Submitted:
12 December 2025
Posted:
15 December 2025
You are already at the latest version
Abstract
Deep brain stimulation (DBS) is increasingly understood as a precision neuromodulation therapy capable of influencing distributed basal ganglia–thalamo–cortical and cerebellothalamic net-works. Although its symptomatic benefits in Parkinson’s disease, essential tremor, and dystonia are well established, the extent to which DBS supports motor learning, adaptive plasticity, and participation in rehabilitation remains insufficiently defined. Traditional interpretations of DBS as a focal or lesion-like intervention are being challenged by electrophysiological and imaging evidence demonstrating multiscale modulation of circuit dynamics. DBS may enhance rehabilitation outcomes by stabilizing pathological oscillations and reducing moment-to-moment variability in motor performance—conditions that enable consistent task ex-ecution and more effective physiotherapy, occupational therapy, and speech–language interven-tions. Yet this potential is not fully realized in clinical practice due to interindividual variability, incomplete mechanistic understanding, and the limited specificity of current connectomic bi-omarkers for predicting functional gains. Technological advances such as tractography-guided targeting, directional leads, sensing-enabled devices, and adaptive stimulation are expanding opportunities to align neuromodulation with individualized circuit dysfunction. Despite these developments, major conceptual and empirical gaps persist. Few studies directly examine how stimulation-induced changes in neural stability interact with structured rehabilita-tion to promote long-term functional recovery. Heterogeneity in therapeutic response and rehabil-itation access further complicates interpretation of outcomes. Clarifying these relationships is es-sential for developing precision frameworks that integrate DBS with rehabilitative strategies. This review synthesizes mechanistic, imaging, and technological evidence to outline a net-work-informed perspective of DBS as a potential facilitator of rehabilitation-driven functional improvement and identifies priorities for future research aimed at optimizing durable functional restoration.
Keywords:
deep brain stimulation
; connectomics
; movement disorders
; Parkinson’s disease
; essential tremor
; dystonia
; adaptive neuromodulation
; rehabilitation
; tractography
; sensing-enabled DBS
1. Introduction
Essential tremor (ET), Parkinson’s disease (PD), and dystonia are the most prevalent chronic movement disorders and major contributors to long-term motor disability worldwide [1,2,3,4]. Their global prevalence continues to rise, driven largely by population ageing and increased life expectancy, underscoring the need for therapeutic strategies that sustain long-term functional independence [5,6,7]. This growing burden highlights the limitations of purely symptomatic approaches and reinforces the importance of interventions that not only control motor features but also enhance functional capacity and participation in daily life.
Deep brain stimulation (DBS) has become the most effective neurosurgical therapy for medication-refractory movement disorders, marking a transition from irreversible ablative procedures to reversible and adjustable neuromodulation [8,9,10,11]. Early interpretations framed DBS as a “functional lesion,” reflecting its ability to suppress pathological activity within targeted nuclei [12,13]. However, accumulating electrophysiological, neurochemical, and imaging evidence has reframed DBS as a network-level intervention, acting through modulation of distributed motor circuits rather than by focal suppression at the stimulation site [14,15,16,17]. Recent advances in connectomics have further highlighted the limitations of classical nucleus-centric models, showing that DBS outcomes are shaped not solely by electrode proximity to anatomical targets but by the broader patterns of circuit engagement and network reorganization enabled through stimulation [18,19,20]. This shift from anatomical to systems-based reasoning challenges traditional assumptions about target selection, mechanisms of action, and the therapeutic reach of DBS.
Despite these mechanistic and technological advances, DBS remains underutilized as a partner to structured rehabilitation, even though neuromodulation can provide a stable physiological substrate for task-specific training, motor learning, and long-term skill acquisition [21,22,23]. By stabilizing motor fluctuations and reducing performance variability, DBS may enable patients to participate more effectively in physiotherapy, occupational therapy, and speech–language interventions. Viewed in this context, DBS acts as a rehabilitation amplifier, creating neural conditions under which plasticity can be harnessed to promote durable functional restoration.
The purpose of this review is to synthesize mechanistic concepts, imaging frameworks, and technological innovations that support a precision, network-based integration of DBS with multidisciplinary rehabilitation. We outline the evolution from lesion-based and nucleus-centric models to modern connectomic paradigms; examine phenotypic and circuit-level heterogeneity; and discuss how DBS, when combined with structured rehabilitation, can optimize motor performance, functional independence, and long-term outcomes in movement disorders.
2. Materials and Methods
Literature Search Strategy and Scope of the Review
This review synthesizes mechanistic, imaging, technological, and clinical evidence relevant to the interaction between DBS and rehabilitation. Literature was identified through searches in PubMed, Scopus, and Web of Science up to December 2025 using combinations of the terms “deep brain stimulation,” “motor learning,” “plasticity,” “connectomics,” “rehabilitation,” “adaptive DBS,” “tractography-guided targeting,” and disorder-specific terms including “Parkinson’s disease,” “essential tremor,” and “dystonia.” Reference lists of key publications were examined to supplement database searches.
No language or date restrictions were applied, although priority was given to mechanistic, imaging, and clinically relevant studies published within the last decade alongside foundational historical work. As this is a conceptual narrative review, no systematic screening, risk-of-bias assessment, or meta-analysis was performed. Studies were selected for relevance to (i) multiscale DBS mechanisms; (ii) imaging supporting circuit-level targeting; (iii) technological innovations in neuromodulation; and (iv) rehabilitation approaches intersecting with DBS.
This review is based solely on previously published studies and does not involve any new research with human participants or animals.
3. Integrated Framework for Network-Level DBS Mechanisms and Clinical Translation
3.1. Epidemiology and Global Burden of Movement Disorders
ET, PD, and dystonia are among the most common chronic movement disorders and together represent substantial long-term sources of disability (Figure 1). ET affects approximately 4–5% of adults over 65 years of age, underscoring its significant public-health impact in ageing populations [1]. The global prevalence of PD is projected to surpass 12 million by 2040, largely driven by demographic ageing and increased life expectancy [2]. Dystonia represents the third most frequent movement disorder encountered in tertiary care, encompassing focal, segmental, generalized, and genetic forms with heterogeneous clinical trajectories [3,4]. Although considerably less prevalent, rare and highly disabling dystonic phenotypes continue to be reported, and emerging case-based evidence demonstrates that DBS can restore meaningful functional capacity even in exceptional or atypical presentations [24,25].
Beyond their cardinal motor manifestations, these conditions impose substantial functional, psychosocial, and socioeconomic burdens. Global modelling indicates a sustained rise in PD-associated disability, reflecting both increased prevalence and progression-related morbidity [5,6,7]. ET, long mischaracterized as a benign disorder, is now recognized as a major contributor to functional dependence, reduced quality of life, and increased healthcare utilization [26]. Although less frequently quantified in burden-of-disease frameworks, dystonia also contributes significantly to disability-adjusted life years, chronic pain, vocational limitations, and long-term care needs [27].
These epidemiological trends emphasize the need for therapeutic strategies that move beyond symptom suppression to restore functional capacity and support sustained independence. When embedded within structured rehabilitation paradigms, DBS offers an opportunity to modulate pathological networks and enhance adaptive plasticity, thereby promoting more durable improvements in daily functioning.
3.2. Historical Evolution of DBS Concepts
3.2.1. From Lesion-Based Surgery to Reversible Neuromodulation
The development of DBS marked a major shift from irreversible ablative procedures toward adjustable neuromodulation (Figure 2). Lesioning techniques such as thalamotomy and pallidotomy demonstrated that interrupting aberrant basal ganglia signaling could reduce tremor, rigidity, and dyskinesias, but concerns regarding irreversibility and adverse effects limited their widespread use [10,11].
The introduction of high-frequency stimulation by Benabid and colleagues in the late 1980s was transformative. Ventral intermediate nucleus (VIM) stimulation reproduced the therapeutic effects of lesions while preserving reversibility and allowing postoperative titration [8,28]. This approach rapidly expanded to Parkinson’s disease (PD), establishing DBS as a viable alternative to lesioning [9].
Early mechanistic interpretations framed DBS as a “functional” or “adjustable lesion,” reflecting its capacity to suppress pathological activity within targeted nuclei [12,13]. Subsequent electrophysiological evidence, however, demonstrated that high-frequency stimulation does not simply silence local neuronal activity. Instead, it imposes a structured exogenous drive that disrupts pathological oscillatory dynamics [14]. This transition from a lesion-based to a network-based explanatory model began to suggest that clinical benefits extend beyond focal inhibition.
3.2.2. Nucleus-Centric DBS and Emerging Complexity
Classical DBS strategies aligned each movement disorder with a canonical target—VIM for essential tremor, the subthalamic nucleus (STN) for PD, and the globus pallidus internus (GPi) for dystonia [29,30], as depicted in Figure 3. This nucleus-based model produced major therapeutic advances, with randomized trials confirming durable improvements across tremor, bradykinesia, rigidity, and dystonia [31,32,33,34,35].
As clinical experience grew, several observations challenged this framework. Physiological responses to stimulation proved more complex than simple suppression, with heterogeneous axonal and somatic effects extending beyond the stimulation site [36,37,38]. Phenotypic variability within ET, PD, and dystonia complicated attempts to generalize stimulation responses [4,18,39].
Additionally, early safety concerns regarding MRI in patients with implanted devices limited high-resolution characterization of stimulation-induced changes [40,41]. The subsequent development of device-specific MRI protocols enabled higher-resolution interrogation of stimulation-related network effects [42], solidifying the conceptual transition from a focal intervention toward a therapy that exerts its benefits by engaging distributed motor circuits.
3.3. Phenotypes and Network Level Heterogeneity
Clinical experience with DBS rapidly demonstrated that major movement disorders exhibit substantial phenotypic heterogeneity, reflected in the variable engagement of basal ganglia–thalamo–cortical and cerebellothalamic networks (Table 1). In PD, tremor-dominant, akinetic–rigid, postural instability / gait disorder (PIGD), and cognitively vulnerable subtypes show distinct circuit dependencies that shape therapeutic response [39,43]. ET and dystonia show comparable diversity, with symptom profiles reflecting differential involvement of motor, cerebellar, and associative pathways [4,44].
Electrophysiological and imaging evidence increasingly supports the view that these conditions represent spectra of circuit dysfunction [15,37]. Tremor severity aligns with cerebellothalamic pathways—especially the dentato-rubro-thalamic path (DRTT)—[16,23], whereas bradykinesia and rigidity relate to hyperdirect cortico–subthalamic projections, and cognitive vulnerability maps onto associative–limbic networks [21,45,46]. In dystonia, responsiveness to GPi stimulation corresponds to pallidothalamic and sensorimotor network engagement [19,33,47,48].
Network specificity also explains therapeutic variability within tremor syndromes: while classic ET responds to VIM stimulation, ET-plus and cerebellar variants may benefit from posterior subthalamic area (PSA) or zona incerta (ZI) targeting, where cerebellothalamic fibers converge [16,18]. Dystonic tremor, reflecting hybrid cerebellothalamic–pallidal involvement, often requires individualized targeting [49]. Rare dystonic presentations, including GA1-related and KMT2B-associated dystonia, can improve meaningfully with GPi-DBS, though outcomes remain variable across syndromes [24,25].
3.4. Local Effects and Multiscale Biological Mechanisms
Building on these network-level distinctions, mechanistic insights into DBS derive from studies of STN stimulation in PD, where electrophysiological and cellular responses have been characterized in greatest detail (Table 2). At the microscale, DBS preferentially activates large myelinated axons while suppressing intrinsic somatic firing, generating orthodromic and antidromic signals that reshape information flow across basal ganglia circuits [12,38]. High-frequency stimulation introduces a more regular firing pattern that counteracts pathological bursting and excessive beta synchrony, reducing moment-to-moment variability in motor output [50,51]
Local responses differ across targets. Human recordings demonstrate that STN stimulation rapidly suppresses intrinsic firing, VIM stimulation evokes a brief activation burst before silencing, and GPi stimulation produces transient inhibition followed by recurrent reactivation—patterns reflecting the unique convergence of afferent and efferent connections at each site [37]. At the mesoscale, DBS suppresses pathological beta oscillations, induces short-latency cortico–subcortical entrainment, and evokes resonant neural activity (ERNA), a high-frequency signature whose amplitude scales with stimulation intensity and differs between STN and GPi [37]. These oscillatory dynamics represent a physiological bridge between local neuronal effects and broader functional improvements, consistent with macroscale network modulation summarized in Table 2.
Beyond neuronal elements, DBS also modulates non-neuronal components of the microenvironment. Astrocytes regulate neurotransmission through activity-dependent glutamate and adenosine release, influence extracellular matrix signaling, fostering conditions that support plasticity. Electrode implantation and chronic stimulation additionally induce glial and epigenetic adaptations—including reductions in astrocytic reactivity and changes in DNA methylation and microRNA expression—that may contribute to long-term functional stability [36].
Together, these multiscale responses illustrate that DBS operates through layered mechanisms encompassing cellular, oscillatory, and network domains. Although not yet indicative of a definitive disease-modifying effect, this multilevel modulation provides a neurophysiological foundation upon which rehabilitation can build by promoting more consistent motor performance and enhancing the capacity for adaptive plasticity, an alignment illustrated in Figure 4, which outlines the principal rehabilitation goals after DBS.
3.5. Imaging Evidence for Network-Level Mechanisms
Imaging studies have been central to reframing DBS mechanisms. Before MRI protocols compatible with implanted hardware became available, PET and SPECT provided the first in vivo evidence that stimulation induces metabolic and perfusion changes in regions distant from the electrode site— including motor cortex, cerebellum, thalamus, and basal ganglia—supporting a circuit-level interpretation of DBS effects [41,52]. Although limited by radiation exposure and temporal resolution, these modalities established the foundational concept that DBS modifies activity across broader motor systems.
The advent of device-specific MRI protocols enabled higher-resolution characterization of these network effects [42] (Table 1). Structural MRI and diffusion tractography studies have demonstrated that clinical outcomes correlate more strongly with stimulation of symptom-relevant pathways than with proximity to nuclear boundaries [48,53,54]. These structural imaging findings reinforce the previously outlined symptom–circuit relationships: stimulation is most effective when it interfaces with the pathways that underlie each motor or cognitive phenotype. Across disorders, pathway-level alignment—not anatomical proximity—emerges as the principal determinant of DBS efficacy.
Functional imaging further supports this distributed-network perspective [21]. Resting-state fMRI identifies connectivity signatures that predict DBS responsiveness—stronger cerebellothalamic coupling in tremor syndromes and restoration of cortico–subcortical flexibility in PD [55,56]. In dystonia, intact GPi connectivity with premotor and cingulate regions predicts faster and more durable clinical improvement [19,48,57].
Longitudinal imaging studies indicate that DBS induces progressive reorganization of motor networks rather than fixed, stimulation-dependent effects. STN stimulation alters cortico–subcortical communication patterns in PD, GPi stimulation normalizes sensorimotor network architecture in dystonia, and VIM/PSA stimulation modulates cerebellothalamic pathways in tremor syndromes, with tract involvement correlating with sustained symptom reduction [16,57,58]. Experimental work further suggests that thalamic stimulation may enhance motor learning, reinforcing the concept that DBS can facilitate adaptive network changes [59].
When considered together, imaging evidence—from early metabolic studies to contemporary structural and functional connectomics—demonstrates that DBS exerts its clinical effects through distributed circuits whose organization shapes symptom expression and treatment responsiveness.
3.6. Surgical and Technological Advances Enabling Precision DBS
Advances in imaging, computational planning, and implantable hardware have progressively shifted DBS from a nucleus-based therapy to a circuit-informed, precision neuromodulation approach (Table 3). High-field MRI now enables reliable visualization of subcortical anatomy, while diffusion tractography provides patient-specific reconstructions of pathways relevant to tremor, bradykinesia–rigidity, and dystonia [15,16,18,19,54]. These modalities support targeting strategies that align electrode placement with symptom-relevant fiber trajectories and reduce reliance on indirect anatomical landmarks [40,42].
Trajectory planning has also evolved with the integration of multimodal image fusion, tractography constraints, and vascular avoidance algorithms, enabling safe implantation while maximizing engagement of intended therapeutic structures [18,42,54]. Intraoperative workflows increasingly incorporate imaging-guided verification or microelectrode recording, offering complementary methods to confirm lead positioning and reducing operative variability[60,61,62].
Hardware innovations have expanded the capacity to tailor stimulation to individual network architecture (Table 3) [63]. Directional leads allow current steering away from structures associated with side effects and toward pathways linked to therapeutic benefit, effectively broadening the clinical stimulation range[64,65]. Sensing-enabled pulse generators can record neural biomarkers such as beta bursts or tremor-related oscillations, providing objective data for programming and chronic physiological assessment [15,66,67]. These systems form the basis for adaptive (closed-loop) DBS, in which stimulation continuously adjusts according to real-time neural states, improving gait and tremor stability and reducing unnecessary energy delivery.
Modern programming platforms incorporate postoperative lead reconstructions and tractography-based pathway models, enabling clinicians to visualize which contacts most effectively engage the patient’s dominant dysfunctional circuit [15,68]. This approach supports efficient, rational programming while facilitating alignment of stimulation with individual functional goals.

Table 4.
Rehabilitation Domains After DBS and Main Functional Goals.
| Domain | Main goals |
|---|---|
| Physiotherapy | Improve gait, balance, amplitude, and dual-task performance |
| Occupational therapy | Enhance dexterity, handwriting, and ADLs |
| Speech–language therapy | Improve articulation, phonation, and intelligibility |
| Cognitive–behavioral support | Maintain executive functioning, mood, and therapy engagement |
| Home / community training | Promote task-specific practice and generalization to daily life |
Table 4. Primary rehabilitation domains and goals following DBS. These domains outline the therapeutic framework typically integrated with neuromodulation-based care.
3.7. Rehabilitation-Integrated DBS: Towards Network Restoration
DBS may facilitate rehabilitation by stabilizing neural dynamics and reducing moment-to-moment motor variability—conditions essential for motor learning [14,67,69]. This physiological regularization enhances responsiveness to physiotherapy and improves task-specific retraining efficiency, partly by reducing motor variability [70]. Clinically, this may translate into improved capacity for locomotor training, including gait and balanced-focused interventions. This clinical effect aligns with recent mechanistic summaries demonstrating that DBS restores more physiologically regular network activity and supports functional performance [71].
Wearable sensor data show that DBS reduces gait irregularity and enhances responsiveness to physiotherapy, especially in balance and lower-limb programs[72]. Remote monitoring studies similarly indicate that periods of lower subthalamic beta activity may correspond to more favorable windows for gait rehabilitation [73]. Balance and postural control remain only partially responsive to DBS alone, reinforcing the need for targeted rehabilitation strategies [74].
A recent Delphi consensus supports early, task-specific physiotherapy after DBS, highlighting benefits in gait amplitude, dual-task performance, and postural stability when training is delivered once stimulation parameters are clinically optimized [70]. Case-based evidence also suggests that combining DBS with intensive, goal-directed rehabilitation can produce additional gains in functional mobility and daily activities beyond stimulation alone [75]. Additional clinical data suggest that structured rehabilitation improves mobility and functional performance even years after DBS implantation [76].
Newer DBS technologies strengthen these clinical applications. Sensing-enabled and adaptive systems offer physiological markers that may help clinicians time therapy sessions to periods of optimal neural stability [77,78,79]. Neuromodulation-enhanced rehabilitation frameworks further propose that DBS may support adaptive plasticity [72,75,80]. Advances in functional mobility assessment techniques, such as integrated motion-capture and pressure-based gait analysis, may further enhance the ability to quantify rehabilitation response after DBS [81].
In this view, DBS may serve as a physiological facilitator of therapy-driven improvement, though confirmation requires mechanistic and clinical validation. Complementary rehabilitative technologies such as virtual reality may also enhance gait and balance training in DBS patients in selected phenotypes [82].
4. Limitations
This review is narrative rather than systematic, and not all relevant literature may have been captured. Heterogeneity in study design, imaging methods, and follow-up restricts comparability. Mechanistic insights derive disproportionately from PD studies.
Rehabilitation protocols after DBS remain highly heterogeneous, with limited evidence to guide optimal timing, intensity, or phenotype-specific adaptations.
5. Future Directions
Future progress in deep brain stimulation (DBS) will require integration of physiological biomarkers, individualized connectomic targeting, and adaptive neuromodulation strategies. Sensing-enabled systems may align stimulation and rehabilitation with neural states favorable for motor learning, while patient-specific pathway modeling could refine circuit selection across phenotypes. Real-world motor monitoring through wearable sensors may also help quantify long-term plasticity and guide rehabilitation dosing. Ultimately, mechanistically informed clinical trials are needed to determine how DBS-induced network stabilization interacts with structured rehabilitation to support durable functional recovery.
6. Conclusions
DBS has progressed from a focal intervention to a systems-level neuromodulation therapy informed by circuit physiology, imaging biomarkers, and technological innovation. Evidence suggests that DBS modulates distributed networks, stabilizes motor output, and may enhance conditions for rehabilitation-driven improvement.
Technological developments, including directional leads, tractography-guided targeting, and adaptive systems, strengthen the interface between stimulation and therapy. Yet integrated frameworks linking neuromodulation with functional recovery remain nascent.
Overall, DBS may act as a physiological facilitator of rehabilitation, a model requiring further mechanistic refinement and clinical validation.
7. Key highlights
- Deep brain stimulation (DBS) enhances the stability of motor performance, creating favorable conditions for structured rehabilitation.
- Connectivity-informed targeting improves clinical outcomes by aligning stimulation with patient-specific circuit architecture.
- Technological advances—including tractography-based planning, directional leads, and sensing-enabled systems—support more precise and individualized neuromodulation.
- Rehabilitation integrated with DBS can amplify functional gains by leveraging stabilized neural dynamics.
- Future frameworks will incorporate adaptive stimulation, biomarker-guided therapy, and real-world motor monitoring to optimize long-term functional restoration.
Author Contributions
Conceptualization, Methodology and Data Curation, O.M-S, B. D-F., F: G.; Formal Analysis: All authors; Writing—Original Draft Preparation: O. M-S.; Writing—Review, Editing and Supervision, O.M-S, E. M, M. B.All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
Ethical approval was not required for this work, as it is a narrative review based exclusively on previously published studies and involves no new data collection from human participants or animals.
Informed Consent Statement
Not applicable. This study did not involve human participants, identifiable data, or new clinical interventions requiring informed consent.
Data Availability Statement
No new data were generated or analyzed in this study. All data discussed in this review are derived from previously published sources.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| DBS | Deep brain stimulation |
| DRTT | Dentato–rubro–thalamic tract |
| ET | Essential tremor |
| ERNA | Evoked resonant neural activity |
| fMRI | Functional magnetic resonance imaging |
| GA1 | Glutaric aciduria type I |
| GPi | Globus pallidus internus |
| KMT2B | Lysine methyltransferase 2B |
| MRI | Magnetic resonance imaging |
| PD | Parkinson’s disease |
| PET | Positron emission tomography |
| PIGD | Postural instability/gait disorder |
| PSA | Posterior subthalamic area |
| SPECT | Single-photon emission computed tomography |
| STN | Subthalamic nucleus |
| VIM | Ventral intermediate nucleus |
| ZI | Zona incerta |
References
- Louis, E.D.; Ferreira, J.J. How common is the most common adult movement disorder? Update on the worldwide prevalence of essential tremor. Mov. Disord. 2010, 25, 534–541. [Google Scholar] [CrossRef]
- Dorsey, E.R.; Sherer, T.; Okun, M.S.; Bloem, B.R. The Emerging Evidence of the Parkinson Pandemic. J. Park. Dis. 2018, 8, S3–S8. [Google Scholar] [CrossRef]
- Steeves, T.D.; Day, L.; Dykeman, J.; Jette, N.; Pringsheim, T. The prevalence of primary dystonia: A systematic review and meta-analysis. Mov. Disord. 2012, 27, 1789–1796. [Google Scholar] [CrossRef] [PubMed]
- Albanese, A.; Bhatia, K.; Bressman, S.B.; DeLong, M.R.; Fahn, S.; Fung, V.S.; Hallett, M.; Jankovic, J.; Jinnah, H.A.; Klein, C.; et al. Phenomenology and classification of dystonia: A consensus update. Mov. Disord. 2013, 28, 863–873. [Google Scholar] [CrossRef] [PubMed]
- Kowal, S.L.; Dall, T.M.; Chakrabarti, R.; Storm, M.V.; Jain, A. The current and projected economic burden of Parkinson's disease in the United States. Mov. Disord. 2013, 28, 311–318. [Google Scholar] [CrossRef]
- Wu, X.-C.; Dong, Y.-Y.; Ying, Y.-C.; Chen, G.-Y.; Fan, Q.; Yin, P.; Chen, Y.-L. The burden of Parkinson’s disease, 1990–2021: a systematic analysis of the Global Burden of Disease study 2021. Front. Aging Neurosci. 2025, 17, 1596392. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Lv, Z.; Dai, Y.; Yu, L.; Zhang, L.; Wang, K.; Hu, P. The global, regional, and National burden of parkinson’s disease in 204 countries and territories, 1990–2021: a systematic analysis for the global burden of disease study 2021. BMC Public Heal. 2025, 25, 3047. [Google Scholar] [CrossRef]
- Benabid, A.; Pollak, P.; Louveau, A.; Henry, S.; de Rougemont, J. Combined (Thalamotomy and Stimulation) Stereotactic Surgery of the VIM Thalamic Nucleus for Bilateral Parkinson Disease. Ster. Funct. Neurosurg. 1987, 50, 344–346. [Google Scholar] [CrossRef]
- Benabid, A.L.; Pollak, P.; Hommel, M.; Gaio, J.M.; De Rougemont, J.; Perret, J. Treatment of Parkinson tremor by chronic stimulation of the ventral intermediate nucleus of the thalamus. Rev Neurol (Paris). 1989, 145, 320–3. [Google Scholar]
- Tasker, R.R. Deep brain stimulation is preferable to thalamotomy for tremor suppression. Surg. Neurol. 1998, 49, 145–153. [Google Scholar] [CrossRef]
- Lozano, A.M. Vim Thalamic Stimulation for Tremor. Arch. Med Res. 2000, 31, 266–269. [Google Scholar] [CrossRef] [PubMed]
- Dostrovsky, J.O.; Lozano, A.M. Mechanisms of deep brain stimulation. Mov. Disord. 2002, 17, S63–S68. [Google Scholar] [CrossRef] [PubMed]
- R., L.; A., L.; W., H.; A., L.; J., D. Simultaneous repetitive movements following pallidotomy or subthalamic deep brain stimulation in patients with Parkinson's disease. Exp. Brain Res. 2002, 147, 322–331. [Google Scholar] [CrossRef]
- Aum, D.J.; Tierney, T.S. Deep brain stimulation foundations and future trends. Front. Biosci. 2018, 23, 162–182. [Google Scholar] [CrossRef] [PubMed]
- Horn, A.; Neumann, W.; Degen, K.; Schneider, G.; Kühn, A.A. Toward an electrophysiological “sweet spot” for deep brain stimulation in the subthalamic nucleus. Hum. Brain Mapp. 2017, 38, 3377–3390. [Google Scholar] [CrossRef]
- Al-Fatly, B.; Ewert, S.; Kübler, D.; Kroneberg, D.; Horn, A.; A Kühn, A. Connectivity profile of thalamic deep brain stimulation to effectively treat essential tremor. Brain 2019, 142, 3086–3098. [Google Scholar] [CrossRef]
- Horn, A.; Fox, M.D. Opportunities of connectomic neuromodulation. NeuroImage 2020, 221, 117180. [Google Scholar] [CrossRef]
- Middlebrooks, E.H.; Tuna, I.S.; Almeida, L.; Grewal, S.S.; Wong, J.; Heckman, M.G.; Lesser, E.R.; Bredel, M.; Foote, K.D.; Okun, M.S.; et al. Structural connectivity–based segmentation of the thalamus and prediction of tremor improvement following thalamic deep brain stimulation of the ventral intermediate nucleus. NeuroImage: Clin. 2018, 20, 1266–1273. [Google Scholar] [CrossRef]
- Corp, D.T.; Joutsa, J.; Darby, R.R.; Delnooz, C.C.S.; van de Warrenburg, B.P.C.; Cooke, D.; Prudente, C.N.; Ren, J.; Reich, M.M.; Batla, A.; et al. Network localization of cervical dystonia based on causal brain lesions. Brain 2019, 142, 1660–1674. [Google Scholar] [CrossRef]
- Hollunder, B.; Ostrem, J.L.; Sahin, I.A.; Rajamani, N.; Oxenford, S.; Butenko, K.; Neudorfer, C.; Reinhardt, P.; Zvarova, P.; Polosan, M.; et al. Mapping dysfunctional circuits in the frontal cortex using deep brain stimulation. Nat. Neurosci. 2024, 27, 573–586. [Google Scholar] [CrossRef]
- Horn, A.; Al-Fatly, B.; Neumann, W.-J.; Neudorfer, C. Connectomic DBS: An introduction. In Connectomic Deep Brain Stimulation; Elsevier, 2022; pp. 3–23. [Google Scholar] [CrossRef]
- Kilic, U.; Smets, C.; Deng, Z.; Boogers, A.; Mc Laughlin, M.; De Vloo, P.; George, D.D.; Nuttin, B. A Narrative Review on the Current Landscape of Invasive Neuromodulation for Poststroke Motor Recovery: Mechanisms, Challenges, and Future Directions. Neuromodulation Technol. Neural Interface 2025, 28, 1093–1103. [Google Scholar] [CrossRef]
- Middlebrooks, E.H.; Okromelidze, L.; E Carter, R.; Jain, A.; Lin, C.; Westerhold, E.; Peña, A.B.; Quiñones-Hinojosa, A.; Uitti, R.J.; Grewal, S.S. Directed stimulation of the dentato-rubro-thalamic tract for deep brain stimulation in essential tremor: a blinded clinical trial. Neuroradiol. J. 2021, 35, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Chacón, A.; Mateo-Sierra, O.; Pérez-Sánchez, J.R.; De la Casa-Fages, B.; Grandas, F.; De Castro, P.; Miranda, C. Long-Term Outcomes of GPi Deep Brain Stimulation in a Child with Glutaric Aciduria Type 1 (GA1). Mov. Disord. Clin. Pr. 2024, 11, 1311–1313. [Google Scholar] [CrossRef]
- Buzo, E.L.; De la Casa-Fages, B.; Sánchez, M.G.; Sánchez, J.P.; Carballal, C.F.; Vidorreta, J.G.; Sierra, O.M.; Chicote, A.C.; Grandas, F. Pallidal deep brain stimulation response in two siblings with atypical adult-onset dystonia related to a KMT2B variant. J. Neurol. Sci. 2022, 438, 120295. [Google Scholar] [CrossRef]
- Gerbasi, M.E.; Nambiar, S.; Reed, S.; Hennegan, K.; Hadker, N.; Eldar-Lissai, A.; Cosentino, S. Essential tremor patients experience significant burden beyond tremor: A systematic literature review. Front. Neurol. 2022, 13, 891446. [Google Scholar] [CrossRef]
- Olesen, J.; Gustavsson, A.; Svensson, M.; Wittchen, H.-U.; Jönsson, B. The economic cost of brain disorders in Europe. Eur. J. Neurol. 2012, 19, 155–162. [Google Scholar] [CrossRef]
- Benabid, A.; Pollak, P.; Hoffmann, D.; Gervason, C.; Hommel, M.; Perret, J.; de Rougemont, J.; Gao, D. Long-term suppression of tremor by chronic stimulation of the ventral intermediate thalamic nucleus. Lancet 1991, 337, 403–406. [Google Scholar] [CrossRef]
- Limousin, P.; Martinez-Torres, I. Deep Brain Stimulation for Parkinson’s Disease. Neurotherapeutics 2008, 5, 309–319. [Google Scholar] [CrossRef]
- Kupsch, A.; Benecke, R.; Müller, J.; Trottenberg, T.; Schneider, G.-H.; Poewe, W.; Eisner, W.; Wolters, A.; Müller, J.-U.; Deuschl, G.; et al. Pallidal Deep-Brain Stimulation in Primary Generalized or Segmental Dystonia. New Engl. J. Med. 2006, 355, 1978–1990. [Google Scholar] [CrossRef] [PubMed]
- Volkmann, J.; Wolters, A.; Kupsch, A.; Müller, J.; A Kühn, A.; Schneider, G.-H.; Poewe, W.; Hering, S.; Eisner, W.; Müller, J.-U.; et al. Pallidal deep brain stimulation in patients with primary generalised or segmental dystonia: 5-year follow-up of a randomised trial. Lancet Neurol. 2012, 11, 1029–1038. [Google Scholar] [CrossRef] [PubMed]
- Deuschl, G.; Schade-Brittinger, C.; Krack, P.; Volkmann, J.; Schäfer, H.; Bötzel, K.; Daniels, C.; Deutschländer, A.; Dillmann, U.; Eisner, W.; et al. A Randomized Trial of Deep-Brain Stimulation for Parkinson's Disease. New Engl. J. Med. 2006, 355, 896–908. [Google Scholar] [CrossRef] [PubMed]
- Vidailhet, M.; Vercueil, L.; Houeto, J.-L.; Krystkowiak, P.; Benabid, A.-L.; Cornu, P.; Lagrange, C.; Du Montcel, S.T.; Dormont, D.; Grand, S.; et al. Bilateral Deep-Brain Stimulation of the Globus Pallidus in Primary Generalized Dystonia. New Engl. J. Med. 2005, 352, 459–467. [Google Scholar] [CrossRef]
- Weaver, F.M. Bilateral Deep Brain Stimulation vs Best Medical Therapy for Patients With Advanced Parkinson DiseaseA Randomized Controlled Trial. JAMA 2009, 301, 63–73. [Google Scholar] [CrossRef]
- Fasano, A.; Lozano, A.M. Deep brain stimulation for movement disorders. Curr. Opin. Neurol. 2015, 28, 423–436. [Google Scholar] [CrossRef]
- Davidson, B.; Milosevic, L.; Kondrataviciute, L.; Kalia, L.V.; Kalia, S.K. Neuroscience fundamentals relevant to neuromodulation: Neurobiology of deep brain stimulation in Parkinson's disease. Neurotherapeutics 2024, 21, e00348. [Google Scholar] [CrossRef]
- Neumann, W.-J.; A Steiner, L.; Milosevic, L. Neurophysiological mechanisms of deep brain stimulation across spatiotemporal resolutions. Brain 2023, 146, 4456–4468. [Google Scholar] [CrossRef]
- McIntyre, C.C.; Anderson, R.W. Deep brain stimulation mechanisms: the control of network activity via neurochemistry modulation. J. Neurochem. 2016, 139, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Marras, C.; Lang, A. Parkinson's disease subtypes: lost in translation? J. Neurol. Neurosurg. Psychiatry 2012, 84, 409–415. [Google Scholar] [CrossRef]
- Boutet, A.; Madhavan, R.; Elias, G.J.B.; Joel, S.E.; Gramer, R.; Ranjan, M.; Paramanandam, V.; Xu, D.; Germann, J.; Loh, A.; et al. Predicting optimal deep brain stimulation parameters for Parkinson’s disease using functional MRI and machine learning. Nat. Commun. 2021, 12, 3043. [Google Scholar] [CrossRef] [PubMed]
- Kokkonen, A.; Honkanen, E.A.; Corp, D.T.; Joutsa, J. Neurobiological effects of deep brain stimulation: A systematic review of molecular brain imaging studies. NeuroImage 2022, 260, 119473. [Google Scholar] [CrossRef]
- Boutet, A.; Lozano, A.M. Deep Brain Stimulation and Magnetic Resonance Imaging: Future Directions. In Magnetic Resonance Imaging in Deep Brain Stimulation; Springer International Publishing: Cham, 2022; pp. 121–122. [Google Scholar] [CrossRef]
- Thenganatt, M.A.; Jankovic, J. Parkinson Disease Subtypes. JAMA Neurol. 2014, 71, 499–504. [Google Scholar] [CrossRef]
- Bhatia, K.P.; Bain, P.; Bajaj, N.; Elble, R.J.; Hallett, M.; Louis, E.D.; Raethjen, J.; Stamelou, M.; Testa, C.M.; Deuschl, G.; et al. Consensus Statement on the classification of tremors. from the task force on tremor of the International Parkinson and Movement Disorder Society. Mov. Disord. 2017, 33, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Nambu, A.; Tokuno, H.; Takada, M. Functional significance of the cortico–subthalamo–pallidal ‘hyperdirect’ pathway. Neurosci. Res. 2002, 43, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.-L.; Chen, Y.-C.; Tu, P.-H.; Liu, T.-C.; Chen, M.-C.; Wu, H.-T.; Yeap, M.-C.; Yeh, C.-H.; Lu, C.-S.; Chen, C.-C. Subthalamic high-beta oscillation informs the outcome of deep brain stimulation in patients with Parkinson's disease. Front. Hum. Neurosci. 2022, 16, 958521. [Google Scholar] [CrossRef]
- Hanekamp, S.; Simonyan, K. The large-scale structural connectome of task-specific focal dystonia. Hum. Brain Mapp. 2020, 41, 3253–3265. [Google Scholar] [CrossRef]
- Raghu, A.L.B.; Eraifej, J.; Sarangmat, N.; Stein, J.; FitzGerald, J.J.; Payne, S.; Aziz, T.Z.; Green, A.L. Pallido-putaminal connectivity predicts outcomes of deep brain stimulation for cervical dystonia. Brain 2021, 144, 3589–3596. [Google Scholar] [CrossRef]
- Nagel, J.M.; Wolf, M.E.; Blahak, C.; Runge, J.; Schrader, C.; Dressler, D.; Saryyeva, A.; Krauss, J.K. Thalamic Deep Brain Stimulation for Dystonic Head Tremor: A Long-Term Study of 18 Patients. Mov. Disord. Clin. Pr. 2025. [Google Scholar] [CrossRef]
- Montgomery, E.B.; Gale, J.T. Mechanisms of action of deep brain stimulation (DBS). Neurosci. Biobehav. Rev. 2008, 32, 388–407. [Google Scholar] [CrossRef]
- Lozano, A.M.; Lipsman, N. Probing and Regulating Dysfunctional Circuits Using Deep Brain Stimulation. Neuron 2013, 77, 406–424. [Google Scholar] [CrossRef]
- Ceballos-Baumann, A.O.; Boecker, H.; Bartenstein, P.; von Falkenhayn, I.; Riescher, H.; Conrad, B.; Moringlane, J.R.; Alesch, F. A Positron Emission Tomographic Study of Subthalamic Nucleus Stimulation in Parkinson Disease. Arch. Neurol. 1999, 56, 997–1003. [Google Scholar] [CrossRef] [PubMed]
- Hvingelby, V.; Khalil, F.; Massey, F.; Hoyningen, A.; Xu, S.S.; Candelario-McKeown, J.; Akram, H.; Foltynie, T.; Limousin, P.; Zrinzo, L.; et al. Directional deep brain stimulation electrodes in Parkinson’s disease: meta-analysis and systematic review of the literature. J. Neurol. Neurosurg. Psychiatry 2025, 96, 188–198. [Google Scholar] [CrossRef]
- Vassal, F.; Dilly, D.; Boutet, C.; Bertholon, F.; Charier, D.; Pommier, B. White matter tracts involved by deep brain stimulation of the subthalamic nucleus in Parkinson’s disease: a connectivity study based on preoperative diffusion tensor imaging tractography. Br. J. Neurosurg. 2020, 34, 187–195. [Google Scholar] [CrossRef]
- Kahan, J.; Urner, M.; Moran, R.; Flandin, G.; Marreiros, A.; Mancini, L.; White, M.; Thornton, J.; Yousry, T.; Zrinzo, L.; et al. Resting state functional MRI in Parkinson’s disease: the impact of deep brain stimulation on ‘effective’ connectivity. Brain 2014, 137, 1130–1144. [Google Scholar] [CrossRef] [PubMed]
- Shang, R.; He, L.; Ma, X.; Ma, Y.; Li, X. Connectome-Based Model Predicts Deep Brain Stimulation Outcome in Parkinson's Disease. Front. Comput. Neurosci. 2020, 14, 571527. [Google Scholar] [CrossRef]
- Okromelidze, L.; Tsuboi, T.; Eisinger, R.; Burns, M.; Charbel, M.; Rana, M.; Grewal, S.; Lu, C.-Q.; Almeida, L.; Foote, K.; et al. Functional and Structural Connectivity Patterns Associated with Clinical Outcomes in Deep Brain Stimulation of the Globus Pallidus Internus for Generalized Dystonia. Am. J. Neuroradiol. 2020, 41, 508–514. [Google Scholar] [CrossRef]
- Filip, P.; Jech, R.; Fečíková, A.; Havránková, P.; Růžička, F.; Mueller, K.; Urgošík, D. Restoration of functional network state towards more physiological condition as the correlate of clinical effects of pallidal deep brain stimulation in dystonia. Brain Stimul. 2022, 15, 1269–1278. [Google Scholar] [CrossRef]
- Terzic, L.; Voegtle, A.; Farahat, A.; Hartong, N.; Galazky, I.; Nasuto, S.J.; Andrade, A.d.O.; Knight, R.T.; Ivry, R.B.; Voges, J.; et al. Deep brain stimulation of the ventrointermediate nucleus of the thalamus to treat essential tremor improves motor sequence learning. Hum. Brain Mapp. 2022, 43, 4791–4799. [Google Scholar] [CrossRef] [PubMed]
- Atsumi, H.; Matsumae, M. Fusing of Preoperative Magnetic Resonance and Intraoperative O-arm Images in Deep Brain Stimulation Enhance Intuitive Surgical Planning and Increase Accuracy of Lead Placement. Neurol. Med.-Chir 2021, 61, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Vinke, R.S.; Selvaraj, A.K.; Geerlings, M.; Georgiev, D.; Sadikov, A.; Kubben, P.L.; Doorduin, J.; Praamstra, P.; Bloem, B.R.; Bartels, R.H.; et al. The Role of Microelectrode Recording and Stereotactic Computed Tomography in Verifying Lead Placement During Awake MRI-Guided Subthalamic Nucleus Deep Brain Stimulation for Parkinson’s Disease. J. Park. Dis. 2022, 12, 1269–1278. [Google Scholar] [CrossRef]
- Massager, N.; Nguyen, A.; Pouleau, H.-B.; Dethy, S.; Morelli, D. Deviation of DBS Recording Microelectrodes during Insertion Assessed by Intraoperative CT. Ster. Funct. Neurosurg. 2023, 101, 161–169. [Google Scholar] [CrossRef]
- Krauss, J.K.; Lipsman, N.; Aziz, T.; Boutet, A.; Brown, P.; Chang, J.W.; Davidson, B.; Grill, W.M.; Hariz, M.I.; Horn, A.; et al. Technology of deep brain stimulation: current status and future directions. Nat. Rev. Neurol. 2020, 17, 75–87. [Google Scholar] [CrossRef]
- Moreno-Escobar, M.C.; Elkins, R.; Murray, A.; Brandmeir, N.; Brandmeir, C.; Pallavaram, S.; Tripathi, R.; Elkins, R.A. Directional Deep Brain Stimulation Programming in Parkinson's Disease and Essential Tremor Patients: An Institution-Based Study. Cureus 2025, 17. [Google Scholar] [CrossRef]
- Umemura, A.; Mizuno, H.; Maki, M.; Masago, A. Image-guided optimization of current steering in STN-DBS for Parkinson's disease. Front. Neurol. 2025, 16, 1618480. [Google Scholar] [CrossRef] [PubMed]
- Gilron, R.; Little, S.; Perrone, R.; Wilt, R.; de Hemptinne, C.; Yaroshinsky, M.S.; Racine, C.A.; Wang, S.S.; Ostrem, J.L.; Larson, P.S.; et al. Long-term wireless streaming of neural recordings for circuit discovery and adaptive stimulation in individuals with Parkinson’s disease. Nat. Biotechnol. 2021, 39, 1078–1085. [Google Scholar] [CrossRef]
- Neumann, W.-J.; Turner, R.S.; Blankertz, B.; Mitchell, T.; Kühn, A.A.; Richardson, R.M. Toward Electrophysiology-Based Intelligent Adaptive Deep Brain Stimulation for Movement Disorders. Neurotherapeutics 2019, 16, 105–118. [Google Scholar] [CrossRef] [PubMed]
- Dembek, T.A.; Roediger, J.; Horn, A.; Reker, P.; Oehrn, C.; Dafsari, H.S.; Li, N.; Kühn, A.A.; Fink, G.R.; Visser-Vandewalle, V.; et al. Probabilistic sweet spots predict motor outcome for deep brain stimulation in Parkinson disease. Ann. Neurol. 2019, 86, 527–538. [Google Scholar] [CrossRef]
- Altoum, S.; Suliman, O.; Abulaban, N. Clinical Outcomes and Pathophysiological Correlates of Deep Brain Stimulation in Parkinson’s Disease: A Systematic Review. J. Adv. Med. Med Res. 2025, 37, 342–354. [Google Scholar] [CrossRef]
- Guidetti, M.; Marceglia, S.; Bocci, T.; Duncan, R.; Fasano, A.; Foote, K.D.; Hamani, C.; Krauss, J.K.; Kühn, A.A.; Lena, F.; et al. Physical therapy in patients with Parkinson’s disease treated with Deep Brain Stimulation: a Delphi panel study. 2024. [Google Scholar] [CrossRef]
- Wójcik, R.; Dębska, A.; Zaczkowski, K.; Szmyd, B.; Podstawka, M.; Bobeff, E.J.; Piotrowski, M.; Ratajczyk, P.; Jaskólski, D.J.; Wiśniewski, K. Deep Brain Stimulation for Parkinson’s Disease—A Narrative Review. Biomedicines 2025, 13, 2430. [Google Scholar] [CrossRef] [PubMed]
- Salzmann, L.; Bichsel, O.; Rohr-Fukuma, M.; Naef, A.C.; Stieglitz, L.; Oertel, M.F.; Bujan, B.; Jedrysiak, P.; Lambercy, O.; Imbach, L.L.; et al. Lower limb motor effects of DBS neurofeedback in Parkinson’s disease assessed through IMU-based UPDRS movement quality metrics. Sci. Rep. 2025. [Google Scholar] [CrossRef]
- Marano, M.; Tinkhauser, G.; Anzini, G.; Leogrande, G.; Ricciuti, R.; Paniccia, M.; Belli, A.; Pierleoni, P.; Di Lazzaro, V.; Raggiunto, S. Subthalamic beta power and gait in Parkinson's disease during unsupervised remote monitoring. Park. Relat. Disord. 2025, 107903. [Google Scholar] [CrossRef]
- Lonergan, B.; Seemungal, B.M.; Ciocca, M.; Tai, Y.F. The Effects of Deep Brain Stimulation on Balance in Parkinson’s Disease as Measured Using Posturography—A Narrative Review. Brain Sci. 2025, 15, 535. [Google Scholar] [CrossRef] [PubMed]
- Ferriero, G.; Magro, V.M.; Ferrara, P.E.; Ariani, M.; Coraci, D.; Codazza, S.; Maggi, L.; Ronconi, G. Deep-Brain Stimulation and Intensive Rehabilitation in a Patient with Parkinson Disease: A Case Report. Am. J. Case Rep. 2025, 26, e946308. [Google Scholar] [CrossRef]
- Canesi, M.; Lippi, L.; Rivaroli, S.; Vavassori, D.; Trenti, M.; Sartorio, F.; Meucci, N.; de Sire, A.; Siri, C.; Invernizzi, M. Long-Term Impact of Deep Brain Stimulation in Parkinson’s Disease: Does It Affect Rehabilitation Outcomes? Medicina 2024, 60, 927. [Google Scholar] [CrossRef]
- Bouthour, W.; Mégevand, P.; Donoghue, J.; Lüscher, C.; Birbaumer, N.; Krack, P. Biomarkers for closed-loop deep brain stimulation in Parkinson disease and beyond. Nat. Rev. Neurol. 2019, 15, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Zhu, G.; Shi, L.; Zhang, C.; Wu, B.; Yang, A.; Meng, F.; Jiang, Y.; Zhang, J. Closed-Loop Adaptive Deep Brain Stimulation in Parkinson’s Disease: Procedures to Achieve It and Future Perspectives. J. Park. Dis. 2023, 13, 453–471. [Google Scholar] [CrossRef]
- Oliveira, A.M.; Coelho, L.; Carvalho, E.; Ferreira-Pinto, M.J.; Vaz, R.; Aguiar, P. Machine learning for adaptive deep brain stimulation in Parkinson’s disease: closing the loop. J. Neurol. 2023, 270, 5313–5326. [Google Scholar] [CrossRef]
- Calabrò, R.S. Integrating Body Schema and Body Image in Neurorehabilitation: Where Do We Stand and What’s Next? Brain Sci. 2025, 15, 373. [Google Scholar] [CrossRef]
- Köchli, S.; Casso, I.; Delevoye-Turrell, Y.N.; Schmid, S.; Rose, D.C.; Whyatt, C. A New Methodological Approach Integrating Motion Capture and Pressure-Sensitive Gait Data to Assess Functional Mobility in Parkinson’s Disease: A Two-Phase Study. Sensors 2025, 25, 5999. [Google Scholar] [CrossRef]
- Surridge, R.; Stilp, C.; Johnson, C.; Brumitt, J. The Use of Virtual Reality to Improve Gait and Balance in Patients with Parkinson’s Disease: A Scoping Review. Virtual Worlds 2025, 4, 13. [Google Scholar] [CrossRef]
Figure 1.
Projected prevalence of major movement disorders (2000–2050). Values reflect approximate population-level trends derived from published epidemiological data. These projections illustrate the growing global burden of movement disorders and underscore the need for therapeutic strategies that enhance functional capacity and reduce long-term disability.
Figure 1.
Projected prevalence of major movement disorders (2000–2050). Values reflect approximate population-level trends derived from published epidemiological data. These projections illustrate the growing global burden of movement disorders and underscore the need for therapeutic strategies that enhance functional capacity and reduce long-term disability.
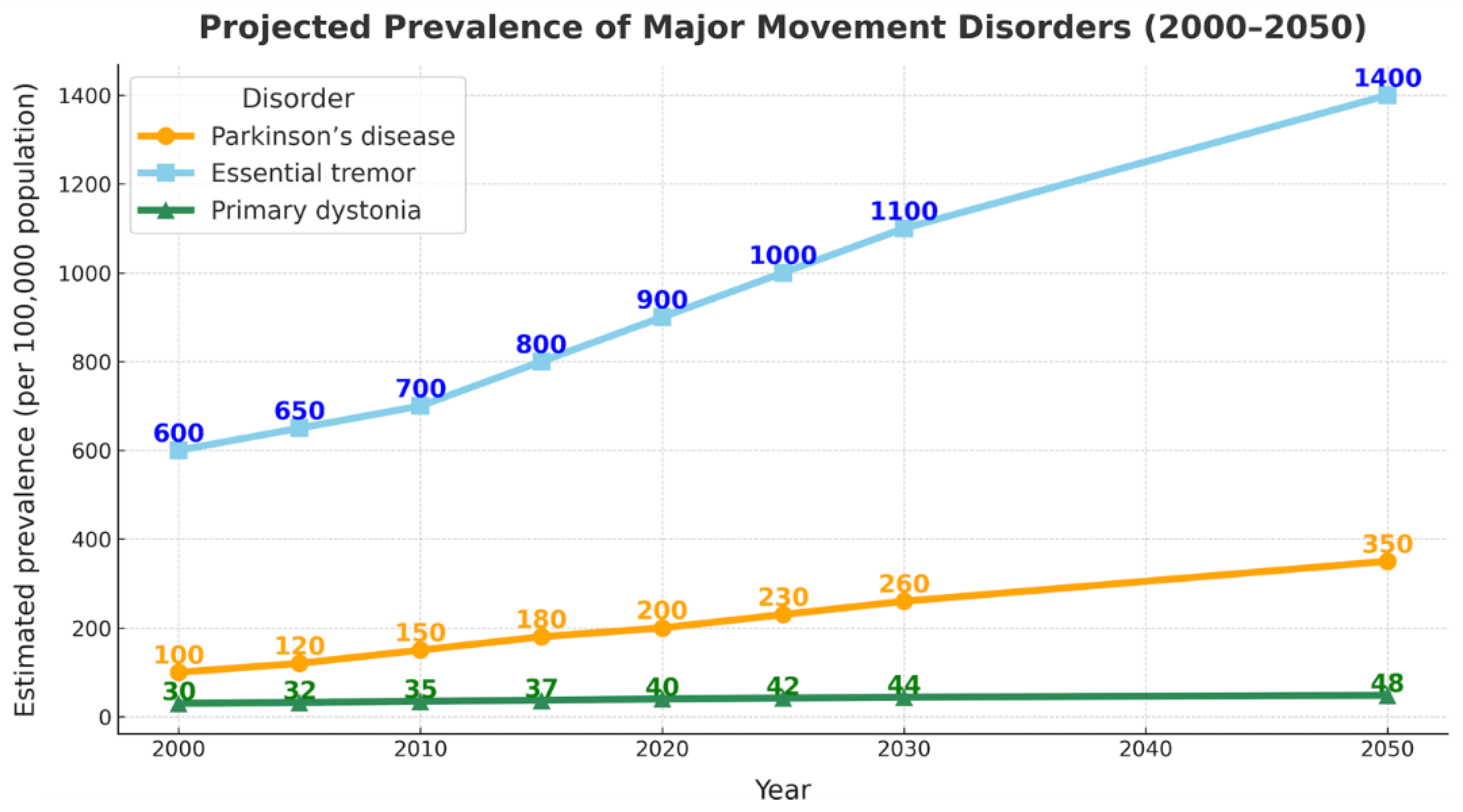
Figure 2.
Conceptual evolution of deep brain stimulation (DBS). Five major eras illustrate the progression from lesion-based interventions to modern, network-guided neuromodulation. Early irreversible lesioning was replaced by high-frequency DBS, later reinterpreted within network-level frameworks. Advances in connectomics enabled pathway-specific targeting, and from 2020 onward, sensing-enabled and adaptive DBS technologies have driven the transition toward rehabilitation-integrated neuromodulation.
Figure 2.
Conceptual evolution of deep brain stimulation (DBS). Five major eras illustrate the progression from lesion-based interventions to modern, network-guided neuromodulation. Early irreversible lesioning was replaced by high-frequency DBS, later reinterpreted within network-level frameworks. Advances in connectomics enabled pathway-specific targeting, and from 2020 onward, sensing-enabled and adaptive DBS technologies have driven the transition toward rehabilitation-integrated neuromodulation.
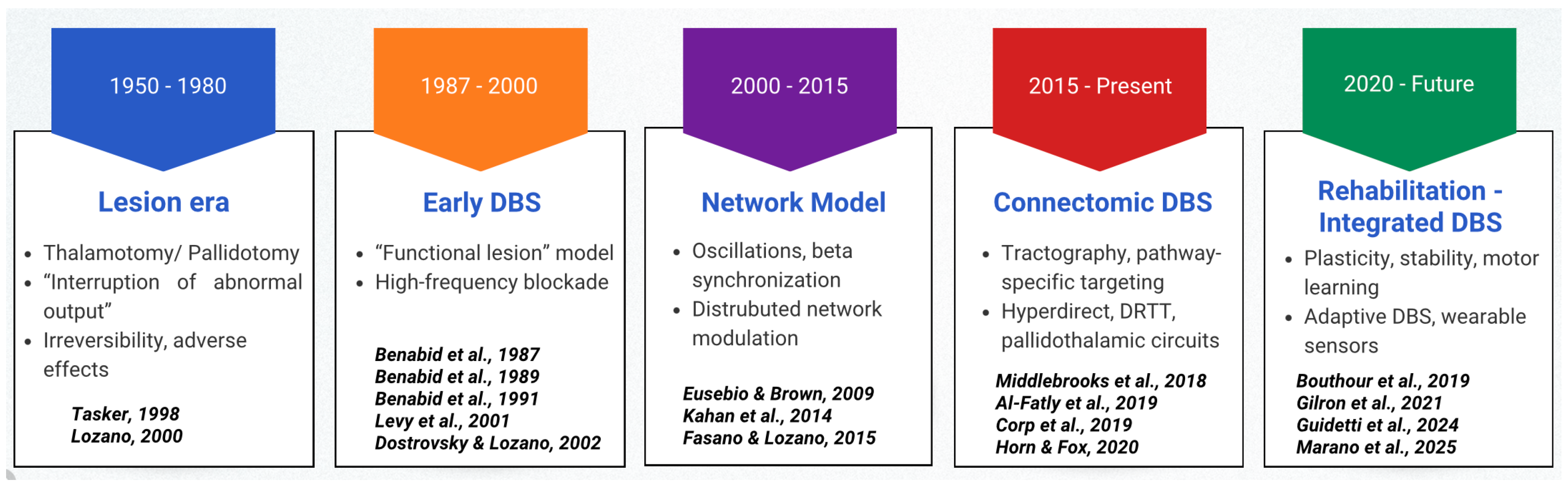
Figure 3.
Pathways, DBS targets, and key physiological effects across movement disorders. Schematic overview of dominant dysfunctional circuits, preferred DBS targets, and associated physiological effects across movement disorders.
Figure 3.
Pathways, DBS targets, and key physiological effects across movement disorders. Schematic overview of dominant dysfunctional circuits, preferred DBS targets, and associated physiological effects across movement disorders.
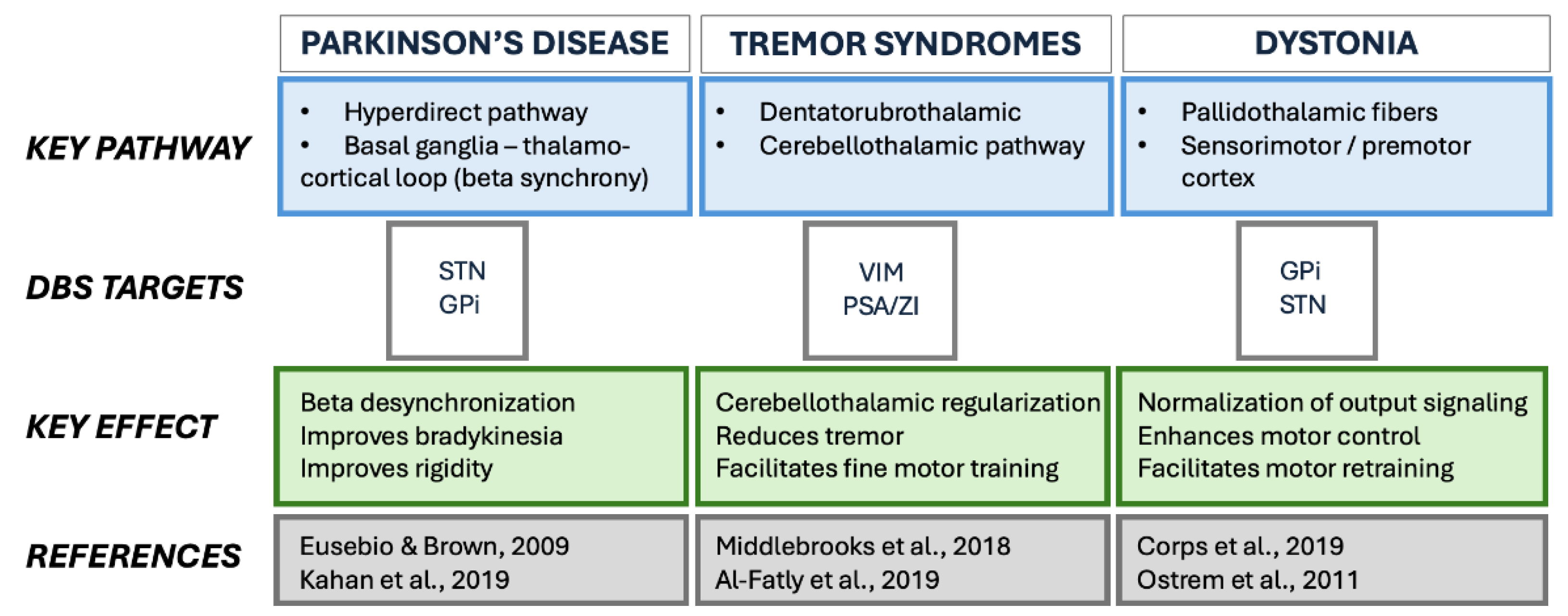
Figure 4.
Integrative overview of DBS mechanisms, disease-specific circuit engagement, key technological advances, and rehabilitation domains. Connectomic imaging and pathway-informed targeting link multiscale neuromodulation effects with clinical and rehabilitative applications.
Figure 4.
Integrative overview of DBS mechanisms, disease-specific circuit engagement, key technological advances, and rehabilitation domains. Connectomic imaging and pathway-informed targeting link multiscale neuromodulation effects with clinical and rehabilitative applications.
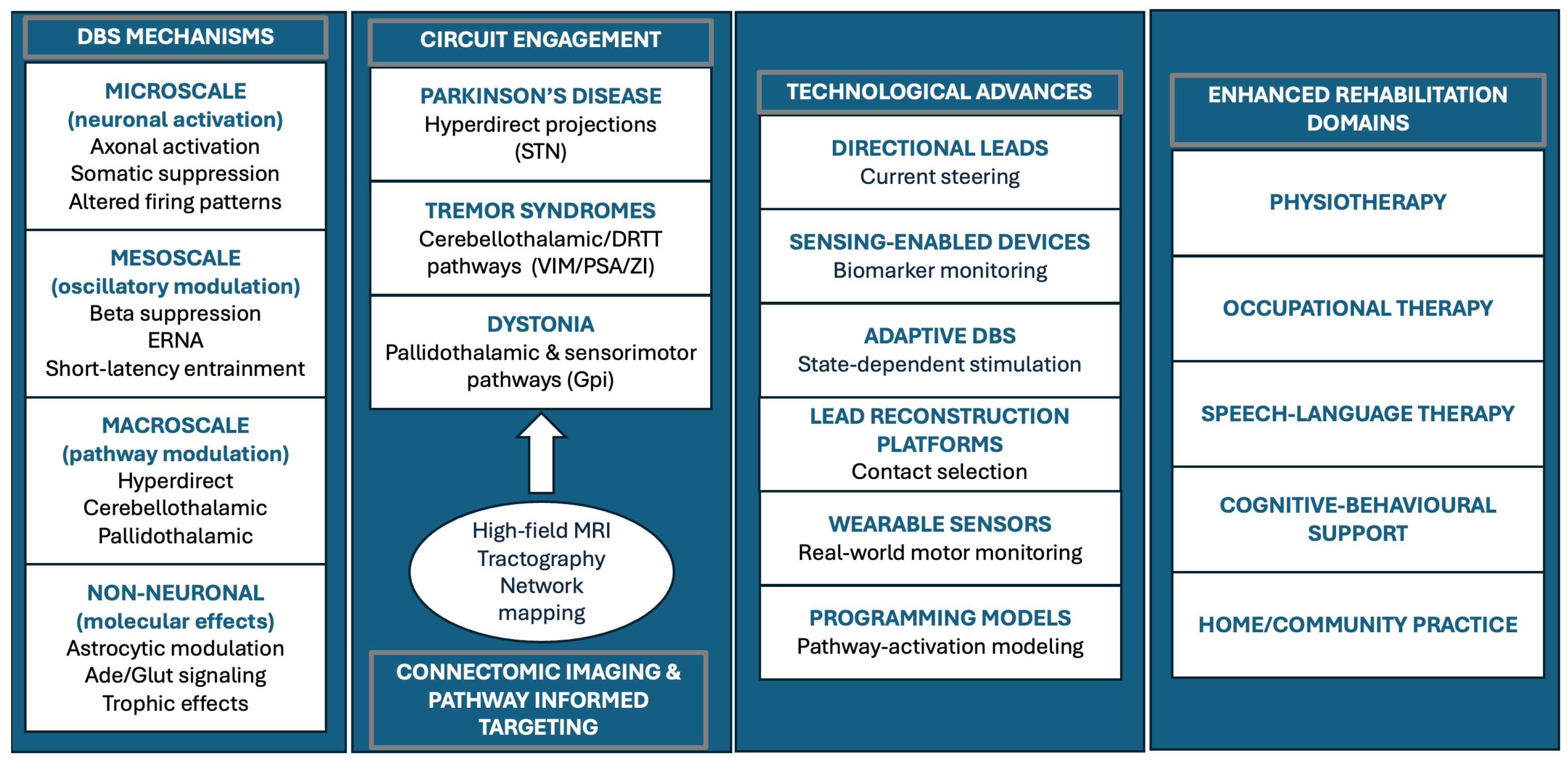
Table 1.
Phenotypes, Dominant Circuits, and Rehabilitation Implications in DBS.
| Technology | Core feature | Clinical / rehabilitation relevance |
|---|---|---|
| High-field MRI + tractography |
Patient-specific visualization of relevant pathways | Improves targeting precision and reduces side effects, supporting alignment of stimulation with functional goals |
| Directional leads | Current steering toward therapeutic pathways | Widens therapeutic window; improves stability for high-intensity rehabilitation |
| Sensing-enabled DBS | Continuous monitoring of physiological biomarkers | Enables objective programming and reduces variability affecting therapy performance |
| Adaptive DBS (closed-loop) |
Stimulation delivered when biomarkers exceed thresholds | Improves gait/tremor stability and supports timing of rehabilitation tasks |
| Wearable motor sensors | Continuous monitoring of gait, tremor, bradykinesia | Enables therapy personalization and home-based training |
| Connectomic programming platforms |
Lead reconstructions + pathway-activation modeling | Supports individualized programming based on patient-specific networks |
Table 1. Phenotype–circuit–rehabilitation mapping in movement disorders. Dominant dysfunctional networks are summarized alongside key rehabilitation implications; PD: Parkinson’s disease; DRTT: dentato–rubro–thalamic tract; STN: subthalamic nucleus; GPi: globus pallidus internus.
Table 2.
Multiscale Biological Mechanisms of DBS and Their Relevance for rehabilitation.
| Mechanistic level | Key mechanisms | Rehabilitation relevance |
|---|---|---|
| Microscale (neuronal) |
Axonal activation; somatic suppression; altered firing patterns | Stabilizes motor output and supports consistent performance during training |
| Mesoscale (oscillatory) |
Beta suppression; ERNA; short-latency entrainment | Enhances motor learning and improves within-session stability |
| Macroscale (network) |
Modulation of hyperdirect, cerebellothalamic, and pallidothalamic circuits | Aligns stimulation with gait, fine-motor, and functional rehabilitation goals |
| Non-neuronal/ molecular |
Astrocytic modulation, adenosine release, trophic signaling | Supports adaptive plasticity and learning-dependent improvement |
Table 2. Multiscale neuronal, oscillatory, network-level, and non-neuronal mechanisms of DBS relevant to functional rehabilitation, illustrating how these mechanisms relate to rehabilitative potential.
Table 3.
Technological Innovations in DBS and Their Functional/Rehabilitative Implications.
| Technology | Core feature | Clinical / rehabilitation relevance |
|---|---|---|
| High-field MRI + tractography |
Patient-specific visualization of relevant pathways | Improves targeting precision and reduces side effects, supporting alignment of stimulation with functional goals |
| Directional leads | Current steering toward therapeutic pathways | Widens therapeutic window; improves stability for high-intensity rehabilitation |
| Sensing-enabled DBS | Continuous monitoring of physiological biomarkers | Enables objective programming and reduces variability affecting therapy performance |
| Adaptive DBS (closed-loop) |
Stimulation delivered when biomarkers exceed thresholds | Improves gait/tremor stability and supports timing of rehabilitation tasks |
| Wearable motor sensors | Continuous monitoring of gait, tremor, bradykinesia | Enables therapy personalization and home-based training |
| Connectomic programming platforms | Lead reconstructions + pathway-activation modeling | Supports individualized programming based on patient-specific networks |
Table 3. Key DBS technologies and their clinical and rehabilitation implications.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



