Submitted:
11 December 2025
Posted:
14 December 2025
You are already at the latest version
Abstract
Breast cancer remains the most prevalent malignancy among women worldwide, with chemotherapy serving as a cornerstone of treatment across neoadjuvant, adjuvant, and metastatic settings. While chemotherapy improves survival, it frequently imposes significant physical, psychological, and socioeconomic burdens that compromise quality of life (QoL). This review synthesizes current evidence on the impact of breast cancer chemotherapy on QoL, encompassing physical symptoms (fatigue, neuropathy, gastrointestinal distress), emotional disturbances (depression, anxiety, cognitive impairment), social challenges (relationship strain, loss of productivity), and financial toxicity. The heterogeneity of these effects is influenced by factors such as age, menopausal status, disease stage, socioeconomic background, and racial disparities. Key chemotherapeutic agents—including anthracyclines, taxanes, and platinum compounds—are discussed alongside their mechanisms and toxicity profiles. The review also highlights the importance of patient-reported outcomes (PROs) in accurately assessing QoL and guiding supportive care. Interventions such as physical rehabilitation, psychosocial support, pharmacological management, and nutritional therapies are explored as strategies to mitigate treatment burden. As breast cancer survivorship grows, integrating QoL considerations into oncologic decision-making is essential to optimize both clinical outcomes and patient well-being.
Keywords:
breast cancer
; quality of life
; antineoplastic agents
; chemotherapy
; patient reported outcome measures
; medical oncology
1. Introduction
Breast cancer remains the most commonly diagnosed cancer in women worldwide, with over 2.3 million new cases annually and representing a leading cause of cancer-related mortality globally [1]. Chemotherapy plays a critical role in the multimodal management of breast cancer, including neoadjuvant (pre-surgical), adjuvant (post-surgical), and metastatic treatment settings. Neoadjuvant chemotherapy is often used to downstage tumors, enabling breast-conserving surgery and providing prognostic information based on tumor response [2,3]. Studies have shown that patients achieving pathological complete response (pCR) after neoadjuvant chemotherapy have significantly improved long-term outcomes [4]. In comparison, adjuvant chemotherapy is administered to eradicate microscopic residual disease after surgery and is a standard component in early-stage, high-risk cases [5]. As breast cancer survival improves due to advances in such systemic therapies, there is increasing emphasis on the long-term well-being of survivors. While these therapies significantly improve disease-free survival (DFS) and overall survival (OS), they are not without adverse effects, which can impair patient quality of life (QoL). Chemotherapy is associated with various side effects—including fatigue, neuropathy, cognitive impairment, and emotional distress—that can significantly diminish QoL during and after treatment [6,7]. Moreover, these effects may persist long after treatment completion, affecting return to work, social relationships, and psychological well-being. In clinical trials such as KEYNOTE-522, patient-reported outcomes (PROs) indicated measurable declines in physical and emotional functioning during both neoadjuvant and adjuvant chemotherapy phases [8]. These findings highlight the need for comprehensive QoL monitoring throughout the treatment continuum. The aim of this review is to evaluate the current evidence on how chemotherapy for breast cancer affects patient-reported and clinically assessed QoL across different treatment stages. By exploring both the short- and long-term consequences of chemotherapy on various QoL domains, this article seeks to inform clinicians, researchers, and policymakers about the trade-offs between survival benefits and lived experiences.
2. Impact of Chemotherapy on Physical Domain of QoL
2.1. Fatigue and Physical Functioning
CRF is among the most frequently reported and distressing side effects of chemotherapy in breast cancer patients, with significant implications for physical functioning and QoL. Unlike normal tiredness, CRF is persistent, not alleviated by rest, and affects daily living, physical activity, cognition, and psychosocial well-being [9]. Studies consistently report that more than 40% of breast cancer patients undergoing chemotherapy experience clinically significant fatigue [10,11,12]. This prevalence is highest during treatment, where cumulative toxicity, inflammation, and anemia compound the sensation of exhaustion. CRF affects all subgroups of patients but is especially pronounced in those receiving anthracycline-taxane combinations, older adults, and individuals with comorbid depression or anemia. While some relief from fatigue occurs shortly after chemotherapy ends, for many patients, symptoms persist for months or even years [13]. Longitudinal data indicate that up to 60% of survivors report ongoing fatigue one year post-treatment, and a notable subset experiences chronic fatigue that remains unresolved even after five years [13]. This prolonged fatigue impairs return to work, exercise tolerance, and social reintegration, further exacerbating emotional distress and reducing long-term QoL [14]. Fatigue leads to reduced physical functioning, which can manifest as decreased endurance, muscle weakness, and slower recovery after physical exertion. Patients commonly report difficulty walking, climbing stairs, or performing basic household activities. These impairments are often compounded by deconditioning, which may begin during treatment and continue post-therapy due to avoidance of physical activity. The resulting cycle of inactivity and fatigue contributes to functional decline and, in older patients, increases the risk of frailty and falls [15,16,17].
2.2. Neuropathy and Pain
CIPN is a common and often debilitating side effect of taxane- and platinum-based chemotherapies used in breast cancer treatment. It arises from cumulative damage to sensory neurons in the peripheral nervous system, leading to symptoms such as numbness, tingling, burning pain, and loss of coordination, particularly in the hands and feet. CIPN not only reduces physical function but can also lead to chronic pain, psychological distress, and treatment modification, ultimately compromising both QoL and therapeutic outcomes. CIPN occurs in approximately 60–70% of cancer patients during chemotherapy, particularly with agents like paclitaxel and docetaxel [18,19]. Although some symptoms resolve after treatment ends, up to 30–40% of patients experience persistent neuropathy for months or even years, with symptoms ranging from mild paresthesia to severe pain that interferes with daily activities [20]. CIPN significantly affects mobility, dexterity, and fine motor control, contributing to difficulties in walking, driving, dressing, and performing occupational tasks. These limitations, particularly when accompanied by chronic neuropathic pain, reduce physical independence and elevate the risk of falls, especially in older patients. CIPN has also been associated with greater emotional distress, reduced social engagement, and decreased health-related QoL scores, particularly in domains of physical functioning and role limitations [21,22,23]. Although some patients experience gradual symptom resolution over 6–12 months, CIPN can become irreversible, especially at higher cumulative doses of neurotoxic agents or with repeated cycles [24]. Longitudinal studies reveal that a significant proportion of breast cancer survivors suffer from long-term sensory deficits and pain, impacting work reintegration, sleep, and physical activity levels. The chronic nature of CIPN and the lack of effective neuroprotective strategies highlight a major unmet need in breast cancer survivorship care [24,25].
2.3. Nausea, Vomiting, and Gastrointestinal Distress
Nausea, vomiting, and GI distress remain among the most distressing and functionally disruptive physical side effects of chemotherapy in breast cancer patients. Despite advances in antiemetic therapies, these symptoms continue to impact nutrition, hydration, daily functioning, and overall QoL. CINV are particularly prevalent with highly emetogenic regimens, such as anthracycline–cyclophosphamide combinations. Up to 70% of breast cancer patients report significant nausea, and a substantial subset continues to experience anticipatory or breakthrough vomiting even with guideline-based antiemetic prophylaxis [26]. GI effects also include diarrhea, constipation, mucositis, and bloating, which are often underreported but significantly impair comfort, mobility, and nutrition. These symptoms can persist for days after each chemotherapy cycle, leading to cumulative distress across multiple treatments. CINV and mucosal inflammation contribute to loss of appetite, early satiety, and altered taste (dysgeusia), which reduce oral intake and caloric absorption [27]. Diarrhea or vomiting can lead to dehydration, electrolyte imbalances, and weight loss, exacerbating fatigue and increasing hospitalization risk. Some patients are forced to modify or restrict their diets, avoiding nutrient-dense foods due to GI sensitivity. In severe cases, chemotherapy must be delayed or dose-reduced, potentially compromising treatment efficacy. Malnutrition not only delays physical recovery but also impairs immune function, increases treatment-related toxicities, and contributes to poorer long-term survival outcomes in breast cancer patients [28,29]. The GI burden of chemotherapy also significantly interferes with daily routines, social engagement, and psychological health. Persistent nausea or bowel irregularities limit patients' ability to work, travel, or engage in physical activity. The anticipation of nausea may lead to anxiety, food aversion, and social withdrawal, worsening emotional QoL [28,30]. In some patients, these symptoms become conditioned responses, reinforcing a cycle of anticipatory nausea and avoidance behavior [31].
2.4. Sexual Health and Menopausal Symptoms
Sexual dysfunction and menopausal symptoms are frequently underrecognized but deeply impactful consequences of chemotherapy in breast cancer patients [32]. These effects arise from gonadal toxicity, hormonal disruption, and psychological distress, and manifest as reduced libido, vaginal atrophy, dyspareunia, and infertility—all of which significantly affect QoL, self-esteem, and intimate relationships [33]. Chemotherapy-induced changes in sexual health are multifactorial. The abrupt onset of menopause caused by cytotoxic damage to ovarian follicles leads to a decline in estrogen levels, which reduces sexual desire, impairs vaginal lubrication, and increases discomfort during intercourse. Additionally, body image concerns related to hair loss, mastectomy, or weight changes may lead to decreased sexual confidence and avoidance of intimacy. Many patients also report psychological barriers—such as anxiety, depression, and fear of recurrence—which further diminish libido and sexual satisfaction [34]. Vaginal atrophy—characterized by thinning of the vaginal epithelium, loss of elasticity, and decreased lubrication—is a direct consequence of chemotherapy-induced hypoestrogenism. This condition results in dyspareunia (painful intercourse), vaginal dryness, and irritation, which can persist for months to years post-treatment [35,36]. Women treated with adjuvant endocrine therapy (e.g., tamoxifen or aromatase inhibitors) may experience worsened urogenital symptoms, compounding the effects initiated by chemotherapy. These changes often remain unaddressed in clinical care, despite their significant burden on QoL [37]. For premenopausal women, chemotherapy poses a significant risk of premature ovarian failure (POF) and infertility [38,39]. The incidence of chemotherapy-induced amenorrhea varies with age, drug type, and cumulative dose but can reach 60% or more in women over 40 receiving anthracycline- and taxane-based regimens [7,40,41]. The resulting infertility can have profound emotional consequences, particularly for younger women with unmet reproductive goals. While ovarian suppression with gonadotropin releasing hormone (GnRH) analogs and fertility preservation strategies (e.g., oocyte cryopreservation) are available, they are not universally implemented or accessible. Menopausal symptoms such as hot flashes, mood swings, insomnia, and cognitive disturbances further exacerbate the decline in sexual and physical well-being during and after chemotherapy [42].
3. Psychological and Emotional Effects
3.1. Depression and Anxiety
Depression and anxiety are among the most prevalent psychological comorbidities affecting women undergoing chemotherapy for breast cancer, with notable impact on QoL, treatment adherence, and long-term outcomes. These conditions are not only highly prevalent during chemotherapy but often persist beyond treatment, underscoring the need for vigilant psychological monitoring and intervention. Numerous studies report high rates of depression and anxiety among breast cancer patients during and after chemotherapy. For instance, a large-scale UK cohort found that 35% of patients exhibited clinically significant symptoms of depression or anxiety before starting radiotherapy, with persistent symptoms observed up to five years post-treatment [43]. Similarly, an observational cohort study found that up to 50% of women had depression or anxiety in the first year after diagnosis, with one in six continuing to experience psychological distress at every follow-up over five years [44]. Risk factors for these psychological conditions include younger age at diagnosis, lower educational level, poor social support, prior psychiatric history, financial strain, and advanced disease stage [45,46]. Moreover, treatment side effects like CIPN significantly increase the risk for depression and anxiety. A retrospective study showed that breast cancer patients with CIPN had a 1.5-fold higher risk of developing depression and anxiety within a year post-treatment compared to those without CIPN [47]. Importantly, psychological distress often begins around the time of diagnosis and can peak during intensive treatment periods such as chemotherapy cycles. In a prospective study, depression severity peaked around 12–14 weeks and again at 32 weeks of chemotherapy. Depression was strongly associated with anxiety, physical symptom burden, and specific chemotherapy regimens like Adriamycin-Cytoxan [48]. Social isolation, lack of intimate relationships, and absence of psychosocial support were also major predictors of persistent emotional disorders [44].
3.2. Cognitive Impairment
Cognitive impairment, commonly referred to as "chemo brain" or cancer-related cognitive dysfunction, is a recognized adverse effect of chemotherapy in breast cancer patients, particularly impacting memory, attention, executive function, and processing speed [49]. This constellation of symptoms can significantly hinder QoL and functional independence, often persisting long after treatment completion. Breast cancer patients frequently report impairments in working memory, verbal fluency, multitasking, and executive control following chemotherapy [50,51,52,53]. Objective neuropsychological testing corroborates these complaints, demonstrating mild to moderate deficits, especially in executive functioning and episodic memory. The mechanisms are believed to involve inflammatory cytokines, oxidative stress, mitochondrial dysfunction, and direct neurotoxicity that affect white matter integrity and hippocampal plasticity [54]. Neuroimaging studies have shown gray matter reductions in frontal and temporal regions post-chemotherapy, correlating with cognitive complaints, particularly among patients treated with anthracycline- and taxane-based regimens [55,56]. These structural brain changes may be partially reversible, but longitudinal data indicate that a subset of patients experience long-lasting or even permanent changes in cognitive function. Cognitive symptoms typically emerge during chemotherapy, with peak intensity in the first few weeks to months after treatment initiation. While some patients demonstrate partial cognitive recovery within 6–12 months post-treatment, longitudinal research reveals that 20–30% of survivors report persistent cognitive difficulties even after several years, particularly in those with higher cumulative chemotherapy exposure, older age, or concurrent hormonal therapy [57]. Cognitive recovery is further complicated by comorbid depression, anxiety, and fatigue, all of which are independently associated with perceived and actual cognitive deficits. As a result, “chemo brain” often exists within a broader neuropsychological and emotional symptom cluster, emphasizing the need for holistic survivorship assessment.
3.3. Body Image and Self-Perception
Body image disturbance is one of the most prominent psychological consequences of chemotherapy and breast cancer treatment. Hair loss (alopecia), mastectomy, and changes in body weight disrupt a woman’s perception of femininity and identity, often resulting in lower self-esteem and heightened emotional distress. Chemotherapy-induced alopecia is particularly distressing and frequently reported as one of the most traumatic side effects, not only because of its visual impact but also due to its symbolic association with illness and loss of control [58]. This is especially true for younger women who place greater importance on physical appearance and fertility [59]. Mastectomy, whether with or without reconstructive surgery, has profound and long-lasting effects on body image. The loss of a breast is not only perceived as a physical disfigurement but also as a loss of sexual identity and femininity [60]. Women often describe feelings of shame, unattractiveness, and reduced desirability, which can impair intimacy and partner relationships [61]. One study found that women reported higher satisfaction with their breast image and sexual function after reconstructive procedures, though emotional challenges still persisted [62]. Weight gain, another common chemotherapy side effect, also significantly impacts body satisfaction. It is often poorly anticipated and can create additional emotional burden, especially when compounded by fatigue and reduced physical activity. Weight-related distress is closely linked to feelings of lack of control and disempowerment during treatment [61]. These appearance-related changes contribute to an altered self-image, diminished self-worth, and social withdrawal, creating a cycle that negatively affects overall QoL. Importantly, cultural and racial identity can further compound the distress caused by chemotherapy-induced appearance changes. For example, Black women with breast cancer may experience hair loss as a deeper violation of identity and femininity due to cultural ties to hair aesthetics and historical stigmatization. The inability to find appropriate wigs for their hair texture and color further intensifies psychological distress and reduces coping efficacy [63]. Interventions such as cognitive-behavioral therapy (CBT), exercise programs, peer support groups, and guided psychosocial support have shown promising effects in improving body image and self-esteem among breast cancer survivors [64,65,66]. These strategies aim to support emotional adjustment, foster positive self-image, and reestablish a sense of normalcy in survivors’ lives.
4. Socioeconomical Well-Being
4.1. Social Role and Relationship Changes
Chemotherapy for breast cancer often initiates profound shifts in a patient’s social identity and interpersonal relationships. These transformations may result in changes to partner dynamics, increased social isolation, and experiences of stigmatization, all of which can compromise overall QoL and emotional well-being [67,68,69]. Breast cancer treatment, particularly chemotherapy, affects not only the patient but also their intimate partners. Emotional distress, physical exhaustion, body image concerns, and sexual dysfunction often disrupt marital satisfaction and sexual intimacy [70]. Many partners report feeling helpless or excluded from the care process, which may lead to emotional distance or conflict. On the patient’s side, the impact of alopecia, mastectomy, and treatment-induced menopausal symptoms can result in diminished self-worth and avoidance of intimacy, which further strains relationships [60]. However, some relationships become more cohesive during this experience, with shared adversity strengthening emotional bonds—demonstrating the diversity of psychosocial outcomes in intimate partnerships. Physical fatigue, emotional exhaustion, and altered appearance (e.g., hair loss, surgical scars) can lead many women to withdraw socially during and after chemotherapy. This is often compounded by reduced capacity to work, engage in leisure activities, or fulfill family responsibilities, resulting in a sense of disconnection from prior roles and routines. Some patients avoid public outings or interactions for fear of pity, awkward questions, or unsolicited advice. Over time, this isolation may evolve into chronic loneliness, especially for single women or those with limited support networks [69]. Such social withdrawal has been associated with increased risks of depression, anxiety, and poorer treatment adherence. Social stigma remains a powerful psychosocial burden for many breast cancer patients. Cultural misconceptions about cancer as a “death sentence” or “contagious” illness can lead to marginalization, particularly in societies where physical beauty, fertility, or womanhood are tightly linked to social value. Patients have reported experiences of being treated differently by colleagues, acquaintances, or even healthcare providers after diagnosis and visible treatment changes. Stigmatization often results in reduced help-seeking behavior, internalized shame, and increased psychological distress [71,72,73].
4.2. Return to Work and Productivity
Returning to work (RTW) after chemotherapy is a critical milestone for many breast cancer survivors, symbolizing a return to normalcy, financial stability, and social integration [74]. However, the journey back into the workforce is often delayed, incomplete, or permanently disrupted by the physical, cognitive, and emotional aftereffects of cancer treatment [75]. Employment outcomes are influenced by a range of factors including fatigue, cognitive impairment, workplace accommodations, job type, and psychosocial support. Although many women return to work within the first year following treatment, significant variability exists. Studies have reported that up to 40% of breast cancer survivors fail to resume employment within 12 months, and those who do often return with reduced hours or diminished productivity [76]. The likelihood of RTW is lower among women with physically demanding jobs, lower education levels, or jobs that offer little flexibility. Chemotherapy-related fatigue, pain, and cognitive impairments are the most cited physical barriers to full work reintegration [77]. In particular, survivors report difficulties with concentration, short-term memory, and multitasking, which can undermine workplace performance even after apparent physical recovery [78]. A large prospective cohort study provides critical insight into the complex relationship between breast cancer treatment and RTW outcomes. Among 1,874 working-age women with stage I–III breast cancer in France, 21% had not returned to work two years after diagnosis. The study found that patients receiving systemic therapy regimens involving trastuzumab—especially in combination with chemotherapy and/or hormone therapy—faced significantly higher odds of non-RTW compared to those treated with chemotherapy and hormone therapy alone. Moreover, physical toxicities (CTCAE grade ≥3), arm morbidity, and patient-reported psychological symptoms such as anxiety and depression independently increased the likelihood of non-RTW [79]. The nature of a survivor's occupation also plays a significant role in post-treatment employment outcomes. Women in manual labor or service sector jobs often face greater challenges due to physical demands and limited flexibility. Conversely, those in professional or managerial roles, especially with supportive employers, report better outcomes [80,81]. Workplace accommodations, such as part-time hours, task modifications, or remote work options, are strongly associated with higher rates of successful reintegration and job retention [80]. However, workplace stigma and discrimination also remain barriers. Some survivors report subtle biases, reduced responsibilities, or being overlooked for promotions due to assumptions about their health status or future availability. These experiences can diminish self-efficacy and job satisfaction, potentially prompting voluntary exit from the workforce [82]. Long-term follow-up studies have shown that breast cancer survivors are more likely than the general population to experience underemployment, reduced income, or early retirement. Productivity loss persists even among those who return to work, with many reporting a mismatch between their current performance and pre-diagnosis expectations. Financial toxicity, stemming from medical expenses and loss of income, further compounds stress and may force premature return to work before full recovery—often to the detriment of both health and productivity [83].
4.3. Financial Toxicity
Financial toxicity refers to the objective and subjective burden of cancer-related costs and is increasingly recognized as a major determinant of health-related QoL in breast cancer survivors [84]. Chemotherapy, in particular, contributes significantly to this burden through direct medical expenses, indirect productivity losses, and insurance limitations that persist well into survivorship. The cost of breast cancer chemotherapy can be substantial, encompassing not only drug expenses but also supportive medications (e.g., antiemetics, growth factors), infusion services, imaging, lab tests, and follow-up appointments [84]. Many patients incur high out-of-pocket costs, especially those on high-deductible insurance plans or lacking supplemental coverage. The financial strain is intensified for patients who require extended or combination regimens, or who experience complications requiring hospitalization [85]. The burden is particularly pronounced in low- and middle-income settings, where out-of-pocket expenses often lead to catastrophic health spending and treatment abandonment [86]. Even in countries with widespread health insurance coverage, many patients experience coverage limitations for novel or targeted therapies, reconstructive surgery, fertility preservation, or integrative support services (e.g., mental health, physical therapy). In the United States, underinsurance remains a critical issue: patients may have insurance but still face cost-related nonadherence, such as skipping medications or delaying follow-up care due to financial concerns [87,88]. Furthermore, administrative complexity in claims processing and prior authorization can delay access to necessary treatments and increase psychological distress. Chemotherapy-related side effects such as fatigue, cognitive impairment, and physical debilitation contribute to temporary or permanent work absence, reducing income and employer-provided benefits [89]. Some women are forced to reduce hours or shift to lower-paying jobs to accommodate ongoing health limitations. For self-employed or hourly workers, the absence of paid sick leave or job security can lead to significant economic vulnerability, especially for single mothers or sole-income providers. The financial stress of income loss is compounded by accumulating debt, housing insecurity, and food insecurity, all of which further compromise physical and mental health. Beyond material hardship, financial toxicity is strongly associated with depression, anxiety, and lower treatment satisfaction [90]. Patients experiencing high financial burden are more likely to forego care, reduce adherence to supportive medications, or decline costly but effective therapies, ultimately worsening health outcomes. In addition, the stress associated with managing bills, debt collection, and insurance disputes can erode social relationships and reduce overall QoL.
5. Measuring QoL in Breast Cancer Patients
5.1. QoL Assessment Tools
Accurately measuring QoL in breast cancer patients undergoing chemotherapy is essential for evaluating treatment burden, long-term survivorship, and patient-centered care. Several standardized, validated instruments have been developed for this purpose, each capturing multiple domains of patient well-being (Figure 1), including physical, emotional, cognitive, and social functioning. Among the most widely used tools are the EORTC QLQ-C30, QLQ-BR23, FACT-B, and SF-36 (Table 1) [91,92]. The EORTC QLQ-C30 is a 30-item core questionnaire developed by the European Organisation for Research and Treatment of Cancer (EORTC). It assesses general QoL in cancer patients across five functional domains (physical, emotional, social, role, and cognitive), three symptom domains (fatigue, pain, nausea/vomiting), and overall global health status. This instrument is designed to be complemented by disease-specific modules, the most common for breast cancer being the QLQ-BR23. The QLQ-BR23 adds 23 items specifically related to breast cancer, addressing symptoms such as body image, sexual functioning, breast and arm symptoms, and side effects from systemic therapy [93,94]. Studies confirm that this combination provides comprehensive and sensitive assessment of chemotherapy-related QoL impairments in breast cancer populations, and both tools have been validated across multiple cultures and languages. A study established updated reference values for PROs using EORTC QLQ-C30 and EORTC QLQ-BR23 in breast cancer and other breast conditions using data from over 1,400 patients. Compared to those with benign breast diseases, patients with breast cancer reported worse overall QoL, particularly in emotional and cognitive functioning [94]. Another cross-sectional study assessed the QoL among 284 breast cancer survivors in Saudi Arabia using the EORTC QLQ-C30 and BR23 questionnaires. Overall, patients reported good global health and functioning scores, with insomnia and fatigue being the most prominent symptoms. Younger patients (≤50 years), as well as pre- and perimenopausal women, demonstrated better physical and role functioning compared to older or postmenopausal counterparts. Sexual enjoyment was higher among premenopausal women. Systemic therapy side effects were more noticeable in those who underwent breast-conserving surgery. Menopausal status emerged as a key predictor of physical functioning [95].
The FACT-B is another breast cancer-specific QoL instrument, comprising the 27-item FACT-G (general cancer version) and an additional 10 breast cancer–specific items. The FACT-B measures well-being across physical, social/family, emotional, functional, and additional breast cancer concerns [96]. Its use is widespread in both clinical trials and survivorship studies. Notably, it emphasizes patient-reported treatment burden and emotional adjustment, making it particularly valuable for evaluating chronic toxicities or long-term chemotherapy effects. The FACT-B has demonstrated high internal consistency, construct validity, and responsiveness to clinical change in breast cancer populations undergoing chemotherapy or endocrine therapy. For example, a study investigated the relationship between fatigue, QoL, and functional capacity in post-operative breast cancer patients undergoing adjuvant chemotherapy. Among 30 participants in their third chemotherapy cycle, assessments using the FACIT-Fatigue Scale, FACT-B questionnaire, and 6-minute walk test (6MWT) revealed a strong negative correlation between fatigue and QoL, especially in the total FACT-B, FACT-G, and trial outcome index (TOI) scores. Fatigue also showed a moderate association with reduced functional capacity [97].
The SF-36 is a generic health status instrument with 36 items covering eight health domains, including physical functioning, vitality, social functioning, and general health perceptions [98]. Although not cancer-specific, it is frequently used in comparative health studies and survivorship research. Its utility in breast cancer lies in benchmarking QoL outcomes against the general population or other chronic disease groups. However, it lacks sensitivity to chemotherapy-specific side effects such as alopecia, menopausal symptoms, or breast surgery complications. A study evaluated the impact of lymphedema on health-related QoL (HRQOL) in breast cancer survivors more than one year after surgery using the SF-36. Among 96 patients, HRQOL scores did not differ significantly between those with and without lymphedema on any SF-36 subscale. However, when compared to 104 individuals from the general population, breast cancer survivors scored lower across nearly all SF-36 domains, indicating a persistent reduction in overall QoL. Notably, vitality and mental health components of the SF-36 did not differ significantly from the general population, suggesting some recovery in psychological aspects. These findings emphasize the utility of SF-36 in capturing subtle QoL deficits in long-term breast cancer survivors [99].
5.2. Methodological Considerations
The accurate assessment of QoL in breast cancer patients undergoing chemotherapy depends heavily on timing, assessment modality, and interpretive frameworks [100]. Misalignment between when and how QoL is measured can significantly impact data validity and the clinical relevance of findings. The timing of QoL assessment plays a crucial role in capturing the full spectrum of patient experiences [101]. Assessments during treatment tend to reflect acute toxicities such as nausea, fatigue, and emotional distress, while post-treatment evaluations often capture longer-term impacts like persistent neuropathy, sexual dysfunction, and psychological adjustment. Studies show that QoL tends to worsen during chemotherapy and then partially recover post-treatment, although certain domains like fatigue and cognitive function may remain impaired for months or even years [102]. Importantly, longitudinal assessments—spanning pre-treatment, mid-treatment, and post-treatment phases—are superior to single time-point analyses because they track the trajectory of change, allowing clinicians to differentiate between transient effects and persistent issues. Furthermore, capturing QoL at clinically meaningful intervals, such as immediately after a chemotherapy cycle or 6 months post-completion, improves the sensitivity of these tools to detect patient-relevant outcomes.
PROs are essential for understanding how patients perceive their symptoms and functional status. Tools such as the EORTC QLQ-C30 and FACT-B rely on patients’ direct input, offering high face validity for subjective experiences like pain, emotional distress, and social isolation. PROs have been shown to predict survival outcomes, unplanned hospitalizations, and treatment discontinuation better than clinician-reported metrics in several studies. In contrast, clinician-assessed metrics, such as Common Terminology Criteria for Adverse Events (CTCAE), often underreport subjective symptoms like fatigue and neuropathy, leading to a mismatch between clinical documentation and patient reality [103]. This discrepancy is especially problematic for long-term toxicities, which are harder to observe objectively during brief follow-up visits (Table 2). Integrating PROs into clinical trials and electronic health records is now recommended by most regulatory bodies to enhance patient-centered care and real-world outcome tracking [104].
6. Variability Across Patient Subgroups
6.1. Age and Menopausal Status
Age and menopausal status are critical modifiers of the chemotherapy experience in breast cancer patients, influencing not only treatment tolerance and side effect profiles but also psychosocial adaptation, fertility concerns, and long-term QoL [105,106]. The physiological and psychosocial landscape differs markedly between younger, premenopausal women and older, postmenopausal women, leading to distinct survivorship challenges and varying degrees of resilience. Younger women (<50 years) diagnosed with breast cancer often experience more aggressive tumor biology, leading to the use of more intensive chemotherapy regimens [107]. While they may demonstrate better physical recovery, they face heightened emotional and psychosocial stressors [108]. Chemotherapy-induced amenorrhea and infertility are particularly distressing, as many young patients have not yet completed their reproductive plans. This threat to fertility, combined with abrupt chemically induced menopause, contributes to emotional distress, sexual dysfunction, and identity disruption [109]. Younger survivors are also more likely to report depression, anxiety, and body image dissatisfaction post-chemotherapy, partly due to their life stage, concerns about career disruption, and disrupted family or relationship roles [107]. Despite often being more physically fit, they report lower QoL scores compared to older counterparts, primarily driven by emotional and social domains [110]. In contrast, older patients (≥65 years) may receive less aggressive chemotherapy regimens, often adjusted due to concerns about comorbidities, polypharmacy, and decreased physiological reserves. This group is at higher risk of dose reductions, treatment interruptions, and chemotherapy-related toxicities, such as cardiotoxicity, neuropathy, and functional decline [111,112,113]. Cognitive impairment, especially when combined with baseline deficits, may be more pronounced and longer lasting in older adults [114]. Despite these physical vulnerabilities, some studies report that older patients may demonstrate greater emotional resilience, possibly due to life experience, retirement status, or lower expectations of physical functioning. Older survivors often prioritize treatment goals differently, valuing functional independence and symptom control over aggressive survival extension, and may be less distressed by body image changes or fertility loss [115]. Menopausal status independently affects chemotherapy side effects and long-term symptoms. Premenopausal women undergoing abrupt menopause due to chemotherapy experience hot flashes, insomnia, and vaginal atrophy, which contribute to emotional distress and sexual dysfunction. Postmenopausal women may already be acclimated to such changes but face additive toxicities when chemotherapy is followed by endocrine therapies like aromatase inhibitors, further impairing bone health and QoL [116].
6.2. Socioeconomic and Racial Disparities
Disparities in breast cancer care and outcomes are deeply influenced by socioeconomic status and racial/ethnic background, shaping access to treatment, symptom management, psychosocial coping, and long-term QoL [117]. These disparities are rooted in systemic inequities and are magnified during chemotherapy, when demands on financial, informational, and social resources peak. Patients from lower socioeconomic backgrounds and racial minority groups often face significant barriers to timely and equitable breast cancer care. These include delays in diagnosis, limited access to specialist oncology services, underinsurance or lack of insurance, and geographic inaccessibility of high-quality cancer centers. These structural barriers result in late-stage diagnoses, receipt of non-standard or less intensive chemotherapy regimens, and increased treatment discontinuation [118]. Studies show that Black and Hispanic women are more likely to experience chemotherapy delays, dose reductions, or less frequent use of targeted therapies, which contributes to worse survival and increased recurrence risk [119]. Additionally, these groups are disproportionately affected by financial toxicity, exacerbating stress, reducing treatment adherence, and lowering overall health-related QoL [120,121]. Coping mechanisms also vary by race and socioeconomic status. Racial and ethnic minorities often report greater reliance on spirituality, family support, and faith-based coping, which can be protective but may also mask unmet psychological needs [122]. Limited access to psychosocial services, including mental health counseling, support groups, or sexual health counseling, places these populations at higher risk of untreated emotional distress and depression. Furthermore, cultural stigmas surrounding mental health or cancer itself can hinder open communication with providers and discourage help-seeking behavior. Low socioeconomic status patients also have fewer opportunities for health education, reducing their treatment literacy and capacity for informed decision-making, which can lead to poorer adherence and lower satisfaction with care [123]. Cultural beliefs play a pivotal role in shaping breast cancer experiences. For example, in some communities, cancer is seen as a shameful or taboo diagnosis, contributing to secrecy, isolation, and delayed presentation for care. In Black communities, hair holds deep cultural and historical significance; thus, chemotherapy-induced alopecia can be particularly distressing and symbolic, impacting self-worth and cultural identity [124,125]. Patients often struggle to find wigs or hairpieces that match their hair texture and style, compounding feelings of alienation. Language barriers, health literacy challenges, and culturally discordant care models also reduce patient satisfaction and trust, further entrenching disparities in QoL during and after chemotherapy [126].
6.3. Metastatic vs. Early-Stage Disease
The impact of chemotherapy on QoL in breast cancer patients diverges significantly between those with early-stage (curable) disease and those with metastatic (incurable) disease. These differences stem from treatment goals, disease trajectory, and patient expectations, which in turn shape emotional coping, symptom prioritization, and engagement with supportive care services [127,128]. For patients with early-stage breast cancer, chemotherapy is administered with curative intent—as either neoadjuvant or adjuvant therapy. These patients typically endure intense, time-limited regimens that result in acute declines in physical, emotional, and social QoL. Fatigue, alopecia, nausea, cognitive changes, and sexual dysfunction are common, but are often framed as temporary sacrifices for long-term survival [129]. While distress may be high during treatment, many early-stage patients demonstrate substantial QoL recovery within 6–12 months post-chemotherapy. However, this group is not without psychosocial burden. The “survivor paradox” describes the persistent fear of recurrence, body image concerns, and anxiety about long-term toxicities (e.g., infertility, cardiotoxicity), which may continue long after treatment completion. Expectations of “returning to normal” may be thwarted by lingering symptoms and functional losses, especially in younger women or those without adequate support. In contrast, chemotherapy for metastatic breast cancer is administered with palliative intent, aiming to prolong life, control symptoms, and maintain functional independence. Patients with metastatic breast cancer face a chronic disease trajectory, where QoL preservation often outweighs aggressive disease eradication. Unlike early-stage patients, those with metastatic breast cancer must navigate continuous or cyclical chemotherapy, with cumulative side effects and uncertain endpoints. QoL in metastatic breast cancer is shaped by the constant threat of disease progression, evolving symptom burden, and complex emotional states—including grief, existential distress, and anticipatory loss [130]. Studies show that metastatic breast cancer patients prioritize fatigue reduction, pain control, mental clarity, and family functioning over extended survival, emphasizing the need for patient-centered, symptom-guided treatment plans. Integration of palliative care services, early in the treatment continuum, has been shown to improve both symptom burden and emotional outcomes in this group. Furthermore, metastatic breast cancer patients often feel excluded from survivorship narratives, which predominantly focus on cure and remission. This exclusion can intensify isolation, complicate coping, and reduce access to psychosocial resources tailored for chronic illness management [131].
7. Interventions and Supportive Care to Mitigate QoL Decline
7.1. Physical Rehabilitation and Exercise
Physical rehabilitation and structured exercise programs have emerged as essential components of supportive care for breast cancer patients undergoing chemotherapy (Table 3), as they directly mitigate some of the most debilitating side effects, notably fatigue, impaired mobility, and reduced physical endurance. Chemotherapy often leads to a decline in aerobic capacity, muscle strength, and overall physical functioning, which in turn can limit daily activities and worsen QoL. Integrating aerobic and resistance exercise during and after treatment helps counter these declines, particularly when the program is tailored to the individual’s capabilities and health status [132]. One of the most consistent findings across studies is the positive effect of exercise on CRF, a pervasive and persistent symptom that is often unrelieved by rest. Supervised aerobic and resistance training significantly reduced fatigue levels both during and after chemotherapy in multiple randomized controlled trials. For example, the PACT study demonstrated that an 18-week exercise intervention led to short- and long-term reductions in CRF among breast cancer patients, confirming the sustained benefits of physical activity during adjuvant treatment [133]. Similarly, a four-week multimodal rehabilitation program incorporating aerobic, strength, and flexibility training improved fatigue scores, QoL, and cardiopulmonary function in breast cancer patients who had completed chemotherapy [134]. Exercise interventions also play a vital role in restoring mobility, especially for patients experiencing treatment-induced limitations in joint function. Aerobic training, when combined with resistance and flexibility exercises, has been shown to improve shoulder range of motion, muscular strength, and physical performance, thereby facilitating return to pre-treatment levels of physical function [135]. Real-world implementations of physical therapy-based programs in clinical settings confirm these findings, showing reduced fatigue and improved aerobic capacity among diverse cancer populations, including those with breast cancer [136]. Walking-based interventions, even at low to moderate intensity, are effective for reducing fatigue when practiced consistently during chemotherapy. A nationwide prospective cohort study found that increasing weekly walking by as little as 111–162 minutes (low intensity) or 54–108 minutes (moderate intensity) significantly improved fatigue symptoms during and after chemotherapy [137]. Importantly, home-based or telehealth-guided programs are feasible and accessible options that have demonstrated comparable efficacy, offering flexibility and broader reach, especially in underserved populations [138].
7.2. Psychosocial Interventions
Psychosocial interventions, including counseling, CBT, and peer support programs, play a critical role in mitigating the emotional and mental health impacts of chemotherapy in breast cancer patients. These interventions target the high prevalence of anxiety, depression, fear of recurrence, body image disturbance, and social isolation that often accompany the cancer experience and negatively impact QoL [139,140,141]. Professional psychological counseling provides a structured, empathetic space for patients to process their diagnosis, treatment experiences, and emotional responses. Evidence suggests that both individual and group counseling significantly improve psychological well-being, reduce symptoms of depression and anxiety, and enhance patients’ coping capacities. Counseling is particularly effective when initiated early in the treatment trajectory and maintained through survivorship. Culturally tailored counseling approaches have also been shown to enhance trust and engagement, especially in diverse and underserved populations [142]. CBT is one of the most widely studied psychosocial interventions in oncology and has demonstrated robust efficacy in reducing anxiety, depressive symptoms, insomnia, and cancer-related fatigue in breast cancer patients. CBT targets maladaptive thought patterns and emotional responses, equipping patients with strategies to reframe negative beliefs, develop problem-solving skills, and increase psychological flexibility. Several randomized controlled trials have confirmed that CBT significantly improves emotional regulation, sleep quality, and treatment-related distress, especially when delivered during or shortly after chemotherapy. Internet- and telehealth-based CBT platforms have expanded accessibility, making it a scalable and cost-effective intervention, particularly valuable during periods of medical isolation or rural inaccessibility [143,144]. Peer support programs—where patients connect with others undergoing or recovering from similar treatments—offer a unique form of emotional validation and practical guidance. These interventions foster a sense of community, shared experience, and mutual encouragement, which can be especially powerful in reducing loneliness and existential distress. Studies show that patients participating in peer-led support groups report higher QoL, improved treatment adherence, and enhanced coping skills. Importantly, peer support is not limited to traditional support groups [145,146]. Online communities, social media groups, and structured mentorship programs (e.g., one-on-one matching with survivors) have gained traction and provide flexible, stigma-free platforms for connection. These are especially helpful for younger patients or those in remote locations, and can complement formal therapy with real-time, lived-experience insights [147,148].
7.3. Pharmacological Management
Pharmacological interventions play a critical role in alleviating the adverse effects of chemotherapy on QoL in breast cancer patients. These interventions target a wide array of symptoms, including CIPN, depression, and menopausal disturbances, with varying degrees of efficacy and side effect profiles. CIPN is a frequent and debilitating complication, particularly associated with taxane-based regimens [149]. Pharmacologic treatments for CIPN have had limited success. Duloxetine, a serotonin-norepinephrine reuptake inhibitor (SNRI), was one of the few agents with promising efficacy. However, a systematic review and meta-analysis evaluated the efficacy and safety of duloxetine for the prevention and treatment of CIPN across seven randomized controlled trials involving 645 patients. The findings showed no statistically significant difference between duloxetine and placebo in either treating (RR 0.92) or preventing (RR 1.02) CIPN. Overall, current evidence does not strongly support the use of duloxetine for CIPN, highlighting the need for more rigorous and comprehensive clinical trials [150]. Although other agents like gabapentin and tricyclic antidepressants have been used off-label, their efficacy is inconsistent, and side effects often limit their long-term use [151,152]. Depression in breast cancer patients is common during and after chemotherapy, and its pharmacological treatment must be approached cautiously due to potential interactions with cancer therapies. Selective serotonin reuptake inhibitors (SSRIs) such as sertraline and citalopram are commonly prescribed and have shown benefits in reducing depressive symptoms. However, some SSRIs (e.g., paroxetine, fluoxetine) may inhibit the CYP2D6 enzyme, which is crucial for metabolizing tamoxifen, thereby potentially reducing its effectiveness [153]. Importantly, a large population-based cohort study investigated the association between SSRI use and breast cancer-specific mortality. Among 23,669 breast cancer patients in England, SSRI users showed a 27% higher risk of breast cancer mortality compared to non-users. However, this association weakened when the analysis was limited to patients with a history of depression or compared against users of other antidepressants, suggesting confounding by indication. Notably, long-term SSRI use was still linked to increased mortality, even among those with prior depression [154]. Alternatives like venlafaxine (an SNRI) are preferred when drug interaction is a concern [155]. Pharmacological treatment should be integrated with psychosocial support to maximize effectiveness and adherence. Chemotherapy often induces premature menopause, resulting in vasomotor symptoms (e.g., hot flashes), sexual dysfunction, and osteoporosis. Hormone replacement therapy (HRT) is generally contraindicated in breast cancer survivors, especially those with hormone receptor-positive tumors. Non-hormonal pharmacologic options include venlafaxine, gabapentin, and clonidine, which have shown efficacy in managing vasomotor symptoms [155,156]. For genitourinary symptoms like vaginal atrophy, non-estrogen treatments such as vaginal moisturizers and DHEA suppositories may offer relief. However, in severe cases, low-dose topical estrogens might be used with caution under strict oncologic guidance [157].
7.4. Nutritional and Complementary Therapies
Nutrition plays a critical role in supporting the health and recovery of breast cancer patients undergoing chemotherapy. A plant-based diet rich in vegetables, fruits, and whole grains is broadly recommended for breast cancer survivors due to its potential to reduce recurrence risk and improve overall well-being [158]. Specific nutritional strategies such as carbohydrate restriction may be beneficial for postmenopausal women with estrogen receptor-positive tumors [159]. Additionally, time-restricted feeding, such as a 13-hour overnight fast, has shown promise in reducing treatment-related side effects [160]. Incorporating cruciferous vegetables, flaxseed, soy, green tea, and coffee may offer chemoprotective benefits, while alcohol should be minimized. Omega-3 fatty acids may improve bone health during aromatase inhibitor therapy but carry the risk of chemotherapy resistance, underscoring the need for individualized guidance [161]. Acupuncture has emerged as a supportive intervention for managing a variety of chemotherapy-induced side effects. It has demonstrated efficacy in alleviating hot flushes, CPIN, joint pain associated with aromatase inhibitors, and vulvodynia [162]. Systematic reviews have confirmed the potential of acupuncture to reduce the frequency of hot flashes, though results on pain relief and hot flash severity remain mixed [163]. Yoga, a widely adopted mind–body practice, has shown consistent benefits in improving physical and emotional well-being among breast cancer patients [163]. Meta-analysis and clinical trial report that yoga significantly reduces fatigue, improves sleep quality, alleviates depression and anxiety, and enhances overall QoL in women undergoing chemotherapy [164,165]. This feasibility trial examined the impact of personalized yoga therapy on weight change and QoL in women undergoing treatment for early-stage or locally advanced breast cancer. Among 29 participants receiving chemotherapy, those in the yoga group—who completed an average of 1.7 sessions per week—maintained their weight, while those in the control group gained an average of 2.63% body weight (p=0.024). Yoga participants also experienced stable QoL and fatigue levels, contrasting with declines reported in the control group. Although compliance was lower than expected and no significant changes were observed in inflammatory biomarkers (TNFα, CRP), the findings suggest yoga therapy may help mitigate treatment-related weight gain and preserve QoL during chemotherapy [165]. A study also showed that yoga can reduce chemotherapy-induced nausea and counteract weight gain associated with treatment, which may be clinically significant for prognosis [166]. Furthermore, yoga contributes to psychological resilience by providing structured physical activity, breathwork, and meditative techniques, making it an ideal adjunct in integrative oncology care models [167].
8. Research Gaps and Future Directions
As cancer treatment continues to move toward precision medicine, tailoring QoL interventions based on individual biology, treatment responses, and PROs is an emerging imperative. Integrating genomic data, such as pharmacogenomics and tumor profiling, can not only guide drug selection and dosage but also predict susceptibility to specific side effects—allowing clinicians to proactively manage toxicities that impact QoL [168]. For instance, certain genetic polymorphisms in CYP450 enzymes influence how patients metabolize chemotherapy and antidepressants, which may affect their symptom burden and response to supportive medications. Furthermore, real-time monitoring of PROs via digital platforms—like symptom tracking apps and wearable sensors—can enable adaptive supportive care interventions, delivering timely adjustments based on patient feedback. This dynamic approach not only optimizes symptom management but enhances patient engagement and satisfaction with care [169,170]. Despite these promising developments, more research is needed to validate predictive biomarkers for QoL outcomes and to develop clinical frameworks for implementing personalized QoL interventions in routine oncology practice.
Next, most QoL research in breast cancer focuses on the acute and subacute phases of chemotherapy, often within the first 1–2 years post-treatment. However, many survivors live decades beyond diagnosis, and long-term sequelae—such as cognitive decline, sexual dysfunction, cardiovascular complications, and social reintegration challenges—are often underreported and understudied. Monitoring QoL outcomes beyond 5 years is critical to capturing the full survivorship experience, especially for those on extended endocrine or maintenance therapies. Emerging studies call for prospective, longitudinal research that examines not only clinical and biological factors but also socioeconomic and psychosocial dynamics that evolve over time. Such studies should include diverse populations, including racial minorities, elderly patients, and those with comorbid conditions, to ensure findings are generalizable and equity-oriented.
Despite widespread recognition of QoL as a central component of cancer care, its integration into clinical decision-making remains inconsistent [171]. Tools such as decision aids, value frameworks, and shared decision-making models offer pathways to center patient preferences in treatment planning. Decision aids, when embedded in clinical workflows, can help patients weigh the trade-offs between treatment efficacy and QoL impacts, especially in contexts like dose-intensified chemotherapy, fertility preservation, or mastectomy reconstruction. Shared decision-making also enhances communication and trust between patients and clinicians, improving satisfaction, adherence, and psychological outcomes [172]. For example, when patients are informed about the likelihood of fatigue, neuropathy, or menopausal symptoms, they are more likely to report realistic expectations, adopt coping strategies, and utilize supportive care services. To standardize QoL inclusion in care pathways, future efforts must focus on creating validated, user-friendly tools that integrate QoL data into electronic health records and oncology guidelines.
9. Conclusion
Chemotherapy remains a cornerstone of breast cancer treatment, yet it exerts significant and multifaceted impacts on patients' QoL. These effects span physical, emotional, cognitive, and social domains, often persisting long after treatment ends. By examining chemotherapy’s influence across diverse patient populations and disease stages, this review highlights the urgent need for integrated, personalized, and equitable supportive care strategies. Advances in patient-reported outcomes, survivorship monitoring, and individualized interventions—including exercise, psychosocial support, pharmacologic management, and complementary therapies—can meaningfully mitigate these burdens. Future oncology care must prioritize QoL alongside survival, embedding it as a central outcome in both clinical decision-making and cancer policy.
Funding
This research receives no external funding.
Acknowledgments
None.
Conflicts of Interest
The authors have no conflicts of interest to declare.
References
- Arnold, M; Morgan, E; Rumgay, H; Mafra, A; Singh, D; Laversanne, M; et al. Current and future burden of breast cancer: Global statistics for 2020 and 2040. The Breast 2022, 66, 15–23. [Google Scholar] [CrossRef]
- Qari, AS; Mowais, AH; Alharbi, SM; Almuayrifi, MJ; Al Asiri, AA; Alwatid, SA; et al. Adjuvant and Neoadjuvant Therapy for Breast Cancer: A Systematic Review. Ejbh 2024, 156–66. [Google Scholar] [CrossRef]
- Masood, S. Neoadjuvant chemotherapy in breast cancers. Womens Health (Lond) 2016, 12, 480–91. [Google Scholar] [CrossRef]
- Cook, M; Johnson, N. Pre-surgical chemotherapy for breast cancer may be associated with improved outcomes. The American Journal of Surgery 2018, 215, 931–4. [Google Scholar] [CrossRef]
- Chew, HK. Adjuvant therapy for breast cancer. West J Med 2001, 174, 284–7. [Google Scholar] [CrossRef]
- Buziashvili, JI; Stilidi, IS; Asymbekova, EU; Mackeplishvili, ST; Tugeeva, EF; Ahmedyarova, NK; et al. Comprehensive assessment of quality of life in patients during neoadjuvant chemotherapy. Medicinskij Alfavit 2022, 26–31. [Google Scholar] [CrossRef]
- Langeh, U; Kumar, V; Ahuja, P; Singh, C; Singh, A. An update on breast cancer chemotherapy-associated toxicity and their management approaches. Health Sciences Review 2023, 9, 100119. [Google Scholar] [CrossRef]
- Dent, R; Cortés, J; Pusztai, L; McArthur, H; Kümmel, S; Bergh, J; et al. Neoadjuvant pembrolizumab plus chemotherapy/adjuvant pembrolizumab for early-stage triple-negative breast cancer: quality-of-life results from the randomized KEYNOTE-522 study. JNCI: Journal of the National Cancer Institute 2024, 116, 1654–63. [Google Scholar] [CrossRef]
- Al Maqbali, M; Al Sinani, M; Al Naamani, Z; Al Badi, K; Tanash, MI. Prevalence of Fatigue in Patients With Cancer: A Systematic Review and Meta-Analysis. Journal of Pain and Symptom Management 2021, 61, 167–189.e14. [Google Scholar] [CrossRef] [PubMed]
- Hajj, A; Chamoun, R; Salameh, P; Khoury, R; Hachem, R; Sacre, H; et al. Fatigue in breast cancer patients on chemotherapy: a cross-sectional study exploring clinical, biological, and genetic factors. BMC Cancer 2022, 22, 16. [Google Scholar] [CrossRef] [PubMed]
- Muthanna, FMS; Iqbal, MS; Karuppannan, M; Abdulrahman, E; Adulyarat, N; Al-Ghorafi, MAA; et al. Prevalence and associated factors of fatigue among breast cancer patients in Malaysia—A prospective study. J App Pharm Sci 2022, 12, 131–9. [Google Scholar] [CrossRef]
- Álvarez-Bustos, A; de Pedro, CG; Romero-Elías, M; Ramos, J; Osorio, P; Cantos, B; et al. Prevalence and correlates of cancer-related fatigue in breast cancer survivors. Support Care Cancer 2021, 29, 6523–34. [Google Scholar] [CrossRef]
- Thong, MSY; van Noorden, CJF; Steindorf, K; Arndt, V. Cancer-Related Fatigue: Causes and Current Treatment Options. Curr Treat Options Oncol 2020, 21, 17. [Google Scholar] [CrossRef]
- Muthanna, FMS; Karuppannan, M; Hassan, BAR; Mohammed, AH. Impact of fatigue on quality of life among breast cancer patients receiving chemotherapy. PHRP 2021, 12, 115–25. [Google Scholar] [CrossRef]
- Gilliam, LAA; St. Clair, DK. Chemotherapy-Induced Weakness and Fatigue in Skeletal Muscle: The Role of Oxidative Stress. Antioxid Redox Signal 2011, 15, 2543–63. [Google Scholar] [CrossRef] [PubMed]
- Schneider, CM; Hsieh, CC; Sprod, LK; Carter, SD; Hayward, R. Cancer treatment-induced alterations in muscular fitness and quality of life: the role of exercise training. Annals of Oncology 2007, 18, 1957–62. [Google Scholar] [CrossRef]
- Uslu, A; Canbolat, O. Relationship Between Frailty and Fatigue in Older Cancer Patients. Seminars in Oncology Nursing 2021, 37, 151179. [Google Scholar] [CrossRef] [PubMed]
- Wu, S; Xiong, T; Guo, S; Zhu, C; He, J; Wang, S. An up-to-date view of paclitaxel-induced peripheral neuropathy. Journal of Cancer Research and Therapeutics 2023, 19, 1501. [Google Scholar] [CrossRef]
- Rahman, N; Sukumar, J; Lustberg, MB. Chronic chemotherapy-induced peripheral neuropathy: living with neuropathy during and after cancer treatments. Annals of Palliative Medicine 2025, 14, 19616–19216. [Google Scholar] [CrossRef]
- Maihöfner, C; Diel, I; Tesch, H; Quandel, T; Baron, R. Chemotherapy-induced peripheral neuropathy (CIPN): current therapies and topical treatment option with high-concentration capsaicin. Support Care Cancer 2021, 29, 4223–38. [Google Scholar] [CrossRef]
- Jheng, Y-W; Chan, Y-N; Wu, C-J; Lin, M-W; Tseng, L-M; Wang, Y-J. Neuropathic Pain Affects Quality of Life in Breast Cancer Survivors with Chemotherapy-Induced Peripheral Neuropathy. Pain Management Nursing 2024, 25, 308–15. [Google Scholar] [CrossRef]
- Schwab, L; Visovsky, C. Psychological distress and quality of life in breast cancer survivors with taxane-induced peripheral neuropathy: A scoping review. Front Oncol 2023, 12, 1005083. [Google Scholar] [CrossRef]
- Gordon, BS; Gbadamosi, B; Jaiyesimi, IA. The relationship between chemotherapy-induced neuropathy and quality of life in breast cancer survivors. JCO 2018, 36, e22111–e22111. [Google Scholar] [CrossRef]
- Zhang, S. Chemotherapy-induced peripheral neuropathy and rehabilitation: A review. Seminars in Oncology 2021, 48, 193–207. [Google Scholar] [CrossRef] [PubMed]
- Mahfouz, FM; Li, T; Joda, M; Harrison, M; Horvath, LG; Grimison, P; et al. Sleep dysfunction associated with worse chemotherapy-induced peripheral neurotoxicity functional outcomes. Support Care Cancer 2024, 32, 46. [Google Scholar] [CrossRef]
- Gozzo, T de O; de Souza, SG; Moysés, AMB; Panobianco, MS; de Almeida, AM. Incidence and management of chemotherapy-induced nausea and vomiting in women with breast cancer. Rev Gaúcha Enferm 2014, 35, 117–23. [Google Scholar] [CrossRef]
- Singh, KP; Kober, KM; Ernst, B; Sachdev, J; Brewer, M; Zhu, Q; et al. Multiple Gastrointestinal Symptoms Are Associated With Chemotherapy-Induced Nausea In Patients With Breast Cancer. Cancer Nurs 2022, 45, 181–9. [Google Scholar] [CrossRef] [PubMed]
- Adam, R; Haileselassie, W; Solomon, N; Desalegn, Y; Tigeneh, W; Suga, Y; et al. Nutritional status and quality of life among breast Cancer patients undergoing treatment in Addis Ababa, Ethiopia. BMC Womens Health 2023, 23, 428. [Google Scholar] [CrossRef]
- Camilleri, GM; Delrieu, L; Bouleuc, C; Pierga, J-Y; Cottu, P; Berger, F; et al. Prevalence and survival implications of malnutrition and sarcopenia in metastatic breast cancer: A longitudinal analysis. Clinical Nutrition 2024, 43, 1710–8. [Google Scholar] [CrossRef]
- Stewart, DJ. Nausea and Vomiting in Cancer Patients. In Nausea and Vomiting; CRC Press, 1991. [Google Scholar]
- Rodríguez, M. Individual differences in chemotherapy-induced anticipatory nausea. Front Psychol 2013, 4. [Google Scholar] [CrossRef]
- Haris, I; Hutajulu, SH; Astari, YK; Wiranata, JA; Widodo, I; Kurnianda, J; et al. Sexual Dysfunction Following Breast Cancer Chemotherapy: A Cross-Sectional Study in Yogyakarta, Indonesia. Cureus n.d., 15, e41744. [Google Scholar] [CrossRef] [PubMed]
- Park, H; Yoon, HG. Menopausal symptoms, sexual function, depression, and quality of life in Korean patients with breast cancer receiving chemotherapy. Support Care Cancer 2013, 21, 2499–507. [Google Scholar] [CrossRef] [PubMed]
- Fallbjörk, U; Rasmussen, BH; Karlsson, S; Salander, P. Aspects of body image after mastectomy due to breast cancer – A two-year follow-up study. European Journal of Oncology Nursing 2013, 17, 340–5. [Google Scholar] [CrossRef]
- Lester, J; Pahouja, G; Andersen, B; Lustberg, M. Atrophic Vaginitis in Breast Cancer Survivors: A Difficult Survivorship Issue. J Pers Med 2015, 5, 50–66. [Google Scholar] [CrossRef]
- Biglia, N; Bounous, VE; D’Alonzo, M; Ottino, L; Tuninetti, V; Robba, E; et al. Vaginal Atrophy in Breast Cancer Survivors: Attitude and Approaches Among Oncologists. Clinical Breast Cancer 2017, 17, 611–7. [Google Scholar] [CrossRef]
- Sousa, MS; Peate, M; Jarvis, S; Hickey, M; Friedlander, M. A clinical guide to the management of genitourinary symptoms in breast cancer survivors on endocrine therapy. Ther Adv Med Oncol 2017, 9, 269–85. [Google Scholar] [CrossRef]
- Hulvat, MC; Jeruss, JS. Maintaining Fertility in Young Women with Breast Cancer. Curr Treat Options Oncol 2009, 10, 308–17. [Google Scholar] [CrossRef] [PubMed]
- Mathelin, C; Brettes, J-P; Diemunsch, P. Premature ovarian failure after chemotherapy for breast cancer. Bull Cancer 2008, 95, 403–12. [Google Scholar]
- Pourali, L; Taghizadeh Kermani, A; Ghavamnasiri, MR; Khoshroo, F; Hosseini, S; Asadi, M; et al. Incidence of Chemotherapy-Induced Amenorrhea After Adjuvant Chemotherapy With Taxane and Anthracyclines in Young Patients With Breast Cancer. Iran J Cancer Prev 2013, 6, 147–50. [Google Scholar]
- Cosimo, SD; Alimonti, A; Ferretti, G; Sperduti, I; Carlini, P; Papaldo, P; et al. Incidence of chemotherapy-induced amenorrhea depending on the timing of treatment by menstrual cycle phase in women with early breast cancer. Annals of Oncology 2004, 15, 1065–71. [Google Scholar] [CrossRef]
- So, WKW; Law, BMH; Ng, MSN; He, X; Chan, DNS; Chan, CWH; et al. Symptom clusters experienced by breast cancer patients at various treatment stages: A systematic review. Cancer Medicine 2021, 10, 2531–65. [Google Scholar] [CrossRef] [PubMed]
- Hopwood, P; Sumo, G; Mills, J; Haviland, J; Bliss, JM. The course of anxiety and depression over 5 years of follow-up and risk factors in women with early breast cancer: Results from the UK Standardisation of Radiotherapy Trials (START). The Breast 2010, 19, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Burgess, C; Cornelius, V; Love, S; Graham, J; Richards, M; Ramirez, A. Depression and anxiety in women with early breast cancer: five year observational cohort study. BMJ 2005, 330, 702. [Google Scholar] [CrossRef]
- Dadheech, A; Kumawat, S; Sharma, D; Gothwal, RS; Dana, R; Meena, C; et al. The Prevalence of Anxiety and Depression in Breast Cancer Patients and their Correlation with Socio-Demographic Factors. Asian Pac J Cancer Care 2023, 8, 675–9. [Google Scholar] [CrossRef]
- Tsaras, K; Papathanasiou, IV; Mitsi, D; Veneti, A; Kelesi, M; Zyga, S; et al. Assessment of Depression and Anxiety in Breast Cancer Patients: Prevalence and Associated Factors. Asian Pac J Cancer Prev 2018, 19. [Google Scholar] [CrossRef]
- McNeish, BL; Richardson, JK; Whitney, DG. Chemotherapy-induced peripheral neuropathy onset is associated with early risk of depression and anxiety in breast cancer survivors. European J Cancer Care 2022, 31. [Google Scholar] [CrossRef]
- Reece, JC; Chan, Y-F; Herbert, J; Gralow, J; Fann, JR. Course of depression, mental health service utilization and treatment preferences in women receiving chemotherapy for breast cancer. General Hospital Psychiatry 2013, 35, 376–81. [Google Scholar] [CrossRef]
- REN, X; BORIERO, D; CHAISWING, L; BONDADA, S; CLAIR DKST; BUTTERFIELD, DA. Plausible Biochemical Mechanisms of Chemotherapy-induced Cognitive Impairment (“Chemobrain”), a Condition That Significantly Impairs the Quality of Life of Many Cancer Survivors. Biochim Biophys Acta Mol Basis Dis 2019, 1865, 1088–97. [Google Scholar] [CrossRef]
- Oliva, G; Giustiniani, A; Danesin, L; Burgio, F; Arcara, G; Conte, P. Cognitive impairment following breast cancer treatments: an umbrella review. The Oncologist 2024, 29, e848–63. [Google Scholar] [CrossRef]
- Andryszak, P; Wiłkość, M; Żurawski, B; Izdebski, P. Verbal fluency in breast cancer patients treated with chemotherapy. Breast Cancer 2017, 24, 376–83. [Google Scholar] [CrossRef] [PubMed]
- Amani, O; Mazaheri, MA; Moghani, MM; Zarani, F; Choolabi, RH. Chemotherapy-induced cognitive impairment in breast cancer survivors: A systematic review of studies from 2000 to 2021. Cancer Reports 2024, 7, e1989. [Google Scholar] [CrossRef]
- Yang, Y; Hendrix, CC. Cancer-Related Cognitive Impairment in Breast Cancer Patients: Influences of Psychological Variables. Asia-Pacific Journal of Oncology Nursing 2018, 5, 296–306. [Google Scholar] [CrossRef]
- Nordhjem, BJT; Hjalgrim, LL. Cancer-related cognitive impairment and hippocampal functioning: The role of dynamin-1. Neurotherapeutics 2024, 22, e00508. [Google Scholar] [CrossRef] [PubMed]
- Li, X; Chen, H; Lv, Y; Chao, HH; Gong, L; Li, C-SR; et al. Diminished gray matter density mediates chemotherapy dosage-related cognitive impairment in breast cancer patients. Sci Rep 2018, 8, 13801. [Google Scholar] [CrossRef]
- Silverman, DHS; Sleurs, C; Gavrila Laic, RA; Amidi, A; Chen, BT; Deprez, S; et al. Neuroimaging studies of cognitive dysfunction following cancer and treatment. Journal of Clinical and Experimental Neuropsychology n.d., 0, 1–27. [Google Scholar] [CrossRef]
- Das, A; Ranadive, N; Kinra, M; Nampoothiri, M; Arora, D; Mudgal, J. An Overview on Chemotherapy-induced Cognitive Impairment and Potential Role of Antidepressants. Curr Neuropharmacol 2020, 18, 838–51. [Google Scholar] [CrossRef]
- Watanabe, T; Yagata, H; Saito, M; Okada, H; Takayama, T; Imai, H; et al. Abstract P5-15-09: National survey of chemotherapy-induced appearance issues in breast cancer patients. Cancer Research 2015, 75, P5-15-09-P5-15–09. [Google Scholar] [CrossRef]
- Fonseca, EEC; Pereira, SCDC; Pereira, EDAT; Constante, ES; Bindi, MCV. Body image perceptions of women with breast cancer undergoing antineoplastic chemotherapy. JHS 2022, 2, 2–12. [Google Scholar] [CrossRef]
- Katz, A. My body my self: Body image and sexuality in women with cancer. CONJ 2009, 19, E1–4. [Google Scholar] [CrossRef]
- Partridge, A. Abstract SP114: Body Image and Sexual Health. Cancer Research 2021, 81. [Google Scholar] [CrossRef]
- Sghaier, A; Kaabia, O; Bouchahda, R. (265) Self-Image after Breast Cancer. The Journal of Sexual Medicine 2024, 21, qdae002.228. [Google Scholar] [CrossRef]
- Pleasant, VA; Purkiss, AS; Merjaver, SD. Redefining the “crown”: Approaching chemotherapy-induced alopecia among Black patients with breast cancer. Cancer 2023, 129, 1629–33. [Google Scholar] [CrossRef]
- Fadaei, S; Janighorban, M; Mehrabi, T. P656 Study of the effect of cognitive behavioral counseling on body image alterations in women who have undergone mastectomy. International Journal of Gynecology & Obstetrics 2009, 107, S601–S601. [Google Scholar] [CrossRef]
- Zhao, W; Chong, YY; Chien, WT. Effectiveness of cognitive-based interventions for improving body image of patients having breast cancer: A systematic review and meta-analysis. Asia Pac J Oncol Nurs 2023, 10, 100213. [Google Scholar] [CrossRef] [PubMed]
- Lin, T; Ping, Y; Jing, CM; Xu, ZX; Ping, Z. The efficacy of internet-based cognitive behavior therapy for psychological health and quality of life among breast cancer patients: a systematic review and meta-analysis. Front Psychol 2025, 15. [Google Scholar] [CrossRef]
- Wang, Y; Feng, W. Cancer-related psychosocial challenges. Gen Psychiatr 2022, 35, e100871. [Google Scholar] [CrossRef]
- Charalambous, A; Kaite, CP; Charalambous, M; Tistsi, T; Kouta, C. The effects on anxiety and quality of life of breast cancer patients following completion of the first cycle of chemotherapy. SAGE Open Med 2017, 5, 2050312117717507. [Google Scholar] [CrossRef]
- R. K, L. S, P. B, S. G, R. L-P. Psychosocial experiences of breast cancer survivors: a meta-review. J Cancer Surviv 2024, 18, 84–123. [CrossRef]
- Rodrigues-Machado, N; Bonfill-Cosp, X; Quintana, MJ; Santero, M; Bártolo, A; Olid, AS. Sexual dysfunction in women with breast cancer: a systematic review. Support Care Cancer 2025, 33, 332. [Google Scholar] [CrossRef] [PubMed]
- Wang, C; Qiu, X; Yang, X; Mao, J; Li, Q. Factors Influencing Social Isolation among Cancer Patients: A Systematic Review. Healthcare (Basel) 2024, 12, 1042. [Google Scholar] [CrossRef]
- Ding, Y; Huang, Q; Wu, F; Yang, Y; Wang, L; Zong, X; et al. Impact of social support on cognitive function in patients with breast cancer undergoing chemotherapy: The chain-mediating role of fatigue and depression. Asia-Pacific Journal of Oncology Nursing 2025, 12, 100743. [Google Scholar] [CrossRef]
- Jin, R; Xie, T; Zhang, L; Gong, N; Zhang, J. Stigma and its influencing factors among breast cancer survivors in China: A cross-sectional study. European Journal of Oncology Nursing 2021, 52, 101972. [Google Scholar] [CrossRef]
- Park, J; Shubair, M. Returning to Work After Breast Cancer: A Critical Review. International Journal of Disability Management 2013, 8, e1. [Google Scholar] [CrossRef]
- Merdawati, L; Lin, H-C; Pan, C-H; Huang, H-C. Factors Associated With Not Returning to Work Among Breast Cancer Survivors. Workplace Health Saf 2025, 73, 216–26. [Google Scholar] [CrossRef]
- Tan, CJ; Yip, SYC; Chan, RJ; Chew, L; Chan, A. Investigating how cancer-related symptoms influence work outcomes among cancer survivors: a systematic review. J Cancer Surviv 2022, 16, 1065–78. [Google Scholar] [CrossRef]
- Joly, F; Lange, M; Dos Santos, M; Vaz-Luis, I; Di Meglio, A. Long-Term Fatigue and Cognitive Disorders in Breast Cancer Survivors. Cancers (Basel) 2019, 11, 1896. [Google Scholar] [CrossRef]
- Peipins, LA; Dasari, S; Rodriguez, JL; White, MC; Hodgson, ME; Sandler, DP. Employment After Breast Cancer Diagnosis and Treatment Among Women in the Sister and the Two Sister Studies. J Occup Rehabil 2021, 31, 543–51. [Google Scholar] [CrossRef]
- Dumas, A; Vaz Luis, I; Bovagnet, T; El Mouhebb, M; Di Meglio, A; Pinto, S; et al. Impact of Breast Cancer Treatment on Employment: Results of a Multicenter Prospective Cohort Study (CANTO). JCO 2020, 38, 734–43. [Google Scholar] [CrossRef] [PubMed]
- Blinder, V; Eberle, C; Patil, S; Gany, FM; Bradley, CJ. Women With Breast Cancer Who Work For Accommodating Employers More Likely To Retain Jobs After Treatment. Health Affairs 2017, 36, 274–81. [Google Scholar] [CrossRef]
- Tracy, JK; Adetunji, F; Kibria, GMA; Swanberg, JE. Cancer-work management: Hourly and salaried wage women’s experiences managing the cancer-work interface following new breast cancer diagnosis. PLOS ONE 2020, 15, e0241795. [Google Scholar] [CrossRef] [PubMed]
- Stergiou-Kita, M; Qie, X; Yau, HK; Lindsay, S. Stigma and work discrimination among cancer survivors: A scoping review and recommendations: Stigmatisation et discrimination au travail des survivants du cancer : Examen de la portée et recommandations. Can J Occup Ther 2017, 84, 178–88. [Google Scholar] [CrossRef]
- van Muijen, P; Weevers, N l. e. c.; Snels, I a. k.; Duijts, S f. a.; Bruinvels, D j.; Schellart, A j. m.; et al. Predictors of return to work and employment in cancer survivors: a systematic review. European Journal of Cancer Care 2013, 22, 144–60. [Google Scholar] [CrossRef]
- Ehsan, AN; Wu, CA; Minasian, A; Singh, T; Bass, M; Pace, L; et al. Financial Toxicity Among Patients With Breast Cancer Worldwide. JAMA Netw Open 2023, 6, e2255388. [Google Scholar] [CrossRef]
- Lee, KL; Eniu, A; Booth, CM; MacDonald, M; Chino, F. Financial Toxicity and Breast Cancer: Why Does It Matter, Who Is at Risk, and How Do We Intervene? Am Soc Clin Oncol Educ Book 2025, 45, e473450. [Google Scholar] [CrossRef]
- Ngan, TT; Van Minh, H; Donnelly, M; O’Neill, C. Financial toxicity due to breast cancer treatment in low- and middle-income countries: evidence from Vietnam. Support Care Cancer 2021, 29, 6325–33. [Google Scholar] [CrossRef]
- Yabroff, KR; Gansler, T; Wender, RC; Cullen, KJ; Brawley, OW. Minimizing the burden of cancer in the United States: Goals for a high-performing health care system. CA: A Cancer Journal for Clinicians 2019, 69, 166–83. [Google Scholar] [CrossRef]
- Zhao, J; Zheng, Z; Han, X; Davidoff, AJ; Banegas, MP; Rai, A; et al. Cancer History, Health Insurance Coverage, and Cost-Related Medication Nonadherence and Medication Cost-Coping Strategies in the United States. Value in Health 2019, 22, 762–7. [Google Scholar] [CrossRef]
- Yang, Y; Ah, DV. Cancer-related cognitive impairment: updates to treatment, the need for more evidence, and impact on quality of life—a narrative review. Annals of Palliative Medicine 2024, 13, 1265280–1261280. [Google Scholar] [CrossRef] [PubMed]
- Perry, LM; Hoerger, M; Seibert, K; Gerhart, JI; O’Mahony, S; Duberstein, PR. Financial Strain and Physical and Emotional Quality of Life in Breast Cancer. J Pain Symptom Manage 2019, 58, 454–9. [Google Scholar] [CrossRef] [PubMed]
- Hasanah, U; Ahmad, M; Prihantono, P; Usman, AN; Arsyad, A; Agustin, DI. The quality of life assessment of breast cancer patients. Breast Dis n.d., 43, 173–85. [Google Scholar] [CrossRef] [PubMed]
- Montazeri, A. Health-related quality of life in breast cancer patients: A bibliographic review of the literature from 1974 to 2007. J Exp Clin Cancer Res 2008, 27, 32. [Google Scholar] [CrossRef] [PubMed]
- Tan, ML; Idris, DB; Teo, LW; Loh, SY; Seow, GC; Chia, YY; et al. Validation of EORTC QLQ-C30 and QLQ-BR23 questionnaires in the measurement of quality of life of breast cancer patients in Singapore. Asia Pac J Oncol Nurs 2014, 1, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Karsten, MM; Roehle, R; Albers, S; Pross, T; Hage, AM; Weiler, K; et al. Real-world reference scores for EORTC QLQ-C30 and EORTC QLQ-BR23 in early breast cancer patients. European Journal of Cancer 2022, 163, 128–39. [Google Scholar] [CrossRef]
- Imran, M; Al-Wassia, R; Alkhayyat, SS; Baig, M; Al-Saati, BA. Assessment of quality of life (QoL) in breast cancer patients by using EORTC QLQ-C30 and BR-23 questionnaires: A tertiary care center survey in the western region of Saudi Arabia. PLOS ONE 2019, 14, e0219093. [Google Scholar] [CrossRef]
- Brady, MJ; Cella, DF; Mo, F; Bonomi, AE; Tulsky, DS; Lloyd, SR; et al. Reliability and validity of the Functional Assessment of Cancer Therapy-Breast quality-of-life instrument. J Clin Oncol 1997, 15, 974–86. [Google Scholar] [CrossRef]
- Amarsheda, SB; Bhise, AR. Association of Fatigue, Quality of Life and Functional Capacity in Breast Cancer Patients Receiving Adjuvant Chemotherapy. Asian Pacific Journal of Cancer Care 2021, 6, 59–64. [Google Scholar] [CrossRef]
- Ware, JE; Sherbourne, CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 1992, 30, 473–83. [Google Scholar] [CrossRef] [PubMed]
- Lee, SH; Min, Y-S; Park, HY; Jung, T-D. Health-Related Quality of Life in Breast Cancer Patients with Lymphedema Who Survived More than One Year after Surgery. J Breast Cancer 2012, 15, 449–53. [Google Scholar] [CrossRef]
- Janabi, S; Gharaibeh, L; Aldeeb, I; Abuhaliema, A. Quality of Life Assessment of Breast Cancer Patients Undergoing Chemotherapy in Jordan: A Cross-Sectional Study. Int J Breast Cancer 2025, 2025, 9936131. [Google Scholar] [CrossRef]
- Sanghera, S; Coast, J; Walther, A; Peters, TJ. The Influence of Recall and Timing of Assessment on the Estimation of Quality-Adjusted Life-Years When Health Fluctuates Recurrently. Value in Health 2025, 28, 275–84. [Google Scholar] [CrossRef]
- Byar, KL; Berger, AM; Bakken, SL; Cetak, MA. Impact of adjuvant breast cancer chemotherapy on fatigue, other symptoms, and quality of life. Oncol Nurs Forum 2006, 33, E18-26. [Google Scholar] [CrossRef]
- Minasian, LM; O’Mara, A; Mitchell, SA. Clinician and Patient Reporting of Symptomatic Adverse Events in Cancer Clinical Trials: Using CTCAE and PRO-CTCAE® to Provide Two Distinct and Complementary Perspectives. Patient Relat Outcome Meas 2022, 13, 249–58. [Google Scholar] [CrossRef]
- Huynh-Dagher, S; Duong, T-A; Tournigand, C; Kempf, E; Lamé, G. Concordance between patient-reported outcomes and CTCAE clinician-reported toxicities during outpatient chemotherapy courses: a retrospective cohort study in routine care. ESMO Real World Data and Digital Oncology 2025, 8. [Google Scholar] [CrossRef]
- Partridge, AH. Chemotherapy in Premenopausal Breast Cancer Patients. Breast Care (Basel) 2015, 10, 307–10. [Google Scholar] [CrossRef] [PubMed]
- Yeo, W; Pang, E; Liem, GS; Suen, JJS; Ng, RYW; Yip, CCH; et al. Menopausal symptoms in relationship to breast cancer-specific quality of life after adjuvant cytotoxic treatment in young breast cancer survivors. Health Qual Life Outcomes 2020, 18, 24. [Google Scholar] [CrossRef] [PubMed]
- Anders, CK; Johnson, R; Litton, J; Phillips, M; Bleyer, A. Breast Cancer Before Age 40 Years. Semin Oncol 2009, 36, 237–49. [Google Scholar] [CrossRef] [PubMed]
- Pancakarsa, EP; Soemitro, MP; Budianto, A; Abdurahman, M; Rizki, KA; Azhar, Y; et al. Analysis of Risk Factors for Psychological Stress in Breast Cancer Patients: Observational Study in West Java, Indonesia. 2024, 8, 4648–56. [Google Scholar] [CrossRef]
- Gorman, JR; Usita, P; Madlensky, L; Pierce, JP. Young Breast Cancer Survivors: Their Perspectives on Treatment Decisions and Fertility Concerns. Cancer Nurs 2011, 34, 32–40. [Google Scholar] [CrossRef]
- Howard-Anderson, J; Ganz, PA; Bower, JE; Stanton, AL. Quality of Life, Fertility Concerns, and Behavioral Health Outcomes in Younger Breast Cancer Survivors: A Systematic Review; Journal of the National Cancer Institute: JNCI, 2012; Volume 104, pp. 386–405. [Google Scholar] [CrossRef]
- Oliveira, RF; Oliveira, AI; Cruz, AS; Ribeiro, O; Afreixo, V; Pimentel, F. Polypharmacy and drug interactions in older patients with cancer receiving chemotherapy: associated factors. BMC Geriatr 2024, 24, 557. [Google Scholar] [CrossRef]
- Sutanto, H. Tackling polypharmacy in geriatric patients: Is increasing physicians’ awareness adequate? Archives of Gerontology and Geriatrics Plus 2025, 2, 100185. [Google Scholar] [CrossRef]
- Maggiore, RJ; Feng, T; Dale, W; Gross, CP; Tew, WP; Mohile, SG; et al. Measures of polypharmacy and chemotherapy toxicity in older adults with cancer. JCO 2013, 31, 9545–9545. [Google Scholar] [CrossRef]
- Vega, JN; Dumas, J; Newhouse, P. Cognitive Effects of Chemotherapy and Cancer-Related Treatments in Older Adults. Am J Geriatr Psychiatry 2017, 25, 1415–26. [Google Scholar] [CrossRef]
- Springer, F; Matsuoka, A; Obama, K; Mehnert-Theuerkauf, A; Uchitomi, Y; Fujimori, M. Quality of life in older patients with cancer and related unmet needs: a scoping review. AO 2025, 64, 516–26. [Google Scholar] [CrossRef]
- Rosenberg, SM; Partridge, AH. Premature menopause in young breast cancer: effects on quality of life and treatment interventions. J Thorac Dis 2013, 5, S55–61. [Google Scholar] [CrossRef] [PubMed]
- Le, NK; Gabrick, KS; Chouairi, F; Mets, EJ; Avraham, T; Alperovich, M. Impact of socioeconomic status on psychological functioning in survivorship following breast cancer and reconstruction. The Breast Journal 2020, 26, 1695–701. [Google Scholar] [CrossRef] [PubMed]
- Scott, ECS; Hoskin, PJ. Health inequalities in cancer care: a literature review of pathways to diagnosis in the United Kingdom. eClinicalMedicine 2024, 76, 102864. [Google Scholar] [CrossRef] [PubMed]
- Puckett, Y; Sule, AA. Disparity in Early Detection of Breast Cancer. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2025. [Google Scholar]
- Ping, C; Andrade, DC; Housten, A; Doering, M; Goldstein, E; Politi, MC. A Scoping Review of Interventions to Address Financial Toxicity in Pediatric and Adult Patients and Survivors of Cancer. Cancer Med 2025, 14, e70879. [Google Scholar] [CrossRef]
- Ragavan, MV; Mora, RV; Winder, K; Incudine, A; Cunningham, R; Stivers, T; et al. Impact of a Comprehensive Financial Resource on Financial Toxicity in a National, Multiethnic Sample of Adult, Adolescent/Young Adult, and Pediatric Patients With Cancer. JCO Oncology Practice 2023, 19, e286–97. [Google Scholar] [CrossRef]
- Nguyen, AW. Religion and Mental Health in Racial and Ethnic Minority Populations: A Review of the Literature. Innovation in Aging 2020, 4, igaa035. [Google Scholar] [CrossRef]
- Coughlin, SS; Vernon, M; Hatzigeorgiou, C; George, V. Health Literacy, Social Determinants of Health, and Disease Prevention and Control. J Environ Health Sci 2020, 6, 3061. [Google Scholar]
- Clarke-Jeffers, P; Keyte, R; Connabeer, K. “Hair is your crown and glory” – Black women’s experiences of living with alopecia and the role of social support. Health Psychol Rep 2024, 12, 154–65. [Google Scholar] [CrossRef]
- Pleasant, VA; Purkiss, AS; Merjaver, SD. Redefining the “crown”: Approaching chemotherapy-induced alopecia among Black patients with breast cancer. Cancer 2023, 129, 1629–33. [Google Scholar] [CrossRef]
- Karliner, LS; Hwang, ES; Nickleach, D; Kaplan, CP. Language barriers and patient-centered breast cancer care. Patient Educ Couns 2011, 84, 223–8. [Google Scholar] [CrossRef]
- Heidary, Z; Ghaemi, M; Hossein Rashidi, B; Kohandel Gargari, O; Montazeri, A. Quality of Life in Breast Cancer Patients: A Systematic Review of the Qualitative Studies. Cancer Control 2023, 30, 10732748231168318. [Google Scholar] [CrossRef]
- Coates, AS; Hürny, C; Peterson, HF; Bernhard, J; Castiglione-Gertsch, M; Gelber, RD; et al. Quality of life scores predict outcome in metastatic but not in early breast cancer. The Breast 2001, 10, 164–70. [Google Scholar] [CrossRef]
- İzci, F; İlgün, AS; Fındıklı, E; Özmen, V. Psychiatric Symptoms and Psychosocial Problems in Patients with Breast Cancer. J Breast Health 2016, 12, 94–101. [Google Scholar] [CrossRef]
- Park, M; Yu, S-Y; Jeon, H-L; Song, I. Factors Affecting Health-Related Quality of Life in Patients With Metastatic Breast Cancer. Journal of Breast Cancer 2023, 26, 436–45. [Google Scholar] [CrossRef] [PubMed]
- Zhan, Y; Feder, SL; Lustberg, M; Batten, J; Knobf, MT. Health-Related Quality of Life in Women With Metastatic Breast Cancer: An Integrative Review. Journal of Advanced Nursing 2025, 81, 3485–503. [Google Scholar] [CrossRef] [PubMed]
- Kocamaz, D; Düger, T. Breast Cancer and Exercise. In Breast Cancer Biology; Afroze, D, Rah, B, Ali, S, Shehjar, F, Ishaq Dar, M, S. Chauhan, S, et al., Eds.; IntechOpen, 2020. [Google Scholar] [CrossRef]
- May, AM; Velthuis, M; Travier, N; Steins Bisschop, CN; Van Der Wall, E; Peeters, P. Physical activity during cancer treatment (PACT) study: Short- and long-term effects on fatigue of an 18-week exercise intervention during adjuvant chemotherapy in patients with breast or colon cancer. JCO 2014, 32, 9535–9535. [Google Scholar] [CrossRef]
- Do, J; Cho, Y; Jeon, J. Effects of a 4-Week Multimodal Rehabilitation Program on Quality of Life, Cardiopulmonary Function, and Fatigue in Breast Cancer Patients. J Breast Cancer 2015, 18, 87. [Google Scholar] [CrossRef]
- Noble, M; Jamnik, R. Physical Activity during Breast Cancer Treatment. The Health & Fitness Journal of Canada 2009, 5–8 Pages. [Google Scholar] [CrossRef]
- Leach, HJ; Covington, KR; Pergolotti, M; Sharp, J; Maynard, B; Eagan, J; et al. Translating Research to Practice Using a Team-Based Approach to Cancer Rehabilitation: A Physical Therapy and Exercise-Based Cancer Rehabilitation Program Reduces Fatigue and Improves Aerobic Capacity. Rehabilitation Oncology 2018, 36, 206–13. [Google Scholar] [CrossRef]
- Mattick, LJ; Lin, P-J; Mustian, KM; Peppone, LJ; Gada, U; Samuel, SR; et al. Walking dose required to achieve a clinically meaningful reduction in cancer-related fatigue among patients with breast cancer receiving chemotherapy: A URCC NCORP nationwide prospective cohort study. JCO 2024, 42, 12008–12008. [Google Scholar] [CrossRef]
- Bahçaci, U; Uysal, SA; Namal, E. Relaxation training via tele-rehabilitation program in patients with breast cancer receiving chemotherapy during COVID-19. DIGITAL HEALTH 2024, 10, 20552076241261909. [Google Scholar] [CrossRef]
- Fereidouni, Z; Dehghan Abnavi, S; Ghanbari, Z; Gashmard, R; Zarepour, F; Khalili Samani, N; et al. The Impact of Cancer on Mental Health and the Importance of Supportive Services. Galen Med J 2024, 13, e3327. [Google Scholar] [CrossRef] [PubMed]
- Galway, K; Black, A; Cantwell, MM; Cardwell, CR; Mills, M; Donnelly, M. Psychosocial interventions to improve quality of life and emotional wellbeing for recently diagnosed cancer patients. Cochrane Database Syst Rev 2012, 2012, CD007064. [Google Scholar] [CrossRef]
- Dinapoli, L; Colloca, G; Di Capua, B; Valentini, V. Psychological Aspects to Consider in Breast Cancer Diagnosis and Treatment. Curr Oncol Rep 2021, 23, 38. [Google Scholar] [CrossRef]
- D’Egidio, V; Sestili, C; Mancino, M; Sciarra, I; Cocchiara, R; Backhaus, I; et al. Counseling interventions delivered in women with breast cancer to improve health-related quality of life: a systematic review. Qual Life Res 2017, 26, 2573–92. [Google Scholar] [CrossRef]
- Jelvehzadeh, F; Dogaheh, ER; Bernstein, C; Shakiba, S; Ranjbar, H. The effect of a group cognitive behavioral therapy on the quality of life and emotional disturbance of women with breast cancer. Support Care Cancer 2022, 30, 305–12. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M; Huang, L; Feng, Z; Shao, L; Chen, L. Effects of cognitive behavioral therapy on quality of life and stress for breast cancer survivors: a meta-analysis. Minerva Med 2017, 108, 84–93. [Google Scholar] [CrossRef]
- Tan, Y; Qin, M; Liao, B; Wang, L; Chang, G; Wei, F; et al. Effectiveness of Peer Support on Quality of Life and Anxiety in Breast Cancer Patients: A Systematic Review and Meta-Analysis. Breast Care (Basel) 2023, 18, 49–59. [Google Scholar] [CrossRef]
- Tehrani, AM; Farajzadegan, Z; Rajabi, FM; Zamani, AR. Belonging to a peer support group enhance the quality of life and adherence rate in patients affected by breast cancer: A non-randomized controlled clinical trial*. J Res Med Sci 2011, 16, 658–65. [Google Scholar] [PubMed]
- Ruiz-Romeo, M; Ciria-Suarez, L; Medina, JC; Serra-Blasco, M; Souto-Sampera, A; Flix-Valle, A; et al. Empowerment among breast cancer survivors using an online peer support community. Support Care Cancer 2025, 33, 56. [Google Scholar] [CrossRef]
- Aristokleous, I; Karakatsanis, A; Masannat, YA; Kastora, SL. The Role of Social Media in Breast Cancer Care and Survivorship: A Narrative Review. Breast Care (Basel) 2023, 18, 193–9. [Google Scholar] [CrossRef]
- Bao, T; Basal, C; Seluzicki, C; Li, SQ; Seidman, AD; Mao, JJ. Long-term chemotherapy-induced peripheral neuropathy among breast cancer survivors: prevalence, risk factors, and fall risk. Breast Cancer Res Treat 2016, 159, 327–33. [Google Scholar] [CrossRef]
- Chow, R; Novosel, M; So, OW; Bellampalli, S; Xiang, J; Boldt, G; et al. Duloxetine for prevention and treatment of chemotherapy-induced peripheral neuropathy (CIPN): systematic review and meta-analysis. BMJ Support Palliat Care 2023, 13, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Magnowska, M; Iżycka, N; Kapoła-Czyż, J; Romała, A; Lorek, J; Spaczyński, M; et al. Effectiveness of gabapentin pharmacotherapy in chemotherapy-induced peripheral neuropathy. Ginekol Pol 2018, 89, 200–4. [Google Scholar] [CrossRef]
- Mezzanotte, JN; Grimm, M; Shinde, NV; Nolan, T; Worthen-Chaudhari, L; Williams, NO; et al. Updates in the treatment of chemotherapy-induced peripheral neuropathy. Curr Treat Options Oncol 2022, 23, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Binkhorst, L; Mathijssen, RHJ; van Herk-Sukel, MPP; Bannink, M; Jager, A; Wiemer, EAC; et al. Unjustified prescribing of CYP2D6 inhibiting SSRIs in women treated with tamoxifen. Breast Cancer Res Treat 2013, 139, 923–9. [Google Scholar] [CrossRef]
- Busby, J; Mills, K; Zhang, S-D; Liberante, FG; Cardwell, CR. Selective serotonin reuptake inhibitor use and breast cancer survival: a population-based cohort study. Breast Cancer Research 2018, 20, 4. [Google Scholar] [CrossRef]
- Biglia, N; Torta, R; Roagna, R; Maggiorotto, F; Cacciari, F; Ponzone, R; et al. Evaluation of low-dose venlafaxine hydrochloride for the therapy of hot flushes in breast cancer survivors. Maturitas 2005, 52, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Santen, RJ; Stuenkel, CA; Davis, SR; Pinkerton, JV; Gompel, A; Lumsden, MA. Managing Menopausal Symptoms and Associated Clinical Issues in Breast Cancer Survivors. The Journal of Clinical Endocrinology & Metabolism 2017, 102, 3647–61. [Google Scholar] [CrossRef]
- Hickey, M; Saunders, C; Partridge, A; Santoro, N; Joffe, H; Stearns, V. Practical clinical guidelines for assessing and managing menopausal symptoms after breast cancer. Annals of Oncology 2008, 19, 1669–80. [Google Scholar] [CrossRef]
- Romanos-Nanclares, A; Willett, WC; Rosner, BA; Collins, LC; Hu, FB; Toledo, E; et al. Healthful and unhealthful plant-based diets and risk of breast cancer in U.S. women: results from the Nurses’ Health Studies. Cancer Epidemiol Biomarkers Prev 2021, 30, 1921–31. [Google Scholar] [CrossRef] [PubMed]
- Farvid, MS; Spence, ND; Rosner, BA; Barnett, JB; Holmes, MD. Associations of low-carbohydrate diets with breast cancer survival. Cancer 2023, 129, 2694–704. [Google Scholar] [CrossRef] [PubMed]
- Gabel, K; Cares, K; Varady, K; Gadi, V; Tussing-Humphreys, L. Current Evidence and Directions for Intermittent Fasting During Cancer Chemotherapy. Advances in Nutrition 2022, 13, 667–80. [Google Scholar] [CrossRef]
- Shen, S; Unger, JM; Crew, KD; Till, C; Greenlee, H; Gralow, J; et al. Omega-3 fatty acid use for obese breast cancer patients with aromatase inhibitor-related arthralgia (SWOG S0927). Breast Cancer Res Treat 2018, 172, 603–10. [Google Scholar] [CrossRef]
- Zhang, Y; Sun, Y; Li, D; Liu, X; Fang, C; Yang, C; et al. Acupuncture for Breast Cancer: A Systematic Review and Meta-Analysis of Patient-Reported Outcomes. Front Oncol 2021, 11, 646315. [Google Scholar] [CrossRef]
- Sasaki, Y; Cheon, C; Motoo, Y; Jang, S; Park, S; Ko, S-G; et al. Complementary and Alternative Medicine for Breast Cancer Patients: An Overview of Systematic Reviews. YAKUGAKU ZASSHI 2019, 139, 1027–46. [Google Scholar] [CrossRef]
- Cramer, H; Lauche, R; Klose, P; Lange, S; Langhorst, J; Dobos, GJ. Yoga for improving health-related quality of life, mental health and cancer-related symptoms in women diagnosed with breast cancer. Cochrane Database of Systematic Reviews 2017, 2017. [Google Scholar] [CrossRef]
- Greaney, SK; Amin, N; Prudner, BC; Compernolle, M; Sandell, LJ; Tebb, SC; et al. Yoga Therapy During Chemotherapy for Early-Stage and Locally Advanced Breast Cancer. Integr Cancer Ther 2022, 21, 15347354221137285. [Google Scholar] [CrossRef] [PubMed]
- Chen, T; Klein, P; Xing, T; Shao, T. Abstract P2-12-03: A yoga program for breast cancer patients undergoing chemotherapy: Effects on quality of life and chemotherapy-associated symptoms. Cancer Research 2020, 80, P2-12-03-P2-12–03. [Google Scholar] [CrossRef]
- S, A; K, A; Shetty, A; S Shetty, V. Exploring the Role of Yoga in Alleviating Chemotherapy - Induced Fatigue and Nausea-Vomiting in Women with Breast Cancer - A Narrative Review. J Ayurveda Integr Med Sci 2025, 10, 155–9. [Google Scholar] [CrossRef]
- Rofaiel, S; Muo, EN; Mousa, SA. Pharmacogenetics in breast cancer: steps toward personalized medicine in breast cancer management. Pharmgenomics Pers Med 2010, 3, 129–43. [Google Scholar] [CrossRef]
- Prakash, GH; SK, D; Pk, K; Arun, V; Yadav, D; Gopi, A; et al. 422P Digital Patient-Reported Outcomes in Cancer Care: Analysis of Quality of Life and Symptom Trajectories Using a Mobile Health Platform. ESMO Open 2025, 10. [Google Scholar] [CrossRef]
- Aanes, SG; Wiig, S; Nieder, C; Haukland, EC. Implementing digital patient-reported outcomes in routine cancer care: barriers and facilitators. ESMO Real World Data and Digital Oncology 2024, 6, 100088. [Google Scholar] [CrossRef]
- Giesinger, J; Kemmler, G; Meraner, V; Gamper, E-M; Oberguggenberger, A; Sperner-Unterweger, B; et al. Towards the Implementation of Quality of Life Monitoring in Daily Clinical Routine: Methodological Issues and Clinical Implication. Breast Care (Basel) 2009, 4, 148–54. [Google Scholar] [CrossRef] [PubMed]
- Søndergaard, SR; Bechmann, T; Maae, E; Nielsen, AWM; Nielsen, MH; Møller, M; et al. Shared decision making with breast cancer patients - does it work? Results of the cluster-randomized, multicenter DBCG RT SDM trial. Radiother Oncol 2024, 193, 110115. [Google Scholar] [CrossRef]
Figure 1.
Multidimensional impact of chemotherapy on quality of life in breast cancer survivors. The physical domain includes fatigue, pain, gastrointestinal disturbances, and sexual/menopausal symptoms. Psychological impacts encompass depression, anxiety, cognitive impairment, self-image, and body perception. Social consequences involve changes in relationships, social roles, and challenges in returning to work or maintaining productivity. Economic burden is reflected through financial toxicity due to treatment costs. Cultural influences shape illness perception, spirituality, and beliefs surrounding treatment. Together, these interconnected factors underscore the need for holistic, patient-centered survivorship care.
Figure 1.
Multidimensional impact of chemotherapy on quality of life in breast cancer survivors. The physical domain includes fatigue, pain, gastrointestinal disturbances, and sexual/menopausal symptoms. Psychological impacts encompass depression, anxiety, cognitive impairment, self-image, and body perception. Social consequences involve changes in relationships, social roles, and challenges in returning to work or maintaining productivity. Economic burden is reflected through financial toxicity due to treatment costs. Cultural influences shape illness perception, spirituality, and beliefs surrounding treatment. Together, these interconnected factors underscore the need for holistic, patient-centered survivorship care.
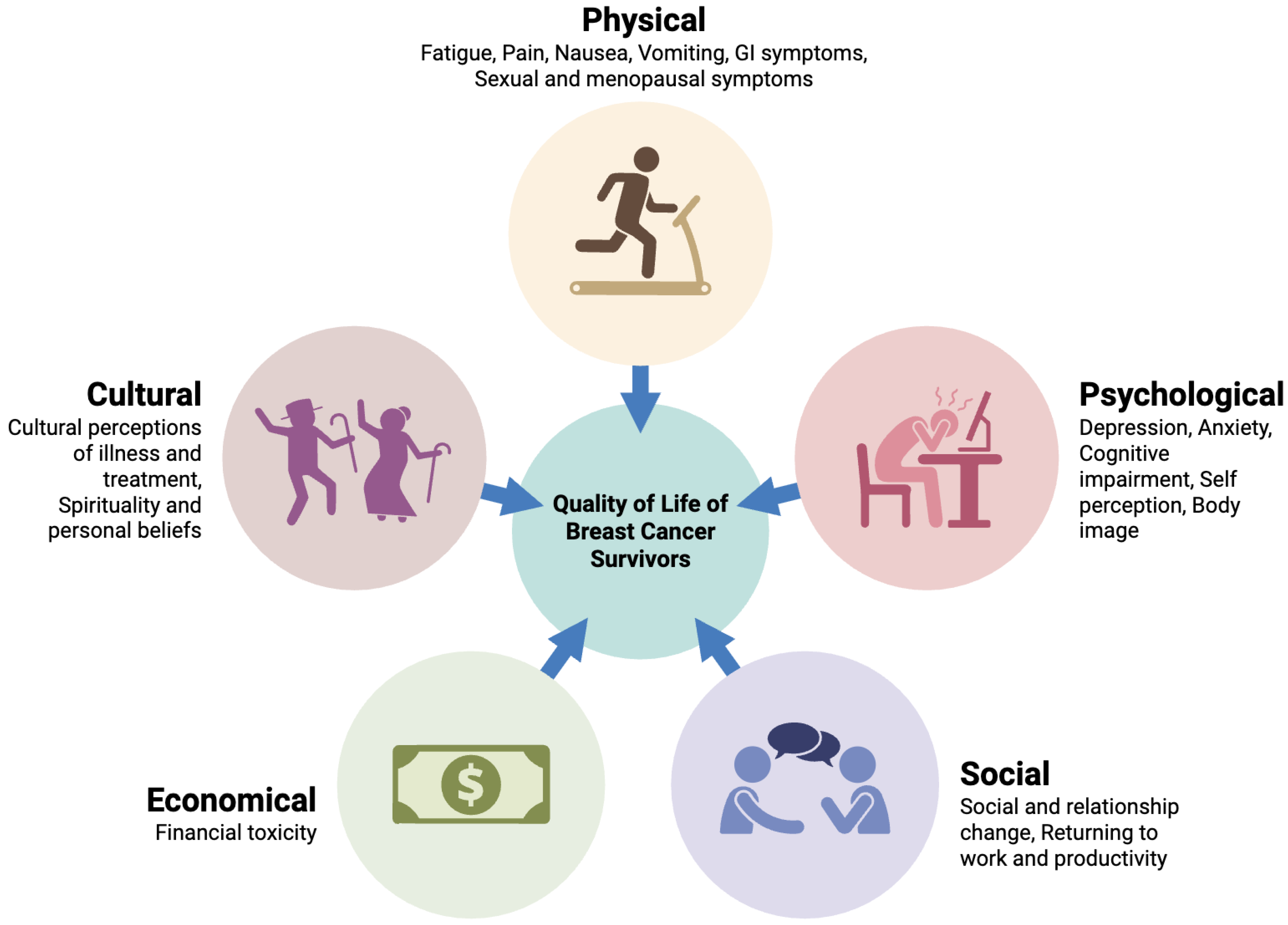

Table 1.
Comparison of breast cancer QoL assessment tools.
| Feature | EORTC QLQ-C30 + QLQ-BR23 | FACT-B (Functional Assessment of Cancer Therapy – Breast) | SF-36 (Short Form-36 Health Survey) |
|---|---|---|---|
| Developer | European Organisation for Research and Treatment of Cancer (EORTC) | FACIT Group (originally by David Cella and colleagues) | RAND Corporation / Boston Health Research Institute |
| Purpose | Cancer-specific QoL assessment with breast cancer module | Breast cancer-specific QoL assessment with general + disease items | Generic health status measure across diseases |
| Target Population | Cancer patients; QLQ-BR23 for breast cancer specifically | Breast cancer patients | General adult population |
| Structure | QLQ-C30: 30 items (global + 5 functional + 3 symptom + 6 single items) QLQ-BR23: 23 items (breast-specific) |
37 items total (FACT-G core + 10 breast-specific items) | 36 items across 8 health domains |
| Domains Measured | - Physical, role, cognitive, emotional, social functioning - Fatigue, nausea, pain, appetite, sleep, financial - BR23: body image, arm symptoms, sexual functioning |
- Physical well-being - Social/family well-being - Emotional well-being - Functional well-being - Breast-specific concerns |
- Physical functioning - Role limitations - Bodily pain - General health - Vitality - Social functioning - Emotional well-being |
| Scoring System | 0–100 linear transformation; higher score = better functioning / worse symptoms | 0–4 Likert scale (total score 0–148); higher = better QoL | 0–100 for each domain; higher = better health |
| Time Frame Referenced | Past week | Past 7 days | Past 4 weeks |
| Psychometric Validity | Widely validated in cancer populations; BR23 specific to breast cancer | Strong reliability and validity in breast cancer populations | Broadly validated across general populations and diseases |
| Sensitivity to Change | High sensitivity to treatment effects (e.g., chemo, surgery, radiation) | High sensitivity in detecting QoL changes due to breast cancer | Less sensitive to cancer-specific QoL changes |
| Strengths | - Disease-specific detail - Modules available for different cancers - Good responsiveness in clinical trials |
- Brief and easy to use - Breast-specific - Suitable for trials and clinics |
- Comprehensive overview of general health - Normative data available |
| Limitations | - Slightly longer to administer (53 items total) - May require license for use |
- Less detailed symptom tracking compared to EORTC - License required |
- Not cancer-specific - Misses disease-relevant issues (e.g., body image) |
| Languages & Global Use | Available in >100 languages; widely used in Europe & trials | Available in >60 languages; used globally | Available in many languages; widespread in public health |
| Best Use Case | Clinical trials and studies requiring detailed breast-specific QoL data | Routine clinical practice and patient monitoring | General population studies or comparison across conditions |
Table 2.
Comparison of patient-reported outcomes vs. clinician-reported metrics in breast cancer QoL assessment.
Table 2.
Comparison of patient-reported outcomes vs. clinician-reported metrics in breast cancer QoL assessment.
| Dimension | Patient-Reported Outcomes (PROs) | Clinician-Reported Metrics |
|---|---|---|
| Definition | Direct reports from patients about their health status, symptoms, and functional impact—without interpretation by clinicians. | Observations, diagnoses, or measurements made by clinicians using clinical exams, lab tests, or standard toxicity scales. |
| Common Tools/Instruments | - EORTC QLQ-C30 / QLQ-BR23 - FACT-B - SF-36 - PROMIS - PRO-CTCAE |
- CTCAE (Common Terminology Criteria for Adverse Events) - ECOG/Karnofsky Performance Status - Lab/imaging results |
| Primary Focus | Subjective experience of symptoms (fatigue, pain, anxiety, daily functioning, body image, etc.) | Objective signs of toxicity, disease progression, or functional decline |
| Sensitivity to Change | High sensitivity to subtle changes in physical, emotional, or cognitive symptoms. | Often insensitive to mild or subjective symptoms; detects only clinically observable or measurable changes. |
| Examples of What Is Measured | - Pain, fatigue, insomnia - Emotional distress - Sexual health - Physical functioning - Cognitive symptoms |
- Neutropenia, anemia - Organ function tests - Tumor size changes - Performance status |
| Strengths | - Captures real patient experience - Enables early detection of QoL decline - Enhances shared decision-making |
- Standardized, objective measurements - Critical for treatment safety, dosing, and trial comparability |
| Limitations | - Subject to reporting bias - Requires patient literacy and engagement - May lack standardization across populations |
- May underestimate symptom burden - Ignores subjective domains (e.g., mood, sexuality) - Less patient-centered |
| Use in Clinical Trials | Increasingly used to assess treatment tolerability and QoL endpoints (e.g., PRO-CTCAE mandated in some trials) | Longstanding use in toxicity grading and clinical safety monitoring |
| Regulatory Relevance | Recognized by FDA/EMA for supporting drug labeling when validated; critical for value-based, patient-centered care | Required for drug approval, trial protocols, and adverse event reporting |
Table 3.
Interventions and supportive care to mitigate QoL decline in breast cancer chemotherapy.
| Intervention Type | Target Symptoms/QoL Domains | Mechanism of Action | Examples / Modalities |
|---|---|---|---|
| Physical Exercise & Rehabilitation | Fatigue, physical function, pain, lymphedema, sleep, mood | Improves mitochondrial function, reduces inflammation, enhances muscle mass and endurance | Aerobic training (e.g., walking), resistance exercise, supervised rehab programs |
| Psychosocial Interventions | Anxiety, depression, emotional distress, body image, coping | Cognitive restructuring, emotional support, behavioral activation | CBT (Cognitive Behavioral Therapy), mindfulness-based stress reduction (MBSR), peer support groups |
| Pharmacologic Management | Neuropathy, depression, menopausal symptoms, nausea, anemia | Neurotransmitter modulation, hormonal replacement, symptom suppression | - Duloxetine for CIPN - SSRIs/SNRIs for depression - Gabapentin for hot flashes - 5-HT3 antagonists for nausea |
| Complementary Therapies | Sleep disturbance, stress, anxiety, fatigue, pain | Modulation of autonomic nervous system, endorphin release, stress hormone reduction | Acupuncture, yoga, massage, aromatherapy, Tai Chi, meditation |
| Nutritional Support | GI distress, fatigue, malnutrition, immune function, weight management | Supports gut microbiota, mitigates mucositis, provides metabolic substrates | Dietitian-led plans, high-protein meals, hydration strategies, enteral support if needed |
| Sexual Health Counseling | Libido loss, vaginal dryness, body image, relationship intimacy | Psychoeducation, behavioral therapy, local hormonal treatment | Vaginal moisturizers/lubricants, pelvic floor therapy, couples therapy |
| Hormone Replacement / Management | Menopausal symptoms (e.g., hot flashes, vaginal atrophy), osteoporosis | Symptom relief via estrogen modulation (non-hormonal preferred in hormone-receptor+ cases) | Gabapentin, clonidine, SSRIs/SNRIs; vaginal estrogens in select cases |
| Financial Counseling | Financial toxicity, employment loss, insurance stress | Resource navigation, cost-sharing strategies, patient advocacy | Oncology social worker support, patient navigation services, financial aid programs |
| Patient Navigation & Education | Empowerment, treatment adherence, communication, decision-making | Enhances health literacy, reduces anxiety, supports shared decision-making | Nurse navigators, survivorship care plans, educational workshops |
| Digital & Remote Monitoring | Symptom tracking, timely intervention, continuity of care | Early detection of worsening symptoms, reduced clinic burden | PRO platforms, telemedicine, mobile health apps (e.g., for fatigue, mood) |
| Spiritual / Existential Support | Meaning-making, emotional resilience, end-of-life planning | Addresses spiritual well-being, helps coping with fear of recurrence or mortality | Chaplaincy, existential therapy, life review interventions |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



