
Submitted:
09 December 2025
Posted:
09 December 2025
You are already at the latest version
Abstract
Background and Clinical Significant: Sacrococcygeal joint dislocation is an extremely rare traumatic condition in the pediatric population and is typically caused by direct trauma to the gluteal region. Most reported cases have been managed conservatively with analgesics or manual reduction, and the application of a caudal epidural block in children with this entity has, to our knowledge, never been previously described. Case Presentation: A 14-year-old girl presented with aggravated coccydynia following a second fall. Six months earlier, she had been diagnosed with sacrococcygeal dislocation after her initial fall, and her symptoms had been well controlled at a Numerical Rating Scale (NRS) score of 3 with acetaminophen and nonsteroidal anti-inflammatory drugs. However, after the recent reinjury, her pain worsened to an NRS score of 6 and did not improve despite continued conservative pharmacologic treatment. Radiographic examination at our institution confirmed anterior angular displacement of the coccyx. Accordingly, an ultrasound-guided caudal epidural block was performed using mepivacaine and dexamethasone. At follow-up evaluations conducted 2 weeks and 2 months after the procedure, her pain had decreased to an NRS score of 2, accompanied by functional improvement. Conclusions: This case suggests that caudal epidural block may serve as a safe and potentially effective therapeutic option for pediatric patients experiencing coccygeal pain following traumatic sacrococcygeal joint dislocation.
Keywords:
pediatric trauma
; sacrococcygeal dislocation
; coccydynia
; caudal epidural block
; regional anesthesia
1. Introduction
Sacrococcygeal dislocation, in which the coccyx becomes separated from the sacrum and is displaced either anteriorly or posteriorly, is rarely reported in pediatric patients [1]. Sacrococcygeal dislocation is primarily caused by trauma, and anterior dislocation is more common than posterior dislocation [2]. The resulting coccydynia refers to pain arising from the coccygeal region, and because no standardized treatment has been established, the condition may progress to chronic pain. In addition, in female patients, it may pose potential complications during labor [3]. Treatment options include physical therapy, nonsteroidal anti-inflammatory drugs (NSAIDs), steroid injections into the joint, manual reduction, surgical fixation of the sacrum and coccyx, and coccygectomy [4,5,6]. Caudal epidural block is widely used for managing lower sacral and coccygeal pain, providing both anti-inflammatory effects and modulation of sympathetic activity. Although caudal block is considered a safe procedure in pediatric patients, its use for alleviating pain associated with sacrococcygeal dislocation is rarely reported. We describe the case of a 14-year-old girl with persistent coccydynia following sacrococcygeal dislocation whose symptoms improved after a caudal epidural block. This case highlights the potential utility of caudal epidural block as a safe and effective interventional option for refractory coccygeal pain in pediatric patients.
2. Case Presentation
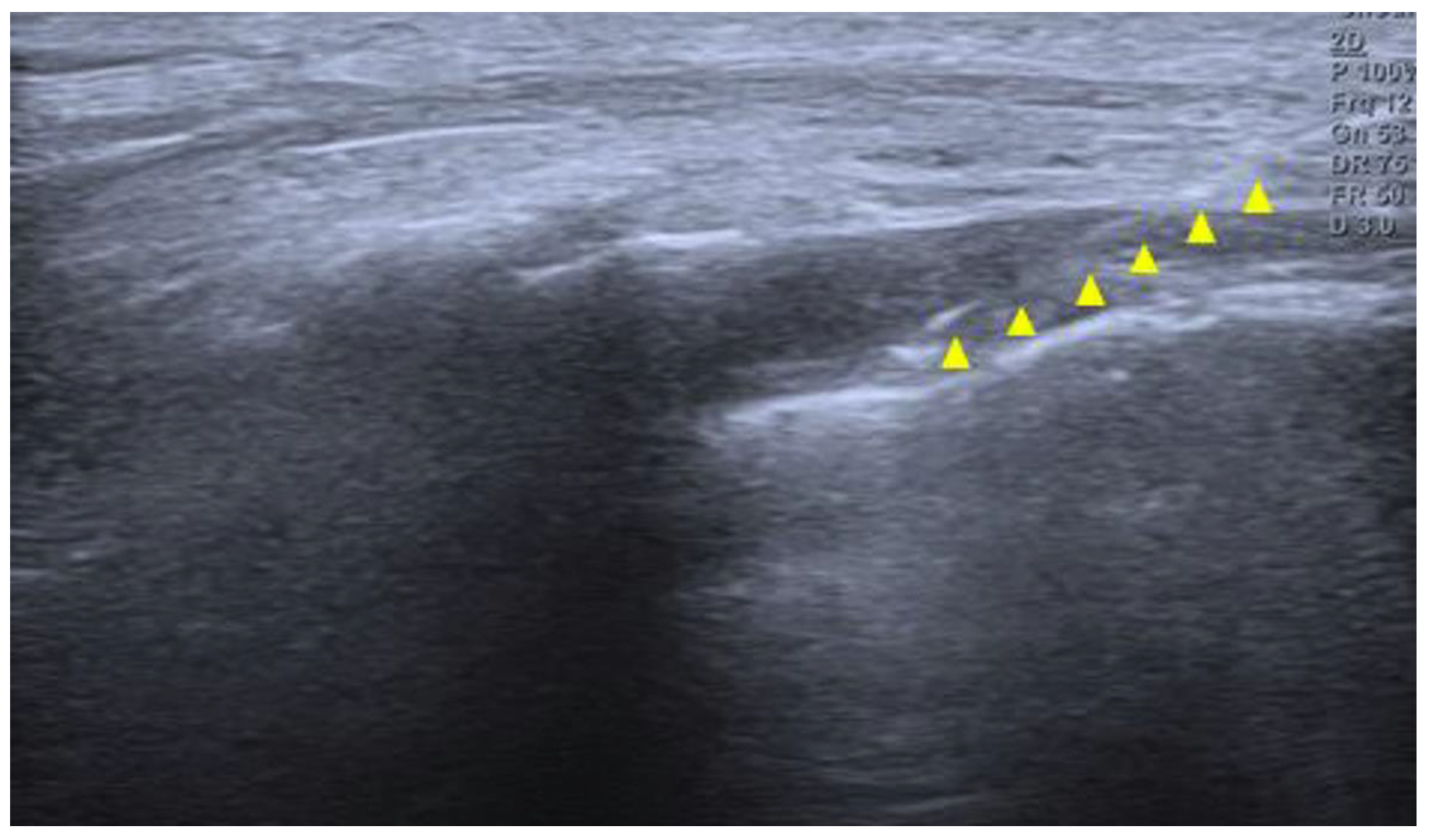
A 14-year-old girl developed coccygeal pain following a fall inside a bus six months earlier. At that time, she was diagnosed with sacrococcygeal dislocation at an outside hospital and was prescribed acetaminophen and NSAIDs, which maintained her symptoms at a Numerical Rating Scale (NRS) score of approximately 3. However, one month prior to presentation, she sustained a second fall to the same area, after which her pain worsened despite continued pharmacologic treatment, reaching an NRS score of 6. She was therefore referred to our pain clinic. The radiographs obtained at the time of the initial injury were unavailable. Radiography performed at our institution demonstrated anterior angulation of the coccyx (Figure 1). Physical examination revealed tenderness over the sacrum and coccyx. The patient was able to sit but could not remain seated for prolonged periods due to pain, and reported worsening pain upon standing. No cutaneous abnormalities or swelling were noted over the coccygeal region. She denied defecation-related pain. For pain control, an ultrasound-guided caudal epidural block was performed (Figure 2). Under sterile conditions, the patient was positioned prone, and the sacral hiatus was identified using ultrasound. After local anesthesia of the skin at the needle insertion site, a butterfly catheter was advanced toward the sacral hiatus under an out-of-plane view, traversing the sacrococcygeal ligament. The needle was then redirected in-plane into the epidural space. A mixture of 8 mL of 2% mepivacaine, 1 mL of 0.9% normal saline, and 5 mg of dexamethasone was injected. At the 2-week follow-up, although the qualitative character of pain remained similar, the patient reported an increased ability to remain seated and a reduced frequency of pain when standing. Her pain intensity decreased significantly to an NRS score of 2, accompanied by noticeable functional improvement. At the 2-month follow-up, her pain remained at an NRS score of 2, and she maintained a level of daily functioning without significant limitations.
3. Discussion
Sacrococcygeal dislocation is rare in pediatric patients [7]. Only a small number of cases have been reported in the literature to date [1,2,7]. Most cases are known to result from falls or direct trauma to the buttock region [2]. The sacrum and coccyx are connected at the sacrococcygeal joint, an amphiarthrodial articulation that allows limited flexion and extension. This joint is stabilized by the anterior and posterior sacrococcygeal ligaments, the lateral sacrococcygeal ligaments, and the anococcygeal raphe. Surrounding pelvic floor musculature, including the levator ani and the gluteus maximus, also contributes to regional support. Sacrococcygeal dislocation refers to malalignment or marked anterior angulation of the articulation between the sacrum and coccyx, which can be identified on radiographic evaluation. In particular, dynamic lateral radiographs define pathologic instability when the coccygeal flexion angle exceeds 25°, or when the coccyx demonstrates more than 25% anterior translation relative to its normal position [8]. Such dislocation can cause pain when it results in injury to the sacrococcygeal joint and its supporting ligaments.
The pain that develops after sacrococcygeal dislocation is primarily somatic in origin and arises from injury to the periosteum, joint capsule, and surrounding ligamentous structures. This region is innervated by the coccygeal plexus, a small plexus formed by the ventral rami of the sacral nerves S4 and S5 and the coccygeal nerve Co1 [9]. The anococcygeal nerve, which branches from this plexus, provides sensory innervation to the sacrococcygeal junction and the skin over the coccygeal tip. Additional innervation arises from terminal branches of the sacral nerves and sympathetic fibers originating from the inferior hypogastric sympathetic chain. Consequently, nociceptive stimuli from the dislocated sacrococcygeal region are transmitted primarily through the S4–Co1 nerve roots, and patients typically experience exacerbation of pain when sitting on a hard surface or rising from a seated position. In particular, the abrupt pain that occurs when rising from a seated position is recognized as a characteristic symptom of coccygeal instability. Maigne et al. [10] reported that this positional pain is a specific finding observed only in patients with coccygeal dislocation or hypermobility [11]. Anterior displacement or shearing forces applied to the coccyx during trauma can directly stimulate nociceptors, producing pain and referred symptoms through both somatic and sympathetic pathways. Consequently, the exacerbation of pain when sitting or rising from a seated position after sacrococcygeal dislocation can be understood as the result of this complex interplay of nociceptive transmission mechanisms.
Caudal epidural block is an effective procedure for managing coccygeal pain as well as lower lumbar and sacral discomfort, and it is one of the most commonly performed nerve blocks in pediatric patients. The technique involves injecting local anesthetics into the sacral epidural space, thereby blocking sensory and sympathetic fibers, including the sacral and coccygeal nerve roots. It provides effective relief of somatic pain originating from the periosteum and joint capsule, and depending on the volume administered, the injectate may spread to the level of the ganglion impar, offering potential suppression of visceral pain [12]. When corticosteroids are added, the block can further attenuate local inflammatory responses by reducing the release of inflammatory mediators such as prostaglandins, substance P, and pro-inflammatory cytokines (e.g., IL-6), thereby mitigating peripheral sensitization. Thus, caudal epidural block relieves coccygeal pain both by interrupting somatic nociceptive transmission and by diminishing sympathetic-mediated pain pathways. Ganglion impar block is typically used in patients with chronic coccydynia [13], targeting the sympathetic ganglion located anterior to the coccyx with local anesthetic to achieve pain relief. In contrast, caudal epidural block provides a broader approach. Although it may be particularly effective for pain with an inflammatory component, its blockade of sacral nerve roots and potential spread to the sympathetic ganglion can yield pain-relieving effects comparable to those of a ganglion impar block [14].
Previous reports of pediatric sacrococcygeal dislocation have described symptom improvement with conservative management, such as pharmacologic treatment or manual reduction [1,7]. In the present case, the patient initially responded to medication; however, after sustaining an additional traumatic event, her pain worsened and meaningful improvement could no longer be expected with pharmacologic therapy alone. Because the sacrococcygeal joint remains anatomically immature in growing children, sacrococcygeal dislocation may resemble an injury involving the growth plate, as suggested in previous studies. In such situations, reduction maneuvers or more invasive interventions should be approached with caution, as they may increase the risk of further injury or secondary complications. Hamoud et al. [1] reported that coccygeal fracture–dislocation in younger patients often improves effectively with conservative treatment alone, while manual reduction shows a high failure rate and is therefore not recommended. Considering these factors, we selected caudal epidural block as a relatively safe intervention with the potential to provide therapeutic benefit. The patient experienced both pain relief and functional improvement following the procedure. Thus, this case is meaningful in demonstrating that persistent pain following traumatic sacrococcygeal dislocation in a pediatric patient may improve with caudal epidural block. This report has several limitations. It describes a single case with a relatively short follow-up period. Furthermore, the causal relationship between radiographic findings and clinical symptoms cannot be clearly established, and the association between sacrococcygeal dislocation, pain generation, and subsequent improvement following the block remains difficult to definitively determine.
4. Conclusions
In pediatric patients with coccygeal pain following traumatic sacrococcygeal dislocation, caudal epidural block may serve as a non-invasive and effective therapeutic option. Accumulation of additional similar cases will be necessary to further evaluate the efficacy and long-term outcomes of this treatment approach.
Author Contributions
Conceptualization, J.C. ; methodology, J.C., D.H.K.; software, J.C.; validation, J.C., ; formal analysis, J.C.; investigation, J.C., J.H.C., Y.H.S, H.R.C., H.Y.G., J.Y.J., J.S.P. and J.Y.J., S.K.; resources, J.C.; data curation, J.C.; writing—original draft preparation, J.C.; writing—review and editing, J.C.; visualization, J.C., H.S.S.; supervision, J.C.; project administration, J.C.; funding acquisition, J.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Soonchunhyang University College of Medicine (IRB number : SCHCA 2025-11-029, approved on 5 December 2025).
Informed Consent Statement
Patient consent was waived by the Institutional Review Board because the report contains no identifiable personal information and all clinical data were fully anonymized.
Data Availability Statement
Data is contained within the article.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| NRS | Numerical Rating Scale |
| NSAIDs | Nonsteroidal anti-inflammatory drugs |
References
- Hamoud, K.; Abbas, J. Fracture dislocation of the sacro-coccygeal joint in a 12-year-old boy. A case report and literature review. Orthop. Traumatol. Surg. Res. 2015, 101, 871–873. [Google Scholar] [CrossRef] [PubMed]
- Panigrahi, V.P.; Adsul, N.; Chahal, R.S.; Kalra, K.L.; Acharya, S. Traumatic posterior dislocation of sacrococcygeal joint: A case report and review of the literature. Surg. Neurol. Int. 2020, 11, 197. [Google Scholar] [CrossRef] [PubMed]
- Raissaki, M.T.; Williamson, J.B. Fracture dislocation of the sacro-coccygeal joint: MRI evaluation. Pediatr. Radiol. 1999, 29, 642–643. [Google Scholar] [CrossRef] [PubMed]
- Maigne, J.Y.; Chatellier, G.; Faou, M.L.; Archambeau, M. The treatment of chronic coccydynia with intrarectal manipulation: A randomized controlled study. Spine (Phila Pa. 1976) 2006, 31, E621–627. [Google Scholar] [CrossRef] [PubMed]
- Bergkamp, A.B.; Verhaar, J.A. Dislocation of the coccyx: A case report. J. Bone Joint Surg. Br. 1995, 77, 831–832. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.Y.; Han, C.W.; Kim, Y.H. Joystick reduction and percutaneous pinning for an acutely anteriorly dislocated coccyx: A case report. J. Orthop. Trauma 2004, 18, 388–389. [Google Scholar] [CrossRef] [PubMed]
- Kanabur, P.; Gowd, A.; Bulkeley, J.A.; Behrend, C.J.; Carmouche, J.J. Symptomatic sacrococcygeal joint dislocation treated using closed manual reduction: A case report with 36-month follow-up and review of literature. Trauma Case Rep. 2017, 12, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Maigne, J.Y.; Tamalet, B. Standardized radiologic protocol for the study of common coccygodynia and characteristics of the lesions observed in the sitting position. Clinical elements differentiating luxation, hypermobility, and normal mobility. Spine (Phila Pa. 1976) 1996, 21, 2588–2593. [Google Scholar] [CrossRef] [PubMed]
- Woon, J.T.; Stringer, M.D. Clinical anatomy of the coccyx: A systematic review. Clin. Anat. 2012, 25, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Maigne, J.Y.; Doursounian, L.; Chatellier, G. Causes and mechanisms of common coccydynia: Role of body mass index and coccygeal trauma. Spine (Phila Pa. 1976) 2000, 25, 3072–3079. [Google Scholar] [CrossRef] [PubMed]
- Maigne, J.Y.; Guedj, S.; Fautrel, B. Coccygodynia: Value of dynamic lateral x-ray films in sitting position. Rev. Rhum. Mal. Osteoartic. 1992, 59, 728–731. [Google Scholar] [PubMed]
- Lundblad, M.; Eksborg, S.; Lonnqvist, P.A. Secondary spread of caudal block as assessed by ultrasonography. Br. J. Anaesth. 2012, 108, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Gonnade, N.; Mehta, N.; Khera, P.S.; Kumar, D.; Rajagopal, R.; Sharma, P.K. Ganglion impar block in patients with chronic coccydynia. Indian J. Radiol. Imaging 2017, 27, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Sencan, S.; Yolcu, G.; Bilim, S.; Kenis-Coskun, O.; Gunduz, O.H. Comparison of treatment outcomes in chronic coccygodynia patients treated with ganglion impar blockade versus caudal epidural steroid injection: A prospective randomized comparison study. Korean J. Pain 2022, 35, 106–113. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(A) Anteroposterior pelvic radiograph showing no visible fracture but overall coccygeal axis deviation. (B) Dynamic lateral view showing anterior angulation of the coccyx at the sacrococcygeal junction. (C) Seated lateral view demonstrating accentuated anterior displacement, suggestive of coccygeal instability.
Figure 1.
(A) Anteroposterior pelvic radiograph showing no visible fracture but overall coccygeal axis deviation. (B) Dynamic lateral view showing anterior angulation of the coccyx at the sacrococcygeal junction. (C) Seated lateral view demonstrating accentuated anterior displacement, suggestive of coccygeal instability.
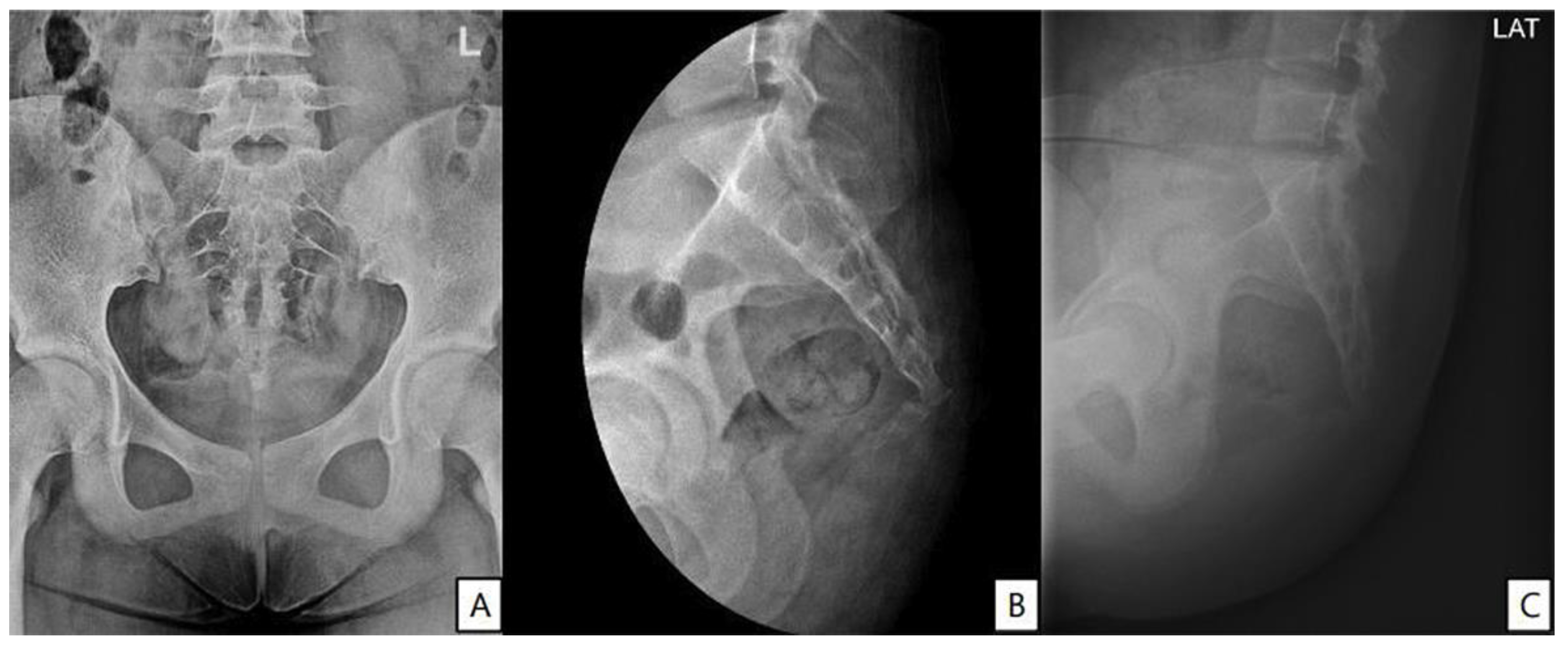
Figure 2.
Ultrasound image of the sacral hiatus during caudal epidural block. The needle is seen advancing through the sacrococcygeal ligament into the caudal epidural space under real-time guidance (yellow triangle).
Figure 2.
Ultrasound image of the sacral hiatus during caudal epidural block. The needle is seen advancing through the sacrococcygeal ligament into the caudal epidural space under real-time guidance (yellow triangle).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



