
Submitted:
11 December 2025
Posted:
15 December 2025
You are already at the latest version
Abstract
Background: Acute pulmonary embolism (PE), particularly massive and high-risk submassive PE, carries mortality rates exceeding 50% and 15%, respectively. Anticoagulation alone does not effectively reduce mortality. Thrombolytic therapy improves outcomes but poses a substantial bleeding risk. Indigo aspiration thrombectomy alleviates right ventricular pressure overload in acute massive or high-risk submassive PE; however, its effect on PE-related mortality is unknown. This study aimed to determine whether Indigo aspiration thrombectomy improved right heart function and reduced PE-related mortality. Methods: This retrospective cohort study included 46 patients diagnosed with acute massive or high-risk submassive PE who underwent Indigo aspiration thrombectomy between January 2020 and August 2025. The study was conducted in the intensive care unit at China Medical University Hospital, Taichung, Taiwan. Efficacy endpoints were right heart parameters; safety endpoints included major bleeding events and 90-day mortality. Kaplan–Meier survival curve analysis was also performed. Results: Indigo aspiration thrombectomy significantly improved right heart parameters. Pulmonary artery (PA) systolic and mean pressures decreased by 23% (from 57.2 to 44.3 mmHg, p = 0.001; from 35.0 to 26.8 mmHg, p < 0.001). PA pulsatility index increased by 50%, and the right ventricular to left ventricular diameter ratio decreased by 30%. For acute massive PE, the major bleeding rate was 31.3% and PE-related mortality was 25.0%. For acute high-risk submassive PE, the major bleeding and PE-related mortality rates were both 3.3%. Conclusions: Indigo aspiration thrombectomy considerably improves right heart failure and may reduce PE-related mortality in patients with acute massive or high-risk submassive PE.
Keywords:
acute pulmonary embolism
; Indigo aspiration thrombectomy
; right heart failure
; pulmonary artery pressure
; pulmonary artery pulsatility index
1. Introduction
The incidence of acute pulmonary embolism (PE) is approximately 1/1000 [1]. Anticoagulants are the primary treatment for acute PE [2]. However, one-quarter of patients require emergent thrombolysis due to a high risk of death [3].
The European Society of Cardiology guidelines classify acute PE into four risk categories: high risk (massive), intermediate-high risk (high-risk submassive), intermediate-low risk (low-risk submassive), and low risk [4]. Acute massive PE signifies hemodynamic instability, such as a systolic blood pressure < 90 mmHg or obstructive shock. It accounts for approximately 5–10% of acute PE cases and carries a 90-day mortality rate of >50% with heparin alone [5]. Thrombolytic therapy (systemic or catheter-directed) is the primary treatment, and surgical thrombectomy may be used as an adjunct in cases of circulatory failure. Extracorporeal membrane oxygenation (ECMO) may be required for obstructive shock [6]. Acute submassive PE indicates increased right heart strain and mildly elevated troponin I levels. If the ratio of right ventricular (RV) to left ventricular (LV) diameter exceeds 1 [7], this condition is typically classified as acute high-risk submassive PE. Acute high-risk submassive PE comprises 10–20% of acute PE and carries a 90-day mortality rate of >15% with heparin alone. Thrombolytic therapy or surgical embolectomy is often performed in selected patients [8]. However, even with thrombolysis or embolectomy, acute massive or high-risk submassive PE still carries a high mortality rate [9].
The Penumbra Indigo® Aspiration System (Penumbra Inc., California, USA) is a large-bore aspiration thrombectomy device approved by the U.S. Food and Drug Administration for treating acute PE. Recent data indicate that, compared to thrombolytic therapy or surgical embolectomy, Indigo aspiration thrombectomy improves radiographic outcomes and has a lower incidence of major bleeding [10]. However, the survival benefit associated with Indigo aspiration thrombectomy remains unclear. This study aimed to determine whether Indigo aspiration thrombectomy improved right heart function and reduced PE-related mortality.
2. Materials and Methods
2.1 Study Design and Population
Data were retrieved from electronic hospital records, and written informed consent was waived due to the retrospective study design. The study protocol conformed to the ethical guidelines of the Institutional Review Board of China Medical University Hospital (CMUH114-REC3-201).
This observational, retrospective cohort study included 179 adult patients with acute massive or high-risk submassive PE who were consecutively admitted to the intensive care unit of China Medical University Hospital, Taichung, Taiwan, between January 2020 and August 2025. Patients who did not undergo Indigo aspiration thrombectomy were excluded from the study. A total of 46 patients were ultimately included in the statistical analysis (Strengthening the Reporting of Observational Studies in Epidemiology flowchart; Figure 1). Given the large proportion of patients with cancer, we excluded cases in which cancer was the cause of death to focus on Kaplan–Meier survival analysis on acute PE. For example, one patient was excluded from the acute massive PE group due to endometrial cancer with metastasis. Three patients were excluded from the acute high-risk submassive PE group because of duodenal cancer with metastasis, endometrial cancer with metastasis, and ruptured hepatocellular carcinoma.
2.2 Vital Signs (Blood Pressure, Heart Rate, Shock index, Respiratory Rate, Partial Pressure of Arterial Oxygen [PaO2]/Fraction of Inspired Oxygen [FiO2] ratio)
Vital signs included blood pressure, heart rate, and respiratory rate. The shock index was calculated as the ratio of heart rate to blood pressure; values > 1 indicate clinical shock. The PaO₂/FiO₂ ratio was used to assess oxygenation. A PaO2/FiO2 ratio of 200–300 indicates mild desaturation, 100–200 indicates moderate desaturation, and <100 indicates severe desaturation.
2.3 Right Heart Parameters (Pulmonary Artery [PA] Pressure, Right Atrial Pressure, PA Pulsatility Index, RV/LV Diameter Ratio)
A Swan–Ganz right heart catheter was used to measure PA pressure and right atrial pressure. The PA pulsatility index was calculated as the ratio of PA pulse pressure to right atrial pressure. A PA pulsatility index < 1.8 indicates right heart failure [11].
2.4 Severity Evaluation (Percentage of Main Trunk or Bilateral, Mastora Obstruction Index, PE Severity Index)
If thrombi are distributed in the main PA or bilaterally, they are typically considered more severe. The Mastora occlusion index assesses the overall thrombus burden in the PA. A 1–5 scale is applied to each point based on the severity of occlusion: mediastinal artery occlusion, 5 points; lobar artery occlusion, 6 points; and segmental artery occlusion, 20 points. The maximum total score is 155. Scores > 85 indicate high risk, 55–85 indicate intermediate risk, and < 55 indicate low risk [12].
The PE severity index is a clinical tool that incorporates multiple factors, including age, sex, history of cancer or heart failure, heart rate, systolic blood pressure, respiratory rate, temperature, altered mental status, and oxygen saturation. A score > 140 (class V) indicates high risk, 110–140 (class IV–V) indicates intermediate-high risk, 80–110 (class III–IV) indicates intermediate-low risk, and < 80 (class I–II) indicates low risk [13].
2.5 Indigo Thrombectomy in Acute Massive or High-Risk Submassive PE
For acute massive or high-risk submassive PE, thrombolytic therapy is the preferred treatment. However, when patients have contraindications to thrombolysis (such as post-surgery, hemorrhagic stroke, recent ischemic stroke, malignant intracranial neoplasm, or active bleeding), clinicians may consider Indigo aspiration thrombectomy. A small proportion of patients undergo thrombectomy to establish a pathway for subsequent thrombolysis.
2.6 Statistical Analysis
The sample size was calculated to detect a clinically significant 67% reduction in the safety endpoint. Considering a 30% mortality rate in acute massive PE and 10% in acute high-risk submassive PE after thrombolysis, 177 patients (59 vs. 118) were required for 90% power at a two-sided alpha of 0.05, assuming 10% of cases would be non-evaluable. For research purposes, when the number of eligible patients with acute PE exceeded 177, only patients who underwent Indigo aspiration thrombectomy were included. Ultimately, 46 patients were analyzed.
Data are presented as mean ± standard deviation or as absolute numbers and percentages. Student’s t-test was used to determine p-values, with p < 0.05 considered statistically significant. Kaplan–Meier 90-day survival curves were used to compare the acute massive and high-risk submassive PE groups. All analyses were performed using SPSS version 30.0 (IBM Corp., Armonk, NY, USA).
3. Results
3.1 Baseline Clinical Characteristics
Table 1 summarizes the baseline clinical characteristics of the study population, classified as acute massive or high-risk submassive PE. The mean age at diagnosis was 59 ± 16 years, and most patients were female (67.4%). Chronic conditions present in > 10% of patients included deep vein thrombosis (56.5%), hypertension (41.3%), cancer (34.8%), diabetes mellitus (21.7%), surgery (21.7%), immobility (19.6%), and hemorrhage stroke (10.9%). Notably, one-third of patients had cancer.
Regarding severity assessment, there was no significant difference in the proportion of lesions located in the main pulmonary artery or bilaterally. Although acute massive PE appeared to carry a greater thrombus burden than high-risk submassive PE, this difference was not statistically significant (87.0 vs. 78.4, p = 0.05). Since acute massive PE is defined by a systolic blood pressure <90 mmHg at admission, it showed a strong positive correlation with the PE severity index clinical score (161.6 vs. 127.1, p = 0.003).
Due to obstructive shock in acute massive PE, thrombolytic therapy using the EkoSonic intravascular system (EKOS) was applied at a relatively high rate, supplemented by ECMO support. In contrast, the proportion of EKOS thrombolysis in patients with high-risk submassive PE was lower, reflecting contradictions to thrombolytic therapy, such as post-surgery status, hemorrhagic stroke, or recent ischemic stroke.
3.2 Follow-Up of Laboratory Tests on the Day of Admission
The results of laboratory tests are presented in Table 2. Blood counts were measured on the day of admission. Patients with the massive subtype had higher initial white blood cell counts than those with the high-risk submassive subtype, indicating a more pronounced stress-related systemic inflammatory response in acute massive PE (13.6 vs. 9.9 K/μL, p = 0.02). Regarding coagulation factors, patients with acute massive PE exhibited lower fibrinogen levels but higher D-dimer levels, suggesting a higher thrombotic burden than those with acute high-risk submassive PE.
Among the biochemical indices, markers related to heart and kidney function were significantly elevated in the patients with massive PE, reflecting early organ injury. Although acute massive PE is associated with a higher systemic inflammatory response, initial high-sensitivity C-reactive protein levels were comparable to those in submassive PE due to its delayed response characteristics.
3.3 Analyses of Indigo Thrombectomy Treatment Effect on Vital Signs and Right Heart Parameters
Table 3 summarizes the changes in vital signs and right heart parameters before and after thrombectomy. There were no statistically significant differences in blood pressure, heart rate, shock index, or respiratory rate before and after thrombectomy. However, the PaO₂ / FiO₂ ratio improved significantly after thrombectomy. Indigo aspiration thrombectomy significantly reduced PA systolic and mean pressures (from 57.2 to 44.3 mmHg, p = 0.01; from 35.0 to 26.8 mmHg, p < 0.001) and right atrial pressure (from 15.8 to 8.5 mmHg, p < 0.001). PA pulsatility index also increased markedly (from 2.2 to 3.3, p < 0.001). The RV/LV diameter ratio improved substantially, decreasing from 1.35 on pre-procedural computed tomography to 0.94 on follow-up echocardiography 48 h post-thrombectomy (p < 0.001). These improvements in right heart failure, including PA pressures, PA pulsatility index, and RV / LV ratio, are illustrated in Figure 2.
3.4 Clinical Outcomes after Indigo Thrombectomy
Table 4 presents the clinical outcomes following Indigo aspiration thrombectomy. Regarding vital signs, and consistent with the fundamental definition of massive APE, a significant proportion of patients with acute massive PE presented with elevated shock indices before thrombectomy. Concerning RV parameters, many patients with massive APE continued to show elevated PA pulsatility index and RV/LV diameter ratios after the procedure, indicating a limited response in terms of right heart failure improvement.
Patients with acute massive PE had a significantly higher incidence of major bleeding than those with acute submassive PE (31.3% vs. 3.3%, p = 0.007). No cases of intracranial hemorrhage or fatal bleeding occurred in either group.
Due to the high proportion of patients with cancer, the difference in 90-day all-cause mortality between the two groups was not statistically significant. In the acute massive PE group, one death involving a patient with metastatic endometrial cancer was excluded. In the acute high-risk submassive PE group, three cancer-related deaths were excluded (metastatic duodenal cancer, metastatic endometrial cancer, and ruptured hepatocellular carcinoma). After excluding these cases, the 90-day PE-related mortality rate remained significantly higher in the acute massive PE group than in the high-risk submassive PE group (25.0% vs. 3.3%, p = 0.02).
3.5 Ninety-day PE-related Survival Rate Analyzed by Kaplan–Meier Survival Curves
Figure 3 illustrates the Kaplan–Meier survival curves for patients with acute massive and acute high-risk submassive PE. The 90-day PE-related survival rate for patients with massive PE was 11/15 (73.3%), while that for patients with high-risk submassive PE was 26/27 (96.3%). Overall, patients with acute massive PE demonstrated significantly higher PE-related mortality than those with high-risk submassive PE (log-rank test p = 0.026).
4. Discussion
In this study, we evaluated potential treatment options to improve PE-related mortality in patients with acute massive or high-risk submassive PE beyond basic anticoagulation therapy. Indigo thrombectomy has been applied to alleviate right heart failure and is typically used for more severe PE. In acute massive PE, Indigo thrombectomy is often employed as a pre-thrombolytic adjunct, while in acute high-risk submassive PE, it can serve as a direct alternative to thrombolysis in patients at high bleeding risk [14].
Indigo continuous aspiration thrombectomy produces immediate hemodynamic improvements, including reductions in PA systolic and mean pressures [15,16], followed by improvement in the PaO2/FiO2 ratio [17]. RV-PA uncoupling, defined as reduced tricuspid annular plane systolic excursion with elevated PA systolic pressure resulting in a tricuspid annular plane systolic excursion/PA systolic pressure ratio < 0.4 [18], is alleviated by Indigo thrombectomy, which rapidly reduces PA systolic pressure while maintaining normal tricuspid annular plane systolic excursion. The PA pulsatility index, derived from the ratio of PA pulse pressure to right atrial pressure, reflects RV function [19]. By reducing right atrial pressure while maintaining PA pulse pressure, Indigo thrombectomy improves PA pulsatility index and mitigates the risk of right heart failure [20]. Following Indigo aspiration thrombectomy, both right atrial and ventricular pressures improve concurrently due to reductions in PA pressures. At 48-h follow-up, the RV/LV diameter ratio typically decreased by approximately 30% [21,22,23]; a ratio > 1 indicates high risk for right heart failure, while < 1 eliminates this risk [24].
In practice, catheter-directed thrombolysis has gradually replaced systemic thrombolysis to reduce the risk of cerebral hemorrhage, and percutaneous catheter aspiration thrombectomy has largely replaced surgical embolectomy to minimize vascular injury [25,26]. For acute massive PE, suction thrombectomy combined with thrombolysis is used to reduce bleeding and mortality, with ECMO (especially VA-ECMO) applied if obstructive shock occurs [27,28]. In this study, 56.3% of patients with acute massive PE received ECMO, including 50.0% VA-ECMO, 12.5% VAV-ECMO, and 12.5% VV-ECMO. Despite combined therapy, 90-day mortality decreased from >50% after heparinization alone to 15–45% after combined thrombolysis, with an average of 30% [29]. Acute high-risk submassive PE (such as RV/LV ratio >1) carries elevated mortality and often requires thrombolysis in addition to anticoagulation. Catheter-directed thrombolysis reduces 90-day mortality from >15% to 7–15% [30]. However, in certain situations, pharmaco-mechanical thrombectomy (such as Indigo aspiration thrombectomy) must be employed to reduce the risk of major hemorrhage associated with thrombolytic therapy. Contraindications to thrombolysis include post-surgery, hemorrhagic stroke, ischemic stroke within the preceding 6 months, malignant intracranial neoplasm, or active bleeding [31]. Patients with cancer face both hypercoagulability and bleeding risks due to an abnormally rich blood supply and tumor-related inflammation [32]. In this study, three patients had malignant hepatocellular carcinoma, three had endometrial cancer, two had lung cancer, two had tongue cancer, one had duodenal cancer, one had a malignant renal tumor, and one had a malignant intracranial neoplasm. Both patient groups exhibited elevated cardiac troponin I levels (> 0.04 ng/mL), indicating acute RV strain [33]. Overall, 87.5% of patients with acute massive PE and 46.7% patients with high-risk submassive PE had elevated troponin I levels.
In the acute massive PE group, the 90-day major bleeding rate was approximately 30%, and the 90-day PE-related mortality decreased from 30% to 25%. Subgroup analysis showed that combined Indigo thrombectomy and thrombolysis (10/16, 62.5%) had a PE-related mortality of 20.0%, whereas Indigo thrombectomy alone (6/16, 37.5%) had a PE-related mortality of 33.3%. These findings indicate that Indigo thrombectomy can further reduce mortality by 30% even when thrombolysis-related bleeding risk cannot be avoided. In the acute high-risk submassive PE group, the 90-day major bleeding rate decreased from 10% to 3%, and PE-related mortality decreased from 10% to 3%. Subgroup analysis showed that Indigo thrombectomy alone (21/30, 70%) had a PE-related mortality of 4.8%, while rescue thrombolysis following thrombectomy (9/30, 30%) had 0% mortality. These results indicate that Indigo thrombectomy not only reduces the risk of major bleeding but also lowers PE-related mortality when thrombolysis is contraindicated [34]. In summary, although thrombectomy and thrombolysis yield comparable all-cause mortality rates for acute massive and high-risk submassive PE, thrombectomy rapidly improves PA pressure and reduces right heart failure, resulting in superior PE-related survival [35].
This study has some limitations. First, despite achieving a sample size and statistical power of 90% for acute massive and high-risk submassive PE, Indigo aspiration thrombectomy still exhibits considerable selection bias, particularly among patients with cancer. Second, this study was conducted at a single center and may not be generalizable to other hospitals. Third, the influence of ECMO in massive PE remains unclear. Finally, prospective randomized studies are needed to verify these findings under specific circumstances.
5. Conclusions
In this study, Indigo aspiration thrombectomy substantially improves right heart failure and may help reduce PE-related mortality in patients with acute massive or high-risk submassive PE. For acute massive PE, Indigo aspiration thrombectomy can enhance therapeutic efficacy when thrombolytic therapy is insufficient. For acute high-risk submassive PE, when contraindications such as post-surgery, hemorrhagic stroke, recent ischemic stroke, malignant intracranial neoplasm, or active bleeding exist, Indigo aspiration thrombectomy can replace thrombolytic therapy with comparable efficacy.
Author Contributions
Conceptualization, YK. L.; methodology, YK. L. and DL. C.; data curation, YK. L., KY. L, LC. H, and CC. W; formal analysis, DL. C.; investigation, YK. L. and HW. C.; writing – original draft, YK. L.; writing – review and editing, DL. C.; supervision, AS. L., CH. H., and KC. C. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
This study was approved by the Institutional Review Board of China Medical University Hospital (CMUH114-REC3-201) for data collection and analysis.
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study.
Data Availability Statement
The original contributions presented in this study are included in the article, and further inquiries can be directed to the corresponding authors.
Acknowledgments
All authors thank Dr. Ching-Yi Chou, Dr. Wen-De Tang, and Dr. Kee-Koon Ng at China Medical University Hospital for their excellent clinical team support.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ECMO | Extracorporeal membrane oxygenation |
| EKOS | EkoSonic endovascular system |
| FiO2 | Fraction of inspired oxygen |
| LV | Left ventricular |
| PA | Pulmonary artery |
| PE | Pulmonary embolism |
| PaO2 | Partial pressure of arterial oxygen |
| RV | Right ventricular |
References
- Hsu, S.H.; Ko, C.H.; Chou, E.H.; Herrala, J.; Lu, T.C.; Wang, C.H.; Chang, W.T.; Huang, C.H.; Tsai, C.L. Pulmonary embolism in United States emergency departments, 2010–2018. Sci Rep 2023, 13, 9070. [Google Scholar] [CrossRef] [PubMed]
- Freund, Y.; Cohen-Aubart, F.; Bloom, B. Acute pulmonary embolism: A review. JAMA 2022, 328, 1336–1345. [Google Scholar] [CrossRef]
- Bottega, T.S.; Vier, M.G.; Baldiaserotto, H.; Oliveira, E.P.; Diaz, C.L.M.; Fernandes, C.J. Thrombolysis in acute pulmonary embolism. Rev Assoc Med Bras 1992, 2020(66), 263–267. [Google Scholar] [CrossRef]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.J.; Harjola, V.P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J 2020, 41, 543–603. [Google Scholar] [CrossRef]
- Gupta, R.; Ammari, Z.; Dasa, O.; Ruzieh, M.; Burlen, J.J.; Shunnar, K.M.; Nguyen, H.T.; Xie, Y.; Brewster, P.; Chen, T.; et al. Long-term mortality after massive, submassive, and low-risk pulmonary embolism. Vasc Med 2020, 25, 141–149. [Google Scholar] [CrossRef]
- Polaková, E.; Veselka, J. Management of massive pulmonary embolism. Int J Angiol 2022, 31, 194–197. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.U.; Cho, Y.D.; Choi, S.H.; Yoon, Y.H.; Park, J.H.; Park, S.J.; Lee, E.S. Assessing the severity of pulmonary embolism among patients in the emergency department: Utility of RV/LV diameter ratio. PLOS One 2020, 15, e0242340. [Google Scholar] [CrossRef] [PubMed]
- Kolkailah, A.A.; Hirji, S.; Piazza, G.; Ejiofor, J.I.; Ramirez Del Val, F.; Lee, J.; McGurk, S.; Aranki, S.F.; Shekar, P.S.; Kaneko, T. Surgical pulmonary embolectomy and catheter-directed thrombolysis for treatment of submassive pulmonary embolism. J Card Surg 2018, 33, 252–259. [Google Scholar] [CrossRef]
- Secemsky, E.; Chang, Y.; Jain, C.C.; Beckman, J.A.; Giri, J.; Jaff, M.R.; Rosenfield, K.; Rosovsky, R.; Kabrhel, C.; Weinberg, I. Contemporary management and outcomes of patients with massive and submassive pulmonary embolism. Am J Med 2018, 131, 1506–1514.e0. [Google Scholar] [CrossRef]
- Raza, H.A.; Horowitz, J.; Yuriditsky, E. Indigo aspiration system for thrombectomy in pulmonary embolism. Future Cardiol 2023, 19, 469–475. [Google Scholar] [CrossRef]
- Iannaccone, M.; Sławek-Szmyt, S.; Gamardella, M.; Fumarola, F.; Mangione, R.; Savio, D.; Russo, F.; Boccuzzi, G.; Araszkiewicz, A.; Chieffo, A. The role of pulmonary artery pulsatility index to assess the outcomes following catheter directed therapy in patients with intermediate-to-high and high-risk pulmonary embolism. Cardiovasc Revasc Med 2025, S1553-8389(25)00044-2. [Google Scholar] [CrossRef]
- Lerche, M.; Bailis, N.; Akritidou, M.; Meyer, H.J.; Surov, A. Pulmonary vessel obstruction does not correlate with severity of pulmonary embolism. J Clin Med 2019, 8, 584. [Google Scholar] [CrossRef]
- Natanzon, S.S.; Fardman, A.; Chernomordik, F.; Mazin, I.; Herscovici, R.; Goitein, O.; Ben-Zekry, S.; Younis, A.; Grupper, A.; Matetzky, S.; et al. PESI score for predicting clinical outcomes in PE patients with right ventricular involvement. Heart Vessels 2022, 37, 489–495. [Google Scholar] [CrossRef]
- Al Soueidy, A.; Miller, G.; Hussain, S.; Rachoin, J.S.; Hunter, K.; Iliadis, E. Aspiration thrombectomy compared to catheter directed thrombolysis in pulmonary embolism: Outcomes from a tertiary referral center. Cardiol J 2025, 32, 347–356. [Google Scholar] [CrossRef] [PubMed]
- Chandra, V.M.; Khaja, M.S.; Kryger, M.C.; Sista, A.K.; Wilkins, L.R.; Angle, J.F.; Sharma, A.M. Mechanical aspiration thrombectomy for the treatment of pulmonary embolism: A systematic review and meta-analysis. Vasc Med 2022, 27, 574–584. [Google Scholar] [CrossRef]
- Leong, D.W.; Ayadi, B.; Dexter, D.J.; Rosenberg, M.; Horowitz, J.M.; Chuang, M.L.; Dohad, S. Continuous mechanical aspiration thrombectomy performs equally well in main versus branch pulmonary emboli: A subgroup analysis of the EXTRACT-PE trial. Catheter Cardiovasc Interv 2023, 101, 468–475. [Google Scholar] [CrossRef]
- Calé, R.; Pereira, A.R.; Ferreira, F.; Alegria, S.; Morgado, G.; Martins, C.; Ferreira, M.; Gomes, A.; Judas, T.; Gonzalez, F.; et al. Continuous Aspiration Mechanical Thrombectomy for the management of intermediate- and high-risk pulmonary embolism: Data from the first cohort in Portugal. Rev Port Cardiol 2022, 41, 533–545. [Google Scholar] [CrossRef]
- Zeba, F.; Singh, I.; Gomez, J.; Khosla, A. Right ventricular-pulmonary arterial uncoupling thresholds in acute pulmonary embolism. Lung 2025, 203, 71. [Google Scholar] [CrossRef] [PubMed]
- Moady, G.; Mobarki, L.; Or, T.; Shturman, A.; Atar, S. Echocardiography-based pulmonary artery pulsatility index correlates with outcomes in patients with acute pulmonary embolism. J Clin Med 2025, 14, 2685. [Google Scholar] [CrossRef] [PubMed]
- Iannaccone, M.; Gamardella, M.; Fumarola, F.; Mangione, R.; Botti, G.; Russo, F.; Boccuzzi, G. Pulmonary artery pulsatility index evaluation in intermediate-to-high and high-risk pulmonary embolism patients underwent transcatheter intervention. Eur Heart J 2024, 45 (Suppl 1), ehae666.2324. [Google Scholar] [CrossRef]
- Sista, A.K.; Horowitz, J.M.; Tapson, V.F.; Rosenberg, M.; Elder, M.D.; Schiro, B.J.; Dohad, S.; Amoroso, N.E.; Dexter, D.J.; Loh, C.T.; et al. Indigo aspiration system for treatment of pulmonary embolism: Results of the EXTRACT-PE trial. JACC Cardiovasc Interv 2021, 14, 319–329. [Google Scholar] [CrossRef]
- Moriarty, J.M.; Dohad, S.Y.; Schiro, B.J.; Tamaddon, H.; Heithaus, R.E.; Iliadis, E.A.; Dexter, D.J.; Shavelle, D.M.; Leal, S.R.N.; Attallah, A.S.; et al. Clinical, functional, and quality-of-life outcomes after computer assisted vacuum thrombectomy for pulmonary embolism: Interim analysis of the STRIKE-PE Study. J Vasc Interv Radiol 2024, 35, 1154–1165.e6. [Google Scholar] [CrossRef] [PubMed]
- Sławek-Szmyt, S.; Stępniewski, J.; Kurzyna, M.; Kuliczkowski, W.; Jankiewicz, S.; Kopeć, G.; Darocha, S.; Mroczek, E.; Pietrasik, A.; Grygier, M.; et al. Catheter-directed mechanical aspiration thrombectomy in a real-world pulmonary embolism population: A multicenter registry. Eur Heart J Acute Cardiovasc Care 2023, 12, 584–593. [Google Scholar] [CrossRef]
- Zhang, R.S.; Yuriditsky, E.; Truong, H.P.; Zhang, P.; Greco, A.A.; Elbaum, L.; Mukherjee, V.; Hena, K.; Postelnicu, R.; Alviar, C.L.; et al. Real-time risk stratification in acute pulmonary embolism: The utility of RV/LV diameter ratio. Thromb Res 2025, 250, 109323. [Google Scholar] [CrossRef]
- Warren, B.E.; Tan, K.T.; Jaberi, A.; Donahoe, L.; de Perrot, M.; McInnis, M.C.; Granton, J.T.; Mafeld, S. Procedure-related mortality in aspiration thrombectomy for pulmonary embolism: A MAUDE Database Analysis of the Inari FlowTriever and Penumbra indigo Systems. J Endovasc Ther 2024, 15266028241307848. [Google Scholar] [CrossRef]
- Cueto-Robledo, G.; Rivera-Sotelo, N.; Roldan-Valadez, E.; Narvaez-Oriani, C.A.; Cueto-Romero, H.D.; Gonzalez-Hermosillo, L.M.; Hidalgo-Alvarez, M.; Barrera-Jimenez, B. A brief review on failed hybrid treatment for massive pulmonary embolism: Catheter-directed thrombolysis (CDT) and pharmaco-mechanical thrombolysis (PMT). Curr Probl Cardiol 2022, 47, 101294. [Google Scholar] [CrossRef] [PubMed]
- Glazier, H.A.; Kaki, A. Role of extracorporeal membrane oxygenation in the treatment of massive pulmonary embolism. Int J Angiol 2024, 33, 107–111. [Google Scholar] [CrossRef]
- Munagala, R.; Patel, H.; Sathe, P.; Singh, A.; Narasimhan, M. The use of veno-arterial extracorporeal membrane oxygenation (VA-ECMO) for acute high risk pulmonary embolism: A systematic review. Curr Cardiol Rev 2025, 21, e1573403X339627, e1573403. [Google Scholar] [CrossRef] [PubMed]
- Silver, M.J.; Giri, J.; Duffy, Á.; Jaber, W.A.; Khandhar, S.; Ouriel, K.; Toma, C.; Tu, T.; Horowitz, J.M. Incidence of mortality and complications in high-risk pulmonary embolism: A systematic review and meta-analysis. J Soc CardioVasc Angiogr Interv 2023, 2, 100548. [Google Scholar] [CrossRef]
- Zhang, R.S.; Maqsood, M.H.; Sharp, A.S.P.; Postelnicu, R.; Sethi, S.S.; Greco, A.; Alviar, C.; Bangalore, S. Efficacy and safety of anticoagulation, catheter-directed thrombolysis, or systemic thrombolysis in acute pulmonary embolism. JACC Cardiovasc Interv 2023, 16, 2644–2651. [Google Scholar] [CrossRef]
- Pieraccini, M.; Guerrini, S.; Laiolo, E.; Puliti, A.; Roviello, G.; Misuraca, L.; Spargi, G.; Limbruno, U.; Breggia, M.; Grechi, M. Acute massive and submassive pulmonary embolism: Preliminary validation of aspiration mechanical thrombectomy in patients with contraindications to thrombolysis. Cardiovasc Intervent Radiol 2018, 41, 1840–1848. [Google Scholar] [CrossRef]
- Mai, A.S.; Matetić, A.; Elgendy, I.Y.; Lopez-Mattei, J.; Kotronias, R.A.; Sun, L.Y.; Yong, J.H.; Bagur, R.; Van Spall, H.G.C.; Mamas, M.A. The association between cancer diagnosis, care, and outcomes in 1 million patients hospitalized for acute pulmonary embolism. Int J Cardiol 2023, 371, 354–362. [Google Scholar] [CrossRef]
- Yang, L.; Li, B.; Chen, H.; Belfeki, N.; Monchi, M.; Moini, C. The role of troponin in the diagnosis and treatment of acute pulmonary embolism: Mechanisms of elevation, prognostic evaluation, and clinical decision-making. Cureus 2024, 16, e67922. [Google Scholar] [CrossRef] [PubMed]
- Tsukagoshi, J.; Wick, B.; Karim, A.; Khanipov, K.; Cox, M.W. Perioperative and intermediate outcomes of patients with pulmonary embolism undergoing catheter-directed thrombolysis vs percutaneous mechanical thrombectomy. J Vasc Surg Venous Lymphat Disord 2024, 12, 101958. [Google Scholar] [CrossRef] [PubMed]
- Jaber, W.A.; Gonsalves, C.F.; Stortecky, S.; Horr, S.; Pappas, O.; Gandhi, R.T.; Pereira, K.; Giri, J.; Khandhar, S.J.; Ammar, K.A.; et al. Large-bore mechanical thrombectomy versus catheter-directed thrombolysis in the management of intermediate-risk pulmonary embolism: Primary results of the Peerless randomized controlled trial. Circulation 2025, 151, 260–273. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
STROBE flow chart for patients with acute massive or high-risk submassive PE. A total of 179 adult patients with acute massive or high-risk submassive PE hospitalized between January 2020 and August 2025 were screened for evaluation. Patients who did not undergo Indigo thrombectomy were excluded from the study. A total of 46 patients were ultimately included in the statistical analysis. Given the large proportion of patients with cancer, cases in which cancer was the cause of death were excluded to focus on Kaplan–Meier survival analysis on acute PE. K-M, Kaplan‒Meier; PE, pulmonary embolism; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology.
Figure 1.
STROBE flow chart for patients with acute massive or high-risk submassive PE. A total of 179 adult patients with acute massive or high-risk submassive PE hospitalized between January 2020 and August 2025 were screened for evaluation. Patients who did not undergo Indigo thrombectomy were excluded from the study. A total of 46 patients were ultimately included in the statistical analysis. Given the large proportion of patients with cancer, cases in which cancer was the cause of death were excluded to focus on Kaplan–Meier survival analysis on acute PE. K-M, Kaplan‒Meier; PE, pulmonary embolism; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology.
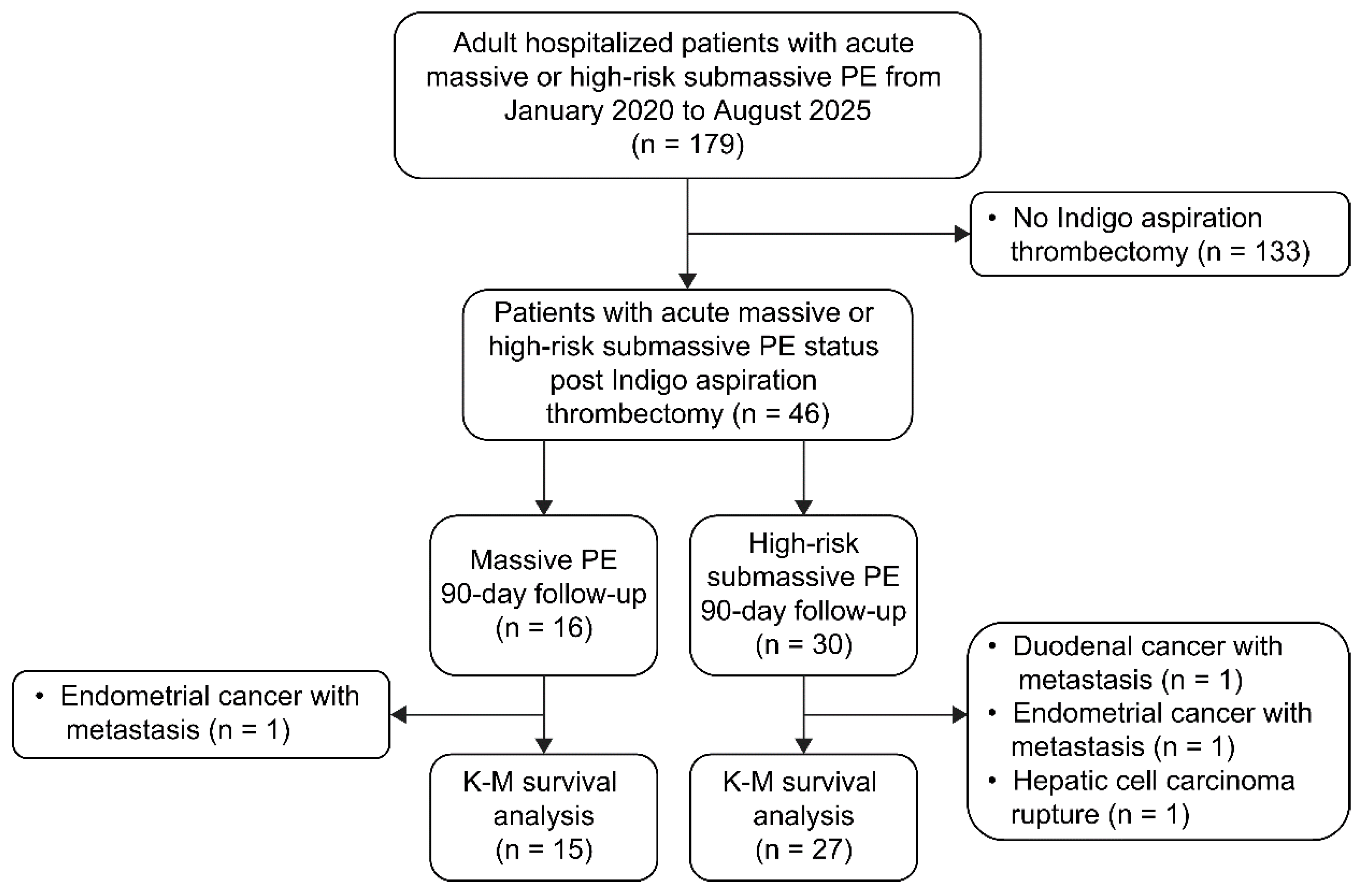
Figure 2.
(A) Reduction in PA systolic pressure by 23% (from 57.2 to 44.3 mmHg, p = 0.001) before and after thrombectomy; (B) Reduction in PA mean pressure by 23% (from 35.0 to 26.8, p < 0.001) before and after thrombectomy; (C) Increase in PA pulsatility index by 50% (from 2.2 to 3.3, p < 0.001) before and after thrombectomy; (D) Reduction in RV/LV diameter ratio by 30% (from 1.35 to 0.94, p < 0.001) between baseline and 48 h post-thrombectomy. Abbreviations: PA, pulmonary artery; RV, right ventricle; LV, left ventricle; RV/LV, right ventricular–to–left ventricular diameter ratio.
Figure 2.
(A) Reduction in PA systolic pressure by 23% (from 57.2 to 44.3 mmHg, p = 0.001) before and after thrombectomy; (B) Reduction in PA mean pressure by 23% (from 35.0 to 26.8, p < 0.001) before and after thrombectomy; (C) Increase in PA pulsatility index by 50% (from 2.2 to 3.3, p < 0.001) before and after thrombectomy; (D) Reduction in RV/LV diameter ratio by 30% (from 1.35 to 0.94, p < 0.001) between baseline and 48 h post-thrombectomy. Abbreviations: PA, pulmonary artery; RV, right ventricle; LV, left ventricle; RV/LV, right ventricular–to–left ventricular diameter ratio.
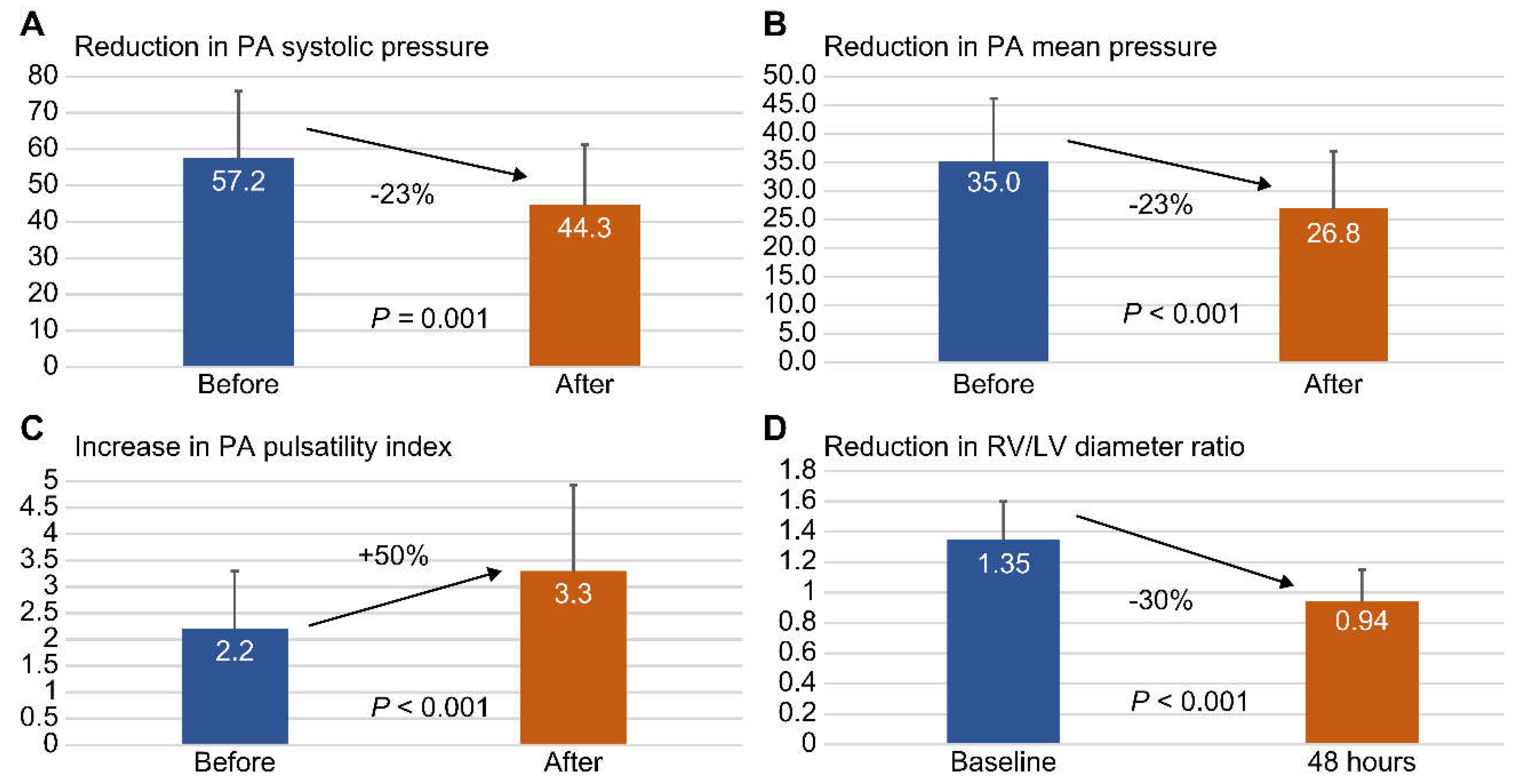
Figure 3.
Kaplan–Meier 90-day PE-related survival in patients with acute massive and high-risk submassive PE. The 90-day survival rate was 11/15 (73.3%) for acute massive PE and 26/27 (96.3%) for high-risk submassive PE. Patients with acute massive PE had a significantly higher PE-related mortality than those with high-risk submassive PE (log-rank test p = 0.026). Abbreviations: PE, pulmonary embolism.
Figure 3.
Kaplan–Meier 90-day PE-related survival in patients with acute massive and high-risk submassive PE. The 90-day survival rate was 11/15 (73.3%) for acute massive PE and 26/27 (96.3%) for high-risk submassive PE. Patients with acute massive PE had a significantly higher PE-related mortality than those with high-risk submassive PE (log-rank test p = 0.026). Abbreviations: PE, pulmonary embolism.
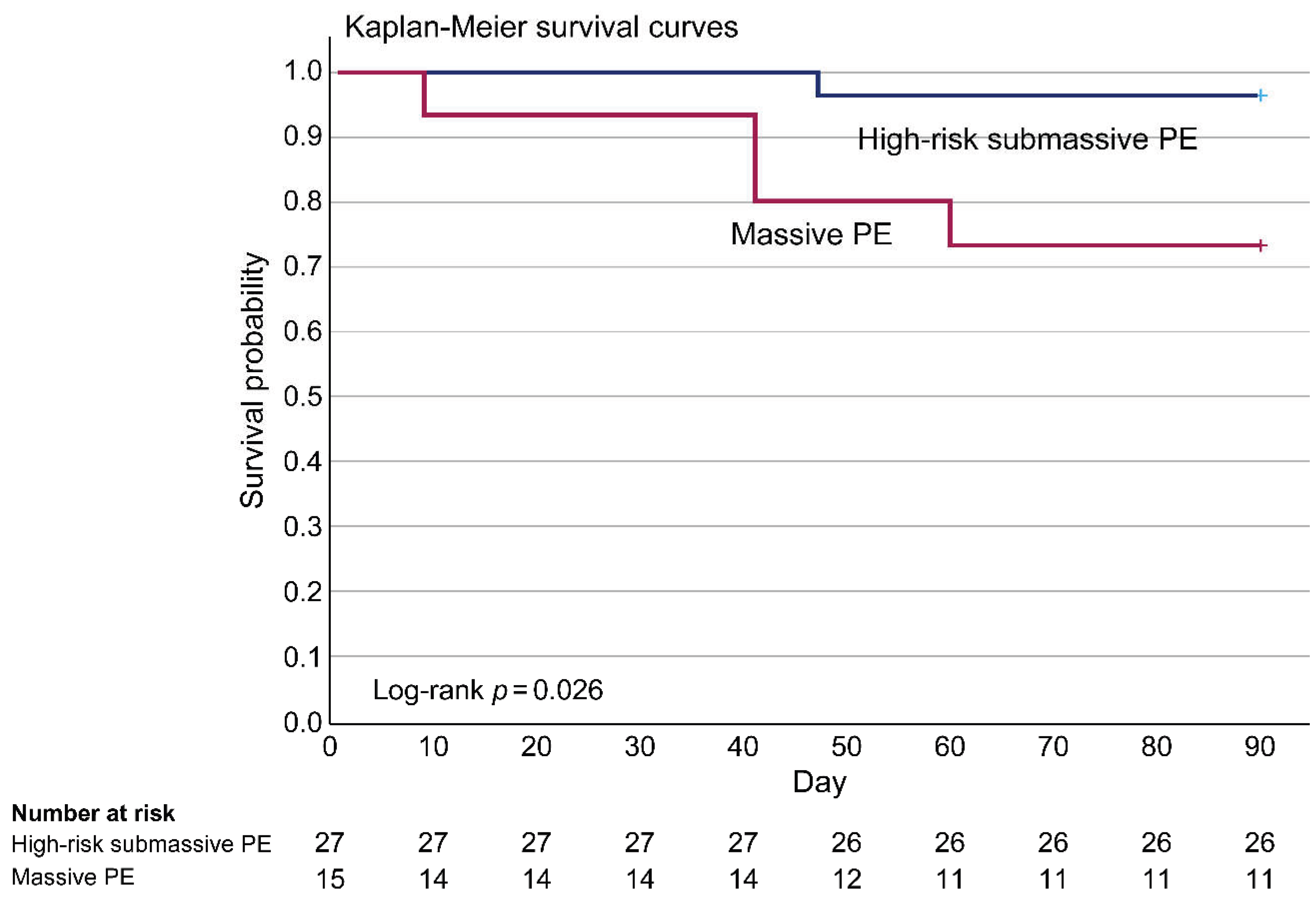

Table 1.
Baseline clinical characteristics of study participants by pulmonary embolism type (massive vs. high-risk submassive)
Table 1.
Baseline clinical characteristics of study participants by pulmonary embolism type (massive vs. high-risk submassive)
| All (n = 46) |
Massive PE (n = 16) |
High-risk submassive PE (n = 30) |
p-value | |
|---|---|---|---|---|
| Age (y), mean ± SD | 59 ± 16 | 61 ± 15 | 55 ± 19 | 0.21 |
| Female sex, n (%) | 31 (67.4) | 12 (75.0) | 19 (63.3) | 0.43 |
| Body mass index (kg/m2), mean ± SD | 27.4 ± 6.3 | 26.5 ± 5.9 | 27.9 ± 6.5 | 0.50 |
| Chronic disease | ||||
| Pregnancy, n (%) | 20 (4.3) | 1 (6.3) | 1 (3.3) | 0.65 |
| Smoking, n (%) | 4 (8.7) | 1 (6.3) | 3 (10.0) | 0.68 |
| Surgery, n (%) | 10 (21.7) | 2 (12.5) | 8 (26.7) | 0.28 |
| Immobility, n (%) | 9 (19.6) | 3 (18.8) | 6 (20.0) | 0.92 |
| Atrial fibrillation, n (%) | 2 (4.3) | 0 (0.0) | 2 (6.7) | 0.30 |
| Diabetes mellitus, n (%) | 10 (21.7) | 5 (31.3) | 5 (16.7) | 0.26 |
| Hypertension, n (%) | 19 (41.3) | 9 (56.3) | 10 (33.3) | 0.14 |
| Coronary artery disease, n (%) | 2 (4.3) | 0 (0.0) | 2 (6.7) | 0.30 |
| Cancer, n (%) | 16 (34.8) | 3 (18.8) | 13 (43.3) | 0.10 |
| Heart failure, n (%) | 2 (4.3) | 1 (6.3) | 1 (3.3) | 0.65 |
| Hemorrhagic stroke, n (%) | 5 (10.9) | 1 (6.3) | 4 (13.3) | 0.47 |
| Ischemic stroke, n (%) | 3 (6.5) | 1 (6.3) | 2 (6.7) | 0.96 |
| Autoimmune disease, n (%) | 3 (6.5) | 2 (12.5) | 1 (3.3) | 0.24 |
| Deep vein thrombosis, n (%) | 26 (56.5) | 7 (43.8) | 19 (63.3) | 0.21 |
| Severity evaluation | ||||
| Main trunk or bilateral, n (%) | 23 (50.0) | 9 (56.3) | 14 (46.7) | 0.55 |
| Mastora obstruction index, mean ± SD | 81.4 ± 14.1 | 87.0 ± 12.0 | 78.4 ± 14.4 | 0.05 |
| PE severity index at admission, mean ± SD | 139.1 ± 39.2 | 161.6 ± 35.5 | 127.1 ± 36.1 | 0.003 |
| Additional procedure | ||||
| Surgical embolectomy, n (%) | 0 (0) | 0 (0) | 0 (0) | - |
| Systemic thrombolysis, n (%) | 0 (0) | 0 (0) | 0 (0) | - |
| Catheter-directed thrombolysis, n (%) | 21 (45.7) | 10 (62.5) | 9 (30.0) | 0.03 |
| EkoSonic endovascular system, n (%) | 24 (52.2) | 12 (75.0) | 12 (40.0) | 0.02 |
| ECMO, n (%) | 9 (19.6) | 9 (56.3) | 0 (0.0) | <0.001 |
| Inferior vena cava filter, n (%) | 37 (80.4) | 11 (68.8) | 26 (86.7) | 0.15 |
ECMO, extracorporeal membrane oxygenation; PE, pulmonary embolism; SD, standard deviation.
Table 2.
Baseline blood counts and biochemical indices of study participants, depending on the presence of massive pulmonary embolism
Table 2.
Baseline blood counts and biochemical indices of study participants, depending on the presence of massive pulmonary embolism
| All (n = 46) |
Massive PE (n = 16) |
High-risk submassive PE (n = 30) |
p-value | |
|---|---|---|---|---|
| Blood counts | ||||
| WBC (K/μL), mean ± SD | 11.2 ± 5.2 | 13.6 ± 4.9 | 9.9 ± 5.0 | 0.02 |
| Hemoglobin (%), mean ± SD | 11.4 ± 2.1 | 12.1 ± 2.1 | 11.0 ± 2.1 | 0.09 |
| Platelet (K/μL), mean ± SD | 232.2 ± 152.9 | 183.0 ± 95.8 | 258.4 ± 171.7 | 0.11 |
| Coagulation factors | ||||
| Fibrinogen (mg/dL), mean ± SD | 302.1 ± 123.5 | 238.6 ± 69.3 | 335.9 ± 133.2 | 0.009 |
| D-dimer (ng/mL), mean ± SD | 25315.1 ± 26166.4 | 37310.4 ± 29480.9 | 18917.6 ± 22162.1 | 0.02 |
| Biochemical indices | ||||
| Troponin-I (ng/mL), mean ± SD | 0.33 ± 0.60 | 0.65 ± 0.83 | 0.15 ± 0.31 | 0.005 |
| Troponin-I > 0.04 ng/mL, n (%) | 28 (60.9) | 14 (87.5) | 14 (46.7) | 0.006 |
| eGFR (mL/min), mean ± SD | 80.5 ± 39.5 | 57.6 ± 26.4 | 93.6 ± 40.0 | 0.003 |
| hsCRP (mg/dL), mean ± SD | 4.7 ± 5.3 | 4.5 ± 4.8 | 4.8 ± 5.7 | 0.86 |
hsCRP, high-sensitivity C-reactive protein; eGFR, estimated glomerular filtration rate; PE, pulmonary embolism; SD, standard deviation; WBC, white blood cells.
Table 3.
Treatment effects of Indigo thrombectomy on study participants with pulmonary embolism
| Before thrombectomy (n = 46) |
After thrombectomy (n = 46) |
p-value | |
|---|---|---|---|
| Vital signs | |||
| Systolic blood pressure, mean ± SD | 119.3 ± 23.1 | 125.7 ± 23.0 | 0.19 |
| Mean artery pressure, mean ± SD | 89.5 ± 16.7 | 92.4 ± 14.9 | 0.37 |
| Diastolic blood pressure, mean ± SD | 74.6 ± 15.5 | 75.8 ± 14.6 | 0.69 |
| Heart rate, mean ± SD | 100.8 ± 23.1 | 96.9 ± 21.1 | 0.40 |
| Shock index, mean ± SD | 0.88 ± 0.30 | 0.81 ± 0.29 | 0.22 |
| Respiratory rate, mean ± SD | 22.0 ± 5.7 | 20.0 ± 4.4 | 0.06 |
| PaO2 / FiO2 ratio, mean ± SD | 137.3 ± 57.6 | 270.6 ± 84.5 | <0.001 |
| Right heart parameters | |||
| PA systolic pressure, mean ±SD | 57.2 ± 18.8 | 44.3 ± 16.9 | 0.001 |
| PA mean pressure, mean ± SD | 35.0 ± 11.1 | 26.8 ± 10.1 | <0.001 |
| PA diastolic pressure, mean ± SD | 23.9 ± 9.6 | 18.1 ± 8.7 | 0.003 |
| Right atrial pressure, mean ± SD | 15.8 ± 4.9 | 8.5 ± 3.2 | <0.001 |
| PA pulsatility index, mean ± SD | 2.2 ± 1.1 | 3.3 ± 1.6 | <0.001 |
| RV / LV diameter ratio, mean ± SD | 1.35 ± 0.25 | 0.94 ± 0.21 | <0.001 |
FiO2, fraction of inspired oxygen; LV, left ventricular; PA, pulmonary artery; PaO2, partial pressure of arterial oxygen; RV, right ventricular; SD, standard deviation.
Table 4.
Clinical outcomes of study participants depending on the presence of massive pulmonary embolism
Table 4.
Clinical outcomes of study participants depending on the presence of massive pulmonary embolism
|
All (n = 46) |
Massive PE (n = 16) |
High-risk submassive PE (n = 30) |
p-value | ||
| Vital signs | |||||
| Mean artery pressure before thrombectomy, mean ± SD | 89.5 ± 16.7 | 80.6 ± 17.0 | 94.2 ± 14.7 | 0.007 | |
| Mean artery pressure after thrombectomy, mean ± SD | 92.4 ± 14.9 | 89.5 ± 16.2 | 94.0 ± 14.2 | 0.33 | |
| Shock index before thrombectomy, mean ± SD | 0.88 ± 0.30 | 1.11 ± 0.35 | 0.76 ± 0.18 | <0.001 | |
| Shock index after thrombectomy, mean ± SD | 0.81 ± 0.29 | 0.92 ± 0.40 | 0.75 ± 0.20 | 0.06 | |
| PaO2 / FiO2 ratio before thrombectomy, mean ± SD | 137.3 ± 57.6 | 128.4 ± 59.1 | 142.1 ± 57.2 | 0.45 | |
| PaO2 / FiO2 ratio after thrombectomy, mean ± SD | 270.6 ± 84.5 | 272.1 ± 97.4 | 269.8 ± 78.6 | 0.93 | |
| Right heart parameters | |||||
| PA mean pressure before thrombectomy, mean ± SD | 35.0 ± 11.1 | 39.1 ± 12.1 | 32.8 ± 10.0 | 0.07 | |
| PA mean pressure after thrombectomy, mean ± SD | 26.8 ± 10.1 | 28.3 ± 10.4 | 26.0 ± 10.1 | 0.47 | |
| PA pulsatility index before thrombectomy, mean ± SD | 2.2 ± 1.1 | 2.0 ± 0.9 | 2.3 ± 1.2 | 0.30 | |
| PA pulsatility index after thrombectomy, mean ± SD | 3.3 ± 1.6 | 3.7 ± 1.6 | 2.6 ± 1.2 | 0.02 | |
| RV / LV diameter ratio before thrombectomy, mean ± SD | 1.35 ± 0.25 | 1.44 ± 0.2 | 1.29 ± 0.24 | 0.06 | |
| RV / LV diameter ratio after thrombectomy, mean ± SD | 0.94 ± 0.21 | 1.05 ± 0.2 | 0.88 ± 0.19 | 0.01 | |
| Major bleeding | |||||
| BARC 3B bleeding, n (%) | 6 (13.0) | 5 (31.3) | 1 (3.3) | 0.007 | |
| BARC 3C bleeding, n (%) | 0 (0.0) | 0 (0.0) | 0 (0.0) | - | |
| BARC 5 bleeding, n (%) | 0 (0.0) | 0 (0.0) | 0 (0.0) | - | |
| Mortality | |||||
| 90-day all-cause mortality, n (%) | 9 (19.6) | 5 (31.3) | 4 (13.3) | 0.15 | |
| 90-day PE-related mortality, n (%) | 5 (10.9) | 4 (25.0) | 1 (3.3) | 0.02 | |
BARC, bleeding academic research consortium; FiO2, fraction of inspired oxygen; LV, left ventricular; PaO2, partial pressure of arterial oxygen; PA, pulmonary artery; PE, pulmonary embolism; RV, right ventricular; SD, standard deviation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



