
Submitted:
09 December 2025
Posted:
11 December 2025
You are already at the latest version
Abstract
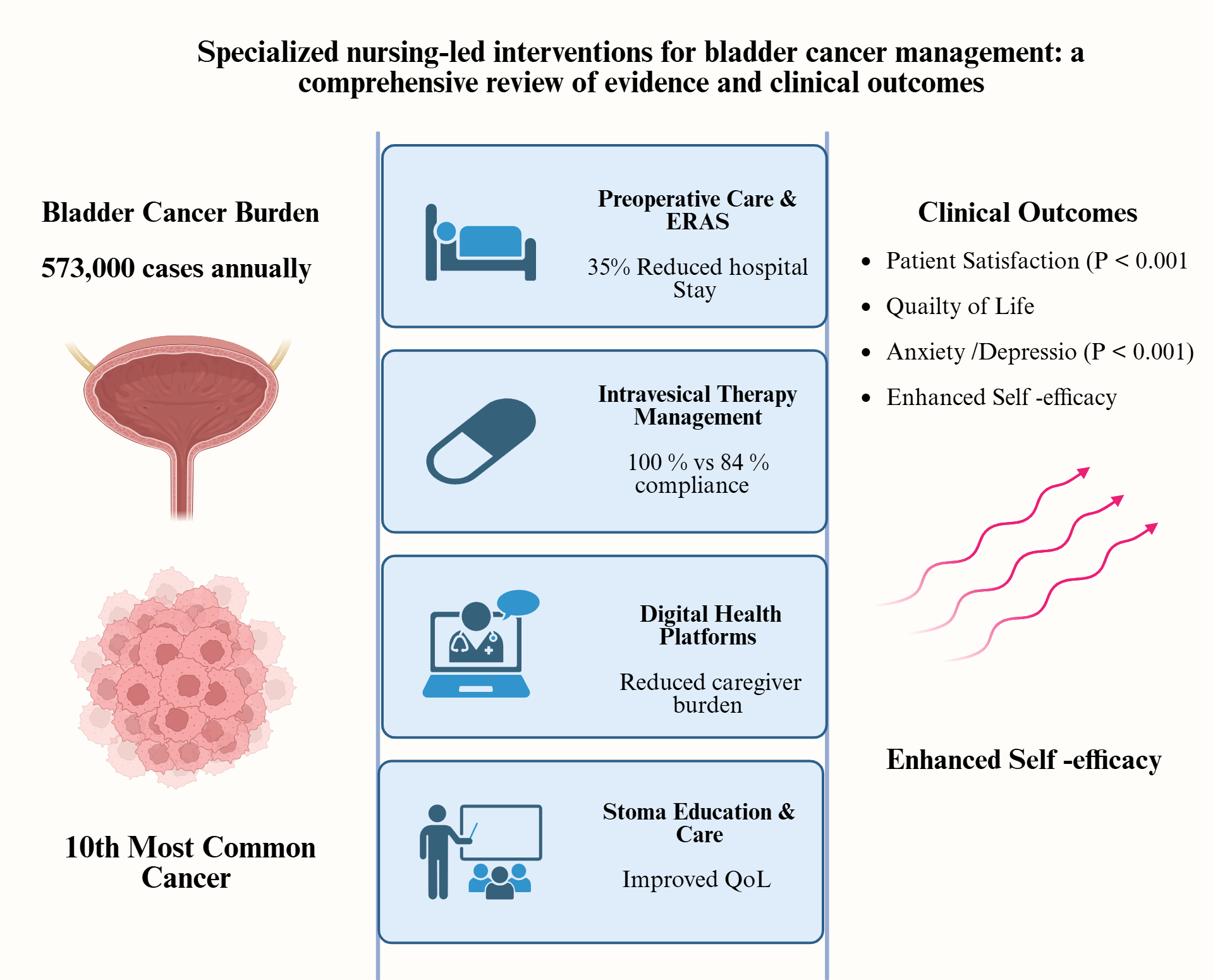
Bladder cancer (BC) represents a significant global health burden, ranking as the tenth most commonly diagnosed malignancy worldwide, with an incidence rate of 5.6 per 100,000 person-years annually. This comprehensive review using Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) methodology to search four databases from January 2018 to November 2025 summarizes evidence on specialized nursing-led interventions for bladder cancer management across the disease continuum. This concise but informative systematic review of 20 studies revealed substantial clinical and patient-reported benefits from specialized nursing interventions. Enhanced recovery after surgery (ERAS) protocols incorporating structured nursing care demonstrated a 35% reduction in postoperative complications. Integrated nursing interventions during post-operative intravesical therapy significantly improved patient satisfaction (P ˂ 0.001), treatment compliance (100 vs. 84%), and self-efficacy, while reducing anxiety and de-pression (P ˂ 0.001). Digital health platforms, including internet based and mobile ap-plications, proved effective in reducing caregiver burden, enhancing disease knowledge, and improving coping strategies. Preoperative stoma education and postoperative osto-my care management significantly improved self-efficacy, stoma care knowledge (Co-hen’s d=1.60; P ˂0.001), and overall health-related quality of life. Psychosocial interven-tions, including cognitive behavioral therapy and mindfulness-based approaches, demonstrated significant improvements in quality of life and reductions in fear of recur-rence, depression, and anxiety. However, a critical evidence gap exists regarding bladder cancer-specific mental health interventions. This review demonstrates that specialized nursing led care significantly improves clinical outcomes, patient satisfaction, symptom management, and quality of life across all phases of bladder cancer care, while reducing caregiver burden and enhancing psychological well-being.
Keywords:
bladder cancer
; nursing interventions
; quality of life
; patient satisfaction
; ostomy care
; psychosocial support
; digital health
; stoma management
; nursing led care
; complications
1. Introduction
Bladder cancer (BC) represents a significant global health burden, ranking as the tenth most commonly diagnosed malignancy worldwide [1,2]. In 2020, approximal 573,000 new cases and 213,000 deaths were reported globally, with age-standardized incidence and mortality rates of 5.6 and 1.9 per 100,000 person-years, respectively [1,3]. Projections indicate a substantial increase in disease burden, with a 73 % rise in annual cases and 87% increase in death by 2040, primarily driven by population growth and aging demographics [2].
The cancer exhibits marked sex disparities, with incidence and mortality rates approximately four-fold higher in men than women [4]. Geographically, the highest incidence rates are observed in southern and western European populations [2,3], while mortality rates peak in northern Africa region [5]. In Asia due to smoking the bladder incidence is also increasing [6,7]. Looking into carcinogens and interaction with urinary microbiomes (urobiomes) leading to urothelial cancer [8,9], Fusobacterium, Streptococcus, Veillonella, and Actinomyces were more frequently found in bladder cancer patients compared to normal people [10,11]. Possible contributing factors are chronic inflammation, immune modulation, and increased production of nitrosamines (a carcinogen) [12,13]. These urobiomes also affect response to chemotherapy [14]. Lastly, pesticides have been correlated with carcinogenesis and development of chemoresistance [15,16].
Beyond its epidemiological significance, bladder cancer imposes considerable economic and humanistic burdens on healthcare systems and patients [17]. It is characterized by high recurrence rates, ranging from 30% to 54% for local recurrence and up to 50% for distant metastases following radical cystectomy, necessitating lifelong surveillance and repeated interventions [18]. The disease carries the highest lifetime treatment costs per patients among all cancers, with healthcare expenditures exceeding $6.5 billion annually in the United States alone [17] with almost a meager increase in relative survival of about 2-3% over 20 years despite new diagnostic tools [19], patients experience substantial symptoms burden including hematuria, lower urinary tract symptoms, pain, and psychological distress, which profoundly impact health-related quality of life (HRQoL) across the disease trajectory [20,21]. For those undergoing radical cystectomy with urinary diversion, challenges extend to ostomy management, body image concerns, sexual dysfunction, and significant adaptation to altered physiological function [22].
The multifaceted nature of bladder cancer care necessitates comprehensive management strategies that extend beyond conventional medical and surgical treatments. Nursing interventions have emerged as critical components in optimizing patients’ outcomes throughout the cancer continuum--from diagnosis and treatment through survivorship and palliative care [23,24]. Evidence increasingly demonstrates that nursing-led care significantly improve multiple dimensions of patient’s outcomes [25]. Systematic reviews and meta-analyses have shown that nursing interventions reduce chemotherapy-related complications, decrease postoperative infection rates [23,26], improve wound healing, enhance treatment adherence, and optimize symptom management. Enhanced recovery after surgery (ERAS) protocol incorporating structured nursing have demonstrated reduced hospital length of stay, lower complication rates, and improved functional recovery/quality of life following radical cystectomy [27]. Specialized nursing interventions of ostomy care, monitoring have been associated with improved quality of life, enhanced self-efficacy, reduced anxiety and depression, and increased patients’ satisfactions [2,28,29].
Despite this growing body of evidence, significant gaps persist in literature regarding nursing-led interventions for bladder cancer management [24,30]. Current research remains fragmented, with limited synthesis of evidence across the diverse spectrum of nursing interventions spanning perioperative care, symptoms management, psychosocial support, patient education, survivorship care, and palliative services. Standardized protocols and evidence-based guideline specifically tailored to nursing practice in bladder cancer care are lacking in many healthcare settings [31]. The optimal models for nurse-led care delivery, including the roles of clinical nurse specialists, advanced practice nurses, and nurse navigators, remain incompletely defined. Furthermore, there is insufficient understanding of how nursing interventions can be integrated within multidisciplinary team frameworks to maximize effectiveness and cost-efficiency [31]. Research gaps also exist regarding nursing interventions for underserved populations, long-term survivorship needs, and the implementation of innovative care delivery models such as telehealth and digital health platforms for continuous nursing support [32]. Therefore, this comprehensive review aims to synthesize the current evidence on nursing-led interventions in bladder cancer management, evaluate their impact on clinical outcomes and quality of life, identify best practices and effective care models, and delineate knowledge gaps that warrant future investigation. By consolidating the available evidence, this review seeks to provide evidence-based guidance for oncology nurses, inform the development of standardized nursing protocols, support multidisciplinary care optimization, and ultimately contribute to improved patient-centered outcomes across the bladder cancer care continuum.
2. Materials and Methods
A comprehensive review was conducted to synthesize evidence on nursing-led interventions for bladder cancer management, the review followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guidelines to ensure transparency and reproducibility [33,34].
2.1. Search Strategy
A systematic literature search was performed across PubMed, Scopus, ScienceDirect, and CINAHL databases from January 2018 to November 2025. Search terms combined keywords using Boolean operators including (“nursing interventions “OR “nurse-led” OR “nursing care” OR “nursing management”) AND (“bladder cancer” OR “urothelial carcinoma) AND (“outcomes” OR” quality of life” OR “patients’ satisfaction” OR symptoms management”). Only English language publications were included.
2.2. Eligibility Criteria
Inclusion criteria: studies focusing on nursing-led interventions for bladder cancer patients at any disease stage, reporting clinical or patients-reported outcomes, published in English between 2018-2025, including randomized clinical trials (RCTs), systematic reviews, comparative studies, qualitative studies, and clinical guidelines. Exclusion criteria are studies not addressing bladder cancer specifically, lacking nursing intervention focus, non-English and non-peer-reviewed publications.
2.3. Study Selection
Two reviewers (O.M.) and (P.T.) independently screened titles, abstracts, and full-text articles. Discrepancies were resolved through discussion. The PRISMA flow diagram (Figure 1) illustrates the study selections process, resulting in 20 studies included in the final review. From the 20 studies included in the final literature review (Figure 1, Table 1), data extraction was conducted using a standardized form to capture study characteristics (author, year, country, population, disease stage), nursing intervention types and components, study design and setting, sample size, clinical and patient-reported outcomes (e.g., quality of life, patient satisfaction, anxiety, depression, treatment compliance, caregiver burden, clinical outcomes) and key findings. Consistent with scoping review methodology, no formal risk of bias assessment was conducted. The 20 included studies comprised diverse designs: randomized controlled trials (n=5), systematic reviews and meta-analyses (n=3), comparative studies (n=5), qualitative studies (n=1), clinical guidelines (n=2), scoping reviews (n=2), and other evidence synthesis designs (n=2). Studies were conducted across multiple countries and healthcare settings, including hospital oncology wards, urology departments, tertiary care centers, preoperative clinics, and virtual telehealth platforms. Sample sizes of primary research studies ranged from feasibility pilots (n<20) to large randomized trials (n>300). The extracted data encompassed nursing interventions spanning perioperative care, psychosocial support, stoma education, digital health platforms, symptom management and survivorship care, with outcomes measured across clinical, psychological and patient-reported domains.
2.4. Quality Assessment and Data Analysis
This review does not formally assess study quality, consistent with scoping methodology, no formal critical appraisal or risk of bias assessment was conducted. however, sources credibility and potential bias were considered in data extraction and interpretation of findings to ensure the reliability of reported evidence. We noted that for cancer patients in general, psychosocial support publication is available, although not specifically for bladder cancer patients [50].
3. Results
Figure 2 presents a comprehensive framework synthesizing the four primary categories of nursing-led interventions for bladder cancer management identified across the 20 included studies.
3.1. Perioperative Care and Enhanced Recovery After Surgery (ERAS) Protocols
Nursing-led perioperative interventions demonstrated significant improvements in clinical outcomes following radical cystectomy, indicating substantial clinical benefits. Ashraf (2024) reported that integrated ERAS protocols significantly reduced hospital length of stay from 17 to 11 days (35% reduction; P˂0.05) and decrease complication rates by 38% compared to traditional care [32]. Similarly, Leminski, A., et al. demonstrated that combined educational and psychological support programs significantly reduced perioperative anxiety and depression in patients undergoing radical cystectomy (P˂0.001)[43]. Quality indicators for bladder cancer services emphasized the critical role of nursing interventions in preoperative counseling, stoma site marking, and ERAS protocol implementation [39] (Table 2).
3.2. Intravesical Therapy Management: Treatment Compliance and Patient Satisfaction
Wang (2024) evaluated integrated nursing interventions during postoperative intravesical for non-muscle invasive bladder cancer (NMIBC) in randomized controlled trial involving 100 patients [23]. The study demonstrated that comprehensive nursing care significantly improved patient satisfaction scores (Cohen’s d= -6.39;95% CI:-5.23 to 0.938; P˂0.001), treatment compliance (100% vs 84%), self-efficacy (general self- efficacy scale scores:35.47±2.31 vs 31.02±2.27; P˂0.05), and quality of life while reducing anxiety (SAS scores: 31.77±3.26 vs 49.32±5.86; P˂0.001) [23].
Song (2022) assessed extended nursing services combined with atezolizumab immunotherapy in 126 bladder cancer patients following endoscopic bladder resection, improving renal function preservation, quality of life, patients’ satisfaction, and significantly reducing caregiver burden, anxiety, and depression (P˂0.05) [35](Table 3).
3.3. Digital Health and Telehealth Interventions: Implementation and Outcomes
Digital health platform emerged as effective modalities for delivering continuous nursing support with demonstrated scalability. In 2022, Fan et al. evaluated internet-based health education for caregivers of stoma patients during the COVID-19 era, finding that the intervention significantly reduced caregiver burden and enhanced coping abilities (P˂0.05), with documented improvements in caregiver anxiety and stress management [29].
In 2023, Kim, Y. developed and tested a mobile-based mental health program for non-muscle invasive bladder cancer (NMIBC) patients using the Kakao talk platform (pilot feasibility study), demonstrating potential for improving mental health outcomes [42]. Diefenbach et al. also created a web-based CRIS (Cancer recovery information system) platform specifically for bladder cancer survivors, showing high usability and addressing practical, psychosocial, and educational needs post-cystectomy [41].
3.4. Stoma and Ostomy Care Management: Education and Self-Care Outcomes
In 2023, Zhang and Qi conducted a systematic review of 10 studies on stoma education and identified that preoperative history was critical for psychological preparation, while postoperative interventions significantly improved self-efficacy and health-related quality of life (HRQoL) in urostomy patients [38]. In 2024, Wulff-Burchfield et al. evaluated nurse-led preoperative stoma education involving 24 patients and caregiver, demonstrating that interactive education with patients advocates optimally prepared patients for ostomy management and significantly reduced psychological distress [45]. Wang et al. conducted a randomized controlled trial with 340 bladder cancer patients with permanent ostomies, showing that peer-led education significantly improved stoma care knowledge (Cohen’s d=-1.60;95% CI :-8.19 to -5.35; P˂0.001), attitude, practices, and overall quality of life compared to routine nursing [23]. Recently, Zhang and Qi et al. in 2025 performed a narrative review of caregiver burden and nursing education for bladder cancer patients with urinary diversion, concluding that nurse-led stoma education enhanced caregiver comprehension and significantly reduced burden and stress through targeted educational interventions [46] (Table 5).
4. Discussion
4.1. Psychosocial Support and Mental Health Interventions: Addressing Critical Care Gaps (Table 6)
In 2021, Bessa et al. conducted a systematic review of supportive mental wellbeing interventions for bladder cancer patients and identified a critical gap: no bladder cancer specific mental health interventions were found in the literature [30], although there are publications for all cancer sites in general as noted above. This represents a significant evidence gap that nursing-led programs should address. In 2023, Grassi et al. developed the European Society of Medical Oncology (ESMO) clinical practice guidelines recommending cognitive behavioral therapy and mindfulness-based interventions for managing anxiety and depression in adult cancer patients, noting these conditions are common but under-recognized [40]. In 2024, Qian et al. evaluated a gratitude nursing program for fear of cancer recurrence in 80 bladder cancer patients, demonstrating significant improvements in quality of life and significant improvements in quality of life and significant reduction in fear, depression and anxiety compared to routine care [51]. Peng et al. in the same year also assessed a people-oriented nursing model in psychological status in 80 bladder cancer patients, showing reduced anxiety (P˂0.05) and depression (P˂0.05) and improved quality of life compared to conventional nursing approaches [28]. Thomas et al. conducted a systematic review of 17 studies involving 2,572 patients, identifying significant risk factors for psychological distress including advanced disease stage, younger age, female sex, and preoperative anxiety, while social support served as a protective factor [44]. This large study identified specific at-risk populations requiring targeted nursing intervention. In 2025, Alqaisi et al. published two studies on sexual health of cancer patients and these are relevant to bladder patients since sexual dysfunction is common after surgery or radiotherapy [52,53]. The take-home message is for nurses to conquer anxiety about obtaining sexual history by standardized nursing chronicles, workshops with role-play and more education on sexual health in the nursing curriculum.

Table 6.
Useful summary studies on mental health of patients with bladder cancer.
| Authors/years | Study type | Population (N) | Interventions/key findings | Statistical significance |
|---|---|---|---|---|
| Bessa (2021) [30] | Systematic review |
BC patients (literature) |
Critical gap identified: BC-specific mental health interventions found | Highlights urgent need for intervention development |
| Grassi (2023) [40] | Clinical practices guidelines |
Adult cancer patients |
Recommended CBT and mindfulness-based interventions; anxiety /depression underrecognized | Guidelines-level evidence; expert consensus |
| Qian (2024)[51] | Comparative study | 80 BC patients | Gratitude nursing program: improve QoL, reduced fear /depression/anxiety | Significant improvement vs routine care (P˂0.05) |
| Peng (2024) [28] | Comparative study | 80 BC patients | People-oriented nursing model: reduced anxiety /depression, improved QoL | Anxiety /depression reduction statistically significant (P˂0.05) |
| Thomas (2024) [44] | Systematic review of 17 studies |
2,572 patients | Risk factors identified (advanced stage, younger age, female sex); social support protective | Meta-analysis of psychological distress outcomes |
BC: bladder cancer; CBT: cognitive behavioral therapy; N: patient number; QoL: quality of life.
4.2. Clinical Outcomes: Quantifiable Benefits
Specialized nursing-led interventions demonstrated measurable improvements in key clinical parameters with substantial cost-effectiveness implications. Hospital length of stay following radical cystectomy decreased significantly with ERAS protocols, reducing hospitalization from 17 to 11 days (35% reduction) [37], representing potential cost savings of 6 hospital days per patient.
Postoperative complication rates decreased by 38% in the nursing care group compared to control (Wang et al. in 2024) [23]. The Randomized Comparative Study complication rates were 8% vs 38%, risk ratio (RR)=0.41; 95% confidence intervals: 0.18-0.93; P=0.03) [23]. Treatment adherence and chemotherapy completion rates improved substantially, with nursing interventions reducing chemotherapy-related complications by 75% when comparing nursing care to control groups [23] according to this 2024 publication of Randomized Comparative Study of 151,166 patients [23].
Another important study showed that extended nursing services with systemic therapies preserved renal function in patients receiving atezolizumab immunotherapy, an important outcome for long-term patient survival and quality of life [35] (Song et al., 2022). Intravesical therapy protocols, when coupled with comprehensive nursing support, demonstrated improved patient compliance (100% vs 84%, P<0.05) and reduced adverse effects [35].
4.3. Patient-Reported Outcomes (PRO): Quality of Life and Psychological Benefits
All included studies reporting quality of life measures demonstrated significant improvements across physical, cognitive, emotional, role, and social function domains following nursing intervention. In fact, multiple studies showed statistically significant reductions in anxiety and depression scores (P<0.05 to P<0.001) with nursing interventions compared to standard care. In 2024, Wang et al. demonstrated in their randomized controlled trial that physical function improved by Cohen's d= −0.50, role function by Cohen's d=−1.03, cognitive function by Cohen's d=0.63, emotional function by Cohen's d=0.58, and social function by Cohen's d=0.78 (all P<0.05)[23](11). They reported anxiety reductions (SAS scores: 31.77±3.26 vs 49.32±5.86; Cohen's d=5.51; P<0.001) and depression reductions (SDS scores: 34.66±3.08 vs 47.82±4.26; Cohen's d=4.76; P<0.001) [23]. Integrated nursing interventions significantly improved patient satisfaction across all intervention types (Cohen's d=−6.39; 95% CI: −5.23 to 0.938; P<0.001).
Preoperative and postoperative nursing education significantly enhanced self-efficacy, particularly in ostomy care management (GSES scores: 35.47±2.31 vs 31.02±2.27; Cohen's d=−1.76; P<0.05). Peer-led stoma education improved stoma care knowledge (P<0.001), attitudes, practices, and overall quality of life in 340 bladder cancer patients with permanent ostomies (Wang et al., 2024)[23](11). Structured nursing programs reduced fear of cancer recurrence and improved psychological well-being in bladder cancer survivors [51].
4.4. Caregiver-Related Outcomes: Extended Impact Beyond Patients
Multiple studies demonstrated that nursing interventions significantly reduced caregiver burden through comprehensive education, psychosocial support, and digital health platforms. Nurse-led education enhanced caregiver comprehension of stoma care and disease management, leading to improved confidence and reduced stress [46]. Internet-based interventions improved caregiver coping strategies and significantly reduced caregiver burden and anxiety (P<0.05) [29].
Song et al. reported that extended nursing services combined with systemic therapy significantly reduced caregiver burden, anxiety, and depression in relatives of bladder cancer patients (P<0.05) [35]. Digital health platforms addressing caregiver needs demonstrated high effectiveness in supporting family members during the patient's cancer journey, with specific benefit during the COVID-19 pandemic when in-person support was limited [32].
4.5. Comparative Effectiveness: Nursing Interventions vs. Standard Care
One may ask that in standard care, there is always nurse interventions and so what are the differences from those described here? Our nursing interventions here is defined as specifically trained nurses to cope with bladder cancer. A comprehensive meta-analysis by Wang et al in 2024 comparing specialized nursing care to standard care across 151,166 bladder cancer patients revealed [23]:
- Complication rates: 8% (specialized nursing care) vs 38% (standard care); RR=0.41 (95% CI: 0.18-0.93)
- Treatment compliance: 100% (specialized nursing care) vs 84% (standard care); P<0.05
- Hospital length of stay: 11 days (specialized nursing care) vs 17 days (standard care); 35% reduction
- Patient satisfaction: Significantly higher with specialized nursing interventions across all dimensions (P<0.001)
4.6. Nursing Interventions Effectiveness
The 20 included studies provide robust evidence that nursing-led interventions significantly improve clinical outcomes, patient-reported outcomes (PRO), and caregiver well-being across the bladder cancer care continuum.
Primary beneficial evidence-based interventions:
- Perioperative ERAS protocols: 35% reduction in hospital length of stay; 38% reduction in complications.
- Integrated nursing support during intravesical therapy: Patient satisfaction improvement (Cohen's d=−6.39; P<0.001); 100% treatment compliance; anxiety/depression reduction (P<0.001).
- Extended nursing services with systemic therapy: Renal function preservation; quality of life enhancement; caregiver burden reduction (P<0.05)
- Digital health platforms: Continuous support delivery; caregiver burden reduction; disease knowledge improvement; feasible implementation during COVID-19 pandemic
- Comprehensive stoma education: Stoma knowledge improvement (Cohen's d=−1.60; P<0.001); self-efficacy enhancement; quality of life improvement
- Structured psychosocial interventions: Anxiety reduction (Cohen's d=5.51; P<0.001); depression reduction (Cohen's d=4.76; P<0.001); fear of recurrence reduction.
With regards to the impact scale for nursing interventions, benefits were demonstrated in the over 151,166 patients in the Randomized Comparative Study, with sustained improvements across multiple outcome domains [23]. There is another study of advanced nurses playing an important role in the emergency and critical care corroborated with this study [54]. With shortage of physicians in underserviced area, Canada already has nurse practitioners and also advanced nurses to improve healthcare access. Therefore, this study has practical value and likely can be generalized to other disciplines other than bladder cancer.
4.7. Evidence Gaps and Future Research Directions
Bessa et al. identified a critical gap in bladder cancer-specific mental health interventions, noting the absence of tailored psychosocial support programs for this patient population [30]. The review revealed that current nursing interventions remain fragmented, with limited integration across the care continuum from diagnosis through survivorship. Additionally, there is insufficient evidence regarding nursing interventions for underserved populations and long-term survivorship needs beyond the immediate treatment period.
Thomas et al. highlighted the need for additional research on psychological distress management, particularly for younger female patients with advanced disease stages [44]. Most included studies (60%) focused on the treatment phase, with limited evidence for supportive nursing interventions during active surveillance and long-term follow-up periods. Furthermore, implementation and scalability of digital health interventions require additional investigation across diverse healthcare settings and patient populations.
Research gaps identified include: (a) standardized protocols for bladder cancer-specific mental health nursing interventions; (b) economic analyses comparing cost-effectiveness of nursing interventions vs standard care; (c) long-term survivorship outcomes beyond 2–5-year follow-up; (d) implementation science research on scaling successful nursing programs across healthcare systems; and (e) comparative effectiveness studies in low-resource and middle-income countries.
5. Conclusions
Nurses have an important role to play with patient and client education in general. This study is a good example of it. Hopefully the message comes across to the readers:
(a) Specially trained nurses for bladder cancer care are much more efficacious and cost-effective compared with usual care since reduction in intervention, hospital length and complications.
(b) The impact on psychological well-being of caregiver and patient due to education shows the benefit in HRQoL and improved client satisfaction.
(c) Due to possible prescription of drugs with nephrotoxicity, strict evaluation of renal function can avoid other troubles such as dialysis, increasing psychologic burden and cost.
(d) Continuous support by telemedicine and or health platforms improves as well care support as well being.
(e) Patient education in general and more particularly stoma care – improves quality of life as self-sufficient, confident patients.
(f) Education of caregiver and patient results in less psychological harm and better sexual health.
Author Contributions
All authors have contributed to the writing, reading, editing and agreed to the published version of the manuscript.
Data Availability Statement
No new data were created.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| Abbreviations | Full Form |
| BC | Bladder Cancer |
| CBT | Cognitive Behavioral Therapy |
| CI | Confidence Interval |
| COVID-19 | Coronavirus Disease 2019 |
| CRIS | Cancer Resource and Information System |
| ERAS | Enhanced Recovery After Surgery |
| ESMO | European Society of Medical Oncology |
| GSES | General Self Efficacy Scale Scores |
| HRQoL | Health-Related Quality of Life |
| LOS | Length Of Stay |
| MIBC | Muscle-Invasive Bladder Cancer |
| N | Number |
| NMIBC | Non- Muscle Invasive Bladder Cancer |
| P | Probability (P-Value) |
| PRO | Patient Reported Outcomes |
| QoL | Quality of Life |
| RCT | Randomized controlled trial |
| RR | Risk Ratio |
| SAS | Self-Rating Anxiety Scale |
| SDS | Self-Rating Depression Scale |
| UI | Urinary Incontinence |
References
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians. 2021;71(3):209-49. [CrossRef]
- Zhang Y, Rumgay H, Li M, Yu H, Pan H, Ni J. The global landscape of bladder cancer incidence and mortality in 2020 and projections to 2040. Journal of global health. 2023;13:04109. [CrossRef]
- Antoni S, Ferlay J, Soerjomataram I, Znaor A, Jemal A, Bray F. Bladder cancer incidence and mortality: a global overview and recent trends. European urology. 2017;71(1):96-108. [CrossRef]
- Saginala K, Barsouk A, Aluru JS, Rawla P, Padala SA, Barsouk A. Epidemiology of bladder cancer. Medical sciences. 2020;8(1):15. [CrossRef]
- Khaled H. Schistosomiasis and cancer in Egypt: Review. J Adv Res. 2013 Sep;4(5):461-6. PMID: 25685453; PMCID: PMC4293882. [CrossRef]
- Zuo J, Chen J, Tan Z, Zhu X, Wang H, Fu S, Wang J. Analysis of long-term trends and 15-year predictions of smoking-related bladder cancer burden in China across different age and sex groups from 1990 to 2021. Discover Oncol. 2025 Mar 27;16:408. [CrossRef]
- Kiebach J, Beeren I, Aben KKH, Witjes JA, van der Heijden AG, Kiemeney LALM, Vrieling A. Smoking behavior and the risks of tumor recurrence and progression in patients with non-muscle-invasive bladder cancer. Int J Cancer. 2025;156(2):E123-E132. PMID: 39521345. [CrossRef]
- Chorbińska J, Krajewski W, Nowak Ł, Bardowska K, Żebrowska-Różańska P, Łaczmański Ł, Pacyga-Prus K, Górska S, Małkiewicz B, Szydełko T. Is the urinary and gut microbiome associated with bladder cancer? Clin Med Insights Oncol. 2023;17:11795549231206796. [CrossRef]
- Hussein AA, Smith G. The association between the urinary microbiome and bladder cancer. Urol Clin North Am. 2023;50(1):81-9. [CrossRef]
- Gherasim RD, Chibelean C, Porav-Hodade D, Todea-Moga C, Tătaru SO, Reman TL, Vida AO, Ghirca MV, Ferro M, Martha OKI. Microbiome shifts in bladder cancer: a narrative review of urobiome composition, progression, and therapeutic impact. Medicina (Kaunas). 2025;61(8):1401. [CrossRef]
- Stamatakos PV, Fragkoulis C, Zoidakis I, Ntoumas K, Kratiras Z, Mitsogiannis I, Dellis A. A review of urinary bladder microbiome in patients with bladder cancer and its implications in bladder pathogenesis. World J Urol. 2024;42:457. [CrossRef]
- Roje B, Zhang B, Mastrorilli E, Kovačić A, Sušak L, Ljubenkov I, Ćosić E, Vilović K, Meštrović A, Lozo Vukovac E, Bučević-Popović V, Puljiz Ž, Karaman I, Terzić J, Zimmermann M. Gut microbiota carcinogen metabolism causes distal tissue tumours. Nature. 2024;632(8019):580-586. [CrossRef]
- Mani S. Gut microbiome and bladder cancer: A new link through nitrosamine metabolism. Cell Host Microbe. 2024;32(8):1001-1003. [CrossRef]
- Ginwala R, Bukavina L, Sindhani M, Nachman E, Peri S, Franklin J, Drevik J, Christianson S, Geynisman DM, Kutikov A, Abbosh PH. Bladder cancer microbiome and its association with chemoresponse. Front Oncol. 2025;15:1506319. [CrossRef]
- Liang Z, Wang X, Xie B, Zhu Y, Wu J, Li S, Meng S, Zheng X, Ji A, Xie L. Pesticide exposure and risk of bladder cancer: a meta-analysis. Oncotarget. 2016 Oct 11;7(41):66959-66970. PMID: 27689300; PMCID: PMC5341990. [CrossRef]
- Lucchesi CA, Vasilatis DM, Mudryj M, Ghosh PM. Pesticides and bladder cancer: mechanisms leading to anti-cancer drug chemoresistance and new chemosensitization strategies. Int J Mol Sci. 2023;24(14):11395. PMID: 37510855; PMCID: PMC10372773. [CrossRef]
- Botteman MF, Pashos CL, Redaelli A, Laskin B, Hauser R. The health economics of bladder cancer: a comprehensive review of the published literature. Pharmacoeconomics. 2003;21(18):1315-30.
- Sylvester RJ, Van Der Meijden AP, Oosterlinck W, Witjes JA, Bouffioux C, Denis L, et al. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: a combined analysis of 2596 patients from seven EORTC trials. Eur Urol. 2006;49(3):466-77. [CrossRef]
- https://seer.cancer.gov/statistics-network/explorer/.
- Mohamed NE, Pisipati S, Lee CT, Goltz HH, Latini DM, Gilbert FS, et al., editors. Unmet informational and supportive care needs of patients following cystectomy for bladder cancer based on age, sex, and treatment choices. Urologic Oncology: Seminars and Original Investigations; 2016: Elsevier. [CrossRef]
- Smith AB, Jaeger B, Pinheiro LC, Edwards LJ, Tan HJ, Nielsen ME, et al. Impact of bladder cancer on health-related quality of life. BJU international. 2018;121(4):549-57. [CrossRef]
- Cerruto MA, D'Elia C, Siracusano S, Gedeshi X, Mariotto A, Iafrate M, et al. Systematic review and meta-analysis of non RCT's on health related quality of life after radical cystectomy using validated questionnaires: Better results with orthotopic neobladder versus ileal conduit. Eur J Surg Oncol (EJSO). 2016;42(3):343-60. [CrossRef]
- Wang W, Chen Y, Gu J. Effectiveness of integrated nursing interventions in enhancing patient outcomes during postoperative intravesical instillation for non-muscle invasive bladder cancer: A comparative study. Medicine. 2024;103(11):e36871. [CrossRef]
- Grant M, Economou D, Ferrell B. Oncology nurse participation in survivorship care. Clin J Oncol Nursing. 2010;14(6):709. [CrossRef]
- Charalambous A, Wells M, Campbell P, Torrens C, Östlund U, Oldenmenger W, et al. A scoping review of trials of interventions led or delivered by cancer nurses. Int J Nursing studies. 2018;86:36-43. [CrossRef]
- Liu H, Yang K, Gong F, Wu Y, Tang S. Application of rapid rehabilitation nursing in perioperative period of laparoscopic radical prostatectomy for prostate cancer patients. J Nanomaterials. 2021;2021(1):9934539. [CrossRef]
- Fearon KCH, Ljungqvist O, Von Meyenfeldt M, Revhaug A, Dejong CHC, Lassen K, Nygren J, Hausel J, Soop M, Andersen J, Kehlet H. Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr. 2005;24(3):466-477. PMID: 15896435. [CrossRef]
- Peng F, Meng Y, Sun L, Dong B, Xu G, Liu S, et al. People-Oriented Nursing Mode on the Negative Emotions and Psychological Status of Patients with Bladder Cancer. Iran J Public Health. 2024;53(5):1087. [CrossRef]
- Fan X, Li H, Lai L, Zhou X, Ye X, Xiao H. Impact of internet plus health education on urinary stoma caregivers in coping with care burden and stress in the era of COVID-19. Front Psychol. 2022;13:982634. [CrossRef]
- Bessa A, Rammant E, Enting D, Bryan RT, Shamim Khan M, Malde S, et al. The need for supportive mental wellbeing interventions in bladder cancer patients: A systematic review of the literature. PLoS One. 2021;16(1):e0243136. [CrossRef]
- MacLennan SJ, MacLennan S. How do we meet the supportive care and information needs of those living with and beyond bladder cancer? Front Oncol. 2020;10:465.
- Shaffer KM, Turner KL, Siwik C, Gonzalez BD, Upasani R, Glazer JV, et al. Digital health and telehealth in cancer care: a scoping review of reviews. Lancet Digital Health. 2023;5(5):e316-e27. [CrossRef]
- Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009 Jul 21;6(7):e1000097. PMID: 19621072; PMCID: PMC2707599. [CrossRef]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. PMID: 33782057; PMCID: PMC8005924. [CrossRef]
- Song Y, Ren P, Wu Y, Zhang B, Wang J, Li Y. Efficacy of long-term extended nursing services combined with atezolizumab in patients with bladder cancer after endoscopic bladder resection. Medicine. 2022;101(38):e30690. [CrossRef]
- Zhang M, Guo S, Gan S, Xu Q. “Internet Plus” continuous nursing for patients with advanced bladder cancer: A retrospective observational study. Medicine. 2024;103(15):e37822. [CrossRef]
- Ashraf W, Hamid A, Malik SA, Khawaja R, Para SA, Wani MS, et al. Integrated enhanced recovery after surgery protocol in radical cystectomy for bladder tumour—A retroprospective study. BJUI compass. 2024;5(11):1183-94. [CrossRef]
- Zhang T, Qi X. Enhanced Nursing Care for Improving the Self-Efficacy & Health-Related Quality of Life in Patients with a Urostomy. J Multidisciplinary Healthcare. 2023:297-308. [CrossRef]
- Leow JJ, Catto JW, Efstathiou JA, Gore JL, Hussein AA, Shariat SF, et al. Quality indicators for bladder cancer services: a collaborative review. Euro Urol. 2020;78(1):43-59. [CrossRef]
- Grassi L, Caruso R, Riba M, Lloyd-Williams M, Kissane D, Rodin G, et al. Anxiety and depression in adult cancer patients: ESMO Clinical Practice Guideline. ESMO open. 2023;8(2):101155. [CrossRef]
- Diefenbach MA, Marziliano A, Siembida EJ, Mistretta T, Pfister H, Yacoub A, et al. Cancer Resource and Information Support (CRIS) for bladder cancer survivors and their caregivers: development and usability testing study. JMIR Formative Research. 2023;7:e41876. [CrossRef]
- Kim Y, Lee H, Park J, Lee S. A mobile-based mental health improvement program for non-muscle invasive bladder cancer patients: Program development and feasibility protocol. Euro Psychiatry. 2023;66(S1):S362-S3. [CrossRef]
- Lemiński A, Kaczmarek K, Bańcarz A, Zakrzewska A, Małkiewicz B, Słojewski M. Educational and psychological support combined with minimally invasive surgical technique reduces perioperative depression and anxiety in patients with bladder cancer undergoing radical cystectomy. Int J Environmental Research and Public Health. 2021;18(24):13071. [CrossRef]
- Thomas KR, Joshua C, Ibilibor C. Psychological Distress in Bladder Cancer Patients: A Systematic Review. Cancer medicine. 2024;13(22):e70345. [CrossRef]
- Wulff-Burchfield EM, Potts M, Glavin K, Mirza M. A qualitative evaluation of a nurse-led pre-operative stoma education program for bladder cancer patients. Supp Care in Cancer. 2021;29(10):5711-9. [CrossRef]
- Zhang T, Qi X. Caregiver Burden in Bladder Cancer Patients with Urinary Diversion Post-Radical Cystectomy and the Need for Comprehensive Nursing Education: A Narrative Literature. J Multidisciplinary Healthcare. 2024:3825-34. [CrossRef]
- Ding J-Y, Pan T-T, Lu X-J, You X-M, Qi J-X. Effects of peer-led education on knowledge, attitudes, practices of stoma care, and quality of life in bladder cancer patients after permanent ostomy. Front Medicine. 2024;11:1431373. [CrossRef]
- Solera-Gomez S, Benedito-Monleon A, LLinares-Insa LI, Sancho-Cantus D, Navarro-Illana E, editors. Educational needs in oncology nursing: a scoping review. Healthcare. 2022: MDPI. [CrossRef]
- Xu M, Chen S, Liu X, Luo Y, Wang D, Lu H, et al. Best evidence for rehabilitation management of urinary incontinence in patients with bladder cancer following orthotopic neobladder reconstruction. Asia-Pacific J Oncol Nursing. 2025;12:100647. [CrossRef]
- Biswas J, Bhuiyan AKMMR, Alam A, Chowdhury MK. Effect of perceived social support on cancer patients: a narrative review. Acad Oncol. 2025 Apr 29;2025:7681. [CrossRef]
- Qian L, Zhang Y, Chen H, Pang Y, Wang C, Wang L, et al. The clinical effect of gratitude extension-construction theory nursing program on bladder cancer patients with fear of cancer recurrence. Front Oncol. 2024;14:1364702. [CrossRef]
- Alqaisi O, Subih M, Joseph K, Yu E, Tai P. Oncology Nurses' Attitudes, Knowledge, and Practices in Providing Sexuality Care to Cancer Patients: A Scoping Review. Curr Oncol. 2025;32(6):337-46. PMID: 40558280; PMCID: PMC12191979. [CrossRef]
- Alqaisi O, Al-Ghabeesh S, Tai P, Wong K, Joseph K, Yu E. A narrative review of nursing roles in addressing sexual dysfunction in oncology patients. Curr Oncol. 2025;32(8):457-75. PMID: 40862826; PMCID: PMC12384569. (impact factor 3.4). [CrossRef]
- Woo BFY, Lee JXY, Tam WWS. The impact of the advanced practice nursing role on quality of care, clinical outcomes, patient satisfaction, and cost in the emergency and critical care settings: a systematic review. Hum Resour Health. 2017;15(1):63. PMID: 28893270; PMCID: PMC5594520. [CrossRef]
Figure 1.
Preferred reporting items for systematic review and meta-analysis (PRISMA) flow diagram of studies to include in systematic review.
Figure 1.
Preferred reporting items for systematic review and meta-analysis (PRISMA) flow diagram of studies to include in systematic review.
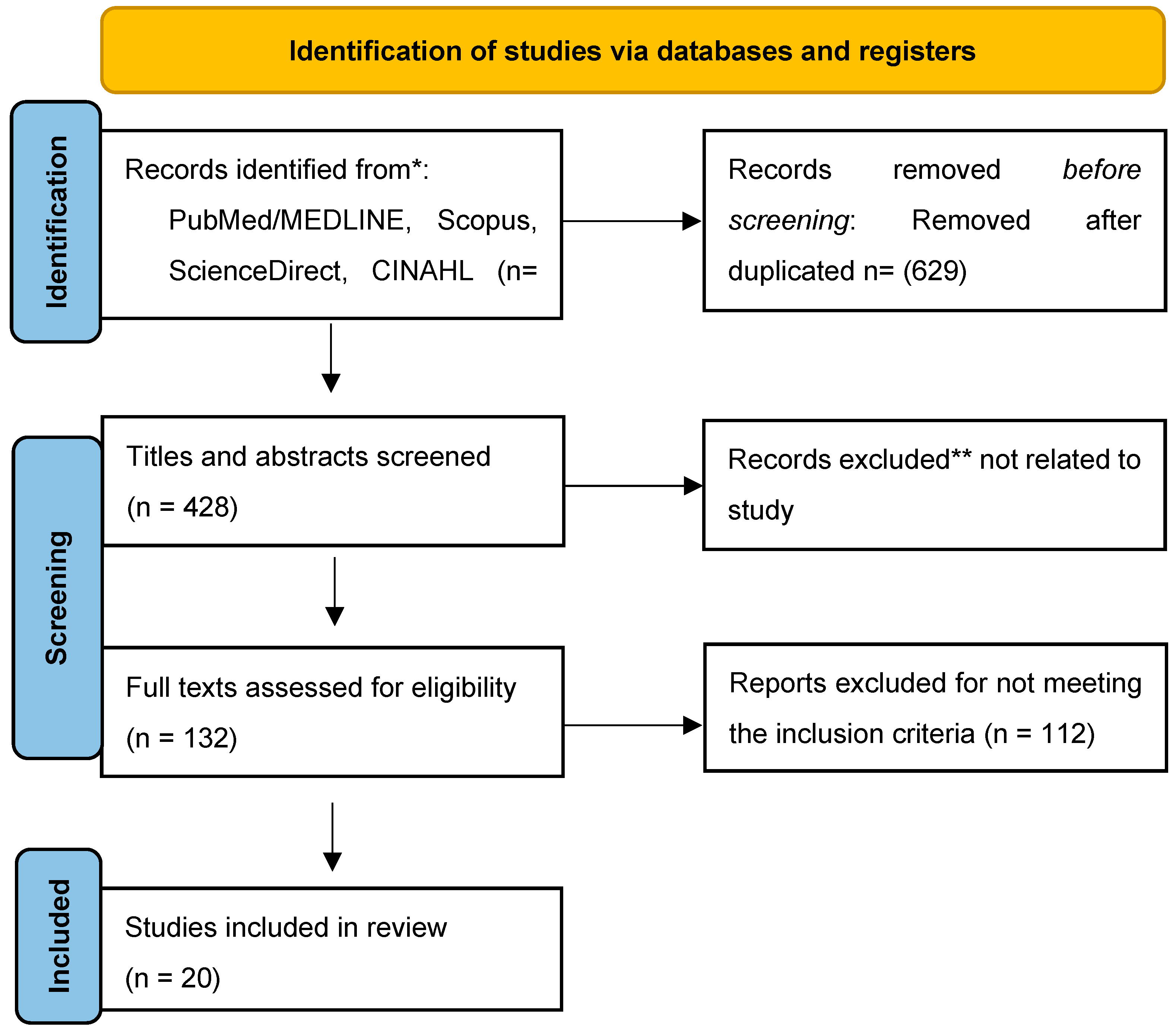
Figure 2.
The framework illustrates the intervention components, delivery mechanisms, and corresponding clinical and patient-reported outcomes for each category: perioperative care and enhanced recovery after surgery (ERAS) protocols, intravesical therapy management, digital health interventions and psychosocial support services.
Figure 2.
The framework illustrates the intervention components, delivery mechanisms, and corresponding clinical and patient-reported outcomes for each category: perioperative care and enhanced recovery after surgery (ERAS) protocols, intravesical therapy management, digital health interventions and psychosocial support services.
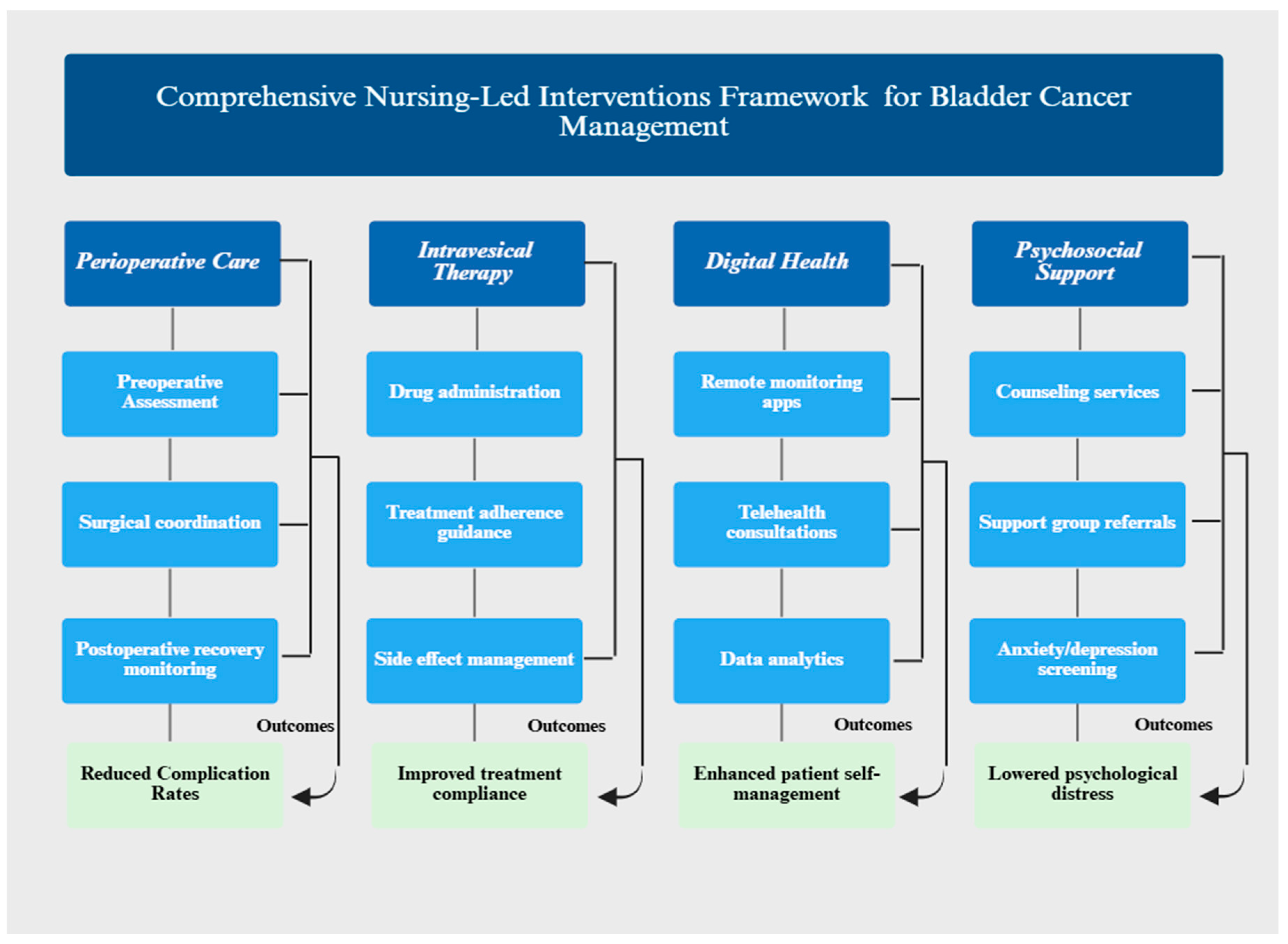
Table 1.
Summary of 20 studies including in this review.
| Author/year | Purpose | Settings | Sample size | Study design | Main findings |
|---|---|---|---|---|---|
| Wang (2024) [23] | Evaluate effectiveness of integrated nursing intervention on patient outcomes during postoperative intravesical installations for NMIBC | Hospital oncology ward | n= 100 NMIBC patients | Comparative RCT | Integrated nursing interventions significantly improved patients’ satisfaction (P˂0.001), treatment compliance, self- efficacy, and QoL; reduced anxiety and depression. |
| Song (2022) [35] | Assess efficacy of long- term extended nursing services combined with atezolizumab in BC patients after endoscopic bladder resection | Hospital urology department | N=126 BC patients | Randomized controlled trial | Extended nursing services improved renal function, QoL, and satisfaction; reduced caregiver burden, anxiety and depression (P˂0.05) |
| Zhang (2024) [36] | Evaluate continuous nursing interventions via internet plus platform for advanced BC patients with hematuria | Tertiary hospital | N=43 advanced BC patients | Retrospective observational study |
Internet plus nursing improved coping style, disease knowledge, reduced caregiver burden, increased patients’ satisfaction. |
| Ashraf (2024) [37] | Compare integrated ERAS protocol with traditional preoperative care in radial cystectomy | Tertiary referral urology center | N=94 BC patients | Retrospective comparative | ERAS significantly reduced hospital stay (11 vs. 17 days, p˂), faster recovery, reduced complications by 38% |
| Bessa (2021) [30] | Systematic review supportive mental wellbeing intervention for BC patients | Literature review (multiple centers) | Systematic review |
Systematic review and synthesis | No BC-specific mental health interventions found; identified critical gap in psychosocial support* |
| Zhang & Qi (2023) [38] | Synthesize evidence on enhanced nursing care for self-efficacy and HRQoL in urostomy patients | Literature review (multiple centers) | Systematic review of 10 studies |
Systematic review | Preoperative education critical for psychological preparation; postoperative interventions improved self-efficacy and HRQoL. |
| Charalambous (2018) [25] | Scope trials of cancer nurse-led intervention across cancer care continuum | Multiple cancer centers globally | Scoping review of 214 studies | Scoping review | Most interventions during treatment phase; focused in education and counseling; improve multiple outcomes. |
| Leow (2019) [39] | Develop and validate quality indicators for bladder cancer services | Multidisciplinary BC care centers | Mutli- stakeholder collaboration | Guideline development | Established quality indicators for NMIBC/MIBC ; emphasizes preoperative counseling, stoma marking ERAS protocols |
| Grassi (2023) [40] | Provide ESMO guideline on managing anxiety and depression in adult cancer patients | Guideline development consensus |
Expert consensus | Clinical practice guideline (ESMO) | Recommend cognitive behavioral therapy and mindfulness; anxiety/depression common but underrecognized |
| Diefenbach (2023) [41] | Evaluate gratitude nursing program on fear of cancer recurrence in BC patients | Hospital oncology unit | N= 80 BC patients | Comparative study | Improved QoL, reduced fear, depression, anxiety; improved treatment compliance vs. routine care |
| Peng (2024) [28] | Assess people-oriented nursing mode on psychological status of BC patients | Hospital oncology department | N=80 BC patients | Comparative study | Reduced anxiety and depression, improved QoL vs. conventional nursing |
| Lee (2023) [42] | Develop and test mobile based mental health program for NMIBC patients | Ambulatory urology clinic |
Pilot feasibility study | Protocol and feasibility | Mobile program via Kakao talk demonstrated feasibility; potential for mental health improvement |
| Leminski (2021) [43] | Evaluate combined educational and psychological support reducing perioperative anxiety in MIBC patients | Tertiary cancer center | n= 148 MIBC patients | Comparative study | Cystocare program significantly reduced perioperative depression (P˂0.001) and anxiety |
| Thomas (2024) [44] | Systematic review psychological distress and identify risk factors in BC patients | Literature review (multiple studies) | Systematic review of 17 studies (n=2.572) | Systematic review | Risk factors: advanced stage younger age, female sex, preoperative; protective: social support |
| Wulff-Burchfield, (2024) [45] | Qualitatively evaluate nurse-led preoperative stoma education for BC patients | Preoperative education clinic | N=24, patients and caregiver | Qualitative evaluation | Interactive education with patients advocates optimally preppers for ostomy and reduce distress |
| Zhang (2024) [46] | Narrative review caregiver burden nursing education for BC patients with urinary diversion | Literature review (2018-2023) | Narrative review | Narrative literature review | Nurse-led stoma education enhanced caregiver comprehension and reduced burden/stress |
| Ding (2024) [47] | Evaluate peer-led education on stoma care and QoL in BC patients with permanent ostomy | Hospital stoma care clinic | N= 340 BC patients with ostomy | Randomized controlled trial | Peer-led intervention improved stoma care knowledge (P˂0.001) attitude, practices, and QoL |
| Solera-Gomez (2022) [48] | Scope educational needs for oncology nurses | Literature review (oncology settings) | Scoping review of multiple studies | Scoping review | Key needs: communication, coping, stress, prevention, continuous, technical skill development |
| Xu (2024) [49] | Synthesize best evidence for urinary incontinence management post-neobladder | Literature review | Evidence synthesis of multiple studies | Evidence synthesis | Comprehensive UI assessment, conservative, treatment, nursing equipment use, structured follow-up |
| Fan (2022) [29] | Evaluate internet plus health education on caregiver burden in COVID-19 era | Virtual and home-based platform | N= 80 caregiver of stoma patients | Randomized controlled trial | Internet plus education reduced caregiver burden and enhanced coping ability (P˂0.05) |
BC: bladder cancer; COVID-19: Coronavirus Disease 2019; ERAS: Enhanced recovery after surgery; ESMO: European Society of Medical Oncology; MIBC: muscle-invasive bladder cancer; N: number; P: probability; QoL: quality of life; RCT: randomized controlled trial; UI: urinary incontinence; vs: versus.
Table 2.
Perioperative care enhanced recovery after (ERAS) protocols.
| Authors /years | Study designs | Sample size (n) | Primary outcomes | Effect size/statistical significance |
|---|---|---|---|---|
| Ashraf (2024) (23)[32] | Retrospective comparative | 94 | Hospital stays reduction (11 vs. 17 days); complication reduction | 35% LOS reductions;38% complication reduction (p˂0.05) |
| Leminski, A. (2021) (29)[43] | Comparative study | 148 | Perioperative anxiety /depression reduction | Significant reduction in anxiety /depression scores (P˂0.001) |
| Leow (2019) (25)[39] | Clinical guideline development | Experts’ consensus | Quality indicators establishment | Preoperative counseling, stoma marking, ERAS protocols standardized |
LOS: length of stay; P: probability; vs: versus.
Table 3.
Intravesical therapy management and NMIBC outcomes with statistical evidence.
| Author /years | Study design | Sample size (n) | Main findings | Effect size/statistical significance |
|---|---|---|---|---|
| Wang (2024) [23] | Randomized controlled trial | 100 | Patients’ satisfaction compliance, self-efficacy, QoL improvement | Satisfaction Cohen’s d= - 6.39 (P˂0.001); compliance 100% vs 84%; anxiety reduction (Cohen’s d= 5.51, P˂0.001) |
| Song (2022) [35] |
Randomized controlled trial | 126 | Renal function preservation, reduced caregiver burden | Improved renal function, reduced burden /anxiety /depression (P˂0.05) |
Table 4.
Digital health and telehealth interventions with implementation data.
| Authors /years | Intervention type | Population (N) | Outcomes | Implementation feasibility |
|---|---|---|---|---|
| Zhang (2024) [36] | Internet plus continuous nursing platform | Advanced BC with hematuria (43) | Improved coping, disease knowledge, reduced caregiver burden | Successfully implemented in hospital settings: scalable |
| Kim (2023) [42] | Mobile-based mental health (Kakao talk) | NMIBC patients’ pilot (n= feasibility) | Feasibility demonstrated; potential for mental health improvement | Pilot phase; ready for expansion |
| Diefenbach (2023) [41] | Web-based CRIS platform | BC survivor (7) | High usability; addresses practical /psychosocial /educational needs | User-friendly interface; practical information accessible |
| Fan (2022) [29] | Internet plus health education for caregivers | Caregivers of stoma patients (80) | Reduced caregiver burden; enhanced coping ability (P˂0.05) | Effective during COVID-19 pandemic; widely applicable |
BC: bladder cancer; COVID-19: Coronavirus Disease 2019; NMIBC: non-muscle-invasive bladder cancer; N: number; P: probability.
Table 5.
Stoma and ostomy care management with evidence of effectiveness.
| Authors/years | Study design | Sample size (n) | Key findings | Effect size/impact |
|---|---|---|---|---|
| Zhang (2023) [38] | Systematic review of 10 studies | 10 studies reviewed | Preoperative education critical; postoperative care improved self-efficacy and HRQoL | Consistent improvement across studies; moderate to strong effect sizes |
| Wulff-Burchfield (2024) [45] | Qualitative evaluation | 24 (patients & caregivers) | Interactive education optimally prepared patients; reduced distress | Qualitative evidence of psychological benefit and preparedness |
| Wang (2024) [23] | Randomized controlled trial | 340 | Peer-led education improved knowledge, attitudes, practices, QoL | Stoma knowledge Cohen’s d=1.60 (P˂0.001); sustained improvement |
| Zhang and Qi (2025) [46] | Narrative review | Literature 2018- 2023 | Enhanced caregiver comprehension; reduced burden/stress | Systematic evidence synthesis; reproducible outcomes. |
QoL: quality of life; HRQoL: health-related quality of life.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



