Submitted:
23 December 2025
Posted:
24 December 2025
You are already at the latest version
Abstract
Timely identification of infectious disease threats is essential for public health readiness. Conventional indicator-based surveillance systems, while dependable for tracking established pathogens, frequently lack the agility and sensitivity to detect new infections promptly. Syndromic surveillance, which examines pre-diagnostic and non-specific health indicators from many data sources in near real time, serves as a significant complementary method that improves early warning and situational awareness. This narrative study analysed global experiences with syndromic surveillance from 2000 to 2025, utilising peer-reviewed literature and institutional records. Four primary data streams were examined: emergency department and hospital records, pharmacy and over-the-counter (OTC) sales, participative citizen-generated data, and hybrid multi-source systems. Syndromic indicators identified outbreaks two to fourteen days before to standard laboratory reporting across many trials. Data from the emergency department exhibited the highest sensitivity and specificity (respectively 47.34% and 91.95% according to ), whereas pharmacy and participative data offered early indicators at the community level. Integrated systems like ESSENCE (United States) and SurSaUD® (France) attained enhanced accuracy yet necessitated significant data integration and governance capabilities. Syndromic surveillance enhances epidemic preparation by detecting atypical health-seeking behaviours and variations from baseline patterns prior to formal diagnosis. Nonetheless, its efficacy is contingent upon data quality, interoperability, and contextual adaption. Countries like Bulgaria could improve national early-warning capabilities and overall health security through the gradual adoption of pilot projects and integration with existing surveillance networks.
Keywords:
syndromic surveillance
; infectious disease
; early warning
; epidemic preparedness
; data integration
1. Introduction
Epidemiological surveillance is defined as “the ongoing, systematic collection, analysis, and interpretation of health data essential to the planning, implementation, and evaluation of public health practice, closely integrated with the timely dissemination of [this information] to those who need to know”[1]. Transformed into epidemiological information, it is the basis for planning and conducting control programs and evaluating their effectiveness.
Since the revision of the International Health Regulations in 2005, the role of surveillance as a major component of public health has increased[2]. For this purpose, the collected information is analysed and interpreted, and the results are widely disseminated. The frequency and prevalence of infectious diseases, as well as the main determinants of diseases, are tracked. In this way, a type of safety net is created, incidents are identified and trends in the development of infectious diseases are tracked.
The data acquired from surveillance systems serves three interconnected purposes. Primarily for the rapid identification and fast response in epidemics or emerging health concerns requiring immediate containment measures. Secondly, for the systematic evaluation and monitoring of essential health indicators—such as illness prevalence, immunisation rates, and antibiotic resistance—which provide trend analysis, benchmarking, and adjustments to preventive measures. Moreover, effective surveillance facilitates evidence-based decision-making and permits the assessment of the impact and effectiveness of public health interventions.
The design of surveillance systems varies across settings and countries according to specific public health needs, resource constraints, and governance arrangements. Given the surveillance methodology adopted so far, the existing traditional surveillance systems are generally not sensitive enough for the early identification of emerging diseases and clusters[3]. Even with a prompt notification, the link to a specific disease is not always obvious, and the setting of a possible diagnosis could be delayed over time. Second, the aetiological link between initial clinical presentation and a notifiable pathogen may not be apparent, delaying case confirmation even when reporting is timely. Third, the ongoing decentralisation of health services—although intended to enhance efficiency—can fragment information flows and attenuate data quality, complicating the coordination of surveillance operations[4]. Contemporary guidance emphasises the recommendation for digitalisation, interoperability and real-time integration of the existing systems to accelerate date capture and the turn-around time[5].
Based on the models for collecting information, the surveillance of diseases can be divided into Indicator-based surveillance (IBS), Event-based surveillance (EBS) and syndromic surveillance.
The most utilized system for disease detection and reporting is the disease specific surveillance or IBS which involves routine notification of diseases and health events through notifiable disease surveillance systems. Many countries maintain a predefined list of diseases or conditions of interest which use standardized case definitions to ensure consistency and comparability. Such kinds of systems can be employed on a national level.
In contrast, EBS aggregates ad-hoc signals from laboratories, media reports, digital platforms, and other non-traditional sources, thereby complementing IBS by detecting unusual occurrences that fall outside formal reporting pathways. Integrating indicator-based (indicator-based surveillance – IBS) with event-based components (event-based surveillance EBS) can markedly improve sensitivity, specificity and overall responsiveness[6]. In a period that is marked by fast pathogen introduction and increased global interconnection, such advancements are essential for satisfying the core-capacity requirements of the International Health Regulations (2005)2 and for protecting the health of the public.
The third type of surveillance which can be utilized - syndromic surveillance, is based on non-specific health indicators collected for purposes other than surveillance and where possible are automatically generated for allowing early detection of human or veterinary public health threats[7]. The alterations in the epidemiology of infectious diseases enable the creation of a syndromic surveillance system to meet the new demands. By transcending established norms, the syndrome-based approach enhances the sensitivity of case detection relative to alternative methods.
Identification of Contemporary Needs
One of the most important components of a prompt response to public health emergencies is the early detection of novel or emerging infectious diseases. The contemporary changing climatic and social context due to global warming and armed conflict requires public health to accommodate for the growing uncertainty and even potential deliberate use of biological agents[8]. The rapid progression of climate change is altering the ecology of numerous pathogens and their vectors[9,10,11] broadening the potential distribution of diseases such as West Nile virus, dengue, chikungunya, and vibrio infections into temperate regions. Recent forecasts indicate that, under moderate-to-high emission scenarios, the climatic suitability for West Nile virus in Western Europe may increase three- to five-fold by mid-century, endangering millions of immunologically naïve individuals—a trend already suggested by the emergence of infected Culex mosquitoes in the United Kingdom during the summer of 2025[12]. In this context, contemporary surveillance systems must identify infections that may emerge in geographically and seasonally atypical locations. Flexible, real-time detection is essential for effective epidemic control. Even minor delays of a few days in identifying atypical clinical clusters significantly increase the potential for transmission, especially when community immunity is poor and healthcare resources are limited. As a result, adapting surveillance systems for swift responsiveness — whether to a vector-borne arbovirus in a warming climate or a totally new respiratory pathogen — has become a top priority on global health-security agendas.
In recent years, the need to develop rapid response capabilities has been starkly illustrated by two high-impact events: the COVID-19 pandemic[10,13,14], and the unprecedented 2022 outbreak of Mpox registered on the territory of Europe and North America. Both diseases meet the criteria for new or re-emerging infections, yet each revealed different facets of the same vulnerability—how quickly an undetected pathogen can propagate when early-warning signals are missed.
The causative agent of COVID-19, SARS-CoV-2, was unknown to medicine until clinicians in Wuhan, China reported a cluster of severe, unexplained pneumonia on 31 December 2019[15]. By 11 February 2020 the virus had been genetically characterised and officially named, but sustained community transmission was already global, underscoring the narrow window for containment once silent spread has begun[16,17,18,19]. The observed variations in metrics like mortality, lethality, and excess mortality can be largely attributed to the differing monitoring capabilities and methodologies employed at country level[17]. The epidemic outbreak of Mpox in 2022 was observed on the territory of Europe and North America, where previously no cases were registered. Within three months, more than 100 nations had reported infections, prompting the World Health Organization to declare a Public Health Emergency of International Concern[20].
These two instances reveal the fundamental limitations of traditional notifiable disease surveillance. Conventional approaches are designed to identify diseases that are already well-defined and predictable within specific clinical or geographic parameters; syndromic manifestations that deviate from these frameworks may go undetected until an outbreak is firmly established. Empirical assessments of early-alert systems demonstrate that restrictive reporting criteria diminish sensitivity to anomalous trends in healthcare use, hence postponing the identification of developing [21,22].
To address this detection gap, public health practice is progressively transitioning to multi-source, real-time surveillance systems that integrate electronic health records, over-the-counter pharmaceutical sales, social media discussions, and various open-source intelligence sources. The integration of heterogeneous data (including pre-diagnostic data that integrates observations on symptoms before laboratory confirmation) enhances the probability of detecting weak, atypical signals, such as abrupt increases in non-specific respiratory complaints or dermatological consultations, prior to laboratory confirmation. The experiences with COVID-19 and Mpox offer strong empirical support for the development of broad-spectrum early-warning systems which rely on established thresholds and are activated for validation each time critical values are surpassed. These systems should be designed to detect unusual health-seeking behaviours across various channels, thereby reducing the time from signal to response and ultimately mitigating disease transmission5.
2. Materials and Methods
This article is a narrative review that comparatively examines syndromic monitoring methodologies and provides insights on syndromic data management. Based on the hypothesis of syndromic systems’ higher sensitivity and baseline specificity, it aspires to evaluate syndromic signals’ overall effect on public health – whether they naturally complement traditional surveillance activities or creates additional burden with false-positive escalations and increased noise. The main goal was to integrate current literature and practical experiences to explore reported benefits, constraints, and strategic functions of syndromic surveillance in modern public health settings.
Relevant peer-reviewed literature, technical reports, and institutional publications were located by electronic searches of prominent biomedical databases, including PubMed, Scopus, and Web of Science. The mentioned databases were screened for papers discussing syndromic and participatory surveillance, emergency and primary care data for public health uses, automated syndromic surveillance systems, ICD codes utility for early detection, pre-diagnostic chief complaint data uses, public health approaches to early detection, surveillance in the context of mass gatherings, sales of nonprescription remedies, early warning indicators for public health. The search encompassed publications published from 2000 to 2025, illustrating the period during which syndromic surveillance has achieved considerable global prominence.
This study utilised secondary data from publicly accessible literature and reports, hence no ethical approval was necessary. Although this review does not follow a systematic PRISMA protocol, it applies a structured approach to literature identification, inclusion, and synthesis to ensure transparency.
3. Results and Discussion
3.1. International Experience in Syndromic Surveillance Implementation
Syndromic Surveillance Based on Emergency Department and Hospital Data
Addressing the deficiencies in conventional notifiable-disease systems requires a clearly delineated multi-channel framework that simultaneously employs clinical, laboratory, administrative, and unconventional data sources5. The conceptual basis for this technique was established shortly after the September 11, 2001, attacks, when U.S. public health organisations investigated the potential of near-real-time logs from emergency department admissions as an early-warning indicator for significant bioterrorism incidents. The discussions—ultimately formalised in systems like BioSense and ESSENCE—revealed that passive, clinician-initiated reporting is inherently less informative than the ongoing electronic collection and automated analysis of comprehensive ED registries[23,24]. Selective submission may exclude clinically mild or unusual symptoms, thereby create systematic gaps and obscuring the true onset of an outbreak.
The latency inherent in conventional case-notification processes is equally concerning; individual records must initially meet case-definition criteria, followed by validation, transmission, and manual curation before aggregate analysis can commence. This administrative delay, frequently quantified in days, diminishes the temporal resolution required for swift intervention and ultimately compromises confidence in the resultant situational assessment[25].
In 2002, the experience of multiple healthcare facilities in the USA validated a model that categorises complaints or illnesses based on ICD-9 codes, so confirming the benefits of syndromic surveillance. Espino’s study indicated that the screening sensitivity was 44% and the specificity was 97%, with the analysis of reported complaints (diagnosed before confirmed diagnosis) demonstrating the highest significance relative to the clinical diagnosis[26]. The methods of processing pre-diagnostic data based on symptoms, without pre-diagnostic coding, exhibited contrasting results. At a specificity threshold of 93%, the sensitivity of pre-diagnostic data compared to the confirmed diagnosis was 2 to 3% lower [27]. Nonetheless, the integration of the two models is characterised by enhanced accuracy[27]. Data availability for specific diseases associated with highly specific disease manifestations shapes to a great extent findings related to efficiency of syndromic surveillance. Highly generic symptoms as those reported for acute respiratory infections are expected to score high on sensitivity but low on the specificity scale[28] while specific symptoms and exposure history relevant to some syndromes such as gastroenteritis were pointed to lead to immediate diagnostic implications[29]. An explanation for the inaccuracies associated with symptom assessment is provided by the findings of Roberts’ research team, which indicate that the same disease may present with varying symptoms among different patients. Expanding the definitions, as proposed by the implementation of operational ICDs, may address the identified issue[30].
3.2. Syndromic Surveillance – Basic Indicators, Approaches and Utility
Contemporary medical practice aspires to accuracy indicating one or multiple work diagnoses during a single visit. The majority of reports on syndromic surveillance supply data on ICD-9 code, work diagnosis, free-text symptoms, sex, patient residence, and visit location, while all report an ICD-9 clinical diagnosis, along with age and visit time[31,32]. The reviewed literature evaluates the data analysis in relation to the potential for early detection of national security threats stemming from the intentional deployment of biological agents.
In the 2002 Winter Olympic Games in Utah, a comparable system was implemented, wherein the patient numbers from prior periods were analysed against those registered for the corresponding current period. Values surpassing the 95% confidence interval were deemed indicative of concern to mitigate false alarms[25,33]. Practical experience confirms thresholds may be modified based on a prior risk assessment[34] resulting in tailored risk-based surveillance models allowing for resource allocation according to emergency needs[35]. Various syndromic surveillance systems employ distinct methodologies for syndrome partitioning based on their research [25,36,37,38]. The age of the patients is a significant variable to consider. Changes in disease demographics may indicate the emergence of a new infection, as evidenced by the study conducted in Syria during the COVID-19 pandemic[39].
3.3. Pharmacy and Over-the-Counter (OTC) Sales Data
A significant amount of preclinical data is derived by observing trends in pharmaceutical sales. A rise in over-the-counter drug sales—such as antipyretics, cough suppressants, or gastrointestinal treatments—can act as an early indicator of increasing disease prevalence in the community[25]. Mandl’s surveillance model posits that these data sources precede emergency department utilisation, illustrating the inherent latency between symptom onset and individuals’ decisions to pursue medical care[34]. Pharmacy-based sales metrics reflect the behavioural change that takes place when individuals initially encounter symptoms and pursue over the counter (OTC) relief[34]. Numerous studies have identified these indicators as easy to collect, epidemiologically significant, and timely enough for public health decision-making[40,41,42,43,44,45,46].
The literature accessed indicates that deviations in pharmaceutical demand frequently arise prior to similar indicators appearing in standard clinical data. Sales increases in antidiarrhoeal or rehydration products have been observed approximately two weeks prior to clinically confirmed diarrhoeal outbreaks[45].. In contrast, unusual acquisitions of antipyretics, cough suppressants, or other respiratory treatments generally result in emergency department identifications occurring approximately 2.8 days later (range: 2–7 days)[46].. Das et al.[47]. indicate that, despite the advantageous lead time, the overall sensitivity of pharmacy-based surveillance is inferior to that of emergency department visit counts, primarily due to variations in performance associated with disease aetiology[47].. OTC sales may inadequately reflect pathogens that produce mild or ambiguous early symptoms, while they are more effective for conditions that necessitate prompt self-treatment, such as influenza-like illness.
The predictive value of pharmaceutical sales data is context-specific, influenced by cultural norms, socioeconomic factors, healthcare-seeking behaviour, and the structure of national pharmacy markets. In contexts characterised by prevalent self-medication and well-established digital reporting systems in pharmacies, sales data can serve as an early and cost-effective indicator. In contrast, in nations with robust physician-gatekeeper systems or restricted over-the-counter access, the signal may be weak or delayed. A Japanese study indicated minimal additional benefit from monitoring pharmacy transactions for influenza spread, likely due to local consultation patterns and dispensing regulations[48].
3.4. Participatory and Citizen-Generated Data
Alongside conventional clinical data acquired from primary care providers, preclinical data sources (patient and OTC sales-generated information) give significant insights for early detection. One such source is to citizen-generated information, wherein citizens report and evaluate the severity of newly encountered symptoms linked to infectious diseases. Despite the limited adoption of this data in public health practice, research during seasonal influenza outbreaks and subsequent COVID-19 waves has revealed a strong association between self-reported symptoms and laboratory-confirmed illnesses[49,50,51].
A significant benefit of participatory surveillance systems is their flexibility and adaptability. These systems depend on voluntary contributions from the general populace, allowing for facile configuration to monitor a wide range of ailments. This method has demonstrated efficacy not just during respiratory virus epidemics but also in situations of increased threat from infections like the Zika virus and Salmonella species[50].
3.5. Other Innovative and Hybrid Models
Syndromic surveillance is particularly effective in identifying emerging or previously undiagnosed diseases prior to formal clinical diagnosis. Experts recommend aligning surveillance algorithms with established patterns of disease seasonality and cyclicity to ensure that these systems deliver meaningful and timely alerts. By considering anticipated variations within standard epidemiological parameters, the system can concentrate on detecting genuinely anomalous events, thus minimising false-positive signals[34]..
Empirical studies of the late 20th and early 21st centuries set out to clarify the utility of "unorthodox" pre-diagnostic data for early disease detection by expanding their scope to include pharmacy sales and Internet searches. The methods used are simple and are limited to determining a critical threshold for each indicator. Deviations from it are subject to in-depth analysis. Wagner’s study of different surveillance methods uses an influenza A epidemic as a subject and aims to measure the timeliness of different indicators to detect a peak in morbidity. The gold standard is two consecutive weeks in which more than 1% of the samples were positive for the presence of the pathogen of interest. His measured sensitivity ranged from 32% (for paediatric referrals for flu-like symptoms) to 81% (for emergency room visits). Specificity ranges from 63% (sentinel reports) to 75% (emergency department visits). The results showed that emergency examination data were not only the most accurate but also ahead of the gold standard by 4 weeks, while paediatric care seeking was delayed by 5 weeks compared to the gold standard[33].. This finding regarding the early timeliness of the emergency medical care demand indicator is supported by other studies that conclude that data is applicable to increasing hospital care capacity prior to entering a peak wave[52,53]. The main advantage of emergency and outpatient registries is the prior availability of data on prevalent syndromes[34]. Figure 1 summarizes platform integration and communication channels establishment according to the literature sources[23,24,25,26,27,28,29,30,31,32,33,34].
Table 1 summarises the comparative advantages and limitations of the main data sources used in syndromic surveillance. Mean values from the different research processed point to an average sensitivity and specificity of respectively 52.64% and 87.67% of different syndromic surveillance approaches. Emergency department (ED) data solely had an average of 47.34% sensitivity and 91.95% specificity according to the five different sources reporting measurements for these indicators. Average measures of timeliness from the analysed literature show lead time of 5.75 days.
Across studies, syndromic surveillance consistently offers earlier outbreak detection (2–14 days ahead of laboratory confirmation). Emergency department-based systems exhibit advantages in terms of timeliness as well as the highest sensitivity, while pharmacy sales and participatory data enhance early community-level awareness. Multi-source systems achieve the best balance between sensitivity and specificity but demand significant infrastructure and data-governance capacity. The efficacy of syndromic surveillance is significantly contingent upon data quality, integration, and contextual interpretation. Systems devoid of defined standards, compatible platforms, or consistent data inputs are susceptible to generating false alarms or overlooking critical signals. The equilibrium between sensitivity and specificity continues to be a fundamental scientific difficulty. Although expansive syndromic criteria can enhance early signal detection, they may also produce false positives that strain public health resources. Correspondingly, ethical and legal problems about personal data utilisation and privacy safeguarding must be tackled via transparent governance and comprehensive data-protection frameworks.
Incorporating artificial intelligence (AI) and machine-learning algorithms into syndromic surveillance can improve forecasting capabilities and anomaly identification. These devices can autonomously detect variations from baseline patterns and minimise response time during outbreaks. Syndromic surveillance possesses significant potential to enhance national and regional health security frameworks, contingent upon its integration into a well-coordinated and evidence-based surveillance ecosystem[55,56,57].
4. Conclusion
Biological and societal variables collectively impact the effectiveness of different methods of surveillance. The results of syndromic surveillance procedures may differ geographically, shaped by social norms and the prevalence of specific infection categories. The efficacy of the strategy depends on the accuracy of the initial risk assessment and the thresholds set, which must be modified based on observations of seasonality and cyclicality at a national or regional level.
The implementation of syndromic surveillance relies on the integration of various electronic systems and collaboration among the institutions that provide data to the platforms. The aggregation of data on syndromes should reflect prior risk-analysis to improve pandemic readiness. Future research should focus on assessing syndromic monitoring via pilot deployments that evaluate accuracy, timeliness, and public health impact, while investigating integration with AI-driven predictive analytics.
Author Contributions
Conceptualization, Z.G.. and V.R.; methodology, V.R.; validation, Z.G.; formal analysis, Z.G..; investigation, Z.G. and V.R..; resources, Z.G.; data curation, V.R.; writing—original draft preparation, Z.G and V.R..; writing—review and editing, Z.G. and V.R..; visualization, Z.G.; supervision, V.R.. All authors have read and agreed to the published version of the manuscript
Funding
Contract BG16RFPR002-1.014-0017 „Center of Competence ImmunoPathogen“, procedure BG16RFPR002-1.014 „ Sustainable development of Centers of Excellence and Centers of Competence, including specific infrastructures or their associations of the NRRI “, Programme „Research, Innovation and Digitalization for Smart Transformation 2021 – 2027".
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Acknowledgments
Contract BG16RFPR002-1.014-0017 „Center of Competence ImmunoPathogen“, procedure BG16RFPR002-1.014 „ Sustainable development of Centers of Excellence and Centers of Competence, including specific infrastructures or their associations of the NRRI “, Programme „Research, Innovation and Digitalization for Smart Transformation 2021 – 2027".
Conflicts of Interest
The authors declare no conflict of interest.
References
- Thacker, S. B., & Berkelman, R. L. Public health surveillance in the United States. Epidemiologic reviews, 1988; 10(1):164-190.
- World Health Organization. (2008). International health regulations (2005). World Health Organization.
- Milinovich, G. J., Williams, G. M., Clements, A. C., & Hu, W.. Internet-based surveillance systems for monitoring emerging infectious diseases. The Lancet infectious diseases, 2014 Feb; 14(2): 160-168. [CrossRef]
- Djibuti, M., Rukhadze, N., Hotchkiss, D. R., Eisele, T. P., & Silvestre, E. A. Health systems barriers to effective use of infectious disease surveillance data in the context of decentralization in Georgia: A qualitative study. Health Policy, 2007; 83(2-3): 323–331. [CrossRef]
- Xu, L., Zhou, C., Luo, S., Chan, D. K., McLaws, M. L., & Liang, W. Modernising infectious disease surveillance and an early-warning system: the need for China’s action. The Lancet Regional Health–Western Pacific, 2022; 23. [CrossRef]
- Serres K, Erazo D, Despréaux G, Vincenti-González MF, Van Bortel W, Arsevska E, Dellicour S. Integrating indicator-based and event-based surveillance data for risk mapping of West Nile virus, Europe, 2006 to 2021. Euro Surveill. 2024 Oct;29(44):2400084. https://pmc.ncbi.nlm.nih.gov/articles/PMC11528904/. [CrossRef]
- Sala Soler M, Fouillet A, Viso AC, Josseran L, Smith GE, Elliot AJ, et al. Assessment of syndromic surveillance in Europe. Lancet 2011;378:1833–4.
- O.W. Morgan, R.W. Pinner. Surveillance of Infectious Diseases, Editor(s): Moselio Schaechter (2009). Encyclopedia of Microbiology (Third Edition), Academic Press, 759-774.
- Semenza JC, Paz S. Climate change and infectious disease in Europe: Impact, projection and adaptation, The Lancet Regional Health - Europe, 2021 Oct; Volume 9: 100230. [CrossRef]
- Getzova Zh, Hristova I, Kunchev A, Doycheva V, Bogdanov N, Sshalamanov D., Risks from the emergence of viral hemorrhagic fevers in Bulgaria and Europe, General Medicine, 2022;3:54:60.
- Rupasinghe R, Chomel BB, Martínez-López B.Climate change and zoonoses: A review of the current status, knowledge gaps, and future trends, Acta Tropica, 2022 Feb; (226): 106225. [CrossRef]
- UK Health Security Agency (2025) First detection of West Nile virus in UK mosquitoes, available at: https://www.gov.uk/government/news/first-detection-of-west-nile-virus-in-uk-mosquitoes, last accessed: 05.12.2025.
- Tambo E, El-Dessouky AG, Khater EIM, Xianonng Z, Enhanced surveillance and response approaches for pilgrims and local Saudi populations against emerging Nipah, Zika and Ebola viral diseases outbreaks threats, Journal of Infection and Public Health, 2020 May; 13:5:674-678. [CrossRef]
- Afrooghe A, Damavandi AR, Ahmadi E. Reverse zoonosis and monkeypox: Time for a more advanced global surveillance system for emerging pathogens, New Microbes and New Infections, 2022 July; (48):101013. [CrossRef]
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020 Feb 15;395(10223):497-506. [CrossRef]
- Awadasseid A, Wu Y, Tanaka Y, Zhang W. Initial success in the identification and management of the coronavirus disease 2019 (COVID-19) indicates human-to-human transmission in Wuhan, China. Int J Biol Sci. 2020 Apr 6;16(11):1846-1860. [CrossRef]
- Wang H, Paulson KR, Pease S, et al. Estimating excess mortality due to the COVID-19 pandemic: a systematic analysis of COVID-19-related mortality, 2020–21, The Lancet, 2022 March; 399:10334:1513-1536. [CrossRef]
- Odone A, Delmonte D, Gaetti G, Signorelli C. Doubled mortality rate during the COVID-19 pandemic in Italy: quantifying what is not captured by surveillance, Public Health,2021 Jan; Volume 190:108-115. [CrossRef]
- Shah, M. R. T., Ahammed, T., Anjum, A., Chowdhury, A. A., & Suchana, A. J. Finding the real COVID-19 case-fatality rates for SAARC countries. Biosafety and health, 2021;3(3): 164-171. [CrossRef]
- WHO Director-General declares mpox outbreak a public health emergency of international concern- https://www.who.int/news/item/14-08-2024-who-director-general-declares-mpox-outbreak-a-public-health-emergency-of-international-concern, last accessed: 30 June 2025.
- O’Connell EK, Zhang G, Leguen F, et al. Innovative Uses for Syndromic Surveillance. Emerging Infectious Diseases. 2010;16(4):669-671. [CrossRef]
- Honeyman D, Gurdasani D, Notaras A, et al. Global Epidemiology of Outbreaks of Unknown Cause Identified by Open-Source Intelligence, 2020–2022. Emerging Infectious Diseases. 2025 Feb;31(2):298-308. [CrossRef]
- Barthell, E. N., Cordell, W. H., Moorhead, et al. The Frontlines of Medicine Project: A proposal for the standardized communication of emergency department data for public health uses including syndromic surveillance for biological and chemical terrorism. Annals of Emergency Medicine, 2002; 39:4:422–429. [CrossRef]
- Foldy, S., Biedrzycki, P. A., Barthell, E. N., Healy-Haney, N., Baker, B. K et al. Syndromic surveillance using regional emergency medicine internet. Annals of emergency medicine, 2004: 44(3), 242-246. [CrossRef]
- Gesteland, P. H., Gardner, R. M., Tsui, F. C., Espino, J., Rolfs, R.T. et al. Automated syndromic surveillance for the 2002 Winter Olympics. Journal of the American Medical Informatics Association, 2003; 10(6), 547-554. [CrossRef]
- Espino JU, Wagner MM. Accuracy of ICD-9-coded chief complaints and diagnoses for the detection of acute respiratory illness. Proc AMIA Symp., 2001; 164-8. PMID: 11833477.
- Reis, B. Y., & Mandl, K. D. Syndromic surveillance: the effects of syndrome grouping on model accuracy and outbreak detection. Annals of Emergency Medicine, 2004; 44:3: 235–241. [CrossRef]
- Morbey R. Communicating the detection capabilities of syndromic surveillance systems. Online J Public Health Inform. 2019 May 30;11(1):e304. https://pmc.ncbi.nlm.nih.gov/articles/PMC6606168/. [CrossRef]
- GUASTICCHI G, GIORGI ROSSI P, LORI G, et al. Syndromic surveillance: sensitivity and positive predictive value of the case definitions. Epidemiology and Infection. 2009;137(5):662-671. https://www.cambridge.org/core/journals/epidemiology-and-infection/article/syndromic-surveillance-sensitivity-and-positive-predictive-value-of-the-case-definitions/B7AC1092414E3A2D54A9A1C8B1548F9E. [CrossRef]
- Roberts, R.R, Einstein, A., Ahmad, I., Gore, R., Kampe, L.M. et al. Improving Syndrome Surveillance Case Definitions and Outcomes by Using Existing Data. Annals of Emergency Medicine, 2005; 46:3, 24. [CrossRef]
- Barthell E.N., Aronsky D., Cochrane D.G., Cable G. et al. For the Frontlines Work Group. The frontlines of medicine project progress report: standardized communication of emergency department triage data for syndromic surveillance. Annals of Emergency Medicine, 2004; 44:3, 247–252. [CrossRef]
- Lober W.B., Karras B.T., Wagner M.M., Overhage J.M., Davidson A.J., Fraser H. et al. Roundtable on bioterrorism detection: information system–based surveillance. Journal of the American Medical Informatics Association, 2002; 9(2), 105-115. [CrossRef]
- Wagner M.M., Tsui FC, Espino J.U. et al. The Emerging Science of Very Early Detection of Disease Outbreaks. Journal of Public Health Management and Practice, 2001; 7:6, 51–59. [CrossRef]
- Mandl, K.D.. Implementing Syndromic Surveillance: A Practical Guide Informed by the Early Experience. Journal of the American Medical Informatics Association, 2003; 11:2, 141–150. [CrossRef]
- Cameron AR, Meyer A, Faverjon C, Mackenzie C. Quantification of the sensitivity of early detection surveillance. Transbound Emerg Dis. 2020 Nov;67(6):2532-2543. [CrossRef]
- McNabb, S. J., Jajosky, R. A., Hall-Baker, P. A., Adams, D. A., Sharp, P., Anderson, W.J. et al. Centers for Disease Control and Prevention (CDC). Summary of notifiable diseases—United States, 2005. MMWR Morb Mortal Wkly Rep, 2007; 54(53), 1-92.
- Pang X, Wang X, Wang Q, Gao T, Li X Chapter 8 - Infectious Disease Surveillance and Early Warning System During Beijing Olympic Games, Editor(s): Weizhong Yang, Early Warning for Infectious Disease Outbreak, Academic Press, 2017; 163-180. [CrossRef]
- Sugishita Y., Sugawara T., Ohkusa Y., Ishikawa T., Yoshida M, Endo, H. Syndromic surveillance using ambulance transfer data in Tokyo, Japan. Journal of Infection and Chemotherapy, 2020; 26(1), 8-12. [CrossRef]
- Tarnas MC, Desai AN, Parker DM,Almhawish N, Zakieh O, Rayes D, et al. Syndromic surveillance of respiratory infections during protracted conflict: experiences from northern Syria 2016-2021, International Journal of Infectious Diseases, 2022; Volume 122, 337-344. [CrossRef]
- Welliver RC, Cherry JD, Boyer KM, et al. Sales of nonprescription cold remedies: a unique method of influenza surveillance. Pediatr Res 1979;13:1015--7.
- Angulo FJ, Tippen S, Sharp DJ, et al. A community waterborne outbreak of salmonellosis and the effectiveness of a boil water order. Am J Public Health 1997;87:580—4.
- Proctor ME, Blair KA, Davis JP. Surveillance data for waterborne illness detection: an assessment following a massive waterborne outbreak of Cryptosporidium infection. Epidemiol Infect 1998;120:43--54.
- Stirling R, Aramini J, Ellis A, et al. Waterborne cryptosporidiosis outbreak, North Battleford, Saskatchewan, Spring 2001. Can Commun Dis Rep 2001;27:185--92.
- Hogan WR, Tsui F-C, Ivanov O, et al. Early detection of pediatric respiratory and diarrheal outbreaks from retail sales of electrolyte products. J Am Med Inform Assoc 2003;10:555--62.
- Magruder S. Evaluation of over-the-counter pharmaceutical sales as a possible early warning indicator of public health. Johns Hopkins University Applied Physics Laboratory Technical Digest 2003; 24:349--53.
- Pivette, M., Mueller, J. E., Crépey, P., & Bar-Hen, A. (2014). Drug sales data analysis for outbreak detection of infectious diseases: a systematic literature review. BMC infectious diseases, 14, 604. [CrossRef]
- Das D, Metzger K, Heffernan R, Balter S, Weiss D, Mostashari F: Monitoring over-the-counter medication sales for early detection of disease outbreaks-New York City. MMWR Morb Mortal Wkly Rep. 2005, 54 (Suppl): 41-46.
- Yoshida M, Matsui T, Ohkusa Y, Kobayashi J, Ohyama T, Sugawara T, Yasui Y, Tachibana T, Okabe N: Seasonal influenza surveillance using prescription data for anti-influenza medications. Jpn J Infect Dis. 2009, 62: 233-235. [CrossRef]
- Chunara R., Goldstein E., Patterson-Lomba O. et al. Estimating influenza attack rates in the United States using a participatory cohort. Sci Rep 2015; 5, 9540. [CrossRef]
- Guerrisi C, Turbelin C, Blanchon T, et al. Participatory Syndromic Surveillance of Influenza in Europe, The Journal of Infectious Diseases, 2016; Volume 214, Issue suppl_4:S386–S392. [CrossRef]
- Mahmud AS, Chowdhury S, Sojib KH, et al.Participatory syndromic surveillance as a tool for tracking COVID-19 in Bangladesh, Epidemics, 2021; Volume 35, 100462. [CrossRef]
- Thomas, R.G., Hemphill, RR.,Aronsky, D. Syndromic surveillance for infectious disease outbreaks using chief complaint data. Annals of Emergency Medicine, 2004; 44(4), S124. [CrossRef]
- Bellazzini MA, Minor KD. ED syndromic surveillance for novel H1N1 spring 2009, The American Journal of Emergency Medicine, 2011; 29:1, 70-74. [CrossRef]
- Rosenkötter N, Ziemann A, Riesgo LG, Gillet JB, Vergeiner G, Krafft T, Brand H. Validity and timeliness of syndromic influenza surveillance during the autumn/winter wave of A (H1N1) influenza 2009: results of emergency medical dispatch, ambulance and emergency department data from three European regions. BMC Public Health. 2013 Oct 1;13:905. https://pmc.ncbi.nlm.nih.gov/articles/PMC3852468/. [CrossRef]
- Chikotie, T., Watson, B., Kimanuka, U., & Banda, T. (2025, May). Leveraging Electronic Syndromic Surveillance Synthetic Data to Predict Diarrhoea in Zimbabwean Children Under-Five: An Explainable AI Framework. In 2025 IST-Africa Conference (IST-Africa) (pp. 1-10). IEEE.
- Parums, D. V. (2023). infectious disease surveillance using artificial intelligence (AI) and its role in epidemic and pandemic preparedness. Medical science monitor: international medical journal of experimental and clinical research, 29, e941209-1.
- Lake, I. R., Colón-González, F. J., Barker, G. C., Morbey, R. A., Smith, G. E., & Elliot, A. J. (2019). Machine learning to refine decision making within a syndromic surveillance service. BMC Public Health, 19(1), 559.
Figure 1.
Suggested model of Hybrid/Multi-source System information exchange [23,24,25,26,27,28,29,30,31,32,33,34].
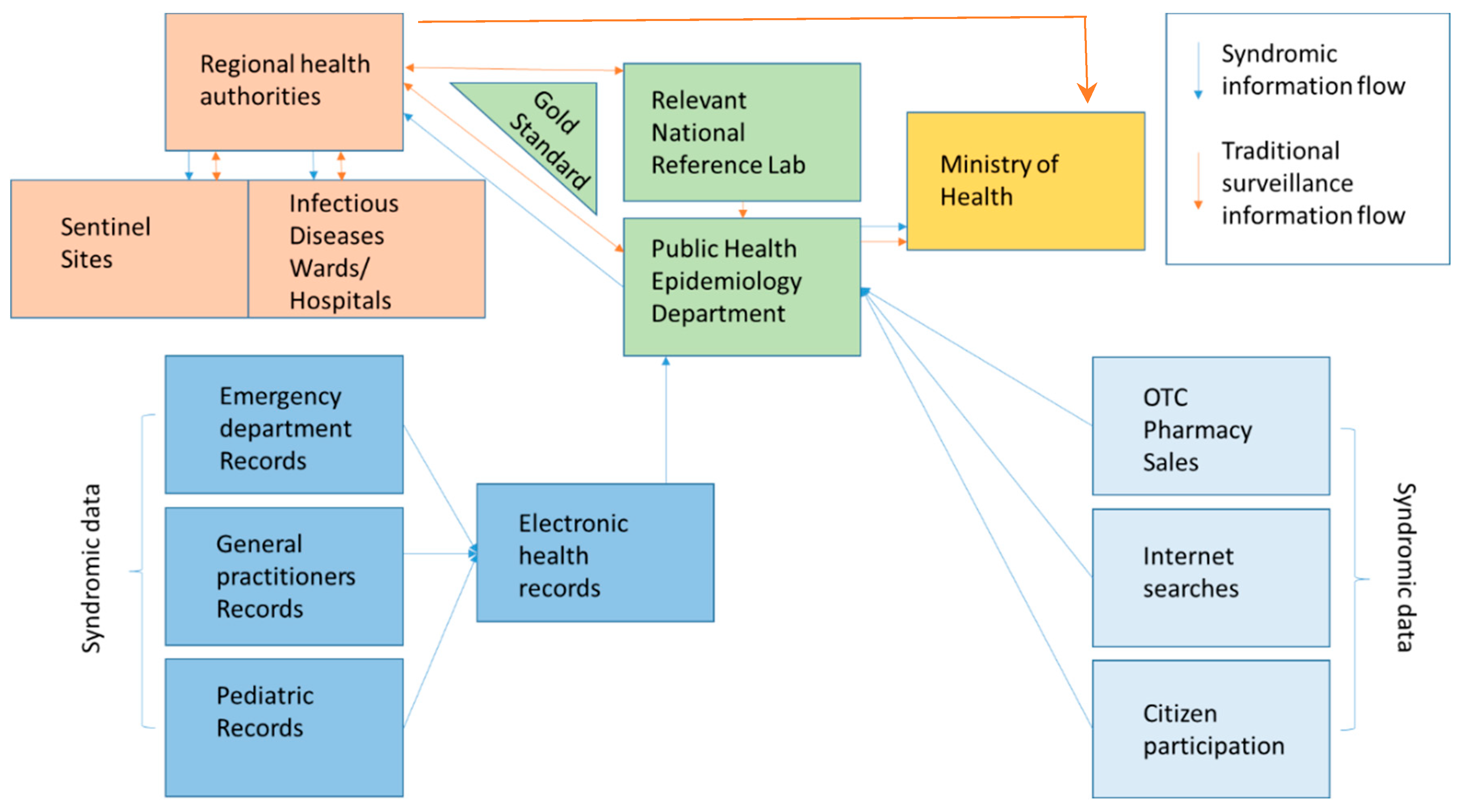

Table 1.
Comparative advantages and limitations of syndromic surveillance data sources.
| Data Source | Example System / Study | Lead Time (vs. Lab Confirmation) | Sensitivity / Specificity | Advantages | Limitations |
|---|---|---|---|---|---|
| Emergency Department Records | Espino et al. [26] | 4–7 days earlier | Sensitivity 44%, Specificity 97% | Timely, structured, standardized ICD coding | Requires integration across facilities; may miss mild cases |
| Emergency Department Records | Morbey R. [28] | Up to 7 days earlier | Sensitivity 100% for seasonal influenza and 0% for seasonal adenovirus | Early; adaptable | Detection highly dependent on system organization |
| Emergency Department Records | Reis, B. Y., & Mandl, K. D. [27] | 1-day detection approach | Sensitivity 26-47% Specificity 93% |
Early, information available in real-time, possibility to incorporate different data sources (symptom-based/diagnostic); temporal smoothing filters might reduce noise | Chief complaints lower accuracy |
| Emergency Department Records | Guasticchi G, Giorgi Rossi P, Lori G, et al. [29] | - | Variable, disease-specific: Sensitivity 22.2-90.2 |
Information routinely collected, Automated | Results are highly dependent on syndrome definition |
| Emergency Department Records | Rosenkötter N, Ziemann A, Riesgo LG et al.[54] | Up to 8 days earlier | Variable depending on country and source: Sensitivity 0-100%, Specificity 57.1-88.9% |
Strong validity and timeliness of data | Results differ across countries due to differences in catchment population. In some cases identification of events is later than references. |
| Pharmacy / OTC Sales | Das et al., 2005 [47]; Hogan et al., 2003 [44] | 2–14 days earlier | Variable, disease-specific | Early community signal; inexpensive; easy to automate | False positives; context-dependent on self-medication patterns |
| Participatory (Citizen Reports) | Chunara et al. 2015[49]; Mahmud et al., 2021 [51] | 3–5 days earlier | High correlation with lab-confirmed data | Engages public; rapid; adaptable | Participation bias; data validation required |
| Hybrid / Multi-source Systems | Foldy et al. 2004 [24] | 2–10 days earlier | Improved combined sensitivity | Comprehensive, scalable; high analytic power | Requires strong IT infrastructure and privacy safeguards |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



