
Submitted:
22 December 2025
Posted:
23 December 2025
You are already at the latest version
Abstract
Background: Childhood obesity represents the most common nutritional and metabolic disorder in industrialized countries and constitutes a major public health concern. In Italy, 20–25% of school-aged children are overweight and 10–14% are obese, with marked regional variability [1–6]. Excess adiposity in childhood is frequently associated with hypertension, dyslipidemia, insulin resistance, and non-alcoholic fatty liver disease (NAFLD), predisposing to future cardiovascular disease (CVD). Objective: To investigate anthropometric indicators of cardiometabolic risk in 810 children and adolescents aged 7–17 years who underwent assessment for competitive sports eligibility at the Sports Medicine Unit of Modena, evaluate baseline knowledge of cardiovascular health aligned with ESC, AAP [2023], and EASO guidelines. [4–6] Methods: 810 children and adolescents aged 7–17 years undergoing competitive sports eligibility assessment at the Sports Medicine Unit of Modena underwent evaluation of BMI percentile, waist circumference (WC), waist-to-height ratio (WHtR), and blood pressure. Cardiovascular knowledge and lifestyle habits were assessed via a a previously used questionnaire. Anthropometric parameters, blood pressure (BP), and lifestyle-related knowledge and behaviors were assessed using standardized procedures. Overweight and obesity were defined according to WHO BMI-for-age percentiles. Elevated BP was classified based on the 2017 American Academy of Pediatrics age-, sex-, and height-specific percentiles. Statistical analyses included descriptive statistics, group comparisons, chi-square tests with effect size estimation, correlation analyses, and multivariable logistic regression models. Results: Overall, 22% of participants were overweight and 14% obese. WHtR > 0.5 was observed in 28% of the sample and was more frequent among overweight/obese children (p < 0.001). Elevated BP was detected in 12% of participants with available measurements (n = 769) and was significantly associated with excess adiposity (χ² = 7.21, p < 0.01; Cramér’s V = 0.27). In multivariable logistic regression analyses adjusted for age and sex, WHtR > 0.5 (OR 2.14, 95% CI 1.32–3.47, p = 0.002) and higher sedentary time (OR 1.41 per additional daily hour, 95% CI 1.10–1.82, p = 0.006) were independently associated with elevated BP, whereas BMI percentile lost significance when WHtR was included in the model. Lifestyle knowledge scores were significantly lower among overweight and obese participants compared with normal-weight peers (p < 0.01). Conclusions: WHtR is a sensitive early marker of cardiometabolic risk, often identifying at-risk children missed by BMI alone. Baseline cardiovascular knowledge was suboptimal. The observed gaps in cardiovascular knowledge underscore the importance of integrating anthropometric screening with structured educational interventions to promote healthy lifestyles and long-term cardiovascular prevention.
Keywords:
pediatric obesity
; waist-to-height ratio (WHtR)
; cardiometabolic risk
; early cardiovascular prevention
; lifestyle education
1. Introduction
Childhood obesity has reached epidemic proportions globally and is increasingly recognized as a major determinant of long-term cardiovascular morbidity [1,2,3,4]. Excess body weight acquired during childhood tracks strongly into adulthood and contributes to the early development of hypertension, dyslipidemia, insulin resistance, and structural cardiovascular alterations. Importantly, atherosclerotic processes begin early in life, well before the clinical manifestation of cardiovascular disease, highlighting the critical importance of early identification and prevention strategies.
In Europe, and particularly in Italy, the prevalence of pediatric overweight and obesity remains alarmingly high despite decades of public health initiatives [1,2,3]. National surveillance data indicate that approximately one in three Italian children carries excess body weight, with significant regional and socioeconomic disparities. These trends raise concern not only for future cardiovascular disease burden but also for the early emergence of cardiometabolic alterations during childhood and adolescence.
Pediatric obesity is not a homogeneous condition. Central adiposity plays a pivotal role in the pathophysiology of early cardiometabolic risk. Visceral fat tissue is metabolically active and promotes chronic low-grade inflammation through increased secretion of pro-inflammatory cytokines and altered adipokine profiles, contributing to insulin resistance, endothelial dysfunction, arterial stiffness, and ectopic fat deposition [7,8]. These mechanisms accelerate vascular aging and may lead to early blood pressure elevation and cardiac remodeling even in young individuals [9,10].
Anthropometric indicators represent simple, low-cost, and widely applicable tools for early risk stratification. Although BMI percentile remains the most commonly used measure in pediatric practice, it does not adequately capture fat distribution or visceral adiposity. In contrast, waist-to-height ratio (WHtR) provides a reliable and age-independent estimate of central fat accumulation and has shown stronger associations with cardiometabolic risk factors, including hypertension, dyslipidemia, insulin resistance, and subclinical atherosclerosis [10,11,12,13,14,15]. A WHtR threshold of 0.5 has been proposed as a practical cut-off for identifying increased cardiometabolic risk in children and adolescents.
Beyond biological risk factors, lifestyle behaviours and cardiovascular health literacy play a crucial role in shaping early risk trajectories. Physical inactivity, excessive sedentary behaviour, and unhealthy dietary habits frequently cluster with obesity and central adiposity. Educational interventions focusing on nutrition and physical activity have demonstrated beneficial effects on both knowledge and cardiometabolic profiles [15,16,17,18]. However, data integrating anthropometric screening with cardiovascular education in Italian pediatric populations remain limited.
Children undergoing competitive sports eligibility assessment represent a unique and underexplored population. Although they are often perceived as healthy and physically active, cardiometabolic risk factors may remain undetected without targeted screening. Sports medicine evaluations offer a structured and repeated point of contact with healthcare professionals and thus represent an underutilized opportunity for both early risk identification and cardiovascular education.
The present study aimed to assess anthropometric indicators of cardiometabolic risk and baseline cardiovascular health knowledge in a large cohort of children and adolescents undergoing competitive sports eligibility evaluation. By integrating biological and behavioural dimensions, this study seeks to highlight the role of WHtR as an early marker of cardiometabolic vulnerability and to underscore the importance of education in pediatric cardiovascular prevention.
2. Methods
A cross-sectional study was conducted among 810 children and adolescents aged 7–17 years presenting for mandatory competitive sports eligibility assessment at the Sports Medicine Unit of Modena. In Italy, participation in competitive sports requires a specialist medical evaluation including anthropometric measurements, blood pressure assessment, and electrocardiography. Children with chronic systemic diseases affecting growth or metabolism were excluded.
2.1. Anthropometric Assessment
Height was measured to the nearest 0.1 cm using a wall-mounted stadiometer, and body weight was measured to the nearest 0.1 kg using a calibrated digital scale, with participants wearing light clothing and no shoes. BMI was calculated as kg/m2 and expressed as age- and sex-specific percentiles according to WHO growth reference standards. Waist circumference was measured midway between the lowest rib and the iliac crest using a non-elastic tape, and WHtR was calculated as waist circumference divided by height. A WHtR >0.5 was considered indicative of increased cardiometabolic risk [11,13,14,15].
2.2. Blood Pressure Measurement
Resting blood pressure was measured after at least five minutes of seated rest using validated pediatric devices and appropriate cuff sizes. Blood pressure was classified according to age-, sex-, and height-specific percentiles in accordance with the 2017 American Academy of Pediatrics guidelines.
2.3. Cardiovascular Knowledge and Lifestyle Assessment
Cardiovascular awareness and lifestyle habits were assessed using a 20-item questionnaire previously used in pediatric cardiovascular prevention settings [16,17,18]. Items evaluated knowledge of physical activity recommendations, dietary risk factors, sedentary behaviour, and the association between overweight and cardiovascular disease. Responses were scored as correct or incorrect, and a composite knowledge score was calculated as the percentage of correct answers. Internal consistency in the present cohort was acceptable (Cronbach’s α = 0.76). Average daily sedentary time was self-reported and expressed as hours per day [4,9,16].
2.4. Statistical Analysis
Data were analysed using descriptive statistics, with means ± standard deviations (SD) for continuous variables and percentages for categorical variables. Normality was assessed using Shapiro–Wilk tests. Independent t-tests or Mann–Whitney U tests were used as appropriate. Chi-square tests evaluated associations between categorical variables, with Cramér’s V estimating effect sizes (small 0.1, medium 0.3, large 0.5).
Pearson correlation coefficients quantified relationships between anthropometric measures, blood pressure, and sedentary behaviour. Multiple logistic regression analyses were performed to assess the independent contribution of WHtR, BMI percentile, and sedentary time to elevated blood pressure, adjusting for age and sex. Multicollinearity was assessed using variance inflation factors, and model fit was evaluated using the Hosmer–Lemeshow test. Cardiovascular knowledge scores were compared across BMI categories using analysis of covariance (ANCOVA), controlling for age and sex. Analyses involving blood pressure were conducted using complete-case analysis. Statistical significance was set at p <0.05.
3. Results
A total of 810 children and adolescents were included in the anthropometric analyses. Of these, 389 (48.0%) were female and 417 (51.5%) were male, while sex data were unavailable for four participants (0.5%), who were excluded from sex-stratified analyses. The mean age of the study population was 13.6 ± 2.1 years. Baseline demographic and anthropometric characteristics are summarized in Table 1.
Mean body mass index was 20.3 ± 3.4 kg/m2. According to WHO BMI-for-age percentiles, 64% of participants were classified as normal weight, 22% as overweight, and 14% as obese.
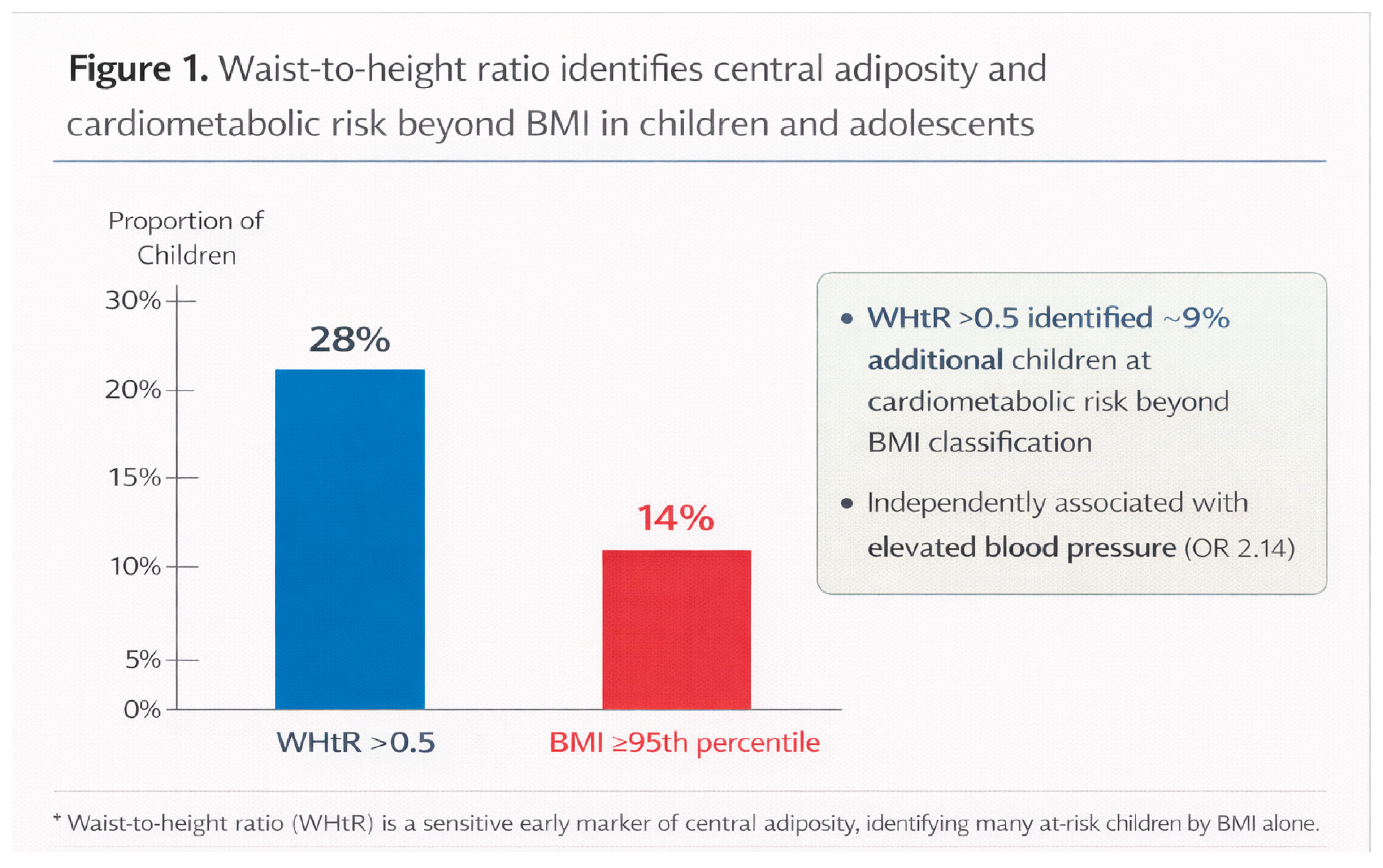
A WHtR >0.5 was observed in 28% of the overall cohort, indicating a high prevalence of central adiposity. Importantly, WHtR identified a subset of children with increased cardiometabolic risk who would not have been classified as overweight or obese based on BMI criteria alone. Approximately 9% of participants with normal BMI percentiles exhibited a WHtR >0.5, highlighting the added discriminatory value of WHtR beyond BMI classification (Figure 1).
The prevalence of WHtR >0.5 increased progressively across BMI categories, being lowest among normal-weight participants and highest among obese children (p <0.001 by chi-square test), confirming the strong association between excess body mass and central fat accumulation.
Resting blood pressure measurements were available for 769 participants (94.9%). Elevated blood pressure, defined according to age-, sex-, and height-specific percentiles, was detected in 12% of the evaluated cohort.
Elevated blood pressure was significantly more prevalent among participants with excess adiposity. Specifically, children classified as overweight or obese exhibited a higher proportion of elevated blood pressure compared with their normal-weight peers (χ2 = 7.21, p <0.01), with a moderate effect size (Cramér’s V = 0.27), indicating a clinically meaningful association (Table 2).
When stratified by central adiposity, participants with WHtR >0.5 showed a markedly higher prevalence of elevated blood pressure compared with those with WHtR ≤0.5 (p <0.001), underscoring the relevance of central fat distribution in early blood pressure elevation.
To assess the independent contribution of anthropometric and lifestyle factors to elevated blood pressure, multivariable logistic regression analyses were performed, adjusting for age and sex (Table 2; Figure 2).
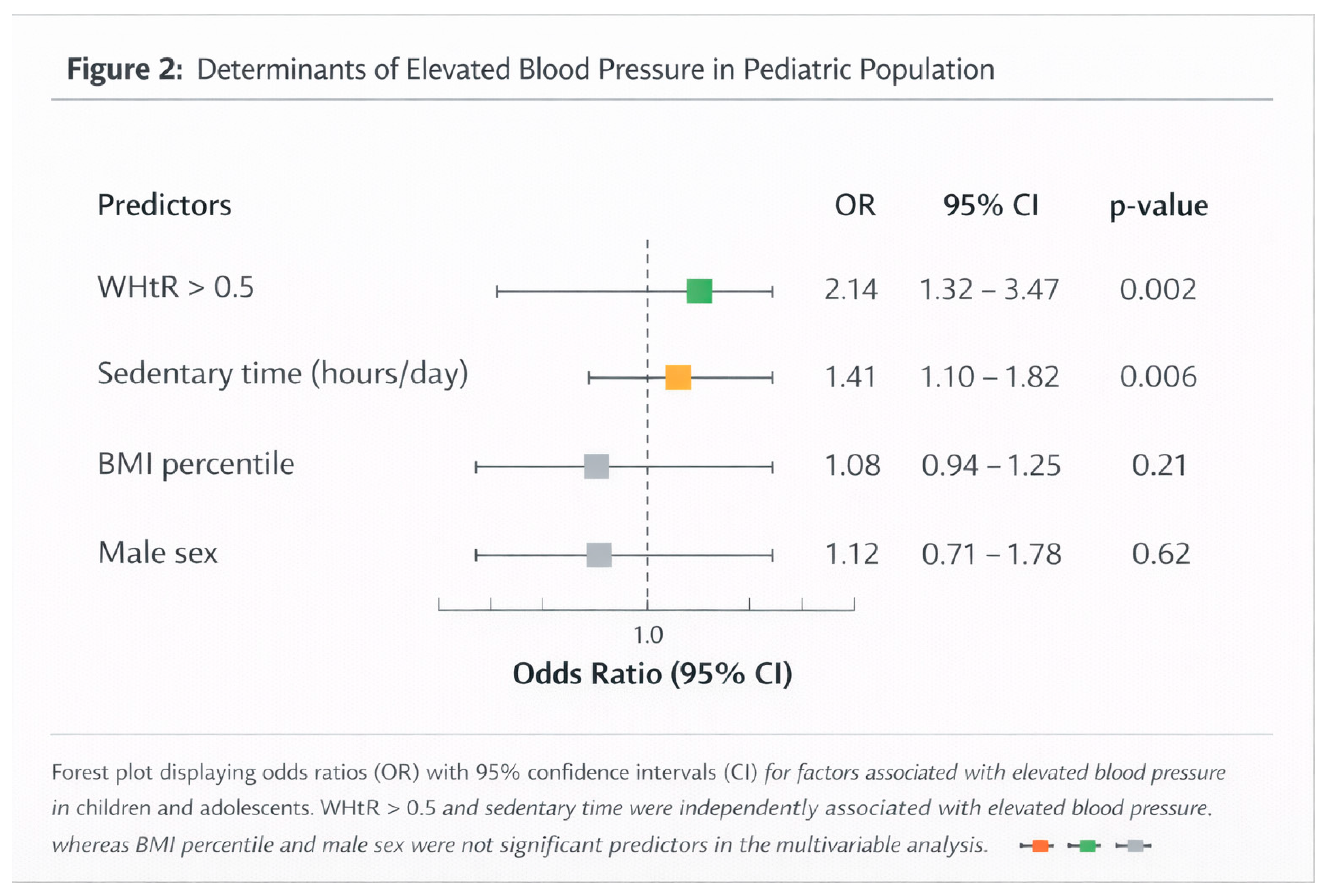
In these models, WHtR >0.5 emerged as an independent predictor of elevated blood pressure (OR 2.14, 95% CI 1.32–3.47, p = 0.002). Additionally, sedentary time was independently associated with elevated blood pressure, with a 41% increase in odds per additional hour per day (OR 1.41, 95% CI 1.10–1.82, p = 0.006).
In contrast, BMI percentile did not retain statistical significance when WHtR was included in the model, suggesting that central adiposity, rather than overall body mass, represents the primary anthropometric determinant of early blood pressure elevation in this population. No evidence of multicollinearity was detected among predictors, and model fit was adequate.
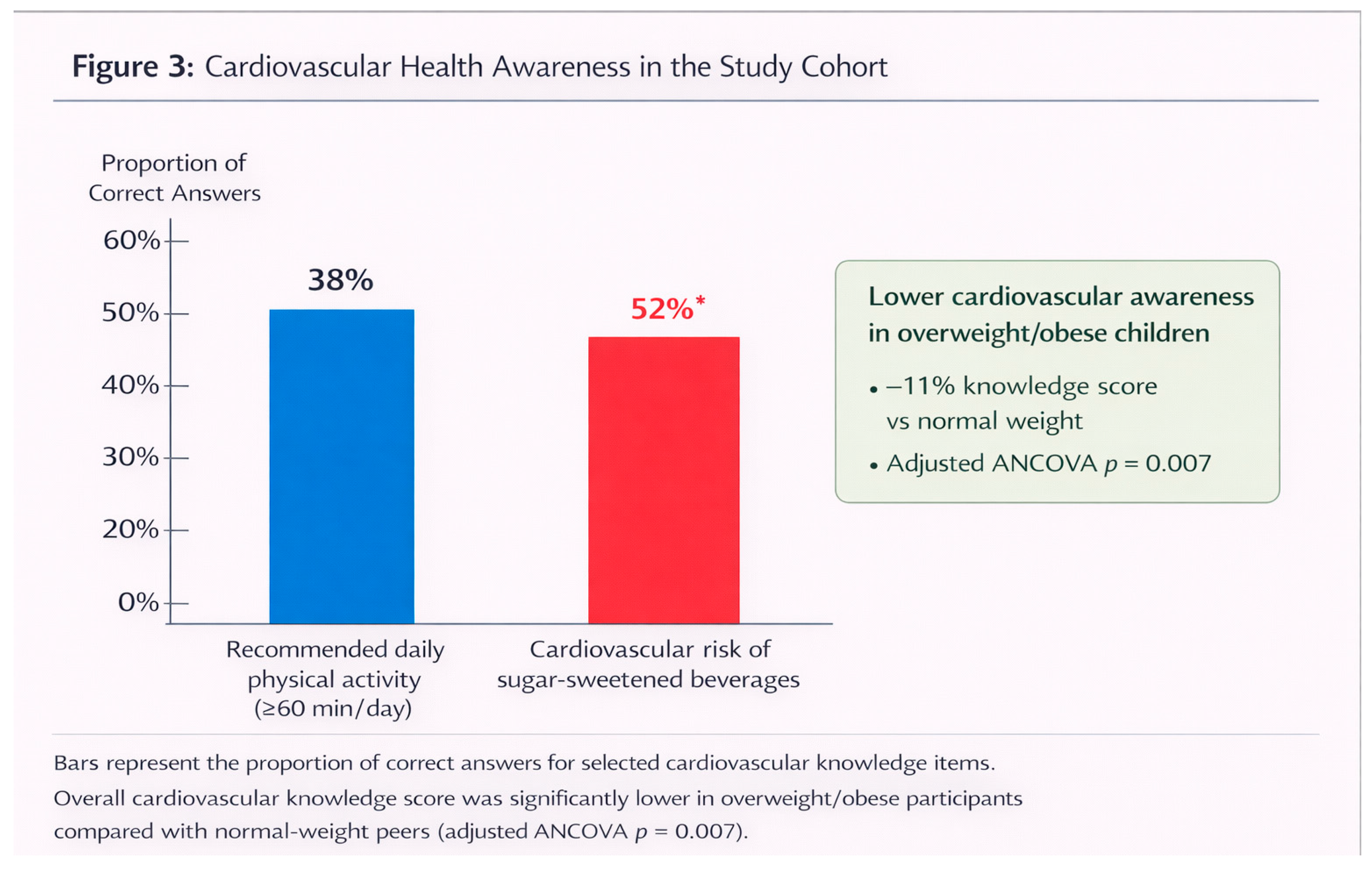
Baseline cardiovascular health knowledge was generally limited across the cohort. Only 38% of participants correctly identified recommended daily levels of physical activity, and 52% underestimated the cardiovascular risks associated with excessive consumption of sugar-sweetened beverages (Figure 3).
Cardiovascular knowledge scores differed significantly across BMI categories. Overweight and obese participants demonstrated significantly lower knowledge scores compared with normal-weight peers (mean difference 11%, p <0.05). This association remained statistically significant after adjustment for age and sex using analysis of covariance (F = 7.43, p = 0.007), indicating that reduced cardiovascular awareness clustered with excess adiposity independently of demographic factors.
4. Discussion
The present study provides robust evidence supporting the integration of anthropometric screening and educational strategies in early cardiovascular prevention among children and adolescents. In a large cohort undergoing competitive sports eligibility assessment, waist-to-height ratio (WHtR) emerged as a particularly sensitive indicator of early cardiometabolic risk, outperforming BMI in identifying children with elevated blood pressure and central adiposity. In parallel, the study highlights substantial gaps in cardiovascular health knowledge, especially among overweight and obese participants, underscoring the critical role of education in shaping early risk trajectories.
A key finding of this study is the high prevalence of central adiposity, as reflected by a WHtR >0.5 in nearly one-third of participants. Importantly, WHtR identified a clinically relevant subgroup of children with normal BMI percentiles but increased central fat accumulation (Figure 1). This observation confirms and extends previous evidence showing that BMI alone may underestimate cardiometabolic risk in pediatric populations, as it does not capture fat distribution or visceral adiposity [11,12,13,14,15]. Central adiposity is metabolically active and plays a pivotal role in the pathophysiology of early cardiovascular risk through mechanisms involving chronic low-grade inflammation, altered adipokine secretion, insulin resistance, endothelial dysfunction, and increased arterial stiffness [7,8,9]. These processes can accelerate vascular aging and promote early elevations in blood pressure, even in the absence of overt obesity.
The association between central adiposity and elevated blood pressure observed in this study is clinically meaningful. Elevated blood pressure was significantly more prevalent among children with WHtR >0.5, and this relationship remained robust after adjustment for age and sex in multivariable logistic regression analyses (Table 2; Figure 2). Notably, when WHtR was included in the model, BMI percentile lost statistical significance, suggesting that fat distribution rather than overall body mass is the primary anthropometric determinant of early blood pressure elevation in this population. These findings align with growing evidence that WHtR represents a simple, age-independent, and highly informative screening tool for early cardiometabolic risk stratification in children and adolescents [11,12,13,15].
Beyond anthropometric factors, lifestyle behaviours emerged as important contributors to early cardiovascular risk. Sedentary time was independently associated with elevated blood pressure, with a progressive increase in risk for each additional hour of daily sedentary behaviour. This finding reinforces the concept that physical inactivity and prolonged sedentary behaviour exert deleterious effects on vascular health, independent of adiposity [19,20,21]. Sedentary lifestyles promote visceral fat accumulation, impair insulin sensitivity, and contribute to autonomic imbalance and vascular dysfunction, thereby amplifying cardiometabolic vulnerability during critical developmental periods.
Equally concerning is the low level of baseline cardiovascular health knowledge observed in this cohort. Despite undergoing sports medical evaluation, fewer than half of participants demonstrated adequate awareness of recommended physical activity levels, dietary risk factors, or the link between obesity and cardiovascular disease (Figure 3). Importantly, cardiovascular knowledge scores were significantly lower among overweight and obese children, even after adjustment for age and sex. This clustering of biological risk and reduced health literacy suggests a bidirectional relationship in which limited awareness may contribute to unhealthy behaviours, while excess adiposity may further reinforce adverse lifestyle patterns.
The relevance of these findings is further amplified by recent Italian data demonstrating a persistent decline in youth physical activity and sports participation following the COVID-19 pandemic, accompanied by increased sedentary behaviour [22]. Although the present cohort represents a positively selected population—children and adolescents eligible for competitive sports—the prevalence of central adiposity, elevated blood pressure, and limited cardiovascular knowledge remains substantial. This observation strongly suggests that the burden of early cardiometabolic risk in the general pediatric population is likely even greater.
Sports medicine evaluations represent a unique and underutilized opportunity for early cardiovascular prevention. These assessments provide structured, repeated contact with healthcare professionals and allow for the simultaneous evaluation of anthropometric risk factors and delivery of targeted educational messages. The integration of routine WHtR measurement into sports eligibility screening is particularly appealing due to its simplicity, low cost, and strong association with cardiometabolic outcomes. Coupling anthropometric screening with brief, structured educational interventions may enhance awareness, promote healthier lifestyle choices, and facilitate early behavioural change.
From a broader public health perspective, the findings of this study support a proactive, multidimensional approach to pediatric cardiovascular prevention. Educational interventions implemented in schools, sports settings, and family environments have been shown to improve physical activity levels, dietary habits, and cardiometabolic profiles [23,24,25,26]. Early lifestyle modifications, even when modest, can yield meaningful physiological benefits, including improved insulin sensitivity, reduced inflammatory burden, and enhanced endothelial function, with long-term implications for cardiovascular health.
Overall, this study reinforces current international recommendations advocating for early identification of cardiometabolic risk and the promotion of healthy behaviours beginning in childhood [4,5,6,16,17,18]. The combined assessment of central adiposity, blood pressure, lifestyle behaviours, and cardiovascular knowledge offers a comprehensive framework for early risk stratification and intervention. By fostering awareness and healthy habits at a young age, such strategies hold the potential to alter lifelong cardiovascular trajectories and reduce the future burden of cardiovascular disease.
5. Limitations
Limitations include the cross-sectional design and reliance on self-reported lifestyle data. The population was also limited to children and adolescents undergoing sports eligibility screening. Nonetheless, the large sample and comprehensive assessment of anthropometric and behavioural variables provide strong evidence for the early identification of risk and the critical role of education in promoting cardiovascular health.
Longitudinal studies with objective activity monitoring, metabolic profiling, and cardiovascular imaging are warranted to assess the long-term impact of early interventions.
Although the questionnaire was not originally developed as a formal psychometric instrument, the acceptable internal consistency observed in this large pediatric cohort supports its use for estimating baseline cardiovascular knowledge.
6. Conclusions
Early recognition of cardiometabolic risk in children is feasible using simple anthropometric measures, particularly WHtR. Baseline cardiovascular knowledge is limited, particularly among overweight/obese children, emphasizing the importance of education.
Educational interventions combining anthropometric screening with promotion of physical activity, healthy nutrition, and cardiovascular awareness are essential for fostering healthy behaviours, ensuring current well-being, and preventing long-term cardiovascular disease. [24,25,26]
These findings support the integration of structured school- and family-based prevention programmes into routine pediatric care, complementing broader public health strategies to mitigate long-term cardiovascular risk.
Funding
No external funding was received.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Istituto Superiore di Sanità (ISS). OKkio alla SALUTE—Indagine nazionale 2023: i dati nazionali. EpiCentro. 2024. Available online: https://www.epicentro.iss.it/okkioallasalute/indagine-2023-dati (accessed on 12 December 2025).
- World Health Organization; Regional Office for Europe. Italy: over 20% of children are overweight, says new report. WHO Europe news release. 2020 Dec 9. Available online: https://www.who.int/europe/news/item/09-12-2020-italy-over-20-of-children-are-overweight-says-new-report (accessed on 12 December 2025).
- Nittari, G.; Scuri, S.; Petrelli, F.; Pirillo, I.; Di Luca, N.M.; Grappasonni, I. Fighting obesity in children from European World Health Organization member states: epidemiological data, medical-social aspects and prevention programs. Clin Ter. 2019, 170, e223–e230. [Google Scholar] [PubMed]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Hampl, S.E.; Hassink, S.G.; Skinner, A.C.; et al. Clinical Practice Guideline for the Evaluation and Treatment of Children and Adolescents With Obesity. Pediatrics 2023, 151, e2022060640. [Google Scholar] [CrossRef] [PubMed]
- Hassapidou, M.; et al. EASO and EFAD Position Statement on Medical Nutrition Therapy for the Management of Overweight and Obesity in Children and Adolescents. Obes Facts 2023, 16, 29–52. [Google Scholar] [CrossRef] [PubMed]
- Hertiš Petek, T.; Marčun Varda, N. Childhood Cardiovascular Health, Obesity, and Some Related Disorders: Insights into Chronic Inflammation and Oxidative Stress. Int J Mol Sci. 2024, 25, 9706. [Google Scholar] [CrossRef] [PubMed]
- Calcaterra, V.; Regalbuto, C.; Porri, D.; et al. Inflammation in Obesity-Related Complications in Children: The Protective Effect of Diet and Its Potential Role as a Therapeutic Agent. Biomolecules 2020, 10, 1324. [Google Scholar] [CrossRef] [PubMed]
- Delvecchio, M.; Salerno, M.; Acquafredda, A.; et al. Cardiovascular Implications in Idiopathic and Syndromic Obesity in Childhood: An Update. Front Endocrinol (Lausanne) 2020, 11, 330. [Google Scholar] [CrossRef] [PubMed]
- Mihuta, M.S.; et al. Subclinical Atherosclerosis Progression in Obese Children with Relevant Cardiometabolic Risk Factors Can Be Assessed through Carotid Intima Media Thickness. Appl Sci (Basel) 2021, 11, 10721. [Google Scholar] [CrossRef]
- Zong, X.; Kelishadi, R.; Hong, Y.M.; et al. Establishing international optimal cut-offs of waist-to-height ratio for predicting cardiometabolic risk in children and adolescents aged 6–18 years. BMC Med. 2023, 21, 349. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Dou, Y.; Chen, H.; et al. Performance of waist-to-height ratio as a screening tool for identifying cardiometabolic risk in children: a meta-analysis. Diabetol Metab Syndr. 2021, 13, 66. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Shim, Y.S.; Yoon, J.S.; et al. Distribution of waist-to-height ratio and cardiometabolic risk in children and adolescents: a population-based study. Sci Rep. 2021, 11, 9524. [Google Scholar] [CrossRef] [PubMed]
- López-González, D.; Miranda-Lora, A.; Klünder-Klünder, M.; et al. Diagnostic performance of waist circumference measurements for predicting cardiometabolic risk in mexican children. Endocr Pract. 2016, 22, 1170–1176. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Dou, Y.L.; Xiong, F.; et al. Waist-to-height ratio remains an accurate and practical way of identifying cardiometabolic risks in children and adolescents. Acta Paediatr. 2018, 107, 1960–1967. [Google Scholar] [CrossRef] [PubMed]
- Martino, F.; Bassareo, P.P.; Martino, E.; et al. Cardiovascular prevention in childhood: a consensus document of the Italian Society of Cardiology Working Group on Congenital Heart Disease and Cardiovascular Prevention in Paediatric Age. J Cardiovasc Med (Hagerstown) 2023, 24, 492–505. [Google Scholar] [CrossRef] [PubMed]
- Tully, L.; Ní Choncubhair, S.; Korczak, D.J.; et al. Guidelines for treating child and adolescent obesity: a narrative review of recommendations. Front Nutr. 2022, 9, 902865. [Google Scholar] [CrossRef] [PubMed]
- Maffeis, C.; et al. The treatment of obesity in children and adolescents: consensus position statement of the Italian Society of Pediatric Endocrinology and Diabetology and the Italian Society of Pediatrics. Nutr Metab Cardiovasc Dis. 2023, 33, 1113–1134. [Google Scholar] [CrossRef] [PubMed]
- Horner, D.; et al. Screen Time Is Associated With Cardiometabolic and Cardiovascular Disease Risk in Childhood and Adolescence. J Am Heart Assoc. 2025, 14, e041486. [Google Scholar] [CrossRef] [PubMed]
- Yasin, S.; Hasnain, M.; Khan, F.R.; et al. Association Between Obesity, Digital Screen Time, and Early-Onset Hypertension in Adolescents: A Prospective Cohort Study. Cureus 2025, 17, e79975. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Prevention of overweight and obesity in children. Health Promotion Knowledge Gateway. 2025 Mar 24. Available online: https://knowledge4policy.ec.europa.eu/health-promotion-knowledge-gateway/prevention-overweight (accessed on 12 December 2025).
- Lodi, E.; Gasparini, P.A.; Brusini, A.; Poli, M.L.; Savino, G.; Modena, M.G. Unraveling the Impact of COVID-19 Lockdowns on Youth Sports and Physical Activity: Insights From a Retrospective Cohort Study in Italy. Int J Pediatr. 2025, 2025, 1339516. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Manojlovic, M.; et al. Effects of school-based physical activity interventions on physical fitness and cardiometabolic health in children and adolescents with disabilities: a systematic review. Front Physiol. 2023, 14, 1180639. [Google Scholar] [CrossRef] [PubMed]
- Marsigliante, S.; et al. Effects on Children’s Physical and Mental Well-Being of a Physical-Activity-Based School Intervention Program: A Randomized Study. Int J Environ Res Public Health 2023, 20, 1927. [Google Scholar] [CrossRef] [PubMed]
- Santos-Beneit, G.; et al. School-Based Cardiovascular Health Promotion in Adolescents: A Cluster Randomized Clinical Trial. JAMA Cardiol. 2023, 8, 816–824. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Prevention of overweight and obesity in children. Health Promotion Knowledge Gateway. 2025 Mar 24. Available online: https://knowledge4policy.ec.europa.eu/health-promotion-knowledge-gateway/prevention-overweight (accessed on 12 December 2025).

Table 1.
Baseline demographic and anthropometric characteristics of the study cohort.
| Variable | Value |
|---|---|
| Participants, n | 810 |
| Age, years (mean ± SD) | 13.6 ± 2.1 |
| Sex, n (%) | Female 389 (48.0); Male 417 (51.5); Missing 4 (0.5)* |
| BMI, kg/m2 (mean ± SD) | 20.3 ± 3.4 |
| Weight status (WHO BMI-for-age), % | Normal weight 64; Overweight 22; Obesity 14 |
| WHtR > 0.5, % | 28 |
| Blood pressure available, n | 769 |
| Elevated blood pressure†, % | 12 |
* Four participants had missing sex data in sex-stratified analyses, as reported. †Classified according to 2017 American Academy of Pediatrics age-, sex-, and height-specific percentiles.
Table 2.
Key associations reported in univariable analyses.
| Association (Exposure → Outcome) | Direction (as Reported) | Test/Metric Reported | p-Value |
|---|---|---|---|
| Overweight/obesity → Elevated BP | Higher prevalence with excess adiposity | χ2 = 7.21; Cramér’s V = 0.27 | <0.01 |
| Overweight/obesity → WHtR >0.5 | More frequent in overweight/obese | Chi-square | <0.001 |
| Overweight/obesity → Cardiovascular knowledge score | Lower score vs. normal weight | Group comparison (adjusted analysis reported separately) | <0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



