Submitted:
21 December 2025
Posted:
22 December 2025
You are already at the latest version
Abstract
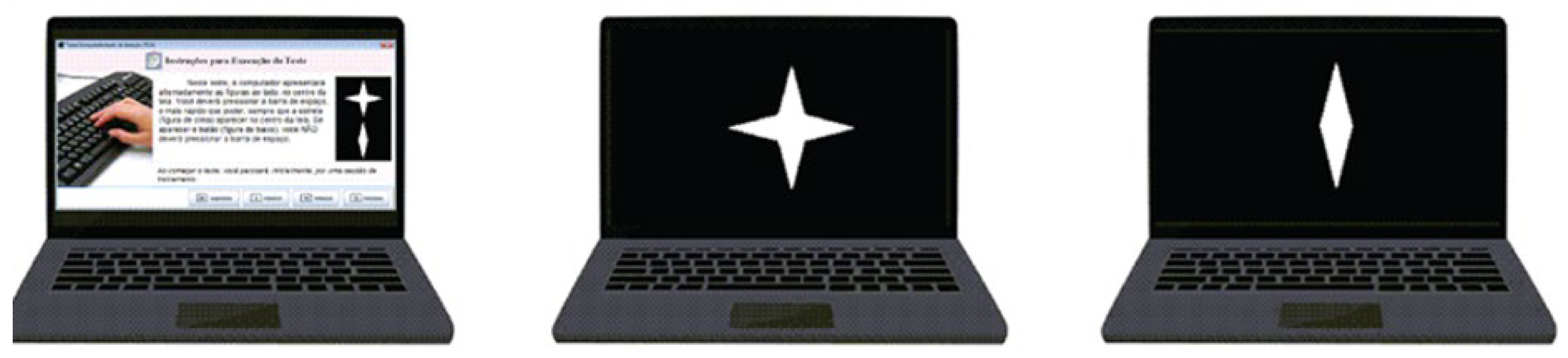
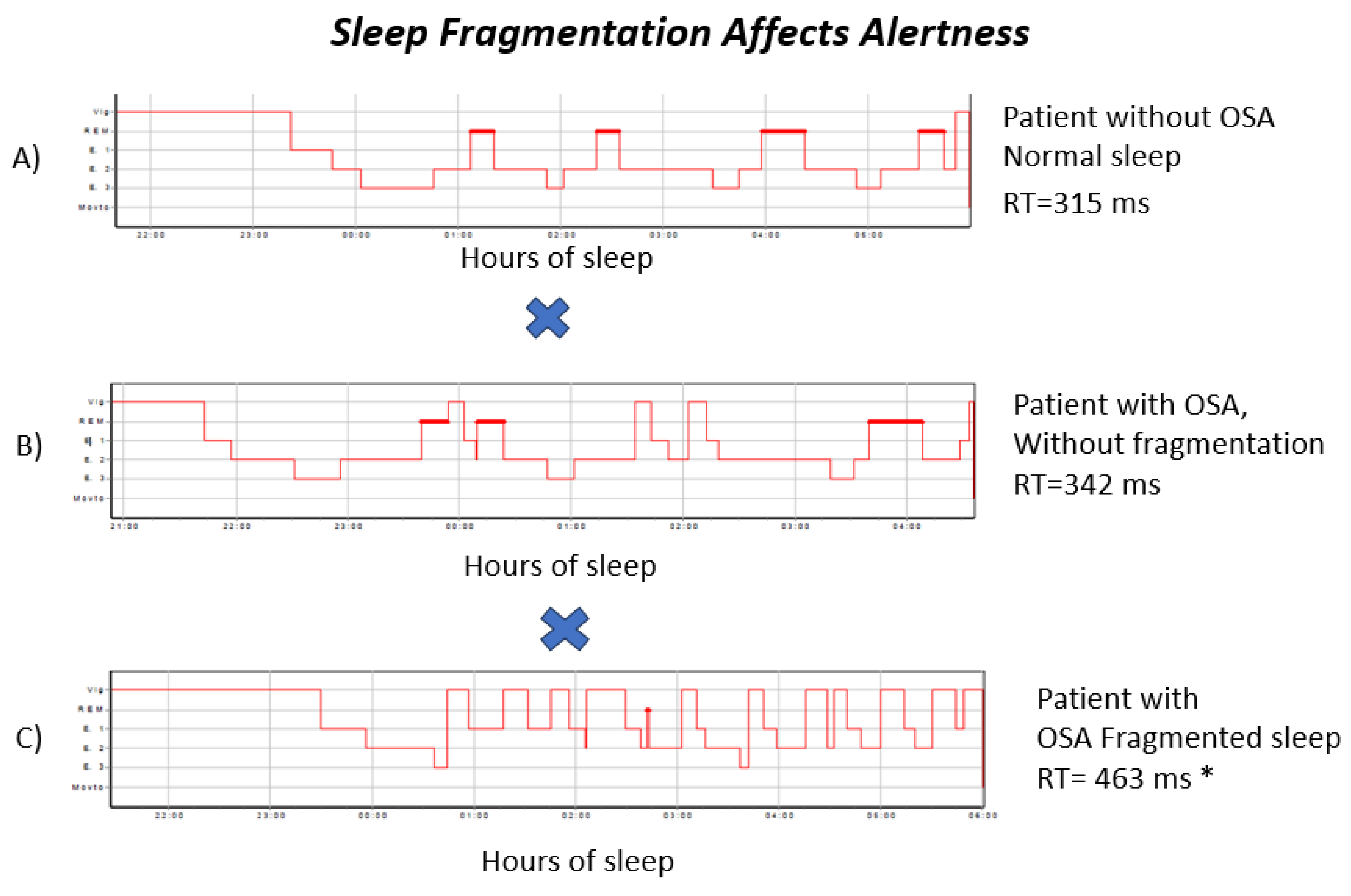
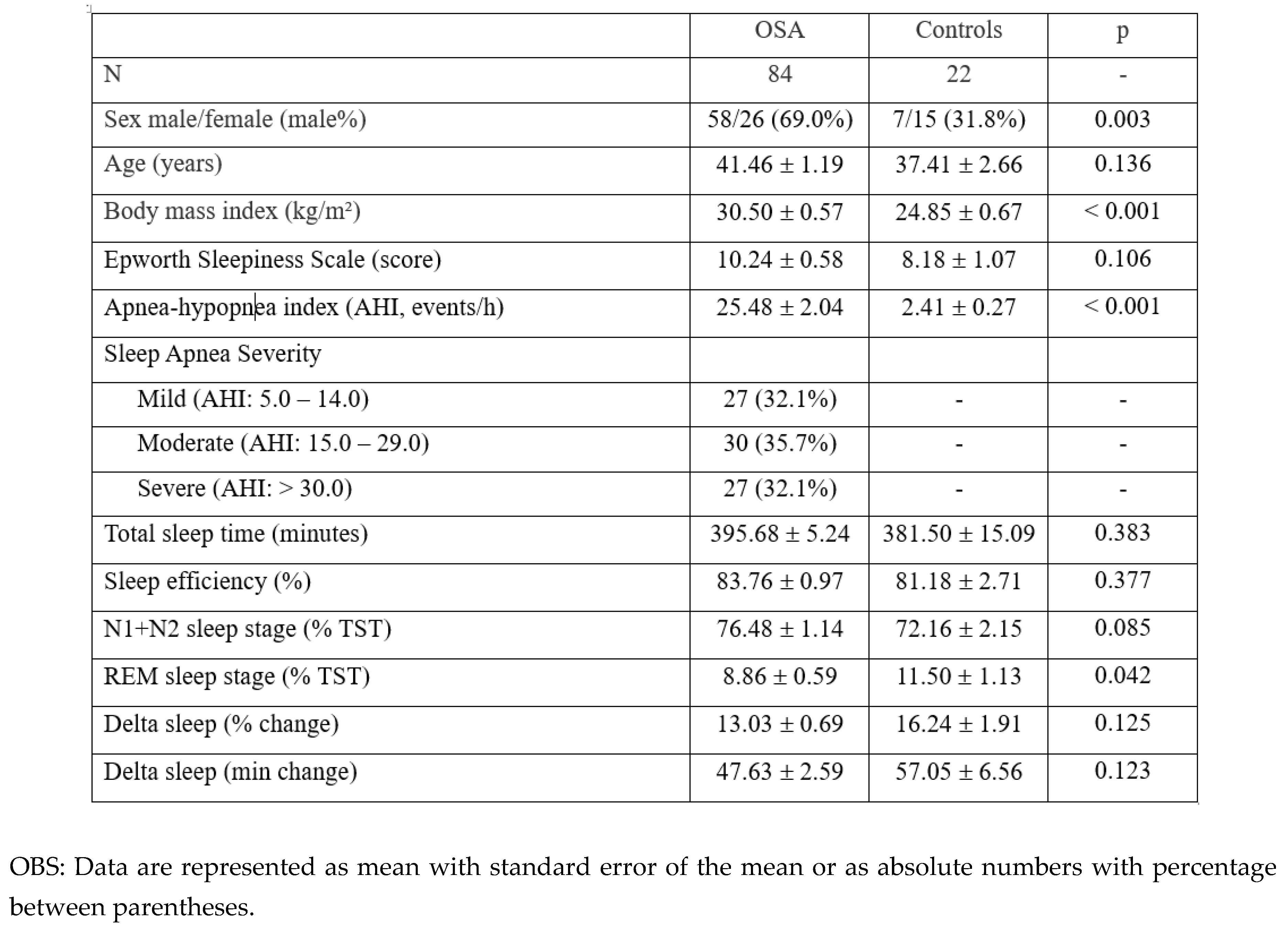
Background: Obstructive sleep apnea (OSA) is associated with slower response speed, yet conventional severity classification based on the apnea–hypopnea index (AHI) shows limited ability to predict cognitive outcomes. AHI aggregates distinct pathophysiological processes intermittent hypoxemia and sleep fragmentation. Within emerging precision sleep medicine frameworks, disentangling these mechanisms is critical for improved phenotyping and personalized risk assessment. This study aimed to replicate prior findings using a Go/No-Go Continuous Visual Attention Test (CVAT) and to identify the most informative polysomnographic predictor of attentional performance in OSA. Methods: All participants underwent full-night type I polysomnography and a 15-minute Go/No-Go CVAT. After exclusions, 84 patients with OSA and 22 polysomnographically normal controls were analyzed. Attentional performance was indexed by standardized reaction time (Z-score), referenced to a normative database (n = 1,244). Within the OSA group, multiple linear regression with backward elimination evaluated hypoxemia and sleep fragmentation metrics. Results: Patients with OSA demonstrated significantly slower reaction times than controls (p = 0.005). Within OSA, AHI was not associated with attentional performance (p = 0.398). In the final regression model, sleep stage shifts—reflecting sleep–wake instability—emerged as the sole independent predictor of attentional slowing (β = 0.27, p = 0.013), whereas all hypoxemia indices were excluded. Conclusions: Sleep-stage instability represents a key cognitive vulnerability marker in OSA, independent of respiratory event burden. Integrating sleep fragmentation metrics into precision sleep medicine models may enhance individualized phenotyping, identify patients at higher neurocognitive risk, and inform targeted interventions focused on stabilizing sleep architecture rather than relying solely on AHI-based severity classification.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Polysomnography and Parameter Quantification
2.3. Attention Assessment
2.4. Reference Group
2.5. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics
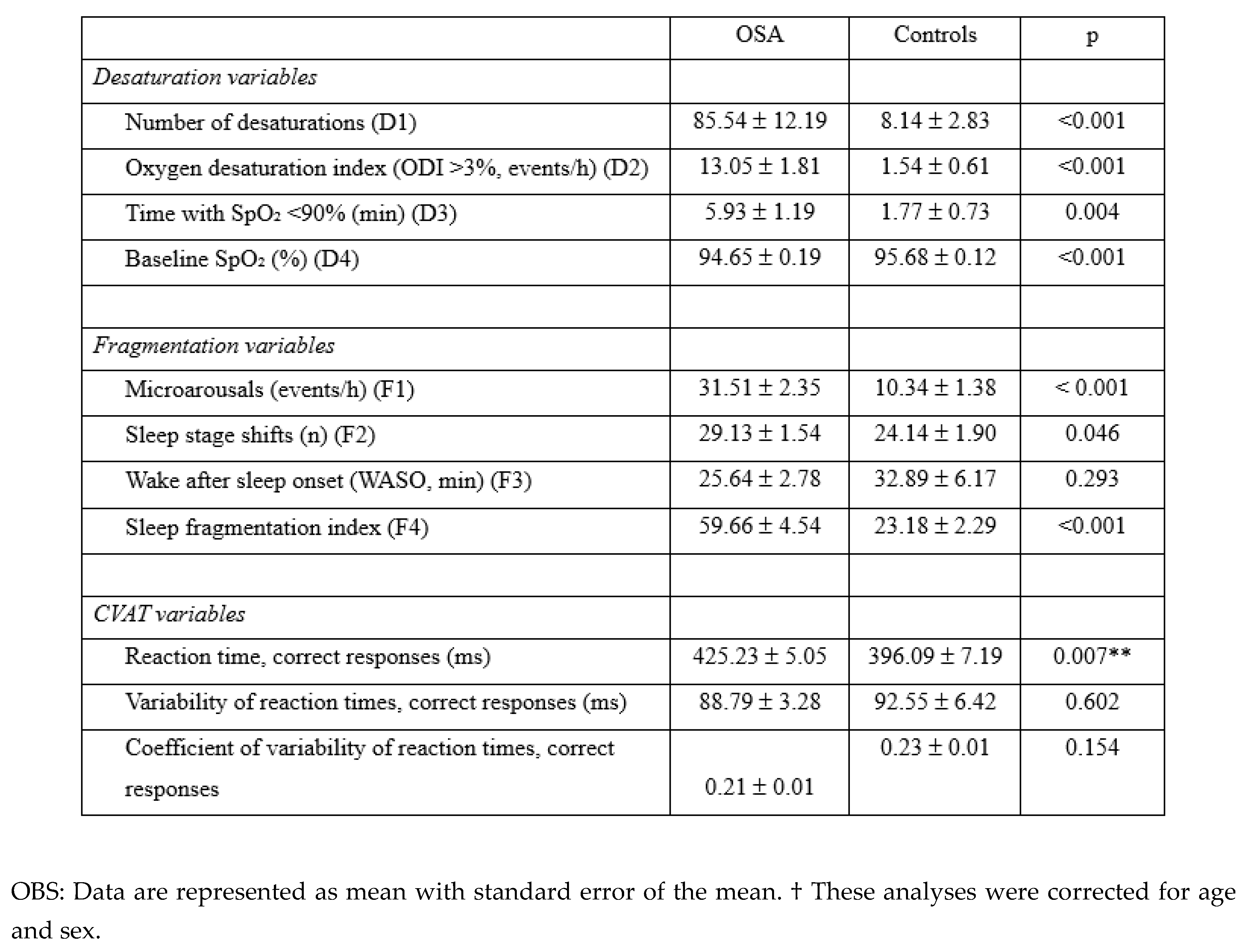
3.2. Desaturation and Sleep Fragmentation
3.3. First Objective
3.4. Second Objective
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bezerra, M.L.d.S.; van Duinkerken, E.; Simões, E.; Schmidt, S.L. General low alertness in people with obstructive sleep apnea. J. Clin. Sleep Med. 2024, 20, 689–698. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, M.L.d.S.; van Duinkerken, E.; Simões, E.; Schmidt, S.L. General low alertness in people with obstructive sleep apnea. J. Clin. Sleep Med. 2024, 20, 689–698. [Google Scholar] [CrossRef] [PubMed]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef]
- Georgeson, T.; Atkins, L.; Zahnleiter, A.; I Terrill, P.; Eeles, E.; Coulson, E.J.; Szollosi, I. Sleep fragmentation and hypoxaemia as key indicators of cognitive impairment in patients with obstructive sleep apnoea. Sleep Sci. Pr. 2025, 9, 1–11. [Google Scholar] [CrossRef]
- Kainulainen, S.; Duce, B.; Korkalainen, H.; Leino, A.; Huttunen, R.; Kalevo, L.; Arnardottir, E.S.; Kulkas, A.; Myllymaa, S.; Töyräs, J.; et al. Increased nocturnal arterial pulsation frequencies of obstructive sleep apnoea patients is associated with an increased number of lapses in a psychomotor vigilance task. ERJ Open Res. 2020, 6. [Google Scholar] [CrossRef]
- Angelelli, P.; Macchitella, L.; Toraldo, D.M.; Abbate, E.; Marinelli, C.V.; Arigliani, M.; De Benedetto, M. The Neuropsychological Profile of Attention Deficits of Patients with Obstructive Sleep Apnea: An Update on the Daytime Attentional Impairment. Brain Sci. 2020, 10, 325. [Google Scholar] [CrossRef]
- Lezak, M. D.; Howieson, D. B.; Bigler, E. D.; Tranel, D. Neuropsychological assessment, 5th ed.; Oxford University Press, 2012. [Google Scholar]
- Nance, R.M.; Fohner, A.E.; McClelland, R.L.; Redline, S.; Bryan, R.N.; Desiderio, L.; Habes, M.; Longstreth, J.W.; Schwab, R.J.; Wiemken, A.S.; et al. The Association of Upper Airway Anatomy with Brain Structure: The Multi-Ethnic Study of Atherosclerosis. Brain Imaging Behav. 2024, 18, 1–9. [Google Scholar] [CrossRef]
- Simões, E.N.; Padilla, C.S.; Bezerra, M.S.; Schmidt, S.L. Analysis of Attention Subdomains in Obstructive Sleep Apnea Patients. Front. Psychiatry 2018, 9, 435. [Google Scholar] [CrossRef]
- Bezerra, M.L.d.S.; van Duinkerken, E.; Simões, E.; Schmidt, S.L. General low alertness in people with obstructive sleep apnea. J. Clin. Sleep Med. 2024, 20, 689–698. [Google Scholar] [CrossRef]
- Ghaderi, S.; Mohammadi, S.; Mohammadi, M. Obstructive sleep apnea and attention deficits: A systematic review of magnetic resonance imaging biomarkers and neuropsychological assessments. Brain Behav. 2023, 13, e3262. [Google Scholar] [CrossRef]
- Laffan, A.; Caffo, B.; Swihart, B.J.; Punjabi, N.M. Utility of Sleep Stage Transitions in Assessing Sleep Continuity. Sleep 2010, 33, 1681–1686. [Google Scholar] [CrossRef]
- Morrell, M.J.; Finn, L.; Kim, H.; Peppard, P.E.; Badr, M.S.; Young, T. Sleep Fragmentation, Awake Blood Pressure, and Sleep-Disordered Breathing in a Population-based Study. Am. J. Respir. Crit. Care Med. 2000, 162, 2091–2096. [Google Scholar] [CrossRef] [PubMed]
- Silverman, I.W. Sex Differences in Simple Visual Reaction Time: A Historical Meta-Analysis. Sex Roles 2006, 54, 57–68. [Google Scholar] [CrossRef]
- E Beaudin, A.; Younes, M.; Gerardy, B.; Raneri, J.K.; Allen, A.J.M.H.; Gomes, T.; Gakwaya, S.; Sériès, F.; Kimoff, J.; Skomro, R.P.; et al. Association between sleep microarchitecture and cognition in obstructive sleep apnea. Sleep 2024, 47. [Google Scholar] [CrossRef]
- Djonlagic, I.E.; Guo, M.; Igue, M.; Kishore, D.; Stickgold, R.; Malhotra, A. Continuous Positive Airway Pressure Restores Declarative Memory Deficit in Obstructive Sleep Apnea. Am. J. Respir. Crit. Care Med. 2021, 203, 1188–1190. [Google Scholar] [CrossRef]
- Benkirane, O.; Simor, P.; Mairesse, O.; Peigneux, P. Sleep Fragmentation Modulates the Neurophysiological Correlates of Cognitive Fatigue. Clocks Sleep 2024, 6, 602–618. [Google Scholar] [CrossRef] [PubMed]
- Long, N.M.; Kuhl, B.A. Bottom-Up and Top-Down Factors Differentially Influence Stimulus Representations Across Large-Scale Attentional Networks. J. Neurosci. 2018, 38, 2495–2504. [Google Scholar] [CrossRef]
- Wood, C.; Bianchi, M.T.; Yun, C.-H.; Shin, C.; Thomas, R.J. Multicomponent Analysis of Sleep Using Electrocortical, Respiratory, Autonomic and Hemodynamic Signals Reveals Distinct Features of Stable and Unstable NREM and REM Sleep. Front. Physiol. 2020, 11. [Google Scholar] [CrossRef]
- Halassa, M.M.; Sherman, S.M. Thalamocortical Circuit Motifs: A General Framework. Neuron 2019, 103, 762–770. [Google Scholar] [CrossRef]
- Jiang-Xie, L.-F.; Drieu, A.; Bhasiin, K.; Quintero, D.; Smirnov, I.; Kipnis, J. Neuronal dynamics direct cerebrospinal fluid perfusion and brain clearance. Nature 2024, 627, 157–164. [Google Scholar] [CrossRef]
- Ren, R.; Zhang, Y.; Yang, L.; Somers, V.K.; Covassin, N.; Tang, X.; 22. Association Between Arousals During Sleep and Hypertension Among Patients With Obstructive Sleep Apnea. J. Am. Hear. Assoc. 2022, 11, e022141. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.



