
Submitted:
17 December 2025
Posted:
18 December 2025
You are already at the latest version
Abstract
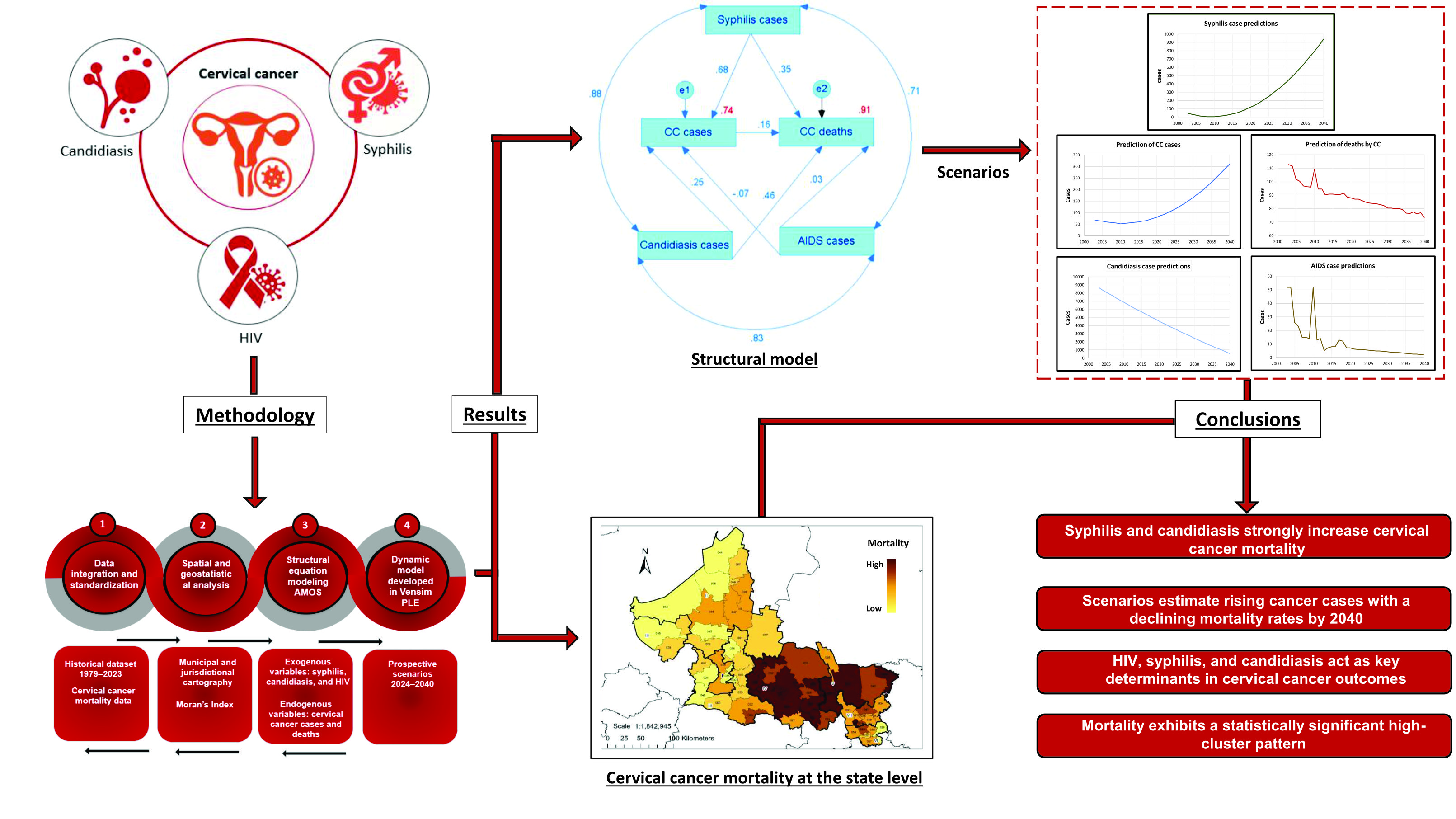
This study analyzes the evolution and spatial distribution of cervical cancer mortality. Furthermore, it develops a dynamic simulation model for estimating the evolution of the disease up to 2040. This manuscript details an ecological and retrospective study that an-alyzed official mortality, morbidity, and population data from the 58 municipalities that constitute the state of San Luis Potosi. We used Moran's index, linear correlation, structur-al equation modeling, Excel predictions, and Vensim simulation software to conduct this study. The evolution of deaths from cervical cancer shows a downward trend; mortality follows a clustered distribution pattern, and it is not random. The struc-tural model showed a correlation coefficient of 0.68 between syphilis cases and cervical cancer cases, with a coefficient of 0.35 for deaths. Candidiasis correlated with cervical cancer at a coeffi-cient of 0.25 and with deaths from the same disease at a coefficient of 0.46. The coefficients of determination for cervical cancer cases and deaths were 0.74 and 0.91, respectively. This shows that these co-infections—syphilis and candidiasis—are a risk factor for cervi-cal cancer mortality. The estimated mortality rates per 100,000 inhab-itants for 2025, 2030, 2035, and 2040 were 5.5, 5.1, 4.8, and 4.4, respectively. The prediction indicates an in-crease in the number of CC cases and deaths from this cause.
Keywords:
cervical cancer
; mortality
; dynamic model
; sexually transmitted infections
; risk factors
1. Introduction
As is well known, cervical cancer (CC) is one of the most prevalent diseases and has one of the highest mortality rates among women, despite the introduction, in 2006, of the vaccine against the Human Papillomavirus (HPV), which is the -causative agent of the disease [1]. Globally, it ranks fourth among cancers diagnosed in women and is the leading cause of death in women in low- and middle-income countries [2]. In 2022, the standardized incidence and mortality rates in Latin America and the Caribbean were 21.9 and 11.1, respectively, per 100,000 women aged between 15 and 85 years old, above those reported for Asia, Europe and Oceania and only below those reported for Africa [3]. In Mexico, in 2024, 5,014 cases of severe cervical dysplasia and CC were recorded in situ, and 4,540 cases of malignant cervical tumors were registered. April 2025, 1,343 and 953 cases were reported, respectively. For the same month in 2024, 1,252 cases of malignant cervical tumors were registered [4]. The above data show that, in this country, there has been no decrease in the number of cases.
Precursor lesions of CC can be eliminated because through timely detection using cervical cytology (PAP smear or cervical cytology) or HPV testing as secondary prevention; they can also be identified and treated via conization in a colposcopy clinic when necessary. It is clear that early diagnosis is vital for any disease, and CC is no exception, since reducing mortality from this disease depends on it [5,6].
The early detection and appropriate treatment of precursor lesions prevent progression to cervical cancer in 80% of cases. This considered, why do so many women die from this disease? From a public health perspective, CC represents a significant problem in de-veloping countries, not only because of its high incidence rate but also because it mainly affects people from the most disadvantaged social classes, who have less access to health services and gynecological care [7].
In Mexico, most cases of cervical cancer are detected in advanced stages, leading to long and very painful terminal illnesses for woman and their families. Effective early de-tection programs have been shown to decrease the occurrence of new cases and mortality from this type of cancer; however, no reduction has occurred in Mexico even though an early detection program based on cytology (PAP) has been implemented for approximate-ly half a century. This is due, as has been said on many occasions, to a lack of highly trained personnel to take samples and interpret cytological studies, a lack of infrastructure required to achieve broad coverage, long waiting times for both the PAP test and the delivery of results, delays in timely care and follow-up of cases, the beliefs of and social barriers against women, and inequality, resulting in high incidence and mortality rates, especially in regions with low socioeconomic development [8,9,10]. In this context, primary prevention through vaccination is the best option in developing countries such as Mexico, a country where the vaccine was introduced in 2008 and where CC is a significant public health problem [11].
It is important to mention that HPV, the causative agent of CC, refers to a group of viruses belonging to the Papillomaviridae family. These can infect the skin or mucous membranes and are mostly transmitted through sexual relations and genital skin-to-skin contact. HPV infection is the most common sexually transmitted infection (STI), in both heterosexual and same-gender relationships.
A total of 90 % of cervical infections are asymptomatic and usually clear up on their own within one to two years without causing lesions; only 5% to 10% of cases lead to pre-neoplastic lesions or cancer, which is due to viral persistence. CC is considered to be the long-term result of an untreated STI caused by certain HPV genotypes [12,13,14].
On the other hand, there are widely described cofactors that favor HPV infection and the development of CC. These are: persistent infection with high-risk oncogenic HPV (viral types 16 and 18), the specific hormonal load of each woman, genetic factors (women with a family history of CC), immunosuppression such as that associated with Human Immunodeficiency Virus (HIV) infection, being a smoker or having a history of smoking, using hormonal contraceptives, high parity, and co-infection with other sexually transmitted infections such as Chlamydia trachomatis, HIV, syphilis, or candidiasis. Other factors include early initiation of sexual activity (before age 18), having or having previously had multiple sexual partners (involving both the woman and her partner); consuming a diet deficient in folates and vitamins A, C, and E; and never having undergone a cytological study [12,15,16] or HPV test.
Taking into account the above, this study was carried out to analyze the evolution, geographic distribution, and prediction of cervical cancer (CC) mortality in the State of San Luis Potosí, Mexico, and to develop a dynamic simulation model to estimate it up to 2040. To achieve this objective, robust trend analysis tools, geographic models, structural and holistic models, and simulation software were used. The importance of the results of studies of this type is that they help those involved in decision-making and the proposal, modification, and implementation of national programs and services offered by the health sector, as well as in understanding the presence of other risk factors.
2. Results
The evolution of mortality rates in 1979-2023 is shown in Figure 1, where we can see that, in 1979, the rate was 4.77, before increasing until peaking at 11.80 in 1990. Since this year, the mortality rate has been decreasing, albeit with fluctuations; for example, in 2023, a rate of 5.4 per 100,000 women was recorded.
The average mortality rate due to CC in the State of San Luis Potosí is presented in Figure 2 a), and we can observe that it has not been distributed homogeneously throughout the state territory, since there are 12 municipalities with very high mortality, whose rates range between 13.56 and 16.42 deaths from CC per 100,000 women.
Tamasopo (036) was the municipality with the highest average CC-related mortality rate in the study period, with a value of 16.42, followed by Rayón (023), with 15.13; Lagunillas (019), with 14.22; Cerritos (008), with 13.76; Ciudad Fernández (011), with 13.56; Rioverde (024), with 13.10; Huehuetlán (018), with 12.73; Alaquines (002), with 15.52; Ciudad Val-les (013), with 12.35; Ébano (016), with 12.08; San Nicolás Tolentino (030), with 11.90; and finally, Tierra Nueva (043), with 10.93. It should be noted that the municipalities with very high CC-related mortality rates are mainly located in Health Jurisdictions (HJs) IV (Ri-overde) and V (Ciudad Valles). On the other hand, the municipality with the lowest aver-age mortality rate between 1979 and 2023 was Vanegas (044), with only 3.95 deaths from CC per 100 thousand women.
The above information is relevant, given that the distribution of mortality due to CC is not random, as when performing a geostatistical analysis using the Moran Index test (Figure 2 b), we found that mortality follows a clustered distribution pattern (Z=5.43, p-value<0.001), with less than 1% probability that this pattern is random.
On the other hand, all relationships between variables were statistically significant and positive, except for those between cases of CC and candidiasis, cases of CC and AIDS, and death from CC and AIDS. The model indicates that, if cases of syphilis increase, cases and deaths from CC increase, as is also true for candidiasis. Syphilis has a standardized regression weight for CC cases of 0.68, whereas, for CC deaths, CC cases and syphilis have standardized regression weights of 0.16 and 0.35, respectively. The coefficients of determination for cases of CC and CC deaths were 0.74 and 0.91, respectively (Figure 3). However, the model does not consider all the factors that can determine CC cases and deaths from the same disease.
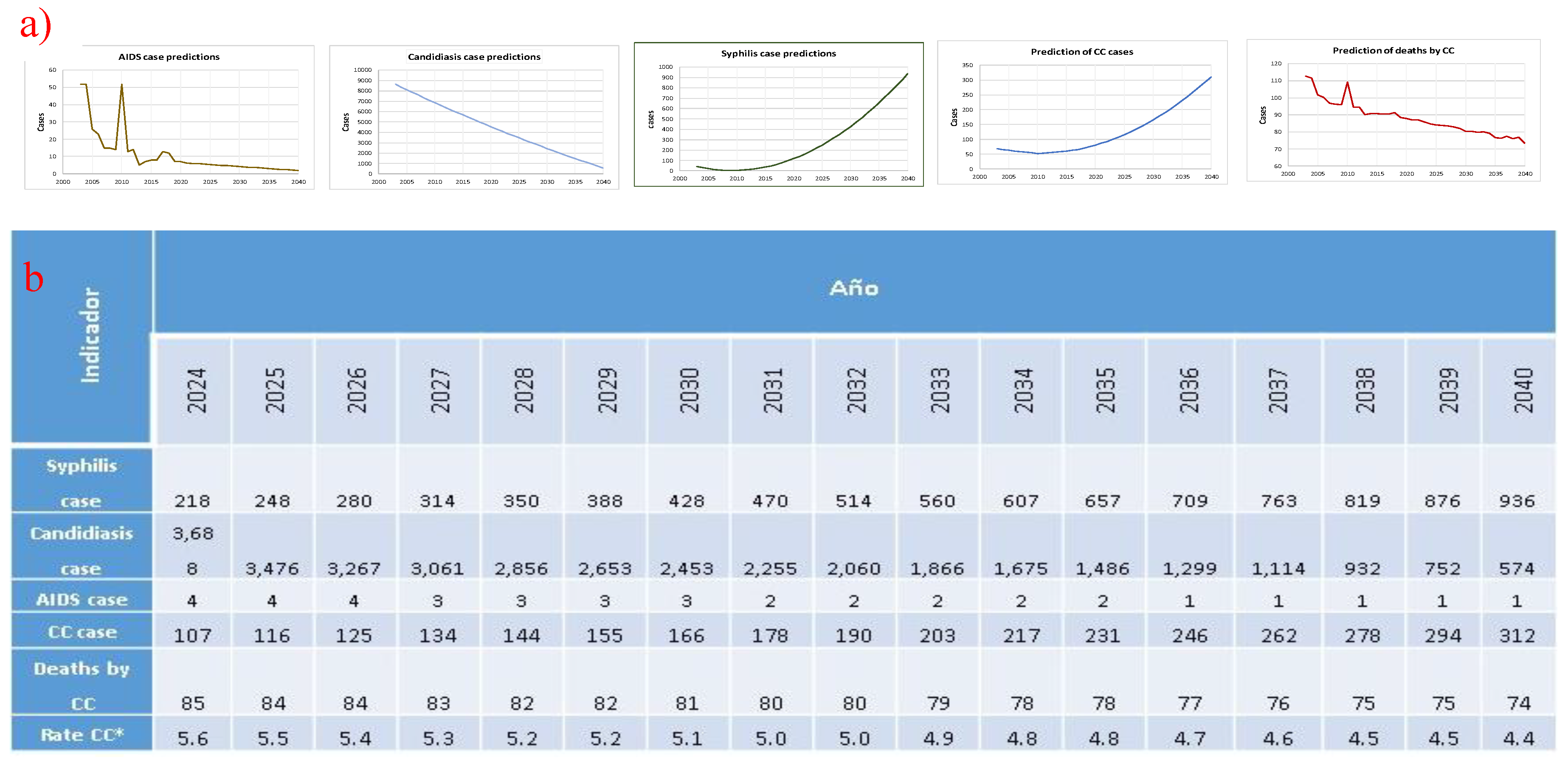
Figure 4 shows a dynamic model used for estimating mortality predictions up to 2040, developed via Vensim. We observed that syphilis cases will more than double in 10 years and almost quadruple in 15 years starting from 2025 (Figure 5a), while CC cases are expected to increase by double to nearly triple in 15 years. However, CC deaths and mortality rates are expected to undergo a sustained decrease (Figure 5b).
3. Discussion
Within the natural history of a disease and for intervention with treatments, there are many different aspects that make it difficult to understand specific prognosis, survival, or mortality within populations; these factors are varied, so understanding them is essential to guide or redirect treatments and, thus, improve patient outcomes, which, for obvious reasons, is reflected in health. This has traditionally been addressed via bivariate analyses, using data from cross-sectional studies, since these are limited to making predictions with baseline values, without considering co-variates and their effects over time [27,28]; hence, we propose to use multivariate dynamic models, which are of great use for planning in both clinical services and at the public health level [29] and whose importance lies in establishing the cost-effectiveness of a treatment, in the prognosis of the mortality or survival of a disease and to identify new risk factors. One study published in 2020 attempted to achieve this goal, taking into account variables of patients suffering from CC, such as age at diagnosis, the stage of the disease, and metastasis, using lymph node invasion as a marker. In their results, the authors establish that the dynamics of mortality rates, according to the model that they proposed, showed a better prognosis at 5 years than the Cox model [28,30].
On the other hand, in 2020, the WHO, through the Cervical Cancer Elimination Modelling Consortium (CCEMC), presented two independent, dynamic, multivariate models whose results highlight the importance of taking immediate action against cervical cancer to reduce related mortality by a third in the next 10 years. The models include HPV infection, cervical carcinogenesis, and screening and treating precancerous and invasive cancer [31].
One limitation of the aforementioned multivariate models is that they do not process the cross-relationships that may exist between factors. The structural model used in this study is robust, allowing for the identification of multiple linear and cross-relationships between factors, as well as the statistical significance of each one [32]. Furthermore, the simultaneous presence of several risk factors has both an additive and a multiplicative effect on the increased risk with respect to each factor considered separately [33].
The highest rates of incidence and mortality from cervical cancer occur in low- and middle-income countries. This reflects significant inequalities stemming from a lack of access to national HPV vaccination programs and cervical cancer screening and treatment services, as well as social and economic determinants [22]. In 2018, it was established that the mortality rate from CC in Latin America and the Caribbean was three times higher than that in North America, highlighting the inequalities in access to and quality of health care in different areas of the Region of the Americas [34]. Indeed, Mexico has the highest mortality rate due to CC of the member countries of the Organization for Economic Cooperation and Development (OECD) [35].
Thus, there is a greater burden from cervical cancer and other gynecological cancers on women living in low- and middle-income countries (LMICs) than in those living in high-income countries. Socioeconomic inequalities and inequalities in access to health services have considerable impacts on cervical cancer mortality [23,36]. Our study found a general decreasing trend in observed mortality rates from cervical cancer, although it has fluctuated. This may be due to HPV vaccination campaigns and health service coverage for early detection. Deaths are expected to decrease by 12.9% by 2040. However, in cases of CC, an upward trend was observed; if a women's living conditions do not improve, an increase of 329.4% is expected by 2020.
Likewise, it was found that the geographical distribution of CC mortality rates is not homogeneous in the studied territory and that this is not random or by coincidence; rather, the 12 municipalities identified as having very high rates are characterized by the following issues: In nine (75%) municipalities, between 18.4%1 and 21.00% of the population has no affiliation to health services, with all nine being above the state average of 16.45%. Of the 12 municipalities mentioned, 5 (41.6%) have an illiteracy rate between 7.55% and 10.94%, above the state average of 6.22%. In addition, in 83.3% of them, the female population is greater than 50%, and in 66.67%, the female population aged between 15 and 49 years old makes up between 47.45% and 51.67% of the overall female population [37]. These characteristics likely influence mortality rates, and as long as inequality is not addressed, the likelihood of eradicating cervical cancer in low-income countries remains diminished.
Although it has already been reported that there is a low prevalence of preneoplastic lesions compared to a high prevalence of microbial infection in the cervix [38], inflammation of the lower genital tract in all women is commonly caused by vaginal infections, whose anatomical proximity implies the infection of the cervix. One of these infections is vaginal candidiasis. In a study conducted in 2014, it was observed that, for 25.4% of women, the presence of Candida in the vagina was the specific cause of inflammation [39]. In other studies addressing the same problem, different percentages of Candida presence are reported [39,40], and although it is argued that the increase in vaginal candidiasis is due to it being an emerging infection considered an opportunistic mycosis, despite the indiscriminate use of antifungals and the increased numbers of both women using hormonal contraceptives and immunocompromised individuals, these research studies do not establish a relationship between infection and the development of preneoplastic lesions of the cervix or cervical cancer, much less establish it as a risk factor for mortality from cervical cancer. However, in our study, we found that vaginal candidiasis has a standardized regression weight on deaths from CC of 0.460, which is statistically significant, meaning that it represents a risk factor for mortality.
The interplay between human microbiota and cancer is increasingly being recognized [41]. For some time now, it has been proposed that microbiome communities play a role in the development, progression, and metastasis, as well as in the response to treatment, of various types of cancer. The genus Candida constitutes a group of opportunistic pathogens present as part of the microbiota of different typographic areas in humans, such as the skin, oropharyngeal cavity, gastrointestinal tract, and genital system [42]. Specifically, the relationship between C. albicans and cancer has been recognized for many years. It is still debated whether this yeast infection is merely a consequence of the cancer or if it actively contributes to its development [43]. Recently, research has suggested that C. albicans may be involved in the development of some types of cancer by increasing host susceptibility through several processes, including inflammation, the stimulation of immune responses mediated by type 17 helper T cells (Th17), the production of compounds with carcinogenic potential, and the ability to mimic the compositions of the molecular structures of human cells [44]. Although the association between C. albicans and varied cancers, such as oral cavity, esophageal, stomach, colorectal, liver, skin and even breast cancer, has been described, as have the potential mechanisms of carcinogenesis by this microorganism [45,46], there is no evidence regarding the relationship and possible involvement of any member of the Candida genus in the development of CC. Population-based studies generally conclude that there is no association between C. albicans and the detection of preneoplastic and neoplastic lesions in cervical cancer [47,48,49]. However, these studies do not consider the impact of using a dynamic model.
Another agent considered a risk factor for the development of CC, and which in our study is shown to be a determinant in the mortality of women experiencing this disease, is HIV. HIV-associated cancers are more severe and cause increased mortality in the infected population due to loss of control of the immune system [50,51]. People infected with HIV are more susceptible to developing cancer than uninfected individuals, and they usually have coinfection with oncoviruses such as Human Herpesvirus 8, Epstein–Barr Virus, Hepatitis B and C Viruses, or HPV [52]. This last causative agent of CC is considered a definitive cancer-causing factor in AIDS, since it is traditionally distinctive in patients with HIV, in whom it is common to observe a drop in the CD4 lymphocyte count, an indicator of the quality of the immune system [53,54]. Thus, HIV infection, coupled with immunosuppression, inflammation, and coinfection with oncogenic viruses, predisposes patients to the development of cancers, such as, in the case at hand, CC [55].
A previous study found that the prevalence of HPV infection is not higher in patients with syphilis, nor does it affect the evolution of preneoplastic lesions of the cervix. The relationship between these factors has been investigated because both infections are sexually transmitted [56]. In another study, it was found that in patients with CC, the prevalence of STIs was higher, with syphilis being present in 7.2% of the studied patients [57]. Studies that explain whether or not there is a relationship have not been conducted, and neither have studies that combine several risk factors. In our study, syphilis was identified as a risk factor, with standardized regression weights of 0.680 and 0.350 for CC cases and deaths; both relationships are statistically significant. This risk factor proved to be the most important, and it is expected that the number of cases will increase by 324% by 2040.
The main limitation of this study is the inclusion of only three sexually transmitted infections, although others, such as herpes, chancre, and lymphogranuloma, were initially considered, but the correlations with cervical cancer cases and deaths were not significant. Furthermore, the model used does not explain 100% of the variation in cervical cancer cases and deaths.
The predictions of the future scenarios produced using the model in our study show a sustained three-time increase in the number of CC cases, rising from 116 in 2025 to 312 in 2040. For mortality rates, a sustained, though very small, decrease is predicted, decreasing from 5.5 to 4.4 per 100,000 women between 2025 and 2040. This considered, in a study conducted in 2025, Li et al. mention that, of the CC cases reported in 2022, 52.67% of patients died from this disease. Their study describes the global demographic projections of the incidence and mortality of CC worldwide for 2030, estimating increases of 14.8% in the number of new cases and 17.8% in mortality.
The authors state that there are marked geographical and socioeconomic disparities, since in countries with a low human development index (HDI), incidence rates were twice as high and mortality rates five times higher than those in countries with a very high HDI. On the other hand, CC was among both the three most frequent cancers and the main causes of cancer death in women between 15 and 44 years old, highlighting the persistence and widening of inequalities at the global level and the need to establish national strategies to reduce the gap and move towards the elimination of cervical cancer, which is the WHO's objective [58,59]. The above is also reflected in countries such as Mexico, where CC is a public health problem.
4. Materials and Methods
2.1. Type of Research Methods and Data Used.
This study was a retrospective ecological study. Secondary databases were used with data from the 58 municipalities making up the State of San Luis Potosí, Mexico, in 1979-2023. The trend was estimated by obtaining data on deaths from cervical cancer for 1979-2011 from the dynamic cubes of the General Directorate of Epidemiology (DGE) [17] and for 2012-2023 from the National Institute of Statistics and Geography (INEG) of Mexico [18]. The population data were obtained from the National Population Council (CONAPO) [19]. Rates were estimated per 100,000 women.
2.2. Spatial Analysis
The modeling of both the average rates of CC deaths for 1979-2023 and their spatial distribution was carried out via ArcMap software version 10.1 using the World Geodetic System (WGS) 1984 coordinate system. To do this, the territorial limits of the State of San Luis Potosí, as well as its 58 individual municipalities, were derived from the state and municipal political division maps of Mexico at a scale of 1:250000 from INEGI; these maps were in Shape File (SHP) format. Cartographic data from the polygonal entities of both the state and the municipalities were extracted and saved in an SHP.
Subsequently, a health administration layer was constructed for the State of San Luis Potosí, specifically for the seven Health Jurisdictions (HJs) comprising the state. Using in-formation from the Unique Health Establishment Code (CLUES) catalog of the Ministry of Health [20], average mortality rates due to chronic cancer were modeled at the municipal level.
Finally, the “Join Data” tool was used to add the average mortality rate data for the municipalities to the attribute table of the previously mentioned municipal territorial boundaries layer. The rate values were represented using colors in 5 categories, classified via the “Natural Breaks (Jenks)” method.
A geostatistical analysis of the average death rates for CC was carried out to deter-mine if there was a clustered, dispersed, or random distribution pattern [21]; in this case, the average rates were analyzed as a numerical attribution of the polygons making up the municipalities of the State of San Luis Potosí.
According to the scientific literature, clinical indicators were considered as direct and indirect risk factors for deaths from congenital heart disease. Based on the factors showing significant correlations in previous analyses, the following indicators were used: For the health services of the State of San Luis Potosí, data on new cases of the following diseases in women in 2003 were obtained: urogenital candidiasis (candidiasis), acquired syphilis (syphilis), acquired immunodeficiency syndrome (AIDS), and malignant tumor of the cer-vix (CC cases). The development of cervical cancer after an HPV infection can take be-tween 10 and 20 years, although in people with weakened immune systems, it can be faster (between 5 and 10 years) [22]; these years were taken into account when developing the dynamic model. Deaths due to CC in 2023 were considered, statistics for which were obtained from data reported by INEGI, since it has been found that average survival is approximately 10 years [23].
Based on these factors, a structural equation model (structural model) was built via AMOS software for analyzing multiple relationships between the included factors. In this model, AIDS, syphilis, and candidiasis were considered explanatory (exogenous) factors, while CC cases and CC deaths were defined as endogenous (dependent) variables. This approach made it possible to evaluate both the direct effects of and the cross-interactions between the factors, offering a comprehensive view of the dynamics influencing the be-havior of CC-related mortality. In this structural model, standardized coefficients were used to express the effects on a common scale of standard deviations, allowing for com-parison of the relative influence of each variable.
2.3. Future Scenario for the Factors Considered.
To identify the trend and project the future evolution of candidiasis and syphilis, historical series from 2003 to 2023 were analyzed, except for AIDS, for which historical se-ries were analyzed from 2004 to 2020.
Regarding the cases of candidiasis and syphilis, the corresponding quadratic regres-sion models were fitted (24) to estimate and project the trends. For analyzing AIDS cases, a decreasing exponential model was applied [25]. Using these equations in Excel, corre-sponding projections up to 2040 were developed, reviewed, and validated for each of the aforementioned factors. Artificial intelligence (AI) tools were used in the process of build-ing the models and generating the projections.
2.4. Prediction of CC Cases and CC Deaths
A dynamic model was developed via Vensim PLE software (https://vensim.com/software/); its configuration was based on the structural model. The standardized coefficients of the structural model were converted to non-standardized values, since it was necessary to express them in the original scale of the data to apply them to real cases. Supported by AI, the converted values were adjusted and two equations were created to estimate the predictions of CC cases and CC deaths:
- (A)
- Cases of CC = 29.8303 + (cases of candidiasis * 0.0035) + (cases of syphilis * 0.299) + (cases of AIDS * −0.07)
- (B)
- Deaths due to CC = −2.21765e+06 + (74344.8 * cases of CC) − (22229.1 * cases of syphilis) + (5204.51 * cases of AIDS) − (260.205 * cases of candidiasis).
The equations were integrated into the dynamic model, as were the predictions made in Excel for syphilis, candidiasis, and AIDS using lookup functions, allowing for their in-tegration into dynamic simulations and the prospective representation of the evolution of each factor for CC cases and deaths [26].
2.5. Statistical Analysis.
For the geostatistical analysis, “Moran’s Index” test was used. This tool measures spatial autocorrelation using both the geographic locations and numerical attributions of different entities. A 95% confidence level was considered, with Z=1.96 and a probability of 0.05. Using AMOS software, a structural equation model was developed to analyze multiple relationships, including the cross-relationships between the endogenous and exogenous variables used.
The models used for predicting the exogenous variables were as follows:
- (A)
- For candidiasis, we used “cases of candidiasis = 1.11209286*(year²) − 4714.17087*(year) + 4,989,396.71”. This model showed a strong match between the real data and the simulated values (R² = 0.923).
- (B)
- For syphilis, we used “syphilis cases = 0.98684211* (year − 2003)² − 12.33721805*(year − 2003) + 41.57857143”, with this model showing an acceptable degree of similarity with respect to the observed series (R² = 0.802).
- (C)
- For AIDS, we used “(t) = 6.1191•e^ (−0.0895 (t − 2020))”, where t represents the year in question.
5. Conclusions
Health authorities in the State of San Luis Potosí, Mexico, as well as those in any country, can rely on this study’s geographical results to design strategies, primarily those from the 12 municipalities with very high mortality rates from CC. Sexually transmitted diseases must be reduced or at least controlled, especially syphilis, as it has been identified as a significant risk factor for cervical cancer cases and deaths, and it is expected to undergo almost exponential growth in the next 15 years.
Strategies should focus on two issues: first, controlling coinfection factors, especially for women infected with HIV, and second, preventing, diagnosing, and controlling cervical cancer. Similarly, establishing relationships between risk factors and CC is extremely important to optimally propose prevention and management strategies; however, researchers must consider that the disease is multifactorial and that the factors present must be analyzed using robust techniques that allow for identifying multiple linear and cross-dependency relationships, as this will achieve the most accurate results. Hence, the importance of structural equation models and dynamic models that allow us to generate future scenarios for both morbidity and mortality from CC is clear.
The structural model showed that CC cases depended on syphilis, candidiasis, and AIDS, while CC deaths depended on both these three diseases and on CC cases themselves.
In a country such as Mexico, vaccination is the best tool to prevent HPV infection in young women and to prevent the development of pre-neoplastic and neoplastic lesions in both adolescents and adults. On the other hand, training in implementing the correct Pap smear technique is a powerful tool in prevention, but it should be remembered that the process for performing cervical cytology allows for evaluating the health status of the vulvovaginal anatomical region and the collection of simple samples that, together with the signs and symptoms, allow for the rapid detection of candidiasis and syphilis; therefore, comprehensively preparing and training the health personnel in charge of taking samples for Pap is essential.
CC in Mexico is a public health problem, whether due to social inequality, economic backwardness, geographical distances acting as a barrier to accessing health services, the limited number of educational campaigns with a cultural focus on both men and women, etc., it is important to think about effective prevention strategies and their immediate application.
Author Contributions
Conceptualizaciti, D.G-H., Y.T-F., O.P-R. and C.D.C-R.; methodology, D.G-H., O.P-R. and C.D.C-R.; validation, D.G-H., O.P-R., C.D.C-R, Y.T-F., S.O.G-E. and. E.G-J.; formal analysis, D.G-H., O.P-R, C.D.C-R. and E.G-J.; investigation, D.G-H. and O.P-R.; resources, S.O.G-E., E.G-J. and Y.T-F.; data curation, D.G-H., O.P-R. and C.D.C-R.; writing—original draft preparation, Y.T-F., D.G-H. and O.P-R.; writing—review and ed-iting, Y.T-F., S.O.G-E. and E.G-J.; Visualization, Y.T-F. and S.O.G-E.; project administra-tion, E.G-J., S.O.G-E. and Y.T-F. All authors have read and agreed to the published version of the manuscript-.
Funding
No external funding.
Informed Consent Statement
This does not apply because the data comes from third-party databases.
Data Availability Statement
The data presented in this study are available on request from the corresponding author (D.G-H). This researcher keeps the original databases and those used in the treatments for generating the models.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CC | Cervical Cancer |
| HPV | Human Papillomavirus |
| STI | Sexually Transmitted Infection |
| HIV | Human Immunodeficiency Virus |
| AIDS | Acquired Immunodeficiency Syndrome |
| DGE | General Directorate of Epidemiology |
| INEG | National Institute of Statistics and Geography |
| CONAPO | National Population Council |
| WGS | World Geodetic System |
| SHP | Shape File |
| HJs | Health Jurisdictions |
| CLUES | Unique Health Establishment Code |
References
- Nazzal Nazal, Omar.; Cuello Fredes, Mauricio. Evolución histórica de las vacunas contra el Virus Papiloma Humano. Revista chilena de obstetricia y ginecología. 2014, 79, 455-458. [CrossRef]
- Hull, R.; Mbele, M.; Makhafola, T.; Hicks, C.; Wang, S-M.; Reis, R.M.; Mehrotra, R.; Mkhize-Kwitshana, Z.; Kibiki, G.; Bates, D.O.; Dlamini, Z. Cervical cancer in low and middleincome countries. Oncol Lett. 2020; 20, 2058–2074. [CrossRef]
- International Agency for Research on Cancer, WHO. Cancer TODAY | IARC - https://gco.iarc.who.int. Data version: Globocan 2022 (version 1.1).
- Secretaría de Salud. Subsecretaría de prevención y promoción de la salud. Dirección General de Epidemiología. Gobierno de México. Boletín Epidemiológico. Sistema Nacional de Vigilancia Epidemiológica. Sistema Único de Información. Semana Epidemiológica. Número 51 / Volumen 41 / Semana 51 / Del 15 al 21 de diciembre del 2024.
- Secretaría de Salud. Subsecretaría de prevención y promoción de la salud. Dirección General de Epidemiología. Gobierno de México. Boletín Epidemiológico. Sistema Nacional de Vigilancia Epidemiológica. Sistema Único de Información. Semana Epidemiológica. Número 15 / Volumen 42 / Semana 15 / Del 6 al 12 de abril del 2025.
- Sarenac, T.; Mikov, M. Cervical cancer, different treatments and importance of bile acids as therapeutic agents in this disease. Front Pharmacol. 2019; 10, 484. [CrossRef]
- Shekhar, S.; Sharma, C.; Thakur, S.; Raina, N. Cervical cancer screening: knowledge, attitude and practices among nursing staff in a tertiary level teaching institution of rural India. Asian Pacific J Cancer Prevent. 2013;14, 3641-3645. [CrossRef]
- Torres-Poveda, K.J.M; Arredondo-López, A.A.; Duarte-Gómez, M.B. La mujer indígena, vulnerable a cáncer cervicouterino: Perspectiva desde modelos conceptuales de salud pública. Salud Tabasco. 2008; 14:807-815. https://biblat.unam.mx/hevila/SaludenTabasco/2008/vol14/no3/5.pdf.
- Instituto Nacional de Salud Pública. Síntesis sobre Políticas de Salud. Prevención y control del cáncer cervical en México. https://insp.mx/assets/documents/webinars/2021/CISP_Cancer_Cervical.pdf.
- Terán-Figueroa, Y.; Muñiz-Carreón, P.; Fernández Moya, M.; Galán-Cuevas, S.; Noyola-Rangel, N.; Gutiérrez-Enríquez, S.O.; Ortiz-Valdez, L.A.; Cruz-Valdez, A. Repercusión del cáncer cervicouterino en pacientes con limitaciones de acceso a los servicios de salud. Ginecol Obstet Mex. 2015; 83:162-172. https://www.medigraphic.com/pdfs/ginobsmex/gom-2015/gom153e.pdf.
- Ochoa Carrillo, F.J. Gaceta Mexicana de Oncología. 2015; 14, 214-221. [CrossRef]
- Secretaría de Salud. Campaña de mitigación del rezago de esquemas de vacunación contra el Virus del Papiloma Humano (VPH), 2023. Lineamientos generales. Programa de vacunación universal. https://www.gob.mx/cms/uploads/attachment/file/852406/LINEAMIENTOS_VACUNA_VPH_2023.pdf.
- de Sanjosé, S.; Brotons, M.; Pavón, M.A. The natural history of human papillomavirus infection. Best Practice & Research Clinical Obstetrics & Gynaecology. 2018; 47, 2– 13. [CrossRef]
- Doorbar, J., Egawa, N.; Griffin, H.; Kranjec, C.; Murakami, I. Human papillomavirus molecular biology and disease association. Rev Med Virol. 2015; 25 S, 2–23. [CrossRef]
- Castellsagué Piqué, X.; de Sanjosé Llongueras, S.; Bosch Jose, F.J. Epidemiología de la infección por VPH y del cáncer de cuello de útero. Nuevas opciones preventivas. En: Carreras Collado R, Xercavins Montosa J y Checa Vizcaíno MA. Virus del Papiloma Human y Cáncer de Cuello de Útero. Madrid, España: Editorial Médica Panamericana; 2007, p. 14 – 17.
- Chesson, H.W.; Dunne, E.F.; Hariri, S.; Markowitz, L.E. The estimated lifetime probability of acquiring human papillomavirus in the United States. Sex Transm Dis. 2014; 41, 660–4. [CrossRef]
- Secretaría de Salud. DGIS. Cubos dinámicos. Defunciones. 2025. http://www.dgis.salud.gob.mx/contenidos/basesdedatos/bdc_defunciones_gobmx.html.
- Instituto Nacional de Geografía y Estadística. Datos abiertos. Registros administrativos- estadísticas. Vitales. Estadísticas de defunciones registradas. https://www.inegi.org.mx/datosabiertos/.
- Gobierno de México. Consejo Nacional de Población. Reconstrucción y proyecciones de la población de los municipios de México 1990-2040. 2024, (https://www.gob.mx/conapo/documentos/reconstruccion-y-proyecciones-de-la-poblacion-de-los-municipios-de-mexico-1990-2040.
- Secretaría de Salud. SSA: DGIS, Histórico de bases CLUES. http://gobi.salud.gob.mx/Bases_Clues.html.
- Environmental Systems Research Institute. ESRI: Cómo funciona Autocorrelación espacial (I de Moran global). https://pro.arcgis.com/es/pro-app/latest/tool-reference/spatial-statistics/h-how-spatial-autocorrelation-moran-s-i-spatial-st.htm.
- Organización Mundial de la Salud. Cáncer de cuello uterino. 17 de noviembre de 2023. https://www.who.int/es/news-room/fact-sheets/detail/cervical-cancer.
- Terán-Figueroa, Y.; García-Díaz, J.; González-Rubio, M.V.; Gaytán-Hernández, D.; Gutiérrez-Enríquez, S.O. Mortalidad y supervivencia por cáncer cervicouterino en beneficiarias del Seguro Popular en el estado de San Luis Potosí, México. Periodo 2005-2012. Acta Universitaria. 2020, 30, e2412. http://doi.org/10.15174.au.2020.2412.
- Obando, J.; Peña, P.; Obando, L.; Franco, A. Importancia de los modelos de regresión no lineales en la interpretación de datos de la COVID-19 en Colombia. Revista Habanera de Ciencias Médicas. 2020, 19 S1. http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1729519X2020000400014&lng=es&tlng.
- Manabe, H.; Manabe, T.; Honda, Y.; Kawade, Y.; Kambayashi, D.; Manabe, Y.; Kudo, K. Simple mathematical model for predicting COVID-19 outbreaks in Japan based on epidemic waves with a cyclical trend. BMC Infect Dis. 2024, 24, 465. [CrossRef]
- Gaytán-Hernández, D.; Díaz-Oviedo, A.; Gallegos-García, V.; Terán-Figueroa, Y. Situación futura de la cardiopatía isquémica en el estado de San Luis Potosí: un modelo dinámico predictivo. Archivos de cardiología de México. 2018, 88, 140-147. [CrossRef]
- Diario Oficial de la Federación, Secretaría de Gobernación, México Norma Oficial Mexicana NOM- 014-SSA-1994, para la prevención, detección, diagnóstico, tratamiento, control y vigilancia epidemiológica del cáncer uterino. 18 de mayo de 2007.
- Scher, H.I.; Solo, K.; Valant, J.; Todd, M.B.; Mehra, M. Prevalence of Prostate Cancer Clinical States and Mortality in the United States: Estimates Using a Dynamic Progression Model. PLoS One. 2015, 13, e0139440. [CrossRef]
- Yang, Z.; Hou, Y.; Lyu, J.; Liu, D.; Chen Z. Dynamic prediction and prognostic analysis of patients with cervical cancer: a landmarking analysis approach. Ann Epidemiol. 2020, 44:45-51. [CrossRef]
- Kasaie, P.; Stewart, C.; Humes, E.; Gerace, L.; Hyle, E.P.; Zalla, L.C.; Rebeiro, P.F.; Silverberg, M.J.; Rubtsova, A.A.; Rich, A.J.; Gebo, K.; Lesko, C.R.; Fojo, A.T.; Lang, R.; Edwards, J.K.; Althoff, K.N. Impact of subgroup-specific heterogeneities and dynamic changes in mortality rates on forecasted population size, deaths, and age distribution of persons receiving antiretroviral treatment in the United States: a computer simulation study. Ann Epidemiol. 2023, 87: S1047-2797. [CrossRef]
- Li, L.; Yang, Z.; Hou, Y.; Chen, Z. Moving beyond the Cox proportional hazards model in survival data analysis: a cervical cancer study. BMJ Open. 2020, 19, e033965. [CrossRef]
- Batista, J.; Coenders, G. Modelos de ecuaciones estructurales. Madrid: La Muralla, 2000.
- González Guzmán, R.; Alcalá Ramírez, J. Enfermedad isquémica del corazón, epi-demiología y prevención. Rev Facultad Med UNAM. 2010, 53, 35-43. https://www.medigraphic.com/pdfs/facmed/un-2010/un105h.pdf.
- Organización Panamericana de la Salud. Cáncer Cervicouterino. Washington: OPS https://www.paho.org/hq/index.php?option=com_content&view=article&id=5420:2018-cervicalcancer&Itemid=3637&lang=es.
- The Global Cancer Observatory. International Agency for Research on Cancer. Mexico Source: Globocan 2020. Ginebra: World Health Organization, 2021. https://gco.iarc.fr/today/data/factsheets/populations/484-mexico-fact-sheets.pdf ).
- Silva Filho, A.L.D.; Romualdo, G.R.; Pinhati, M.E.S.; Neves, G.L.; Oliveira, J.A.; Moretti-Marques, R.; Nogueira-Rodrigues, A.; Tsunoda, A.T.; Cândido, E.B. Exploring cervical cancer mortality in Brazil: an ecological study on socioeconomic and healthcare factors. Int J Gynecol Cancer. 2025, 35,101851. [CrossRef]
- Instituto Nacional de Geografía y Estadística. Datos abiertos. Información Demográfica y Social. Censos y Conteos. Censos y Conteos de Población y Vivienda 2020. https://www.inegi.org.mx/datosabiertos/.
- Canfell, K.; Kim, J.J.; Brisson, M.; Keane, A.; Simms, K.T.; Caruana, M.; Burger, E.A.; Martin, D.; Nguyen, D.T.N.; Bénard, É.; Sy, S.; Regan, C.; Drolet, M.; Gingras, G.; Laprise, J.F.; Torode, J.; Smith, M.A.; Fidarova, E.; Trapani, D.; Bray, F.; Ilbawi, A.; Broutet, N.; Hutubessy, R. Mortality impact of achieving WHO cervical cancer elimination targets: a comparative modelling analysis in 78 low-income and lower-middle-income countries. Lancet. 2020, 22, 591-603. [CrossRef]
- Kanyina, E.W.; Kamau, L.; Muturi, M. Cervical precancerous changes and selected cervical microbial infections, Kiambu County, Kenya, 2014: a cross sectional study. BMC Infect Dis. 2017, 17, 647. [CrossRef]
- Bhojani, K.R.; Garg, R. Cytopathological study of cervical smears and correlation of findings with risk factors. Int J Biol Med Res. 2011, 2, 757–61. https://www.biomedscidirect.com/journalfiles/IJBMRF2011245/cytopathological-study-of-cervical-smears-and-corelation-of-findings-with-risk-factors.pdf.
- Claeys, P.; Gonzalez, C.; Gonzalez, M.; Van Renterghem, L.; Temmerman, M. Prevalence and risk factors of sexually transmitted infections and cervical neoplasia in women’s health clinics in Nicaragua. J Sex Transm Infect. 2002, 78:204–207. [CrossRef]
- Gilbert, J.A.; Blaser, M.J.; Caporaso, J.G.; Jansson, J.K.; Lynch, S.V.; Knight, R. Current understanding of the human microbiome. Nat. Med. 2018, 24, 392–400. [CrossRef]
- Talapko, J.; Juzbaši´c, M.; Matijevi´c, T.; Pustijanac, E.; Beki´c, S.; Kotris, I.; Škrlec, I. Candida albicans-The Virulence Factors and Clinical Manifestations of Infection. J. Fungi. 2021, 7, 79. [CrossRef]
- Cullin, N.; Azevedo Antunes, C.; Straussman, R.; Stein-Thoeringer, C.K.; Elinav, E. Microbiome and cancer. Cancer Cell. 2021, 39, 1317-1341. [CrossRef]
- Yu, D.; Liu, Z. The research progress in the interaction between Candida albicans and cancers. Front. Microbiol. 2022, 13, 988734. [CrossRef]
- Talapko, J.; Meštrović, T.; Dmitrović, B.; Juzbašić, M.; Matijević, T.; Bekić, S.; Erić, S.; Flam, J.; Belić, D.; Petek Erić, A.; Milostić Srb, A.; Škrlec, I. A Putative Role of Candida albicans in Promoting Cancer Development: A Current State of Evidence and Proposed Mechanisms. Microorganisms. 2023. 11, 1476. [CrossRef]
- Wang, X.; Zhang, W.; Wu, W.; Wu, S.; Young, A.; Yan, Z. Is Candida albicans a contributor to cancer? A critical review based on the current evidence. Microbiol Res. 2023, 272:127370. [CrossRef]
- Yang, S.W.; Lee, Y.C.; Lee, Y.S.; Chang, L.C.; Lai, Y.R. Risk assessment of malignant transformation of oral leukoplakia in patients with previous oral squamous cell carcinoma. Int J. Oral. Maxillofac. Surg. 2022, 51, 1394–1400. [CrossRef]
- Engberts, M.K.; Vermeulen, C.F.; Verbruggen, B.S.; van Haaften, M.; Boon, M.E.; Heintz, A.P. Candida and squamous (pre)neoplasia of immigrants and Dutch women as established in population-based cervical screening. Int J Gynecol Cancer. 2006, 16, 1596-600. [CrossRef]
- Engberts, M.K., Verbruggen, B.S., Boon, M.E., van Haaften, M., Heintz, A.P. Candida and dysbacteriosis: a cytologic, population-based study of 100,605 asymptomatic women concerning cervical carcinogenesis. Cancer-Am Cancer Soc. 2007, 111, 269–274. [CrossRef]
- Coghill, A.E.; Shiels, M.S.; Suneja, G.; Engels, E.A. Elevated Cancer-Specific Mortality Among HIV-Infected Patients in the United States. J Clin Oncol. 2015, 33, 2376-83. [CrossRef]
- Robbins, H.A.; Pfeiffer, R.M.; Shiels, M.S.; Li, J.; Hall, H.I.; Engels, E.A. Excess cancers among HIV-infected people in the United States. J Natl Cancer Inst. 2015, 107, dju503. [CrossRef]
- Berretta, M.; Di Francia, R.; Stanzione, B.; Facchini, G.; LLeshi, A.; De Paoli, P.; Spina, M.; Tirelli, U. New treatment strategies for HIV-positive cancer patients undergoing antiblastic chemotherapy. Expert Opin Pharmacother. 2016, 7, 2391-2403. [CrossRef]
- Sabattini, E.; Bacci, F.; Sagramoso, C.; Pileri, S.A. WHO classification of tumours of haematopoietic and lymphoid tissues in 2008: an overview. Pathologica. 2010, 102, 83-7. PMID: 21171509.
- Shmakova, A.; Germini, D.; Vassetzky, Y. HIV-1, HAART and cancer: A complex relationship. Int J Cancer. 2020, 146, 2666-2679. [CrossRef]
- Dias Neto, N.M.; Moura Dias, V.G.N.; Christofolini, D.M. Is syphilis infection a risk factor for cervicovaginal HPV occurrence? A case-control study. J Infect Public Health. 2024, 17, 102472. [CrossRef]
- Abebe, M.; Eshetie, S.; Tessema, B. Prevalence of sexually transmitted infections among cervical cancer suspected women at University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia. BMC Infect Dis. 2021, 21: 378. [CrossRef]
- Li, Z.; Liu, P.; Yin, A.; Zhang, B.; Xu, J.; Chen, Z.; Zhang, Z.; Zhang, Y.; Wang, S.; Tang, L.; Kong, B.; Song, K. Global landscape of cervical cancer incidence and mortality in 2022 and predictions to 2030: The urgent need to address inequalities in cervical cancer. Int J Cancer. 2025, 157(2): 288-297. [CrossRef]
- Organización Mundial de la Salud. Estrategia mundial para acelerar la eliminación del cáncer del cuello uterino como problema de salud pública. 2022. https://iris.who.int/bitstream/handle/10665/359000/9789240039124-spa.pdf?sequence=1.
Figure 1.
Evolution of Cervical Cancer mortality rates in the period 1979-2023 in the State of San Luis Potosí, Mexico.
Figure 1.
Evolution of Cervical Cancer mortality rates in the period 1979-2023 in the State of San Luis Potosí, Mexico.
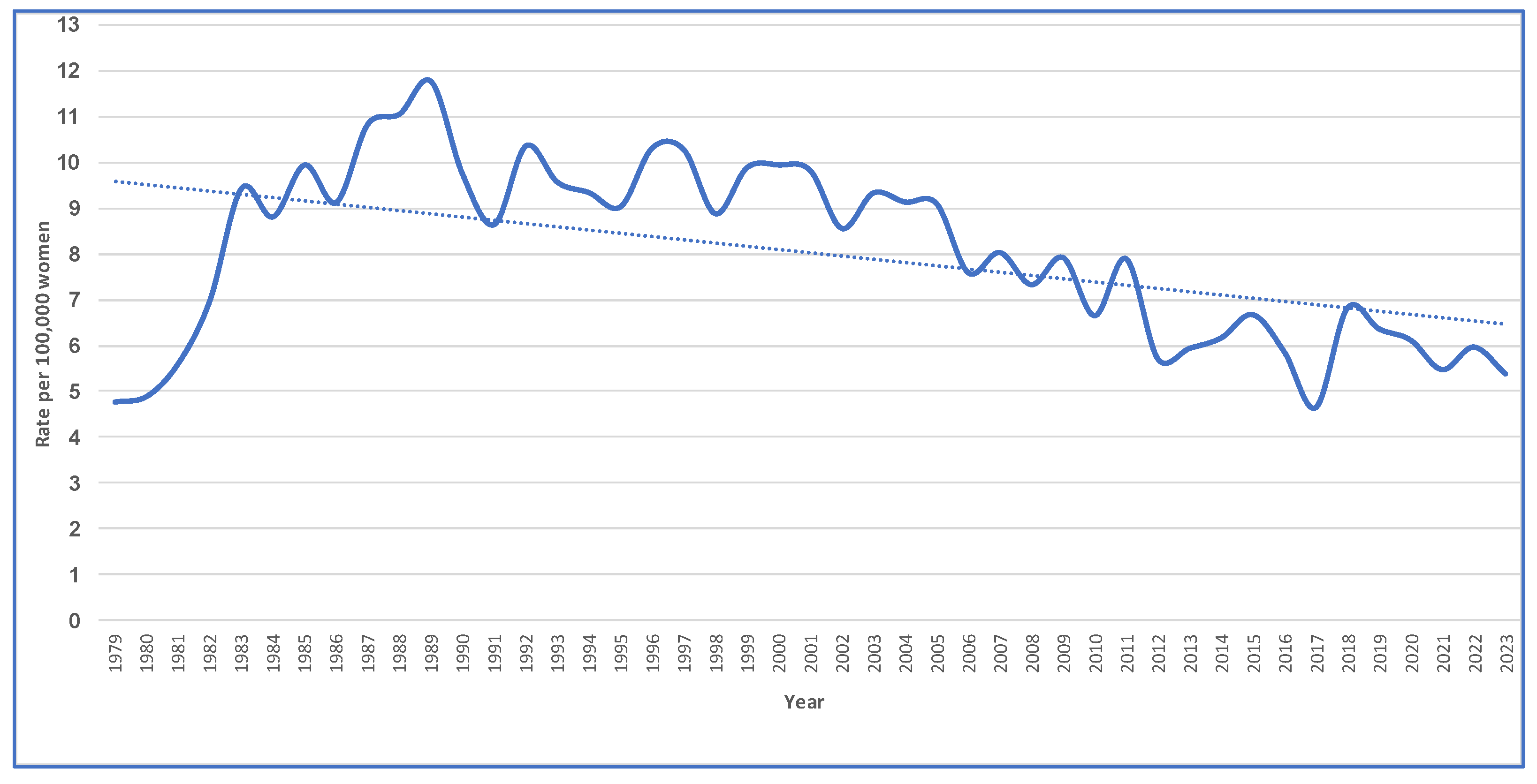
Figure 2.
Geographic distribution of average mortality from cervical cancer in the state of San Luis Potosí, Mexico, during the period 1979-2023. a) Map of State of San Luis Potosí, Mexico; b) Spatial autocorrelation report. Rate per 100,000 women.
Figure 2.
Geographic distribution of average mortality from cervical cancer in the state of San Luis Potosí, Mexico, during the period 1979-2023. a) Map of State of San Luis Potosí, Mexico; b) Spatial autocorrelation report. Rate per 100,000 women.
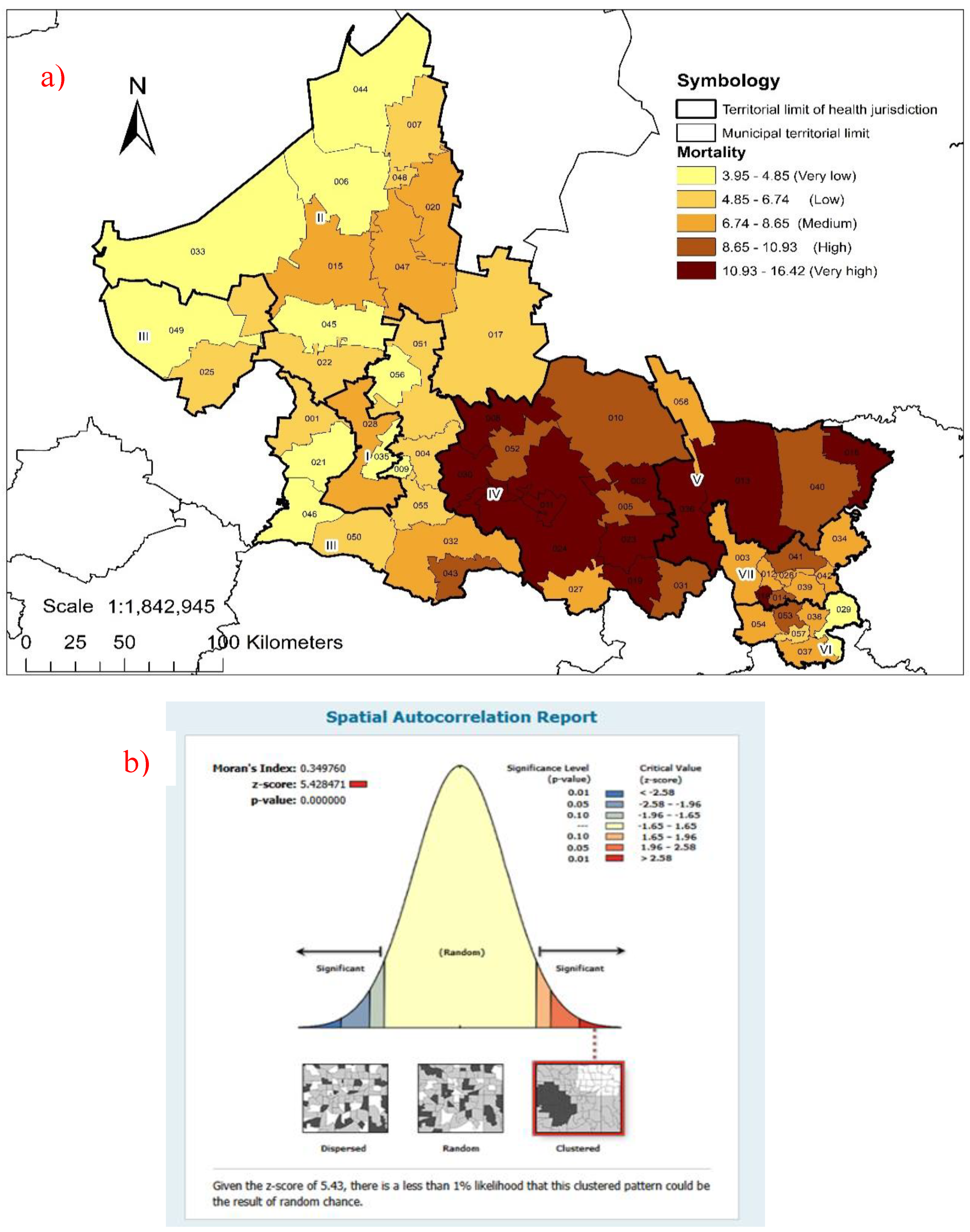
Figure 3.
Structural model of the factors (2003), CC cases (2013) and CC deaths (2023) in the State of San Luis Potosí, Mexico.
Figure 3.
Structural model of the factors (2003), CC cases (2013) and CC deaths (2023) in the State of San Luis Potosí, Mexico.
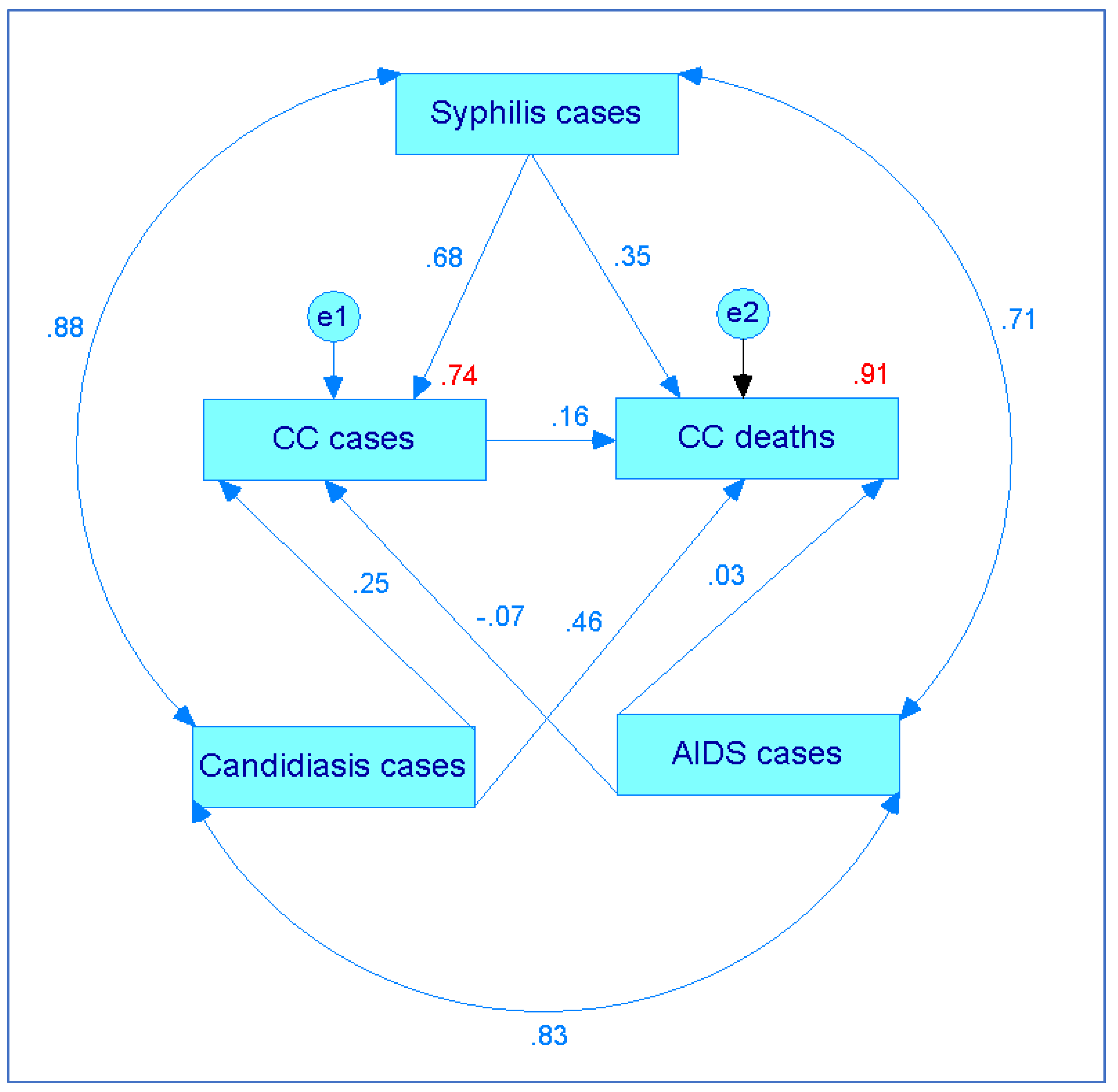
Figure 4.
Dynamic model of the factors (2003), Cervical Cancer cases (2013) and deaths (2023) in the State of San Luis Potosí, Mexico.
Figure 4.
Dynamic model of the factors (2003), Cervical Cancer cases (2013) and deaths (2023) in the State of San Luis Potosí, Mexico.
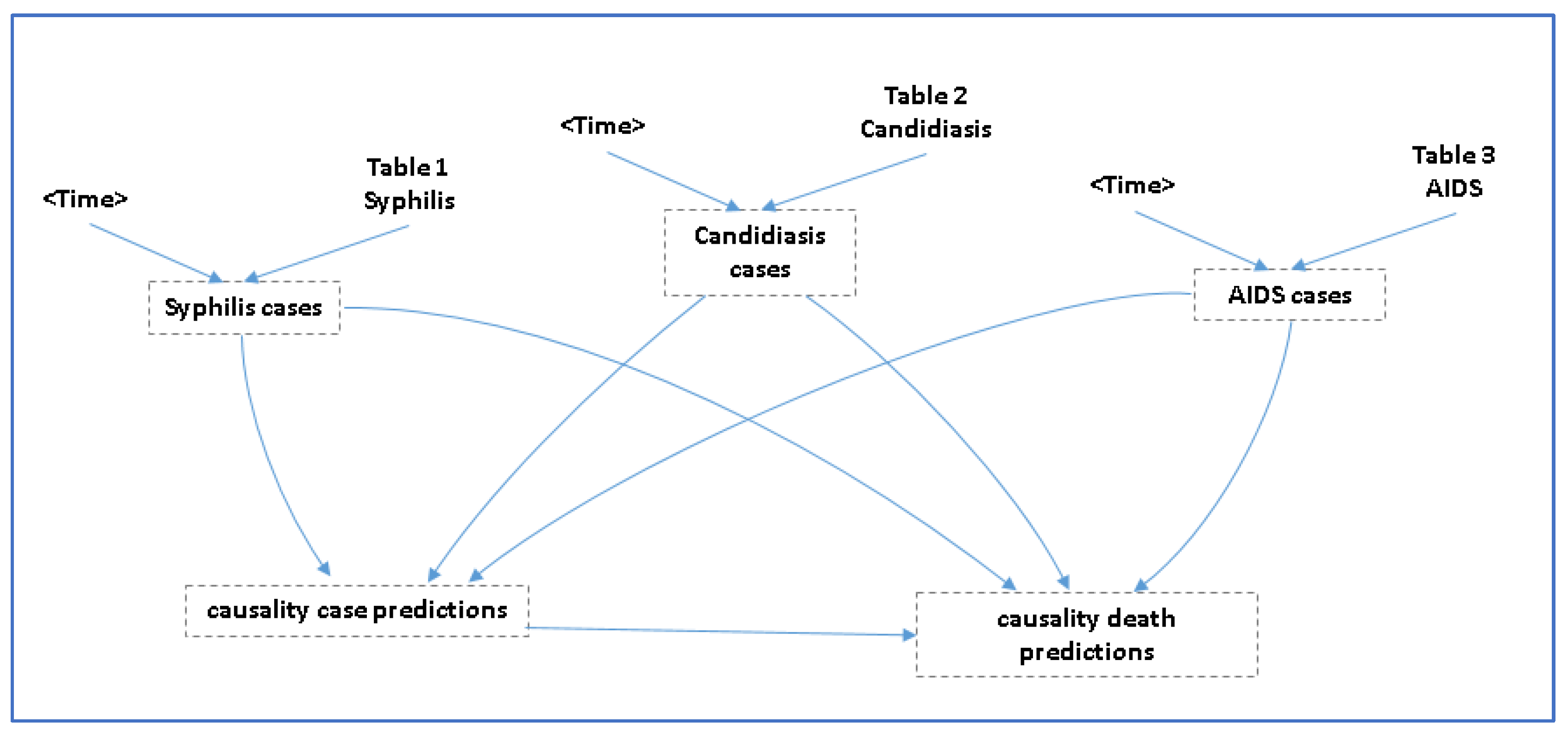
Figure 5.
Predictive values of the analyzed factors, cases of cervical cancer, deaths from cervical cancer, and the mortality rate from cervical cancer in the State of San Luis Potosí, Mexico. Rate per 100,000 women
Figure 5.
Predictive values of the analyzed factors, cases of cervical cancer, deaths from cervical cancer, and the mortality rate from cervical cancer in the State of San Luis Potosí, Mexico. Rate per 100,000 women
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



