Submitted:
04 December 2025
Posted:
05 December 2025
You are already at the latest version
Abstract
Off-label use of glutamatergic agents is increasingly common in psychiatry, yet standardized protocols for outpatient dosing are lacking. This report describes the pharmacological management and dosing adjustments required for three patients receiving dextromethorphan (DXM) and piracetam for obsessive–compulsive disorder.Three adult women with severe OCD were treated in a routine clinical setting. Treatment history varied from naïve to treatment-resistant. All patients commenced treatment with a nighttime regimen of oral DXM and piracetam to minimize potential side effects while maintaining existing psychotropic regimens.One patient achieved full remission on a once-nightly regimen. The last two patients showed a "wearing-off" effect, that their symptoms got better quickly after they woke up but then came back in the late afternoon, which neccesitated the schedule to be changed from once a day to twice a day (b.i.d.). This change fixed the afternoon symptom breakthrough without needing to raise the dose.Experience with these cases suggests that while bedtime administration is a safe starting point for routine care, the half-life of the agents may necessitate split dosing for some individuals. The observation that simple schedule adjustments can resolve diurnal symptom fluctuation provides a practical insight for psychiatrists managing OCD with glutamatergic augmentation.
Keywords:
obsessive-compulsive disorder
; OCD
; glutamatergic augmentation
; oral ketamine-class regimen
; dextromethorphan
; DXM
; piracetam
; CYP2D6 inhibition
; twice-daily dosing
; diurnal rebound
; treatment-resistant OCD
; rapid remission
; low-dose regimen
; fluoxetine
; bupropion
; off-label polypharmacy
; NMDA antagonism
; AMPA potentiation
; treatment-naï ve OCD
; private practice
; case series
; rapid-acting antidepressant
; neuroplasticity
; cortico-striato-thalamo-cortical circuit
; Cheung regimen
1. Background
Selective serotonin re-uptake inhibitors (SSRIs) given at the upper end of the dose range, together with exposure-based cognitive-behavioural therapy, are still considered the cornerstone of treatment for obsessive-compulsive disorder [1,2]. Even so, large naturalistic series continue to show that roughly one-third of patients remain symptomatic after several adequate trials [3], and the addition of a dopamine-blocking agent closes the gap for only a minority of these difficult cases [4].
Attention has therefore shifted to the glutamate-rich cortico-striato-thalamo-cortical loops that drive intrusive thoughts and ritualised behaviour [5,6]. In the laboratory, rapid anti-obsessional effects have been reproduced with intravenous ketamine [7] and, more modestly, with oral memantine [8]. Translating those findings to the clinic, however, has proven awkward: ketamine infusions are costly and logistically cumbersome [9], while long-term memantine can be slow to work and is not universally well tolerated [10].
Since 2025 a simpler, fully oral alternative, also known as Cheung Glutamatergic Regimen, has been adopted in several Hong Kong outpatient practices [11]. The protocol uses a low dose of a CYP2D6-inhibiting antidepressant to extend the half-life of dextromethorphan (DXM) given in sub-anaesthetic amounts (30–120 mg/day), with piracetam 600–2400 mg/day as an AMPA-receptor enhancer.
The present report reviews three consecutive patients with obsessive-compulsive disorder treated with this combination in November 2025. The series was chosen not to prove efficacy—something a larger study must tackle—but to explore two immediate, practice-oriented questions: How low can the nightly dose be pushed and still achieve remission, and is giving the entire stack at bedtime enough to keep symptoms in check throughout the day?
2. Methods
This is a retrospective description of consecutive cases seen in the author’s private outpatient practice between May and November 2025.
Obsessive–compulsive disorder was diagnosed by the treating psychiatrist on the basis of a full clinical interview and application of DSM-5 criteria. Comorbid conditions were recorded but are not presented here.
At every visit patients completed the Patient Health Questionnaire-9 (PHQ-9) and the Generalised Anxiety Disorder-7 (GAD-7). Scores were reviewed alongside a semistructured narrative interview that explored diurnal symptom patterns, functional impairment, adverse effects, and medication adherence.
All participants gave written permission for their anonymised clinical information to be reported. For individuals younger than 18 years, parental or guardian consent was obtained in addition to the patient’s written assent.
3. Results
3.1. Case 1: The Dosing and Schedule Sufficient for Rapid Remission
Miss W, a 24-year-old registered nurse, was seen for her first psychiatric assessment on 10 November 2025 after abruptly resigning from her initial hospital post. Until that point she had never consulted mental-health services. The crisis began soon after she started working without close supervision; every routine comment from a senior triggered punishing self-criticism and a spiral of “rabbit-hole” rumination over whether she was fit for the profession. At home she stopped eating, lay awake dreading the next dawn, and made an emergency-department visit for what proved to be severe anxiety. On formal screening she scored 19 on the Patient Health Questionnaire-9 (PHQ-9) and 16 on the Generalised Anxiety Disorder-7 (GAD-7). The interview also uncovered childhood-onset inattentiveness suggestive of undiagnosed ADHD, but the dominant picture was an obsessional form of obsessive–compulsive disorder marked by relentless catastrophic thinking.
Because of the acuteness of her distress, we started an oral glutamatergic protocol at the very first visit. Each night she took fluoxetine 10 mg to inhibit CYP2D6, dextromethorphan (DXM) 30 mg in two 15-mg tablets, piracetam 600 mg, and risperidone 0.5 mg as a low-dose augmenting agent. All medication was scheduled after supper to reduce daytime activation.
Seventeen days later, on 27 November, she returned looking noticeably brighter and reported that the mental free-fall had simply stopped. She was free of restlessness and catastrophic ideation, eating normally, and had already picked up casual nursing shifts while planning a full return to public-sector work. Follow-up scores confirmed the change (PHQ-9 = 3, GAD-7 = 0). DXM was increased to 45 mg nightly to consolidate the response; the rest of the regimen was left unchanged. She denied side-effects throughout.
At the time of writing Miss W remains in full symptomatic and functional remission, working part-time without anxiety or rumination and preparing to rejoin her original hospital. The combination of fluoxetine, nightly DXM 45 mg, piracetam 600 mg, and risperidone 0.5 mg is well-tolerated and requires no additional support.
3.2. Lessons Learnt from Case 1
Miss W’s experience suggests that we may not need large doses or complicated schedules to unlock the glutamatergic “switch” in newly diagnosed obsessive-compulsive disorder (Figure 1). Two details stand out: how little drug was required, and how decisively the bedtime schedule orked.
To begin with, a nightly capsule containing only 30 mg of dextromethorphan, held in circulation by 10 mg of fluoxetine, plus 600 mg of piracetam was enough to flatten scores from PHQ-9 19 to 3 and GAD-7 16 to 0 in just over two weeks. The patient’s catastrophic spirals, fear of sleep, and loss of appetite all melted away while she was still on that entry dose; the later step-up to 45 mg of dextromethorphan was precautionary rather than curative. This mirrors the pattern seen in Cheung’s growing clinical series, where treatment-naïve patients—unburdened by years of polypharmacy or ultrarapid CYP2D6 metabolism—often top out at the same 30-mg plateau [12].
Equally important was timing. Giving fluoxetine, dextromethorphan, and piracetam together after supper lines the drug pulse up with the evening rise in cortical glutamate activity and the synaptic “housekeeping” that follows during early sleep. In Miss W, that single bedtime dose eliminated the sedativeness or dizziness sometimes reported when DXM is taken in the morning, and she began sleeping more deeply as the rumination lifted.
Taken together, the case adds weight to a simple, clinically friendly rule of thumb—start with 30 mg of fluoxetine-boosted dextromethorphan and 600 mg of piracetam at bedtime, and think about higher doses only if symptoms plateau. For young adults meeting their first psychiatrist, that may be all that is needed for a full and durable remission.
3.3. Case 2: When Nocte Dose Not Good Enough
Miss F is a 24-year-old woman who was referred on 18 October 2025 for escalating health-centred anxiety. According to the patient, the problem began several months earlier, soon after she changed jobs. She found herself preoccupied by the idea that she was harbouring a serious but undiagnosed illness. Hours were spent checking her pulse, palpating lymph-nodes, or searching the internet for rare disorders. Palpitations, diffuse muscle tension, and a sense of internal trembling accompanied these thoughts; nights were long, with prolonged sleep-onset latency followed by broken, non-refreshing sleep. Screening questionnaires reflected prominent anxiety (PHQ-9 = 5; GAD-7 = 16). A previous psychiatrist had prescribed duloxetine, but the dose, duration, and benefit were all unclear. On the basis of persistent intrusive health fears, compulsive bodily checking, and accompanying somatic arousal, we formulated the case as obsessive–compulsive disorder with a hypochondriacal theme.
At the first visit we focused on rapid symptomatic relief. Miss F began risperidone 0.5 mg and a tablet of flupentixol/melitracen (Deanxit) each night for ruminative drive and low mood. Alprazolam 0.25 mg and propranolol 10 mg were provided on an as-needed basis for panic surges, and lemborexant 2.5–5 mg was offered for insomnia.
Two weeks later, on 1 November 2025, we introduced an oral glutamatergic protocol patterned after Cheung’s regimen. All glutamatergic agents were taken at bedtime: dextromethorphan 30 mg in two 15-mg tablets, piracetam 600 mg, and the existing risperidone 0.5 mg. Bupropion XL 150 mg was added each morning to improve daytime drive. Within a few nights the patient reported a clear reduction in catastrophic health thoughts; hypnotics were no longer required.
At follow-up on 29 November she described calm, productive mornings but noted that worry still crept in toward late afternoon. To extend coverage we divided the glutamatergic dose: dextromethorphan 30 mg and piracetam 600 mg were given on waking and repeated at night, bringing daily totals to 60 mg and 1 200 mg respectively. Pregabalin 50 mg was started at bedtime for residual somatic tension, while risperidone, bupropion, and the as-needed agents were continued unchanged. She now used alprazolam and propranolol only rarely, reported vivid yet non-disturbing dreams two or three times a week, and was making concrete plans for an overseas holiday in January 2026. Repeat screening showed PHQ-9 = 2 and GAD-7 = 9, consistent with her subjective sense of “much better, just a little worry in the evenings.”
3.4. Lessons Learnt from Case 2
Miss F’s progress throws light on a practical weakness of the “all-at-bedtime” version of the Cheung glutamatergic stack (Figure 2). Taken once nightly, the combination of dextromethorphan 30 mg and piracetam 600 mg calmed her health worries through the night and well into the following morning, yet by late afternoon the same thoughts were slipping back in. She described the pattern clearly: “I’m fine until about five o’clock, then the what-ifs start again.” Screening numbers told the same story—depression had melted away (PHQ-9 = 2) but anxiety was still in the mild range (GAD-7 = 9).
Pharmacokinetics offer a neat explanation. Even with fluoxetine or bupropion on board, and dextromethorphan’s active levels may persist despite discontinuation of the regimen [13], the AMPA boost from a single 600-mg dose of piracetam may fade sooner [14]. Bedtime dosing therefore covers the biologically busy night-time window and the first half of the working day, but by late afternoon plasma concentrations and receptor occupancy are waning—just when fatigue and fewer distractions create a perfect stage for rumination to return.
The solution in Miss F’s case—splitting both glutamatergic agents into morning and evening doses without raising the daily total—proved immediately helpful. Morning stability was preserved, evening “escape” all but disappeared, and the need for rescue alprazolam or propranolol dropped to near zero.
In practice, then, single bedtime dosing remains a sensible starting point: it is simple, aligns with circadian glutamate peaks, and often improves sleep quality. Clinicians should, however, listen for reports of late-day rebound; when that pattern emerges, a twice-daily schedule can plug the gap quickly and without extra medication burden.
3.5. Case 3: Insights upon Dose Scheduling
Miss L is a 20-year-old woman in her second year of nursing school who was referred on 19 May 2025 for a sudden intensification of long-standing anxiety. During the week before the visit she had lived in a near-constant state of alarm, describing palpitations, queasy stomach, fine tremor, sweating, intermittent numbness of her forearms, and little interest in food. Sleep, however, remained intact. Several months earlier two different primary-care clinics had treated her as a straightforward case of depression and generalized anxiety, first with fluoxetine 20 mg, later with escitalopram 10 mg; neither agent brought durable relief. At presentation her Patient Health Questionnaire-9 (PHQ-9) score was 15 and her Generalised Anxiety Disorder-7 (GAD-7) score was 15, both in the moderately severe range. Careful questioning revealed intrusive doubt-laden thoughts and hours of mental checking, leading us to re-frame the problem as predominantly obsessional obsessive–compulsive disorder (OCD).
3.5.1. Early Management (May–June 2025)
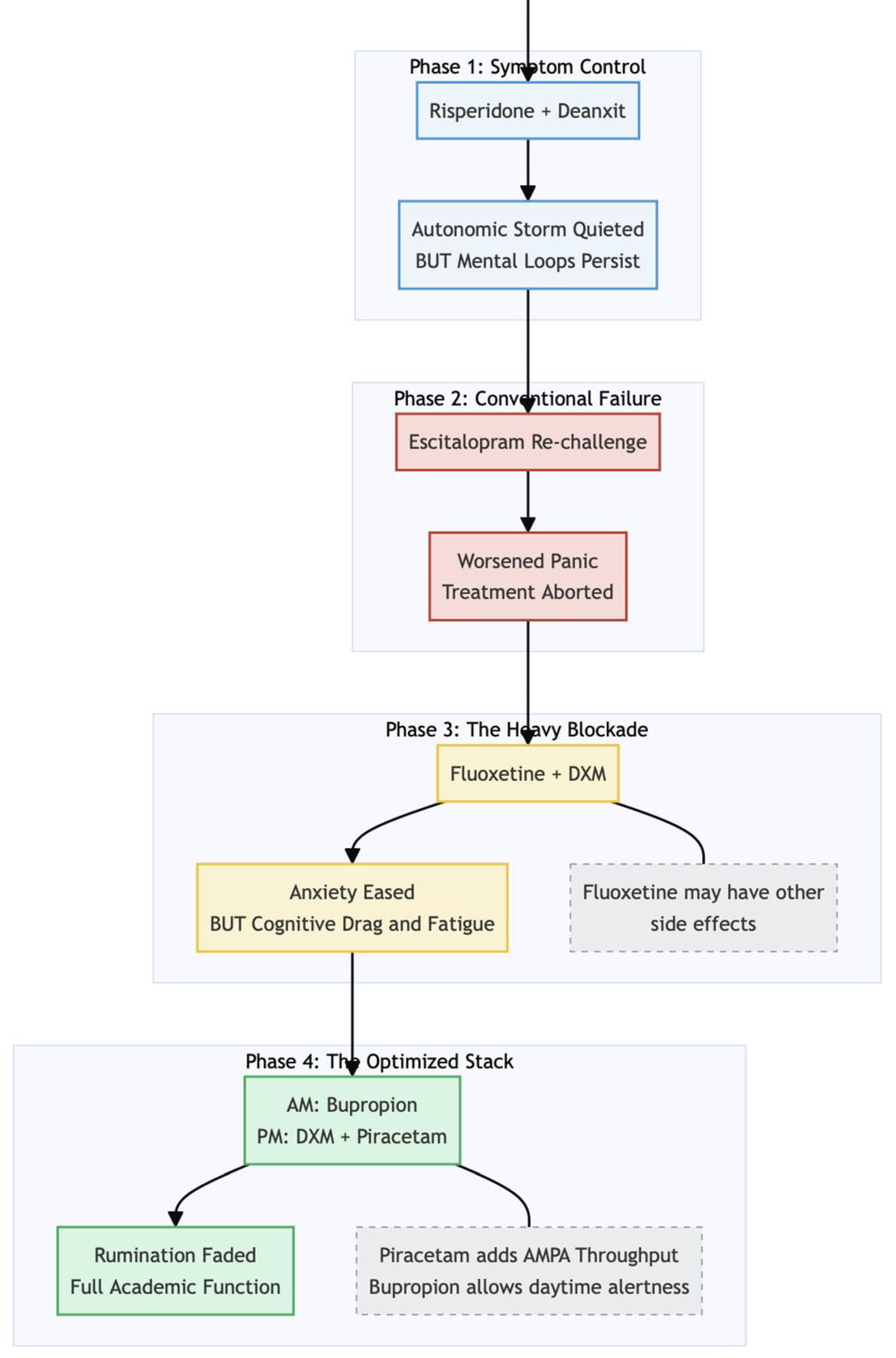
We opted for a symptom-control strategy while planning longer-term therapy. Low-dose risperidone 0.5 mg each night, propranolol 10 mg up to three times daily as needed, and one tablet of flupentixol/melitracen (Deanxit) at bedtime quickly quieted the autonomic storm; by the first week of June her PHQ-9 had fallen to 4 and her GAD-7 to 6.
3.5.2. Trials of Conventional Agents (Late June–July 2025)
Because obsessive rumination persisted, we re-introduced escitalopram at 5 mg and added pregabalin 50 mg nightly. Within ten days the selective-serotonin-reuptake inhibitor worsened panic, so it was withdrawn; pregabalin alone offered little more than sedation.
3.5.3. Shift to a Glutamatergic Approach (August–September 2025)
On 25 August we began an oral ketamine-class regimen first proposed by Cheung: fluoxetine 10 mg nightly to inhibit CYP2D6, plus dextromethorphan (DXM) 30 mg (two 15-mg tablets) at bedtime. One month later anxiety had eased but the patient now grappled with leaden fatigue, poor concentration, a globus sensation, and scant appetite (PHQ-9 = 13, GAD-7 = 11). To address the cognitive drag we discontinued fluoxetine and, on 6 September, completed the Cheung stack by adding piracetam 600 mg nightly. Bupropion XL 150 mg each morning replaced the fluoxetine to provide daylight activation, while risperidone 0.5 mg was retained for its anti-obsessional effect.
3.5.4. Clinical Course (September–October 2025)
Three weeks later Miss L reported that the relentless mental churning had dwindled to brief, manageable episodes. She denied side-effects, although her mother observed occasional daytime sluggishness that the patient herself did not notice. Screening scores on 26 September were PHQ-9 = 11 and GAD-7 = 9. At her most recent review on 24 October she felt “okay so far—much less ruminating,” was attending all classes, and was preparing for her November clinical practicum. Questionnaires had normalised (PHQ-9 = 8, GAD-7 = 6).
3.5.5. Current Medication Profile and Status (24 October 2025)
• Dextromethorphan 30 mg nightly
• Piracetam 600 mg nightly
• Risperidone 0.5 mg nightly
• Flupentixol/melitracen one tablet nightly
• Bupropion XL 150 mg each morning
• Alprazolam 0.25 mg as needed (rarely required)
Miss L is now functioning at her pre-morbid level, attending university without limitation and ready to enter clinical rotations. Obsessive rumination is minimal, somatic anxiety is quiescent, and no significant adverse effects have emerged from the nightly Cheung glutamatergic combination—DXM plus piracetam—used alongside low-dose adjuncts.
3.6. Lessons Learnt from Case 3
Miss L’s course offers a window into how an oral, ketamine-class strategy can be fine-tuned in day-to-day practice (Figure 3). Two details seem to have driven the turnaround.
First, the night she added piracetam 600 mg marked the point where improvement moved from slow and uneven to steady and obvious. Up to that moment she was taking dextromethorphan (DXM) alone and still felt drained, jittery, and stuck in loops of worry. Within three weeks of adding piracetam her rumination had faded to background noise, her energy was back, and both PHQ-9 and GAD-7 scores nearly halved. The simple timeline argues that piracetam supplied the missing piece—extra AMPA throughput—needed to turn DXM’s NMDA blockade into real neuroplastic change. Similar “second-wind” responses after piracetam add-on are described throughout the original protocol paper [11].
Second, the decision to keep the activating drug bupropion in the morning and reserve DXM plus piracetam for bedtime appears to have paid off. Bupropion does inhibit CYP2D6, but not as forcefully as fluoxetine, so giving it 12 hours apart from DXM reduces the risk of unpredictable peaks while still providing daytime drive. Cheung [15] explicitly recommends this split schedule for students or shift-workers who need clear mornings without the buzz that can follow a one-time, all-in dose. This is because bupropion could inhibit CYP2D6 by turning down its gene transcription [16]. Miss L never complained of insomnia or overshoot, yet reported sharper concentration during clinical skills labs—a small but practical endorsement of the timing strategy.
4. Conclusions
Taken together, the three cases underscore both the promise and the boundaries of an all-oral glutamatergic strategy for obsessive–compulsive disorder. The first lesson is that the doses required for a full response can be surprisingly small when the patient has not yet been exposed to high-dose serotonergic or antipsychotic therapy. Miss W, entirely treatment-naïve, reached complete symptomatic and occupational remission with nothing more than dextromethorphan 30 mg and piracetam 600 mg at bedtime.
The second lesson is that pharmacokinetics matter. Miss F’s late-day rebound of health anxiety illustrates how plasma levels of dextrorphan and the functional impact of piracetam wane 12–18 hours after a single nocte dose, even when a CYP2D6 inhibitor is on board [14]. For patients whose obsessions predictably surge toward the end of the day, merely dividing the same total daily dose into morning and evening administrations may seal the gap without adding pill burden or side-effects—as it did in her case.
Finally, Miss L reminds us that not every patient needs such fine-tuning; for some, once-nightly dosing remains both convenient and fully effective. The regimen’s real strength, therefore, lies in its flexibility. Clinicians can start with a simple bedtime schedule confident that many patients will remit, yet they can just as readily shift to split dosing when diurnal escape becomes evident. An inexpensive, easily adjusted oral protocol thus offers a practical bridge between the mechanistic insights gained from ketamine research and the day-to-day realities of outpatient care.
Funding
None declared.
Conflicts of Interest
None declared.
References
- Hirschtritt, M.E.; Bloch, M.H.; Mathews, C.A. Obsessive-Compulsive Disorder: Advances in Diagnosis and Treatment. JAMA 2017, 317, 1358–1367. [Google Scholar] [CrossRef] [PubMed]
- Öst, L.G.; Havnen, A.; Hansen, B.; Kvale, G. Cognitive behavioral treatments of obsessive-compulsive disorder. A systematic review and meta-analysis of studies published 1993–2014. Clin. Psychol. Rev. 2015, 40, 156–169. [Google Scholar] [CrossRef] [PubMed]
- Pallanti, S.; Hollander, E.; Bienstock, C.; Koran, L.; Leckman, J.; Marazziti, D.; Pato, M.; Stein, D.; Zohar, J.; International Treatment Refractory OCD Consortium. Treatment non-response in OCD: Methodological issues and operational definitions. Int. J. Neuropsychopharmacol. 2002, 5, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Dold, M.; Aigner, M.; Lanzenberger, R.; Kasper, S. Antipsychotic Augmentation of Serotonin Reuptake Inhibitors in Treatment-Resistant Obsessive-Compulsive Disorder: An Update Meta-Analysis of Double-Blind, Randomized, Placebo-Controlled Trials. Int. J. Neuropsychopharmacol. 2015, 18, pyv047. [Google Scholar] [CrossRef] [PubMed]
- Milad, M.R.; Rauch, S.L. Obsessive-compulsive disorder: Beyond segregated cortico-striatal pathways. Trends Cogn. Sci. 2012, 16, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Ahmari, S.E.; Spellman, T.; Douglass, N.L.; Kheirbek, M.A.; Simpson, H.B.; Deisseroth, K.; Gordon, J.A.; Hen, R. Repeated cortico-striatal stimulation generates persistent OCD-like behavior. Science 2013, 340, 1234–1239. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, C.I.; Kegeles, L.S.; Levinson, A.; Feng, T.; Marcus, S.M.; Vermes, D.; Flood, P.; Simpson, H.B. Randomized controlled crossover trial of ketamine in obsessive-compulsive disorder: Proof-of-concept. Neuropsychopharmacology 2013, 38, 2475–2483. [Google Scholar] [CrossRef] [PubMed]
- Modarresi, A.; Chaibakhsh, S.; Koulaeinejad, N.; Koupaei, S.R. A systematic review and meta-analysis: Memantine augmentation in moderate to severe obsessive-compulsive disorder. Psychiatry Res. 2019, 282, 112602. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, C.I.; Wheaton, M.; Zwerling, J.; Steinman, S.A.; Sonnenfeld, D.; Galfalvy, H.; Simpson, H.B. Can exposure-based CBT extend the effects of intravenous ketamine in obsessive-compulsive disorder? An open-label trial. J. Clin. Psychiatry 2016, 77, 408–409. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.E.; Jenike, E.A.; Hezel, D.M.; Stack, D.E.; Dodman, N.H.; Shuster, L.; Jenike, M.A. A single-blinded case-control study of memantine in severe obsessive-compulsive disorder. J. Clin. Psychopharmacol. 2010, 30, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Cheung, N. DXM, CYP2D6-Inhibiting Antidepressants, Piracetam, and Glutamine: Proposing a Ketamine-Class Antidepressant Regimen with Existing Drugs. Preprints 2025. [Google Scholar] [CrossRef]
- Cheung, N. Case Series: Marked Improvement in Treatment-Resistant Obsessive–Compulsive Symptoms with Over-the-Counter Glutamatergic Augmentation in Routine Clinical Practice. Preprints 2025. [Google Scholar] [CrossRef]
- Singh, M.A.; Johnson, D. Serotonin Syndrome and Dextromethorphan Toxicity Caused by Drug-Drug Interaction Between Fluoxetine and Bupropion-Dextromethorphan: A Case Report. J. Clin. Psychiatry 2024, 85, 23cr15139. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.H.; Oswald, R.E. Piracetam defines a new binding site for allosteric modulators of alpha-amino-3-hydroxy-5-methyl-4-isoxazole-propionic acid (AMPA) receptors. J. Med. Chem. 2010, 53, 2197–2203. [Google Scholar] [CrossRef] [PubMed]
- Cheung, N. Clinical Experience and Optimisation of the Cheung Glutamatergic Regimen for Refractory Psychiatric Diseases. Preprints 2025. [Google Scholar] [CrossRef]
- Sager, J.E.; Tripathy, S.; Price, L.S.; Nath, A.; Chang, J.; Stephenson-Famy, A.; Isoherranen, N. In vitro to in vivo extrapolation of the complex drug-drug interaction of bupropion and its metabolites with CYP2D6; simultaneous reversible inhibition and CYP2D6 downregulation. Biochem. Pharmacol. 2017, 123, 85–96. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Case 1.
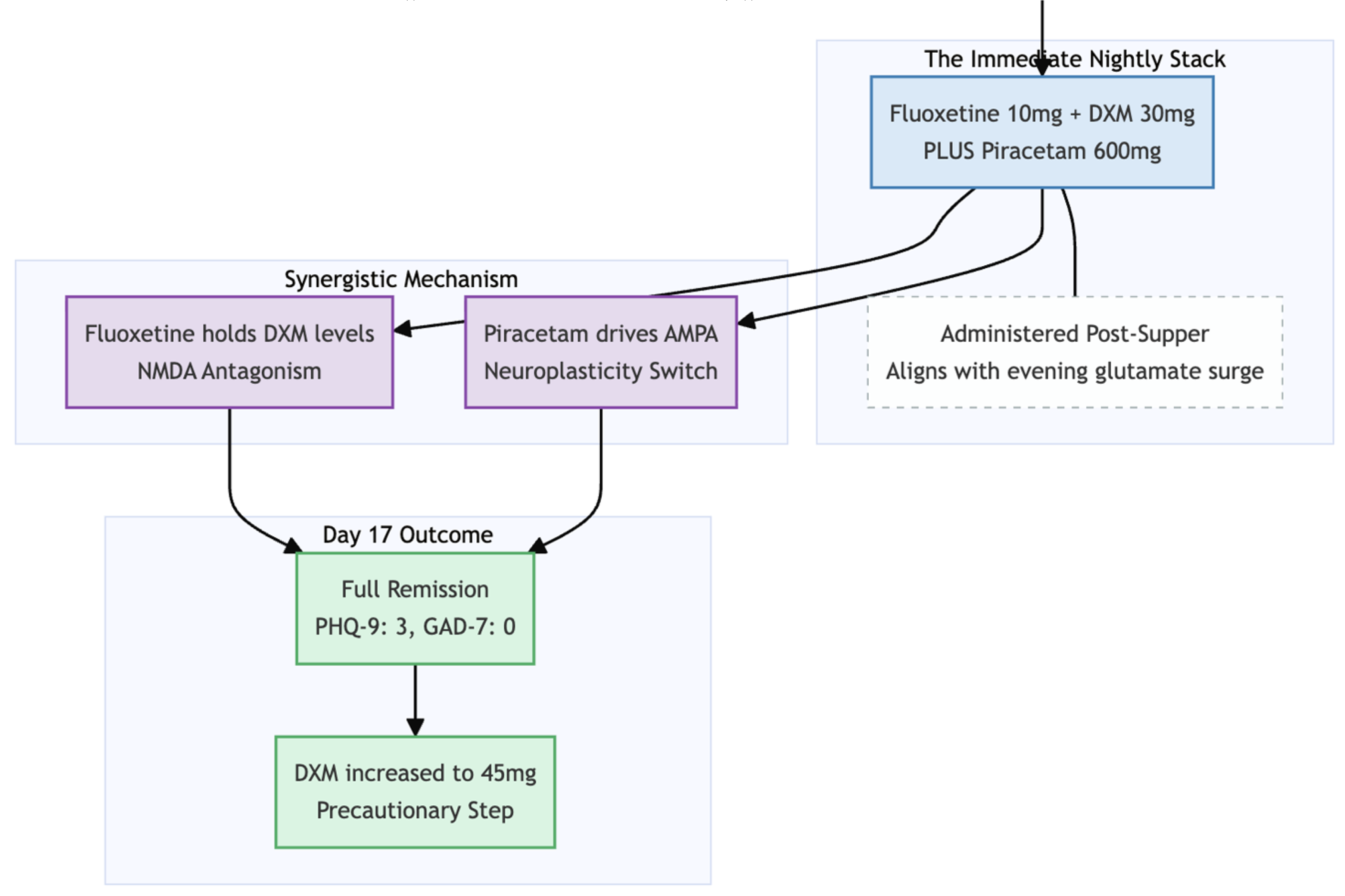
Figure 2.
Case 2.
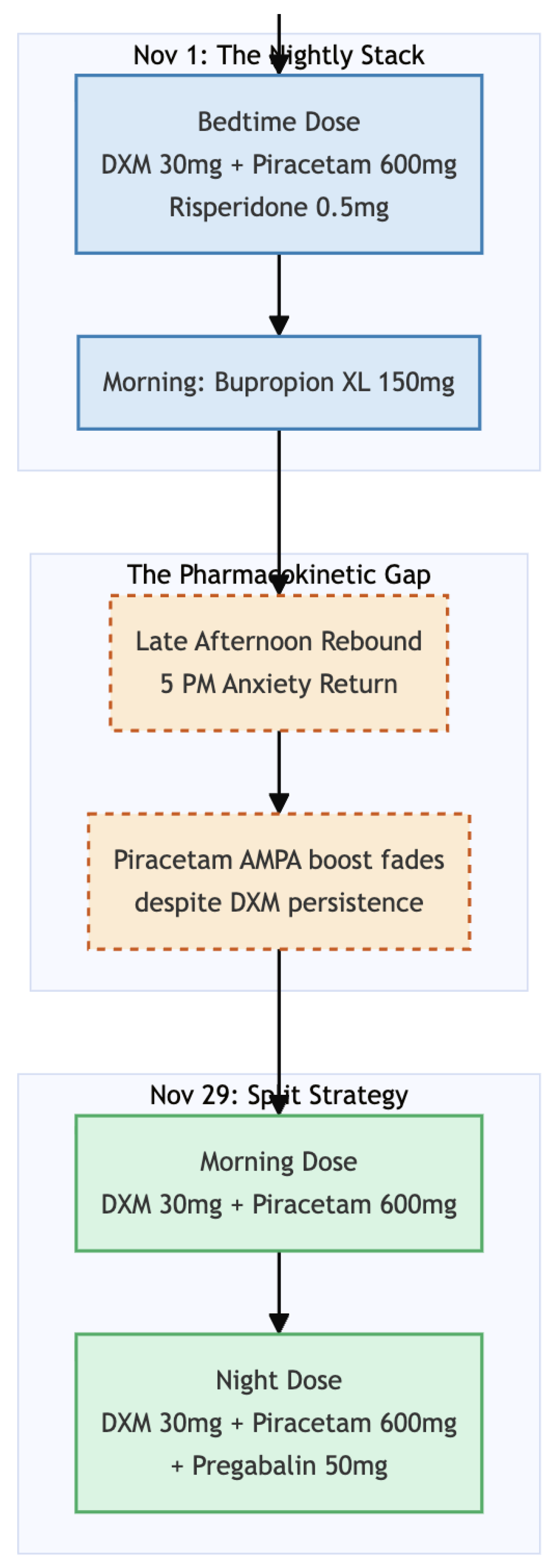
Figure 3.
Case 3.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



