n=7), Chile (n=6), Guatemala (n=5), and Colombia (n=3). Two studies were conducted in Bolivia and Panama respectively, while seven other countries each contributed one study. Altogether, 44,148 individuals were screened between 1975 and 2025. Most study participants were from North America (n=29,093), followed by Central America (n=8,144) and South America (n=6,911). No eligible studies were identified from Caribbean nations, Costa Rica, El Salvador, Guyana, Peru, Uruguay, or Venezuela.
Only one study was conducted between 1975 and 1979. The highest number of studies were carried out between 1990–1999 and 2001–2010 (n=23 each). Only one study was published after 2020.
Indigenous Groups
Across all studies, 111 Indigenous groups were represented (Supplementary Table S1). Nine studies classified participants under broader labels such as Indigenous, mestizo, or Amerindian (including those from Belize, Ecuador, Guatemala, Honduras, Mexico, Nicaragua, and Panama). The Pima Indians were most frequently represented, included in six studies (three in the United States and three in Mexico).
Blood Processing Method and Diagnostic Test
Most studies (47/64; 73%) used venous blood samples analyzed in laboratory settings, while 16 studies (24%) relied on capillary finger-prick methods; two studies did not report the blood processing method. Fasting blood glucose (FBG) was the most common diagnostic test (n=50; 75%), followed by oral glucose tolerance testing (OGTT) (n=41; 61%). Glycated hemoglobin (HbA1c) was used in 9 studies (13%). Nearly half of the studies (n=29; 43%) used both FBG and OGTT in combination (Supplementary Table S2).
Prevalence of Diabetes
The Overall mean prevalence of diabetes among Indigenous and mestizo populations in the Americas was 12% (14% among men and 17% among women). The highest reported prevalence—70%—occurred in 1995 among Native American groups in Arizona (Pima, Maricopa, and Tohono O’odham), with sex-specific estimates of 65% in men and 72% in women. Other high-burden areas included Indigenous groups in Delaware (Apache, Caddo, Comanche) and the Dakotas (Oglala Sioux, Cheyenne River Sioux, and Devils Lake Sioux), where prevalence reached 40% in 1995. In the same year, Delisle et al. reported a prevalence of diabetes of 23.9% in men and 48.6% in women among First Nations groups in Quebec, Canada. In contrast, five studies—conducted in Brazil, Chile, Colombia, Mexico, and Paraguay—reported zero diabetes cases, four of which were conducted between 1990 and 1999 and one in 2011.
Marked geographic disparities were observed. Indigenous populations in the United States and Canada exhibited high mean prevalence estimates (32% and 25%, respectively), while studies in Belize (11%), Nicaragua (10%), Mexico (9%), and Panama (9%) suggested intermediate levels. In South America, prevalence was generally lower, ranging from 0.6% in Argentina to 8% in Brazil. Across the region, mean prevalence was highest in North America (17%), followed by Central America (9%) and South America (5%). A notable exception in South America was observed among the Xavante in Brazil, who exhibited a prevalence of 29% in 2014 (18% in men; 41% in women).
Obesity and Diabetes Clustering
Forty-eight studies (71%) reported mean BMI or the prevalence of obesity (BMI≥30 Km/m2). The prevalence of Diabetes increased in parallel with higher mean BMI or greater proportion of obesity. One exception was a study in Chile [40], which reported low diabetes prevalence despite a mean BMI > 25 kg/m² (Supplementary Tables S3–S5). Clusters of elevated diabetes were consistently found in groups with high prevalence of obesity (Supplementary Table S6).
Sampling methods
Random or cluster sampling was used in 45 studies (62%), while 20 studies (27%) relied on volunteer or invitation-based recruitment. Across the Americas, random/cluster sampling yielded lower diabetes prevalence estimates (combined: 10% among participants of both genders) compared with volunteer-based sampling (combined: 14%). In the United States, the difference was especially pronounced: both gender prevalence of DM of 24% (random/cluster) vs. 55% (volunteers).
Volunteer-based sampling (Supplementary table S7) was most common in Mexico (23%; n=5), followed by Chile and the United States (18%; n=4 each), Brazil and Canada (14%; n=3 each), and Colombia (5%; n=1). Nineteen out of 20 studies (95%) reported response rates. The overall mean response rate was 62% (Supplementary Table S7). Two studies from Brazil—conducted among the Parkatejé and Suyá Indigenous groups—reported the highest response rates at 90%. In contrast, three studies—two from Canada (both involving Ojibway communities) and one from Colombia (Arahuaco)—reported response rates below 50%.
Discussion
This review provides a comprehensive synthesis of 50 years of research conducted between 1975 and 2025 across 16 countries in the Americas. Our findings reveal marked heterogeneity across countries, Indigenous groups, and time periods, underscoring the limitations of treating Indigenous populations as a single epidemiological category. This heterogeneity reflects the combined influence of genetic susceptibility, environmental and socioeconomic contexts, and historical trajectories, as well as differences in diagnostic approaches and sampling methodologies. Accordingly, these findings align with emerging personalized medicine and precision public health frameworks, as well as with international consensus recommendations from the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD)[77,78], which emphasize diabetes strategies tailored to distinct population contexts rather than one-size-fits-all models [77,78,79,80].
Given the wide variation in diabetes frequency across Indigenous groups, along with differences in diagnostic and sampling techniques and the influence of both genetic and modifiable factors that cannot be fully controlled, it is difficult to draw firm conclusions about the true magnitude of variation in diabetes prevalence. Nevertheless, the heterogeneity observed in this review has important implications for personalized medicine and precision public health. The wide variation in diabetes prevalence across Indigenous groups highlights the need for standardized methodologies to measure disease frequency, while simultaneously underscoring the importance of tailored approaches to diabetes prevention and management that take into account environmental, nutritional, and social determinants of health.
By around 1975, the initial year covered by this review, the Indigenous population of the Americas had begun to recover from the severe demographic decline experienced during colonization. Although no hemisphere-wide census existed at that time, regional estimates indicate the presence of tens of millions of Indigenous people across North, Central, and South America, with the largest concentrations in Mexico, Central America, the Andean region, and parts of North America[81,82,83]. By contrast, by 2024–2025, the end of the review period, the Indigenous population is more robust and better documented, with over 58 million Indigenous people in Latin America[81,82,83], 574 federally recognized tribes in the United States[84], and more than 70 First Nations and other native peoples in Canada[85]. In total, this amounts to more than 800 Indigenous peoples in Latin America alone and over 1,000 distinct Indigenous groups across the hemisphere when North American nations and uncontacted Amazonian peoples are included[81,82,84,85].
A major challenge encountered in this review stems from the substantial variability across studies in age distributions, methodological approaches, and the diagnostic cut-off points used to define diabetes. Although this methodological heterogeneity reflects an inherent historical characteristic of the published literature—spanning several decades during which diagnostic tests, classification criteria, and sampling methodologies evolved—it nonetheless limits comparability and may affect the accuracy of prevalence estimates. Despite these constraints, the application of rigorous inclusion criteria and systematic analyses provides the best attainable approximation of the prevalence of diabetes among Indigenous populations of the America, and provides insight into how shifting clinical paradigms influence disease classification within diverse populations.
Pioneering earlier studies conducted by Stein [86], Bennett [87], Henry [88] and Forman [89] in the United States, in the 1960s had previously reported unusually high prevalence of diabetes ranging from 29% to 43%, among the Cherokee, Pima, Cocopah, and Seneca ethnic groups, respectively.
For years, researchers speculated whether indigenous communities south of the U.S. border would follow the same pattern observed among the Pima Indians. This curiosity fueled many subsequent studies. However, in contrast to the strikingly high prevalence of diabetes reported in the North American[29,31,47,66,90] studies, our review suggests a lower diabetes risk among indigenous populations in Latin America, with the notable exception of a study in Brazil, where the Xavante community of Mato Grosso exhibited a prevalence of 28.8%[67].
The extreme prevalence rates observed among the Pima Indians are believed to stem from a combination of genetic predisposition and environmental factors, particularly nutrition and body mass index (BMI)[9]. While this review did not assess diabetes-related risk factors, it is well documented that, despite high obesity rates, the prevalence of diabetes remains relatively low among the Aymara tribes in Chile[91].
Comparability between studies and among native population groups is limited by the diversity of sampling techniques and diagnostic testing methods. Many studies were conducted among volunteers or respondents to open invitations, which may introduce selection bias compared with more statistically rigorous approaches such as random or cluster sampling. Because this type of bias is difficult to control, comparability across studies represents a major limitation of this review. For example, the highest prevalence of diabetes ever reported among Indigenous groups—and possibly among all populations in the Americas—was documented by Lee et al.[31] among the Pima, Maricopa, and Papago Indians of Arizona in 1995, where participants were all volunteers drawn from an official list of eligible individuals.
The greatest strength of this review is its revival of a subject that has faded from academic focus over time. By including papers from monographs and gray literature, we were able to compile the most comprehensive picture of diabetes risk among the indigenous populations of the Americas. However, this study has several unavoidable limitations, primarily the lack of rigorous detailed analysis on contributing factors such as BMI, socioeconomic conditions, cultural dietary patterns, income levels, and other modifiable risk factors. Investigating these determinants is beyond the scope of this review and should be a focus for future research. Furthermore, we did not perform a meta-analysis or calculate pooled effect sizes because the included studies exhibited substantial heterogeneity in study populations, diagnostic tests, and time periods. Instead, we adopted a descriptive approach, presenting prevalence estimates stratified by ethnic group, country, sex, diagnostic test, and diagnostic criteria. This method provides a transparent view of the variability in the prevalence of diabetes across the Americas and aligns with established recommendations for scoping reviews and prevalence studies characterized by methodological diversity. A formal meta-analysis could be considered in a subsequent stage.
As noted previously, despite the profound risks faced by Indigenous peoples of the Americas following European colonization, subsequent population growth, cultural revitalization movements, and increasing legal recognition have contributed to a demographic and cultural resurgence not witnessed since before colonial contact [81,82]. However, despite this growth, research interest in the epidemiology of diabetes among Indigenous populations has declined markedly in recent years, perhaps reflecting a contraction of funding following the golden era of North American studies in the 1970s, 1980s, and 1990s.
Conclusion
The prevalence of diabetes among Indigenous populations in the Americas is highly heterogeneous, with considerably higher rates reported in North America compared with Central and South America. Although genetic predisposition may play an important role, environmental and lifestyle factors likely contribute substantially to these differences. The decline in published studies in recent years suggests a reduction in research focus on this topic. Further investigation into modifiable risk factors—such as diet, physical activity, and socioeconomic conditions—is essential to better understand the epidemiology of diabetes, clarify how these determinants interact, and support the development of targeted interventions to reduce risk and address health disparities among Indigenous populations across the region.
Overall, the observed heterogeneity in diabetes prevalence across Indigenous populations emphasizes the importance the use of standardized methodologies to accurately measure disease prevalence, which are essential for informing personalized care and precision public health approaches to prevention, tailored to the specific environmental and sociocultural contexts of distinct Indigenous groups. These findings align with emerging approaches to personalized diabetes care and precision public health strategies.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/doi/s1, Table S1: Diagnosis test used for the studies of diabetes in indigenous population of the Americas by country; Table S2: Ethnic groups represented in studies of diabetes among indigenous in the Americas by country; Table S3: Body Mass Index and the prevalence of diabetes among indigenous populations of the Americas among males; Table S4: Body Mass Index and the prevalence of diabetes among indigenous populations of the Americas among females; Table S5: Body Mass Index and the prevalence of diabetes among indigenous populations of the Americas among males and females; Table S6: Obesity (%) and the prevalence of diabetes (%) by study and gender in indigenous populations of the Americas; Table S7: Response rate (%) to open invitations by studies of diabetes in indigenous populations in the Americas.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions presented in this study are included in the article and supplementary material. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Denevan, WM. The Native Population of the Americas in 1492; University of Wisconsin Press: Madison, 1976. [Google Scholar]
- Dobyns, HF. Estimating aboriginal American population: An appraisal of techniques with a new hemispheric estimate. Current Anthropology 1966, 7(4), 395–416. [Google Scholar] [CrossRef]
- Campbell, L. American Indian Languages: The Historical Linguistics of Native America; Oxford University Press: New York, 1997. [Google Scholar]
- Eberhard, DM; Simons, GF; Fennig, CD. Ethnologue: Languages of the World; SIL International: Dallas, 2023. [Google Scholar]
- Moseley, C. Atlas of the World’s Languages in Danger; UNESCO Publishing: Paris, 2010. [Google Scholar]
- Nettle, D; Romaine, S. Vanishing Voices: The Extinction of the World’s Languages; Oxford University Press: New York, 2000. [Google Scholar]
- Knowler, WC; Saad, MF; Pettitt, DJ; Nelson, RG; Bennett, PH. Determinants of diabetes mellitus in the Pima Indians. Diabetes Care;PubMed 1993, 16(1), 216–27. [Google Scholar] [CrossRef] [PubMed]
- Pavkov, ME; Hanson, RL; Knowler, WC; Bennett, PH; Krakoff, J; Nelson, RG. Changing patterns of type 2 diabetes incidence among Pima Indians. In Diabetes Care; PubMed, 2007; Volume 30, 7, pp. 1758–63. [Google Scholar] [CrossRef] [PubMed]
- Baier, LJ; Hanson, RL. Genetic Studies of the Etiology of Type 2 Diabetes in Pima Indians: Hunting for Pieces to a Complicated Puzzle. Diabetes 2004, 53(5), 1181–6. [Google Scholar] [CrossRef] [PubMed]
- Page, MJ; McKenzie, JE; Bossuyt, PM; Boutron, I; Hoffmann, TC; Mulrow, CD; et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ (Clinical research ed). 2021;372:n71. Epub 2021/03/31. doi: 10.1136/bmj.n71. PubMed PMID: 33782057; PubMed Central PMCID: PMCPMC8005924 at http://www.icmje.org/conflicts-of-interest/ and declare: EL is head of research for the BMJ; MJP is an editorial board member for PLOS Medicine; ACT is an associate editor and MJP, TL, EMW, and DM are editorial board members for the Journal of Clinical Epidemiology; DM and LAS were editors in chief, LS, JMT, and ACT are associate editors, and JG is an editorial board member for Systematic Reviews. None of these authors were involved in the peer review process or decision to publish. TCH has received personal fees from Elsevier outside the submitted work. EMW has received personal fees from the American Journal for Public Health, for which he is the editor for systematic reviews. VW is editor in chief of the Campbell Collaboration, which produces systematic reviews, and co-convenor of the Campbell and Cochrane equity methods group. DM is chair of the EQUATOR Network, IB is adjunct director of the French EQUATOR Centre and TCH is co-director of the Australasian EQUATOR Centre, which advocates for the use of reporting guidelines to improve the quality of reporting in research articles. JMT received salary from Evidence Partners, creator of DistillerSR software for systematic reviews; Evidence Partners was not involved in the design or outcomes of the statement, and the views expressed solely represent those of the author.
- Barceló, A. Diabetes in the Americas. Epidemiological bulletin 2001, 22(2), 1–3. [Google Scholar]
- World Health Organization (WHO). Diabetes Mellitus: Report of a WHO Study Group. In Tech. Rep. Ser.; World Health Org.: Geneva, 1985; Volume no. 727. [Google Scholar]
- World Health Organization Consultation-Group. Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications. Part 1. Diagnosis and Classification of Diabetes Mellitus; World Health Org.: Geneva, 1999. [Google Scholar]
- World Health Organization. Chronic Respiratory D, Arthritis T. Screening for type 2 diabetes: report of a World Health Organization and International Diabetes Federation meeting; World Health Organization: Geneva, 2003. [Google Scholar]
- World Health Organization. Definition and diagnosis of diabetes mellitus and intermediate hyperglycemia: report of a WHO/IDF consultation. ISBN 92 4 159493 4; © World Health Organization, 2006. [Google Scholar]
- WHO Guidelines Approved by the Guidelines Review Committee. Use of Glycated Haemoglobin (HbA1c) in the Diagnosis of Diabetes Mellitus: Abbreviated Report of a WHO Consultation; World Health Organization, Copyright © World Health Organization: Geneva, 2011. [Google Scholar]
- Knowler, WC; Bennett, PH; Hamman, RF; Miller, M. Diabetes incidence and prevalence in Pima Indians: a 19-fold greater incidence than in Rochester, Minnesota. In Am J Epidemiol.; PubMed, 1978; Volume 108, 6, pp. 497–505. [Google Scholar] [CrossRef] [PubMed]
- Larenas, G; Arias, G; Espinoza, O; Charles, M; Landaeta, O; Villanueva, S; et al. Prevalence of diabetes mellitus in a Mapuche community of Region IX, Chile. Revista medica de Chile 1985, 113(11), 1121–5. [Google Scholar]
- Young, TK; Sevenhuysen, GP; Ling, N; Moffatt, ME. Determinants of plasma glucose level and diabetic status in a northern Canadian Indian population. Cmaj 1990, 142(8), 821–30. [Google Scholar] [PubMed Central]
- Rith-Najarian, SJ; Valway, SE; Gohdes, DM. Diabetes in a northern Minnesota Chippewa tribe: Prevalence and incidence of diabetes and incidence of major complications, 1986-1988. Diabetes Care 1993, 16(1), 266–70. [Google Scholar] [CrossRef]
- Sugarman, J; Percy, C. Prevalence of diabetes in a Navajo Indian community. Am J Public Health;PubMed Central 1989, 79(4), 511–3. [Google Scholar] [CrossRef] [PubMed Central]
- Hall, TR; Hickey, ME; Young, TB. Evidence for recent increases in obesity and non-insulin-dependent diabetes mellitus in a Navajo community. In Am J Hum Biol.; PubMed, 1992; Volume 4, 4, pp. 547–53. [Google Scholar] [CrossRef] [PubMed]
- Sugarman, JR; Gilbert, TJ; Weiss, NS. Prevalence of diabetes and impaired glucose tolerance among Navajo Indians. In Diabetes Care; PubMed, 1992; Volume 15, 1, pp. 114–20. [Google Scholar] [CrossRef] [PubMed]
- Welty, TK; Rhoades, DA; Yeh, F; Lee, ET; Cowan, LD; Fabsitz, RR; et al. Changes in cardiovascular disease risk factors among American Indians: The Strong Heart Study. Annals of Epidemiology 2002, 12(2), 97–106. [Google Scholar] [CrossRef]
- Campos-Outcalt, D; Ellis, J; Aickin, M; Valencia, J; Wunsch, M; Steele, L. Prevalence of cardiovascular disease risk factors in a southwestern Native American tribe. Public Health Rep.;PubMed Central 1995, 110(6), 742–8. [Google Scholar] [PubMed] [PubMed Central]
- Will, JC; Strauss, KF; Mendlein, JM; Ballew, C; White, LL; Peter, DG. Diabetes mellitus among Navajo Indians: findings from the Navajo Health and Nutrition Survey. In J Nutr.; PubMed, 1997; Volume 127, 10 Suppl, pp. 2106S–13S. [Google Scholar] [CrossRef] [PubMed]
- Casper, M; Rith-Najarian, S; Groft, J; Giles, W; Donehoo, R. Blood pressure, diabetes, and body mass index among Chippewa and Menominee Indians: the Inter-Tribal Heart Project Preliminary Data. In Public Health Rep.; PubMed PMID: 8898770; PubMed Central, 1996; Volume 111, Suppl 2(Suppl 2), pp. 37–9. [Google Scholar] [PubMed Central]
- Schulz, LO; Bennett, PH; Ravussin, E; Kidd, JR; Kidd, KK; Esparza, J; et al. Effects of traditional and western environments on prevalence of type 2 diabetes in Pima Indians in Mexico and the U.S. Diabetes Care. PubMed 2006, 29(8), 1866–71. [Google Scholar] [CrossRef] [PubMed]
- Delisle, HF; Ekoe, JM. Prevalence of non-insulin-dependent diabetes mellitus and impaired glucose tolerance in two Algonquin communities in Quebec. CMAJ 1993, 148(1), 41–7. [Google Scholar] [PubMed]
- Harris, SB; Gittelsohn, J; Hanley, A; Barnie, A; Wolever, TMS; Gao, J; et al. The prevalence of NIDDM and associated risk factors in native Canadians. Diabetes Care 1997, 20(2), 185–7. [Google Scholar] [CrossRef]
- Lee, ET; Howard, BV; Savage, PJ; Cowan, LD; Fabsitz, RR; Oopik, AJ; et al. Diabetes and impaired glucose tolerance in three American Indian populations aged 45-74 years. The Strong Heart Study. In Diabetes Care; PubMed, 1995; Volume 18, 5, pp. 599–610. [Google Scholar] [CrossRef] [PubMed]
- Esparza-Romero, J; Valencia, ME; Urquidez-Romero, R; Chaudhari, LS; Hanson, RL; Knowler, WC; et al. Environmentally Driven Increases in Type 2 Diabetes and Obesity in Pima Indians and Non-Pimas in Mexico Over a 15-Year Period: The Maycoba Project. Diabetes Care;PubMed 2015, 38(11), 2075–82. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Urquidez-Romero, R; Esparza-Romero, J; Chaudhari, LS; Begay, RC; Giraldo, M; Ravussin, E; et al. Study design of the Maycoba Project: obesity and diabetes in Mexican Pimas. Am J Health Behav.;PubMed 2014, 38(3), 370–8. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Guerrero-Romero, F; Rodríguez-Morán, M; Sandoval-Herrera, F. Low prevalence of non-insulin-dependent diabetes mellitus in indigenous communities of Durango, Mexico Epub 1997/04/01. In Arch Med Res.; PubMed, 1997; Volume 28, 1, pp. 137–40. [Google Scholar] [PubMed]
- Guerrero-Romero, F; Rodríguez-Moran, M; Sandoval-Herrera, F. Prevalence of NIDDM in indigenous communities of Durango, Mexico. In Diabetes Care; PubMed, 1996; Volume 19, 5, pp. 547–8. [Google Scholar] [CrossRef] [PubMed]
- Alvarado-Osuna, C; Milian-Suazo, F; Valles-Sánchez, V. Prevalence of diabetes mellitus and hyperlipidemia among Otomi indians Epub 2002/01/05. In Salud Publica Mex.; PubMed, 2001; Volume 43, 5, pp. 459–63. [Google Scholar] [PubMed]
- Briceño, I; Barriocanal, LA; Papiha, SS; Ashworth, LA; Gómez, A; Bernal, JE; et al. Lack of diabetes in rural Colombian Amerindians. In Diabetes Care; PubMed, 1996; Volume 19, 8, pp. 900–1. [Google Scholar] [CrossRef] [PubMed]
- Barceló, A; Daroca, MDC; Ribera, R; Duarte, E; Zapata, A; Vohra, M. Diabetes in Bolivia. In Revista Panamericana de Salud Publica/Pan American Journal of Public Health; PubMed Central, 2001; Volume 10, 5, pp. 318–23. [Google Scholar] [PubMed Central]
- Pérez-Bravo, F; Carrasco, E; Santos, JL; Calvillán, M; Larenas, G; Albala, C. Prevalence of type 2 diabetes and obesity in rural Mapuche population from Chile. Nutrition 2001, 17(3), 236–8. [Google Scholar] [CrossRef]
- Santos, JL; Pérez-Bravo, F; Carrasco, E; Calvillán, M; Albala, C. Low prevalence of type 2 diabetes despite a high average body mass index in the Aymara natives from Chile Epub 2001/05/23. In Nutrition; PubMed, 2001; Volume 17, 4, pp. 305–9. [Google Scholar] [CrossRef] [PubMed]
- Benítez, A; Ruffinelli, J; Echagüe de Méndez, G; Medina, U; Rojas de Arias, A; Azorero, R. Obesity, diabetes and other cardiovascular risk factors in the Ayoreos of the Paraguayan Chaco. Diabetes Research and Clinical Practice - DIABETES RES CLIN PRACT 2000, 50, 300. [Google Scholar] [CrossRef]
- Guzman Monteroso, ZM. Prevalencia de diabetes mellitus en la población indígena del departamento de Sololá (1998). Degree Thesis, Universidad de San Carlos de Guatemala. Available online: http://biblioteca.usac.edu.gt/tesis/05/05_7976.pdf (accessed on 25 September 2024).
- de Salvo, VLMA; Rodrigues, D; Baruzzi, RG; Pagliaro, H; Gimeno, SGA. Metabolic and anthropometric profile of Suyá. Xingu Indigenous Park, Central Brazil. Revista Brasileira de Epidemiologia 2009, 12(3). [Google Scholar] [CrossRef]
- Loria, A; Arroyo, P; Fernandez, V; Pardio, J; Laviada, H. Prevalence of obesity and diabetes in the socioeconomic transition of rural Mayas of Yucatan from 1962 to 2000. Ethn Health;PubMed 2020, 25(5), 679–85. [Google Scholar] [CrossRef] [PubMed]
- Tavares, EF; Vieira-Filho, JPB; Andriolo, A; Sañudo, A; Gimeno, SGA; Franco, LJ. Metabolic profile and cardiovascular risk patterns of an Indian tribe living in the Amazon Region of Brazil. Human Biology 2003, 75(1), 31–46. [Google Scholar] [CrossRef] [PubMed]
- Castro-Porras, LV; Rojas-Martinez, R; Romero-Martinez, M; Aguilar-Salinas, CA; Escamilla-Nunez, C. The Trend in the Prevalence of Diabetes Mellitus in the Mexican Indigenous Population From 2000 to 2018. AJPM Focus;PubMed Central 2023, 2(2), 100087. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Riediger, ND; Lix, LM; Lukianchuk, V; Bruce, S. Trends in diabetes and cardiometabolic conditions in a Canadian First Nation community, 2002-2003 to 2011-2012. Prev Chronic Dis.;PubMed 2014, 11, E198. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bruce, SG; Young, TK. Prevalence and risk factors for neuropathy in a canadian first nation community. Diabetes Care 2008, 31(9), 1837–41. [Google Scholar] [CrossRef]
- Gimeno, SG; Rodrigues, D; Canó, EN; Lima, EE; Schaper, M; Pagliaro, H. Cardiovascular risk factors among Brazilian Karib indigenous peoples: Upper Xingu, Central Brazil, 2000-3 Epub 20081121. J Epidemiol Community Health;PubMed 2009, 63(4), 299–304. [Google Scholar] [CrossRef] [PubMed]
- Alvim Rde, O; Mourao-Junior, CA; de Oliveira, CM; Krieger, JE; Mill, JG; Pereira, AC. Body mass index, waist circumference, body adiposity index, and risk for type 2 diabetes in two populations in Brazil: general and Amerindian Epub 2014/06/18. doi: 10.1371/journal.pone.0100223. PloS one;PubMed 2014, 9(6), e100223. [Google Scholar] [PubMed] [PubMed Central]
- Carrasco, P E; Pérez, B F; Angel, B B; Albala, B C; Santos, M JL; Larenas, Y G; et al. Prevalence of type 2 diabetes and obesity in two Chilean aboriginal populations living in urban zones. Revista Medica de Chile 2004, 132(10), 1189–97. [Google Scholar]
- Chateau-Degat, ML; Pereg, D; Egeland, GM; Nieboer, E; Bonnier-Viger, Y; Laouan-Sidi, EA. Diabetes and related metabolic conditions in an aboriginal cree community of quebec, Canada Epub 2009/01/01. In Canadian journal of diabetes; PubMed, 2009; Volume 33, 3, pp. 156–62. [Google Scholar] [CrossRef] [PubMed]
- Barcelo, A GE; Pérez Flores, E; Wong, R; Gerzoff, R; Cafiero, E; Meiners, M. The Central America Diabetes Initiative (CAMDI): Survey of Diabetes, Hypertension and Chronic Disease Risk Factors. Belize, San José, San Salvador, Guatemala City, Managua and Tegucigalpa; Pan American Health Organization: Washington DC, 2011. [Google Scholar]
- Rodriguez-Moran, M; Guerrero-Romero, F; Brito-Zurita, O; Rascon-Pacheco, RA; Perez-Fuentes, R; Sanchez-Guillen, MC. Cardiovascular risk factors and acculturation in Yaquis and Tepehuanos Indians from Mexico Epub 2008/02/19. In Arch Med Res.; PubMed, 2008; Volume 39, 3, pp. 352–7. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, GF; Oliveira, TR; Ikejiri, AT; Andraus, MP; Galvao, TF; Silva, MT; et al. Prevalence of hypertension and associated factors in an indigenous community of central Brazil: a population-based study. In PloS one; PubMed Central, 2014; Volume 9, 1. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- De Oliveira, GF; De Oliveira, TRR; Rodrigues, FF; Corrêa, LF; Ikejiri, AT; Casulari, LA. Prevalence of diabetes mellitus and impaired glucose tolerance in indigenous people from Aldeia Jaguapiru, Brazil. Revista Panamericana de Salud Publica/Pan American Journal of Public Health 2011, 29(5), 315–21. [Google Scholar] [CrossRef]
- Escobedo, J; Chavira, I; Martinez, L; Velasco, X; Escandon, C; Cabral, J. Diabetes and other glucose metabolism abnormalities in Mexican Zapotec and Mixe Indians. Diabet Med.;PubMed 2010, 27(4), 412–6. [Google Scholar] [CrossRef] [PubMed]
- Cardona Arias, JA RPY; Llanes Agudelo, OM. Prevalencia de diabetes mellitus y dislipidemias en indígenas del resguardo Cañamomo-Lomaprieta, Colombia. Investigaciones Andinas. 2011, 24, pp. 414–26. Available online: https://digitk.areandina.edu.co/server/api/core/bitstreams/e5008b4a-7756-4604-a0a5-c84779620f08/content.
- Santos, KM; Tsutsui, ML; Galvão, PP; Mazzucchetti, L; Rodrigues, D; Gimeno, SG. Degree of physical activity and metabolic syndrome: a cross-sectional study among the Khisêdjê group in the Xingu Indigenous Park, Brazil. In Cad Saude Publica; PubMed, 2012; Volume 28, 12, pp. 2327–38. [Google Scholar] [CrossRef] [PubMed]
- Claudia Navarrete, B; Cartes-Velásquez, R. Prevalence of type 2 diabetes and obesity in Pehuenches communities, Alto Biobio. Revista Chilena de Nutricion 2012, 39(3), 7–10. [Google Scholar] [CrossRef]
- Mc Donald, PA; Montenegro, GJ; Cruz, GC; Moreno de Rivera, AL; Cumbrera, OA. Prevalence, sociodemographic distribution, treatment and control of diabetes mellitus in Panama. Diabetology & metabolic syndrome;PubMed;PubMed Central 2013, 5(1), 69. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jimenez-Corona, A; Nelson, RG; Jimenez-Corona, ME; Franks, PW; Aguilar-Salinas, CA; Graue-Hernandez, EO; et al. Disparities in prediabetes and type 2 diabetes prevalence between indigenous and nonindigenous populations from Southeastern Mexico: The Comitan Study. J Clin Transl Endocrinol;PubMed 2019, 16, 100191. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bruce, SG; Riediger, ND; Zacharias, JM; Young, TK. Obesity and obesity-related comorbidities in a Canadian First Nation population. In Chronic Dis Can.; PubMed, 2010; Volume 31, 1, pp. 27–32. [Google Scholar] [PubMed]
- Chen, D; Rivera-Andrade, Á; González, J; Burt, D; Mendoza-Montano, C; Patrie, J. Prevalence of risk factors for noncommunicable diseases in an indigenous community in Santiago Atitlán, Guatemala other conflicts of interest to declare. Rev Panam Salud Publica;PubMed 2017, 41, e7. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Krishnadath, IS; Nahar-van Venrooij, LM; Jaddoe, VW; Toelsie, JR. Ethnic differences in prediabetes and diabetes in the Suriname Health Study. BMJ Open Diabetes Res Care;PubMed 2016, 4(1), e000186. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pacheco, LS; Hernandez-Ontiveros, DA; Iniguez-Stevens, E; Brodine, S; Garfein, RS; Santibanez, M; et al. Prevalence and correlates of diabetes and metabolic syndrome in a rural indigenous community in Baja California, Mexico. BMC Public Health 2018, 18(1), 1397. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dal Fabbro, AL; Franco, LJ; da Silva, AS; Sartorelli, DS; Soares, LP; Franco, LF. High prevalence of type 2 diabetes mellitus in Xavante Indians from Mato Grosso, Brazil Epub 2014/03/14. In Ethn Dis.; PubMed, 2014; Volume 24, 1, pp. 35–40. [Google Scholar] [PubMed]
- Bianchi, MEV; Velasco, GA; López, G; Cusumano, AM. Cardiovascular and renal risk factors and socioeconomics profile in individuals of the wichi ethnia group from “el impenetrable”, chaco, argentina. Revista de Nefrologia, Dialisis y Trasplante 2020, 40(3), 210–20. [Google Scholar]
- Bream, KDW; Breyre, A; Garcia, K; Calgua, E; Chuc, JM; Taylor, L. Diabetes prevalence in rural Indigenous Guatemala: A geographic-randomized cross-sectional analysis of risk. PloS one 2018, 13(8). [Google Scholar] [CrossRef]
- Cataño Bedoya, JU; Botero, JD; Naranjo González, CA; Rúa Molina, DC; Gracia, JR; García Pineda, AF; et al. Prevalence of cardiovascular risk factors in the embera-chami indigenous population of cristianía (Jardín) antioquia, Colombia. Iatreia 2014, 28(1), 5–16. [Google Scholar] [CrossRef]
- Gomes, HLM; Sombra, NM; Cordeiro, EDO; Filho, ZAS; Toledo, NDN; Mainbourg, EMT; et al. Glycemic profile and associated factors in indigenous Munduruku, Amazonas. PloS one;PubMed 2021, 16(9), e0255730. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- de Souza Filho, ZA; Ferreira, AA; Dos Santos, J; Meira, KC; Pierin, AMG. Cardiovascular risk factors with an emphasis on hypertension in the Mura Indians from Amazonia. BMC Public Health;PubMed 2018, 18(1), 1251. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Steinbrook, E; Flood, D; Barnoya, J; Montano, CM; Miller, AC; Rohloff, P. Prevalence of Hypertension, Diabetes, and Other Cardiovascular Disease Risk Factors in Two Indigenous Municipalities in Rural Guatemala: A Population-Representative Survey. Glob Heart 2022, 17(1), 82. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Campbell, JA; Walker, RJ; Dawson, AZ; Egede, LE. Prevalence of Diabetes, Prediabetes, and Obesity in the Indigenous Kuna Population of Panama Epub 2019/02/26. J Racial Ethn Health Disparities;PubMed 2019, 6(4), 743–51. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, CC; Sacuena, ESR; Pinto, AM; Cardoso-Costa, GL; Guerreiro, JF. Anthropometric and metabolic profile of a Brazilian Amerindian group: The Xikrin (Mebengôkre) Epub 2019/05/23. In Am J Hum Biol.; PubMed, 2019; Volume 31, 4, p. e23255. [Google Scholar] [CrossRef] [PubMed]
- Puig-Garcia, M; Caicedo-Montano, C; Marquez-Figueroa, M; Chilet-Rosell, E; Montalvo-Villacis, G; Benazizi-Dahbi, I. Prevalence and gender disparities of type 2 diabetes mellitus and obesity in Esmeraldas, Ecuador: a population-based survey in a hard-to-reach setting Epub 2023/07/02. International journal for equity in health 2023, 22(1), 124. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Davies, MJ; Aroda, VR; Collins, BS; Gabbay, RA; Green, J; Maruthur, NM; et al. Management of hyperglycaemia in type 2 diabetes, 2022. A consensus report by the ADA and the EASD. Diabetologia 2022, 65(12), 1925–66. [Google Scholar] [CrossRef] [PubMed]
- Davies, MJ; D’Alessio, DA; Fradkin, J; Kernan, WN; Mathieu, C; Mingrone, G; et al. Management of hyperglycaemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2018, 41(12), 2669–701. [Google Scholar] [CrossRef]
- McCarthy, MI. Painting a new picture of personalised medicine for diabetes. Diabetologia 2017, 60(5), 793–9. [Google Scholar] [CrossRef]
- Khoury, MJ; Iademarco, MF; Riley, WT. Precision public health for the era of precision medicine. American Journal of Preventive Medicine 2016, 50(3), 398–401. [Google Scholar] [CrossRef]
- Unesco. Indigenous Peoples in Latin America and the Caribbean; UNESCO Publishing: Paris, 2023. [Google Scholar]
- United Nations Economic Commission for Latin A; the C. Indigenous Peoples in Latin America: Advancing Rights and Development; ECLAC: Santiago, Chile, 2020. [Google Scholar]
- Instituto Nacional de Estadística y G. Censo de Población y Vivienda 2020; INEGI: Mexico City, 2020. [Google Scholar]
- Backlund, E; Rowe, G; Lynch, J; Wolfson, MC; Kaplan, GA; Sorlie, PD. Income inequality and mortality: a multilevel prospective study of 521 248 individuals in 50 US states. In International journal of epidemiology; PubMed, 2007; Volume 36, 3, pp. 590–6. [Google Scholar] [CrossRef] [PubMed]
- Statistics, C. Indigenous Peoples in Canada: First Nations, Métis and Inuit; Government of Canada: Ottawa, 2022. [Google Scholar]
- Stein, JH; West, KM; Robey, JM; Tirador, DF; McDonald, GW. The High Prevalence of Abnormal Glucose Tolerance in the Cherokee Indians of North Carolina. Archives of Internal Medicine 1965, 116(6), 842–5. [Google Scholar] [CrossRef]
- Bennett, P; Burch, T; Miller, M. DIABETES MELLITUS IN AMERICAN (PIMA) INDIANS. The Lancet 1971, 298(7716), 125–8. [Google Scholar] [CrossRef]
- Henry, RE; Burch, TA; Bennett, PH; Miller, M. Diabetes in the Cocopah Indians. Diabetes;PubMed 1969, 18(1), 33–7. [Google Scholar] [CrossRef] [PubMed]
- Frohman, LA; Doeblin, TD; Emerling, FG. Diabetes in the Seneca Indians. Plasma insulin responses to oral carbohydrate. Diabetes.;PubMed 1969, 18(1), 38–43. [Google Scholar] [CrossRef] [PubMed]
- Bruce, S. Prevalence and determinants of diabetes mellitus among the Metis of western Canada Epub 2001/09/05. Am J Hum Biol.;PubMed 2000, 12(4), 542–51. [Google Scholar] [CrossRef] [PubMed]
- Santos, JL; Pérez-Bravo, F; Carrasco, E; Calvillán, M; Albala, C. Low prevalence of type 2 diabetes despite a high average body mass index in the aymara natives from Chile. Nutrition 2001, 17(4), 305–9. [Google Scholar] [CrossRef]
Figure 1.
Source: Modified from Page MJ, et al. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. This work is licensed under CC BY 4.0. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/.
Figure 1.
Source: Modified from Page MJ, et al. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. This work is licensed under CC BY 4.0. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/.
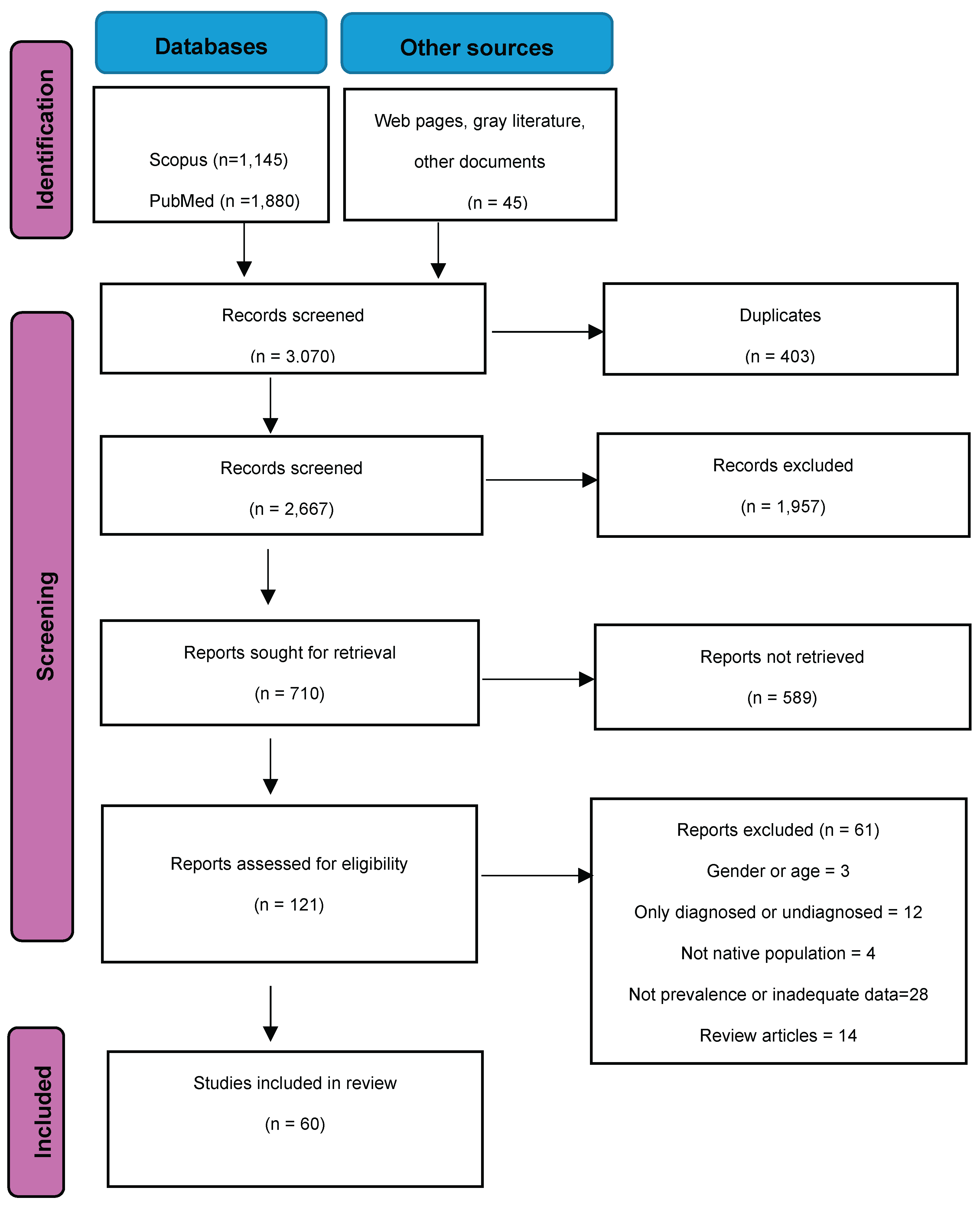
Table 2.
Prevalence of diabetes mellitus in indigenous populations of the Americas.
| Country | Site | Year | Age | N | Ethnicity | Test | Method | Value | Men | Women | Both | ||
| USA[17] | Arizona | 1975 | 25+ | 1,414 | Pima | OGTT | Laboratory | ≥200mg/dl/ | 32.6 | 37.2 | 34.9** | ||
| Chile [18] | Community | 1983 | 20+ | 510 | Mapuche | OGTT | Laboratory | ≥200 mg/dl | 0.4 | 1.4 | 1.0 | ||
| Canada [19] | Ontario | 1986-87 | 20-64 | 671 | Cree, Ojibwa | FBG | Laboratory | ≥126 mg/dl | 10.0 | 11.0 | |||
| USA [20] | Tribe, Minnesota | 1988 | 20+ | 346 | Chippewa | FBG OGTT10 |
Laboratory | ≥140mg/dl ≥200mg/dl |
13.4 | 16.1 | 14.8 | ||
| USA [21] | Arizona | 1987 | 20-74 | 275 | Navajo | FBG | Laboratory | ≥140mg/dl |
9.1 | 10.5 | 9.9 | ||
| USA [22] | Arizona | 1988 | 20+ | 231 | Navajo | FBG OGTT |
Laboratory | ≥140mg/dl ≥200mg/dl |
10.8 | 14.3 | 12.4 | ||
| USA [23] | Rural reservation, Arizona | 1989-90 | 20-74 | 419 | Navajo | FBG OGTT |
Laboratory | ≥140mg/dl ≥200mg/dl |
13.9 (9.2-18.5) |
18.4 (14.0-22.8) |
16.5 (13.2-19.7) |
||
| USA [24] | Multiple | 1989-91 | 45-74 | 3,638 | Akimel O’odham, Pee-Posh, Tohono O’odham, Ak-Chin Community, Apache, Ft. Sill Apache, Caddo, Comanche, Delaware, Kiowa, Wichita, Oglala Sioux, Cheyenne River Sioux, Spirit Lake Sioux | OGTT | Laboratory | ≥200mg/dl/ |
42.1 | 52.7 | |||
| USA [25] | Tucson, Arizona | 1990 | 25-65 | 230 | Pascua Yaqui | FBG OGTT11 |
Laboratory | ≥140mg/dl ≥200mg/dl |
35.4 | 38.9 | |||
| USA [22] |
Rough Rock community | 1992 | 20+ | 827 | Navajo | FBG OGTT |
Laboratory | ≥140mg/dl ≥200mg/dl |
10.8 (4.4, 17.2) | 14.3 (8.5, 20.1) | 12.4 (8.1, 16.7) | ||
| USA [26] | Southwestern US | 1991-92 | 20+ | 575 | Navajo | FBG OGTT |
Laboratory | ≥140 mg/dl ≥200 mg/dl |
19.4 | 24.6 | 22.9 | ||
| USA [27] | Minnesota | 1992-94 | 25+ | 981 | Chippewa and Menominee | FBG OGTT |
Laboratory | ≥140 mg/dl ≥200 mg/dl |
27.00 | 29.00 | 28.00 | ||
| Mexico [28] | Community, Sonora | 1994 | 20+ | 224 | Pima | FBG OGTT |
Laboratory | ≥140 mg/dl ≥200 mg/dl |
5.6 | 8.5 | 6.9 | ||
| USA [28] | Arizona | 1995 | 20+ | 888 | Pima | FBG OGTT |
Laboratory | ≥140 mg/dl ≥200 mg/dl |
34.2 | 40.8 | 38.0 | ||
| Canada [29] | River Desert, Quebec | 1995 | 30-64 | 131 | Algonquins | FBG OGTT |
Laboratory | ≥140mg/dl ≥200mg/dl |
16.3 (7.9–24.7) | 16.3 (9.0–23.6) | |||
| Canada [29] | Lac Simon. Quebec | 1995 | 30-64 | 168 | Algonquins | FBG OGTT |
Laboratory | ≥140mg/dl ≥200mg/dl |
23.9 (12.9–34.9) | 48.6 (38.4–58.8) | |||
| United States[24] | Multiple | 1993-95 | 45-74 | 3,638 | Akimel O’odham, Pee-Posh, Tohono O’odham, Ak-Chin Community, Apache, Ft. Sill Apache, Caddo, Comanche, Delaware, Kiowa, Wichita, Oglala Sioux, Cheyenne River Sioux, Spirit Lake Sioux | OGTT | Laboratory | ≥200mg/dl/ |
48.2 | 61.3 | |||
| Canada [30] | Sandy Lake, Ontario | 1993-95 | 10+ | 728 | Ojibwa-Cree | FBG OGTT |
Laboratory | ≥140mg/dl ≥200mg/dl |
28.0¥ | 24.2¥ | 26.1¥1 | ||
| USA [31] | Arizona | 1995 | 20-74 | 900 | Pima, Maricopa, Papago | FBG OGTT8 |
Laboratory | ≥140mg/dl ≥200mg/dl |
65 (60.3-69.1) |
72 (69.3-75.3) |
70 (67.2-72.2) |
||
| USA [31] | Delaware | 1995 | 20-74 | 400 | Apache, Caddo, Comanche | FBG OGTT8 |
Laboratory | ≥140mg/dl ≥200mg/dl |
38 (33.9-41.8) |
42 (38.6-45.4) |
40 (37.7-42.8) |
||
| USA [31] | N & S Dakota | 1995 | 20-74 | 200 | Ogala, Sioux, Cheyenne, River Sioux, Devils Lake Sioux | FBG OGTT8 |
Laboratory | ≥140mg/dl ≥200mg/dl |
33 (29.0-36.8) |
46 (42.1-49.1) |
40 (37.5-42.8) |
||
| Mexico [32,33] | Maycoba, Sonora | 1995 | 20+ | 226 | Pima | FBG OGTT |
Laboratory | ≥126 mg/dl ≥200 mg/dl |
5.6 | 8.5 | 7.1 | ||
| Mexico [34,35] |
Durango |
1996** | 30-64 | 193 | Tepehuanos, Huicholes, Mexicaneros | FBG OGTT |
Glucometer | ≥140 mg/dl ≥200 mg/dl |
0.0 | 0.0 | 0.0 | ||
| Mexico [36] | Community | 1996-1997 | 15-77 | 91 | Otomíes | FBG | Laboratory | ≥126 mg/dl | - | - | 4.4 (0.1-8.7) |
||
| Colombia [37] | Rural | 1996* | 18+ | 147 | Arhuaco, Arzario, Kogui, Wayuu | OGTT | Glucometer | >10 mmol/l | 0.0 | 0.0 | 0.0 | ||
| Bolivia [38] | Urban El Alto |
1998 | 25+ | 776 | Aymara | OGTT | Glucometer | ≥200 mg/dl | 5.3 (2.2-8.3) |
4.3 (2.7-6.7) |
4.8 (3.4-6.6) |
||
| Bolivia [38] | Urban Cochabamba | 1998 | 25+ | 266 | Quechua | OGTT | Glucometer | ≥200 mg/dl | 7.9 (4.2-14.3) |
8.9 (5.2-14.8) |
8.4 (5.6-12.4) |
||
| Chile [39] | Rural Community |
1998 | 20+ | 319 | Mapuche | OGTT | Laboratory | ≥200 mg/dl | 3.2 (0.7-9.0) |
4.5 (2.2-8.1) |
4.1 (2.2-6.9) |
||
| Chile [40] | Rural Community |
1998 | 20+ | 196 | Aymara | OGTT | Laboratory | ≥200 mg/dl | 1.3 (0.0-7.0 |
1.7 (0.2-6.0) |
1.5 (0.3-4.5) |
||
| Paraguay [41] | Community, Chaco | 1998 | 18-70 | 225 | Ayoreos | FBG or OGTT | Laboratory | ≥126 mg/dl ≥200 mg/dl |
0.0 | 0.0 | 0.0 | ||
| Guatemala [42] | Rural, Urban Sololá |
1998 | 30+ | 400 | Quiche, Cakchiquel, Zutuhil | OGTT | Laboratory | ≥200 mg/dl | - | - | 6.8 | ||
| Brazil [43] | Parque Indígena do Xingu (Mato Grosso) | 1999 | 20+ | 86 | Suyá | FBG | Glucometer | ≥126 mg/dl | 0.0 | 0.0 | 0.0 | ||
| Mexico [44] | Community, Merida | 2000 | 18-81 | 263 | Maya | FBG | Laboratory | ≥126 mg/dl | - | - | 10.6 | ||
| Brazil [45] | Pará | 2000 | 20+ | 122 | Parkateje | FBG or OGTT | Glucometer | ≥126 mg/dl ≥200 mg/dl |
- | - | 1.1 | ||
| Mexico [46] | National | 2000 | 20+ | 3,645 | Multiple indigenous groups | FBG A1c |
Laboratory | ≥126 mg/dl or 6.5% |
4.1 (3.1, 5.2) |
||||
| Canada [47,48] | Sandy Bay Ojibway First Nation, Manitoba |
2002-2003 | 18+ | 482 | Ojibway | FBG | Laboratory | ≥126 mg/dl | 27.0 (21.2–32.7) | 31.0 (25.2–36.7) | 29.0 (25.0–33.1) | ||
| Brazil [49] | Upper Xingu | 2002-2003 | 20+ | 251 | Kalapalo, Kuikuro, Matipu, Nahukwá | FBG | Laboratory | ≥126 mg/dl | 0.0 | 0.0 | 0.0 | ||
| Brazil [50] | Community, Espírito Santo | 2003-2004 | 25-64 | 620 | Guarani, Tupinikin | FBG | Laboratory | ≥126 mg/dl | 2.4 | 2.7 | - | ||
| Chile [51] | Santiago & Arica | 2004** | 18+ | 160 | Aymara | OGTT | Laboratory | ≥200 mg/dl | 2.4 (0.1-12.6) | 8.5 (4.1-15.0) | |||
| Chile [51] | Santiago & Arica | 2004** | 18+ | 147 | Mapuche | OGTT | Laboratory | ≥200 mg/dl | 14.3 (5.4-28.5) | 5.7 (201-12.0) | |||
| Canada [52] | Mistissini, Quebec | 2005 | 18+ | 172 | Cree | FBG | Laboratory | ≥126 mg/dl | 20.0 | ||||
| Belice [53] | National | 2003-2006 | 20+ | 1,192 | Indigenous/ Mestizo ¥ |
FBG or OGTT |
Laboratory | ≥126 mg/dl ≥200 mg/dl |
8.6 (6.0–12.1) |
13.6 (11.1–16.4) |
11.0 (9.0–13.5) |
||
| Guatemala [53] | Urban, Guatemala City | 2003-2006 | 20+ | 1,395 | Indigenous/ Mestizo ¥ |
FBG or OGTT |
Laboratory | ≥126 mg/dl ≥200 mg/dl |
7.8 (5.1–11.8) |
6.8 (4.8–9.4) |
7.3 (5.4–9.7) |
||
| Honduras [53] | Urban, Tegucigalpa | 2003-2006 | 20+ | 1,592 | Indigenous/ Mestizo ¥ |
FBG or OGTT |
Laboratory | ≥126 mg/dl ≥200 mg/dl |
5.0 (2.7–9.1) |
5.3 (3.8–7.2) |
5.1 (3.2–8.0) |
||
| Nicaragua [53] | Urban, Managua | 2003-2006 | 20+ | 1,530 | Indigenous/ Mestizo ¥ |
FBG or OGTT |
Laboratory | ≥126 mg/dl ≥200 mg/dl |
9.5 (7.2–12.5) |
10.8 (8.1–14.2) |
10.2 (8.2–12.6) |
||
| Mexico [46] | National | 2006 | 20+ | 513 | Multiple indigenous groups | FBG A1c |
Laboratory | ≥126 mg/dl or 6.5% |
9.4 (6.8, 12.9) |
||||
| Mexico [54] | Community, Sonora | 2006- | 20-65 | 120 |
Yaquis |
FBG OGTT |
Laboratory | ≥126 mg/dl ≥200 mg/dl |
20.5 | 17.6 | 18.3 | ||
| Mexico [54] | Community, Sonora | 2006-2007 | 20-65 | 158 | Tepehuanos | FBG OGTT |
Laboratory | ≥126 mg/dl ≥200 mg/dl |
- | - | 0.8 | ||
| Brazil [55,56] | Community, Jaguapiru, Mato Grosso do Sul | 2007-2008 | 18-69 | 606 | Guarani, Kaiowa, Terena | FBG OGTT 1 |
Glucometer | ≥126 mg/dl ≥200 mg/dl |
1.5 | 6.8 | 4.5 | ||
| Mexico [57] | Community, Oaxaca | 2010* | 35+ | 394 | Zapotec | FBG OGTT |
Not mentioned | ≥126 mg/dl ≥200 mg/dl |
6.2 | 13.3 | 8.7 | ||
| Mexico [57] | Community, Oaxaca | 2010* | 35+ | 730 | Mixe | FBG OGTT |
Not mentioned | ≥126 mg/dl ≥200 mg/dl |
5.7 | 7.1 | 6.9 | ||
| Colombia [58] | Communities, Caldas | 2010 | 20-69 | 151 | Embera-Chamí | FBG | Laboratory | ≥126 mg/dl | 7.9 | ||||
| Mexico [32,33] | Maycoba, Sonora | 2010 | 20+ | 359 | Pima | FBG OGTT |
Laboratory | ≥126 mg/dl ≥200 mg/dl |
6.0 | 11.8 | 9.0 | ||
| Brazil [59] | Xingu Indigenous Park | 2010-2011 | 20+ | 181 | Khisêdjê | OGTT | Laboratory | ≥200 mg/dl | 2.0 | 6.8 | 3.8 | ||
| Chile [60] | Rural | 2011 | 15+ | 264 | Pehuenche | 2 FBG Or Casual 2 |
Laboratory | ≥126 mg/dl ≥200 mg/dl |
- | - | 0.8 | ||
| Panama [61] | Provinces of Panama & Colon | 2011 | 18+ | 203 | Native American ¥ | FBG A1C |
Laboratory | ≥ 126 mg/dl 6.5% |
5.4 (3.2–7.6) | ||||
| Mexico [62] |
Urban/rural, Chiapas | 2010-2012 | 20+ | 880 | Indigenous ¥ | FBG OGTT |
Laboratory | ≥126 mg/dl ≥200 mg/dl |
3.5 (1.6–5.5) |
5.8 (3.8–7.8) |
4.7 (3.3–6.1) |
||
| Canada [47,63] | Sandy Bay Ojibway First Nation, Manitoba |
2011-2012 | 18+ | 596 | Ojibway | FBG | Laboratory | ≥126 mg/dl | 24.8 (20.0–29.6) | 27.1 (21.9–32.3) | 25.9 (22.4%–29.4) | ||
| Mexico [46] | National | 2012 | 20+ | 1,122 | Multiple indigenous groups | FBG A1c |
Laboratory | ≥126 mg/dl or 6.5% |
12.7 (9.8, 16.3 |
||||
| Guatemala [64] | Community, Atitlán | 2012-2013 | 20-65 | 308 | Tzu’tujil, Kaqchikel, mestizo | FBG | Glucometer | ≥126 mg/dl | 3.0 (1.1-4.8) |
1.3 (0.0-3.2) |
4.6 (1.6, 7.7) |
||
| Surinam [65] | National | 2013 | 15-65 | 279 | Amerindian ¥ | FBG | Laboratory | ≥126 mg/dl | 15.8 | 8.7 | |||
| Mexico [66] | Community Baja California | 2013-2014 | 18+ | 275 | Indigenous/mestizo ¥ | A1c | Micro mehod | ≥6.5% | 18.6 | 22.9 | 21.8 | ||
| Brazil [67] | Community, Mato Grosso | 2010-2012 | 20+ | 948 | Xavante | OGTT | Glucometer | ≥200 mg/dl | 18.4 (14.9–22.2) |
40.6 (36.2–45.1) |
28.8 (25.3–31.1) |
||
| Argentina [68] |
Communities, Chaco | 2014 | 18+ | 156 | Wichi | CBGT | Glucometer | ≥200 mg/dl | 1.7 | 0.0 | 0.6 | ||
| Guatemala [69] | Community, Atitlán | 2015 | 18+ | 394 | Tzu’tujil, Kaqchikel | A1c | Glucometer | ≥6.5% | 12.2 (6.3-8.1) |
14.6 (10.3-18.8) |
13.8 (10.4-17.2) |
||
| Colombia [70] | Cristiania (Jardín) Antioquia | 2015* | 14+ | 145 | Embera-Chamí | FBG | Not mentioned | ≥126 mg/dl | 0.0 | 0.9 | 0.7 | ||
| Brazil [71] | Communities | 2018 | 18+ | 459 | Munduruku | FBG | Glucometer | ≥126 mg/dl | 12.2 | ||||
| Brazil [72] | Community, Amazonia | 2018* | 18+ | 455 | Mura | FBG | Glucometer | ≥126 mg/dl | 3.0 1.8-5.1 |
||||
| Mexico [46] | National | 2018 | 20+ | 1,177 | Multiple indigenous groups | FBG A1c4 |
Laboratory | ≥126 mg/dl or 6.5% |
18.7 15.0, 23.2) |
||||
| Guatemala [73] | Rural | 2018-2019 | 18+ | 640 | Maya | A1c | Micro method | ≥6.5% | 12.2 (7.4-16.9) |
12.9 (9.4 - 16.4) |
12.2 (7.4-16.9) |
||
| Panama [74] | Community | 2019* | 18+ | 211 | Kuna Indians | A1c | Micro method | ≥6.5% | 14.0 | 12.9 | 13.0 | ||
| Brazil [75] | Community, Pará |
2019* | 18+ | 363 | Xikrin (Mebengôkre) | FBG | Laboratory | ≥126 mg/dl | 4.4 | 4.9 | 3.8 | ||
| Ecuador [76] | Municipality | 2022 | 18+ | 111 | Chachi | FBG OGTT3 |
Laboratory | ≥126 mg/dl or ≥200 mg/dl | 0.9 | ||||
(*) Publication year (**) Truncated rates calculated from original data. FBG (Fasting Blood Glucose); OGTT (Oral Glucose Tolerance Test); CBGT (Casual Blood Glucose Test); A1c (Hemoglobin A1c) (1) (FBG ≥126 mg/dl in two occasions, OGTT if FBG ≥100 mg/dl & <126 mg/dl (nonstandard); (2) Two FBG ≥126 mg/dl, or one FBG ≥200 mg/dl (nonstandard); (3) FBG ≥144 mg/dl , OGTT if FBG < 144 mg/dl ; (4) FBG ≥126 mg/dL or A1c ≥6.5%; ¥ Referred as indigenous/mestizo or Native Americans. (8) FBG ≥140 mg/dl or OGTT≥200; (10) OGTT if FBG≥ 115 mg/dl or CBG ≥140 mg/dl and two FBG ≥126 mg/dl. (11) OGTT with 100 gms of glucose. 1Described as age-standardized
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



