1. Introduction
Chronic lymphocytic leukemia (CLL) is the most prevalent adult leukemia in Western nations. It is distinguished by clonal proliferation and accumulation of mature B lymphocytes in peripheral blood, bone marrow, and lymphoid organs [
1]. Despite its indolent character in many situations, CLL has a widely variable clinical presentation and prognosis. Some individuals are asymptomatic for years, while others deteriorate quickly, necessitating early treatment intervention. This diversity has stimulated much investigation into the biochemical and molecular factors that drive CLL development.
Epigenetic alterations, particularly DNA methylation, have emerged as critical players in CLL pathogenesis [
2]. DNA methylation involves the addition of methyl groups to the 5-position of cytosine residues in CpG dinucleotides, often leading to transcriptional silencing of tumor suppressor genes [
3]. Aberrant DNA methylation profiles have been observed in various malignancies, including hematologic cancers, where they serve not only as early events in carcinogenesis but also as prognostic and predictive biomarkers [
4,
5].
One gene of interest in this context is E-Cadherin (CDH1), a transmembrane glycoprotein that mediates calcium-dependent cell-cell adhesion in epithelial tissues. E-Cadherin loss is a hallmark of epithelial-mesenchymal transition (EMT), a process that facilitates tumor cell migration and invasion [
6]. Though CLL is a hematological malignancy, recent evidence suggests that EMT-related pathways may influence leukemic cell trafficking and interactions with the microenvironment [
7]. Promoter methylation of CDH1 has been documented in various cancers and is associated with gene silencing and poor clinical outcomes [
8]. However, data on its methylation status in CLL remain sparse and inconclusive.
Another key molecule involved in tumor progression is Matrix Metalloproteinase-9 (MMP-9). MMP-9 is a member of the MMP family responsible for degrading extracellular matrix components, thereby facilitating tumor invasion, metastasis, and angiogenesis [
9]. In CLL, MMP-9 is not only overexpressed but also contributes to the survival and drug resistance of leukemic cells through autocrine and paracrine mechanisms [
10]. Studies have shown that MMP-9 expression may be regulated epigenetically, and promoter hypomethylation is often linked with its overexpression in cancers [
11]. Investigating the methylation status of the MMP-9 promoter may thus provide insight into its role in CLL pathobiology and prognosis.
Despite increasing interest in epigenetics in CLL, studies assessing the methylation patterns of E-Cadherin and MMP-9 gene promoters in newly diagnosed patients are limited, particularly in Middle Eastern populations. Moreover, the clinical relevance of these epigenetic markers—such as their association with white blood cell count, hemoglobin level, platelet count, and Rai staging—remains to be fully clarified.
The present study aims to evaluate the promoter methylation status of E-Cadherin and MMP-9 genes in newly diagnosed CLL patients compared to healthy controls, using methylation-specific PCR (MSP) and methylation-sensitive restriction enzyme PCR (MSRE-PCR). We also explore the association of these epigenetic changes with clinical and hematological parameters. This work seeks to enhance understanding of the epigenetic landscape of CLL and to determine the potential of E-Cadherin and MMP-9 promoter methylation as biomarkers for disease prognosis and progression. To our knowledge, few studies have jointly evaluated E-Cadherin and MMP-9 promoter methylation in CLL, particularly in Middle Eastern populations. This study therefore aims to characterize their methylation patterns in CLL and to assess their potential clinical and hematologic associations.
2. Materials and Methods
A case-control research was carried out at Azadi Teaching Hospital in Duhok, Iraq. The study included 70 newly diagnosed chronic lymphocytic leukemia (CLL) patients and 70 age- and sex-matched healthy control subjects. All CLL patients were diagnosed using the World Health Organization (WHO) 2017 criteria [
12], which include persistent absolute lymphocytosis (≥5 × 10⁹/L), small mature lymphocytes with clumped chromatin, and B-cell lineage markers (CD19+, CD20+) with co-expression of CD5 and CD23. All patients with cytogenetic or molecular abnormalities, including TP53 mutations, were excluded. A priori sample size calculation was not performed; however, the selected number (n=70 per group) provided adequate power for detecting methylation frequency differences exceeding 20%.
The study protocol was approved by the Research and Ethics Committee of the College of Medicine, University of Duhok. All participants provided written informed consent prior to sample collection, in accordance with the Declaration of Helsinki.
All participants provided peripheral blood samples (5 mL) in EDTA tubes. Hematological parameters such as hemoglobin concentration, total white blood cell count (WBC), absolute lymphocyte count, and platelet count were determined using a Medonic hematology analyzer (Sweden). The Binet staging approach was used for clinical CLL staging [
13].
Genomic DNA was isolated from whole blood using a modified salting-out procedure, which is inexpensive and produces high-purity DNA appropriate for methylation investigations [
14,
15]. To conduct methylation analysis, 1 μg of genomic DNA was converted to sodium bisulfite using the EpiTect Fast Bisulfite Conversion Kit (Qiagen, Germany) per the manufacturer’s recommendations. This chemical modification converts unmethylated cytosine residues to uracil while leaving methylated cytosines unchanged, allowing for differential amplification in subsequent PCR steps.
The methylation status of the E-Cadherin (CDH1) and MMP-9 gene promoters was assessed using two different techniques:
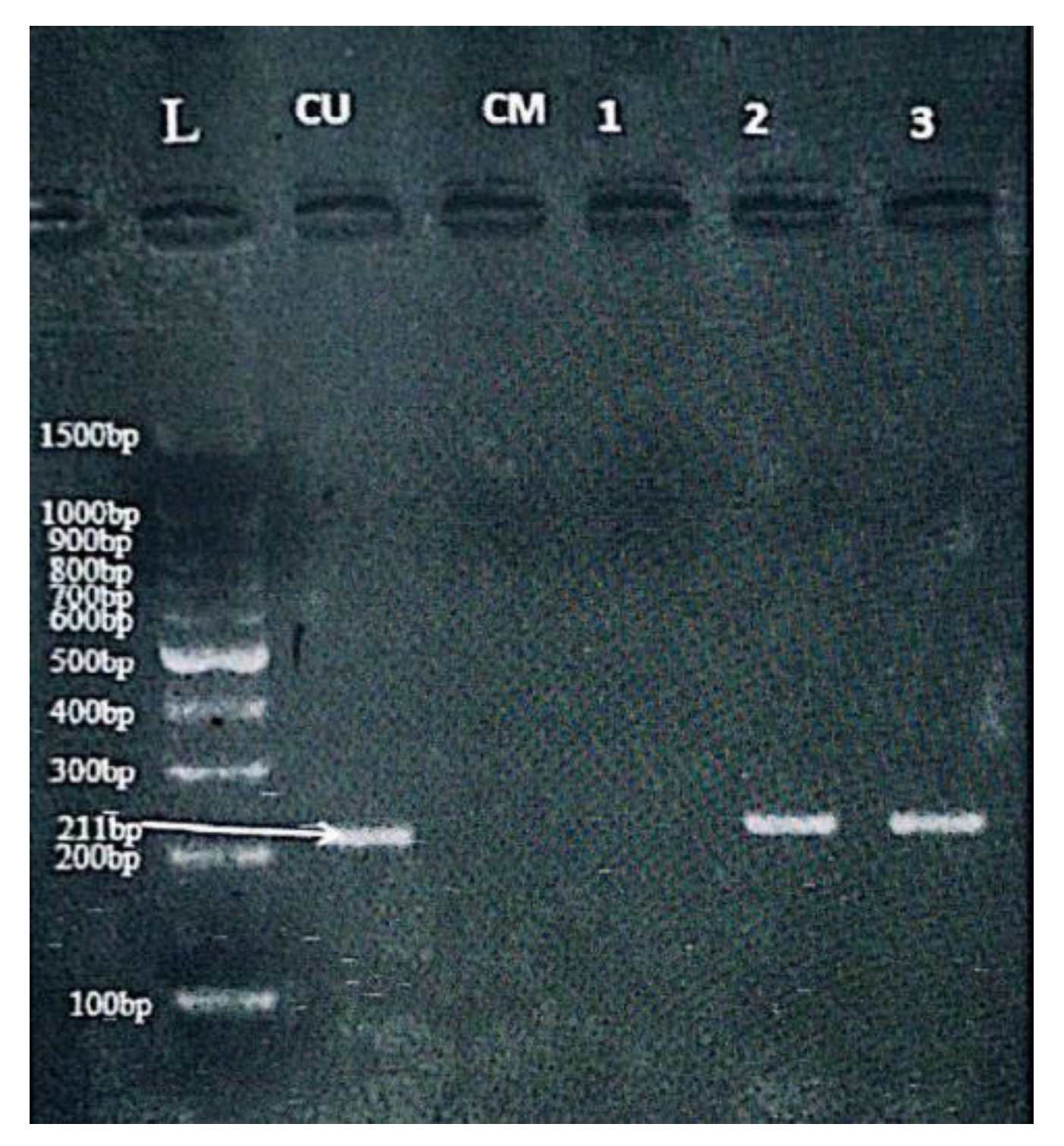
Methylation-Specific PCR (MSP) was used for E-Cadherin gene promoter analysis. Two sets of primers were employed [
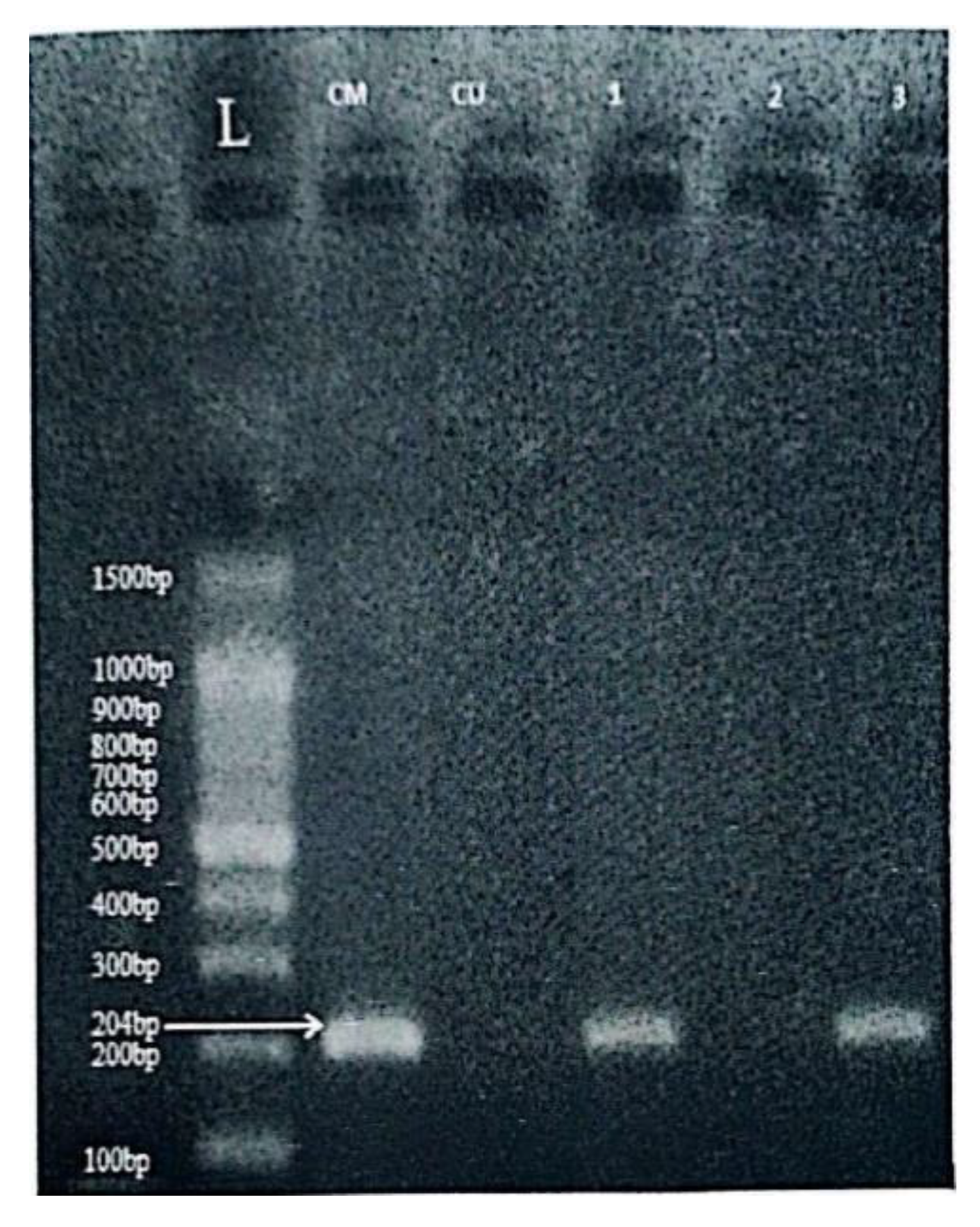
16]—one specific for the methylated sequence and another for the unmethylated version: Methylated CDH1 primers: Forward: 5’-GGTGAATTTTTAGTTAATTAGCCGGTAC-3’; Reverse: 5’-CATAACTAACCGAAAACGCCG-3’. Unmethylated CDH1 primers: Forward: 5’-GGTAGGTGAATTTTTAGTTAATTAGTGGTA-3’; Reverse: 5’-ACCCATAACTAACCAAAAACACCA-3’. PCR amplification was performed in a final volume of 25 µL with an initial denaturation at 95°C for 5 minutes, followed by 35 cycles of 94°C for 30 seconds, 52°C for 30 seconds (annealing), and 72°C for 30 seconds, with a final extension at 72°C for 7 minutes. Amplified products (204 bp for methylated and 211 bp for unmethylated alleles,
Figure 1 and
Figure 2) were analyzed by 2% agarose gel electrophoresis stained with safedye.
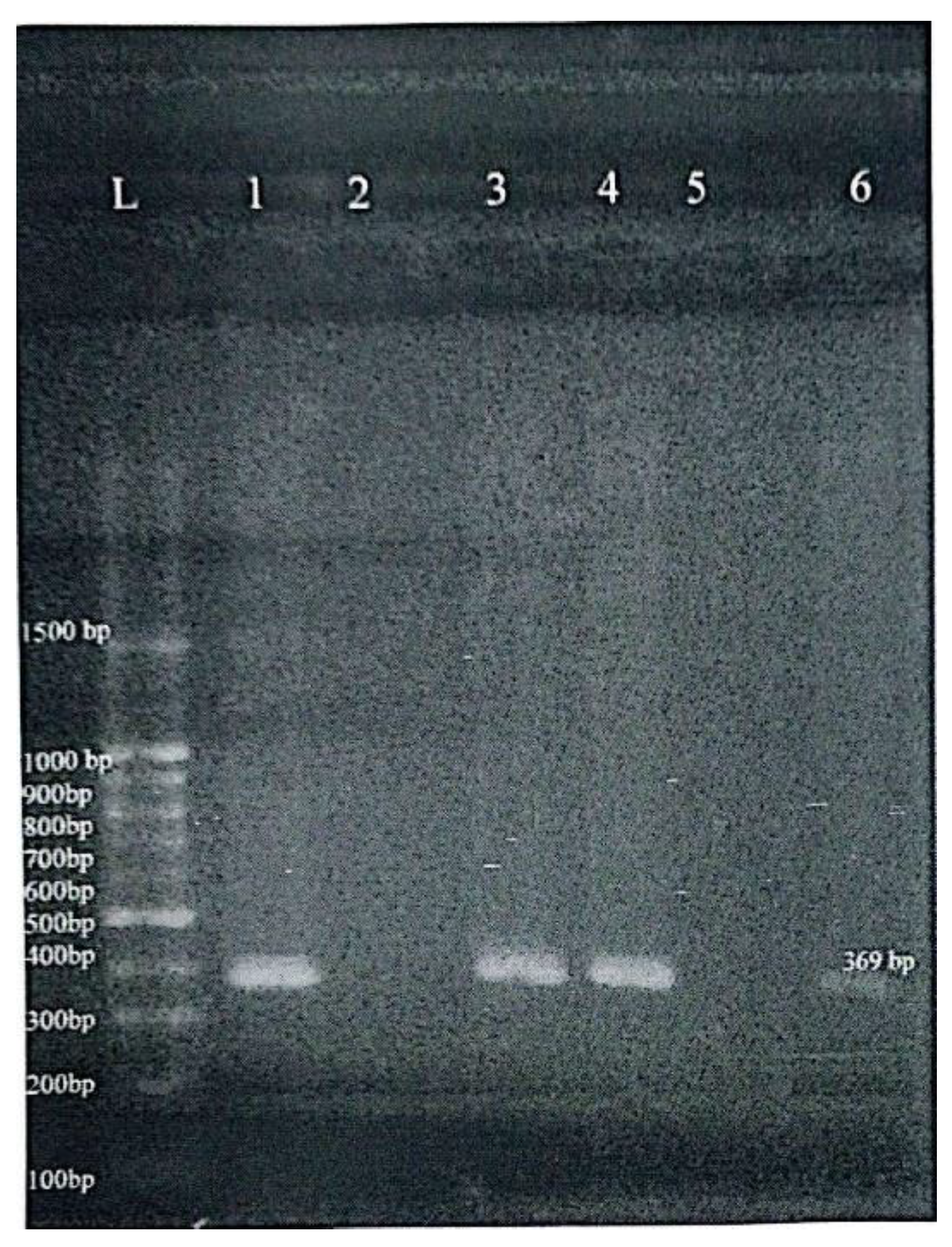
Methylation-Sensitive Restriction Enzyme PCR (MSRE-PCR) was used to determine the methylation status of the MMP-9 gene promoter using specific primers [
17]: Forward: 5’-GCTTCATCCCCCTCCCTCC-3’ and Reverse: 5’-AGCACCAGGACCAGGGGC-3’. Genomic DNA was first digested with the restriction enzyme AciI, which selectively cuts unmethylated CpG sites. PCR was then conducted with the aid of thermal cycler (Applied Biosystems 2720, Singapore) under the following cycling conditions: 95°C for 5 minutes, followed by 35 cycles of 94°C for 30 seconds, annealing at 70°C for 30 seconds, and extension at 72°C for 30 seconds, with a final extension at 72°C for 10 minutes. A 369 bp product indicated a methylated promoter (uncut by the enzyme), whereas absence of amplification implied unmethylation due to enzyme digestion. PCR products were visualized using 100 bp DNA ladders as molecular markers on 2% agarose gels under UV illumination (
Figure 3). Commercial methylated and unmethylated control DNA (EpiTect PCR Control DNA Set, Qiagen) were included in each batch of reactions to ensure assay reliability.
The data were processed with SPSS version 26.0 (IBM, USA). Categorical data were reported as frequencies and percentages, whereas continuous variables were presented as means ± standard deviation. The Chi-square test was used to compare categorical data and the independent sample t-test for continuous variables. A p-value of <0.05 was considered statistically significant.
3. Results
Patient Demographics and Clinical Features
This study included
70 newly diagnosed CLL patients (48 males and 22 females) and
70 age- and sex-matched healthy controls. The median age of patients was 62 years (range: 44–80 years), with a male predominance of 68.6 % (male-to-female ratio 2.18:1). The distribution of clinical stages according to Binet classification (
Table 1) showed that most patients were in
stage A (54.3 %), followed by
stage B (28.6 %) and
stage C (17.1 %). Female patients were more frequently diagnosed at stage A (
77.3 %) compared with males (
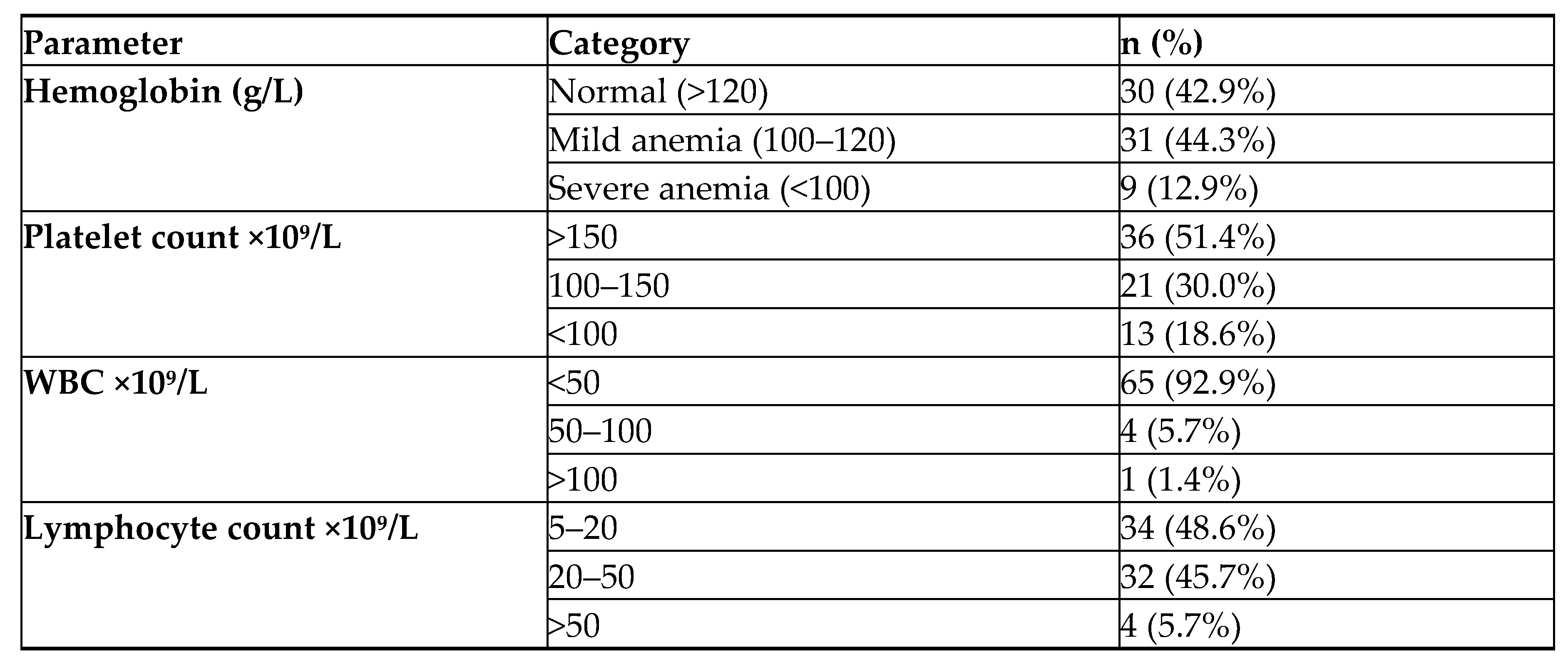
43.8 %, p = 0.022), suggesting earlier-stage disease among women. Hematological parameters revealed a predominance of mild anemia and moderate thrombocytopenia (
Table 2).
E-Cadherin Promoter Methylation
Methylation-specific PCR showed
E-Cadherin promoter methylation in
75.7 % (n = 53) of CLL patients and
77.1 % (n = 54) of healthy controls, revealing no
significant difference (p = 0.91). Among patients, methylation was observed in
86.4 % (n=19) of females and
72.9 % (n=35) of males (p = 0.44). There were
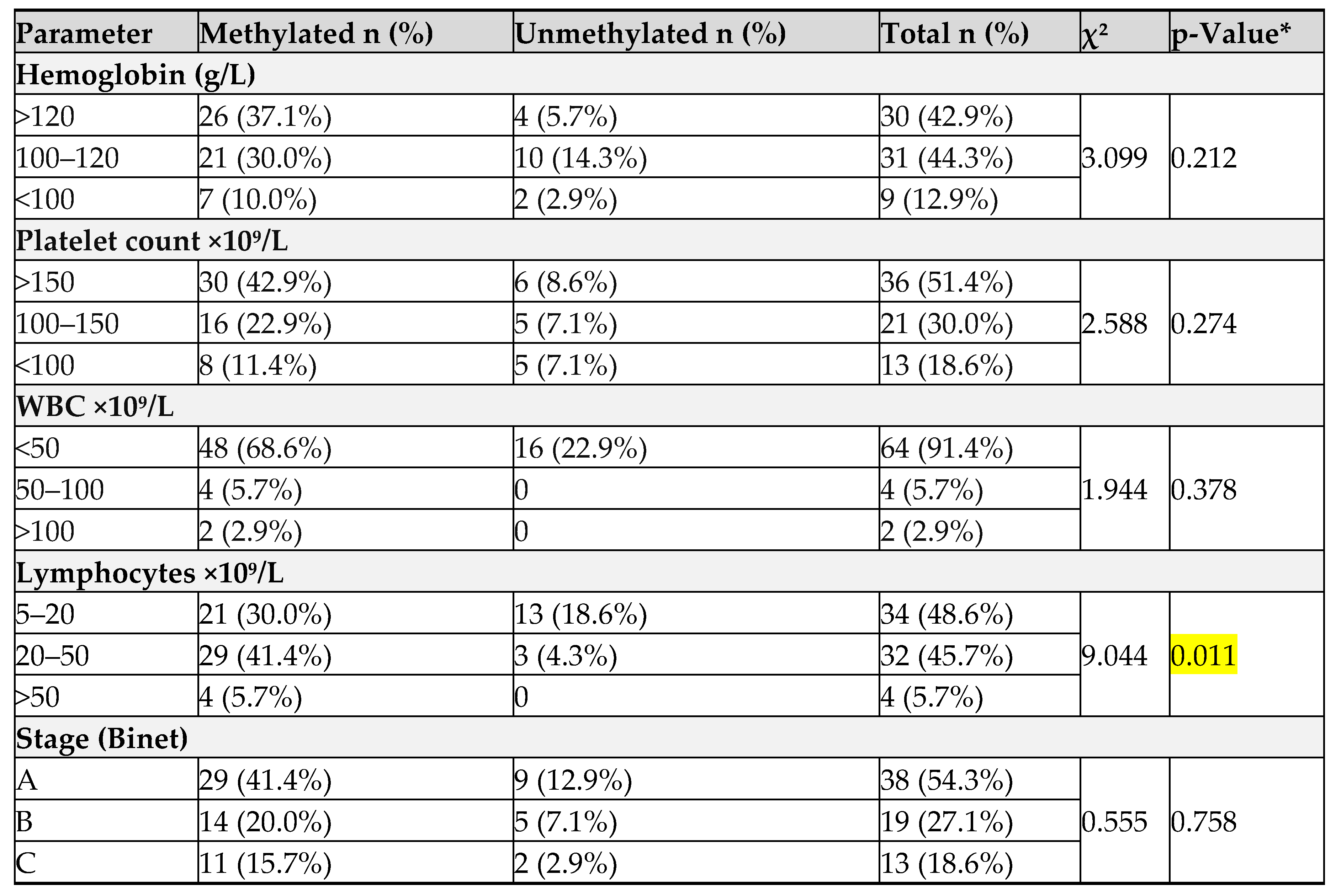
no significant associations between
E-Cadherin methylation and hemoglobin, platelet, total white blood cells (WBC) count and advanced staging, however a significant
association was found with absolute lymphocyte count (p = 0.01) (
Table 3).
MMP-9 Promoter Methylation
In contrast to E-Cadherin, significant differences in methylation status were observed for the MMP-9 gene promoter. Methylation-sensitive restriction enzyme PCR revealed that 70.0% (n = 49) of CLL patients had methylated MMP-9 promoters, compared to 100% (n = 70) of controls (p = 0.001), indicating that promoter hypomethylation is significantly associated with the disease. The remaining 30% (n = 21) of patients exhibited unmethylated MMP-9 promoters, a pattern not seen in any control sample.
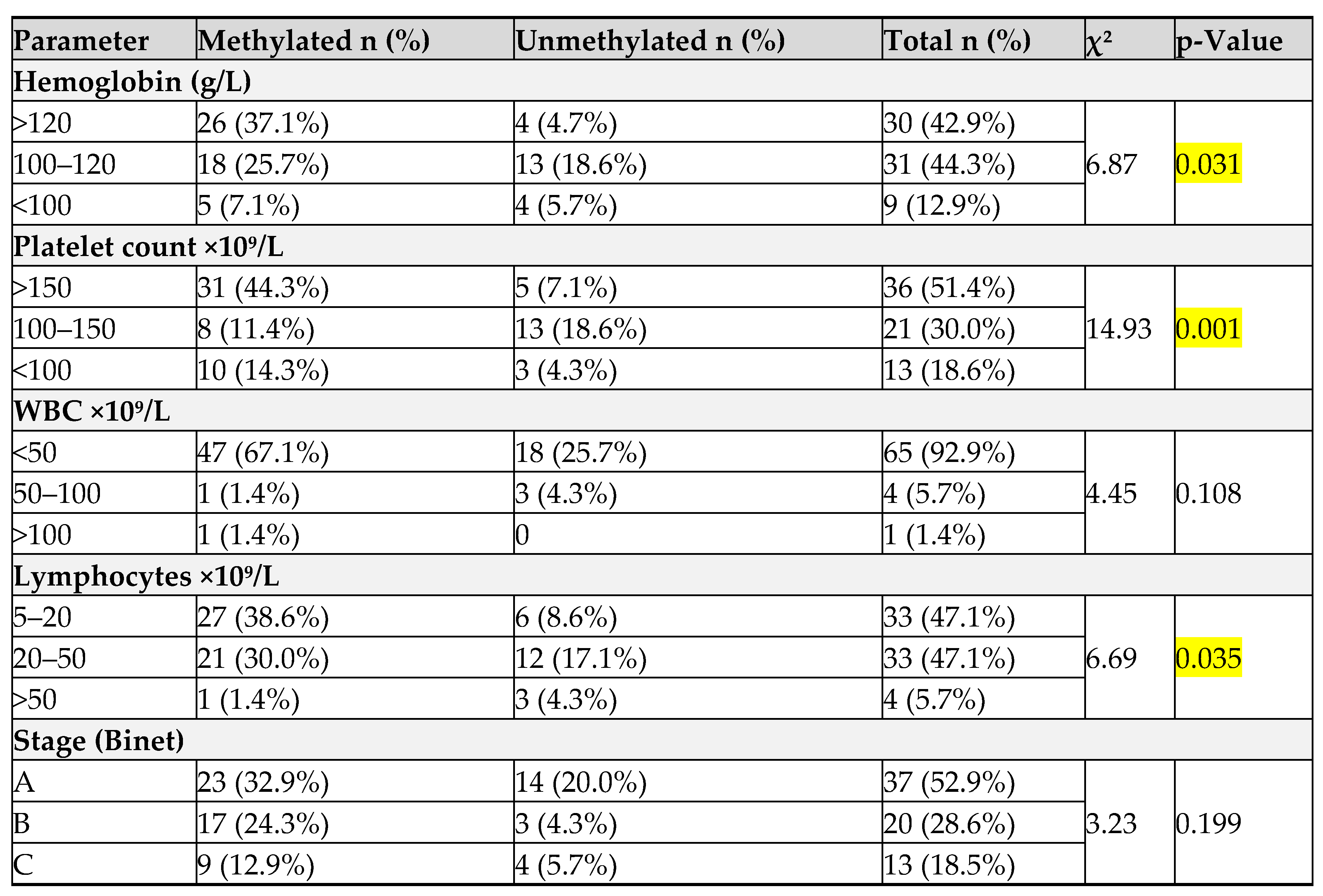
Unmethylated MMP-9 was significantly associated with
female gender (≈ 53 % vs. 19 % in males, p = 0.02), lower hemoglobin levels (p = 0.031), lower platelet counts (p = 0.001), and higher lymphocyte counts (p = 0.035) (
Table 4). No significant differences were observed for WBC, or clinical stage (p > 0.05). These findings imply that MMP-9 promoter demethylation may be linked to particular clinical and biological features, particularly thrombocytopenia, anemia and gender-related differences, although it may not directly reflect disease stage.
4. Discussion
This study assessed the promoter methylation status of two genes—E-Cadherin (CDH1) and Matrix Metalloproteinase-9 (MMP-9)—in newly diagnosed chronic lymphocytic leukemia (CLL) patients, highlighting their potential roles in disease pathogenesis and progression. The main findings indicate a lack of significant association between E-Cadherin methylation and CLL, while loss of MMP-9 promoter methylation was significantly associated with CLL and correlated with certain clinical parameters such as gender, platelet count, hemoglobin level and lymphocytes count.
E-Cadherin, a key adhesion molecule, is frequently hypermethylated in several solid tumors—such as breast, prostate, and gastric cancers—where it contributes to epithelial-mesenchymal transition, tumor invasion and metastasis [
6,
8]. However, in the current study, E-Cadherin promoter methylation was detected in 75.7% of CLL patients and 77.1% of healthy controls, with no significant difference (p = 0.91), suggesting that its methylation may be a non-specific or even age-related epigenetic event in peripheral blood cells rather than a leukemia-specific phenomenon. This aligns with previous findings by Starska et al., who noted that while CDH1 methylation is common, it does not always correlate with malignant transformation [
16].
Furthermore, no significant correlations were found between E-Cadherin methylation and hematological parameters (e.g., hemoglobin, WBC, platelet count) or Binet stage. Although an association with absolute lymphocyte count (p = 0.011), this does not strongly support a diagnostic or prognostic role for CDH1 methylation in CLL, it may reflect general leukocyte turnover rather than a disease-specific mechanism. Previous studies have suggested that CDH1 expression might play a role in the interaction between leukemic cells and the microenvironment [
7], but the present data do not substantiate a meaningful clinical correlation.
In contrast, the MMP-9 promoter methylation status revealed a significant difference between CLL patients and controls. While 100% of the healthy controls exhibited methylated MMP-9 promoters, only 70.0% of CLL cases showed methylation, with the remaining 30.0% being unmethylated (p = 0.001). This hypomethylation in CLL is consistent with the role of MMP-9 as a key effector in matrix remodeling, tumor cell migration, and angiogenesis [
9]. MMP-9 is known to be overexpressed in CLL and contributes to B-cell survival, tissue invasion, and drug resistance through both autocrine and paracrine pathways [
10].
The significant association between unmethylated MMP-9 and low platelet counts (p = 0.001) suggests that demethylation may be linked to more aggressive disease or advanced marrow involvement. Thrombocytopenia is a recognized poor prognostic indicator in CLL [
1], and its correlation with MMP-9 demethylation may reflect the pathological remodeling of the bone marrow niche, facilitating leukemic expansion. While no significant relationship was found with Binet staging (p = 0.199), this may be attributed to sample size limitations or staging insensitivity to subtle molecular changes.
Interestingly, unmethylated MMP-9 status was also significantly more frequent in female patients (53.0%) compared to males (19.0%) (p = 0.02). Gender-specific epigenetic variations have been reported in other hematologic malignancies, and although the mechanism remains unclear, hormonal or chromosomal influences on DNA methylation machinery may play a role. Such findings were similarly observed by Saeed et al., who reported variable TP53 methylation patterns among Iraqi CLL patients with gender differences [
2].
Functional support for the role of MMP-9 promoter methylation comes from prior studies showing that hypomethylation leads to increased MMP-9 mRNA levels, as demonstrated in periapical inflammatory lesions by Campos et al. [
17]. Moreover, Redondo-Muñoz et al. showed that MMP-9 enhances CLL B-cell survival through its hemopexin domain, further reinforcing the biological significance of this gene in CLL progression [
10].
While these results are compelling, this study has limitations. The sample size is modest, which may restrict the ability to detect additional associations. Moreover, the study was cross-sectional and did not include gene expression or protein quantification to directly correlate methylation with functional changes. Future studies should include mRNA expression profiling and protein assays, such as ELISA or immunohistochemistry, to validate the clinical relevance of methylation findings. Additionally, longitudinal analysis would help clarify whether these epigenetic markers predict disease progression or treatment response.
5. Conclusions
Methylation of E-Cadherin promoter was common in both CLL patients and healthy controls, indicating it is not specific or useful for CLL diagnosis or prognosis. In contrast, MMP-9 promoter hypomethylation was significantly more frequent in CLL patients and was associated with lower platelet counts, lower Hemoglobin levels, higher lymphocytes count and female gender, suggesting a link to disease aggressiveness and possible gender-related differences. These results propose MMP-9 promoter methylation as a potential biomarker for CLL progression, though further longitudinal and functional studies are needed to confirm its clinical significance.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was approved by the Research and Ethics Committee of the College of Medicine, University of Duhok (Approval No. 26062022-5-12). All participants provided written informed consent prior to sample collection, in accordance with the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
data available on request.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hallek, M. Chronic lymphocytic leukemia: 2020 update on diagnosis, risk stratification and treatment. Am. J. Hematol. 2019, 94, 1266–1287. [Google Scholar] [CrossRef] [PubMed]
- Saeed, W.H.; Eissa, A.A.; Al-Doski, A.A. Impact Of TP53 Gene Promoter Methylation On Chronic Lymphocytic Leukemia Pathogenesis And Progression. J. Blood Med. 2019, 10, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Esteller, M. Epigenetics in cancer. N. Engl. J. Med. 2008, 358, 1148–1159. [Google Scholar] [CrossRef] [PubMed]
- Calin, G.A.; Dumitru, C.D.; Shimizu, M.; Bichi, R.; Zupo, S.; Noch, E.; Aldler, H.; Rattan, S.; Keating, M.; Rai, K.; et al. Frequent deletions and down-regulation of micro- RNA genes miR15 and miR16 at 13q14 in chronic lymphocytic leukemia. Proc. Natl. Acad. Sci. USA 2002, 99, 15524–15529. [Google Scholar] [CrossRef] [PubMed]
- Abruzzo, L.V.; Herling, C.D.; Calin, G.A.; Oakes, C.; Barron, L.L.; Banks, H.E.; Katju, V.; Keating, M.J.; Coombes, K.R. Trisomy 12 chronic lymphocytic leukemia expresses a unique set of activated and targetable pathways. Haematologica 2018, 103, 2069–2078. [Google Scholar] [CrossRef] [PubMed]
- Berx, G.; Van Roy, F. The E-cadherin/catenin complex: An important gatekeeper in breast cancer tumorigenesis and malignant progression. Breast Cancer Res. 2001, 3, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Calissano, C.; Damle, R.N.; Hayes, G.; Murphy, E.J.; Hellerstein, M.K.; Moreno, C.; Sison, C.; Kaufman, M.S.; Kolitz, J.E.; Allen, S.L.; et al. In vivo intraclonal and interclonal kinetic heterogeneity in B-cell chronic lymphocytic leukemia. Blood 2009, 114, 4832–4842. [Google Scholar] [CrossRef] [PubMed]
- Graff, J.R.; Herman, J.G.; Lapidus, R.G.; Chopra, H.; Xu, R.; Jarrard, D.F.; Isaacs, W.B.; Pitha, P.M.; E Davidson, N.; Baylin, S.B. E-cadherin expression is silenced by DNA hypermethylation in human breast and prostate carcinomas. . 1995, 55, 5195-9–9. [Google Scholar] [PubMed]
- Vandooren, J.; van den Steen, P.E.; Opdenakker, G. Biochemistry and molecular biology of gelatinase B or matrix metalloproteinase-9 (MMP-9): The next decade. Crit. Rev. Biochem. Mol. Biol. 2013, 48, 222–272. [Google Scholar] [CrossRef] [PubMed]
- Redondo-Muñoz, J.; Ugarte-Berzal, E.; Terol, M.J.; Steen, P.E.V.D.; del Cerro, M.H.; Roderfeld, M.; Roeb, E.; Opdenakker, G.; García-Marco, J.A.; García-Pardo, A. Matrix Metalloproteinase-9 Promotes Chronic Lymphocytic Leukemia B Cell Survival through Its Hemopexin Domain. Cancer Cell 2010, 17, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Aitchison, E.E.; Dimesa, A.M.; Shoari, A. Matrix Metalloproteinases in Glioma: Drivers of Invasion and Therapeutic Targets. BioTech 2025, 14, 28. [Google Scholar] [CrossRef] [PubMed]
- Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.; Stein, H.; et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (Revised 4th Edition); IARC: Lyon, France, 2017; pp. 285–290. [Google Scholar]
- Binet, J.; Catovsky, D.; Chandra, P.; Dighiero, G.; Montserrat, E.; Rai, K.R.; Sawitsky, A. Chronic Lymphocytic Leukaemia: Proposals for a Revised Prognostic Staging System. Br. J. Haematol. 1981, 48, 365–367. [Google Scholar] [CrossRef] [PubMed]
- Kashmoola, M.A.; Eissa, A.A.; Al-Takay, D.T.; Al-Allawi, N.A.S. Molecular Characterization of G6PD Deficient Variants in Nineveh Province, Northwestern Iraq. Indian J. Hematol. Blood Transfus. 2014, 31, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Iranpur-Mubarakeh, V.; Esmailizadeh, A.K. Rapid Extraction of High-Quality DNA from Whole Blood Stored at 4°C for Long Period. 2010; Protocol Online. Available online: http://www.protocol-online.org/prot/Protocols/Rapid-Extraction-of-High-Quality-DNA-from-Whole-Blood-Stored-at-4-C-for-Long-Period-4175.html.
- Starska, K.; Forma, E.; Lewy-Trenda, I.; Papież, P.; Woś, J.; Bryś, M. Diagnostic impact of promoter methylation and E-cadherin gene and protein expression levels in laryngeal carcinoma. Wspolczesna Onkol. Oncol. 2013, 3, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Campos, K.; Gomes, C.C.; Farias, L.C.; Silva, R.M.; Letra, A.; Gomez, R.S. DNA Methylation of MMP9 Is Associated with High Levels of MMP-9 Messenger RNA in Periapical Inflammatory Lesions. J. Endod. 2016, 42, 127–130. [Google Scholar] [CrossRef] [PubMed]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).