1. Introduction
Dementia is a neurodegenerative condition that encompasses many forms of cognitive degeneration that impair an individual’s everyday activities. Such changes include alterations in personality and a decline in memory, problem-solving, and spatial understanding, which impact daily life. Alzheimer’s Disease accounts for 60-80% of dementia cases [
1]. Alzheimer’s symptoms result from the buildup of proteins in the form of amyloid plaques and neurofibrillary tangles in the brain [
2], which cause brain cells to die and the brain to shrink. An individual with the disease has a life expectancy of up to 20 years after diagnosis, depending on when the disease is identified [
3]. Along with the physical manifestations, the financial burden can also take a toll. Annual estimated cost for an individual over 65 years of age, including healthcare and unpaid care, is approximately
$81,000, four times the cost to similarly-aged individuals without the disease [
4]. The caregiver experience has been linked to adverse effects; the most-common reported emotions are sadness, worry, frustration, and difficulty coping [
5].
Research shows physiological risk factors (eg, age, exercise) associated with the development of Alzheimer’s. In addition, mental exercises for cognitive function have been demonstrated to prevent dementia and delay dementia progression [
6], suggesting high-order cognitive exercises (such as attained through higher education) might have a protective effect on developing or progressing with dementia. However, there has yet to be a deep dive into the association between Alzheimer’s mortality, United States geography, socioeconomic status, and educational attainment.
We hypothesized that both income and educational attainment would be negatively correlated with Alzheimer’s mortality rates (eg, higher income and education would be associated with lower Alzheimer’s mortality rates), regardless of geographic region.
2. Material and Methods
Alzheimer’s mortality data between 2021 and 2023 were obtained from the CDC Wonder database, and economic and education data were from the U.S. Census Bureau, both of which are publicly-available, anonymized, and aggregated. We selected two disparate U.S. regions to compare. From the Pacific region, the randomly-selected states were Alaska, California, Hawaii, Oregon, and Washington. From the Southern region, the randomly-selected states were Alabama, Kentucky, Mississippi, and Tennessee.
For Alzheimer’s mortality rates, the CDC Wonder database was queried and filtered by state and region. Rates were listed as deaths from Alzheimer’s Disease per 100,000 population age ≥ 65. For demographic data, from each randomly-selected state, the populations of people aged ≥ 65 years and older were selected from the Census data, and, within this population, the household annual income and educational attainment (percent of population with a bachelor’s degree or higher) were found. To analyze an entire regions’ (Pacific vs. Southern) average income, we multiplied each state in that region’s average household income by that states’ population ≥ 65. The regions’ total state incomes were summed and then divided by the sum of the region’s population ≥ 65. To obtain a region’s weighted education rates, for each state, we multiplied the total population ≥ 65 by the percent of people ≥ 65 with a bachelor’s degree or above; we added those numbers and divided by the region’s total population ≥ 65.
Multiple linear regression was used to determine the association between Alzheimer’s mortality and: 1) geography (Pacific vs. Southern), 2) income, and 3) education level.
Microsoft Excel (Redmond, WA; 2021) was utilized for data management. Statistical significance was set as a priority at p < 0.05.
This research was reviewed and deemed not to meet the definition of research by the Northwell Health Institutional Review Board’s (IRB’s) Human Research Protection Program (HSRD24-0133), indicating that formal IRB approval was not required for this study. All observations were collected in compliance with institutional guidelines for patient privacy and data security.
3. Results
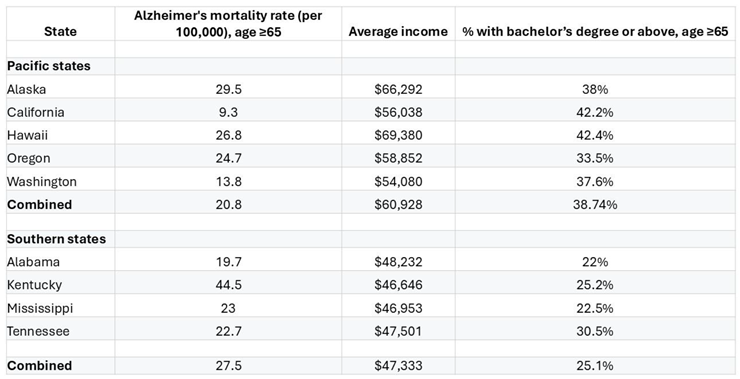
Table 1 shows the associations (among those age ≥ 65) between each state’s Alzheimer’s mortality rate, average income, and educational attainment, grouped by region. Multiple linear regression analysis was performed to clarify the association between region, income, and Alzheimer’s mortality for persons age ≥ 65 (
Table 2).
Table 1.
Alzheimer’s mortality rate, income, education, Pacific vs. South states.
Table 1.
Alzheimer’s mortality rate, income, education, Pacific vs. South states.
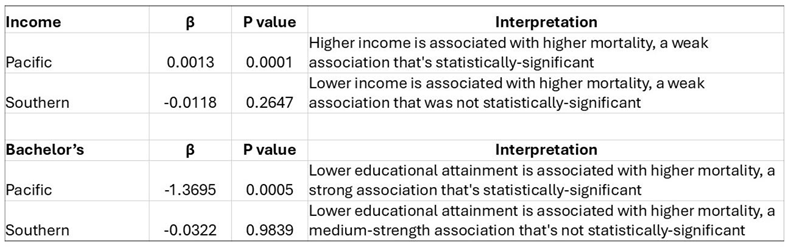
Table 2.
Linear regression analysis of Alzheimer’s mortality, income, and bachelors, by region of states.
Table 2.
Linear regression analysis of Alzheimer’s mortality, income, and bachelors, by region of states.
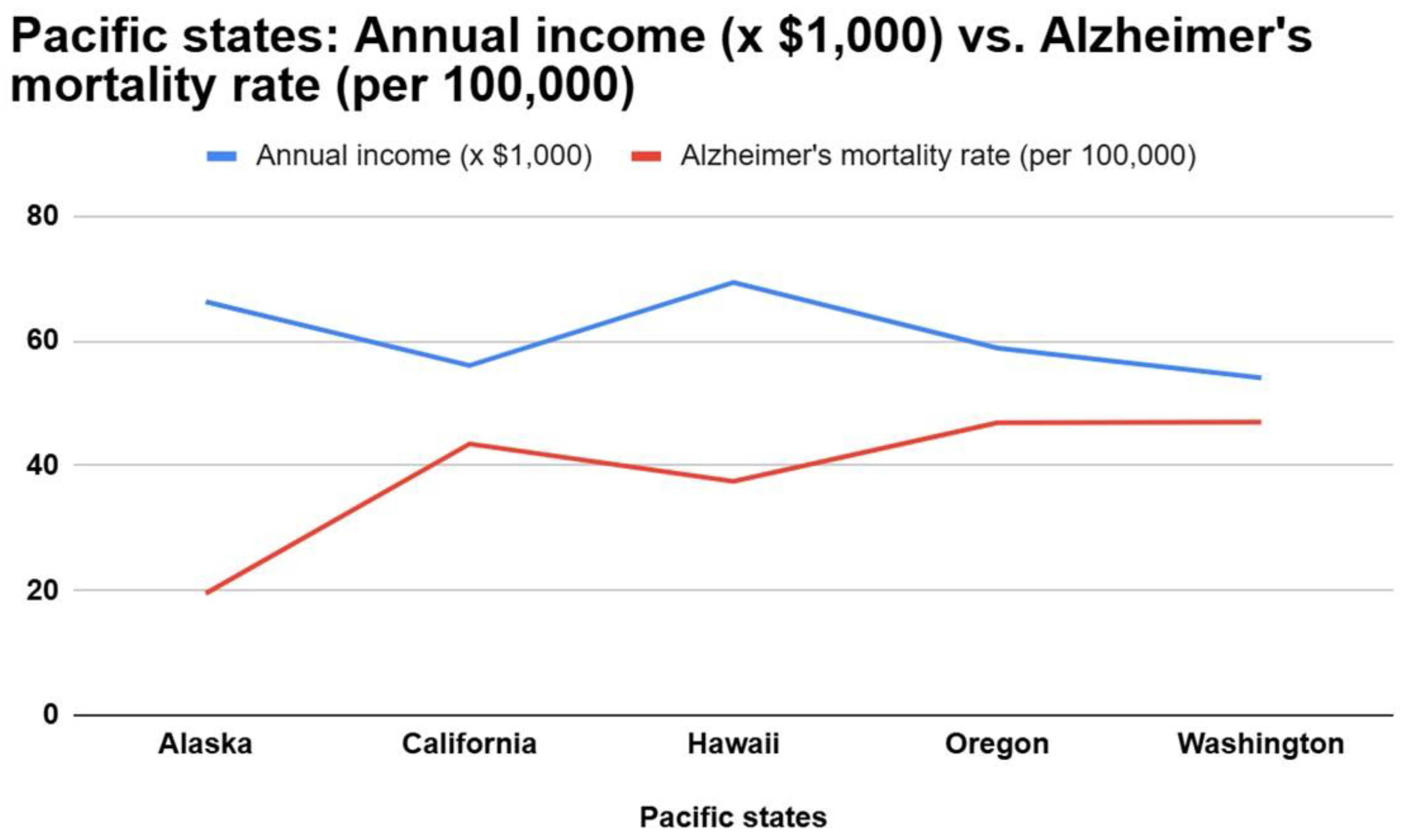
Regarding the association between income and Alzheimer’s mortality for persons age ≥ 65: among the Pacific states, there was a slight positive correlation (i.e., higher income associated with higher mortality), inconsistent with our hypothesis. This was a very weak association (β = 0.0013) that was statistically-significant (p = 0.0001) (
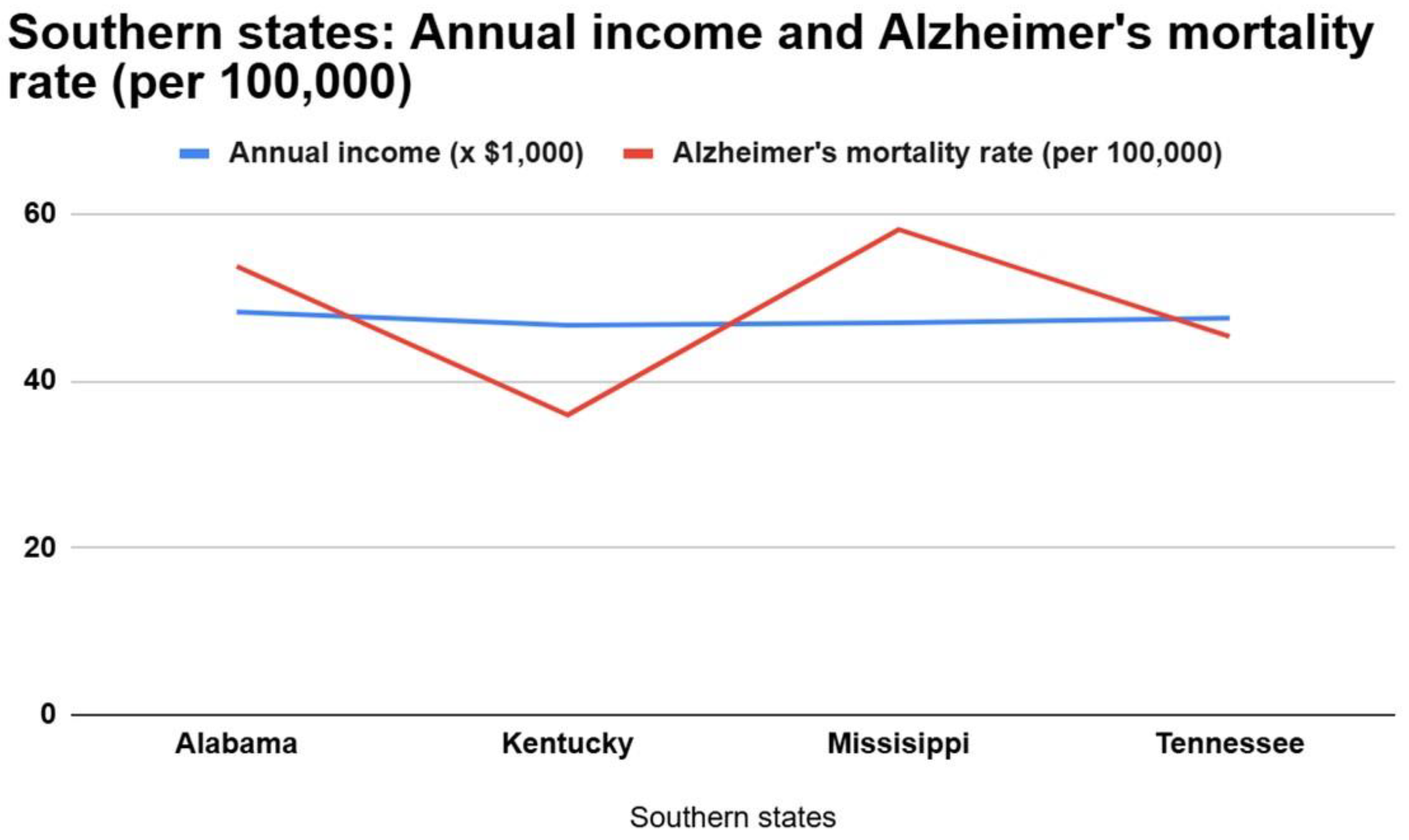
Figure 1). Among Southern states, there was a slight negative correlation (i.e., a higher income associated with lower mortality), concordant with our hypothesis. This was a weak association (β = -0.0118) that was not statistically-significant (p = 0.2647). (
Figure 2)
Figure 1.
Pacific states—Annual income (× $1,000) vs. Alzheimer’s mortality rate (per 100,000).
Figure 1.
Pacific states—Annual income (× $1,000) vs. Alzheimer’s mortality rate (per 100,000).
Figure 2.
Southern states—Annual income (× $1,000) vs. Alzheimer’s mortality rate (per 100,000).
Figure 2.
Southern states—Annual income (× $1,000) vs. Alzheimer’s mortality rate (per 100,000).
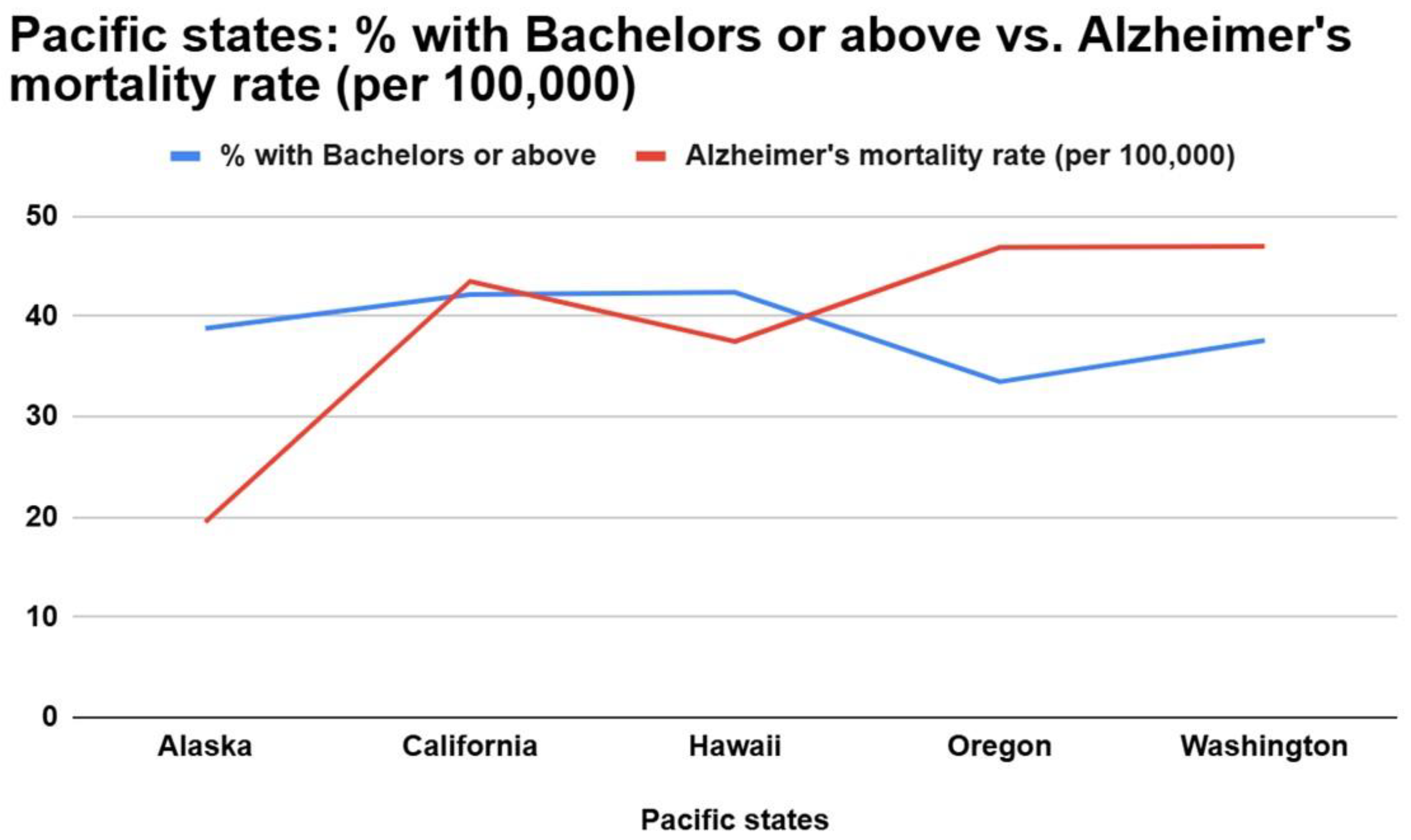
Regarding the association between educational attainment and Alzheimer’s mortality for persons age ≥ 65: among the Pacific states, there was a negative association between educational attainment and Alzheimer’s mortality (i.e., higher education associated with lower mortality), concordant with our hypothesis. This was a moderate association (β = -1.3695) that was statistically-significant (p = 0.0005). (
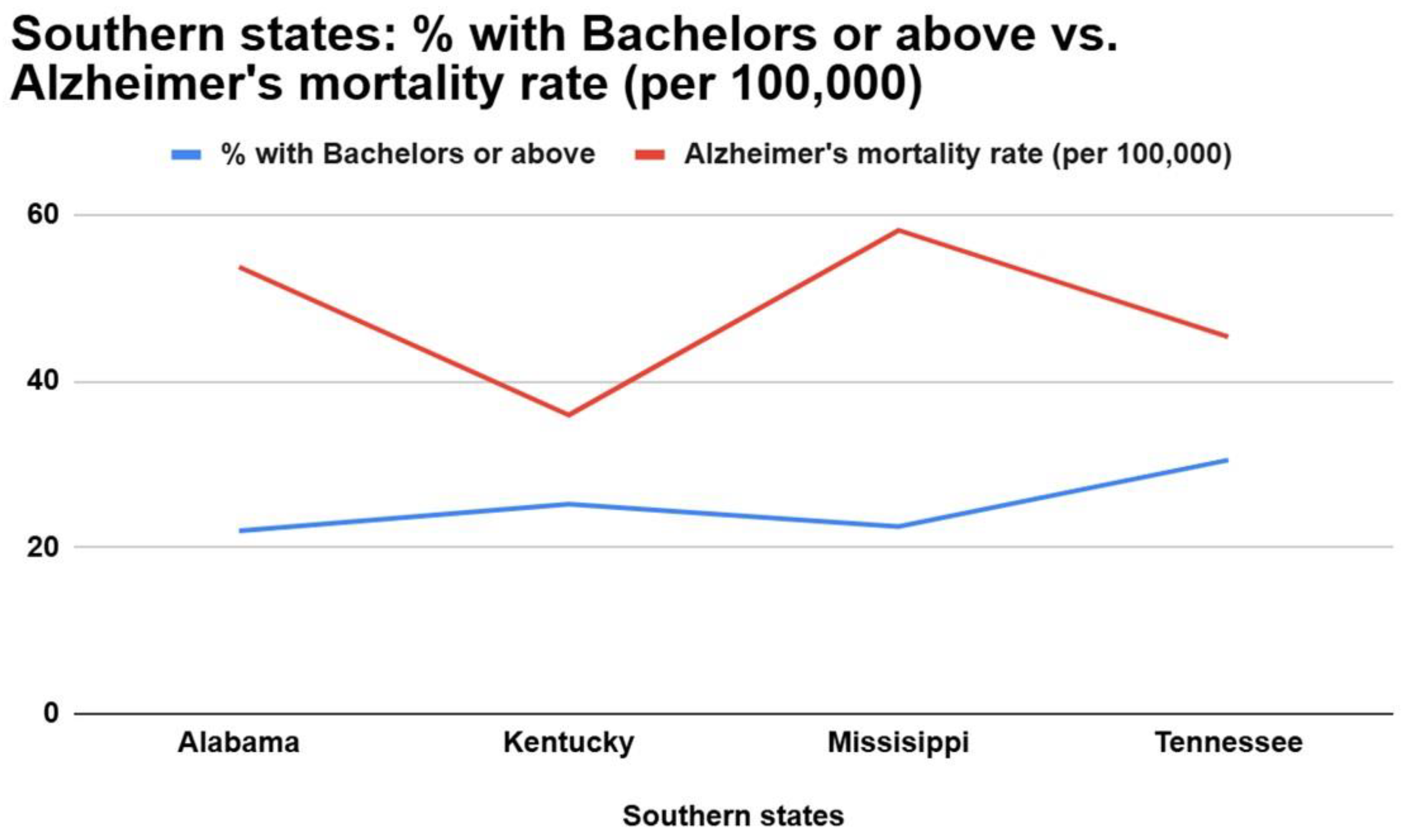
Figure 3) Among the Southern states, a negative correlation (i.e., higher education associated with lower mortality) was observed, consistent with our hypothesis. This was a weak association (β = -0.0322) that was not statistically-significant (p = 0.9839) (
Figure 4).
Figure 3.
Pacific states—Education vs. Alzheimer’s mortality rate (per 100,000).
Figure 3.
Pacific states—Education vs. Alzheimer’s mortality rate (per 100,000).
Figure 4.
Southern states—Education vs. Alzheimer’s mortality rate (per 100,000).
Figure 4.
Southern states—Education vs. Alzheimer’s mortality rate (per 100,000).
4. Discussion
Overall, our data was consistent with our hypothesis that both income and educational attainment would be negatively correlated with Alzheimer’s mortality rates (i.e., higher income and education would be associated with lower Alzheimer’s mortality rates). While, among Pacific states, there was a slight positive correlation between income and Alzheimer’s mortality (i.e., higher income associated with higher mortality), inconsistent with our hypothesis, this was only a very weak association (β = 0.0013).
The positive, but weak, correlation found between Pacific states and income and Alzheimer’s mortality crude rate could be due to several possible contributing factors. The Pacific data sets include Hawaii and Alaska, which are not connected to the contiguous United States, and also, on average, have higher incomes compared to other mainland states [
7]. This is due to several factors, such as Hawaii’s strong tourism industry and a higher cost of living, leading to a correlation of people with higher income being able to afford living in Hawaii, driving up the average income [
8]. Alaska’s higher income can be attributed to similar factors, such as higher costs of living and a higher distribution of wealth due to oil reserves found in Alaska and people receiving universal, passive income, such as permanent fund dividends (PFD) [
9]. Additional confounders might be persons with lower income having less access to healthcare, leading to fewer reported deaths or inaccurately-reported cause of deaths [
10].
Limitations
This study has several limitations. First, comparing only (randomly-selected) Pacific vs. Southern states’ data could have skewed data results. Had we included a greater sampling of states, results may have been different. Another limitation is the number of years (2021-2023) in the analysis; we chose these because they were expediently available in the CDC Wonder database, whereas other years were not. Another possible confounding variable is exposure to the natural environment; this varies greatly by state and is associated with greater cognitive function, but we were unable to explore exposure to the natural environment at the individual level [
11]. Additionally, we focused only on senile dementia (≥65-years-old), and were unable to adjust for gender differences; this may have been important, as there are significant gender discrepancies in Alzheimer’s prevalence among persons ≥65 (1 in 6 women vs. 1 in 11 men) [
12]. Finally, this multivariate analysis only considered 3 variables: state location, income, and education level.
Our results are consistent with previous findings, though none compared specific geographic regions within the United States. Many Alzheimer’s risk factors have been identified. In one study, midlife obesity, physical inactivity, and low education were found to be the most-prominent [
13]. The low education risk factor has also been correlated to Alzheimer’s mortality, such as in a 2018 retrospective Slovakian observational study comparing the Alzheimer’s mortality and socioeconomic factors, Gross Domestic Product, wage, and education [
14]. A 2023 prospective cohort study compared level of socioeconomic status (SES), lifestyle, and incidence of dementia found that participants with higher SES and with a mostly-healthy lifestyle had a significantly-lower risk of incident dementia, Alzheimer’s disease, and vascular dementia compared to participants of lower SES and less-healthy lifestyle [
15]. A retrospective cross-sectional analysis from 2020 using the brains of deceased Alzheimer’s dementia patients found a 2.18 times increase between brains of persons from disadvantaged neighborhoods compared to the rest of the sampled donated brains [
16]. Such literature helped point us in the direction of this study as well as suggest future questions.
References
- Alzheimer’s Association. Available online: https://www.alz.org/alzheimers-dementia/difference-between-dementia-and-alzheimer-s (accessed on 22 November 2025).
- Mayo Clinic: Alzheimer’s Disease. Available online: https://www.mayoclinic.org/diseases-conditions/alzheimers-disease/symptoms-causes/syc-20350447 (accessed on 22 November 2025).
- Alzheimer’s Association. Available online: https://www.alz.org/getmedia/ef8f48f9-ad36-48ea-87f9-b74034635c1e/alzheimers-facts-and-figures.pdf (accessed on 22 November 2025).
- Zissimopoulos, J.; Crimmins, E.; St Clair, P. The Value of Delaying Alzheimer’s Disease Onset. Forum Health Econ. Policy 2014, 18, 25–39. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vellone, E.; Piras, G.; Talucci, C.; Cohen, M.Z. Quality of life for caregivers of people with Alzheimer’s disease. J. Adv. Nurs. 2008, 61, 222–231. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, R. Mental exercises for cognitive function: Clinical evidence. J. Prev. Med. Public Health 2013, 46, S22–S27. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- World Population Review. Available online: https://worldpopulationreview.com/state-rankings/average-income-by-state (accessed on 22 November 2025).
- United States Census Bureau. Available online: https://data.census.gov/map/010XX00US$0400000/ACSST1Y2024/S1902?t=Income+and+Poverty&layer=VT_2024_040_00_PP_D1&loc=35.3334,-121.0782,z1.2860 (accessed on 22 November 2025).
- International Forum of Sovereign Wealth Funds. Available online: https://ifswf.org/members/usa (accessed on 22 November 2025).
- McMaughan, D.J.; Oloruntoba, O.; Smith, M.L. Socioeconomic Status and Access to Healthcare: Interrelated Drivers for Healthy Aging. Front. Public Health 2020, 8, 231. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- National Institute on Aging. Available online: https://www.nia.nih.gov/news/exposure-green-space-may-boost-cognitive-health (accessed on 22 November 2025).
- Pacific Neuroscience Institute. Available online: https://www.pacificneuroscienceinstitute.org/blog/alzheimers-disease/alzheimers-disease-in-women/ (accessed on 22 November 2025).
- Nianogo, R.A.; Rosenwohl-Mack, A.; Yaffe, K.; Carrasco, A.; Hoffmann, C.M.; Barnes, D.E. Risk Factors Associated With Alzheimer Disease and Related Dementias by Sex and Race and Ethnicity in the US. JAMA Neurol. 2022, 79, 584–591. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tóth, P.; Gavurová, B.; Barták, M. Alzheimer’s Disease Mortality according to Socioeconomic Factors: Country Study. Int. J. Alzheimers Dis. 2018, 2018, 8137464. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ou, Y.N.; Zhang, Y.B.; Li, Y.Z.; Huang, S.Y.; Zhang, W.; Deng, Y.T.; Wu, B.S.; Tan, L.; Dong, Q.; Pan, A.; et al. Socioeconomic status, lifestyle and risk of incident dementia: A prospective cohort study of 276730 participants. Geroscience 2024, 46, 2265–2279. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Powell, W.R.; Buckingham, W.R.; Larson, J.L.; Vilen, L.; Yu, M.; Salamat, M.S.; Bendlin, B.B.; Rissman, R.A.; Kind, A.J.H. Association of Neighborhood-Level Disadvantage With Alzheimer Disease Neuropathology. JAMA Netw. Open 2020, 3, e207559. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).