Submitted:
18 December 2025
Posted:
18 December 2025
You are already at the latest version
Abstract
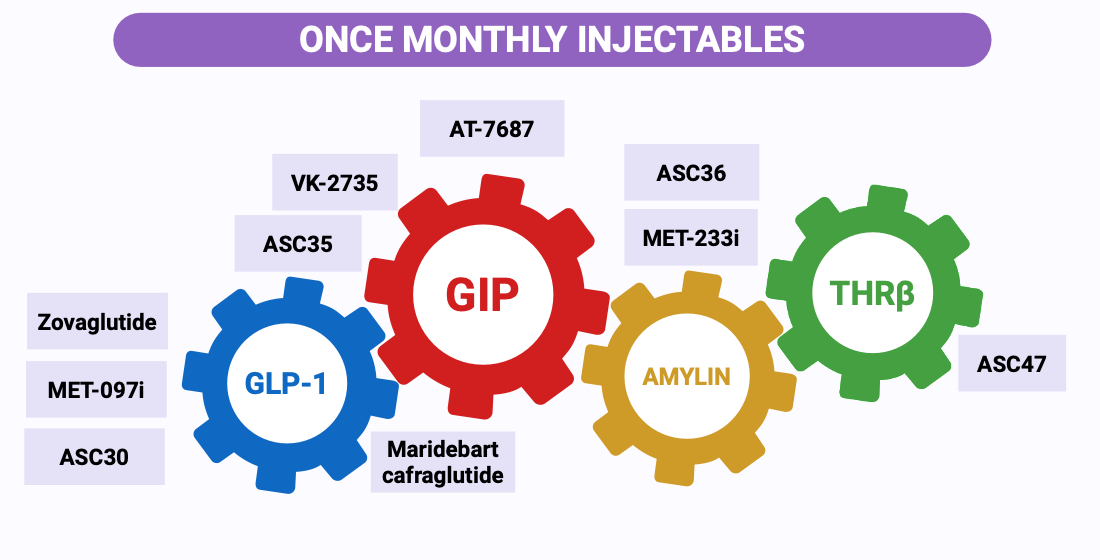
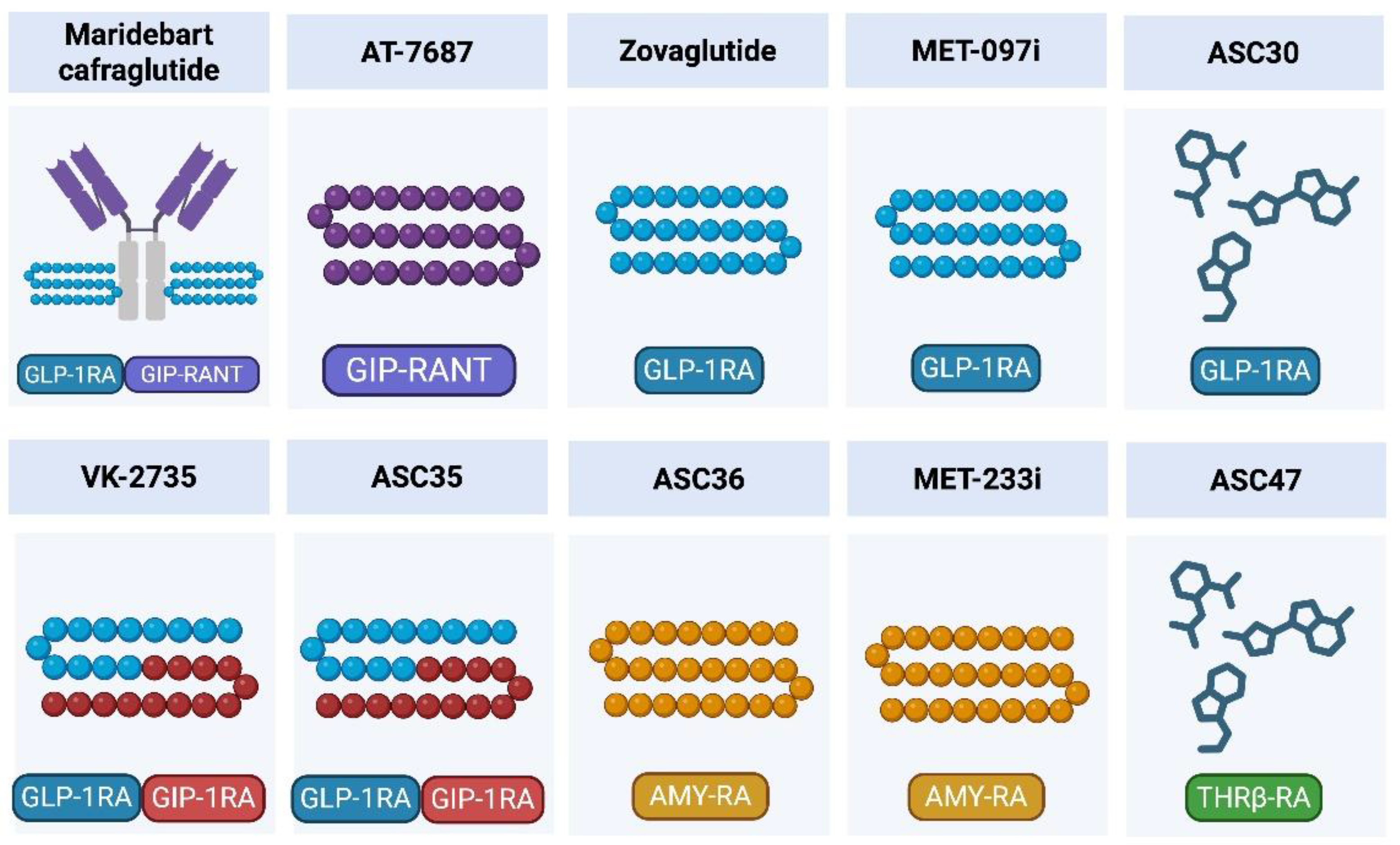
Once-monthly injectable therapies targeting glucagon-like peptide-1 (GLP-1), glucose-dependent insulinotropic polypeptide (GIP), and adjacent metabolic pathways are moving from a conceptual goal to a plausible next step for type 2 diabetes (T2D) and obesity. The most clinically advanced program is maridebart cafraglutide (MariTide), a long-acting GLP-1 receptor agonist conjugated to an Fc-containing scaffold that also mediates sustained GIP receptor antagonism. Across phase 2 trials, once-monthly maridebart has produced clinically meaningful weight loss (~12–16% in adults without diabetes; ~8–12% in those with T2D) together with HbA1c reductions of ~1.2–1.6 percentage points, with a safety profile broadly consistent with GLP-1–based therapy. An exploratory every-8-weeks regimen showed attenuated efficacy, suggesting that monthly dosing may represent a practical lower boundary for maintaining therapeutic exposure and metabolic effect in this format. Beyond maridebart, a rapidly expanding pipeline—including ultra–long-acting GLP-1 analogues, dual GLP-1/GIP agonists, long-acting GIPR antagonists, amylin receptor agonists, and emerging thyroid hormone receptor beta (THRβ) agonists—is actively testing monthly regimens or induction-to-monthly maintenance strategies; however, most readouts remain early and are frequently limited to conference presentations or sponsor communications. Key uncertainties include long-term durability, cardiometabolic outcomes, immunogenicity, and interindividual variability in response, which will ultimately determine how once-monthly regimens integrate with established weekly standards in routine care.
Keywords:
1. Introduction
2. Pharmacologic Principles of Once-Monthly Injectable Therapies
2.1. Rationale for Extending Dosing Intervals
2.2. Molecular Design Strategies for Ultra–Long-Acting Injectables
2.3. PK/PD Requirements for Once-Monthly Regimens
2.4. Safety Considerations for Monthly Dosing

| Asset | Primary target | Secondary target | Reported half-life* | Dominant half-life extension strategy | References |
|---|---|---|---|---|---|
| Native GLP-1 | GLP-1R | — | ~1.5–2 min | Rapid DPP-4 degradation and renal clearance (no protection) | [8] |
| Native GIP | GIPR | — | ~5–7 min | Rapid DPP-4 degradation and renal clearance (no protection) | [9] |
| Liraglutide | GLP-1R | — | ~13 h (~0.5 d) | Fatty-acylation → high albumin binding, reduced clearance | [45] |
| AT-7687 | GIPR antagonism |
— | ~27.4 h (~1.1 d) | Long-acting peptide engineering (program-specific) | [25,97] |
| Tirzepatide | GIPR | GLP-1R | ~120 h (~5 d) | Albumin binding via fatty-acid moiety | [52,56,61] |
| Semaglutide | GLP-1R | — | ~168 h (~7 d) | Albumin binding via fatty-acid moiety | [50,55,60] |
| VK-2735 | GLP-1R | GIPR | ~170–250 h (~7–10 d) | Long-acting peptide scaffold (program-specific) | [21,80,81,82,83,84,85,86] |
| Zovaglutide | GLP-1R | — | ~260–273 h (~11 d) | Extended half-life GLP-1 analogue (likely acylation/albumin-binding based) | [76,77,78] |
| MariTide (maridebart cafraglutide) | GLP-1R | GIPR antagonism |
~343–396 h (~14–16 d) | Peptide–antibody conjugate with FcRn recycling; markedly reduced clearance | [14,20] |
| MET-097i | GLP-1R | — | ~15–16 d | NuSH™ HALO proprietary ultra–long-acting engineering (controlled release + reduced clearance) | [47,48,49,69,70,71,72] |
| ASC36 | Amylin receptor | — | ~15 d | ULAP depot exposure + high intrinsic potency (AISBDD/POTENT) | [92,93] |
| MET-233i | Amylin receptor | — | ~19 d | NuSH™ HALO proprietary ultra–long-acting engineering | [22,73,74,75] |
| ASC35 | GLP-1R | GIPR | t½ ≥30 d | ULAP ultra–long-acting peptide engineering (with AISBDD-guided potency optimization; POTENT) | [91,92] |
| ASC47-103 | THRβ | — | ~26–40 d | ULAP long-acting depot exposure (with AISBDD-driven adipose-selective THRβ agonism; POTENT) | [94,95,96] |
| ASC30 | GLP-1R | — | ~36 d | AISBDD-derived potent small-molecule GLP-1RA formulated via ULAP subcutaneous depot | [87,88,89] |
3. Maridebart Cafraglutide (MariTide): Lead Once-Monthly GLP-1 RA Plus GIPR Antagonist
3.1. Mechanistic Rationale: GLP-1 RA Plus GIPR Antagonism
3.2. Preclinical and Early Clinical Development
3.3. Phase 2 Trials in Obesity Without T2D
3.4. Phase 2 Trials in T2D with Obesity
3.5. Safety and Tolerability Profile
3.6. Key Lessons from Maridebart Cafraglutide for Monthly Therapies
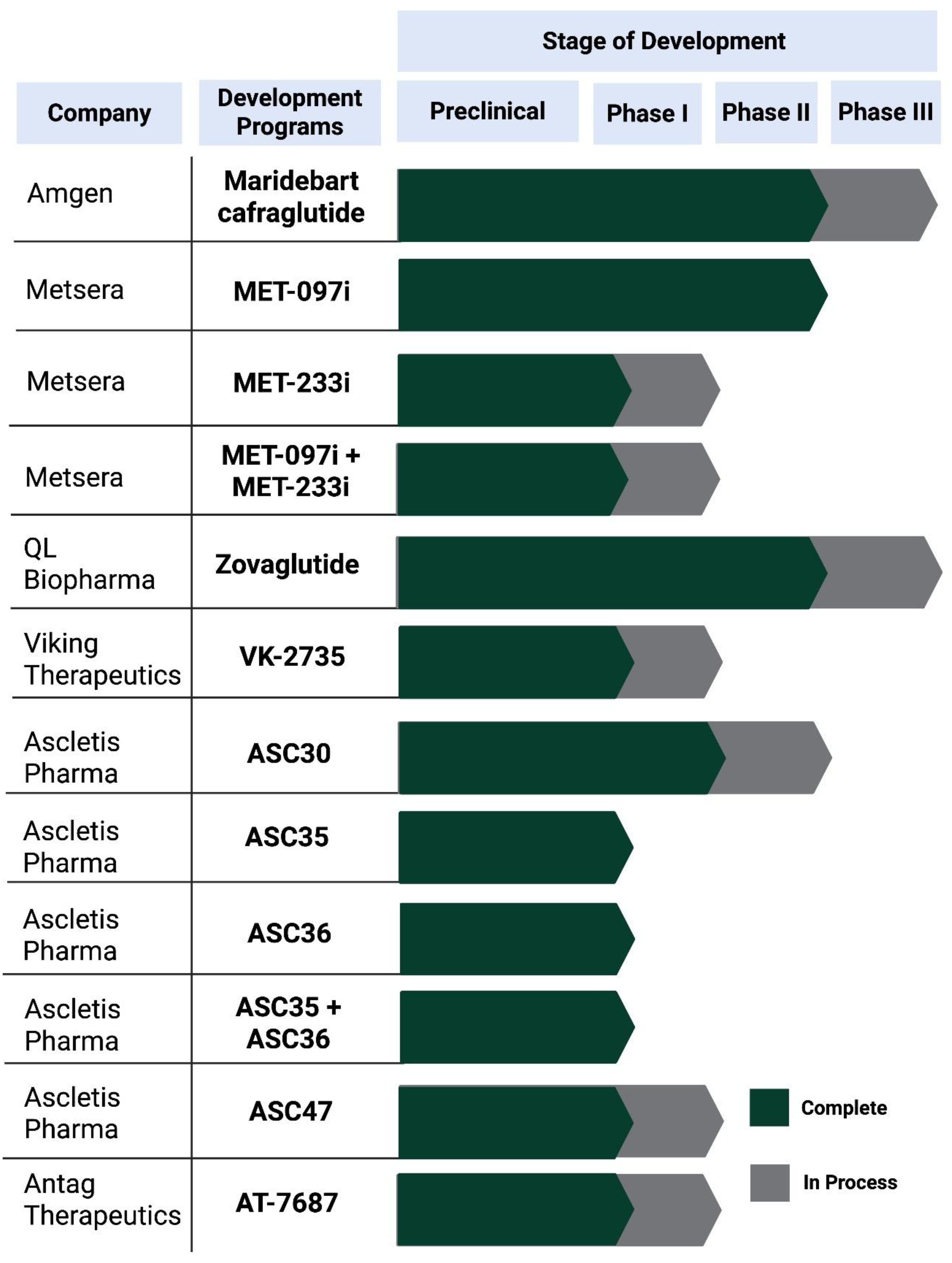
4. Beyond Maridebart: Emerging Once-Monthly Pipelines
4.1. MET-097i: Ultra–Long-Acting GLP-1 RA (NuSH Platform)
4.2. MET-233i: Ultra–Long-Acting Amylin Analogue
4.3. MET-233i + MET-097i: First-in-Class Monthly Multi-NuSH Combination
4.4. Zovaglutide (ZT002): A Once-Monthly Long-Acting GLP-1 RA
4.5. VK-2735: Dual GLP-1/GIP Receptor Agonist with a Maintenance-Oriented Path toward Monthly Dosing
4.6. ASC30: Ultra–Long-Acting Small-Molecule GLP-1 RA with Monthly and Quarterly Injectable Potential
4.7. ASC35: Once-Monthly Subcutaneous GLP-1R/GIPR Dual Peptide Agonist
4.8. ASC36: Once-Monthly Subcutaneous Amylin Receptor Peptide Agonist
4.9. ASC47: Adipose-Targeted, Once-Monthly Subcutaneous THRβ Agonist as a Muscle-Preserving Adjunct to Incretin Therapy
4.10. AT-7687: GIPR Peptide Antagonist with Extended-Interval Development Intent
5. Clinical Positioning and Future Role of Once-Monthly Therapies
5.1. Who Benefits Most from Monthly Dosing?
5.2. Induction-to-Monthly Maintenance and Switching Strategies
5.3. Practical Constraints: Tolerability, Safety Monitoring, Access and Cost
6. Discussion
7. Conclusions
Author Contributions
Funding
Abbreviations
| AI | Artificial intelligence |
| AISBDD | AI-Assisted Structure-Based Drug Discovery |
| BMI | Body mass index |
| cAMP | Cyclic adenosine monophosphate |
| EASD | European Association for the Study of Diabetes |
| ECG | Electrocardiogram |
| GI | Gastrointestinal |
| GIP | Glucose-dependent insulinotropic polypeptide |
| GIPR | Glucose-dependent insulinotropic polypeptide receptor |
| GLP-1 | Glucagon-like peptide-1 |
| GLP-1R | Glucagon-like peptide-1 receptor |
| GLP-1 RA | Glucagon-like peptide-1 receptor agonist |
| HbA1c | Glycated hemoglobin |
| IND | Investigational New Drug |
| LDL-C | Low-density lipoprotein cholesterol |
| NCT | ClinicalTrials.gov identifier |
| NuSH | Nutrient-stimulated hormone |
| PD | Pharmacodynamics |
| PK | Pharmacokinetics |
| PK/PD | Pharmacokinetics/pharmacodynamics |
| Q2W | Once every 2 weeks |
| Q4W | Once every 4 weeks |
| QTc | Corrected QT interval |
| SHBG | Sex hormone–binding globulin |
| SQ | Subcutaneous |
| T2D | Tpe 2 diabetes |
| THRβ | Thyroid hormone receptor beta |
| TSH | Thyroid-stimulating hormone |
| ULAP | Ultra-Long-Acting Platform |
References
- Buse, J.B.; Henry, R.R.; Han, J.; Kim, D.D.; Fineman, M.S.; Baron, A.D. Effects of exenatide (exendin-4) on glycemic control over 30 weeks in sulfonylurea-treated patients with type 2 diabetes. Diabetes Care 2004, 27, 2628–2635. [Google Scholar] [CrossRef]
- Buse, J.B.; Rosenstock, J.; Sesti, G.; Schmidt, W.E.; Montanya, E.; Brett, J.H.; Zychma, M.; Blonde, L. Liraglutide once a day versus exenatide twice a day for type 2 diabetes: a 26-week randomised, parallel-group, multinational, open-label trial (LEAD-6). Lancet 2009, 374, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Dungan, K.M.; Povedano, S.T.; Forst, T.; González, J.G.; Atisso, C.; Sealls, W.; Fahrbach, J.L. Once-weekly dulaglutide versus once-daily liraglutide in metformin-treated patients with type 2 diabetes (AWARD-6): a randomised, open-label, phase 3, non-inferiority trial. Lancet 2014, 384, 1349–1357. [Google Scholar] [CrossRef] [PubMed]
- Pratley, R.E.; Aroda, V.R.; Lingvay, I.; Lüdemann, J.; Andreassen, C.; Navarria, A.; Viljoen, A. Semaglutide versus dulaglutide once weekly in patients with type 2 diabetes (SUSTAIN 7): a randomised, open-label, phase 3b trial. Lancet Diabetes Endocrinol 2018, 6, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Marso, S.P.; Daniels, G.H.; Brown-Frandsen, K.; Kristensen, P.; Mann, J.F.; Nauck, M.A.; Nissen, S.E.; Pocock, S.; Poulter, N.R.; Ravn, L.S.; et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med 2016, 375, 311–322. [Google Scholar] [CrossRef]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jódar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med 2016, 375, 1834–1844. [Google Scholar] [CrossRef]
- Gerstein, H.C.; Colhoun, H.M.; Dagenais, G.R.; Diaz, R.; Lakshmanan, M.; Pais, P.; Probstfield, J.; Riesmeyer, J.S.; Riddle, M.C.; Rydén, L.; et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double-blind, randomised placebo-controlled trial. Lancet 2019, 394, 121–130. [Google Scholar] [CrossRef]
- Moiz, A.; Filion, K.B.; Tsoukas, M.A.; Yu, O.H.Y.; Peters, T.M.; Eisenberg, M.J. Mechanisms of GLP-1 Receptor Agonist-Induced Weight Loss: A Review of Central and Peripheral Pathways in Appetite and Energy Regulation. Am J Med 2025, 138, 934–940. [Google Scholar] [CrossRef]
- Zheng, Z.; Zong, Y.; Ma, Y.; Tian, Y.; Pang, Y.; Zhang, C.; Gao, J. Glucagon-like peptide-1 receptor: mechanisms and advances in therapy. Signal Transduct Target Ther 2024, 9, 234. [Google Scholar] [CrossRef]
- Moiz, A.; Filion, K.B.; Tsoukas, M.A.; Yu, O.H.Y.; Peters, T.M.; Eisenberg, M.J. The expanding role of GLP-1 receptor agonists: a narrative review of current evidence and future directions. EClinicalMedicine 2025, 86, 103363. [Google Scholar] [CrossRef]
- Rodriguez, P.J.; Zhang, V.; Gratzl, S.; Do, D.; Goodwin Cartwright, B.; Baker, C.; Gluckman, T.J.; Stucky, N.; Emanuel, E.J. Discontinuation and Reinitiation of Dual-Labeled GLP-1 Receptor Agonists Among US Adults With Overweight or Obesity. JAMA Netw Open 2025, 8, e2457349. [Google Scholar] [CrossRef] [PubMed]
- Altabas, V.; Orlović, Z.; Baretić, M. Addressing the Shortage of GLP-1 RA and Dual GIP/GLP-1 RA-Based Therapies—A Systematic Review. Diabetology 2025, 6, 52. [Google Scholar] [CrossRef]
- World Health Organization. WHO guideline on the use of glucagon-like peptide-1 (GLP-1) therapies for the treatment of obesity in adults; World Health Organization: Geneva, Switzerland, 2025. [Google Scholar]
- Jastreboff, A.M.; Ryan, D.H.; Bays, H.E.; Ebeling, P.R.; Mackowski, M.G.; Philipose, N.; Ross, L.; Liu, Y.; Burns, C.E.; Abbasi, S.A.; et al. Once-Monthly Maridebart Cafraglutide for the Treatment of Obesity—A Phase 2 Trial. N Engl J Med 2025, 393, 843–857. [Google Scholar] [CrossRef]
- Wu, C.C.; Cengiz, A.; Lawley, S.D. Less frequent dosing of GLP-1 receptor agonists as a viable weight maintenance strategy. Obesity (Silver Spring) 2025, 33, 1232–1236. [Google Scholar] [CrossRef] [PubMed]
- Cengiz, A.; Wu, C.C.; Lawley, S.D. Alternative dosing regimens of GLP-1 receptor agonists may reduce costs and maintain weight loss efficacy. Diabetes Obes Metab 2025, 27, 2251–2258. [Google Scholar] [CrossRef]
- Belančić, A.; Al-Sallami, H.S. Spotlight commentary: Changes in pharmacokinetics following significant weight loss. Br J Clin Pharmacol 2025, 91, 678–680. [Google Scholar] [CrossRef]
- Min, J.S.; Jo, S.J.; Lee, S.; Kim, D.Y.; Kim, D.H.; Lee, C.B.; Bae, S.K. A Comprehensive Review on the Pharmacokinetics and Drug-Drug Interactions of Approved GLP-1 Receptor Agonists and a Dual GLP-1/GIP Receptor Agonist. Drug Des Devel Ther 2025, 19, 3509–3537. [Google Scholar] [CrossRef]
- Del Prato, S.; Kang, J.; Trautmann, M.E.; Stewart, J.; Sorli, C.H.; Derwahl, M.; Soto, A.; Yoon, K.H. Efficacy and safety of once-monthly efpeglenatide in patients with type 2 diabetes: Results of a phase 2 placebo-controlled, 16-week randomized dose-finding study. Diabetes Obes Metab 2020, 22, 1176–1186. [Google Scholar] [CrossRef]
- Véniant, M.M.; Lu, S.C.; Atangan, L.; Komorowski, R.; Stanislaus, S.; Cheng, Y.; Wu, B.; Falsey, J.R.; Hager, T.; Thomas, V.A.; et al. A GIPR antagonist conjugated to GLP-1 analogues promotes weight loss with improved metabolic parameters in preclinical and phase 1 settings. Nat Metab 2024, 6, 290–303. [Google Scholar] [CrossRef]
- Modesto, K.; Chung, K.; Ji, S.; Stubbe, S.; Albers, K.; Lian, B. Abstract 4367152: VANQUISH-2: Phase 3, randomized, double-blind, placebo-controlled trial of weekly subcutaneous administration of VK2735 in obese or overweight adults with type 2 diabetes. Circulation 2025, 152, A4367152–A4367152. [Google Scholar] [CrossRef]
- Minnion, J.S.; Hinds, C.; Reglinska, B. 894-P: MET-233 is an ultra-long-acting amylin receptor agonist. Diabetes 2025, 74 (Suppl. 1), 894–P. [Google Scholar] [CrossRef]
- Hinds, C.; Minnion, J.S.; Zoumpoulidou, G. 794-P: MET-097: Preclinical characterization of a potent and ultra-long-acting GLP-1 receptor agonist. Diabetes 2025, 74 Suppl. 1, 794–P. [Google Scholar] [CrossRef]
- Rosenkilde, M.M.; George, J.T.; Véniant, M.M.; Holst, J.J. GIP Receptor Antagonists in the Pharmacotherapy of Obesity: Physiologic, Genetic, and Clinical Rationale. Diabetes 2025, 74, 1334–1338. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.H.; Sanni, S.J.; Riber, D.; Holst, J.J.; Rosenkilde, M.M.; Sparre-Ulrich, A.H. AT-7687, a novel GIPR peptide antagonist, combined with a GLP-1 agonist, leads to enhanced weight loss and metabolic improvements in cynomolgus monkeys. Mol Metab 2024, 88, 102006. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Yu, S.; Jin, X.; Sheng, L.; YanMu, M.R.; Gao, J.; Lu, J.; Lei, T. The Clinical Application of GLP-1RAs and GLP-1/GIP Dual Receptor Agonists Based on Pharmacological Mechanisms: A Review. Drug Des Devel Ther 2025, 19, 10383–10409. [Google Scholar] [CrossRef]
- Xu, Y.; Drucker, D.J.; Traverso, G.; Beloqui, A. Innovative molecules and delivery technologies enabling the future of GLP-1-based therapies. Endocr Rev 2025, Epub ahead of print. [Google Scholar] [CrossRef]
- Li, Z.; Han, Z.; Sun, R.; Xuan, X.; Huang, C. Long-Term Efficacy Trajectories of GLP-1 Receptor Agonists: A Systematic Review and Network Meta-Analysis. Diabetes Metab Syndr Obes 2025, 18, 3611–3624. [Google Scholar] [CrossRef]
- Ferreira, K.; Kont, E.; Abdelkhalik, A.; Jones, D.; Baker-Knight, J. The out-of-pocket cost of living with obesity: Results from a survey in Spain, South Korea, Brazil, India, Italy, and Japan. Obes Sci Pract 2024, 10, e70000. [Google Scholar] [CrossRef]
- Okunogbe, A.; Nugent, R.; Spencer, G.; Ralston, J.; Wilding, J. Economic impacts of overweight and obesity: current and future estimates for eight countries. BMJ Glob Health 2021, 6, e006351. [Google Scholar] [CrossRef]
- Hauber, A.B.; Nguyen, H.; Posner, J.; Kalsekar, I.; Ruggles, J. A discrete-choice experiment to quantify patient preferences for frequency of glucagon-like peptide-1 receptor agonist injections in the treatment of type 2 diabetes. Curr Med Res Opin 2016, 32, 251–262. [Google Scholar] [CrossRef]
- Gelhorn, H.L.; Poon, J.L.; Davies, E.W.; Paczkowski, R.; Curtis, S.E.; Boye, K.S. Evaluating preferences for profiles of GLP-1 receptor agonists among injection-naïve type 2 diabetes patients in the UK. Patient Prefer Adherence 2015, 9, 1611–1622. [Google Scholar] [CrossRef] [PubMed]
- Trujillo, J.M.; Nuffer, W.; Ellis, S.L. GLP-1 receptor agonists: a review of head-to-head clinical studies. Ther Adv Endocrinol Metab 2015, 6, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Denimal, D. Emerging perspectives on once-weekly insulins in type 1 and type 2 diabetes: a mini-review. Front Endocrinol (Lausanne) 2025, 16, 1656884. [Google Scholar] [CrossRef] [PubMed]
- Qin, L.; Chen, S.; Flood, E.; Shaunik, A.; Romero, B.; de la Cruz, M.; Alvarez, C.; Grandy, S. Glucagon-like Peptide-1 Receptor Agonist Treatment Attributes Important to Injection-Naïve Patients with Type 2 Diabetes Mellitus: A Multinational Preference Study. Diabetes Ther 2017, 8, 321–334. [Google Scholar] [CrossRef]
- Wan, W.; Qin, Q.; Xie, L.; Zhang, H.; Wu, F.; Stevens, R.C.; Liu, Y. GLP-1R Signaling and Functional Molecules in Incretin Therapy. Molecules 2023, 28, 0751. [Google Scholar] [CrossRef]
- Deng, W.; Zhao, Z.; Zou, T.; Kuang, T.; Wang, J. Research Advances in Fusion Protein-Based Drugs for Diabetes Treatment. Diabetes Metab Syndr Obes 2024, 17, 343–362. [Google Scholar] [CrossRef]
- Peri, R.V.; Anchan, H.; Jonnalagadda, K.; Varghese, R.; Gupta, P. Designing GLP-1 delivery: structural perspectives and formulation approaches for optimized therapy. Nutr Diabetes 2025, 15, 53. [Google Scholar] [CrossRef]
- Lu, S.C.; Chen, M.; Atangan, L.; Killion, E.A.; Komorowski, R.; Cheng, Y.; Netirojjanakul, C.; Falsey, J.R.; Stolina, M.; Dwyer, D.; et al. GIPR antagonist antibodies conjugated to GLP-1 peptide are bispecific molecules that decrease weight in obese mice and monkeys. Cell Rep Med 2021, 2, 100263. [Google Scholar] [CrossRef]
- Anastasiou, I.A.; Argyrakopoulou, G.; Dalamaga, M.; Kokkinos, A. Dual and Triple Gut Peptide Agonists on the Horizon for the Treatment of Type 2 Diabetes and Obesity. An Overview of Preclinical and Clinical Data. Curr Obes Rep 2025, 14, 34. [Google Scholar] [CrossRef]
- Emanuelsson, F.; Nordestgaard, B.G.; Benn, M. Genetic variants of glucose-dependent insulinotropic polypeptide (GIP) signalling as proxy for body weight reduction and cardiovascular risk. Eur Heart J 2025. [Google Scholar] [CrossRef]
- Kizilkaya, H.S.; Sørensen, K.V.; Kibsgaard, C.J.; Gasbjerg, L.S.; Hauser, A.S.; Sparre-Ulrich, A.H.; Grarup, N.; Rosenkilde, M.M. Loss of Function Glucose-Dependent Insulinotropic Polypeptide Receptor Variants Are Associated With Alterations in BMI, Bone Strength and Cardiovascular Outcomes. Front Cell Dev Biol 2021, 9, 749607. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.E. Targeting the GIPR for obesity: To agonize or antagonize? Potential mechanisms. Mol Metab 2021, 46, 101139. [Google Scholar] [CrossRef] [PubMed]
- Tan, H.; Su, W.; Zhang, W.; Zhang, J.; Sattler, M.; Zou, P. Albumin-binding domain extends half-life of glucagon-like peptide-1. Eur J Pharmacol 2021, 890, 173650. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, L.B.; Lau, J. The Discovery and Development of Liraglutide and Semaglutide. Front Endocrinol (Lausanne) 2019, 10, 155. [Google Scholar] [CrossRef]
- Přáda Brichtová, E.; Edu, I.A.; Li, X.; Becher, F.; Gomes Dos Santos, A.L.; Jackson, S.E. Effect of Lipidation on the Structure, Oligomerization, and Aggregation of Glucagon-like Peptide 1. Bioconjug Chem 2025, 36, 401–414. [Google Scholar] [CrossRef]
- Metsera, Inc. Metsera Announces Positive Topline Phase 2a Clinical Data for its Ultra-Long Acting GLP-1 Receptor Agonist MET-097i. Business Wire 2025. Available online: https://www.businesswire.com/news/home/20250106419531/en/Metsera-Announces-Positive-Topline-Phase-2a-Clinical-Data-for-its-Ultra-Long-Acting-GLP-1-Receptor-Agonist-MET-097i (accessed on 17 Dec 2025).
- Metsera, Inc. Metsera Pipeline: Advancing Next-Generation Obesity Therapies. Metsera 2024. Available online: https://metsera.com/pipeline/ (accessed on 17 Dec 2025).
- Metsera, Inc. Metsera Reports Positive Phase 2b Results for First-and-Best-in-Class Ultra-Long Acting GLP-1 RA Candidate MET-097i Enabling Rapid Transition into Phase 3. GlobeNewswire 2025. Available online: https://www.globenewswire.com/news-release/2025/09/29/3158095/0/en/Metsera-Reports-Positive-Phase-2b-Results-for-First-and-Best-in-Class-Ultra-long-Acting-GLP-1-RA-Candidate-MET-097i-Enabling-Rapid-Transition-into-Phase-3.html (accessed on 17 Dec 2025).
- Sorli, C.; Harashima, S.I.; Tsoukas, G.M.; Unger, J.; Karsbøl, J.D.; Hansen, T.; Bain, S.C. Efficacy and safety of once-weekly semaglutide monotherapy versus placebo in patients with type 2 diabetes (SUSTAIN 1): a double-blind, randomised, placebo-controlled, parallel-group, multinational, multicentre phase 3a trial. Lancet Diabetes Endocrinol 2017, 5, 251–260. [Google Scholar] [CrossRef]
- Granhall, C.; Donsmark, M.; Blicher, T.M.; Golor, G.; Søndergaard, F.L.; Thomsen, M.; Bækdal, T.A. Safety and Pharmacokinetics of Single and Multiple Ascending Doses of the Novel Oral Human GLP-1 Analogue, Oral Semaglutide, in Healthy Subjects and Subjects with Type 2 Diabetes. Clin Pharmacokinet 2019, 58, 781–791. [Google Scholar] [CrossRef]
- Nauck, M.A.; D’Alessio, D.A. Tirzepatide, a dual GIP/GLP-1 receptor co-agonist for the treatment of type 2 diabetes with unmatched effectiveness regarding glycaemic control and body weight reduction. Cardiovasc Diabetol 2022, 21, 169. [Google Scholar] [CrossRef]
- Brønden, A.; Knop, F.K.; Christensen, M.B. Clinical Pharmacokinetics and Pharmacodynamics of Albiglutide. Clin Pharmacokinet 2017, 56, 719–731. [Google Scholar] [CrossRef]
- Xu, J.; Zhang, Y.; Li, Y.; Zhao, X.; Zhou, W.; Loghin, C.; Tham, L.S.; Cui, X.; Cui, Y.; Wang, W. Pharmacokinetics, Pharmacodynamics, and Safety of Dulaglutide After Single or Multiple Doses in Chinese Healthy Subjects and Patients with T2DM: A Randomized, Placebo-Controlled, Phase I Study. Adv Ther 2022, 39, 488–503. [Google Scholar] [CrossRef]
- Ahmann, A.J.; Capehorn, M.; Charpentier, G.; Dotta, F.; Henkel, E.; Lingvay, I.; Holst, A.G.; Annett, M.P.; Aroda, V.R. Efficacy and Safety of Once-Weekly Semaglutide Versus Exenatide ER in Subjects With Type 2 Diabetes (SUSTAIN 3): A 56-Week, Open-Label, Randomized Clinical Trial. Diabetes Care 2018, 41, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Frías, J.P.; Davies, M.J.; Rosenstock, J.; Pérez Manghi, F.C.; Fernández Landó, L.; Bergman, B.K.; Liu, B.; Cui, X.; Brown, K. Tirzepatide versus Semaglutide Once Weekly in Patients with Type 2 Diabetes. N Engl J Med 2021, 385, 503–515. [Google Scholar] [CrossRef] [PubMed]
- Geiser, J.S.; Heathman, M.A.; Cui, X.; Martin, J.; Loghin, C.; Chien, J.Y.; de la Peña, A. Clinical Pharmacokinetics of Dulaglutide in Patients with Type 2 Diabetes: Analyses of Data from Clinical Trials. Clin Pharmacokinet 2016, 55, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Puig, M.; Shubow, S. Immunogenicity of therapeutic peptide products: bridging the gaps regarding the role of product-related risk factors. Front Immunol 2025, 16, 1608401. [Google Scholar] [CrossRef]
- Nauck, M.A.; Meier, J.J. Management of Endocrine Disease: Are all GLP-1 agonists equal in the treatment of type 2 diabetes? Eur J Endocrinol 2019, 181, R211–R234. [Google Scholar] [CrossRef]
- Wilding, J.P.H.; Batterham, R.L.; Calanna, S.; Davies, M.; Van Gaal, L.F.; Lingvay, I.; McGowan, B.M.; Rosenstock, J.; Tran, M.T.D.; Wadden, T.A.; et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med 2021, 384, 989–1002. [Google Scholar] [CrossRef]
- Jastreboff, A.M.; Aronne, L.J.; Ahmad, N.N.; Wharton, S.; Connery, L.; Alves, B.; Kiyosue, A.; Zhang, S.; Liu, B.; Bunck, M.C.; et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med 2022, 387, 205–216. [Google Scholar] [CrossRef]
- Davies, M.J.; Aroda, V.R.; Collins, B.S.; Gabbay, R.A.; Green, J.; Maruthur, N.M.; Rosas, S.E.; Del Prato, S.; Mathieu, C.; Mingrone, G.; et al. Management of Hyperglycemia in Type 2 Diabetes, 2022. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2022, 45, 2753–2786. [Google Scholar] [CrossRef]
- Douros, J.D.; Mowery, S.A.; Knerr, P.J. The Premise of the Paradox: Examining the Evidence That Motivated GIPR Agonist and Antagonist Drug Development Programs. J Clin Med 2025, 14, 3812. [Google Scholar] [CrossRef]
- Wolfe, M.M.; Boylan, M.O.; Chin, W.W. Glucose-Dependent Insulinotropic Polypeptide in Incretin Physiology: Role in Health and Disease. Endocr Rev 2025, 46, 479–500. [Google Scholar] [CrossRef]
- Pfizer, Inc. Pfizer Completes Acquisition of Metsera. Pfizer Press Release 2025. Available online: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-completes-acquisition-metsera (accessed on 17 Dec 2025).
- Metsera, Inc. Registration Statement on Form S-1. U.S. Securities and Exchange Commission (SEC) 2025. Available online: https://www.sec.gov/Archives/edgar/data/2040807/000119312525004504/d900229ds1.htm (accessed on 17 Dec 2025).
- Hansford, R.; Hinds, C.; Adams, W.J. 765-P: Therapeutic NuSH Cocktails—Coadministration of Ultra-Long-Acting GLP-1, GIP, Glucagon, and Amylin Peptide Analogs Induce Profound Weight Loss in DIO Mice. Diabetes 2025, 74 Suppl. 1, 765–P. [Google Scholar] [CrossRef]
- Metsera, Inc. Metsera Pipeline MET-097i. Metsera 2024. Available online: https://metsera.com/pipeline/#met-097 (accessed on 17 Dec 2025).
- Stoekenbroek, R.; Bisch, J.; Kolluri, S.; Noor, M.A.; Mallory, J.; Cunningham, R.; Hubbard, B.; Marso, S.P. 788-P: A Twelve-Week Trial of MET097—A Potent and Ultra-Long-Acting GLP-1 Receptor Agonist. Diabetes 2025, 74 Suppl. 1, 788–P. [Google Scholar] [CrossRef]
- Metsera, Inc. A Phase 2b Study to Examine the Safety and Efficacy of Four Different Regimens of Once-weekly MET-097 in Adults With Obesity or Overweight. ClinicalTrials.gov 2024. Available online: https://clinicaltrials.gov/study/NCT06712836 (accessed on 17 Dec 2025).
- Metsera, Inc. A Phase 2b Study to Evaluate the Efficacy and Safety of Once-monthly MET-097 in Adults With Obesity or Overweight. ClinicalTrials.gov 2025. Available online: https://www.clinicaltrials.gov/study/NCT06973720 (accessed on 17 Dec 2025).
- Metsera, Inc. Metsera Announces Positive Phase 1 Data of First-in-Class Once-Monthly Amylin Candidate MET-233i. BioSpace 2025. Available online: https://www.biospace.com/press-releases/metsera-announces-positive-phase-1-data-of-first-in-class-once-monthly-amylin-candidate-met-233i (accessed on 17 Dec 2025).
- ClinicalTrials.gov. A Study of MET233 in Combination With MET097 in Individuals With Obesity or Overweight With or Without Diabetes. Available online: https://clinicaltrials.gov/study/NCT06924320 (accessed on 17 Dec 2025).
- QL Biopharm reports Phase 2 results of a monthly dose study evaluating zovaglutide, a novel, extended half-life GLP-1 receptor agonist at EASD 2025. BioSpace (Press Releases) 2025. Available online: https://www.biospace.com/press-releases/ql-biopharm-reports-phase-2-results-of-a-monthly-dose-study-evaluating-zovaglutide-a-novel-extended-half-life-glp-1-receptor-agonist-at-easd-2025 (accessed on 17 Dec 2025).
- 61st EASD Annual Meeting of the European Association for the Study of Diabetes: Vienna, Austria, 15–19 September 2025. Diabetologia 2025, 68 Suppl. 1, 1–754. [CrossRef]
- Beijing QL Biopharmaceutical Co; Ltd. A Study of Zovaglutide in Subjects With Overweight or Obesity (HORIZON-1). Available online: https://clinicaltrials.gov/study/NCT07230119 (accessed on 17 Dec 2025).
- Liu, Q.K. Mechanisms of action and therapeutic applications of GLP-1 and dual GIP/GLP-1 receptor agonists. Front Endocrinol (Lausanne) 2024, 15, 1431292. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. Phase 1 Study to Evaluate the Safety and Tolerability of VK2735. Available online: https://www.clinicaltrials.gov/study/NCT05203237 (accessed on 15 Dec 2025).
- Viking Therapeutics; Inc. Viking Therapeutics Announces Results from Phase 1 Clinical Trial of Dual GLP-1/GIP Receptor Agonist VK2735. Available online: https://ir.vikingtherapeutics.com/2023-03-28-Viking-Therapeutics-Announces-Results-from-Phase-1-Clinical-Trial-of-Dual-GLP-1-GIP-Receptor-Agonist-VK2735 (accessed on 17 Dec 2025).
- Viking Therapeutics; Inc. VK2735 (Subcutaneous & Oral Formulations): Dual GLP-1/GIP Receptor Agonist. Available online: https://vikingtherapeutics.com/pipeline/metabolic-disease-program/vk2735/ (accessed on 17 Dec 2025).
- Viking Therapeutics; Inc. Viking Therapeutics Presents Preclinical Data on Novel Dual GLP-1/GIP Agonists at ObesityWeek® 2021. Available online: https://ir.vikingtherapeutics.com/2021-11-01-Viking-Therapeutics-Presents-Preclinical-Data-on-Novel-Dual-GLP-1-GIP-Agonists-at-ObesityWeek-R-2021 (accessed on 17 Dec 2025).
- Viking Therapeutics; Inc. Viking Therapeutics Announces Initiation of VK2735 Maintenance Dosing Clinical Trial in Patients with Obesity. Available online: https://ir.vikingtherapeutics.com/2025-10-21-Viking-Therapeutics-Announces-Initiation-of-VK2735-Maintenance-Dosing-Clinical-Trial-in-Patients-with-Obesity (accessed on 17 Dec 2025).
- ClinicalTrials.gov. VK2735 for Weight Management Phase 3 (VANQUISH 1). Available online: https://clinicaltrials.gov/study/NCT07104500 (accessed on 17 Dec 2025).
- ClinicalTrials.gov. VK2735 for Weight Management Type 2 Diabetes Phase 3 (VANQUISH 2). Available online: https://clinicaltrials.gov/study/NCT07104383 (accessed on 17 Dec 2025).
- Wu, J.J.; Wang, V. ASC30, a Once-Monthly SQ Injected Small Molecule GLP-1RA in Participants with Obesity: A Phase Ib Study. Proceedings of ObesityWeek®, Atlanta, GA, USA, 2–6 November 2025; p. Poster-174. [Google Scholar]
- Wu, J.J. ASC30, an oral GLP-1 receptor biased small-molecule agonist in participants with obesity: Phase I clinical evaluation. In Proceedings of the 85th Scientific Sessions of the American Diabetes Association (ADA 2025), Chicago, IL, USA, 20–23 June 2025. [Google Scholar]
- Ascletis Pharma Inc. Ascletis’ Oral Small Molecule GLP-1, ASC30, Demonstrated Placebo-Adjusted Weight Loss of 7.7% with Better Gastrointestinal Tolerability in Its 13-Week U.S. Phase II Study in Participants with Obesity or Overweight. Available online: https://www.ascletis.com/single/145.html (accessed on 17 December 2025).
- Wu, J.J. GLP-1R/GIPR Peptide Agonist ASC31 plus ASC47 Shows Superior Weight Loss Compared with Tirzepatide in Diet-Induced Obese Mice. Proceedings of ObesityWeek®, Atlanta, GA, USA, 2–6 November 2025; p. Poster-139. [Google Scholar]
- Ascletis Pharma Inc. Ascletis Selects a Best-in-Class Once-Monthly Subcutaneously Administered GLP-1R/GIPR Dual Peptide Agonist, ASC35, for Clinical Development. Available online: https://www1.hkexnews.hk/listedco/listconews/sehk/2025/1013/2025101300079.pdf (accessed on 17 December 2025).
- Ascletis Pharma Inc. Ascletis Announces Co-formulation of ASC36, Once-Monthly Next-Generation Amylin Receptor Agonist and ASC35, Once-Monthly Next-Generation GLP-1R/GIPR Dual Agonist for Clinical Development. Available online: https://markets.ft.com/data/announce/detail?dockey=600-202511121830PR_NEWS_USPRX____CN22524-1 (accessed on 17 December 2025).
- Ascletis Pharma Inc. Ascletis Selects a Best-in-Class Once-Monthly Subcutaneously Administered Amylin Receptor Agonist, ASC36, for Clinical Development. Available online: https://www.prnewswire.com/apac/news-releases/ascletis-selects-a-best-in-class-once-monthly-subcutaneously-administered-amylin-receptor-agonist-asc36-for-clinical-development-302598393.html (accessed on 17 December 2025).
- Wu, J.J. ASC47, an Adipose-Targeted, Muscle-Preserving Weight Loss Drug Candidate for Obesity, Demonstrated Significant Weight Loss and Preserved Muscle in Diet-Induced Obese Mice. Abstract 0254; Proceedings of the 32nd European Congress on Obesity (ECO 2025). Malaga, Spain, 11-14 May 2025. [Google Scholar]
- Wu, J.J.; Wu, C. 847-P: ASC47, a Muscle-Preserving Weight Loss Drug Candidate for Obesity, in Combination with Semaglutide, Demonstrated Superior Weight Loss to Semaglutide Monotherapy in a Preclinical Model. Diabetes 2025, 74 Suppl 1, 847–P. [Google Scholar] [CrossRef]
- Ascletis Pharma Inc. Ascletis Announces ASC47 in Combination with Semaglutide Demonstrated Up to 56.2% Greater Relative Reduction in Body Weight in Participants with Obesity Compared to Semaglutide Monotherapy. Available online: https://www1.hkexnews.hk/listedco/listconews/sehk/2025/0922/2025092200091.pdf (accessed on 17 December 2025).
- Therapeutics, Antag. Antag Therapeutics initiates Phase 1a trial of AT-7687, a First-in-Class GIPR Antagonist Designed to Address Key Gaps in Obesity Treatment. Available online: https://www.globenewswire.com/news-release/2025/04/02/3054121/0/en/Antag-Therapeutics-initiates-Phase-1a-trial-of-AT-7687-a-first-in-class-GIPR-antagonist-designed-to-address-key-gaps-in-obesity-treatment.html (accessed on 17 December 2025).
- Drucker, D.J. GLP-1-based therapies for diabetes, obesity and beyond. Nat. Rev. Drug Discov. 2025, 24, 631–650. [Google Scholar] [CrossRef]
- Saldívar-Cerón, H.I.; Vargas-Camacho, J.A.; León-Cabrera, S.; Briseño-Díaz, P.; Castañeda-Ramírez, A.E.; Muciño-Galicia, A.E.; Díaz-Domínguez, M.R. Oral Small-Molecule GLP-1 Receptor Agonists: Mechanistic Insights and Emerging Therapeutic Strategies. Sci. Pharm. 2025, 93, 26. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



