
Submitted:
22 December 2025
Posted:
23 December 2025
You are already at the latest version
Abstract
Myocarditis remains a significant global health burden often accompanied by im-mune-mediated myocardial injury, oxidative stress, and unpredictable clinical progres-sion. Experimental autoimmune myocarditis (EAM) models have provided different in-sights into the interconnected roles of T-cell subsets, proinflammatory cytokines, mac-rophage polarization, and mitochondrial dysfunction in both acute inflammation and chronic cardiac remodeling. Hyperbaric oxygen therapy (HBOT), which delivers 100% oxygen at elevated atmospheric pressures, has emerged as a potential multimodal in-tervention capable of affecting several of these pathogenic pathways. Preclinical data demonstrate that HBOT enhances oxygen delivery to the inflamed myocardium, sup-presses the activation of NF-κB and NLRP3 inflammasomes, reduces oxidative stress, preserves mitochondrial function, and promotes immunoregulatory T-cell responses. Despite these promising results, significant translational challenges remain, including protocol variability, lack of long-term outcome data, incomplete mechanistic profiling, and uncertainties regarding optimal timing and patient selection. Future research should try to incorporate already standardized HBOT regimens, multi-omics analyses, advanced imaging, and well-designed early-phase clinical trials to evaluate safety and efficacy in human myocarditis. Overall, the currently available evidence supports HBOT as a bi-ologically plausible and potentially valuable adjunct therapy for autoimmune myocar-ditis, expressing the need for further mechanistic and clinical investigation.
Keywords:
experimental autoimmune myocarditis
; hyperbaric oxygen therapy
; immune modulation
; oxidative stress
; animal studies
; cardiac inflammation
1. Introduction
Myocarditis, whether driven by an infectious trigger or an immune-mediated process, remains a substantial global health challenge. Although diagnostic tools have advanced, many cases still go unrecognized, partly because early inflammatory changes in the myocardium can be clinically silent [1]. When the disease becomes clinically evident, the consequences are often severe. According to the 2021 Global Burden of Disease analysis, approximately 1.32 million individuals developed myocarditis worldwide, corresponding to an age-standardized incidence of about 16 cases per 100,000. High-income regions of the Asia Pacific and North America reported the largest number of new cases, while Central Asia showed a marked upward trend, suggesting underlying regional or environmental factors that warrant closer study [1,2]. The disease’s impact is particularly evident in competitive sports: myocarditis accounts for an estimated 5% to 20% of sudden cardiac deaths in young athletes [2].
Even with improved cardiac Magnetic Resonance Imaging (MRI) protocols and more accessible endomyocardial biopsy, fulminant myocarditis continues to carry a high mortality rate. Roughly one fifth of affected patients either die or require transplantation within a year of diagnosis [3]. The clinical course is unpredictable. Viral infections are still the most common cause of myocarditis, but autoimmune diseases, drug reactions, and unknown (idiopathic) causes also play a big role. Many patients go through an early phase that often goes unnoticed, during which inflammation and changes in the heart’s structure, such as mitochondrial dysfunction and extracellular matrix remodeling, are already happening [4]. This gap between what’s happening in the heart and what doctors can detect shows why we need experimental models that can pinpoint cause-and-effect pathways and test treatments in a controlled way [4]. The experimental autoimmune myocarditis (EAM) model has become one of the best tools for studying how the immune system can damage the heart. In EAM, susceptible rodents are usually immunized with heart muscle proteins or specific peptides mixed with an adjuvant [5]. This model reproduces many key features of human myocarditis, including dense immune cell infiltration (especially Cluster of Differentiation (CD4+) T cells and macrophages), heart muscle cell death, and later collagen deposition. These changes happen in a predictable timeline, letting researchers watch the disease progress from acute inflammation to chronic dilated cardiomyopathy [3,4,5]. Because of this clear timeline, the model has been very useful for studying cytokines, antigen presentation, and the interactions between the innate and adaptive immune systems in cardiac tissue [4]. However, the EAM model has important constraints. The requirement for strong adjuvants, such as complete Freund’s adjuvant, can introduce an exaggerated innate immune response not representative of human disease [5]. Genetic restrictions tied to Major Histocompatibility Complex (MHC) haplotypes mean that certain findings do not readily generalize across strains or species. Most notably, the model excludes viral replication, a key initiating factor in many patient populations. These limitations do not diminish EAM’s value but do highlight the need to interpret its results within a translational framework that accounts for what the model can, and cannot, reproduce [3,4,5].
Hyperbaric oxygen therapy (HBOT) offers a mechanistically distinct intervention worth examining in the context of myocarditis. During HBOT, individuals inhale pure oxygen at pressures two to three times greater than atmospheric levels [6]. This short exposure drives arterial oxygen tension to extremely high values, reaching roughly 1,400 mmHg at 2.0 atmospheres absolute and exceeding 2,200 mmHg at 3.0 atmospheres [7]. Under these conditions, oxygen dissolves directly into plasma at concentrations that can temporarily sustain tissue metabolism independently of hemoglobin-bound oxygen [6,7]. The physiological effects extend beyond oxygen delivery. HBOT has been shown to affect several important pathways in the body. It can reduce the nuclear factor kappa-light-chain-enhancer of activated B cells (NF-kB) activity, boost antioxidant enzymes like superoxide dismutase and catalase, lower pro-inflammatory molecules such as interleukin-1β (IL-1β) and tumor necrosis factor-α (TNF-α), and help mobilize CD34+ progenitor cells that are involved in tissue repair [8]. These effects are relevant to myocarditis, where oxidative stress, harmful immune signaling, and poor healing all contribute to heart damage [8].
This review has four main goals. First, we wanted to examine the current understanding of immune-mediated cardiac injury, with a particular focus on the contributions of oxidative stress and mitochondrial dysfunction. Second, to summarize findings from preclinical studies on HBOT in EAM, including how it affects heart function, tissue changes, and molecular pathways. Third, to consider how realistic it might be to use HBOT safely and effectively alongside current treatments for myocarditis in human populations. Finally, to highlight key areas for future research, like using advanced molecular profiling, imaging biomarkers, and early clinical trials. By combining insights from immunology, hyperbaric medicine, and heart research, this review aims to provide a clear, evidence-based foundation for exploring HBOT as a treatment for autoimmune and inflammatory heart diseases.
2. The Pathophysiology of Autoimmune Myocarditis
Autoimmune myocarditis happens when the immune system gets stuck in a cycle of activation, releasing inflammatory signals and damaging the mitochondria in heart cells. Over time, this leads to scarring and changes in the heart’s structure. Different triggers like viral infections, cancer immunotherapy, or problems with immune regulation can start this process, but the disease usually follows a predictable pattern [9]. It often begins when hidden heart proteins, like α-myosin peptides, are exposed and mistakenly seen as threats by the immune system. Dendritic cells present these proteins to naive T cells, which then move to the heart and create inflammation [10]. At the same time, cytotoxic T cells recognize the same proteins on heart muscle cells and release substances that cause cell death. This cell death releases danger signals, which further stimulate the immune system and worsen the inflammation [11]. A key step in this process involves Th17 cells, which depend on the presence of the inflammatory molecule interleukin-6 (IL-6) to develop. Blocking IL-6 or removing it genetically in mice prevents myocarditis from developing, while restoring IL-6 brings the disease back. Th17 cells enter the heart and release interleukin-17A (IL-17A), which attracts neutrophils and triggers complement activation, two events that lead to long-term damage and weakening of the heart [11]. Other types of T cells release inflammatory molecules like interferon-γ (IFN-γ) and TNF-α, which further compromise cardiac function [12]. Macrophages are another major type of immune cell involved. In the early stages, inflammatory macrophages dominate and release nitric oxide, inflammasome components, and other damaging molecules [12]. If these cells are pushed too far into this state, heart damage gets worse. As healing begins, macrophages shift to a more reparative form that promotes scar formation [13]. However, too much activity in this phase can lead to excessive scarring and stiffness of the heart [12,13].
The activity of different cytokines in autoimmune myocarditis follows a pretty clear timeline. IL-1β and IL-6 appear early and help activate Th17 cells and recruit neutrophils. Animal studies show that blocking IL-1 reduces inflammation and helps the heart work better [14]. Approximately two to three weeks later, TNF-α and IFN-γ levels rise, keeping immune cells active and causing more damage. If this stage isn’t controlled, the heart starts remodeling in ways that can lead to chronic problems. Eventually, anti-inflammatory signals like interleukin-10 (IL-10) and transforming growth factor-β (TGF-β) increase, promoting regulatory T cells and helping form scar tissue. While this helps end the acute inflammation, it may also result in long-term cardiac dysfunction [14].
A lot of the damage in autoimmune myocarditis happens in the mitochondria, the cell’s energy factories. Enzymes like nicotinamide adenine dinucleotide phosphate (NADPH) oxidase and disrupted energy production in mitochondria lead to a surge in reactive oxygen species (ROS) [15]. These molecules damage cell membranes, drain energy, and cause mitochondria to break down further. Results from a recent study show that blocking both this oxidative damage and a key mitochondrial stress pathway can protect the heart [16]. Damaged mitochondria also send out signals that further activate immune cells, especially macrophages. In animal studies, higher mitochondrial oxidative stress is associated with impaired heart function, while antioxidants like melatonin and myricetin can reduce damage and promote cardiac recovery [15,16].
Overall, autoimmune myocarditis is a complex process driven by specific immune cells, inflammatory cytokines, and mitochondrial damage. Each of these elements reinforces the others, creating a loop of ongoing injury. Intervening at any point—either by blocking harmful cytokines, boosting regulatory T cells, shifting macrophages to a healing state, or protecting mitochondria—has been shown to reduce the effects of this disease in animal studies [17]. This is why therapies that work on multiple parts of the disease process, such as HBOT, look promising. HBOT has been shown to reduce key inflammatory pathways, restore immune balance, and strengthen antioxidant defenses, making it an attractive candidate for further research of this condition [18,19].
3. Mechanisms of Hyperbaric Oxygenation in Inflammation and Tissue Repair
As mentioned before, HBOT boosts the oxygen level in the blood to around 2000 mmHg at typical treatment pressures. This extra oxygen can reach inflamed or poorly supplied areas of the heart, helping heart cells get the energy they need and turning on protective responses like antioxidant enzyme production and calming overactive immune reactions [20]. This high oxygen level allows oxygen to reach areas of the heart that are inflamed, swollen, or poorly supplied with blood, which is often present in myocarditis [8]. In this way, HBOT helps overcome local oxygen shortages and protects heart tissue from damage [21]. Interestingly, while it seems paradoxical, brief exposure to high oxygen also triggers the body’s internal defense systems. It activates protective antioxidant enzymes through a process known as redox signaling while at the same time reducing the activity of enzymes that produce harmful ROS, which helps lower overall oxidative stress [22,23].
HBOT also affects important inflammatory pathways. It prevents the activation of NF-κB, a key molecule that drives the production of pro-inflammatory substances like TNF-α, IL-1β, IL-6, and Intercellular Adhesion Molecule-1 (ICAM-1). In doing so, it helps reduce inflammation in the heart and other tissues. HBOT has also been shown to limit activation of the NOD-, LRR- and pyrin domain-containing protein 3 (NLRP3) inflammasome, a key promoter of inflammation in heart injury [24]. Looking beyond just reducing inflammation, HBOT supports tissue repair and also helps stabilize hypoxia-inducible factor 1α (HIF-1α), a protein that encourages new blood vessels to grow. This supports the recruitment of stem cells that repair damaged blood vessels and promote healing in the heart [25]. On top of that, HBOT protects mitochondria by keeping important enzymes working, preventing energy loss, and stopping cell death pathways from turning on. Because mitochondrial damage is a major driver of both heart cell death and immune system activation in myocarditis, this protective effect is especially important [26]. Finally, HBOT helps in rebalancing the immune system [27]. It lowers the number of harmful Th17 immune cells and increases the presence of regulatory T cells, which helps in keeping inflammation in check. This shift has been observed in several models of autoimmune disease [28]. Taken together, the effects of HBOT—such as improved oxygen delivery, reduced oxidative stress, dampened inflammation, better blood vessel repair, mitochondrial protection, and immune system rebalancing—provide a strong and biologically sound reason to explore it as a potential therapy for autoimmune myocarditis. Because many of these mechanisms depend on the magnitude of oxygen tension achieved during treatment, the approximate arterial oxygen levels produced at different hyperbaric pressures are summarized in Table 1.
4. Hyperbaric Oxygen Therapy in Experimental Autoimmune Myocarditis: Preclinical Evidence
Many EAM models, such as the Galectin-3 (Gal-3)–deficient C57BL/6J mice immunized with MyHCα334₋352 peptide as employed by Milinčić et al., provide a genetically susceptible platform to study myocarditis characterized by severe mononuclear cell infiltration, necrosis, and pronounced fibrosis due to Gal-3 deficiency [32]. While direct EAM + HBOT evidence in non–Gal-3 deficient mouse lines is limited, more traditional EAM induction protocols in Lewis or Balb/c rats immunized with cardiac myosin peptides are commonly used to investigate cytokine signaling and fibrotic processes [33]. HBOT regimens in these models typically involve administration of 100% oxygen at 2.5 ATA for approximately 90 minutes per session, delivered daily from days 7 to 21 post-immunization during the therapeutic phase, aligning with standard cardiac HBOT protocols in rodent studies [32]. Functional outcomes reported by Milinčić et al. include significantly improved fractional shortening, reduced left ventricular internal diameters at diastole and systole, decreased myocardial fibrosis, necrosis, and inflammatory infiltration upon histological examination, alongside improved survival or delayed heart failure progression [32]. Histologically, HBOT-treated hearts show decreased mononuclear infiltration and lower myocarditis scores, preservation of cardiomyocytes with reduced degeneration and necrosis, and significant attenuation of fibrosis compared to untreated EAM animals [32,34]. Although direct cytokine quantification post-HBOT in EAM models remains limited, data from EAM rats treated with anti-inflammatory agents demonstrate downregulation of key cytokines IL-1β, IL-6, and TNF-α via NF-κB pathway inhibition, mechanisms likely shared by HBOT therapy [34]. In addition, studies in experimental autoimmune encephalomyelitis (EAE) show that HBOT can reduce pro-inflammatory Th17 cells and increase regulatory T cells (Tregs), suggesting that it might have similar immune-balancing effects in myocarditis [28]. These combined immunomodulatory and tissue-protective actions of HBOT are summarized in Figure 1.
While these results are encouraging, there are still important limitations. Most studies use very specific mouse strains, like Gal-3 deficient mice, and have small group sizes (fewer than 15 animals), which makes it hard to know if the findings are reliable or repeatable [35]. Many experiments also end at day 21 after immunization, so we don’t yet know how HBOT affects long-term heart changes, arrhythmias, or chronic forms of the disease [36]. Furthermore, no systematic studies have been conducted to determine the optimal HBOT pressure, session length, or total treatment time. This lack of data complicates the comparison of results across studies [37]. A summary table (Table 2) consolidates key parameters such as animal models, HBOT protocols, and main findings from other existing studies, illustrating consistent improvements in cardiac function and inflammation.
5. Translational Relevance and Clinical Perspectives
The promising results from animal studies suggest that HBOT could be beneficial for human myocarditis, which remains challenging to treat due to its heterogeneity and limited treatment options. In humans, myocarditis is often caused by viral infections or autoimmune disorders, and it shares important features with EAM models, including T-cell driven inflammation, dysregulated cytokine signaling, and oxidative stress–induced cardiac damage [41,42]. HBOT’s ability to modulate immune responses, reduce oxidative damage, and promote tissue repair through angiogenesis and mitochondrial protection presents a compelling rationale for translational exploration [43].
However, significant barriers complicate the direct translation of animal findings to human clinical use. Timing of intervention is critical; whereas HBOT treatment in animal models typically commences during the acute inflammatory phase, human patients often present with variable disease stages, complicating optimal therapy windows [44]. Furthermore, access to HBOT chambers and practical issues also make it hard to use widely, especially in urgent heart care [45]. Patient selection criteria remain undefined, as myocarditis encompasses a spectrum from self-limited to fulminant disease forms, which may differentially respond to HBOT [9]. While EAM models mimic autoimmune myocarditis, they don’t fully replicate viral forms or the long-term heart changes seen in humans [9]. Future clinical studies should carefully select eligible patients to evaluate the safety and effectiveness of HBOT, and use biomarkers like blood cytokines, T-cell counts, or imaging to monitor therapeutic outcomes [44]. Large, multi-center randomized trials would be needed to really test HBOT as an adjunct or alternative to current immunosuppressive or antiviral therapies, ideally including studies that closely examine cardiac tissue to unravel the underlying mechanisms [46].
6. Risks, Side Effects, and Patient Selection for Hyperbaric Oxygen Therapy
While HBOT is generally safe, like any medical treatment, it carries certain risks and potential side effects. The most common issue is barotrauma, which mainly affects the middle ear. Changes in pressure during treatment can make the ears uncomfortable or even damage the eardrum if not managed carefully. Patients may also experience claustrophobia due to being in tight spaces while confined in the chamber, which can sometimes require sedation or careful psychological support [45]. Less commonly, breathing high-pressure oxygen can cause oxygen toxicity, which could lead to seizures or lung irritation. These serious problems are rare but require close monitoring during sessions. Other possible side effects include temporary changes in vision and fatigue [45].
To keep patients safe, screening is important before starting HBOT. Absolute contraindications include untreated pneumothorax, as the pressure changes can worsen this condition. Relative contraindications include certain lung diseases, uncontrolled seizures, or severe congestive heart failure. Medical history, physical examination, and sometimes imaging are used to assess eligibility [47]. Although HBOT is not yet a standard treatment for myocarditis, if it were to be considered as a therapeutic option in the future, patients would need to be closely monitored for possible adverse effects. Since the incidence of complications can increase with the use of higher pressures (>2.0 ATA) or prolonged treatment courses (>10 sessions), therapy parameters would need careful adjustment to meet patient needs [48].
7. Current Clinical Indications and Outcomes of Hyperbaric Oxygen Therapy
It has already been established that HBOT is a well-known treatment used for many medical conditions. It is especially effective for treating decompression sickness, which can occur in divers who surface too quickly, and for carbon monoxide poisoning, where it helps promptly remove the toxic gas from the blood [49]. In addition, HBOT also has applications in managing diabetic foot ulcers, chronic refractory osteomyelitis, and radiation-induced tissue damage [50]. Studies show that people with diabetic foot ulcers heal faster and have fewer amputations when treated with HBOT [51]. In chronic bone infections, HBOT supports antibiotic therapy and helps resolve infection by improving blood flow and oxygenation in damaged tissues. Radiation injuries, which often cause persistent tissue damage and poor healing, also respond well to HBOT, reducing pain and tissue necrosis [52]. Overall, large patient cohorts treated with HBOT for radiation-induced injuries have shown high rates of symptom improvement or resolution, ranging from approximately 77% to 93% depending on the type of injury. These outcomes are documented in numerous clinical trials and are supported by international guidelines in hyperbaric medicine [53]. The widespread and well-documented efficacy of HBOT in these diverse conditions provides a strong foundation for exploring its use in other diseases, such as autoimmune myocarditis. HBOT has also been studied in other cardiovascular diseases beyond myocarditis, both in animal models and clinical settings. In animal studies of cardiac arrest, it improved the chances of restoring spontaneous circulation and reduced brain damage after resuscitation [50]. This suggests that HBOT may protect heart and brain tissues by improving oxygen delivery during critical injury.
In models of ischemic heart disease, HBOT has been shown to reduce inflammation and limit tissue damage by enhancing oxygen supply to areas affected by reduced blood flow [21]. It also appears to promote the formation of new blood vessels and stimulate repair mechanisms [54]. Some early clinical studies suggested potential benefits in conditions such as refractory angina and chronic heart failure, though larger trials are needed to confirm these findings [55]. Additionally, HBOT has been found to mitigate vascular dysfunction in animal models of systemic inflammatory conditions, which may translate to benefits in cardiovascular diseases linked to inflammation and oxidative stress [56]. Together, these studies point to a growing interest in applying HBOT to a broader range of cardiovascular disorders, with promising preclinical and initial clinical data supporting its role as an adjunct therapy.
8. Hyperbaric Oxygen Therapy and Myocarditis Mechanisms
HBOT has a unique ability to influence various immune and cellular processes that drive myocarditis. The disease typically involves an overactive immune response that damages heart tissue, primarily through inflammation and oxidative stress. HBOT helps calm this immune overreaction by inhibiting a key molecular pathway called NF-κB, which controls the production of many inflammatory molecules, such as TNF-α and IL-6. By reducing these molecules, HBOT lowers inflammation in the heart [57]. At the same time, HBOT promotes the growth and activity of regulatory T cells, which play a crucial role in maintaining the immune system’s balance. These cells help prevent excessive inflammation and tissue damage by counteracting the inflammatory effects of T helper 17 cells. This restoration of balance between different types of immune cells is crucial in controlling myocarditis and preventing its progression [58].
On a cellular level, HBOT also protects mitochondria, the energy centers of heart cells. In myocarditis, mitochondria suffer from oxidative damage, which triggers cell death and worsens heart function. HBOT helps by preserving mitochondrial function, preventing the opening of pores that would otherwise lead to cell death, and reducing the production of harmful ROS. Together, these effects of HBOT directly target the pathways that cause damage in myocarditis, making it a promising therapeutic approach [55]. Several studies in animal models support these findings, showing that HBOT treatment decreases inflammation, reduces oxidative stress, and improves heart function. These results suggest that the mechanisms of HBOT are well-aligned with the complex immunopathology of myocarditis [32,59,60,61].
9. Future Directions
Despite encouraging preclinical findings regarding HBOT in EAM, substantial gaps in knowledge remain that must be addressed to realize its translational potential. Foremost, the current body of evidence suffers from limited sample sizes and a lack of reproducibility across diverse animal models, particularly beyond Galectin-3 deficient mice, raising concerns about generalizability [32]. The absence of standardized HBOT treatment protocols further complicates interpretation since variations in pressure, duration, frequency, and timing across studies obscure the identification of optimal therapeutic regimens, pointing to the urgency for dose-response investigations [45]. Moreover, mechanistic insights into HBOT’s immunomodulatory effects remain incomplete. Multi-omics approaches including transcriptomics, proteomics, and metabolomics could elucidate myocardial tissue alterations and identify biomarkers predictive of response [62]. Combining HBOT with established immunosuppressive therapies represents a promising strategy, potentially yielding additive or synergistic benefits by concurrently targeting immune dysregulation and oxidative stress [28]. Advanced imaging modalities such as cardiac magnetic resonance imaging (MRI) and positron emission tomography (PET) offer powerful noninvasive tools to monitor inflammation, fibrosis, and myocardial remodeling longitudinally, and their integration into HBOT studies could enhance the evaluation of therapeutic efficacy [63]. Additionally, investigating long-term outcomes including cardiac remodeling, arrhythmogenesis, and heart failure progression is crucial, as most current studies focus on acute-phase end-points. Such a comprehensive assessment will help.
10. Conclusions
In summary, HBOT holds promise as a multi-target therapy capable of modulating key immunological and oxidative pathways implicated in myocarditis pathogenesis, but its translation to clinical practice requires overcoming practical and biological obstacles through well-designed human studies. Preclinical evidence in EAM models demonstrates that HBOT improves cardiac function, diminishes inflammation, and limits fibrosis by targeting key inflammatory pathways and restoring immune balance. Despite these encouraging findings, translation into clinical practice remains preliminary, with significant challenges including variability in treatment protocols, limited functional and causal understanding, and the need for robust clinical trials. Future research should focus on standardizing HBOT regimens, exploring combination therapies with established immunosuppressants, and employing advanced imaging and molecular approaches to monitor treatment effects and identify biomarkers. Ultimately, well-designed clinical studies are essential to validate HBOT’s efficacy and safety in human myocarditis, potentially offering a novel therapeutic avenue for this complex and often disabling condition.
Author Contributions
Conceptualization, B.P., A.S., I.S., and V.J.; methodology, B.P., V.Z., R.P., A.S., and I.S.; software, D.K., Z.F.; validation, B.P., V.Z., D.P., A.S., and I.S.; formal analysis, B.P., R.P., and I.S.; investigation, B.P., R.P., M.M., I.S., and A.S.; resources, K.M. and S.B.B.; data curation, B.P., Z.F., A.S., and I.S.; writing—original draft preparation, B.P., R.P., and AS.; writing—review and editing, V.Z., V.J., R.P., A.S., and I.S.; visualization, B.P., A.S., M.M., and I.S.; supervision, V.Z., V.J., and S.B.B.; project administration, V.J.; funding acquisition, V.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest. The study received no external funding.
Abbreviations
The following abbreviations are used in this manuscript:
| ATA CD4+ EAM EAE EPC Gal-3 HIF-1α HBOT IFN-γ ICAM-1 IL-1β IL-6 IL-10 IL-17A MHC MI MyHCα334₋352 MRI NADPH NLRP3 NF-κB PaO2 PET ROS TGF-β Th17 TNF-α Tregs |
Atmospheres Absolute Cluster of Differentiation 4 positive T cells Experimental Autoimmune Myocarditis Experimental Autoimmune Encephalomyelitis Endothelial Progenitor Cells Galectin-3 Hypoxia-inducible factor 1-alpha Hyperbaric Oxygen Therapy Interferon-gamma Intercellular Adhesion Molecule-1 Interleukin-1 beta Interleukin-6 Interleukin-10 Interleukin-17A Major Histocompatibility Complex Myocardial Infarction α-myosin heavy chain peptide (residues 334–352) Magnetic Resonance Imaging Nicotinamide Adenine Dinucleotide Phosphate (oxidase) NOD-, LRR- and pyrin domain-containing protein 3 Nuclear Factor kappa-light-chain-enhancer of activated B cells Arterial Oxygen Tension Positron Emission Tomography Reactive Oxygen Species Transforming Growth Factor-beta T helper 17 cells Tumor Necrosis Factor-alpha Regulatory T cells |
References
- Ren, J.; Liu, W.; Jin, X.; Zhang, C.; Xu, X.; Deng, G.; et al. Global, regional, and national burden of myocarditis and its attributable risk factors in 204 countries and territories from 1990 to 2021: Updated systematic analysis. Front. Public Health 2025, 13, 1542921. [CrossRef]
- Cooper, L.T. Myocarditis. N. Engl. J. Med. 2009, 360, 1526–1538. [CrossRef]
- Chabior, A.; Tymińska, A.; Pawlak, A.; Giordani, A.; Caforio, A.L.P.; Grabowski, M.; et al. Advances in myocarditis management in the light of the latest research and recent guidelines of the European Society of Cardiology. Cardiol. J. 2024, 31, 342–351. [CrossRef]
- Daniels, M.D.; Hyland, K.V.; Wang, K.; Engman, D.M. Recombinant cardiac myosin fragment induces experimental autoimmune myocarditis via activation of Th1 and Th17 immunity. Autoimmunity 2008, 41, 490–499. [CrossRef]
- Draginic, N.D.; Jakovljevic, V.L.; Jeremic, J.N.; Srejovic, I.M.; Andjic, M.M.; Rankovic, M.R.; et al. Melissa officinalis L. supplementation provides cardioprotection in a rat model of experimental autoimmune myocarditis. Oxid. Med. Cell. Longev. 2022, 2022, 1344946. [CrossRef]
- Chung, E.; Zelinski, L.M.; Ohgami, Y.; Shirachi, D.Y.; Quock, R.M. Hyperbaric oxygen treatment induces a 2-phase antinociceptive response of unusually long duration in mice. J. Pain 2010, 11, 847–853. [CrossRef]
- Jones, M.W.; Brett, K.; Han, N.; Cooper, J.S.; Wyatt, H.A. Hyperbaric physics. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, [cited 2025 Dec 3]. Available online: https://www.ncbi.nlm.nih.gov/books/NBK448104/.
- Thom, S.R. Hyperbaric oxygen: Its mechanisms and efficacy. Plast. Reconstr. Surg. 2011, 127, 131S–141S. [CrossRef]
- Caforio, A.L.P.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648. [CrossRef]
- Kaya, Z.; Katus, H.A.; Rose, N.R. Cardiac troponins and autoimmunity: Their role in the pathogenesis of myocarditis and of heart failure. Clin. Immunol. 2010, 134, 80–88. [CrossRef]
- Yamashita, T.; Iwakura, T.; Matsui, K.; Kawaguchi, H.; Obana, M.; Hayama, A.; et al. IL-6–mediated Th17 differentiation through RORγt is essential for the initiation of experimental autoimmune myocarditis. Cardiovasc. Res. 2011, 91, 640–648. [CrossRef]
- Eriksson, U.; Kurrer, M.O.; Schmitz, N.; Marsch, S.C.; Fontana, A.; Eugster, H.P.; et al. Interleukin-6–deficient mice resist development of autoimmune myocarditis associated with impaired upregulation of complement C3. Circulation 2003, 107, 320–325. [CrossRef]
- Tkacz, K.; Rolski, F.; Stefańska, M.; Węglarczyk, K.; Szatanek, R.; Siedlar, M.; et al. TGF-β signalling regulates cytokine production in inflammatory cardiac macrophages during experimental autoimmune myocarditis. Int. J. Mol. Sci. 2024, 25, 5579. [CrossRef]
- Liu, H.; Hanawa, H.; Yoshida, T.; Elnaggar, R.; Hayashi, M.; Watanabe, R.; et al. Effect of hydrodynamics-based gene delivery of plasmid DNA encoding interleukin-1 receptor antagonist-Ig for treatment of rat autoimmune myocarditis: Possible mechanism for lymphocytes and noncardiac cells. Circulation 2005, 111, 1593–1600. [CrossRef]
- Mendoza, A.; Patel, P.; Robichaux, D.; Ramirez, D.; Karch, J. Inhibition of the mPTP and lipid peroxidation is additively protective against I/R injury. Circ. Res. 2024, 134, 1292–1305. [CrossRef]
- Di Florio, D.N.; Beetler, D.J.; McCabe, E.J.; Sin, J.; Ikezu, T.; Fairweather, D. Mitochondrial extracellular vesicles, autoimmunity and myocarditis. Front. Immunol. 2024, 15, 1374796. [CrossRef]
- Barin, J.G.; Čiháková, D. Control of inflammatory heart disease by CD4+ T cells. Ann. N. Y. Acad. Sci. 2013, 1285, 80–96. [CrossRef]
- Capó, X.; Monserrat-Mesquida, M.; Quetglas-Llabrés, M.; Batle, J.M.; Tur, J.A.; Pons, A.; et al. Hyperbaric oxygen therapy reduces oxidative stress and inflammation, and increases growth factors favouring the healing process of diabetic wounds. Int. J. Mol. Sci. 2023, 24, 7040. [CrossRef]
- Chen, L.; Wang, Y.; Zhou, H.; Liang, Y.; Zhu, F.; Zhou, G. The new insights of hyperbaric oxygen therapy: Focus on inflammatory bowel disease. Precis. Clin. Med. 2024, 7, pbae001. [CrossRef]
- Thom, S.R. Oxidative stress is fundamental to hyperbaric oxygen therapy. J. Appl. Physiol. 2009, 106, 988–995. [CrossRef]
- Oliveira, M.; Tanaka, L.; Antonio, E.; Brandizzi, L.; Serra, A.; Dos Santos, L.; et al. Hyperbaric oxygenation improves redox control and reduces mortality in the acute phase of myocardial infarction in a rat model. Mol. Med. Rep. [Internet] 2020, [cited 2025 Dec 3]. Available online: http://www.spandidos-publications.com/10.3892/mmr.2020.10968.
- Schottlender, N.; Gottfried, I.; Ashery, U. Hyperbaric oxygen treatment: Effects on mitochondrial function and oxidative stress. Biomolecules 2021, 11, 1827. [CrossRef]
- Vinkel, J.; Rib, L.; Buil, A.; Hedetoft, M.; Hyldegaard, O. Key pathways and genes that are altered during treatment with hyperbaric oxygen in patients with sepsis due to necrotizing soft tissue infection (HBOmic study). Eur. J. Med. Res. 2023, 28, 507. [CrossRef]
- Qian, H.; Li, Q.; Shi, W. Hyperbaric oxygen alleviates the activation of NLRP-3 inflammasomes in traumatic brain injury. Mol. Med. Rep. 2017, 16, 3922–3928. [CrossRef]
- Fu, Q.; Duan, R.; Sun, Y.; Li, Q. Hyperbaric oxygen therapy for healthy aging: From mechanisms to therapeutics. Redox Biol. 2022, 53, 102352. [CrossRef]
- Chen, W.; Lv, L.; Nong, Z.; Chen, X.; Pan, X.; Chen, C. Hyperbaric oxygen protects against myocardial ischemia-reperfusion injury through inhibiting mitochondria dysfunction and autophagy. Mol. Med. Rep. [Internet] 2020, [cited 2025 Dec 3]. Available online: http://www.spandidos-publications.com/10.3892/mmr.2020.11497.
- Moon, B.-I.; Kim, H.-R.; et al. Attenuation of collagen-induced arthritis by hyperbaric oxygen therapy through altering immune balance in favor of regulatory T cells. Undersea Hyperb. Med. 2017, 44, 321–330. [CrossRef]
- Chiou, H.-Y.C.; Huang, S.-H.; Hung, C.-H.; Tsai, S.-M.; Kuo, H.-R.; Huang, Y.-R.; et al. Hyperbaric oxygen therapy alleviates the autoimmune encephalomyelitis via the reduction of IL-17A and GM-CSF production of autoreactive T cells as well as boosting the immunosuppressive IL-10 in the central nervous system tissue lesions. Biomedicines 2021, 9, 943. [CrossRef]
- Bennett, M.H.; Mitchell, S.J. Emerging indications for hyperbaric oxygen. Curr. Opin. Anaesthesiol. 2019, 32, 792–798. [CrossRef]
- Ortega, M.A.; Fraile-Martinez, O.; García-Montero, C.; Callejón-Peláez, E.; Sáez, M.A.; Álvarez-Mon, M.A.; et al. A general overview on the hyperbaric oxygen therapy: Applications, mechanisms and translational opportunities. Medicina 2021, 57, 864. [CrossRef]
- Mathieu, D., Ed. Handbook on Hyperbaric Medicine [Internet]; Springer: Dordrecht, The Netherlands, 2006 [cited 2025 Dec 3]. Available online: https://link.springer.com/10.1007/1-4020-4448-8.
- Milincic, K.; Miletic Kovacevic, M.; Dulovic, D.; Ljujic, B. Effect of hyperbaric oxygenation on the severity of experimental autoimmune myocarditis in Gal-3 deficient mice. Exp. Appl. Biomed. Res. 2025, ahead of print. [CrossRef]
- Jeuthe, S.; Schmerler, P.; Oh-Ici, D.; Wassilew, K.; Lauer, D.; Mueller, S.; et al. Clinical and histological presentations of experimental autoimmune myocarditis in rats using different immunization schemes. J. Cardiovasc. Magn. Reson. 2014, 16, P282. [CrossRef]
- Otsuka, K.; Terasaki, F.; Ikemoto, M.; Fujita, S.; Tsukada, B.; Katashima, T.; et al. Suppression of inflammation in rat autoimmune myocarditis by S100A8/A9 through modulation of the proinflammatory cytokine network. Eur. J. Heart Fail. 2009, 11, 229–237. [CrossRef]
- Baccouche, B.M.; Mahmoud, M.A.; Nief, C.; Patel, K.; Natterson-Horowitz, B. Galectin-3 is associated with heart failure incidence: A meta-analysis. Curr. Cardiol. Rev. 2023, 19, e171122211004. [CrossRef]
- Fontes, J.A.; Barin, J.G.; Talor, M.V.; Stickel, N.; Schaub, J.; Rose, N.R.; et al. Complete Freund’s adjuvant induces experimental autoimmune myocarditis by enhancing IL-6 production during initiation of the immune response: IL-6 in the initiation of EAM. Immun. Inflamm. Dis. 2017, 5, 163–176. [CrossRef]
- Oruc, M.; Esen, B.; Taylan, M.; et al. The role of duration of hyperbaric oxygen therapy on lung injury: An experimental study. Turk. Thorac. J. 2018, 19, 61–65. [CrossRef]
- Chen, C.; Chen, W.; Li, Y.; Dong, Y.; Teng, X.; Nong, Z.; et al. Hyperbaric oxygen protects against myocardial reperfusion injury via the inhibition of inflammation and the modulation of autophagy. Oncotarget 2017, 8, 111522–111534. [CrossRef]
- Goldstein, L.J.; Gallagher, K.A.; Bauer, S.M.; Bauer, R.J.; Baireddy, V.; Liu, Z.; et al. Endothelial progenitor cell release into circulation is triggered by hyperoxia-induced increases in bone marrow nitric oxide. Stem Cells 2006, 24, 2309–2318. [CrossRef]
- Yamashita, M.; Yamashita, M. Hyperbaric oxygen treatment attenuates cytokine induction after massive hemorrhage. Am. J. Physiol. Endocrinol. Metab. 2000, 278, E811–E816. [CrossRef]
- Leitman, M.; Fuchs, S.; Tyomkin, V.; Hadanny, A.; Zilberman-Itskovich, S.; Efrati, S. The effect of hyperbaric oxygen therapy on myocardial function in post-COVID-19 syndrome patients: A randomized controlled trial. Sci. Rep. 2023, 13, 9473. [CrossRef]
- Shandling, A.H.; Ellestad, M.H.; Hart, G.B.; Crumpa, R.; Marlow, D.; Van Natta, B.; et al. Hyperbaric oxygen and thrombolysis in myocardial infarction: The “HOT MI” pilot study. Am. Heart J. 1997, 134, 544–550. [CrossRef]
- Leroy, A.; Cuisset, T.; Quilici, J.; Paule, P.; Poyet, R.; Bali, L.; et al. An unusual “winter case” of myocarditis. Int. J. Cardiol. 2011, 148, e68–e69. [CrossRef]
- Kindermann, I.; Barth, C.; Mahfoud, F.; Ukena, C.; Lenski, M.; Yilmaz, A.; et al. Update on myocarditis. J. Am. Coll. Cardiol. 2012, 59, 779–792. [CrossRef]
- Heyboer, M.; Sharma, D.; Santiago, W.; McCulloch, N. Hyperbaric oxygen therapy: Side effects defined and quantified. Adv. Wound Care 2017, 6, 210–224. [CrossRef]
- Frustaci, A.; Chimenti, C.; Calabrese, F.; Pieroni, M.; Thiene, G.; Maseri, A. Immunosuppressive therapy for active lymphocytic myocarditis: Virological and immunologic profile of responders versus nonresponders. Circulation 2003, 107, 857–863. [CrossRef]
- Foster, J.H. Hyperbaric oxygen therapy: Contraindications and complications. J. Oral Maxillofac. Surg. 1992, 50, 1081–1086. [CrossRef]
- Zhang, Y.; Zhou, Y.; Jia, Y.; Wang, T.; Meng, D. Adverse effects of hyperbaric oxygen therapy: A systematic review and meta-analysis. Front. Med. 2023, 10, 1160774. [CrossRef]
- Mitchell, S.M.; Moon, R.E. Hyperbaric treatment for decompression sickness: Current recommendations. Undersea Hyperb. Med. 2019, 46, 685–693.
- Van Meter, K.; Sheps, S.; Kriedt, F.; Moises, J.; Barratt, D.; Murphy-Lavoie, H.; et al. Hyperbaric oxygen improves rate of return of spontaneous circulation after prolonged normothermic porcine cardiopulmonary arrest. Resuscitation 2008, 78, 200–214. [CrossRef]
- Zhang, Z.; Zhang, W.; Xu, Y.; Liu, D. Efficacy of hyperbaric oxygen therapy for diabetic foot ulcers: An updated systematic review and meta-analysis. Asian J. Surg. 2022, 45, 68–78. [CrossRef]
- Fang, R.; Galiano, R. Adjunctive therapies in the treatment of osteomyelitis. Semin. Plast. Surg. 2009, 23, 141–147. [CrossRef]
- Niezgoda, J.A.; Serena, T.E.; Carter, M.J. Outcomes of radiation injuries using hyperbaric oxygen therapy: An observational cohort study. Adv. Skin Wound Care 2016, 29, 12–19. [CrossRef]
- Han, C.; Lin, L.; Zhang, W.; Zhang, L.; Lv, S.; Sun, Q.; et al. Hyperbaric oxygen preconditioning alleviates myocardial ischemic injury in rats. Exp. Biol. Med. 2008, 233, 1448–1453. [CrossRef]
- Imperatore, F.; Cuzzocrea, S.; Luongo, C.; Liguori, G.; Scafuro, A.; De Angelis, A.; et al. Hyperbaric oxygen therapy prevents vascular derangement during zymosan-induced multiple-organ-failure syndrome. Intensive Care Med. 2004, 30, 1175–1181. [CrossRef]
- Wilson, H.D.; Wilson, J.R.; Fuchs, P.N. Hyperbaric oxygen treatment decreases inflammation and mechanical hypersensitivity in an animal model of inflammatory pain. Brain Res. 2006, 1098, 126–128. [CrossRef]
- Li, X.; Lu, L.; Min, Y.; Fu, X.; Guo, K.; Yang, W.; et al. Efficacy and safety of hyperbaric oxygen therapy in acute ischaemic stroke: A systematic review and meta-analysis. BMC Neurol. 2024, 24, 55. [CrossRef]
- Alex, J.; Laden, G.; Cale, A.R.J.; Bennett, S.; Flowers, K.; Madden, L.; et al. Pretreatment with hyperbaric oxygen and its effect on neuropsychometric dysfunction and systemic inflammatory response after cardiopulmonary bypass: A prospective randomized double-blind trial. J. Thorac. Cardiovasc. Surg. 2005, 130, 1623–1630. [CrossRef]
- Levitan, D.M.; Hitt, M.; Geiser, D.R.; Lyman, R. Rationale for hyperbaric oxygen therapy in traumatic injury and wound care in small animal veterinary practice. J. Small Anim. Pract. 2021, 62, 719–729. [CrossRef]
- Benkő, R.; Miklós, Z.; Ágoston, V.A.; Ihonvien, K.; Répás, C.; Csépányi-Kömi, R.; et al. Hyperbaric oxygen therapy dampens inflammatory cytokine production and does not worsen the cardiac function and oxidative state of diabetic rats. Antioxidants 2019, 8, 607. [CrossRef]
- Heidler, J.; Cabrera-Orefice, A.; Wittig, I.; Heyne, E.; Tomczak, J.N.; Petersen, B.; et al. Hyperbaric oxygen treatment reveals spatiotemporal OXPHOS plasticity in the porcine heart. PNAS Nexus 2024, 3, pgae210. [CrossRef]
- Dufour, C.R.; Xia, H.; B’chir, W.; Perry, M.C.; Kuzmanov, U.; Gainullina, A.; et al. Integrated multi-omics analysis of adverse cardiac remodeling and metabolic inflexibility upon ErbB2 and ERRα deficiency. Commun. Biol. 2022, 5, 955. [CrossRef]
- Polte, C.L.; Bobbio, E.; Bollano, E.; Bergh, N.; Polte, C.; Himmelman, J.; et al. Cardiovascular magnetic resonance in myocarditis. Diagnostics 2022, 12, 399. [CrossRef]
Figure 1.
Different pathways through which hyperbaric oxygen therapy modulates inflammation and myocardial injury in experimental autoimmune myocarditis.
Figure 1.
Different pathways through which hyperbaric oxygen therapy modulates inflammation and myocardial injury in experimental autoimmune myocarditis.
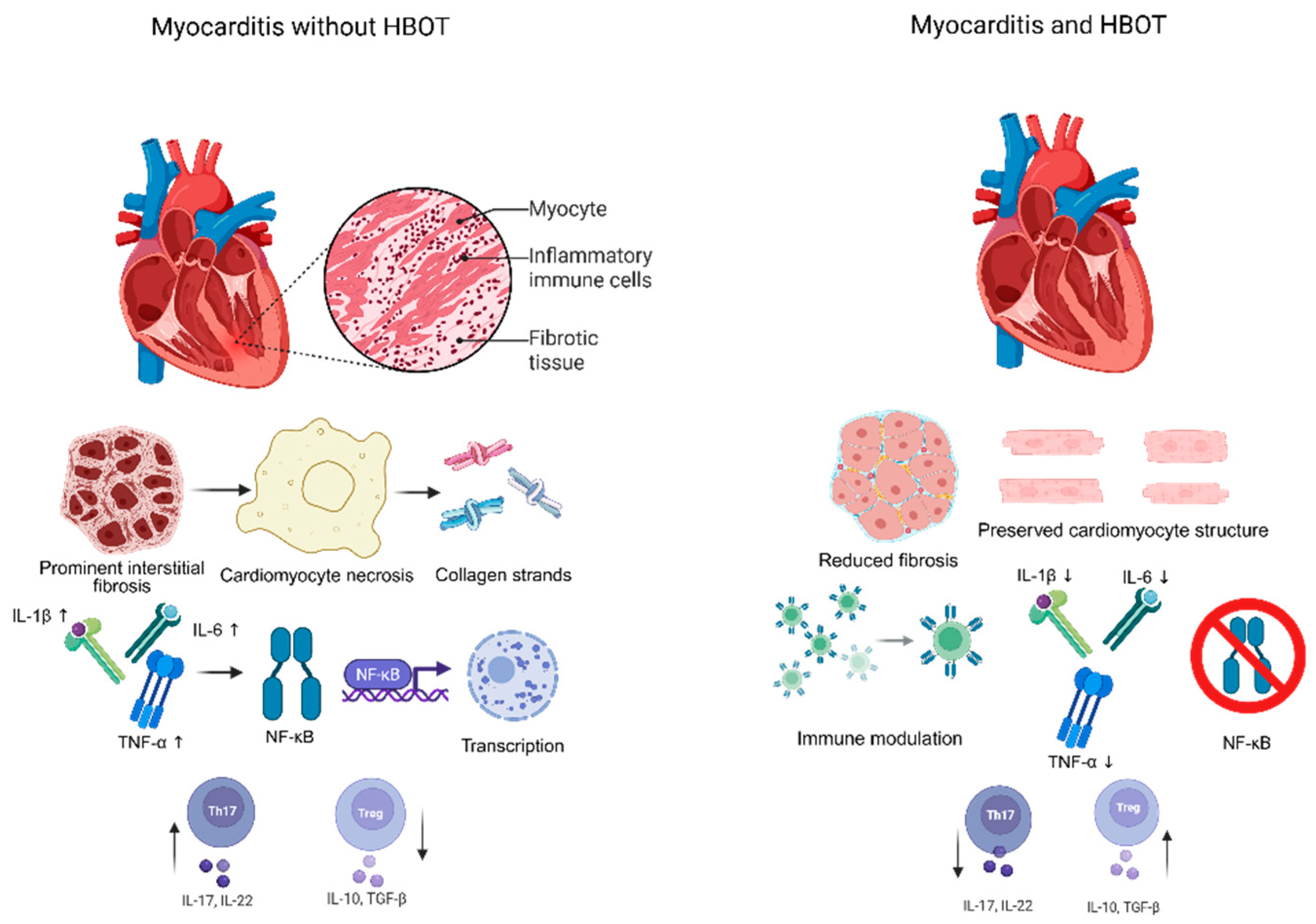

Table 1.
Relationship between pressure in atmospheres absolute (ATA), the breathing gas, and the resulting arterial oxygen tension (PaO2) [8,29,30,31].
| Approximate arterial oxygen tension at different hyperbaric pressures | |||
| ATA (atm abs) | Breathing Gas | Approximate PaO2 (mmHg) | Notes |
| 1.0 | Air | 100 | Normal ambient conditions |
| 1.0 | 100% O2 | 600 | Max dissolved O2 at sea level |
| 1.5 | 100% O2 | 1000 | Moderate hyperbaric oxygenation |
| 2.0 | 100% O2 | 1400 | Common therapeutic pressure |
| 2.5 | 100% O2 | >2000 | Standard HBOT protocol |
| 3.0 | 100% O2 | 2200–2800 | High end clinical HBOT pressure |
Collectively, these preclinical findings support HBOT as a potent multi-modal modulator of immune and oxidative pathways in EAM, providing a compelling rationale for further mechanistic and translational studies to optimize therapeutic regimens and explore applicability to human autoimmune myocarditis.
Table 2.
The outcomes of various HBOT protocols tested in animal models, mainly rats, under different pathological conditions.
Table 2.
The outcomes of various HBOT protocols tested in animal models, mainly rats, under different pathological conditions.
| Effects of different HBOT protocols in animal studies | |||
| Study | Model / Species | HBOT Regimen | Key Outcome(s) |
| Oliveira, Mario S et al., 2020 [21] | Rat myocardial ischemia (acute MI model) | 2.5 ATA, 60 min post-occlusion | ↑ SOD, catalase; ↓ ROS markers; improved survival |
| Chen, Chunxia et al., 2017 [38] | Rat myocardial model | 2.4 ATA, multiple sessions | ↓ TNF-α, IL-1β, IL-6; improved mitochondrial integrity |
| Lee J. Goldstein et al., 2009 [39] | Rat limb ischemia + EPC transplant | 2.4 ATA, 3 h/day × 5 days | ↑ bone marrow nitric oxide & CD34+ EPC → enhanced angiogenesis |
| Masatomo Y, Mamoru Y, 2000 [40] | Hemorrhagic shock in rats | 3.0 ATA, during resuscitation | ↓ systemic TNF-α & IL-6 mRNA and serum levels |
HBOT - Hyperbaric oxygen therapy, ATA - Atmospheres absolute (unit of pressure), MI - Myocardial infarction, ROS - Reactive oxygen species, SOD - Superoxide dismutase (antioxidant enzyme), TNF-α - Tumor necrosis factor α (pro-inflammatory cytokine), IL-1β, IL-6 - Interleukin 1 β / Interleukin 6 (pro-inflammatory cytokines), EPC - Endothelial progenitor cells.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



