Submitted:
02 December 2025
Posted:
05 December 2025
You are already at the latest version
Abstract
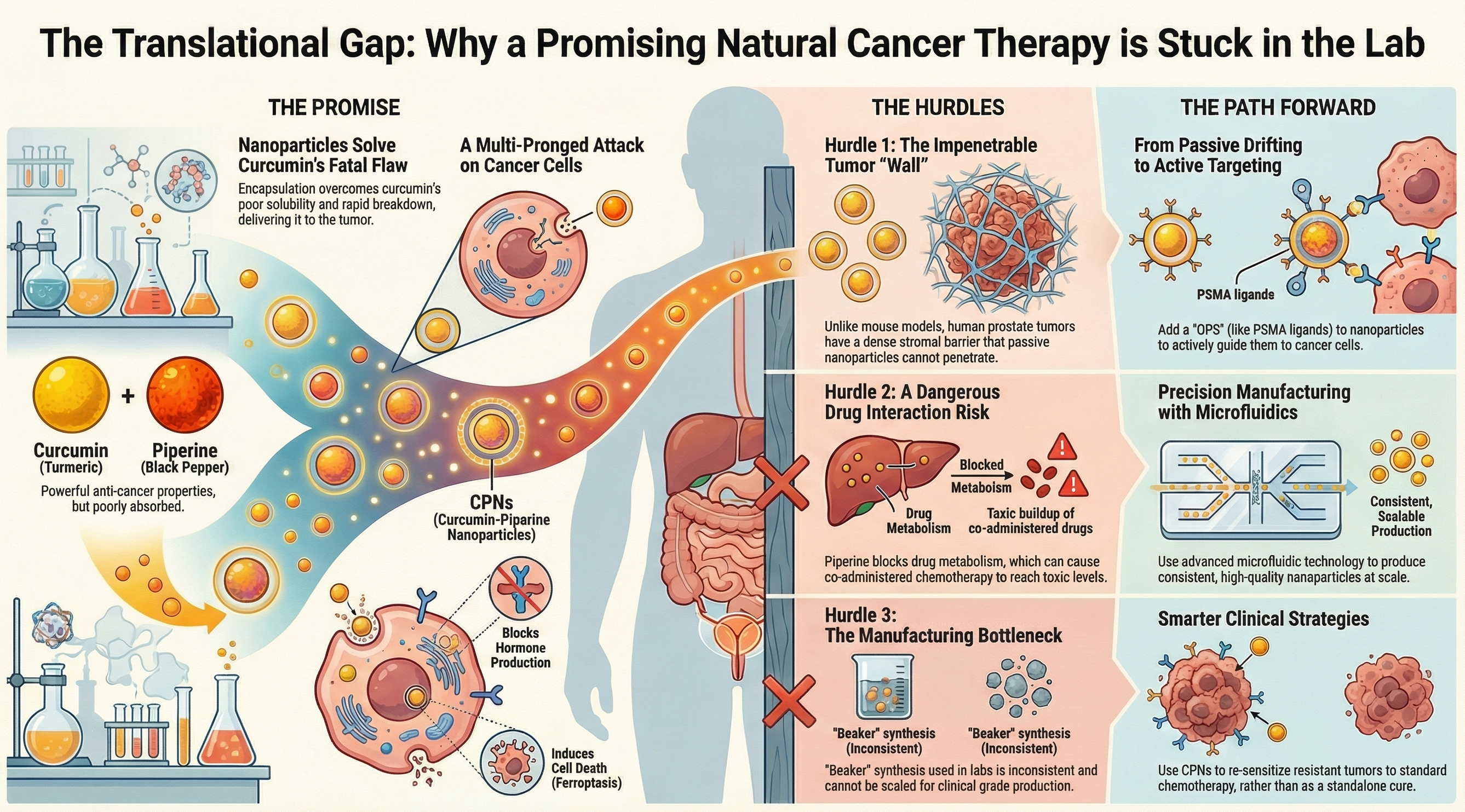
Introduction: Prostate cancer (PC) treatment is limited by resistance mechanisms and cumulative toxicities, necessitating novel therapeutic strategies. While curcumin and piperine exhibit potent anticancer properties, their clinical utility is severely compromised by poor bioavailability and rapid metabolism. Areas covered: This review critically analyzes the preclinical and clinical landscape of curcumin and piperine nanoformulations (CPN) for PC treatment. We utilized PubMed and Scopus (2000–2025) to evaluate molecular mechanisms, focusing on CYP17A1 inhibition, PI3K/Akt/mTOR signaling, and ferroptosis. The report examines the physicochemical attributes of nanocarriers, including PLGA and liposomes, and addresses translational barriers such as the heterogeneity of the Enhanced Permeability and Retention (EPR) effect, stromal density, and piperine-mediated drug–drug interaction risks. Expert opinion: While nano-encapsulation enhances the therapeutic index of curcumin, clinical translation remains stalled by a reliance on passive targeting and insufficient manufacturing scalability. Future success depends on shifting from "beaker" synthesis to microfluidic production (Quality by Design) and adopting active targeting (e.g., PSMA-directed delivery) to penetrate the prostate stroma. Without these strategic pivots and biomarker-driven trials, CPNs risk remaining an academic curiosity rather than evolving into a viable clinical intervention.
Keywords:
steroidogenesis
; cyp17a1
; prostate cancer
; curcumin nanoparticles
; androgen synthesis
; nanoparticle formulations
1. Introduction
Prostate cancer (PC) remains a major global health challenge, with limitations in current treatment options, particularly for advanced and castration-resistant forms of the disease (1, 2). While localized disease is often manageable through active surveillance, prostatectomy, or radiotherapy, the progression to metastatic castration-resistant prostate cancer (mCRPC) marks a lethal turn in the disease trajectory. The standard of care for advanced PC revolves around Androgen Deprivation Therapy (ADT), which aims to suppress the gonadal production of testosterone, the primary fuel for prostate cancer cell proliferation. However, the efficacy of ADT is invariably finite. Tumors inevitably develop resistance mechanisms, transitioning to a castration-resistant state characterized by androgen receptor (AR) amplification, mutations, and, crucially, the upregulation of intratumoral steroidogenesis enzymes that allow the cancer to synthesize its own androgens.
The limitations of current pharmacotherapy, including the significant side effect profiles of taxane chemotherapies (docetaxel, cabazitaxel) and second-generation anti-androgens (abiraterone, enzalutamide), have spurred an intense search for alternative therapeutic agents that offer high efficacy with a more favorable safety profile. Natural compounds, or phytochemicals, have garnered considerable attention in this domain (3). Curcumin, the yellow pigment and principal bioactive component of turmeric, has been extensively studied for its anti-inflammatory, antioxidant, and anticancer properties. Preclinical studies have consistently shown that curcumin can downregulate AR expression, inhibit angiogenesis, and induce apoptosis in PC cells. Similarly, piperine, the pungent alkaloid found in black pepper, has demonstrated independent anticancer activity and, perhaps more importantly, the ability to function as a bioenhancer (4). Despite this immense preclinical promise, the translation of curcumin and piperine into clinical practice has been historically hampered by their dismal pharmacokinetic profiles. Curcumin is notorious for its poor aqueous solubility (approximately 11 ng/mL), instability at physiological pH, and rapid metabolism via hepatic glucuronidation and sulfation (5). Oral administration of free curcumin results in negligible systemic concentrations, often failing to reach the threshold required for therapeutic activity in prostatic tissue. Piperine can partially mitigate this by inhibiting the metabolic enzymes responsible for curcumin's clearance, yet the co-administration of "free" unencapsulated forms remains suboptimal due to asynchronous biodistribution and rapid clearance.
Nanotechnology offers a sophisticated solution to these pharmacological deficiencies. By encapsulating these bioactive agents within nanocarriers, such as polymeric nanoparticles, liposomes, or micelles, researchers aim to enhance solubility, protect the payload from premature degradation, and improve accumulation at the tumor site (6-9). The hypothesis is that a well-engineered "Curcumin-Piperine Nanoparticle" (CPN) system can synchronize the delivery of both agents, maximizing their synergistic potential while minimizing systemic exposure.
Recent research, including studies on the ability of curcumin and piperine nanoformulations to modulate steroidogenesis, highlights their therapeutic potential (Figure 1) (10). However, the journey from a promising engineered nanoparticle in a petri dish to a clinically approved drug is fraught with challenges, often referred to as the "valley of death" in drug development. This report aims to move beyond a superficial summary of "promising results" to provide a critical, deep-dive analysis of the clinical hurdles that currently stall the progress of CPNs.
To provide a comprehensive analysis of this landscape, we conducted a systematic literature search using PubMed, Scopus, and Web of Science databases for articles published between January 2000 and November 2025. Keywords included 'Curcumin', 'Piperine', 'Nanoparticles', 'Prostate Cancer', 'CYP17A1', 'Ferroptosis', and 'Clinical Trials'. We prioritized studies that provided quantitative pharmacokinetic data, mechanistic insights into steroidogenesis, and those addressing specific translational barriers such as the EPR effect and manufacturing scalability. We analyzed the data regarding efficacy in human trials, the nuanced safety risks associated with piperine-mediated drug interactions, the physical barriers of the prostate tumor microenvironment that limit passive drug delivery, and the rigorous manufacturing standards required by regulatory bodies. Through this lens, we evaluate whether CPNs are indeed a viable path to clinical reality or a bridge too far.
2. The Therapeutic Rationale: Unpacking the Molecular Mechanisms
The allure of curcumin and piperine nanoparticles in the context of prostate cancer stems from their multifaceted mechanisms of action and the inherent advantages offered by nanodelivery systems. One of the most compelling mechanisms recently elucidated for CPNs is their ability to interfere with androgen biosynthesis. In mCRPC, tumor cells adapt to low systemic testosterone levels by upregulating the enzyme cytochrome P450 17A1 (CYP17A1). This enzyme possesses dual activities: 17α-hydroxylase activity and 17,20-lyase activity, both of which are essential for the conversion of pregnenolone and progesterone into androgens like dehydroepiandrosterone (DHEA) and androstenedione (6, 10).
2.1. Targeted Enzyme Inhibition
Preclinical evidence strongly suggests that curcumin and piperine, particularly in combination and when formulated as nanoparticles, can interfere with critical pathways driving prostate cancer progression. This is particularly relevant as endogenous androgens are pivotal in the development and progression of PC. In mCRPC, tumor cells adapt to low systemic testosterone levels by upregulating the enzyme cytochrome P450 17A1 (CYP17A1). This enzyme possesses dual activities: 17α-hydroxylase activity and 17,20-lyase activity, both of which are essential for the conversion of pregnenolone and progesterone into androgens like dehydroepiandrosterone (DHEA) and androstenedione. By targeting CYP17A1, (11, 12), these nanoparticles can potentially reduce androgen levels, thereby impacting androgen receptor (AR) signaling, a key driver of prostate cancer growth.
Quantitative Potency: In in vitro assays using NCI-H295R human adrenal cells, curcumin nanoparticles exhibited an IC50 of approximately 9.98 µM for 17α-hydroxylase inhibition. While this is less potent than abiraterone on a molar basis, the inhibition is biologically significant given the high local concentrations achievable via nanoparticle delivery.
Selectivity Profile: A critical limitation of abiraterone is its broad inhibition of steroidogenic enzymes, including CYP21A2, which leads to mineralocorticoid excess and necessitates the co-administration of prednisone to prevent hypertension and hypokalemia. In contrast, curcumin and piperine appear to offer a more targeted inhibition profile, predominantly affecting the 17α-hydroxylase and 17,20-lyase functions without broadly disrupting the cortisol axis to the same deleterious extent (10).
Synergistic Suppression: The combination of curcumin and piperine in a single nanoparticle (CPN) resulted in a statistically significant reduction in downstream metabolites, specifically androstenedione and cortisol, compared to either agent alone. This suggests that the nanoformulation not only delivers the drugs but may facilitate a dual blockade of the steroidogenic pathway, directly starving the AR-positive prostate cancer cells of their requisite ligands.
2.2. Disruption of Oncogenic Signaling Cascades
Beyond the androgen axis, prostate cancer progression relies on a network of survival signaling pathways. CPNs have been shown to exert pleiotropic effects, effectively hitting multiple targets simultaneously, a "polypharmacology" approach that is difficult for cancer cells to bypass via single-point mutations.
2.2.1. The PI3K/Akt/mTOR Axis
Aberrant activation of the PI3K/Akt/mTOR pathway occurs in approximately 40-50% of CRPC cases, often due to the loss of the tumor suppressor PTEN. This pathway drives cell proliferation and survival, rendering cells resistant to apoptosis (Figure 2). Curcumin nanoparticles have been shown to significantly downregulate the phosphorylation of Akt (at Ser473) and mTOR, effectively shutting down this survival signal (7). In PC3 cells, which are PTEN-null and highly aggressive, treatment led to a reduction in cell viability that correlated with the suppression of Akt phosphorylation, a result not achieved by free curcumin at equivalent doses due to poor uptake.
2.2.2. Bcl-2 Family Modulation and Apoptosis
The balance between pro-apoptotic and anti-apoptotic proteins dictates cell fate. CPNs shift this rheostat towards death. Treatment with curcumin-loaded nanoparticles has been observed to downregulate anti-apoptotic proteins Bcl-2 and Bcl-xL while simultaneously upregulating pro-apoptotic effectors Bax and Bak. This disruption of the mitochondrial membrane potential leads to the release of cytochrome c and the activation of the caspase cascade (caspase-3 and caspase-9), culminating in programmed cell death (Figure 2) (13).
2.3. Emerging Mechanisms: Ferroptosis and Autophagy
Recent research has expanded the mechanistic scope of curcumin to include non-apoptotic forms of cell death, which are particularly relevant for eradicating drug-resistant clones.
2.3.1. Ferroptosis Induction
Ferroptosis is an iron-dependent form of regulated cell death characterized by the accumulation of lipid peroxides. It is distinct from apoptosis and necrosis. Curcumin has been identified as an inducer of ferroptosis in cancer cells. It operates by depleting glutathione peroxidase 4 (GPX4), a key enzyme that protects cells from oxidative damage, and by upregulating Acyl-CoA synthetase long-chain family member 4 (ACSL4), which promotes lipid peroxidation (14). Since CRPC cells often develop resistance to apoptosis (e.g., via Bcl-2 overexpression), inducing ferroptosis provides an alternative "kill switch." CPNs, by delivering high intracellular concentrations of curcumin, can overwhelm the cell's antioxidant defenses and trigger this iron-dependent death, a mechanism that is currently being explored as a way to reverse docetaxel resistance (Figure 2) (14).
2.3.2. Autophagy Regulation
Autophagy acts as a double-edged sword in cancer, promoting survival under stress or leading to cell death ("autophagic cell death") if over-activated. Curcumin nanoparticles have been shown to induce autophagy in PC3 cells, evidenced by the upregulation of Beclin-1 and the conversion of LC3-I to LC3-II. Curcumin and piperine nanoparticles have been shown to reduce cancer cell viability and inhibit cell migration across various prostate cancer cell lines, including LNCaP, VCaP, DU145, and PC3 (10). Curcumin-piperine nanoparticles (CPN) have demonstrated the highest efficacy in these studies. The anticancer effects also extend to the induction of apoptosis (programmed cell death) and cell cycle arrest, thereby directly impeding tumor growth. Interestingly, this autophagic flux can be linked to the suppression of the PI3K/Akt/mTOR pathway, which normally inhibits autophagy. In the context of CPN therapy, this massive induction of autophagy appears to exceed the cell's adaptive capacity, contributing to cytotoxicity.
Beyond these direct anticancer actions, curcumin is well-known for its potent anti-inflammatory and antioxidant properties, which can further contribute to a less favorable tumor microenvironment. Moreover, considering the recent advances in development of novel non-steroidal anti-androgen compounds, effect of curcumin-piperine nanoparticles can be further enhanced by combining selective CYP17A1 inhibitors in these nanoformulations (15-18).
3. Nanocarrier Design and Physicochemical Attributes
The efficacy of curcumin and piperine is inextricably linked to the vehicle used to deliver them. "Free" drugs are of little use if they cannot reach the target. The primary challenge hindering the clinical use of free curcumin is its poor pharmacokinetic profile, characterized by low aqueous solubility, rapid metabolism (primarily hepatic glucuronidation and sulfation), and consequently, poor bioavailability. Piperine is often co-administered with curcumin as it can inhibit enzymes involved in curcumin's metabolism, thereby increasing its systemic availability (19). Nanoparticle formulations made from biocompatible, biodegradable, non-toxic and non-immunogenic excipients offer a promising strategy to circumvent these limitations (20-22). The development of nanocarriers is therefore not just a formulation exercise but a critical component of the therapeutic strategy. A summary of the physicochemical properties of various CPN formulations evaluated in prostate cancer models, highlighting the critical parameters of size, zeta potential, and drug loading that dictate biological performance is presented in table 1.
3.1. Polymeric Nanoparticles (PLGA)
Poly(lactic-co-glycolic acid) (PLGA) remains the gold standard for biodegradable nanocarriers due to its FDA approval for human use and controllable hydrolysis rates. The data indicates that PLGA nanoparticles co-loaded with curcumin and piperine typically fall within the 150–200 nm size range (10). This size is theoretically optimal for passive tumor accumulation via the EPR effect (discussed in Section 6.1), as it is large enough to avoid renal filtration (<10 nm) but small enough to extravasate through leaky tumor capillaries. The negative zeta potential (~-30 mV) observed in these formulations is critical for colloidal stability, preventing particle aggregation through electrostatic repulsion. However, a highly negative charge can also repel interaction with the negatively charged cell membrane, which is why surface modification or active targeting ligands (like PSMA antibodies) are often employed to facilitate uptake (23).
3.2. Lipid-Based and Hybrid Systems
Lipid-based carriers, such as liposomes and solid lipid nanoparticles (SLNs), offer the advantage of mimicking biological membranes, facilitating fusion and intracellular delivery provide excellent biocompatibility, but they often exhibit poor storage stability (24). Lipid-polymer hybrid nanoparticles (LPNs) combine the structural integrity of polymers with the biocompatibility of lipids. Yan et al. demonstrated that LPNs could co-encapsulate the hydrophobic drug docetaxel with curcumin (25). Interestingly, these particles exhibited a positive zeta potential (+35.7 mV), likely due to the specific lipid composition or surface coating (Table 1). While positive charges enhance interaction with cell membranes, they can also lead to non-specific binding with serum proteins (opsonization) and rapid clearance by the immune system, a trade-off that requires careful balancing during formulation design (26).
Encapsulating curcumin and piperine within nanoparticles can significantly enhance their solubility and protect them from premature degradation and rapid metabolism (7, 21, 27-30). This protection allows for a higher bioavailability of the bioactive compounds at the tumor tissues. Moreover, nanoparticles can improve cellular uptake. The size, surface properties, and composition of nanoparticles can be engineered to facilitate their passage across biological barriers and promote internalization by cancer cells, potentially through the enhanced permeability and retention (EPR) effect often observed in tumor vasculature (31). This passive targeting, coupled with the potential for active targeting by functionalizing nanoparticles with specific ligands, can lead to preferential accumulation in tumor sites, thereby increasing therapeutic efficacy while minimizing exposure and potential damage to healthy tissues. Some formulations also aim for sustained release and prolonged circulation times, ensuring that the therapeutic agents remain active in the body long enough to exert their anticancer effects. Despite the compelling preclinical rationale, the journey of curcumin and piperine nanoparticles from the laboratory bench to the patient's bedside is fraught with significant clinical hurdles that demand rigorous investigation and innovative solutions.
4. Preclinical Efficacy: The Evidence Base
The translation of CPNs is supported by a robust body of preclinical evidence demonstrating efficacy across in vitro and in vivo models. However, interpreting this data requires understanding the nuances of the models used.
4.1. In Vitro Sensitivity and Cell Line Specificity
The evaluation of Curcumin-Piperine Nanoparticles (CPNs) has relied heavily on a panel of immortalized cell lines that recapitulate distinct pathological stages of prostate cancer progression. The validity of these preclinical findings hinges on the specific genomic and phenotypic characteristics of the models employed. The vast majority of studies utilize the LNCaP, PC3, and DU145 cell lines, which form the gold standard triad for prostate cancer research (34).
LNCaP cells, derived from a lymph node metastasis, retain androgen receptor (AR) expression and PSA secretion (35). They display a CD44low/CD133low phenotype. This makes them an ideal model for androgen-sensitive disease where the CYP17A1-inhibitory mechanism of curcumin is most relevant. Efficacy in this model suggests potential in early CRPC where tumors still rely on the androgen axis. In contrast, PC3 and DU145 cells represent the lethal, androgen-independent phenotype (mCRPC). PC3 cells, derived from a bone metastasis , are AR-negative and typically PTEN-null (36). They express high levels of CD44 (CD44high/CD133low) , correlating with a stem-like, aggressive metastatic potential. DU145 cells, derived from a brain metastasis , are also AR-negative but harbor distinct mutations. In these models, the efficacy of CPNs is not mediated by CYP17A1 inhibition but rather through alternative pathways, primarily the inhibition of the PI3K/Akt/mTOR survival cascade (highly active in PTEN-null PC3 cells) and the induction of ferroptosis (37).
This distinction is critical because the mechanism of CPN efficacy is context-dependent. A robust CPN formulation must demonstrate efficacy across these diverse phenotypes, targeting androgen synthesis in LNCaP-like tumors and survival signaling in PC3-like metastases, to be considered a viable candidate for the heterogeneous landscape of clinical prostate cancer (10). The combination of curcumin and piperine in nanoparticles consistently outperforms single-agent nanoparticles. The "Combination Index" (CI) values reported in these studies frequently fall below 1.0, indicating true synergy rather than just additive effects. This validates the hypothesis that piperine enhances curcumin's intracellular availability and efficacy (38).
4.2. In Vivo Xenograft Performance
The acid test for any nanomedicine is its performance in an animal model. In C4-2 xenograft models (a model of CRPC), intratumoral or systemic administration of PLGA-curcumin nanoparticles resulted in significantly lower tumor volumes compared to free curcumin or vehicle controls (7). Crucially, these studies often report a lack of systemic toxicity (weight loss, hematological changes), highlighting the safety advantage of the nanoparticle format.
It is important to acknowledge that most preclinical studies utilize subcutaneous xenografts, which are highly vascularized and exhibit a pronounced EPR effect. As discussed later, this may overestimate the delivery efficiency compared to the actual clinical scenario of human prostate tumors, which are often orthotopic and characterized by dense stromal barriers.
5. Clinical Translation Landscape
Despite the compelling preclinical rationale, the clinical translation of curcumin and piperine nanoparticles has been slow and fraught with mixed results (Table 2). A critical analysis of the clinical trial landscape reveals a disconnect between the promise seen in mice and the realities of human trials (39, 40). The most formidable barrier is the need for robust clinical validation of efficacy in human prostate cancer patients. While numerous preclinical studies showcase the potential of these nanoformulations, this success often does not translate directly to human trials. A critical lack of well-designed, large-scale Phase I, II, and III clinical trials specifically investigating curcumin and piperine nanoparticles for prostate cancer persistence. Although some clinical trials have explored curcumin (https://clinicaltrials.gov/study/NCT03769766), often in combination with other agents, for various cancers including prostate cancer, specific data on the nanoparticle formulations co-delivering curcumin and piperine remain scarce (https://clinicaltrials.gov/study/NCT02724618). One encouraging development is an ongoing Phase 2 clinical trial exploring curcumin and piperine supplementation in early-stage prostate cancer patients under active surveillance, which may provide valuable insights (https://clinicaltrials.gov/study/NCT04731844).
Even with ongoing trials, defining optimal dosage and treatment regimens is a complex task (41). Determining the most effective and safe dose, the frequency of administration, and the appropriate duration of treatment requires meticulous dose-escalation and efficacy studies. Furthermore, patient selection and the development of predictive biomarkers are crucial. Not all prostate cancer patients will respond equally to this therapeutic approach. Identifying specific molecular signatures or clinical characteristics that predict a favorable response will be essential for tailoring treatment and maximizing benefit.
5.1. Analysis of Clinical Failures and Ongoing Efforts
The failure of the Passildas-Jahanmohan et al. trial is a pivotal learning point for the field. In this study, mCRPC patients received high-dose oral curcumin (6g/day) alongside docetaxel. Despite high compliance, the study was terminated early because the addition of curcumin showed no improvement in PSA response rates or overall survival compared to chemotherapy alone (42). This failure strongly suggests that simple oral supplementation, even at massive doses, is insufficient to achieve therapeutic concentrations in the prostate tumor microenvironment of advanced patients. It validates the need for advanced delivery systems (nanoparticles) rather than just "more powder."
The completed NCT02724618 trial using "Nanocurcumin" (a micellar formulation) in radiotherapy patients also failed to show a significant benefit in preventing radiation toxicity or improving biochemical progression-free survival (b-PFS) (43). "Nano-sizing" alone may not be a magic bullet. The formulation used (SinaCurcumin) acts as a micelle, but without active targeting or specific release mechanisms, it may still suffer from insufficient accumulation in the prostate gland relative to the bladder or rectum.
5.2. The Hope of Active Surveillance
The ongoing Phase III trial (NCT03769766) represents a strategic shift in the clinical application of these compounds. Rather than treating late-stage mCRPC (where the tumor burden is massive and resistance mechanisms are entrenched), this trial focuses on low-risk localized prostate cancer patients under active surveillance. In this setting, the goal is not rapid tumor shrinkage but rather prevention of progression. Curcumin's anti-inflammatory and cytostatic properties may be sufficient to keep indolent tumors in check, delaying the need for radical prostatectomy or radiation. If successful, this could establish a new standard of care for the "watch and wait" population, utilizing CPNs as a safe, long-term maintenance therapy.
The role of these nanoparticles in combination therapies also needs thorough investigation. Prostate cancer is often treated with a multi-modal approach, and understanding the synergistic or antagonistic interactions of curcumin and piperine nanoparticles with standard treatments like ADT, chemotherapy (e.g., docetaxel), or radiotherapy is vital. Preclinical studies combining curcumin with taxanes have shown synergistic cytotoxicity in sensitive PC3 cells, but clinical trials of curcumin with docetaxel have yielded mixed outcomes (44, 45), with one Phase II study in metastatic castration-resistant prostate cancer (mCRPC) patients showing no improvement in progression-free or overall survival when 6g/day of oral curcumin was added to docetaxel (42). For multiple drugs to exhibit synergism in vivo, it is crucial that they reach the tumor microenvironment simultaneously and in the appropriate synergistic dose ratios. While maintaining these ratios is relatively straightforward in vitro, achieving this scenario in vivo is notoriously challenging due to differences in drug solubility and biodistribution profiles. Nanoparticle-based co-delivery of drugs at synergistic dose ratios can synchronize pharmacokinetics, ensuring their simultaneous availability at the target site and in the precise concentrations required for synergistic efficacy. The authors of that study (24) also noted the need for improved formulations for in vivo synergism.
Finally, a key area of interest is the potential of these nanoformulations to overcome drug resistance, particularly in the context of CRPC, which represents an advanced and difficult-to-treat stage of the disease. Co-delivering multiple drugs with different molecular targets ensures that cancer cells are exposed to all agents at once. This simultaneous pressure not only makes it harder for cells to survive and evolve resistance but also reverse the acquired resistance. For instance, studies suggest that curcumin nanoparticles may help restore sensitivity to drugs like docetaxel (46, 47).
6. Critical Hurdles to Translation
The gap between preclinical success and clinical stagnation is not accidental. It is the result of specific, quantifiable hurdles that have yet to be fully addressed.
6.1. The Heterogeneity of the EPR Effect and Stromal Barriers
A fundamental weakness in the current CPN strategy is the over-reliance on the Enhanced Permeability and Retention (EPR) effect (Figure 3). The EPR effect posits that nanoparticles accumulate passively in tumors due to "leaky" blood vessels and poor lymphatic drainage (31). While the EPR effect is robust in rapidly growing murine xenografts, it is highly heterogeneous in human tumors. Clinical analyses show that the phenomenon is inconsistent, varying significantly between patients and even within different regions of the same tumor (48).
Prostate tumors are often characterized by desmoplasia, a dense, collagen-rich stromal matrix that creates high interstitial fluid pressure (IFP). This physical barrier actively resists the convective transport of nanoparticles from the blood vessel into the tumor mass (49). Consequently, passive nanoparticles often accumulate in the perivascular space, failing to penetrate deep into the tumor to reach the cancer cells. This limitation explains why formulations that work beautifully in nude mice often fail in human trials.
6.2. Safety and Tolerability: Piperine's Double-Edged Sword
Ensuring the safety and tolerability of any new therapeutic agent is paramount. While curcumin is "generally recognized as safe" (GRAS) by the FDA and has been used in clinical trials at high doses with minimal toxicity, in some cases high doses have been associated with gastrointestinal disturbances such as nausea and diarrhea. In rare cases, concerns about hepatotoxicity have also been raised, though these effects are not consistently observed (50). The addition of piperine introduces complex safety risks that are often underappreciated in the nutraceutical context but are critical in oncology. While nanoencapsulation strategies can minimize or even eliminate these side effects, they raise new questions about the long-term safety profile of the final pharmaceutical product: the curcumin- and piperine-loaded nanoparticles.
Another critical consideration is the potential for drug interactions. Prostate cancer patients, particularly those with advanced diseases or comorbidities, are often on multiple medications. Curcumin has been reported to potentially interact with cytochrome P450 enzymes or drug transporters, which could alter the pharmacokinetics and pharmacodynamics of co-administered drugs (51). Piperine acts as a bioenhancer by inhibiting CYP3A4 (the primary drug-metabolizing enzyme in the liver) and P-glycoprotein (P-gp, the efflux pump). While this boosts curcumin levels, it indiscriminately boosts the levels of other drugs metabolized by these pathways (Figure 4) (52, 53).
Preclinical studies demonstrate that co-administration of piperine with docetaxel in mice results in a 100% increase (doubling) of the docetaxel plasma Area Under the Curve (AUC) and a significant prolongation of its half-life (54). In humans, Physiologically Based Pharmacokinetic (PBPK) modeling predicts that a daily intake of just 20 mg of piperine can increase the Area Under the Curve (AUC) of CYP3A4 substrates (such as simvastatin, nifedipine, and cyclosporine) by 30% to 59% (52).
Prostate cancer patients are typically older men with comorbidities (cardiovascular disease, hypertension) who are on multiple medications. Furthermore, standard PC treatments like docetaxel and cabazitaxel are CYP3A4 substrates. Co-administration of piperine-containing nanoparticles could inadvertently cause taxane toxicity by inhibiting their clearance, leading to severe neutropenia or neuropathy (Figure 4). This drug-drug interaction (DDI) liability must be rigorously quantified in Phase I trials before combination therapies can be deemed safe.
The safety profiles of excipients and solvents used for nanoparticle preparation add another layer of complexity. Furthermore, the biodistribution of final nanoparticle formulations, their potential accumulation in healthy organs or tissues over time, and their clearance pathways must be thoroughly evaluated. The potential for inducing immunogenic reactions or inflammation should be extensively evaluated. The interaction of these nanosystems with various biological components, including proteins and cells of the immune system, needs careful characterization to avoid unintended adverse effects.
6.3. Pharmaceutical and Manufacturing Challenges (CMC)
Translating a promising nanoparticle formulation from a research laboratory to a clinical-grade product suitable for widespread use involves overcoming significant pharmaceutical and manufacturing hurdles. One of the main obstacles lies in the translational gap between lab-scale method development and large-scale manufacturing, particularly under the constraints of GMP compliance (55, 56). For a nanomedicine to be approved, it must be manufacturable at scale with extreme consistency. This Chemistry, Manufacturing, and Controls (CMC) aspect is often the downfall of academic formulations.
Additionally, unlike small molecule drugs, the efficacy and safety profiles of nanoparticles depend on their physicochemical properties such as size, surface chemistry (e.g., PEGylation to extend circulation time), and composition with a direct impact on biodistribution, clearance, and drug release patterns (57). Therefore, the physicochemical and structural properties of nanoparticles should be maintained during scale-up manufacturing. Consequently, it is crucial to adopt an economically viable, robust, and scalable manufacturing technique from the earliest stages of development to ensure consistent quality and reproducibility during large-scale production. Fine-tuning these characteristics to achieve optimal delivery to prostate tumor tissue while minimizing off-target effects is an ongoing process.
Traditional "beaker" methods of synthesis (e.g., bulk nanoprecipitation) are notoriously difficult to scale. They often suffer from batch-to-batch variability in particle size, polydispersity, and drug loading. Controlling particle size distribution effectively remains a challenge for some nanoformulations (58, 59). A deviation in size of just 50 nm can drastically alter the biodistribution and toxicity profile of the drug (10).
To overcome this, the field is moving toward microfluidic nanoprecipitation. Microfluidic devices use laminar flow in microscopic channels to mix solvents and anti-solvents with precise control over flow rates (FRR) and mixing times (Figure 5). Studies show that microfluidic synthesis can produce PLGA nanoparticles with a narrower size distribution (lower polydispersity index) and a 30% improvement in drug loading efficiency compared to bulk methods (60). This technology allows for the continuous production of high-quality nanoparticles that meet Good Manufacturing Practice (GMP) standards (61, 62).
Regulatory agencies like the FDA now expect a Quality by Design approach (63). This involves defining Critical Quality Attributes (CQAs), such as mean particle size (<200 nm), zeta potential, and encapsulation efficiency, and mapping them to Critical Process Parameters (CPPs) like mixing speed, temperature, and polymer concentration (64). Implementing QbD ensures that safety and efficacy are "built-in" to the product, rather than just tested at the end. The stability and shelf-life of nanoparticle formulations are also crucial. Nanoparticles must remain stable and retain their physicochemical characteristics and drug content under defined storage conditions for an acceptable period (65). This requires careful formulation development, lyophilization strategies, and stability testing (26). Quality control and standardization are non-negotiable for any pharmaceutical product. Robust analytical methods must be established to ensure batch-to-batch consistency in terms of critical quality attributes such as particle size, size distribution, surface charge, drug encapsulation efficiency, drug loading, and in vitro release profiles. Any variability in these parameters can significantly impact the in vivo performance and therapeutic outcome (66).
6.4. Regulatory Complexity and Translational Hurdles
Successfully navigating the complex regulatory landscape is a critical step in bringing any new drug, especially a novel nano-therapeutic, to market. Regulatory agencies like the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA) have specific guidelines and stringent requirements for the characterization, preclinical testing, and clinical evaluation of nanomedicines (67). Meeting these requirements demands comprehensive data packages demonstrating safety, efficacy, and manufacturing quality.
Nanosimilars and complex generics face a higher regulatory bar. Because CPNs contain two active ingredients (curcumin and piperine), they may be classified as fixed-dose combination products. This requires demonstrating the contribution of each component to the overall efficacy and safety, adding significant cost and complexity to the clinical trial design compared to a single-agent drug (9).
A thorough understanding of pharmacokinetics (PK) and pharmacodynamics (PD) in humans is essential. This includes characterizing the absorption, distribution, metabolism, and excretion (ADME) of both the nanoparticle carriers and the encapsulated curcumin and piperine. As previously noted, free curcumin suffers from rapid metabolism and poor absorption, and while nanoparticles aim to overcome this, their behavior in the human body needs to be fully elucidated through clinical PK/PD studies.
Effectively bridging the gap from promising preclinical data to tangible clinical efficacy in humans is a notorious challenge in drug development, often referred to as the valley of death. Many compounds that show remarkable activity in vitro cell cultures or animal models fail to deliver similar results in human clinical trials. This discrepancy can be due to species differences, the complexity of human disease, and the limitations of preclinical models in fully recapitulating the human tumor microenvironment. Most current studies on nanomedicines for prostate cancer, including those involving curcumin, are still in the preclinical phase, highlighting the long road ahead.
Finally, even with optimized formulations, there are inherent challenges in drug delivery to solid tumors like prostate cancer. These include tumor heterogeneity (different characteristics within the same tumor or between tumors in different patients), the presence of a complex and often immunosuppressive tumor microenvironment, poor vascularization in some tumor regions, and high interstitial fluid pressure, all of which can impede the efficient penetration and distribution of nanoparticles within the tumor mass.
7. Charting the Course Forward: Strategies to Overcome Hurdles
Addressing these multifaceted clinical hurdles requires a concerted and strategic approach, leveraging advancements in nanotechnology, personalized medicine, and collaborative research (68). If CPNs are to cross the bridge to clinical reality, the research strategy must evolve from "passive encapsulation" to "active engineering."
7.1. From Passive to Active Targeting
To bypass the limitations of the EPR effect and penetrate the stromal barrier, the next generation of CPNs must utilize active targeting. The field of nanomedicine is continuously evolving, offering opportunities for more sophisticated nanocarrier designs. The development of actively targeted nanoparticles is a key strategy. This involves functionalizing the nanoparticle surface with ligands, such as antibodies, aptamers, or peptides, that specifically bind to receptors overexpressed on prostate cancer cells, like prostate-specific membrane antigen (PSMA). Such active targeting could enhance drug accumulation in the tumor and reduce off-target toxicities.
Prostate-Specific Membrane Antigen (PSMA) is highly overexpressed on the surface of prostate cancer cells (particularly in metastatic disease) but absent on most normal tissues. Conjugating nanoparticles with ligands that bind to PSMA, such as the J591 antibody or small-molecule RNA aptamers, can facilitate receptor-mediated endocytosis. Preclinical studies have demonstrated that PSMA-targeted PLGA nanoparticles exhibit an 8-fold increase in cellular internalization compared to non-targeted counterparts in LNCaP cells (Figure 3). In vivo, this translates to significantly higher tumor accumulation and improved regression of xenografts (69). This shift from "drifting" to "homing" is essential for efficacy in human patients.
7.2. Stimuli-Responsive "Smart" Systems
Reducing systemic toxicity requires ensuring the drug is released only at the tumor site. A promising avenue is the development of stimuli-responsive nanoparticles. These smart carriers are designed to release their therapeutic payload (curcumin and piperine) specifically in response to internal or external stimuli characteristic of the tumor microenvironment (e.g., lower pH, specific enzymes, hypoxia) or applied externally (e.g., light, ultrasound, magnetic field) (70). "Smart" nanoparticles can be engineered to respond to the specific conditions of the tumor microenvironment (TME). Polymers that swell or degrade in the acidic pH of the tumor interstitium (pH 6.5) compared to healthy blood (pH 7.4). Linkers that are cleaved by enzymes overexpressed in PC, such as Matrix Metalloproteinases (MMPs) or Prostate-Specific Antigen (PSA) itself. This ensures the payload is dumped locally, sparing healthy organs (71).
7.3. Personalized Medicine and Biomarkers
The failure of "all-comer" trials suggests that patient selection is critical. Recognizing that prostate cancer is a heterogeneous disease, a one-size-fits-all approach is unlikely to be optimal. Utilizing genomic, proteomic, and metabolomic data from individual patients could help in tailoring treatments. The development of companion diagnostics or predictive biomarkers will be crucial to identify those patients who are most likely to benefit from curcumin and piperine nanoparticle therapy. This would not only improve efficacy but also spare non-responders from potentially ineffective treatment and unnecessary side effects.
Clinical trials should utilize biomarkers to select patients most likely to respond. For example, patients with tumors exhibiting high CYP17A1 expression (LNCaP-like) are candidates for the steroidogenic inhibition mechanism or PTEN loss; and patients with PTEN-null tumors (like PC3) may benefit most from CPNs due to the strong inhibitory effect on the PI3K/Akt pathway, given the specific molecular mechanisms of curcumin (72). Emerging omics technologies could identify patients whose tumors have downregulation of GPX4 or high iron loads, predicting sensitivity to curcumin-induced ferroptosis.
7.4. Collaborative Research Efforts:
Overcoming the complex challenges in translating nanomedicines from bench to bedside necessitates strong multidisciplinary collaborations. This includes fostering partnerships between academic researchers, clinicians specializing in prostate cancer, pharmaceutical industry experts with experience in drug development and manufacturing, and regulatory agencies. Open communication and data sharing within such consortia can accelerate progress and streamline the development pathway.
7.5. Focus on Early-Stage Disease and Prevention:
While much of the focus for novel cancer therapies is on advanced disease, there may also be a role for curcumin and piperine nanoparticles in preventing prostate cancer progression or as an adjunctive therapy in early-stage disease management. Given their generally favorable safety profile, these natural compounds, when effectively delivered, could be explored in settings such as active surveillance for low-risk prostate cancer, potentially delaying or preventing the need for more aggressive interventions.
8. Expert Opinion
The exploration of curcumin and piperine nanoparticles (CPNs) for prostate cancer occupies a precarious space between nutraceutical hype and rigorous pharmacological science. While preclinical data are unequivocally promising, demonstrating the ability to target multiple oncogenic pathways and overcome the inherent pharmacokinetic limitations of free curcumin, the translation to clinical reality remains fragile. To date, no CPN regimen has impacted real-world outcomes such as overall survival or progression-free survival in prostate cancer patients. The negative results from trials involving high-dose free curcumin serve as a sobering reminder that "natural" does not equate to "effective" in the hostile and complex environment of metastatic castration-resistant prostate cancer (mCRPC). However, the field is currently at a pivoted point. The shift from simple oral supplementation to sophisticated, standardized nanoformulations offers a legitimate second chance for these compounds, provided the research community addresses specific, entrenched weaknesses.
Weaknesses and The Trap of Passive Targeting The primary weakness in the current trajectory of CPN research is the over-reliance on the Enhanced Permeability and Retention (EPR) effect. For too long, the field has assumed that "nano-sizing" a drug automatically ensures its accumulation in the tumor. While the EPR effect is robust in rapid-growth murine xenograft models, it is highly heterogeneous in human prostate tumors. Prostate cancer is characterized by a "cold" tumor microenvironment with significant dense desmoplasia, collagen-rich stromal matrix that creates high interstitial fluid pressure. This physical barrier actively resists the convective transport of passive nanoparticles, causing them to accumulate in the perivascular space rather than penetrating deep into the tumor mass to reach the androgen-dependent cells. Continuing to push "passive" PLGA or liposomal formulations into clinical trials without addressing this stromal barrier is a strategy likely destined for failure. The solution lies in precision engineering: the field must move decisively toward ligand-targeted systems. The integration of Prostate-Specific Membrane Antigen (PSMA) ligands onto the surface of CPNs is not merely an enhancement; it is a prerequisite for overcoming the stromal transport barrier. PSMA-targeted carriers utilize receptor-mediated endocytosis to actively internalize the payload, bypassing the limitations of passive diffusion.
The Safety Paradox of Piperine A further critical hurdle that is frequently underappreciated is the safety profile of piperine in the context of combination therapy. In the nutraceutical sector, piperine is lauded as a "bioenhancer." However, in clinical oncology, this bioenhancement comes at a cost. Piperine achieves its effect largely by inhibiting CYP3A4 and P-glycoprotein. In an elderly prostate cancer population, where polypharmacy is the norm, this presents a severe risk of drug-drug interactions (DDIs). Standard-of-care agents such as docetaxel and cabazitaxel are sensitive CYP3A4 substrates (Figure 6). The co-administration of piperine-containing nanoparticles could inadvertently inhibit the clearance of these chemotherapies, leading to unpredictable and potentially fatal toxicities (e.g., severe neutropenia). Therefore, a key challenge that must be solved is the quantification of this risk. Before large-scale efficacy trials can ethically proceed, rigorous Phase I pharmacokinetic studies are required to map the interaction magnitude between CPNs and taxanes. It may be necessary to develop "piperine-free" nano-formulations that utilize alternative solubilization strategies (such as amorphous solid dispersions or nanocrystals) if the DDI risk proves unmanageable.
Manufacturing and Regulatory Complexity Technical limitations in manufacturing also prevent research from advancing as it could. The "Valley of Death" for nanomedicines often lies in the scale-up from the laboratory bench to the manufacturing plant. Many promising CPN formulations described in the literature are synthesized using bulk nanoprecipitation methods ("beaker chemistry") that are difficult to reproduce under Good Manufacturing Practice (GMP) standards. These methods often result in high batch-to-batch variability regarding particle size and drug loading. The regulatory agencies (FDA, EMA) now demand a Quality by Design (QbD) approach. The future of this field depends on the adoption of continuous manufacturing technologies, specifically microfluidic nanoprecipitation. Microfluidics allow for the precise control of mixing times and flow rates, producing nanoparticles with ultra-low polydispersity and consistent drug loading ratios. Without the implementation of these scalable technologies, CPNs will remain an academic curiosity, unable to meet the stringent CMC (Chemistry, Manufacturing, and Controls) requirements for a commercial pharmaceutical product.
Future Evolution and Ultimate Goals How will the field evolve in the future? In the next five to ten years, the standard procedure for advanced prostate cancer will likely not see CPNs replacing current anti-androgens (like enzalutamide) or taxanes. Instead, the future lies in the use of these "botanical nanomedicines" as chemosensitizers (Figure 6). The goal is to utilize CPNs to restore sensitivity to standard therapies. The mechanisms of curcumin specifically the downregulation of Bcl-2 and the induction of ferroptosis are perfectly poised to counteract the resistance mechanisms that tumors develop against docetaxel. Therefore, the future of study lies in the design of "combination nanomedicines," where curcumin is co-encapsulated with a chemotherapy drug in a single, ratiometric particle. This ensures that the sensitizer (curcumin) and the killer (chemotherapy) hit the cancer cell simultaneously and in the correct synergistic ratio, a feat impossible to achieve with separate oral administration. Furthermore, clinical application may shift towards earlier stages of the disease. The current "wait and watch" or active surveillance protocols for low-risk prostate cancer offer a unique window of opportunity. In this setting, the goal is prevention of progression rather than tumor debulking. Given the cytostatic and anti-inflammatory nature of curcumin, a daily, orally bioavailable CPN regimen could serve as a safe, long-term maintenance therapy to delay the need for radical prostatectomy or radiation. If ongoing trials in this specific population (e.g., NCT03769766) show positive results, this could redefine the standard of care for early-stage disease.
Conclusion In conclusion, the bridge to clinical reality for curcumin and piperine nanoparticles is currently under construction. It requires structural reinforcement in the form of active targeting to overcome stromal barriers, safety guardrails regarding piperine’s interactions, and a solid foundation of scalable, microfluidic manufacturing. If the research community can pivot from simply generating new formulations to rigorously addressing these specific translational hurdles, CPNs have the potential to evolve from a promising experimental concept into a valuable tool in the prostate cancer armamentarium.
9. Declarations
Funding: This manuscript was funded by CANCER RESEARCH SWITZERLAND grant number KFS-5557-02-2022 to A.V.P. J.Y. is partially funded by a SWISS GOVERNMENT EXCELLENCE SCHOLARSHIP (ESKAS) grant number 2022.0470. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declaration of Interests: The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Declaration of AI Use: The authors acknowledge the use of Gemini 3.0 (Google) during the preparation of this manuscript. This tool was used for the purpose of correcting language and grammar to improve the clarity and readability of the text. Additionally, Gemini 3.0 was used to assist in the preparation and design of the schematic figures presented in this work. The authors reviewed and edited all AI-generated content and take full responsibility for the integrity and accuracy of the final publication.
References
- Attard, G.; Parker, C.; A Eeles, R.; Schröder, F.; A Tomlins, S.; Tannock, I.; Drake, C.G.; de Bono, J.S. Prostate cancer. Lancet 2016, 387, 70–82. [Google Scholar] [CrossRef]
- Crowley, F.; Sterpi, M.; Buckley, C.; Margetich, L.; Handa, S.; Dovey, Z. A Review of the Pathophysiological Mechanisms Underlying Castration-resistant Prostate Cancer. Res. Rep. Urol. 2021, 13, 457–472. [Google Scholar] [CrossRef]
- Sharma, K.; Lanzilotto, A.; Yakubu, J.; Therkelsen, S.; Vöegel, C.D.; Du Toit, T.; Jørgensen, F.S.; Pandey, A.V. Effect of Essential Oil Components on the Activity of Steroidogenic Cytochrome P450. Biomolecules 2024, 14, 203. [Google Scholar] [CrossRef]
- Manap, A.S.A.; Tan, A.C.W.; Leong, W.H.; Chia, A.Y.Y.; Vijayabalan, S.; Arya, A.; Wong, E.H.; Rizwan, F.; Bindal, U.; Koshy, S.; et al. Synergistic Effects of Curcumin and Piperine as Potent Acetylcholine and Amyloidogenic Inhibitors With Significant Neuroprotective Activity in SH-SY5Y Cells via Computational Molecular Modeling and in vitro Assay. Front. Aging Neurosci. 2019, 11, 206. [Google Scholar] [CrossRef]
- Salehi, B.; Stojanović-Radić, Z.; Matejić, J.; Sharifi-Rad, M.; Anil Kumar, N.V.; Martins, N.; Sharifi-Rad, J. The therapeutic potential of curcumin: A review of clinical trials. Eur. J. Med. Chem. 2019, 163, 527–545. [Google Scholar] [CrossRef]
- Castaño, P.R.; Parween, S.; Pandey, A.V. Bioactivity of Curcumin on the Cytochrome P450 Enzymes of the Steroidogenic Pathway. Int. J. Mol. Sci. 2019, 20, 4606. [Google Scholar] [CrossRef]
- Yallapu, M.M.; Khan, S.; Maher, D.M.; Ebeling, M.C.; Sundram, V.; Chauhan, N.; Ganju, A.; Balakrishna, S.; Gupta, B.K.; Zafar, N.; et al. Anti-cancer activity of curcumin loaded nanoparticles in prostate cancer. Biomaterials 2014, 35, 8635–8648. [Google Scholar] [CrossRef]
- Hegde, M.; Girisa, S.; BharathwajChetty, B.; Vishwa, R.; Kunnumakkara, A.B. Curcumin Formulations for Better Bioavailability: What We Learned from Clinical Trials Thus Far? ACS Omega 2023, 8, 10713–10746. [Google Scholar] [CrossRef]
- Yakubu, J.; Pandey, A.V. Innovative Delivery Systems for Curcumin: Exploring Nanosized and Conventional Formulations. Pharmaceutics 2024, 16, 637. [Google Scholar] [CrossRef]
- Yakubu, J.; Natsaridis, E.; du Toit, T.; Barata, I.S.; Tagit, O.; Pandey, A.V. Nanoparticles with curcumin and piperine modulate steroid biosynthesis in prostate cancer. Sci. Rep. 2025, 15, 13613. [Google Scholar] [CrossRef]
- Pandey, A.V.; Miller, W.L. Regulation of 17,20 Lyase Activity by Cytochrome b5 and by Serine Phosphorylation of P450c17. J. Biol. Chem. 2005, 280, 13265–13271. [Google Scholar] [CrossRef]
- Miller, W.L.; Auchus, R.J. The Molecular Biology, Biochemistry, and Physiology of Human Steroidogenesis and Its Disorders. Endocr. Rev. 2011, 32, 81–151. [Google Scholar] [CrossRef]
- Akter, K.; Gul, K.; Mumtaz, S. Revisiting Curcumin in Cancer Therapy: Recent Insights into Molecular Mechanisms, Nanoformulations, and Synergistic Combinations. Curr. Issues Mol. Biol. 2025, 47, 716. [Google Scholar] [CrossRef]
- Zheng, X.; Liu, J.; Hu, W.; Jiang, B.; Zhou, X.; Zhang, M.; Song, M. Curcumin Induces Autophagy-mediated Ferroptosis by Targeting the PI3K/AKT/mTOR Signaling Pathway in Gastric Cancer. Turk. J. Gastroenterol. 2024, 35, 625–633. [Google Scholar] [CrossRef]
- Wróbel, T.M.; Grudzińska, A.; Yakubu, J.; du Toit, T.; Sharma, K.; Harrington, J.C.; Björkling, F.; Jørgensen, F.S.; Pandey, A.V. Pyridine indole hybrids as novel potent CYP17A1 inhibitors. J. Enzym. Inhib. Med. Chem. 2025, 40, 2463014. [Google Scholar] [CrossRef]
- Wróbel, T.M.; Sharma, K.; Mannella, I.; Oliaro-Bosso, S.; Nieckarz, P.; Du Toit, T.; Voegel, C.D.; Velazquez, M.N.R.; Yakubu, J.; Matveeva, A.; et al. Exploring the Potential of Sulfur Moieties in Compounds Inhibiting Steroidogenesis. Biomolecules 2023, 13, 1349. [Google Scholar] [CrossRef]
- Wróbel, T.M.; Jørgensen, F.S.; Pandey, A.V.; Grudzińska, A.; Sharma, K.; Yakubu, J.; Björkling, F. Non-steroidal CYP17A1 Inhibitors: Discovery and Assessment. J. Med. Chem. 2023, 66, 6542–6566. [Google Scholar] [CrossRef]
- Wróbel, T.M.; Rogova, O.; Sharma, K.; Velazquez, M.N.R.; Pandey, A.V.; Jørgensen, F.S.; Arendrup, F.S.; Andersen, K.L.; Björkling, F. Synthesis and Structure–Activity Relationships of Novel Non-Steroidal CYP17A1 Inhibitors as Potential Prostate Cancer Agents. Biomolecules 2022, 12, 165. [Google Scholar] [CrossRef]
- Martins, d.P.; Sanuelly, A.; Araújo, d.; Pimentel, O.R.; Gomes, A.d.S.; Araujo, F.L.C.; Júnior; Oliveira, J. ; Vasconcelos, d.; Gomes, J.K.; et al. Curcumin plus piperine improve body composition in patients with inflammatory bowel disease: a randomized, double-blind, placebo-controlled clinical trial. Eur. J. Nutr. 2025, 64, 90. [Google Scholar] [CrossRef]
- Danhier, F.; Ansorena, E.; Silva, J.M.; Coco, R.; Le Breton, A.; Préat, V. PLGA-based nanoparticles: An overview of biomedical applications. J. Control. Release 2012, 161, 505–522. [Google Scholar] [CrossRef]
- Seko, I.; Tonbul, H.; Tavukçuoğlu, E.; Şahin, A.; Akbas, S.; Yanık, H.; Öztürk, S.C.; Esendagli, G.; Khan, M.; Capan, Y. Development of curcumin and docetaxel co-loaded actively targeted PLGA nanoparticles to overcome blood brain barrier. J. Drug Deliv. Sci. Technol. 2021, 66, 102867. [Google Scholar] [CrossRef]
- Fonseca, C.; Simões, S.; Gaspar, R. Paclitaxel-loaded PLGA nanoparticles: preparation, physicochemical characterization and in vitro anti-tumoral activity. J. Control. Release 2002, 83, 273–286. [Google Scholar] [CrossRef]
- Puri, R.; Arora, V. Synergistic anticancer efficacy of optimized curcumin-piperine loaded magnetic nanoparticles for the treatment of colorectal cancer. Explor. Target. Anti-tumor Ther. 2025, 6, 1002340. [Google Scholar] [CrossRef]
- Imani, S.; Tagit, O.; Pichon, C. RETRACTED ARTICLE: Neoantigen vaccine nanoformulations based on Chemically synthesized minimal mRNA (CmRNA): small molecules, big impact. npj Vaccines 2024, 9, 14. [Google Scholar] [CrossRef]
- Yan, J.; Wang, Y.; Zhang, X.; Liu, S.; Tian, C.; Wang, H. Targeted nanomedicine for prostate cancer therapy: docetaxel and curcumin co-encapsulated lipid–polymer hybrid nanoparticles for the enhanced anti-tumor activityin vitroandin vivo. Drug Deliv. 2016, 23, 1757–1762. [Google Scholar] [CrossRef]
- Lazzari, S.; Moscatelli, D.; Codari, F.; Salmona, M.; Morbidelli, M.; Diomede, L. Colloidal stability of polymeric nanoparticles in biological fluids. J. Nanoparticle Res. 2012, 14, 920. [Google Scholar] [CrossRef]
- Shahbaz, S.K.; Koushki, K.; Sathyapalan, T.; Majeed, M.; Sahebkar, A. PLGA-Based Curcumin Delivery System: An Interesting Therapeutic Approach in the Treatment of Alzheimer’s Disease. Curr. Neuropharmacol. 2022, 20, 309–323. [Google Scholar] [CrossRef]
- Del Prado-Audelo, M.L.; Caballero-Florán, I.H.; Meza-Toledo, J.A.; Mendoza-Muñoz, N.; González-Torres, M.; Florán, B.; Cortés, H.; Leyva-Gómez, G. Formulations of Curcumin Nanoparticles for Brain Diseases. Biomolecules 2019, 9, 56. [Google Scholar] [CrossRef]
- Yallapu, M.M.; Nagesh, P.K.B.; Jaggi, M.; Chauhan, S.C. Therapeutic Applications of Curcumin Nanoformulations. AAPS J. 2015, 17, 1341–1356. [Google Scholar] [CrossRef]
- Yallapu, M.M.; Jaggi, M.; Chauhan, S.C. Curcumin nanoformulations: a future nanomedicine for cancer. Drug Discov. Today 2012, 17, 71–80. [Google Scholar] [CrossRef]
- Nakamura, Y.; Mochida, A.; Choyke, P.L.; Kobayashi, H. Nanodrug Delivery: Is the Enhanced Permeability and Retention Effect Sufficient for Curing Cancer? Bioconjug. Chem. 2016, 27, 2225–2238. [Google Scholar] [CrossRef]
- Saralkar, P.; Dash, A.K. Alginate Nanoparticles Containing Curcumin and Resveratrol: Preparation, Characterization, and In Vitro Evaluation Against DU145 Prostate Cancer Cell Line. AAPS PharmSciTech 2017, 18, 2814–2823. [Google Scholar] [CrossRef]
- Narayanan, N.K.; Nargi, D.; Randolph, C.; Narayanan, B.A. Liposome encapsulation of curcumin and resveratrol in combination reduces prostate cancer incidence in PTEN knockout mice. Int. J. Cancer 2009, 125, 1–8. [Google Scholar] [CrossRef]
- Su, C.-Y.; Huang, G.-C.; Chang, Y.-C.; Chen, Y.-J.; Fang, H.-W. Analyzing the Expression of Biomarkers in Prostate Cancer Cell Lines. Vivo 2021, 35, 1545–1548. [Google Scholar] [CrossRef]
- Abate-Shen, C.; de Almeida, F.N. Establishment of the LNCaP Cell Line – The Dawn of an Era for Prostate Cancer Research. Cancer Res. 2022, 82, 1689–1691. [Google Scholar] [CrossRef]
- Seim, I.; Jeffery, P.L.; Thomas, P.B.; Nelson, C.C.; Chopin, L.K. Whole-Genome Sequence of the Metastatic PC3 and LNCaP Human Prostate Cancer Cell Lines. G3 Genes|Genomes|Genetics 2017, 7, 1731–1741. [Google Scholar] [CrossRef]
- Ravenna, L.; Principessa, L.; Verdina, A.; Salvatori, L.; Russo, M.A.; Petrangeli, E. Distinct Phenotypes of Human Prostate Cancer Cells Associate with Different Adaptation to Hypoxia and Pro-Inflammatory Gene Expression. PLOS ONE 2014, 9, e96250. [Google Scholar] [CrossRef]
- Bolat, Z.B.; Islek, Z.; Demir, B.N.; Yilmaz, E.N.; Sahin, F.; Ucisik, M.H. Curcumin- and Piperine-Loaded Emulsomes as Combinational Treatment Approach Enhance the Anticancer Activity of Curcumin on HCT116 Colorectal Cancer Model. Front. Bioeng. Biotechnol. 2020, 8, 50. [Google Scholar] [CrossRef]
- Soni, T.P.; Gupta, A.K.; Sharma, L.M.; Singhal, H.; Sharma, S.; Gothwal, R.S. A Randomized, Placebo-Controlled Study to Evaluate the Effect of Bio-Enhanced Turmeric Formulation on Radiation-Induced Oral Mucositis. ORL 2021, 84, 103–113. [Google Scholar] [CrossRef]
- Choi, Y.H.; Han, D.H.; Kim, S.; Kim, M.; Sung, H.H.; Jeon, H.G.; Jeong, B.C.; Seo, S.I.; Jeon, S.S.; Lee, H.M.; et al. A randomized, double-blind, placebo-controlled trial to evaluate the role of curcumin in prostate cancer patients with intermittent androgen deprivation. Prostate 2019, 79, 614–621. [Google Scholar] [CrossRef]
- Barber-Chamoux, N.; Milenkovic, D.; Verny, M.; Habauzit, V.; Pereira, B.; Lambert, C.; Richard, D.; Boby, C.; Mazur, A.; Lusson, J.R.; et al. Substantial Variability Across Individuals in the Vascular and Nutrigenomic Response to an Acute Intake of Curcumin: A Randomized Controlled Trial. Mol. Nutr. Food Res. 2018, 62. [Google Scholar] [CrossRef] [PubMed]
- Passildas-Jahanmohan, J.; Eymard, J.-C.; Pouget, M.; Kwiatkowski, F.; Van Praagh, I.; Savareux, L.; Atger, M.; Durando, X.; Abrial, C.; Richard, D.; et al. Multicenter randomized phase II study comparing docetaxel plus curcumin versus docetaxel plus placebo in first-line treatment of metastatic castration-resistant prostate cancer. Cancer Med. 2021, 10, 2332–2340. [Google Scholar] [CrossRef]
- Saadipoor, A.; Razzaghdoust, A.; Simforoosh, N.; Mahdavi, A.; Bakhshandeh, M.; Moghadam, M.; Abdollahi, H.; Mofid, B. Randomized, double-blind, placebo-controlled phase II trial of nanocurcumin in prostate cancer patients undergoing radiotherapy. Phytotherapy Res. 2019, 33, 370–378. [Google Scholar] [CrossRef]
- Judith, P.J.; Maureen, B.; Mélanie, P.; Fabrice, K.; Isabelle, V.; Pascale, D.; Catherine, A.; Jean-Marc, N.; Hervé, C.; Valérie, D.; et al. Curcumin's effect in advanced and metastatic breast cancer patients treated with first or second-line docetaxel: A randomized trial. Heal. Sci. Rep. 2024, 7, e70052. [Google Scholar] [CrossRef] [PubMed]
- Bayet-Robert, M.; Kwiatowski, F.; Leheurteur, M.; Gachon, F.; Planchat, E.; Abrial, C.; Mouret-Reynier, M.-A.; Durando, X.; Barthomeuf, C.; Chollet, P. Phase I dose escalation trial of docetaxel plus curcumin in patients with advanced and metastatic breast cancer. Cancer Biol. Ther. 2010, 9, 8–14. [Google Scholar] [CrossRef]
- Di Francesco, M.; Pastorino, F.; Ferreira, M.; Fragassi, A.; Di Francesco, V.; Palange, A.L.; Celia, C.; Di Marzio, L.; Cilli, M.; Bensa, V.; et al. Augmented efficacy of nano-formulated docetaxel plus curcumin in orthotopic models of neuroblastoma. Pharmacol. Res. 2023, 188, 106639. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.H.; Kim, B.D.; Lee, T.H.; Kim, H.K.; Lyu, M.J.; Yoon, Y.I.; Goo, Y.T.; Kang, M.J.; Lee, S.; Choi, Y.W. Synergistic co-administration of docetaxel and curcumin to chemoresistant cancer cells using PEGylated and RIPL peptide-conjugated nanostructured lipid carriers. Cancer Nanotechnol. 2022, 13, 1–26. [Google Scholar] [CrossRef]
- Subhan, A.; Parveen, F.; Filipczak, N.; Yalamarty, S.S.K.; Torchilin, V.P. Approaches to Improve EPR-Based Drug Delivery for Cancer Therapy and Diagnosis. J. Pers. Med. 2023, 13, 389. [Google Scholar] [CrossRef]
- Golombek, S.K.; May, J.-N.; Theek, B.; Appold, L.; Drude, N.; Kiessling, F.; Lammers, T. Tumor targeting via EPR: Strategies to enhance patient responses. Adv. Drug Deliv. Rev. 2018, 130, 17–38. [Google Scholar] [CrossRef]
- Halegoua-DeMarzio, D.; Navarro, V.; Ahmad, J.; Avula, B.; Barnhart, H.; Barritt, A.S.; Bonkovsky, H.L.; Fontana, R.J.; Ghabril, M.S.; Hoofnagle, J.H.; et al. Liver Injury Associated with Turmeric—A Growing Problem: Ten Cases from the Drug-Induced Liver Injury Network [DILIN]. Am. J. Med. 2023, 136, 200–206. [Google Scholar] [CrossRef]
- Zhang, W.; Tan, T.M.C.; Lim, L.-Y. Impact of Curcumin-Induced Changes in P-Glycoprotein and CYP3A Expression on the Pharmacokinetics of Peroral Celiprolol and Midazolam in Rats. Drug Metab. Dispos. 2007, 35, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.; Hu, Y.; Zhang, Y.; Zhao, L.; Zhong, D.; Liu, J. Predicting Food–Drug Interactions between Piperine and CYP3A4 Substrate Drugs Using PBPK Modeling. Int. J. Mol. Sci. 2024, 25, 10955. [Google Scholar] [CrossRef]
- Bhardwaj, R.K.; Glaeser, H.; Becquemont, L.; Klotz, U.; Gupta, S.K.; Fromm, M.F. Piperine, a Major Constituent of Black Pepper, Inhibits Human P-glycoprotein and CYP3A4. J. Pharmacol. Exp. Ther. 2002, 302, 645–650. [Google Scholar] [CrossRef]
- Makhov, P.; Golovine, K.; Canter, D.; Kutikov, A.; Simhan, J.; Corlew, M.M.; Uzzo, R.G.; Kolenko, V.M. Co-administration of piperine and docetaxel results in improved anti-tumor efficacy via inhibition of CYP3A4 activity. Prostate 2012, 72, 661–667. [Google Scholar] [CrossRef]
- Operti, M.C.; Bernhardt, A.; Pots, J.; Sincari, V.; Jager, E.; Grimm, S.; Engel, A.; Benedikt, A.; Hrubý, M.; De Vries, I.J.M.; et al. Translating the Manufacture of Immunotherapeutic PLGA Nanoparticles from Lab to Industrial Scale: Process Transfer and In Vitro Testing. Pharmaceutics 2022, 14, 1690. [Google Scholar] [CrossRef]
- Operti, M.C.; Bernhardt, A.; Grimm, S.; Engel, A.; Figdor, C.G.; Tagit, O. PLGA-based nanomedicines manufacturing: Technologies overview and challenges in industrial scale-up. Int. J. Pharm. 2021, 605, 120807. [Google Scholar] [CrossRef] [PubMed]
- Operti, M.C.; Dölen, Y.; Keulen, J.; van Dinther, E.A.W.; Figdor, C.G.; Tagit, O. Microfluidics-Assisted Size Tuning and Biological Evaluation of PLGA Particles. Pharmaceutics 2019, 11, 590. [Google Scholar] [CrossRef]
- Öztürk, K.; Kaplan, M.; Çalış, S. Effects of nanoparticle size, shape, and zeta potential on drug delivery. Int. J. Pharm. 2024, 666, 124799. [Google Scholar] [CrossRef]
- Zhu, M.; Nie, G.; Meng, H.; Xia, T.; Nel, A.; Zhao, Y. Physicochemical Properties Determine Nanomaterial Cellular Uptake, Transport, and Fate. Accounts Chem. Res. 2013, 46, 622–631. [Google Scholar] [CrossRef] [PubMed]
- Lababidi, N.; Sigal, V.; Koenneke, A.; Schwarzkopf, K.; Manz, A.; Schneider, M. Microfluidics as tool to prepare size-tunable PLGA nanoparticles with high curcumin encapsulation for efficient mucus penetration. Beilstein J. Nanotechnol. 2019, 10, 2280–2293. [Google Scholar] [CrossRef] [PubMed]
- Fattahi, A.; Shokoohinia, P.; Hajialyani, M.; Sadrjavadi, K.; Akbari, M.; Rahimi, M.; Khaledian, S. Microfluidic-assisted preparation of PLGA nanoparticles for drug delivery purposes: experimental study and computational fluid dynamic simulation. Res. Pharm. Sci. 2019, 14, 459–470. [Google Scholar] [CrossRef]
- Liu, Y.; Yang, G.; Hui, Y.; Ranaweera, S.; Zhao, C. Microfluidic Nanoparticles for Drug Delivery. Small 2022, 18, e2106580. [Google Scholar] [CrossRef] [PubMed]
- Alshaer, W.; Nsairat, H.; Lafi, Z.; Hourani, O.M.; Al-Kadash, A.; Esawi, E.; Alkilany, A.M. Quality by Design Approach in Liposomal Formulations: Robust Product Development. Molecules 2023, 28, 10. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Kong, X.; Chen, H.; Lu, M.; Liu, X.; Wang, L. Optimization of Laponite Nanogel with Curcumin Incorporation: A Quality by Design Approach. Gels 2025, 11, 677. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Zhang, J.; Watanabe, W. Physical and chemical stability of drug nanoparticles. Adv. Drug Deliv. Rev. 2011, 63, 456–469. [Google Scholar] [CrossRef]
- Rodríguez-Gómez, F.D.; Monferrer, D.; Penon, O.; Rivera-Gil, P. Regulatory pathways and guidelines for nanotechnology-enabled health products: a comparative review of EU and US frameworks. Front. Med. 2025, 12, 1544393. [Google Scholar] [CrossRef]
- Foulkes, R.; Man, E.; Thind, J.; Yeung, S.; Joy, A.; Hoskins, C. The regulation of nanomaterials and nanomedicines for clinical application: current and future perspectives. Biomater. Sci. 2020, 8, 4653–4664. [Google Scholar] [CrossRef]
- Baby, T.; Liu, Y.; Yang, G.; Chen, D.; Zhao, C.-X. Microfluidic synthesis of curcumin loaded polymer nanoparticles with tunable drug loading and pH-triggered release. J. Colloid Interface Sci. 2021, 594, 474–484. [Google Scholar] [CrossRef]
- Esmaeli, M.; Dehabadi, M.D. Curcumin in prostate cancer: a systematic review of molecular mechanisms and nanoformulated therapeutic strategies. BMC Cancer 2025, 25, 1609. [Google Scholar] [CrossRef] [PubMed]
- Nikoletić, A.; Maleković, M.; Kozalak, G.; Palivan, C.G.; Tagit, O. Thermoresponsive Nanocarriers Transduced by Inorganic Nanoparticles: Design Considerations and Applications in Drug Delivery. Helvetica Chim. Acta 2025, 108, e202400193. [Google Scholar] [CrossRef]
- Bevacqua, E.; Curcio, M.; Saletta, F.; Vittorio, O.; Cirillo, G.; Tucci, P. Dextran-Curcumin Nanosystems Inhibit Cell Growth and Migration Regulating the Epithelial to Mesenchymal Transition in Prostate Cancer Cells. Int. J. Mol. Sci. 2021, 22, 7013. [Google Scholar] [CrossRef] [PubMed]
- Sienkiewicz, K.; Yang, C.; Paschal, B.M.; Ratan, A. Genomic analyses of the metastasis-derived prostate cancer cell lines LNCaP, VCaP, and PC3-AR. Prostate 2022, 82, 442–451. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The Dual-Mechanism Blockade of Androgen Biosynthesis by Curcumin-Piperine Nanoparticles (CPNs). Schematic representation of the steroidogenic pathway within the endoplasmic reticulum of prostate cancer cells. Cholesterol is converted sequentially into active androgens (Testosterone and Dihydrotestosterone). The enzyme CYP17A1 serves as a critical gatekeeper, possessing both 17α-hydroxylase and 17,20-lyase activities required for the synthesis of androstenedione from pregnenolone/progesterone. In the untreated state, upregulated CYP17A1 drives intratumoral androgen synthesis, fueling Androgen Receptor (AR) signaling. Treatment with CPNs results in the direct inhibition of CYP17A1 enzymatic activity. Curcumin occupies the active site, blocking substrate conversion, while piperine inhibits the efflux of curcumin, maintaining high intracellular inhibitory concentrations. The downstream effect is a depletion of AR ligands and suppression of tumor cell proliferation.
Figure 1.
The Dual-Mechanism Blockade of Androgen Biosynthesis by Curcumin-Piperine Nanoparticles (CPNs). Schematic representation of the steroidogenic pathway within the endoplasmic reticulum of prostate cancer cells. Cholesterol is converted sequentially into active androgens (Testosterone and Dihydrotestosterone). The enzyme CYP17A1 serves as a critical gatekeeper, possessing both 17α-hydroxylase and 17,20-lyase activities required for the synthesis of androstenedione from pregnenolone/progesterone. In the untreated state, upregulated CYP17A1 drives intratumoral androgen synthesis, fueling Androgen Receptor (AR) signaling. Treatment with CPNs results in the direct inhibition of CYP17A1 enzymatic activity. Curcumin occupies the active site, blocking substrate conversion, while piperine inhibits the efflux of curcumin, maintaining high intracellular inhibitory concentrations. The downstream effect is a depletion of AR ligands and suppression of tumor cell proliferation.
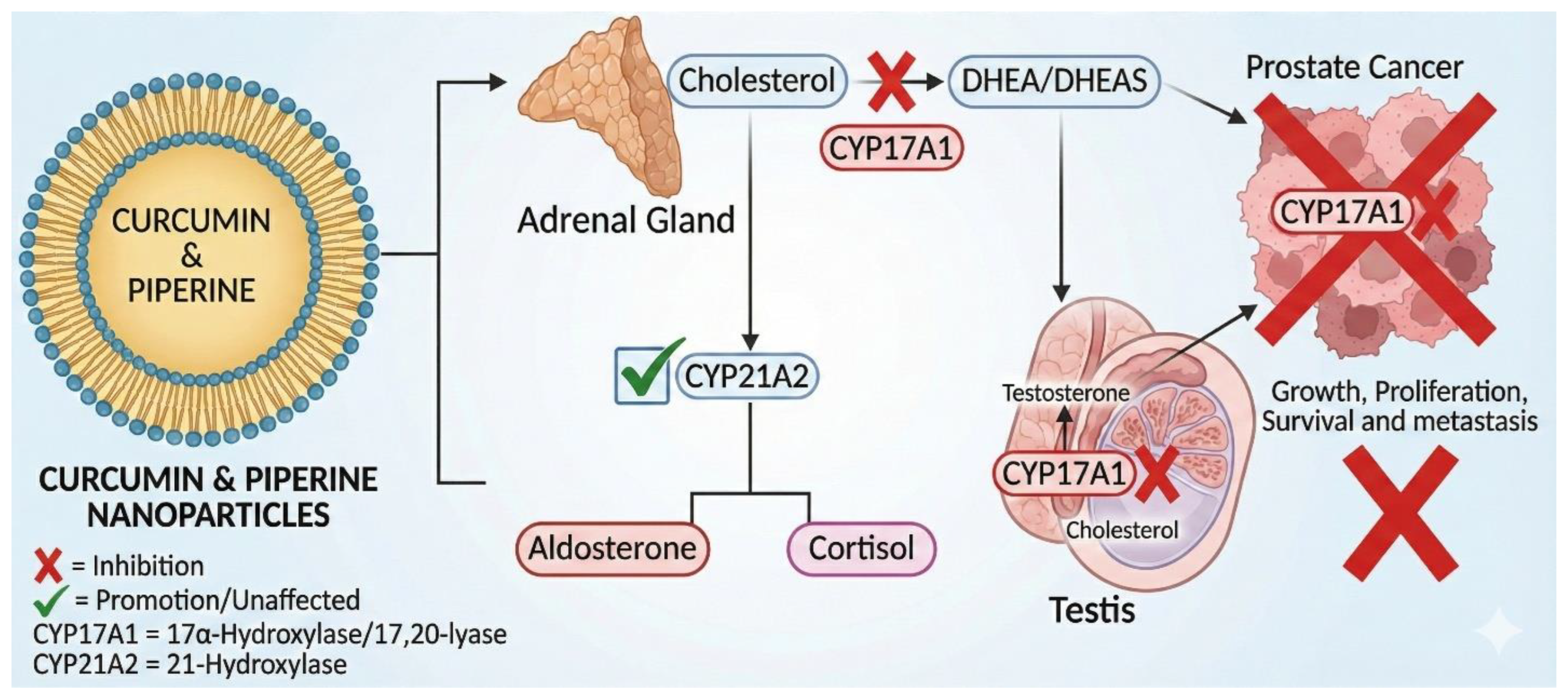
Figure 2.
The integrated mechanisms by which curcumin–piperine nanoparticles (CPNs) inhibit prostate cancer beyond CYP17A1 suppression. (1) The Engine: Curcumin accumulates in the endoplasmic reticulum and inhibits CYP17A1, reducing androgen synthesis. (2) The Shield: Piperine blocks P-gp efflux pumps at the plasma membrane, preventing curcumin expulsion and increasing intracellular drug retention. (3) The Survival Signal: Curcumin inhibits phosphorylation of Akt and mTOR, downregulating pro-survival signaling pathways. (4) The Kill Switch: CPNs deplete GPX4, resulting in lipid peroxide buildup and subsequent ferroptosis. Together, these pathways form a coordinated, multi-node mechanism of prostate cancer cell inhibition.
Figure 2.
The integrated mechanisms by which curcumin–piperine nanoparticles (CPNs) inhibit prostate cancer beyond CYP17A1 suppression. (1) The Engine: Curcumin accumulates in the endoplasmic reticulum and inhibits CYP17A1, reducing androgen synthesis. (2) The Shield: Piperine blocks P-gp efflux pumps at the plasma membrane, preventing curcumin expulsion and increasing intracellular drug retention. (3) The Survival Signal: Curcumin inhibits phosphorylation of Akt and mTOR, downregulating pro-survival signaling pathways. (4) The Kill Switch: CPNs deplete GPX4, resulting in lipid peroxide buildup and subsequent ferroptosis. Together, these pathways form a coordinated, multi-node mechanism of prostate cancer cell inhibition.
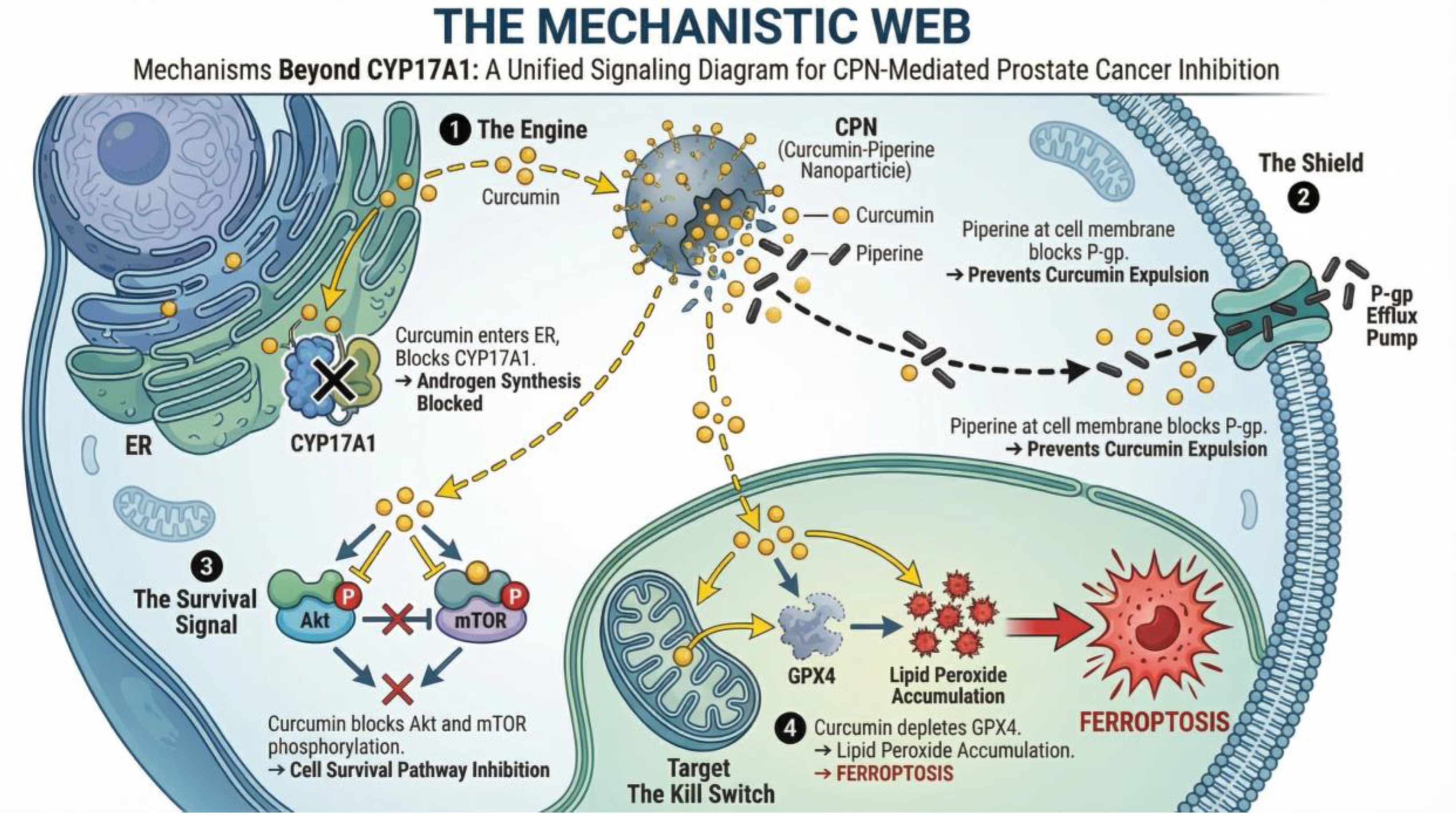
Figure 3.
Overcoming the Stromal Barrier: Passive vs. Active Targeting in Prostate Cancer. Comparison of nanoparticle transport mechanisms within the desmoplastic prostate tumor microenvironment. Conventional nanoparticles rely on the Enhanced Permeability and Retention (EPR) effect. While they extravasate through leaky tumor vasculature, their penetration is severely restricted by the dense collagen-rich stroma and high interstitial fluid pressure (IFP), leading to perivascular sequestration without reaching the tumor core. Nanoparticles functionalized with ligands targeting the Prostate-Specific Membrane Antigen (PSMA) utilize biochemical affinity to overcome physical barriers. These targeted carriers bind specifically to PSMA receptors overexpressed on PC cells, triggering receptor-mediated endocytosis. This active uptake mechanism facilitates the intracellular delivery of the payload, bypassing stromal entrapment and ensuring higher drug concentrations within the malignant cells.
Figure 3.
Overcoming the Stromal Barrier: Passive vs. Active Targeting in Prostate Cancer. Comparison of nanoparticle transport mechanisms within the desmoplastic prostate tumor microenvironment. Conventional nanoparticles rely on the Enhanced Permeability and Retention (EPR) effect. While they extravasate through leaky tumor vasculature, their penetration is severely restricted by the dense collagen-rich stroma and high interstitial fluid pressure (IFP), leading to perivascular sequestration without reaching the tumor core. Nanoparticles functionalized with ligands targeting the Prostate-Specific Membrane Antigen (PSMA) utilize biochemical affinity to overcome physical barriers. These targeted carriers bind specifically to PSMA receptors overexpressed on PC cells, triggering receptor-mediated endocytosis. This active uptake mechanism facilitates the intracellular delivery of the payload, bypassing stromal entrapment and ensuring higher drug concentrations within the malignant cells.
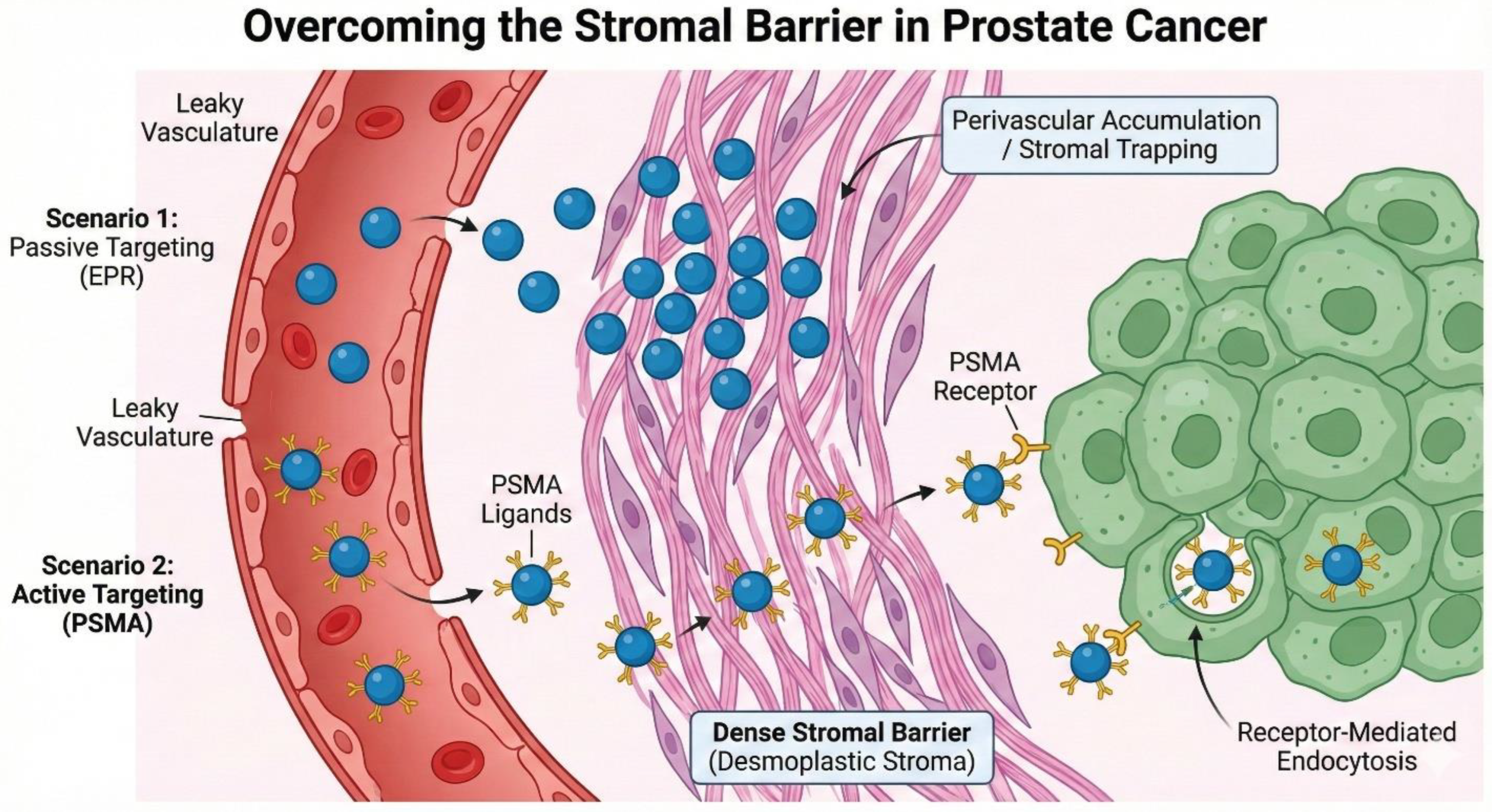
Figure 4.
Mechanistic Basis of Piperine-Taxane Drug-Drug Interactions (DDIs). Schematic illustration of the "Double-Edged Sword" of bioenhancement. (A) Under normal physiological conditions, taxane chemotherapies (e.g., Docetaxel, Cabazitaxel) are extensively metabolized by hepatic CYP3A4 enzymes and actively effluxed by P-glycoprotein (P-gp) transporters, limiting systemic toxicity. (B) The co-administration of piperine results in the dual blockade of these clearance pathways. Piperine acts as a potent inhibitor of both CYP3A4 and P-gp. This inhibition leads to a significant reduction in taxane clearance, causing supra-therapeutic accumulation of the chemotherapy agent in the plasma (increased AUC). While this may enhance tumor killing, it significantly elevates the risk of dose-limiting toxicities such as severe neutropenia and peripheral neuropathy, necessitating strict pharmacokinetic monitoring during combination therapy.
Figure 4.
Mechanistic Basis of Piperine-Taxane Drug-Drug Interactions (DDIs). Schematic illustration of the "Double-Edged Sword" of bioenhancement. (A) Under normal physiological conditions, taxane chemotherapies (e.g., Docetaxel, Cabazitaxel) are extensively metabolized by hepatic CYP3A4 enzymes and actively effluxed by P-glycoprotein (P-gp) transporters, limiting systemic toxicity. (B) The co-administration of piperine results in the dual blockade of these clearance pathways. Piperine acts as a potent inhibitor of both CYP3A4 and P-gp. This inhibition leads to a significant reduction in taxane clearance, causing supra-therapeutic accumulation of the chemotherapy agent in the plasma (increased AUC). While this may enhance tumor killing, it significantly elevates the risk of dose-limiting toxicities such as severe neutropenia and peripheral neuropathy, necessitating strict pharmacokinetic monitoring during combination therapy.
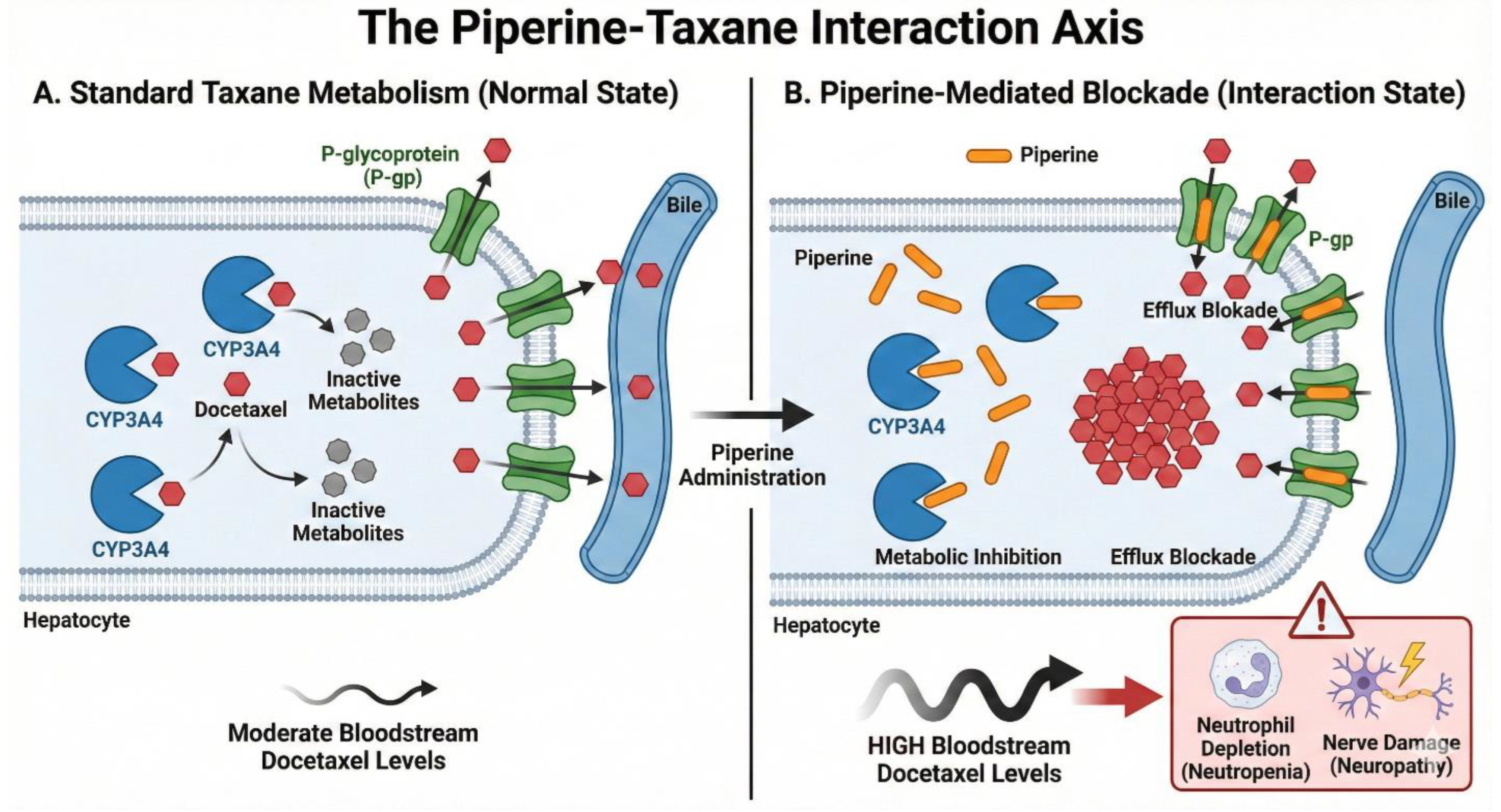
Figure 5.
The traditional bulk “beaker-based” synthesis with microfluidic, Quality-by-Design (QbD)–guided nanoparticle manufacturing. Bulk Synthesis: Mixing reactants and solvents in a batch reactor produces polydisperse particles with high batch-to-batch variability. Microfluidic Synthesis: Controlled mixing of organic (drug/polymer) and aqueous phases within microchannels allows precise regulation of critical process parameters (flow rate, phase ratio), enabling production of uniform, monodisperse nanoparticles (size <200 nm; PDI <0.2). The QbD framework ensures reproducibility, consistency, and predictable nanoparticle quality.
Figure 5.
The traditional bulk “beaker-based” synthesis with microfluidic, Quality-by-Design (QbD)–guided nanoparticle manufacturing. Bulk Synthesis: Mixing reactants and solvents in a batch reactor produces polydisperse particles with high batch-to-batch variability. Microfluidic Synthesis: Controlled mixing of organic (drug/polymer) and aqueous phases within microchannels allows precise regulation of critical process parameters (flow rate, phase ratio), enabling production of uniform, monodisperse nanoparticles (size <200 nm; PDI <0.2). The QbD framework ensures reproducibility, consistency, and predictable nanoparticle quality.
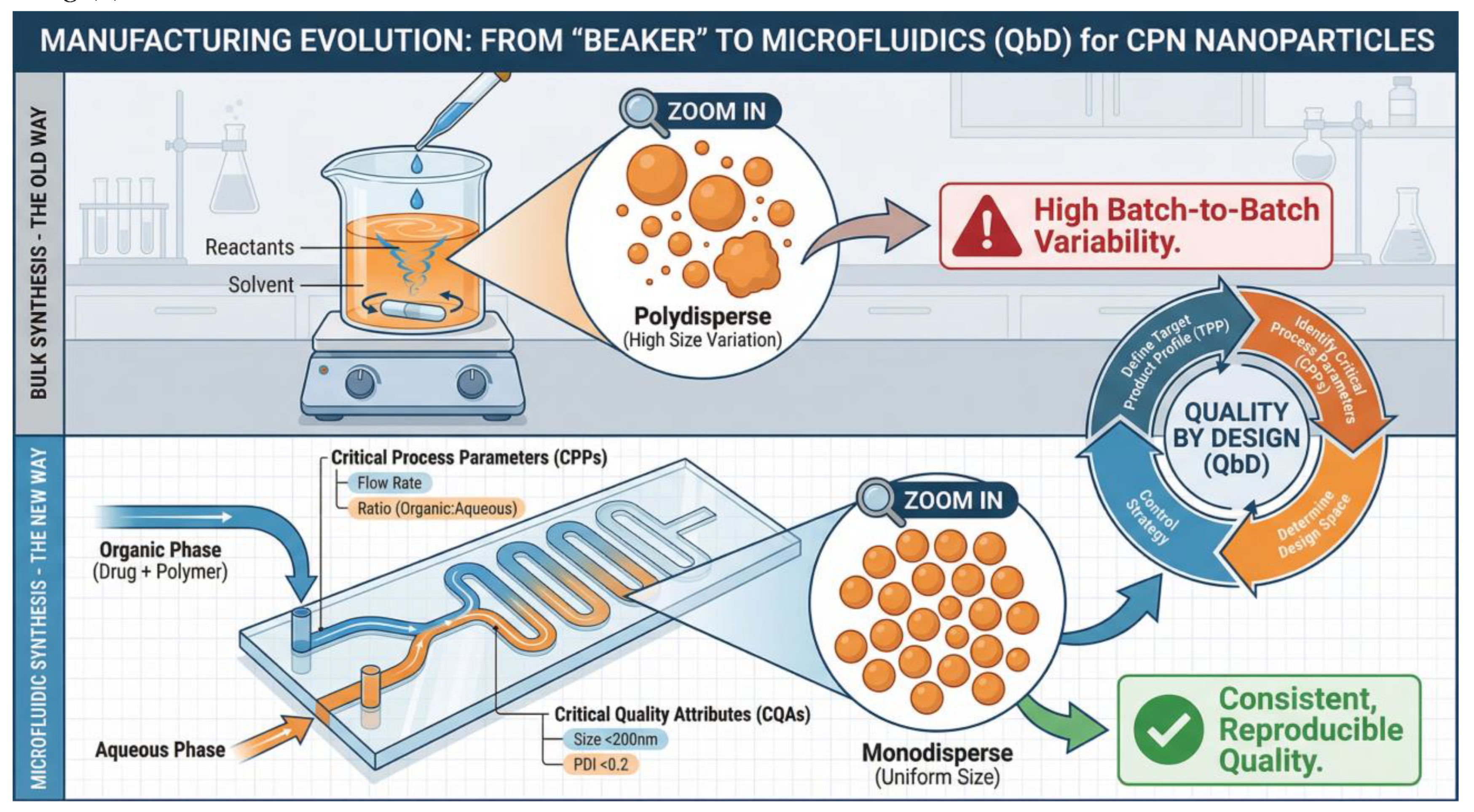
Figure 6.
The "Sensitize-then-Kill" Paradigm: Ratiometric Co-Delivery of Chemotherapy and Chemosensitizers. Design concept for a next-generation "Combination Nanomedicine" aimed at reversing drug resistance in mCRPC. The nanoparticle is engineered to encapsulate both a chemosensitizer (Curcumin/Piperine) and a cytotoxic agent (Docetaxel) at a precise, synergistic molar ratio. Upon cellular internalization, the formulation is designed to rapidly release the sensitizers (Curcumin/Piperine). These agents inhibit efflux pumps (P-gp), downregulate anti-apoptotic proteins (Bcl-2), and suppress survival signaling (PI3K/Akt), effectively "disarming" the cancer cell's defenses. The subsequent release of the cytotoxic payload (Docetaxel) strikes the sensitized cell, maximizing apoptotic death and preventing the emergence of resistant clones. This temporal and spatial synchronization is unachievable with separate oral administration.
Figure 6.
The "Sensitize-then-Kill" Paradigm: Ratiometric Co-Delivery of Chemotherapy and Chemosensitizers. Design concept for a next-generation "Combination Nanomedicine" aimed at reversing drug resistance in mCRPC. The nanoparticle is engineered to encapsulate both a chemosensitizer (Curcumin/Piperine) and a cytotoxic agent (Docetaxel) at a precise, synergistic molar ratio. Upon cellular internalization, the formulation is designed to rapidly release the sensitizers (Curcumin/Piperine). These agents inhibit efflux pumps (P-gp), downregulate anti-apoptotic proteins (Bcl-2), and suppress survival signaling (PI3K/Akt), effectively "disarming" the cancer cell's defenses. The subsequent release of the cytotoxic payload (Docetaxel) strikes the sensitized cell, maximizing apoptotic death and preventing the emergence of resistant clones. This temporal and spatial synchronization is unachievable with separate oral administration.
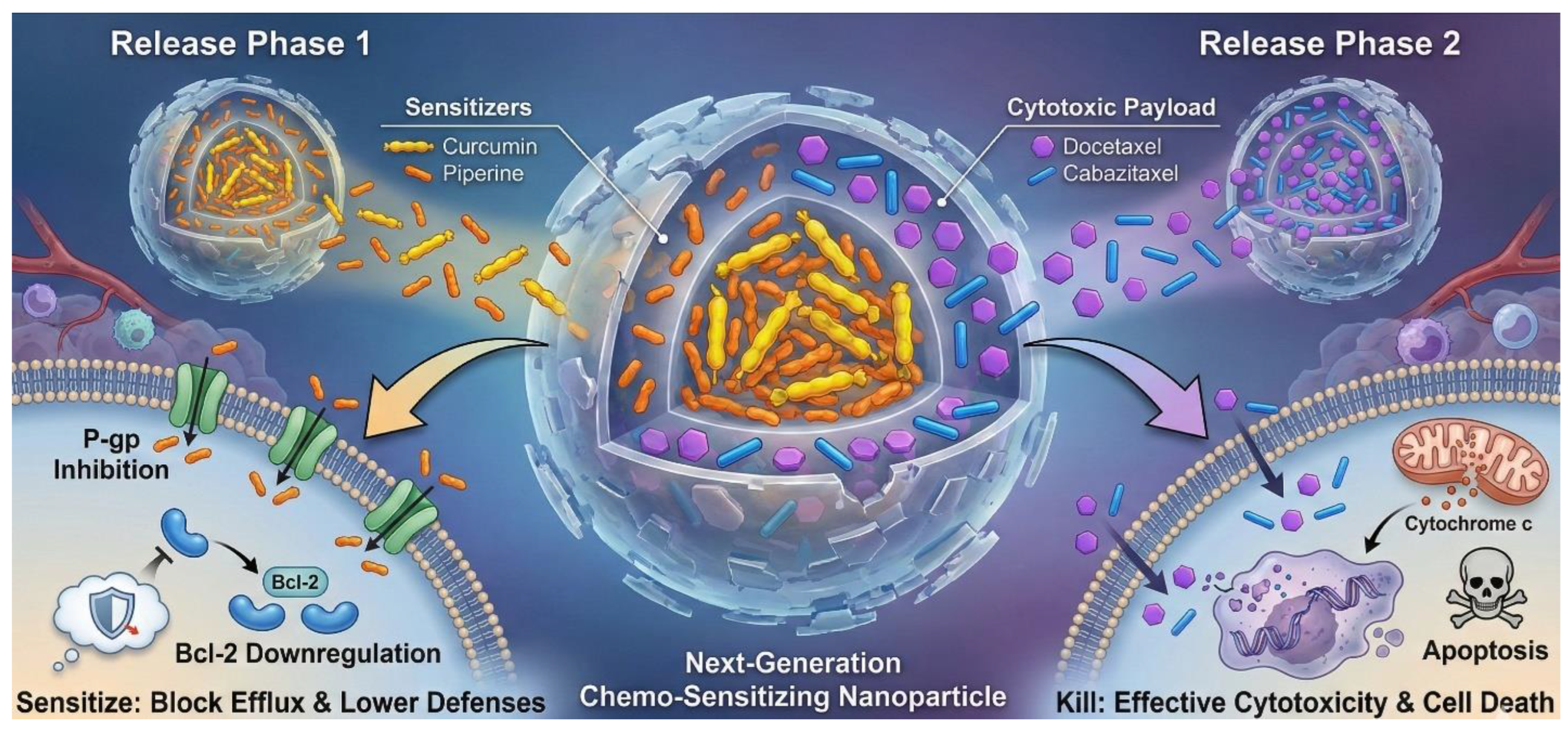

Table 1.
Physicochemical Properties and Outcomes of Curcumin/Piperine Nanoformulations in Prostate Cancer.
Table 1.
Physicochemical Properties and Outcomes of Curcumin/Piperine Nanoformulations in Prostate Cancer.
| Nanoparticle Type | Components | Size (nm) | Zeta Potential (mV) | Drug Loading (DL) / Encapsulation Efficiency (EE) | Model System | Key Biological Outcome | Reference |
| PLGA Nanoparticles | Curcumin + Piperine | 202.5 ± 36.3 | -30.3 ± 0.1 | EE: ~73% (Cur), ~73% (Pip) | PC3, DU145, LNCaP, VCaP | Significant reduction in cell migration; inhibition of CYP17A1 steroidogenesis. | Yakubu et al. (2025) (10) |
| PLGA-PSMA NPs | Curcumin + PSMA Ab | ~150–200 | -28.0 | EE: ~90% | C4-2 Xenografts | Active targeting led to superior tumor accumulation and regression compared to non-targeted NPs. | Yallapu et al. (2014) (7) |
| Lipid-Polymer Hybrid | Curcumin + Docetaxel | 169.6 | +35.7 | High efficiency | PC3 Xenografts | Synergistic cytotoxicity; co-delivery overcame resistance mechanisms. | Yan et al. (2016) (25) |
| Calcium alginate | Curcumin + Resveratrol | 45–60 | −22.01 ± 2.17 | Cur 49.3 ± 4.3 Res 71.0 ± 6.1% | DU-145 | Combination therapy significantly decreased prostatic adenocarcinoma incidence. | Saralkar et al. (2017) (32) |
| Liposomes | Curcumin + Resveratrol | 100–150 | N/A | N/A | PTEN Knockout Mice | Combination therapy significantly decreased prostatic adenocarcinoma incidence. | Narayanan et al. (2009) (33) |
Table 2.
Ongoing and completed clinical trials of curcumin combinations in prostate cancer.
| Trial ID | Phase | Intervention | Population | Endpoints | Status/Results |
| NCT03769766 | Phase 3 | Curcumin (BCM-95) vs Placebo | Low-risk Localized PC (Active Surveillance) | Primary: Disease Progression (pathologic/therapeutic) at 2 years. | Recruiting https://www.clinicaltrials.gov/study/NCT03769766 |
| NCT02724618 Saadipoor A et al. |
Phase 2 | Nanocurcumin (SinaCurcumin) vs Placebo | PC patients undergoing Radiotherapy | Primary: Radiation-induced cystitis/proctitis; Secondary: b-PFS. | Completed. Result: No significant diff in cystitis or tumor response (43). https://clinicaltrials.gov/study/NCT02724618 |
| NCT04731844 | Phase 2 | Curcumin (4g) + Piperine (5mg) | Early-stage PC / MGUS / Smoldering Myeloma | Primary: Response rate; Secondary: Progression Free Survival. | Not yet recruiting https://clinicaltrials.gov/study/NCT04731844 |
| NCT 02095717 Passildas-Jahanmohan et al. |
Phase 2 | Docetaxel + Curcumin (6g) | Metastatic CRPC | PSA Response; Overall Survival. |
Failed/Terminated: No benefit over Docetaxel alone; discontinued for futility. https://clinicaltrials.gov/study/NCT02095717 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



