
Submitted:
02 December 2025
Posted:
03 December 2025
You are already at the latest version
Abstract
Background HIV-serodiscordant heterosexual couples, where one partner is HIV-positive and the other HIV-negative, provide important insights into public health when prevention is declined. Prior studies suggested that HIV-negative female partners may present borderline personality disorder (BPD), often linked to child abuse, trauma, and neglect. Methods This study surveyed 175 couples to assess condom use, followed by qualitative interviews with HIV-negative female partners. Narrative analysis consistently revealed BPD and associated psychopathology, leading to the development of a theoretical model integrating quantitative and qualitative findings to explain how BPD-related psychopathology interacts with relational dynamics and HIV risk behaviours. Results HIV-negative women with BPD who declined prevention frequently exhibited comorbid self-defeating personality disorder (SDPD), dependent personality disorder (DPD), and complex PTSD, adopting health belief models and behaviours that heightened vulnerability to HIV transmission. Comparable findings were not observed in HIV-negative males. Conclusions: Women’s health behaviours are shaped by personality, trauma, and psychosocial factors, which may act as hidden drivers of pandemic transmission. Public health strategies must integrate trauma-informed and personality-focused interventions, recognising the lifelong impact of abuse and neglect to strengthen prevention and reduce the spread of HIV and other sexually transmitted diseases.
Keywords:
borderline personality disorder
; HIV serodiscordant couples
; health behavior
; women’s health
; HIV
; psychiatry
; self-defeating personality disorder
; dependent personality disorder
; complex post-traumatic stress disorder
1. Introduction
While individual health can be seen as a combination of health literacy and health beliefs [1], recently, there has been increased interest in social and psychopathological factors influencing health behaviors and their decline during pandemics of contagious diseases [2]. Social determinants of health are nonmedical factors that include individual traits like education, income, and health beliefs, as well as social and physical environments such as families, schools, workplaces, neighborhoods, social and biological factors, and the political-economic structure of society [3]. Health behaviors refer to the ways in which people influence their own health, either positively or negatively. These actions can be intentional or accidental and may either improve or harm the well-being of the individual or others. In health promotion and prevention, people are active decision-makers when it comes to health prevention and control [4]. According to the Health Belief Model, people are more likely to engage in a health behavior if they believe they are susceptible to the condition, if they perceive it as potentially harmful, and if they believe there are benefits to the health behavior [5].
However, when the AIDS pandemic and, more recently, the COVID-19 pandemic began, in our infectious diseases and psychiatric clinics, we noticed that health literacy was not enough to prevent people from engaging in harmful health behaviors. The ability to read, understand, and act on health information is referred to as functional health literacy [6]. Inadequate health literacy can lead to various negative outcomes, including worsening health, misunderstandings of medical conditions and treatments, difficulties in recognizing and utilizing preventive services, lower self-rated health, reduced adherence to medical advice, increased hospital visits, and higher healthcare costs [7]. The current research examines these theories in HIV-serodiscordant couples, defined by the WHO as two people in a stable relationship where one partner is HIV-positive and the other is HIV-negative [7].
In our previous survey of HIV-serodiscordant heterosexual couples (HSDHC) in infectious disease departments and psychiatric settings completed during study phase 1, we discovered that some psychopathological and psychosocial factors influence the decision in couples to decline HIV prevention (NPC) of sexual transmission [8]. We called this behavior Samos Syndrome (Sindrome di Samo (It.), El Síndrome de Samo (Sp.), Le Syndrôme de Samo (Fr.) [8]). In the HSDHC, the female partner who is HIV-negative and has Samos Syndrome makes a mutual decision with her HIV-positive male partner not to use primary prevention to avoid HIV transmission [9]. We identified the Samos Syndrome roughly 20 years ago [10]. Women with BPD and Samos Syndrome, specifically DP in HSDHC, intentionally choose not to use infection prevention methods during sexual encounters that pose a risk for HIV, despite having sufficient health literacy about the infection [11]. We subsequently confirmed that this condition is more common in women with borderline personality disorder and a history of childhood trauma, sexual abuse, and attachment issues [12]. Samos Syndrome refers to the tendency of individuals—often with a history of childhood violence, abuse, neglect, or trauma—to form romantic, emotionally intimate, and stable sexual relationships with partners who present with significant and debilitating physical, mental, or social conditions [13]. The behavior in question was called “Samos Syndrome” by the authors, based on the story of Zambaco Pacha, a Turkish doctor who visited many leprosaria worldwide in 1800, including one on the Greek island of Samos [13]. According to Zambaco Pacha, Samos Island in Greece was the only place where people with leprosy could participate in community activities. They were also allowed to marry members of the local community [14]. So, it turned out that a woman developed feelings for a man who was highly contagious and suffering from leprosy and bubonic plague [15]. This episode is reported in Guido Ceronetti’s book, The Silence of the Body [15].
HIV progressively weakens the immune system by targeting CD4 T cells and may lead to AIDS if untreated, with AIDS marked by severe immune deficiency and increased susceptibility to infections and cancers; being HIV-positive means the virus is detectable through antibodies, antigens, or viral RNA, though not necessarily symptomatic or indicative of AIDS; furthermore, tansmission occurs via specific infector’s body fluids, blood, semen, vaginal fluids, rectal secretions, and breast milk, from individuals with a detectable viral load, entering the infectee’s bloodstream through mucous membranes, open wounds, or injection [16,17,18,19,20,21]
In DSM-5, the criteria for diagnosing BPD include (1) desperate attempts to avoid perceived or actual separation; (2) a passionate and unpredictable pattern of relationships that switch between extremes of idealization and devaluation; (3) identity disturbance: a notable and ongoing unstable perception of self-awareness and self; (4) at least two potentially harmful impulsive behaviors, such as overspending, drug misuse, reckless driving, sexual activity, binge eating, and others; (5) significant emotional hypersensitivity, such as intense episodic dysphoria, anxiety, or irritability, lasting a few hours or rarely more than a few days, leading to affective instability; (6) persistent feelings of emptiness; (7) inappropriate, intense, or hard-to-control anger, such as frequent outbursts, persistent rage, or recurring violent conflicts; and (8) brief paranoid thoughts or acute dissociation [22].
1.1. Aims
Aim of this study is to examine the intersection of borderline personality disorder (BPD), psychiatric comorbidities, and health risk behaviours in women involved in challenging romantic relationships. It focuses on how relational dynamics may increase vulnerability to HIV and Sexually Transmitted Infections (STIs), particularly through intentional self-harm and neglect of preventive health measures. Key comorbidities, self-defeating personality disorder, dependent personality disorder, and complex PTSD, were empirically explored within this subgroup. Although BPD was not a selection criterion, it emerged as the predominant diagnosis, confirmed via ICD-10/11 and DSM-5/DSM-5-TR based clinical interviews. This diagnostic outcome shaped the thematic analysis and validated the study’s focus on BPD and its associated behavioural risks. We clarify that while aspects of Samos syndrome have been reported in previous publications, the results presented in the current manuscript are entirely novel. This study represents a condensation and theoretical development of our earlier work, as cited in the references, but the methods, conclusions, and integrative framework are presented here for the first time. The manuscript builds upon prior findings to offer a unified analysis and original interpretation that has not been published elsewhere. We have revised the relevant statement to reflect this distinction more clearly.
2. Materials and Methods
2.1. Diagnostic framework
The Materials and Methods should be described with sufficient details to allow others to replic Childhood experiences of emotional neglect, physical or sexual abuse, and invalidating caregiving environments are consistently identified as key developmental precursors to borderline personality disorder (BPD). These relational traumas often disrupt attachment formation and emotional development, leading to enduring difficulties in affect regulation and interpersonal functioning. The biosocial model of BPD suggests that individuals with heightened emotional sensitivity, when raised in chronically invalidating contexts, are particularly vulnerable to developing the disorder. Empirical research supports this framework, showing strong associations between early maltreatment and the emergence of core BPD features, including unstable relationships, identity disturbance, and impulsivity [23,24,25]. Behavioral traits indicative of borderline personality disorder (BPD) are defined according to DSM-5 and DSM-5-TR criteria, which describe a pervasive pattern of instability in relationships, self-image, affect, and impulsivity. A diagnosis requires five or more of nine symptoms, including abandonment fears, unstable relationships, identity disturbance, impulsivity, self-harm, affective instability, chronic emptiness, intense anger, and transient paranoia or dissociation [26,27]. Participants were assessed using ICD-10 and ICD-11 diagnostic categories (World Health Organization, 1992; 2019), which reflect the standards used in our clinical setting and facilitate international comparison. [28,29]. While the ICD framework guided formal diagnostic classification, we also used DSM-5 criteria for Borderline Personality Disorder (American Psychiatric Association, 2013) to shape the conceptual framework of the study [30]. This dual-system approach was necessary because certain features central to BPD, such as affective instability, identity disturbance, and interpersonal dysfunction, are more clearly described in DSM-5 than in ICD-10/11.
2.2. Research Design
We used a convergent parallel mixed-methods design integrating quantitative prevalence data with qualitative insights to examine psychiatric comorbidities, risk behaviours, and health vulnerabilities in women with borderline personality disorder (BPD) in high-risk relational contexts. This simultaneous analysis enhances validity through triangulation and supports both empirical and interpretive outcomes, thereby increasing clinical and public health relevance [31]. Structured instruments, open-ended survey items, and ethnographic observation were used to generate both measurable trends and contextual insights. NVIVO software supported narrative analysis, while quantitative data were managed in Excel and elaborated using MedCalc. This approach enabled triangulation and enriched interpretation, particularly suited to healthcare and education contexts, to understand both outcomes and underlying processes is essential [32,33,34,35,36,37,38].
The study employed a mixed-methods design to triangulate data and generate a layered, reflexive understanding of complex phenomena in mental health practice. Each qualitative method contributes a distinct lens: (1) narrative analysis explored the storied nature of experience, privileging temporality, identity, and meaning-making; (2) thematic analysis identified patterns across data using a theory-driven approach informed by DSM-5, ICD-10/11, and psychodynamic models, allowing for structured coding while remaining open to emergent insights; (3) grounded theory supported theory generation from data, revealing latent processes and mechanisms; and (4) ethnography situates individual narratives within broader cultural and organisational contexts, particularly when direct interviews were not feasible [39,40,41,42,43]. This hybrid strategy aligns with what Bella Williams describes as hybrid qualitative analysis, where thematic analysis is enriched by integrating narrative and ethnographic insights to produce a more nuanced and layered interpretation [44]. Similarly, Creswell suggests that combining qualitative methods can enhance the depth and breadth of inquiry, especially when addressing multifaceted social phenomena [45]. Integrating qualitative approaches into a mixed-method framework enhances validity through triangulation, provides distinct insights via complementarity, informs coding structures through developmental sequencing (e.g., narrative analysis informing thematic analysis), and situates findings in real-world contexts via contextualisation (e.g., ethnographic data). This aligns with integrative evidence synthesis models that layer qualitative methods to refine theoretical constructs and interventions [46].
2.3. Data Collection and Survey
This study employed a mixed-methods approach combining structured surveys, psychiatric interviews, and open-ended questions to explore condom use, relationship history, education, and parental attachments among HIV-serodiscordant couples. NVIVO software supported thematic analysis of transcripts, identifying patterns within psychopathological frameworks for BPD. Structured interviews ensured consistency and comparability, while open-ended and unstructured interviews captured nuanced, experiential data. This dual strategy enabled both statistical mapping and interpretive depth, particularly in understanding how early relational trauma and psychoeducational histories influence risk-taking behaviors. The integration of ethnographic observation further enriched contextual insights, aligning with best practices in healthcare and education research [47,48,49,50,51,52,53,54,55,56]. In Phase 1, structured surveys used standardized, closed-ended questionnaires to assess HIV-related knowledge, attitudes, and behaviors among target HIV-serodiscordant couples, enabling consistent data collection and quantitative analysis. These were followed by structured psychiatric interviews employing validated tools to both explain non-adoption of HIV prevention and generate psychiatric diagnoses, serving diagnostic and explanatory roles within the mixed-methods design. In later phases, unstructured interviews provided open-ended, participant-led narratives that captured lived experiences and emergent themes around HIV prevention, relationships, and mental health, offering contextual depth beyond structured formats.
2.4. Phase 1 (1994-2009)
This phase adopted a cross-sectional quantitative survey with HIV-sero-discordant couples across multiple centres. Phase 1 aimed to investigate the objectives underlying biopsychosocial dynamics in HSDHC, with a focus on individuals diagnosed with borderline personality disorder (BPD). The data collection combined structured surveys and informal interviews to capture both statistical trends and experiential narratives. A total of 175 couples were recruited using purposive sampling across international sites. Interviews explored clinical histories, relational stressors, and mental health profiles. The settings included HIV clinics, genitourinary medicine units, and community psychiatric teams, ensuring ecological validity and a comprehensive lens on the interplay between psychiatric comorbidity and HIV transmission risk.
2.5. Phase 2 (2009–2019)
This phase involved a qualitative, exploratory study with unstructured interviews and narrative analysis, focusing on the phenomenology of Samos Syndrome. Phase 2 (2009–2019) was a qualitative, exploratory study investigating the objectives of relational and psychological experiences in HSDHC, with a focus on the phenomenology of Samos Syndrome—characterized by relational ambivalence, identity fragmentation, and emotional dysregulation. Data collection involved unstructured interviews and narrative analysis, guided by Braun and Clarke’s Thematic Analysis across seven iterative stages. Transcripts were anonymized and analyzed inductively to identify emergent themes reflecting emotional, interpersonal, and diagnostic complexities. The settings mirrored Phase 1, spanning HIV clinics, genitourinary medicine units, and community psychiatric teams, ensuring diverse relational contexts and integrated psychiatric-sexual health perspectives. The participants were the same approached who were in follow-up arms in HIV clinics, hence one member of the 175 HSDHC was identified as Samos, and thus a total of 80 participants.
2.6. Phase 3: (2019-2025)
The design was theory development and synthesis from previous phases, including transcript reviews and final interpretations. Phase 3 (2019–2025) focused on objectives of theory development and synthesis, advancing understanding of relational psychopathology and health vulnerability in HSDHC, particularly those with borderline personality disorder (BPD) and Samos Syndrome. The data collection drew exclusively from previously gathered transcripts, thematic matrices, and analytic memos from Phases 1 and 2. Using abductive reasoning and set-theoretic modeling, we mapped comorbidities across BPD, self-defeating personality disorder (SDPD), dependent personality disorder (DPD), and complex post-traumatic stress disorder (CPTSD). The settings involved academic and analytic environments, with interdisciplinary collaboration across psychiatric and qualitative research teams, maintaining continuity with the multicenter framework established in earlier phases. Set theory and Venn diagrams provided a formalized and visually intuitive framework for modeling theoretical constructs in research, enabling the representation of intersecting psychological, behavioral, and relational domains with conceptual clarity and structural coherence. Applications of Set Theory in Phase 3 were as follows:
- Conceptual Mapping: Sets allow researchers to define and compare categories such as diagnostic groups, behavioral traits, or relational dynamics. For example, BPD, DPD, and trauma histories can be treated as sets whose intersections reveal clinically significant patterns.
- Comorbidity and Overlap: Using intersections (e.g., BPD∩DPD∩SDPD), researchers can formally represent how multiple conditions or experiences co-occur, offering clarity in understanding complex syndromes or behavioral profiles.
- Qualitative Comparative Analysis (QCA): A set-theoretic method that uses Boolean logic to identify necessary and sufficient conditions for outcomes. It’s increasingly used in social sciences to analyze case-based data with configurational complexity.
- Narrative Structuring: Sets can be used to organize narrative data into typologies, where each set represents a thematic or diagnostic domain. This supports both idiographic depth and thematic abstraction.
- Formal Logic Integration: Set theory enables the use of symbolic logic in qualitative research, enhancing transparency and reproducibility in theory-building [57].
2.7. Rigour of the Study
The study followed the criteria established by Guba and Lincoln (1984) to ensure transferability, dependability, credibility, and confirmability. The findings were firmly based on the collected data and underwent audits at multiple centers to enhance reliability. Theories and conclusions aligned with the current understanding of psychopathology, using precise terminology and concepts. Researcher bias was mitigated through data triangulation, the sharing of findings, and feedback from subject-matter experts, as well as blogs, media, and colleagues. Dependability was confirmed as independent researchers worldwide identified Samos Syndrome in their studies and discussions. Transferability was achieved by replicating the study in different geographic locations, which consistently produced similar phenomena [58].
2.8. vResearcher Positionality
The authors acknowledge their positionality as experienced clinicians and researchers, shaping the lens through which this study was conducted. CL brings dual postgraduate training in psychiatry and infectious diseases, offering integrated expertise in mental health and HIV care. MR contributes a strong foundation in population health and service evaluation. Their combined experience in HIV-related research, particularly its psychological and psychiatric dimensions, provides deep insight into both clinical realities and the structural determinants of health. Grounded in a commitment to social justice, equity, and compassionate care, their work seeks to enhance service quality and address systemic barriers to health and behavior.
2.9. Methodology, Theoretical Frameworks, and Theory Construction
The current research adopted a constructivist approach as outlined by Guba and Lincoln (1984), emphasizing the locally constructed nature of reality [42,43]. The epistemological framework was transactional, meaning that knowledge was shaped through interactions between researchers and participants, with patient narratives interpreted through the researchers’ subjective lenses. Methodologically, the study employed a hermeneutic and dialectical approach, focusing on the interpretation and reconstruction of social constructs to develop theories that explain observed phenomena [59,60].
We adopted an ontological perspective to explore the nature of reality, which is shaped by locally and individually constructed views. The epistemology examined the relationship between the knower (researcher) and the subjects being understood, portraying it as a transactional process. This included collecting patients’ narratives alongside researchers’ subjective interpretations of the phenomenological worlds [61]. Since the ontology of constructivism is relativism, we identified multiple realities that vary based on social, psychological, and interpersonal factors. Our approach was hermeneutic and dialectical, and social constructions were strengthened through our interactions with the target population. Therefore, our inquiry focused on understanding and reconstructing to develop theories about the observed phenomena [62].
We primarily used the WHO’s ICD-10/11 but also DSM-5/5TR diagnosis categories. This study employs a Grounded Theory approach, conducting participant observations and semi-structured interviews to gain a deeper understanding of the phenomenon of interest. Through narrative analysis, themes and sub-themes were identified, which informed the development of conceptual frameworks. The findings contribute to both middle-range theories—providing explanations specific to particular contexts—and grand theories, which offer broader theoretical insights [63]. We used the Borsboom et al. (2021) theory construction model, where developing a theory involves five stages [64] (Table 1).
2.9. Data Analysis
Phase 1 of the study included a cross-sectional anonymous survey of HIV-serodiscordant couples. We asked the couples, ‘With 100% being ‘every time you have a sexual relationship,’ how often do you use condoms for HIV prevention?’. The study was conducted in infectious disease departments and community psychiatric teams. The first author (CL) performed the interviews, which were later verified through multidisciplinary team discussions to confirm and triangulate the diagnostic hypotheses. The statistical analysis employed rigorous methods to ensure the reliability of the observed differences in condom use across sociodemographic groups. Confidence intervals were estimated using the Wilson score method, which offers improved accuracy for binomial proportions, particularly in samples of moderate size. To assess the significance of differences between paired groups, two-proportion z-tests were conducted. All comparisons yielded statistically significant results at the conventional alpha level of 0.05, with p-values consistently below 0.001. To elaborate the findings in Phase 1 we employed path analysis to examine direct and indirect associations among study variables within a theoretically specified causal framework. Standardized beta (β) coefficients were estimated using ordinary least squares regression, implemented in AMOS (Analysis of Moment Structures). The model assumed linearity, additivity, and absence of measurement error. Model fit was evaluated using conventional indices. This approach enabled quantification of mediating pathways and assessment of hypothesized structural relationships relevant to the study context [65,66].
In Phase 2, we carried out a narrative analysis of interviews with HIV-serodiscordant couples (see Appendix). Braun and Clarke’s Thematic Analysis involves seven stages. These stages typically include: (1) familiarization with the data: diving into the dataset by reading and rereading transcripts while noting initial ideas; (2) generating initial codes: finding meaningful segments of data and systematically assigning codes; (3) searching for themes: grouping related codes into broader themes that reveal patterns in the data; (4) reviewing themes: refining themes to ensure they align well with the dataset; (5) defining and naming themes: explaining the core of each theme and its relevance to the research question; (6) producing the report: writing a structured analysis that connects themes with supporting data; and (7) reflexivity and interpretation: critically reflecting on the researcher’s role and how it influences the findings [40,67]. To examine relational trajectories and behavioral outcomes linked to Samos Syndrome, the study used a hybrid analytic strategy combining narrative analysis with path modelling. This integrative approach allowed qualitative depth to be translated into structural relationships, supporting a constructivist and pragmatic epistemology. Narrative constructs, such as educational incongruence, parental relationship quality, and emotional dysregulation, were coded and operationalised into variables within a matrix-based path model. Independent, mediating, and dependent variables were mapped to explore relational plausibility rather than causality. Standardised beta coefficients quantified associations, enabling the identification of mechanisms that shape health risk behaviors and inform clinical and psychosocial interventions [68,69,70,71,72].
When direct unstructured interviews were impractical, we adopted a naturalistic ethnographic approach, gathering data through informal, work-based interactions. This method aligns with symbolic interactionism and situated learning theory, emphasizing meaning-making through real-world engagement. Drawing on Lazzari’s ethnographic work in medical settings, we collected narratives from individuals exhibiting signs of Samos Syndrome and reflections from their HIV-positive partners. To analyze these accounts, we applied a dual-framework thematic analysis combining Grounded Theory and Braun and Clarke’s reflexive approach, allowing for inductive theme development and interpretive depth. We also examined educational and familial histories to identify patterns of trauma, later confirmed through interdisciplinary team discussions across centers [73,74,75,76,77].
2.10. Use of Vignettes in Clinical Education
Vignettes are valuable tools in medical education and research, offering realistic yet controlled scenarios that promote ethical reflection, clinical reasoning, and inclusive learning. They support qualitative inquiry and protect patient confidentiality by anonymizing real cases. Used in narrative-driven training, vignettes enhance engagement, critical thinking, and cultural sensitivity. Their structured format allows educators to assess decision-making and diagnostic skills while fostering a deeper understanding of complex clinical situations. Overall, vignettes improve the validity of qualitative data collection and align educational practices with ethical and empirical standards [78,79,80,81,82]. Rather than merging transcripts with fictional vignettes directly, we followed a multi-stage interpretive process. Individual narratives from participants with similar clinical profiles were first analysed separately, then synthesized into composite vignettes representing recurring emotional, relational, and behavioural patterns. Drawing on narrative synthesis and interpretive phenomenology, these fictionalised constructs preserved the integrity of lived experience while distilling complex data into coherent forms. Early narrative analysis informed their structure and meaning-making, and thematic analysis of the unified typology revealed cross-cutting patterns. This approach supports methodological pluralism, balancing idiographic depth with thematic abstraction and ensuring epistemic transparency throughout the analytic process [83,84,85].
2.11. Ethical Consideration
The study adhered to rigorous ethical standards, including the Helsinki Declaration, with all data anonymized and collected through confidential interviews and structured assessments conducted by one of the authors (CL). Participants, particularly HIV-serodiscordant couples, were informed of their right to withdraw and provided consent under a clearly defined ethical framework. To protect identity, real cases were synthesized into fictional vignettes that preserved narrative integrity while ensuring confidentiality. Drawing on Hanna Meretoja’s ethical theory of storytelling, the study treated narrative as a morally engaged practice that fosters self-understanding, perspective-taking, and social critique. Open-ended questions explored relational and psychoeducational factors, and thematic analysis followed Braun and Clarke’s six-phase model, with clustering applied only when BPD was confirmed as the primary influence. All data, including transcripts and audio recordings, were securely stored and destroyed post-analysis, ensuring compliance with ethical and methodological best practices.
The study followed the ethical standards set by the relevant institutional and national committees on human experimentation, as outlined in the Helsinki Declaration (World Medical Association, 2013) [86]. All surveys were anonymized and conducted through confidential interviews via AIDS counseling hotlines, ensuring participant confidentiality and protection [87]. Additionally, structured interviews were conducted by one of the authors (CL). To protect confidentiality and uphold ethical standards, the narratives in this study were created by synthesizing real cases and typical accounts. Ethical approval was secured from the participating couples and relevant healthcare organizations, and all data were fully anonymized before analysis. The right to withdraw was a condition explicitly communicated to all participants during the consent process to ensure informed participation. All eligible individuals, meeting the study’s inclusion criteria, were required to understand and acknowledge this right as part of the ethical framework underpinning the study.
To protect anonymity, accounts from various individuals were merged into fictional vignettes, maintaining the original meaning while ensuring confidentiality. Storytelling, as defined by Hanna Meretoja in The Ethics of Storytelling (2018), is described as a morally complex interpretive practice that goes beyond sharing experiences to actively shape ethical understanding and social possibilities [88]. Drawing on narrative hermeneutics, Meretoja identifies six ethical dimensions that support storytelling: fostering the imagination of alternative futures, enabling self-understanding, facilitating nuanced comprehension of others, reflecting transitional spaces between narratives, enhancing perspective-taking, and serving as ethical inquiry [88]. Meretoja argues that narratives are not ethically neutral but are influenced by historical and cultural contexts, capable of both reinforcing dominant ideologies and encouraging critical change [88]. This ethical framework emphasizes the relational nature of storytelling and the responsibilities associated with narrative acts, particularly in research, education, and public discourse. By developing a theory in which storytelling affects moral imagination and fosters dialogical engagement, Meretoja views narrative as a space for reflective ethical practice and social critique [66]. All collected data, including audio recordings and written transcripts, were securely stored and later destroyed after the analysis was completed [89].
Participants, especially members of HIV-serodiscordant couples, responded to open-ended questions designed to complement a structured psychiatric interview. These questions explored condom use in sexual relationships, previous partnerships, educational background, and parental dynamics, topics previously identified in structured surveys as important factors influencing behavioral patterns and psychoeducational backgrounds (see Appendix; see [90]).
Meeting transcripts were systematically reviewed to identify key themes and subthemes, following Braun and Clarke’s six-phase approach to thematic analysis [91]. The process started with familiarization, during which transcripts were carefully read and re-read to ensure a deep engagement with the data. Initial codes were created to identify meaningful patterns, which were then systematically grouped into broader themes and subthemes [69]. Narratives were analyzed within the established frameworks of BPD, ensuring a structured and rigorous approach to thematic categorization. Thematic clustering was performed only when BPD was thoroughly confirmed as the main factor influencing the observed behaviors and narratives, maintaining validity and coherence in the analysis [92].
3. Results
3.1. Results from the Survey (Phase 1)
Regardless of one partner’s HIV status, we found that a high level of education in either partner was associated with a lower frequency of using sexual precautions (e.g., condoms) during interactions that carried a risk of HIV transmission. Women from higher social class families used sexual prevention less often compared to those from modest social backgrounds. When both partners had problematic relationships with their parents, there was a decrease in the use of HIV prevention methods. Among the couples assessed, HIV-negative women exhibited behavioral traits indicative of BPD, along with histories of chronic depression and child abuse or neglect (Table 2).
The analysis illustrates how educational and relational factors shape condom use among HIV-serodiscordant couples. Men with lower education and women whose education was lower than their HIV-positive partners showed higher adherence to prevention. Women with Samos Syndrome from disadvantaged backgrounds also demonstrated greater condom use than those from higher social classes. Additionally, couples reporting at least one positive parental relationship were more consistent in using protection. These findings illustrate how structural disparities and familial dynamics influence sexual risk-reduction behaviours in serodiscordant contexts (Table 3; Figure 1).
3.2. Qualitative Narrative Analysis (Phase 2)
Prototypical narratives in women with BPD and in HSDHC are presented here, gathered through unobtrusive ethnographic methods and informal interviews that use both structured and unstructured open-ended questions.
3.2.1. First Theme: Attraction to Partners with Complex Health or Behavioural Profiles (ICD-10: BPD Instability in Interpersonal Relationships)
This theme involved conflicting and dependent relationships between HIV-negative women with BPD and partners with complex health or behavioural profiles, aiming to improve their low self-esteem. The explored path included becoming more affectionate with their stable partners and considering whether this pattern could lead to future issues such as problematic relationships, HIV or COVID-19 infection, abuse and violence from aggressive partners, and the development of potential post-traumatic stress disorder (PTSD). More women became HIV-infected, and some experienced feelings of remorse, self-blame, and suicidal thoughts. The typical narrative is: “I tend to fall in love and feel particularly drawn to partners with difficulties that I believe I can solve.”
3.2.1.1. Subtheme: Low Self-Esteem and the Pursuit of Love (ICD-10: Instability in Self-Image)
The typical narratives are, “During childhood, I suffered from abuse and violence. Now I have unprotected sexual relationships with my partner with HIV to show that love is possible,” and “I do not protect myself from the virus of my partner for fear he rejects me.”
3.2.1.2. Subtheme: A Relationship Regardless (ICD-10: Low Self-Esteem)
Common among women with a history of trauma, violence, and BPD is the tendency to blame themselves when relationships with partners fail. These women often invest emotionally in male partners, and when those partners do not reciprocate, they feel guilty and abandoned. In response, they may accommodate their partners’ requests. However, some of these requests might be abusive or, in cases involving infectious diseases, include asking the women not to protect themselves from contagious illnesses, such as requesting they refrain from using condoms. The typical narrative is: “Although my romantic relationship has problems and my partner is HIV positive and has issues with drugs, I do not dare to abandon him. I also feel responsible if the relationship does not work.”
3.2.1.3. Set Theory and Path Analysis
In the second part of this study, we conducted a path analysis to build a theoretical model from our findings. Each narrative was then coded using a structured matrix using a 3-point ordinal scale (0 = absent, 1 = moderate presence, 2 = strong presence) and a 2-point binary scale (0=absent; 1=present) (Table 4).
From these variables we hypothesised the path as the following: (1) Trauma History (TH) → Low Self-Esteem (LSE) → Partner Complexity Attraction (PCA) → Unprotected Intimacy (UPI) → HIV Infection Outcome (HIV+); (2) Low Self-Esteem (LSE) → Self-Blame and Guilt (SBG) → Suicidal Ideation (SI); and (3) Partner Complexity Attraction (PCA) → Accommodation of Risk (AR) → HIV Infection Outcome (HIV+). This structure enables the estimation of beta coefficients for each path, allowing for the testing of directional influence while preserving the narrative logic.
The qualitative phase revealed emotionally intense narratives among HIV-negative women with Borderline Personality Disorder (BPD) in serodiscordant relationships, organized into three thematic clusters aligned with ICD-10 criteria. The central theme, attraction to partners with complex health or behavioural profiles, reflected emotional dependency and idealization, often rooted in unresolved trauma and low self-worth (β = +0.67). The subtheme low self-esteem and the pursuit of love involved trauma reenactment, with unprotected sex used to express affection and avoid rejection (β = +0.58). The third cluster, a relationship regardless, captured persistence in harmful partnerships driven by fear of abandonment and self-blame (β = +0.41). These relational patterns were linked to increased risk of HIV/COVID-19 infection (β = +0.24) and severe psychological consequences, including PTSD and suicidal ideation (β = +0.42), illustrating the deep interplay between symbolic intimacy, relational vulnerability, and mental health outcomes (Figure 3).
3.3.1. Second Theme: Risk-Taking Behaviors (ICD-10: Sex at Risk)
A characteristic of this subtheme is that women with BPD tend to engage in various risk-taking (sexual) behaviors, showing a clear understanding of the health risks (such as HIV, COVID-19, and sexually transmitted diseases), social consequences (like unwanted pregnancies and exploitation by abusive partners), and psychological effects (including regret and guilt after risky behaviors). The typical narrative often becomes, “I have a partner with AIDS, but we usually do not use protection because we love each other.”
3.3.1.1. Subtheme: An Impulsive Attitude Toward Risk and Limited Ability to Predict or Prevent Risks (ICD-10: Unpredictable Actions)
In this subtheme, we identified several risky behaviors that could influence the spread of infectious diseases and affect the health of individuals with BPD. Among those with a history of trauma and low mood, we observed a combination of impulsive actions and decreased awareness of their consequences. The typical stories we collected included, “During childhood, I experienced abuse and violence. Now I have unprotected sexual relationships with my partner with HIV to show that love is possible.”
3.3.1.2. Set Theory and Path Analysis
In the second part of the study, we conducted a path analysis to build a theoretical model from our findings. Each narrative was then coded using a structured matrix using a 3-point ordinal scale (0 = absent, 1 = moderate presence, 2 = strong presence) and a 2-point binary scale (0=absent; 1=present) (Table 5).
Path relationships hypothesized were the following: (1) TH → LM → IMP: Trauma influences mood, which increases impulsivity; (2) IMP → RTSB: Impulsivity drives risk-taking sexual behavior; (3) RTSB → UPI → GR: Risk behavior leads to unprotected intimacy, resulting in guilt/regret (4) LM → ARW → GR: Low mood may reduce awareness of risk, which affects psychological outcomes (5) ARW moderates RTSB → GR: Higher awareness may buffer or intensify guilt.
Narratives from HIV-negative women with BPD in serodiscordant relationships illustrate a central theme of Risk-Taking Behaviors (β = +0.50), where sexual risk is consciously accepted as an expression of emotional loyalty. This paradoxical fusion of love and self-endangerment is reinforced by the subtheme Impulsive Attitude Toward Risk (β = +0.52), linking trauma histories and emotional dysregulation to symbolic acts of intimacy. Unpredictable Actions (β = +0.39) further reflect erratic behaviors that heighten vulnerability. These patterns culminate in Health, Social, and Psychological Effects (β = +0.50), forming a biopsychosocial cascade of illness, relational instability, and emotional distress rooted in unresolved trauma (Figure 5).
3.3.2. Third theme: Role Confusion (ICD-11: Inability to Maintain Close and Mutually Satisfying Relationships)
3.3.2.1. Subtheme: Replacing Empathetic Interactions with Overinvolved Relationships (ICD-11: Issues in Functioning Related to Aspects of the Self and Self-Direction)
We observed this pattern among some professionals with BPD in healthcare who became enmeshed in their relationships with HIV+ clients. To explore the depth of the patients’ suffering, counter-transference often shifted into romantic love, risking the professional relationship due to emotional involvement. The common narrative was, “I fell in love with a person in my care because of my profession (e.g., a client or patient) who had some physical or psychological issue and was COVID-19/HIV positive.”
3.3.2.2. Subtheme: Replacing Empathetic Interactions with Overinvolved Relationships ((ICD-11: Lack of Accuracy About One’s Strengths and Limitations)
In women with BPD, there appears to be a tendency to have limited foresight about the long-term effects of romantic love. To build a satisfying relationship from the beginning, impulsiveness in choosing partners often leads to falling into violent relationships. However, these traits are evident from their very first encounters. We observed that they tend to underestimate the risks posed by others, making some women with BPD highly vulnerable to exploitation and violence from their partners. The typical narration goes, “I tend to fall in love with persons I see as needy or have AIDS, even if I get stuck in challenging stories or the classic ‘lost cause.’ These relationships make me feel helpful,” “Although my romantic relationship has problems and my partner is HIV positive and has issues with drugs, I do not dare to leave him. I also feel responsible if the relationship does not work,” “The more a person has a particular problem (e.g., physical, social, mental), the more I feel fatally attracted to him as I feel I could help improve him.”
3.3.2.3. Set Theory and Path Analysis
In the second part of Phase 2 we conducted a path analysis to build a theoretical model from our findings. Each narrative was then coded using a structured matrix using a 3-point ordinal scale (0 = absent, 1 = moderate presence, 2 = strong presence) and a 2-point binary scale (0=absent; 1=present) (Table 6).
The paths were hypothesized and explained as following: (1) TH → LM → RCT: Trauma history contributes to low mood, which increases susceptibility to romantic counter-transference; (2) RCT → RF → RE: Emotional overinvolvement leads to rescue fantasies, which reinforce entrapment in dysfunctional relationships; (3) LM → IRA → RE: Depressive symptoms impair risk appraisal, increasing vulnerability to exploitation, (4) RF → BER → RE: Rescue fantasies erode boundaries, escalating relational enmeshment and entrapment; (5) IRA moderates RF → RE: Accurate risk appraisal may mitigate or exacerbate the effects of rescue-driven relational entrapment.
The study developed two hypothesised pathways to illustrate how relational and psychological mechanisms contribute to health risk exposure in women with borderline personality disorder (BPD). The first pathway links impulsivity (IPS) to idealisation of fragile romantic partners (RFRI), fostering perceived responsibility (PRR), which leads to relational instability (RI) and increased health risk exposure (HRE). The second pathway focuses on emotional overinvolvement (EOI) in caregiving roles, where excessive investment results in role confusion (RI) and similarly heightens HRE. Path modelling illustrates RI and EOI as the strongest predictors of health risk (β > 0.80), supporting the ICD-11’s view of BPD as involving impaired relational functioning and highlighting the need for clinical strategies that promote relational foresight, boundary regulation, and emotional containment (Table 7; Figure 6).
3. Discussion
The overarching themes identified suggest that women who refuse preventive measures during intimate relationships at risk of HIV infection, and consequently decline any form of preventative health behavior during these risks, often have a history of child abuse and violence. We propose that individuals with BPD, as well as anyone with a background of child abuse, violence, and neglect, may develop pathophilia (from Gr: ‘attraction to illness’), a type of parasuicidal behavior, which can be understood as a form of reduced risk protection characterized by neglect of health behaviors, increased engagement in health risks, and heightened impulsive actions that can be detrimental to their health and well-being. This includes risky sexual relationships leading to STDs, sexual promiscuity, compulsive spending (such as spending beyond one’s means and compulsive hoarding), substance abuse, neglect of health behaviors related to underlying medical conditions (like high carbohydrate intake in diabetes or a sedentary lifestyle), unhealthy lifestyles (including increased social isolation and predominantly indoor living), harmful health behaviors (like anorexia, binge eating, and binge drinking), and enduring or dependent relationships with abusive partners [93,94]. According to the ICD-10 International Classification, BPD is characterized by several aspects, including unstable interpersonal relationships and life-threatening behaviors, such as engaging in risky sexual relationships [95].
3.4.1. Theory No. 1 – BPD Is Often Comorbid with Dependent Personality Disorder
Regarding abusive relationships, which can be psychologically or physically harmful, women with BPD may show intense dependence on others, swinging between the fear of abandonment that drives them to form all-consuming, intense relationships and the fear of being controlled by others, which causes them to end important relationships [96]. The ‘relational addiction’ some women with BPD experience can become so extreme that they stay in abusive relationships, as they admit, because they want to feel helpful to their male partner, who might have social, emotional, or physical issues [97]. ‘‘Interpersonal dependence’ describes the phenomenon of individuals who exhibit a notable level of reliance and a lack of individuality toward another person with whom they have romantic relationships [76]. Because of this emotional reliance, they may sometimes go so far as to give up any independence and endure the heaviest sacrifices of their interests [98]. We suggest that dependent personality disorder is often present alongside BPD in women, characterized by a persistent and exaggerated dependence on others for emotional and physical support, along with a fear of separation. People with DPD often act meek, clingy, and subservient; it usually begins in early adulthood and appears in various situations, often linked to unsatisfactory social interactions [99]. In this context, romantic relationships are often characterized by intense interpersonal conflicts. For women with BPD who have experienced past abuse, these conflicts may unconsciously follow patterns established in previous traumatic relationships, reinforcing cycles of emotional distress and instability. Conflicts in these relationships often lead to increased suicidal ideation, especially during threats of abandonment. In the most temporary cases, parasuicidal sexual behaviors in women with BPD occur during opportunistic sexual encounters with unfamiliar individuals, sex for money to buy drugs, prostitution, or consensual encounters with people who might likely have STIs [103]. Similarly, BPD health behaviors during transmissible pandemics tend to create paradoxical, unprotected social relationships at risk for contagion [77]. There is a neglect of primary prevention, ignoring common sense, and a decreased concern about pandemic spread or a downgrading of awareness campaigns [103].
3.4.2. Theory No. 1 – BPD Is Often Comorbid with Self-Defeating Personality Disorder
BPD relational pathologies recall Buchli’s concept of existential aphasia, asceticism, and anorexia of life [76]. In her book Women Who Love Too Much, Robin Norwood highlights certain characteristics of relational addiction when she suggests that some women love their ideal partner more than they love their actual partner in the relationship (as he is) [100]. According to Norwood, these women with BPD seem to seek emotional pain through violent or abusive spouses; perhaps they tend toward sadness, which they try to combat with the thrill of a shaky love connection [101].
We therefore propose that BPD is comorbid with the DSM-III-R definition of self-defeating personality disorder, which is characterized by a persistent pattern of self-defeating behaviors that begins in early adulthood and continues across various circumstances [102]. The individual in this case, a woman with BPD, often avoids or sabotages enjoyable experiences, is attracted to situations or relationships where she would suffer, and prevents others from helping her. This is indicated by at least five of the following: (1) chooses people and circumstances that lead to disappointment, failure, or mistreatment, despite better options being available; (2) disapproves of or blocks others’ efforts to offer help; (3) reacts to positive events (e.g., a new achievement) with sadness, regret, or behaviors that cause suffering (e.g., an accident); (4) provokes angry or rejecting responses from others and then feels humiliation, defeat, or pain (e.g., publicly ridicules a spouse, provoking anger, and later feels devastated); (5) declines chances for joy or hesitates to admit she is having a good time, even though she can enjoy herself and has enough social skills; (6) cannot complete tasks vital to her goals, despite having shown the ability to do so (e.g., helps classmates with writing papers but cannot write her own); (7) is indifferent to or rejects those who consistently treat her well; (8) engages in excessive self-sacrifice that is not asked for by those benefiting from it; (9) often avoids or undermines pleasurable experiences, denies herself opportunities for fun, or hesitates to admit she is enjoying herself [80]. In another of her bestselling books, *Daily Meditations for Women Who Love Too Much, Robin Norwood introduces the concept of ‘relational dependence,’ suggesting that for some women (herein, with BPD), the dangerous risks involved in a relationship can include the possibility of contracting AIDS through casual sexual contact. According to Norwood, this risk is part of the pursuit of the perfect partner whom the woman aims ‘to change’ or ‘redeem’ through her self-sacrifice, although ‘the lover’ might also be described as ‘wrong partner, uncaring person, and emotionally unavailable guy’ [104].
3.4.3. Theory No. 3: BPD Is Often Comorbid with Complex PTSD
Dusty Miller introduced the term “Trauma Re-enactment Syndrome” in his book “Women Who Hurt Themselves” to describe women who feel compelled to injure themselves [103]. Women with BPD and a history of trauma often self-harm by becoming entangled in abusive relationships because of the interpersonal or familial trauma they experienced as children. This behavior reflects the abuse they endured in childhood, repeatedly reinforcing the belief that they cannot defend themselves against harm, as no one was there to protect them during their adolescence [104].
BPD relationships quickly evolve from superficial acquaintances to deep intimacy [83]. Women with BPD show distinct traits in their relationships, displaying anxious attachment behaviors such as demanding compassion or help, clinging, and watching for closeness [105]. According to another study, young women with BPD are more likely to have engaged in informal relationships, have had more sexual partners in the past year, and experience an earlier start to sexual activity. [106]. They are also more likely to experience poorer overall health, engage in risky relationships during their first sexual encounter, and participate in non-consensual sexual activity [106].
The findings from other researchers’ interpretative phenomenological analyses highlight the gap between the lived experience of self-harm as a way to manage emotions and its classification as a dangerous behavior. Therefore, emphasizing the risks of self-harm may not effectively prevent it [107]. Based on our data, we suggest that the quality of early bonds between children and their parents or caregivers influences individuals to endorse pro-life behaviors throughout their lives, while also helping them develop the skills necessary to evaluate personal risks, health risks, and risks from others [108].
Additionally, we agree with other authors that risk behavior in BPD and its assessment are emotionally dissociated through altered cognitive and metacognitive processes [109]. Altered mentalization processes have been documented in the BPD literature [110]. The consequence is that women with BPD experience some impairment in reality testing related to self-preservation against harm and dangerous events, thereby risking their safety and health by underestimating dangers and overestimating safety [111]. Therefore, we assert that chaotic relationships in BPD—including sexual relationships at risk of HIV transmission—represent a form of Complex Post-Traumatic Stress Disorder (CPTSD). This condition is characterized by re-enacting past abusive relationships and a co-occurring dissociative state, which dulls the ability to accurately assess reality, especially regarding the prevention of harmful behaviors—including sexually transmitted diseases.
Therefore, some symptoms of ICD-11 for CPTSD include that individuals may re-experience traumatic events, such as relationships, in the present moment, actively avoid both internal and external reminders of trauma, exhibit a heightened sense of current danger through hypervigilance and hyperarousal (also symptoms of PTSD), struggle to regulate their emotions—experiencing excessive or insufficient emotional activation—hold a persistent negative view of themselves, and face challenges in forming and maintaining interpersonal relationships [112]. Although the comorbidity of CPTSD and BPD is debated and generally not accepted [113]. Women with BPD carry lingering effects from past traumatic relationships into new ones, often using these relationships as a way to escape their original trauma. They go through stages of intense emotions, dissociation, passive acceptance of traumatic experiences, and sometimes re-enact trauma and violence with substitute partners in both stable and casual relationships. This pattern increases their risk of contracting sexually transmitted diseases from occasional encounters in regular relationships.
3. Conclusions
BPD is a common finding in both inpatient and outpatient psychiatric settings. Although efforts are made to study this condition thoroughly, many aspects often go unnoticed in routine psychiatric assessments, such as how women with BPD manage their sexual health, maintain stable relationships, and engage in health-promoting behaviors. Our findings confirm that self-defeating health behaviors should be considered a key element in diagnosing BPD, and targeted assessments should be included when reporting any vulnerabilities women with BPD may have related to their sexual lives and stable relationships. As demonstrated in the current study, by analyzing romantic relationships at risk of HIV transmission, we suggest that BPD coexists with dependent personality disorder, self-defeating personality disorder, and complex PTSD. These conditions tend to appear during romantic relationships, which pose health risks for the female partner with BPD.
4. Limitations
This study has several limitations. The first relates to the characteristics of qualitative and exploratory research findings, which are closely tied to the practice settings. Therefore, the results are primarily transferable but not generalizable. The second aspect concerns the nature of the phenomena observed and the conclusions drawn from our interpretations. Although other studies support our findings, ongoing debates about the comorbidities in BPD continue, with some authors tending to separate them based on specific categorical models. Finally, we developed our theories by retrospectively reviewing our past findings and did not verify the accuracy of our conclusions with major stakeholders.
Author Contributions
Conceptualization, Carlo Lazzari; methodology, Carlo Lazzari and Jon Rees; validation, Carlo Lazzari, Yitka Graham, and Rebecca Owens; formal analysis, Carlo Lazzari; investigation, Carlo Lazzari and Jon Rees; resources, Carlo Lazzari; data curation, Jon Rees; writing—original draft preparation, Carlo Lazzari; writing—review and editing, Yitka Graham and Rebecca Owens; visualization, Jon Rees; supervision, Carlo Lazzari; project administration, Carlo Lazzari; funding acquisition. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical review and approval were waived for this study because all reported narratives were modified, paraphrased, and altered to comply with privacy and confidentiality requirements. The survey data presented in this manuscript refer to results from previous research phases that were conducted separately from the current study and had already obtained independent ethical approval.
Informed Consent Statement
Informed consent was waived for this study because all reported narratives were modified, paraphrased, and altered to comply with privacy and confidentiality requirements. The survey data presented in this manuscript derive from previous research phases that were conducted separately from the current study and had already obtained independent informed consent under their respective ethical approvals.
Data Availability Statement
Data is unavailable due to privacy or ethical restrictions.
Acknowledgments
The authors acknowledge their colleagues and teams that worked with the target population.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AIDS | Acquired Immunodeficiency Syndrome |
| BPD | Borderline Personality Disorder |
| COVID-19 | Coronavirus Disease 2019 |
| CPTSD | Complex Post-Traumatic Stress Disorder |
| DPD | Dependent Personality Disorder |
| HIV | Human Immunodeficiency Virus |
| HSDHC | HIV Serodiscordant Heterosexual Couples |
| NPC | Non-Prevention Couples |
| SDPD | Self-Defeating Personality Disorder |
| STD | Sexually Transmitted Diseases |
Appendix A
Semi-structured Interview Questionnaire: Samos Syndrome and Relational Health Behaviors
1. Educational Status and Relational Dynamics
- What level of education have you completed?
- What level of education has your partner completed?
- How do differences in education between you and your partner affect decisions about condom use?
- Have you ever felt tension or imbalance in your relationship because of differences in education or status?
Do you feel that educational differences influence how you and your partner communicate or trust each other?
2. Female Education and Relational Agency
- In your experience, how does a woman’s education affect her role in a relationship?
- Have you ever been in a relationship where the woman was more educated than the man? If so, how did that affect the relationship?
- When the woman is more educated, do you think it becomes easier or harder to discuss and agree on using condoms?
- Have you ever felt uncomfortable or inferior in a relationship because of differences in education?
3. Social Disadvantage and Vulnerability
- What was your family’s financial situation like when you were growing up?
- Do you think coming from a disadvantaged background affects how you approach romantic relationships?
- Have you ever felt less confident or more vulnerable in a relationship because of your social background?
- Do you think people from disadvantaged backgrounds are more likely to take risks in relationships?
4. Parental Relationship Quality and Relational Templates
- How would you describe your relationship with your parents during your childhood?
- How would you describe your partner’s relationship with their parents?
- Do you think your relationship with your parents affects how you trust others in adulthood?
- Have you noticed that your childhood experiences influence your decisions about sexual health, like condom use?
5. Protective Factors and Resilience
- What parts of your upbringing helped you build healthy relationships as an adult?
- Do you think having a good relationship with your parents helped you avoid unhealthy relationship patterns?
- What helps you feel safe and respected in a relationship?
- Can you think of a time when you or your partner made a choice to protect your health during a relationship?
References
- Lazzari C, Masino MA. Health psychology and philosophy e. Milan: Libreriauniversitaria.it; 2015. [Italian: Psicologia e filosofia della salute] https://www.libreriauniversitaria.it/psicologia-filosofia-salute-lazzari-carlo/libro/9788862926478.
- Lazzari C, Costigliola P. Can we stop sexual transmission of AIDS?. Bologna: Pitagora; 1993. [Italian: Si può arrestare la trasmissione sessuale dell’AIDS?] https://www.ibs.it/sesso-aids-si-puo-arrestare-libro-carlo-lazzari-paolo-costigliola/e/9788837106782.
- Short SE, Mollborn S. Social determinants and health behaviors: conceptual frames and empirical advances. Curr Opin Psychol. 2015;5:78–84. [CrossRef]
- Munro S, Lewin S, Swart T, Volmink J. A review of health behaviour theories: How useful are these for developing interventions to promote long-term medication adherence for TB and HIV/AIDS? BMC Public Health. 2007;7:104. [CrossRef]
- Skinner CS, Tiro J, Champion VL. Background on the health belief model. In: Glanz K, Rimer BK, Viswanath K, editors. Health behavior: Theory, research, and practice. 5th ed. San Francisco: Jossey-Bass/Wiley; 2015. p. 75–94. https://psycnet.apa.org/record/2015-35837-005.
- Andrus MR, Roth MT. Health literacy: a review. Pharmacotherapy. 2002;22(3):282–302. [CrossRef]
- World Health Organization (WHO). Living with HIV when one partner is positive and the other is negative [Internet]. Geneva: World Health Organization; 2024 [cited 2024 Jun 10]. Available from: https://www.who.int.
- Lazzari C, Rabottini M. Samos syndrome, borderline personality disorder and pathophilia: why we cannot stop pandemics. Int J Psychiatry Res. 2022;4:22–6. [CrossRef]
- Lazzari C, Di Bari MA, Costigliola P, De Ronchi D, Volterra V, Chiodo F. Deliberate HIV infection as a way of committing suicide. Italian Journal of Suicidology 1993; 1:161.
- Lazzari C, Costigliola P, Di Bari MA, De Ronchi D, Volterra V, Chiodo F. AIDS has an increasing diffusion within the heterosexual population. AIDS Patient Care. 1994;8:106. [CrossRef]
- Lazzari C. Samos syndrome, women with borderline personality disorder and risk for sexually transmitted infections and HIV: their role during pandemics. Curr Innov Dis Health Res. 2023;7:12–21. [CrossRef]
- Lazzari C. A guide to the psychological assistance of the HIV positive and AIDS patient. Bologna: Patron; 1992. (Italian: Guida all’assistenza psicologica del paziente HIV positive e con AIDS). https://www.ibs.it/guida-all-assistenza-psicologica-del-libro-carlo-lazzari/e/9788855522311.
- Lazzari C, Costigliola P. Sex and AIDS. Can we stop sexual transmission of AIDS? Bologna: Piagora; 1993. (Italian: Sesso e AIDS. Si puo’ arrestare la transmission sessuale dell’AIDS?) https://www.ibs.it/sesso-aids-si-puo-arrestare-libro-carlo-lazzari-paolo-costigliola/e/9788837106782.
- Zambaco Pacha DA. Voyage chez les lépreux. Paris: Masson; 1880.
- Ceronetti G. Il Silenzio del Corpo. Milano: Adelphi; 1979. (Engl: The Silence of the Body).
- UNAIDS. Global HIV & AIDS statistics — 2023 fact sheet [Internet]. Geneva: UNAIDS; 2023 [cited 2025 Jun 19]. Available from: https://www.unaids.org/en/resources/fact-sheet.
- World Health Organization. HIV/AIDS: Key facts [Internet]. Geneva: WHO; 2023 [cited 2025 Jun 19]. Available from: https://www.who.int/news-room/fact-sheets/detail/hiv-aids.
- Centers for Disease Control and Prevention. HIV Basics [Internet]. Atlanta: CDC; 2023 [cited 2025 Jun 19]. Available from: https://www.cdc.gov/hiv/basics/.
- HIV.gov. How is HIV transmitted? [Internet]. 2023 [cited 2025 Jun 21]. Available from: https://www.hiv.gov/hiv-basics/overview/about-hiv-and-aids/how-is-hiv-transmitted.
- Centers for Disease Control and Prevention. How HIV Spreads [Internet]. 2024 [cited 2025 Jun 21]. Available from: https://www.cdc.gov/hiv/causes/index.html.
- Terrence Higgins Trust. How HIV is transmitted [Internet]. [cited 2025 Jun 21]. Available from: https://www.tht.org.uk/hiv/about-hiv/how-hiv-transmitted.
- Chapman J, Jamil RT, Fleisher C. Borderline personality disorder [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 [cited 2023 Oct 2]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430883/.
- Linehan MM. Cognitive-Behavioral Treatment of Borderline Personality Disorder. New York: Guilford Press; 1993.
- Cattaneo N, Rossi R, Lanfredi M, Cattaneo A. Borderline personality disorder and childhood trauma: exploring the affected biological systems and mechanisms. BMC Psychiatry. 2017;17:221. [CrossRef]
- Salavati M, Selby EA. Childhood maltreatment and borderline personality disorder. In: Theories of Borderline Personality Disorder. Cham: Springer; 2025. p. 57–94.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: APA; 2013.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed, Text Revision (DSM-5-TR). Washington, DC: APA; 2022.
- World Health Organization. (1992). The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines. Geneva: WHO.
- World Health Organization. (2019). International Classification of Diseases for Mortality and Morbidity Statistics (11th Revision). Retrieved from https://icd.who.int.
- American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.). Arlington, VA: APA Publishing.
- Creswell JW, Plano Clark VL. Designing and Conducting Mixed Methods Research. 3rd ed. Thousand Oaks, CA: Sage Publications; 2018.
- Creswell JW, Plano Clark VL. Designing and conducting mixed methods research. 3rd ed. Thousand Oaks (CA): Sage Publications; 2017.
- Fetters MD, Curry LA, Creswell JW. Achieving integration in mixed methods designs—principles and practices. Health Serv Res [Internet]. 2013 Dec [cited 2025 Jun 19];48(6 Pt 2):2134–56. Available from: https://bpb-us-w2.wpmucdn.com/campuspress.yale.edu/dist/3/2905/files/2022/04/Fetters-Curry-Creswell-Integration-MM-HSR-2013.pdf.
- O’Cathain A, Murphy E, Nicholl J. Three techniques for integrating data in mixed methods studies. BMJ [Internet]. 2010 Sep 17 [cited 2025 Jun 19];341:c4587. Available from: https://www.bmj.com/content/341/bmj.c4587.
- Doyle L, Brady A-M, Byrne G. An overview of mixed methods research. J Res Nurs [Internet]. 2016 Dec [cited 2025 Jun 19];21(8):623–35. [CrossRef]
- Johnson RB, Onwuegbuzie AJ, Turner LA. Toward a definition of mixed methods research. J Mixed Methods Res. 2007;1(2):112–33.
- Lumivero. NVivo Qualitative Data Analysis Software [Internet]. Version 14. Denver, CO: Lumivero; 2023 [cited 2025 Jun 20]. Available from: https://lumivero.com/products/nvivo/.
- MedCalc Software Ltd. MedCalc Statistical Software version 23.0.8. Ostend, Belgium: MedCalc Software Ltd.; 2024. Available from: https://www.medcalc.org.
- Riessman CK. Narrative methods for the human sciences. Thousand Oaks: Sage Publications; 2008.
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101:. [CrossRef]
- Terry G, Hayfield N, Clarke V, Braun V. Thematic analysis. In: Willig C, Stainton-Rogers W, editors. The SAGE Handbook of Qualitative Research in Psychology. 2nd ed. London: SAGE; 2017. p. 17–37. [CrossRef]
- Charmaz K. Constructing grounded theory. 2nd ed. London: Sage Publications; 2014. [CrossRef]
- Hammersley M, Atkinson P. Ethnography: Principles in practice. 3rd ed. London: Routledge; 2007.
- Williams B. Hybrid qualitative analysis: Integrating thematic, narrative, and ethnographic approaches. Qual Health Res. 2023;33(4):512–26. [CrossRef]
- Creswell JW. Qualitative inquiry and research design: Choosing among five approaches. 3rd ed. Thousand Oaks: Sage Publications; 2013.
- Dixon-Woods M, Agarwal S, Jones D, Young B, Sutton A. Synthesising qualitative and quantitative evidence: a review of possible methods. J Health Serv Res Policy. 2005;10(1):45–53. [CrossRef]
- Doyle L, Brady A-M, Byrne G. An overview of mixed methods research. J Res Nurs [Internet]. 2016 Dec [cited 2025 Jun 19];21(8):623–35. [CrossRef]
- Johnson RB, Onwuegbuzie AJ, Turner LA. Toward a definition of mixed methods research. J Mixed Methods Res. 2007;1(2):112–33.
- Lumivero. NVivo Qualitative Data Analysis Software [Internet]. Version 14. Denver, CO: Lumivero; 2023 [cited 2025 Jun 20]. Available from: https://lumivero.com/products/nvivo/.
- Patton MQ. Qualitative research & evaluation methods. 4th ed. Thousand Oaks (CA): Sage Publications; 2015.
- Donenberg GR, Wilson HW, Emerson E, Bryant FB. Understanding HIV-risk behavior among adolescents in psychiatric care: links to child abuse and psychiatric disorders. J Am Acad Child Adolesc Psychiatry. 2005;44(8):778–85. [CrossRef]
- Jaccard J, Dodge T, Dittus P. Parent-adolescent communication about sex and birth control: a conceptual framework. New Dir Child Adolesc Dev. 2002;97:9–42. [CrossRef]
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101.
- Gunderson JG, Lyons-Ruth K. BPD’s interpersonal hypersensitivity phenotype: a gene-environment-developmental model. J Pers Disord. 2008;22(1):22–41. [CrossRef]
- George T. Structured Interview | Definition, Guide & Examples. Scribbr. 2022 Jan 27 [cited 2025 Jun 20]. Available from: https://www.scribbr.com/methodology/structured-interview/.
- Brinkmann S. Unstructured and Semi-Structured Interviewing. In: Leavy P, editor. The Oxford Handbook of Qualitative Research. Oxford University Press; 2014 [cited 2025 Jun 20]. Available from: https://academic.oup.com/edited-volume/38166/chapter/333002245.
- Schneider CQ, Wagemann C. Set-theoretic methods for the social sciences: A guide to qualitative comparative analysis. Cambridge: Cambridge University Press; 2012. [CrossRef]
- Lincoln YS, Guba EG. Naturalistic inquiry. Beverly Hills (CA): Sage; 1985. https://archive.org/details/naturalisticinqu00linc.
- Lincoln YS, Guba EG. Naturalistic inquiry. Beverly Hills (CA): Sage; 1985.
- Lincoln YS, Guba EG. The constructivist credo. New York (NY): Routledge; 2013.
- Crotty M. The Foundations of Social Research: Meaning and Perspective in the Research Process [Internet]. London: Sage Publications; 1998 [cited 2025 Jun 20]. Available from: https://uk.sagepub.com/en-gb/eur/the-foundations-of-social-research/book207972.
- Schwandt TA. The Sage Dictionary of Qualitative Inquiry [Internet]. 4th ed. Los Angeles: Sage Publications; 2015 [cited 2025 Jun 20]. Available from: https://uk.sagepub.com/en-gb/eur/the-sage-dictionary-of-qualitative-inquiry/book237361.
- Parahoo K. How to design studies and write research proposals: A guide for nursing, allied health and social care students. 1st ed. London: Elsevier; 2024. [CrossRef]
- Borsboom D, van der Maas HLJ, Dalege J, Kievit RA, Haig BD. Theory construction methodology: A practical framework for building theories in psychology. Perspect Psychol Sci. 2021;16(4):756–772. [CrossRef]
- Olobatuyi ME. A User’s Guide to Path Analysis. Lanham: University Press of America; 2006.
- Latent Variable Models | An introduction to factor, path, and structur [Internet]. Taylor & Francis. 2016. Available from: https://www.taylorfrancis.com/books/edit/10.4324/9781315643199/latent-variable-models-alexander-beaujean-john-loehlin.
- Braun V, Clarke V. Successful qualitative research: A practical guide for beginners. London: SAGE Publications; 2013. https://uk.sagepub.com/en-gb/eur/successful-qualitative-research/book233059.
- Streiner DL. Finding our way: An introduction to path analysis. Can J Psychiatry. 2005;50(2):115–122. [CrossRef]
- Maxwell JA. Using numbers in qualitative research. Qual Inq. 2010;16(6):475–482. [CrossRef]
- . Bamberg M. Narrative analysis: An integrative approach. Clark University; 2020. Available from: https://wordpress.clarku.edu/wp-content/uploads/sites/180/2020/04/OLD-Bamberg-Qualitative-Analysis-Chapter.pdf.
- Fricker M. Epistemic injustice: Power and the ethics of knowing. Oxford: Oxford University Press; 2007. [CrossRef]
- Kidd IJ, Carel H. Epistemic injustice and illness. J Appl Philos. 2017;34(2):172–190. [CrossRef]
- Blumer H. Symbolic interactionism: Perspective and method. Englewood Cliffs, NJ: Prentice-Hall; 1969. Available from: https://archive.org/details/symbolicinteract0000blum.
- Lazzari C, Nusair A, Rabottini M. Psychiatry of radicalization and terrorism in the lone wolf, children, and women: An e-ethnographic approach for analysis. Am J Psychiatry Neurosci. 2019;7(3):57–68. https://sciencepublishinggroup.com/article/10.11648/j.ajpn.20190703.12.
- Lave J, Wenger E. Situated learning: Legitimate peripheral participation. Cambridge: Cambridge University Press; 1991. Available from: https://www.cambridge.org/highereducation/books/situated-learning/6915ABD21C8E4619F750A4D4ACA616CD.
- Brown JS, Collins A, Duguid P. Situated cognition and the culture of learning. Educ Res. 1989;18(1):32–42. https://www.johnseelybrown.com/Situated%20Cognition%20and%20the%20culture%20of%20learning.pdf.
- Denzin NK. Symbolic interactionism and cultural studies. Oxford: Blackwell; 1992.
- Western J, McEllistrem B, Hislop J, Jaap A, Hope D. Vignettes as an innovative qualitative data collection tool in medical education research. Med Sci Educ. 2024;34:975–7. [CrossRef]
- Tremblay M, et al. Developing and using research vignettes to collect qualitative data from healthcare professionals: A scoping review. BMJ Open. 2022;12(1):e057095. Available from: https://bmjopen.bmj.com/content/12/1/e057095.
- Wiles R. Anonymity and confidentiality in medical research: Ethical challenges of vignette methodology. Qual Res. 2013;13(4):480–97. [CrossRef]
- Tremblay M, et al. Developing and using research vignettes to collect qualitative data from healthcare professionals: A scoping review. BMJ Open. 2022;12(1):e057095. Available from: https://bmjopen.bmj.com/content/12/1/e057095.
- Wiles R. Anonymity and confidentiality in medical research: Ethical challenges of vignette methodology. Qual Res. 2013;13(4):480–97. [CrossRef]
- Rizvi S. Using fiction to reveal truth: Challenges of using vignettes to understand participant experiences within qualitative research. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research. 2019;20(1). [CrossRef]
- Gray D, Royall B, Malson H. Hypothetically speaking: Using vignettes as a stand-alone qualitative method. In: Braun V, Clarke V, Gray D, editors. Collecting qualitative data: A practical guide to textual, media and virtual techniques. Cambridge: Cambridge University Press; 2017. p. 67–94. [CrossRef]
- Braun V, Clarke V. Reflecting on reflexive thematic analysis. Qualitative Research in Sport, Exercise and Health. 2019;11(4):589–97. [CrossRef]
- World Medical Association. Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–4. You can also access the full text via JAMA Network. [CrossRef]
- Social Work Institute. Confidentiality in HIV/AIDS counseling: Ethical considerations. London: SWI Publications; 2024. [CrossRef]
- Meretoja H. The ethics of storytelling: Narrative hermeneutics, history, and the possible. Oxford: Oxford University Press; 2018.
- Gupta BB, Mamta. Secure searchable encryption and data management. 1st ed. Boca Raton: CRC Press; 2021. [CrossRef]
- Antonini M, Pontes PS, Melo ES, Alves RS, Gir E, Sorensen W, Reis RK. Psychoeducational influences on sexual behavior in serodiscordant couples: A systematic review. BMC Public Health. 2021;21:1849. [CrossRef]
- Braun V, Clarke V. Thematic analysis: A practical guide. London: SAGE Publications; 2021. https://uk.sagepub.com/en-gb/eur/thematic-analysis/book248481.
- Byrne D. A worked example of Braun and Clarke’s approach to reflexive thematic analysis. Qual Quant. 2022;56:1391–1412. [CrossRef]
- Liggio F. Trattato moderno di psicopatologia della sessualità. Limena (PD): Libreriauniversitaria.it; 2010. ISBN: 9788862920230. Available from: https://www.libreriauniversitaria.it/trattato-moderno-psicopatologia-sessualita-liggio/libro/9788862920230. (Engl: Modern handbook of psychopathology of sexuality).
- Lazzari C, Gandolfi-Colleni G, Trallo F. Eros, sexual diseases and society. Bologna: Pitagora; 1996. ISBN: 9788837108359. Available from: https://www.lafeltrinelli.it/eros-malattie-sessuali-societa-libro-vari/e/9788837108359.
- World Health Organization. International statistical classification of diseases and related health problems. 10th revision, Fifth edition. Geneva: WHO; 2016. Available from: https://apps.who.int/iris/handle/10665/246208.
- Penati G, Cavallari G, Cella M, Salteri A. Disturbo borderline di personalità e Depressione (It: Borderline Peraonlity Disorder and depression). Proceedings from the XVIII International Conference of the Italian Society of Psychiatry, Salsomaggiore Terme (PR), 20-26 Ottobre; c1991. p. 20.
- Freud S. The psychology of love. New York: Penguin; 1991. https://www.penguin.co.uk/books/57338/the-psychology-of-love-by-sigmund-freud/9780141186030.
- Buchli E. Il mito dell’amore fatale. Milan: Baldini Castoldi Dalai; 2006. ISBN: 9788884908612. https://www.lafeltrinelli.it/mito-dell-amore-fatale-libro-enrichetta-buchli/e/9788884908612. (Italian: The myth of the fatal love).
- Simonelli A, Parolin M. Dependent personality disorder. In: Zeigler-Hill V, Shackelford TK, editors. Encyclopedia of personality and individual differences [Internet]. Cham: Springer; 2017. p. 1–11. [CrossRef]
- Norwood R. Women who love too much. London: Pocket Books; 1985. https://www.penguin.co.uk/books/358467/women-who-love-too-much-by-norwood-robin/9780099474128.
- Norwood R. Daily meditations for women who love too much. New York: Penguin; 1997. https://www.penguin.co.uk/books/356254/daily-meditations-for-women-who-love-too-much-by-robin-norwood/9781784751876.
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 3rd ed., rev. Washington, DC: American Psychiatric Association; 1987. https://archive.org/details/diagnosticstatis00amer_1.
- Miller D. Women who hurt themselves: A book of hope and understanding. New York: Basic Books; 2005. https://www.amazon.co.uk/Women-Who-Hurt-Themselves-Understanding/dp/0465045871.
- Fonagy P, Bateman AW. Mechanisms of change in mentalisation-based treatment of BPD. J Clin Psychol. 2006;62(4):411–430. [CrossRef]
- Gunderson JG. Disturbed relationships as a phenotype for borderline personality disorder. Am J Psychiatry. 2007;164(11):1637–1640. [CrossRef]
- Thompson KN, Betts J, Jovev M, Nyathi Y, McDougall E, Chanen AM. Sexuality and sexual health among female youth with borderline personality disorder pathology. Early Interv Psychiatry. 2019;13(3):502–508. [CrossRef]
- Norman H, Marzano L, Oskis A, Coulson M. “My heart and my brain is what’s bleeding, these are just cuts.” An interpretative phenomenological analysis of young women’s experiences of self-harm. Front Psychiatry. 2022;13:914109. [CrossRef]
- Lazzari C, Masino MA. Psychology and philosophy of health. Limena (PD): Libreriauniversitaria.it; 2015. ISBN: 9788862926478. Available from: Libreriauniversitaria.it.[Italian: Psicologia e filosofia della salute].
- Liotti G. Trauma, dissociation and disorganised attachment: three strands of a single braid. Psychotherapy: Theory, Research, Practice, Training. 2004;41(4):472–486. [CrossRef]
- Bateman A, Fonagy P. Mentalisation-based treatment for borderline personality disorder. World Psychiatry. 2010;9(1):11–15. [CrossRef]
- Lazzari C, Shoka A, Masiello I. Chapter 3. Maladaptive behaviors in inpatients with borderline personality disorder: A behavioral game theory explanation. In: Anderson R, editor. Borderline personality disorder: prevalence, management, options, challenges. New York: Nova Science Publishers; 2016. ISBN: 9781536102901. Available from: https://novapublishers.com/shop/borderline-personality-disorder-bpd-prevalence-management-options-and-challenges/.
- Hyland P, Shevlin M, Fyvie C, Cloitre M, Karatzias T. The relationship between ICD-11 PTSD, complex PTSD and dissociative experiences. J Trauma Dissociation. 2019;21(1):62–72. [CrossRef]
- Cloitre M. ICD-11 complex post-traumatic stress disorder: simplifying diagnosis in trauma populations. Br J Psychiatry. 2020;216(3):129–131. [CrossRef]
Figure 1.
Path analysis of the quantitative study.
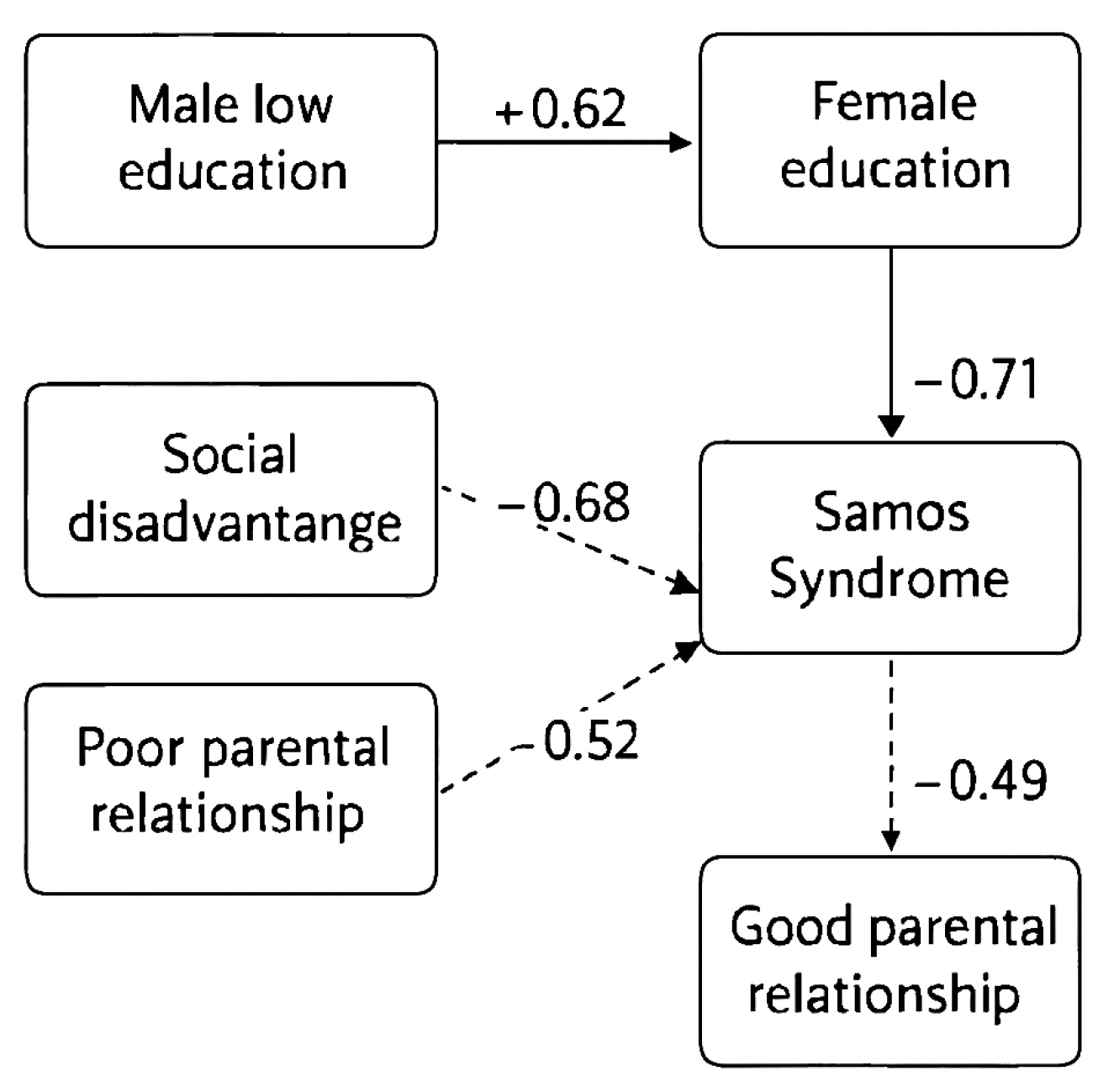
Figure 3.
Path analysis with beta coefficients.
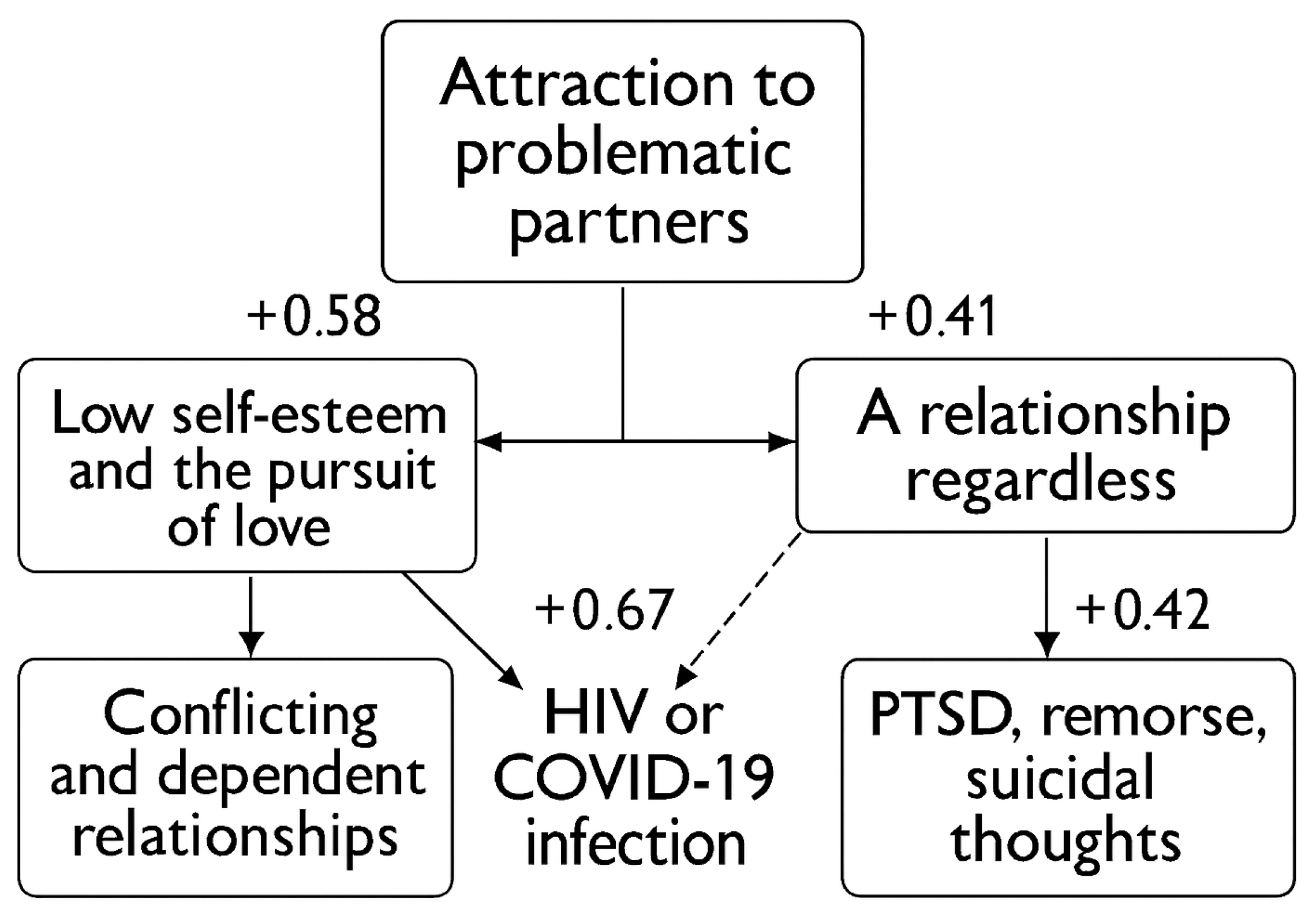
Figure 5.
Path analysis with beta coefficients.
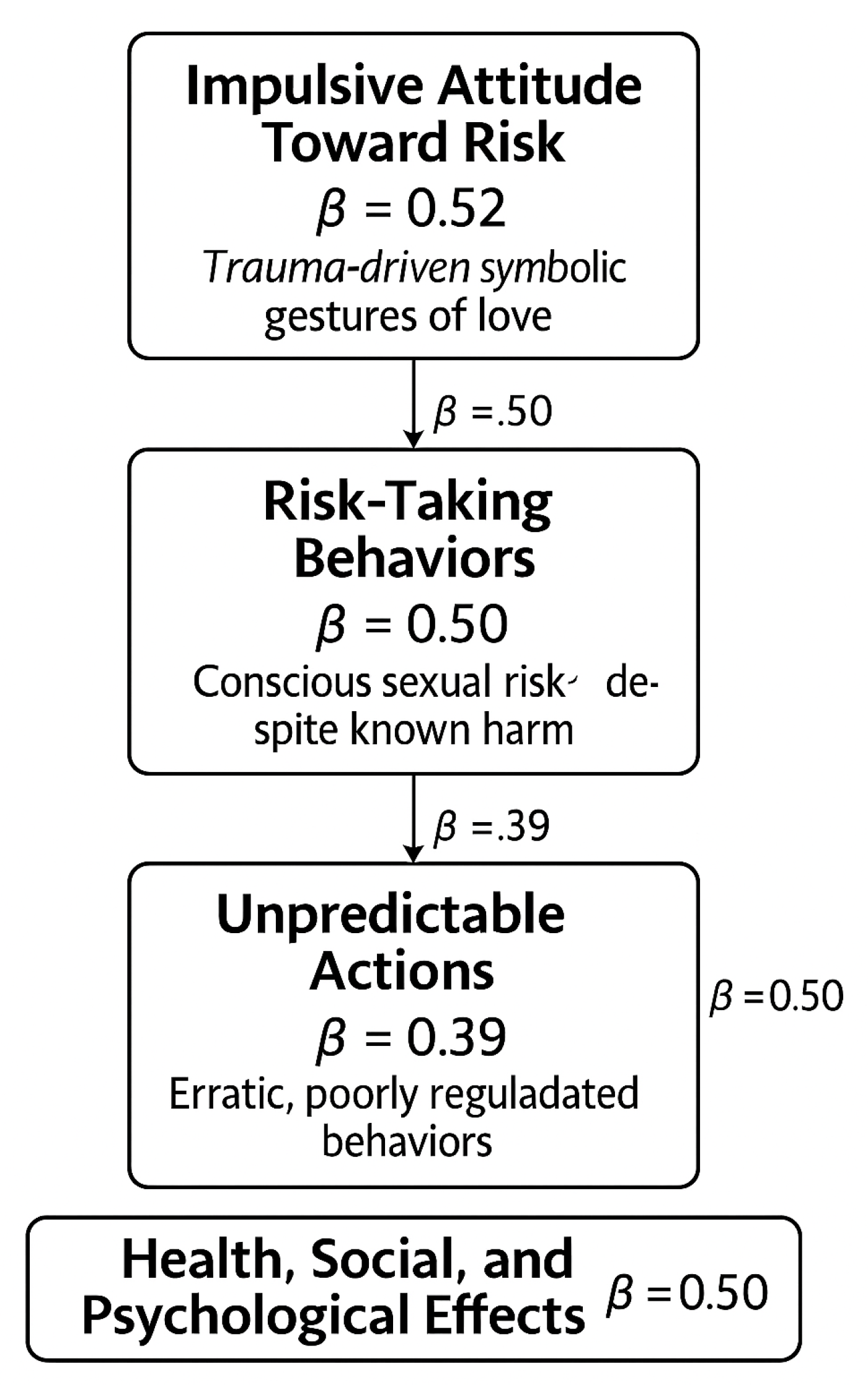
Figure 6.
Path graph with beta coefficients.
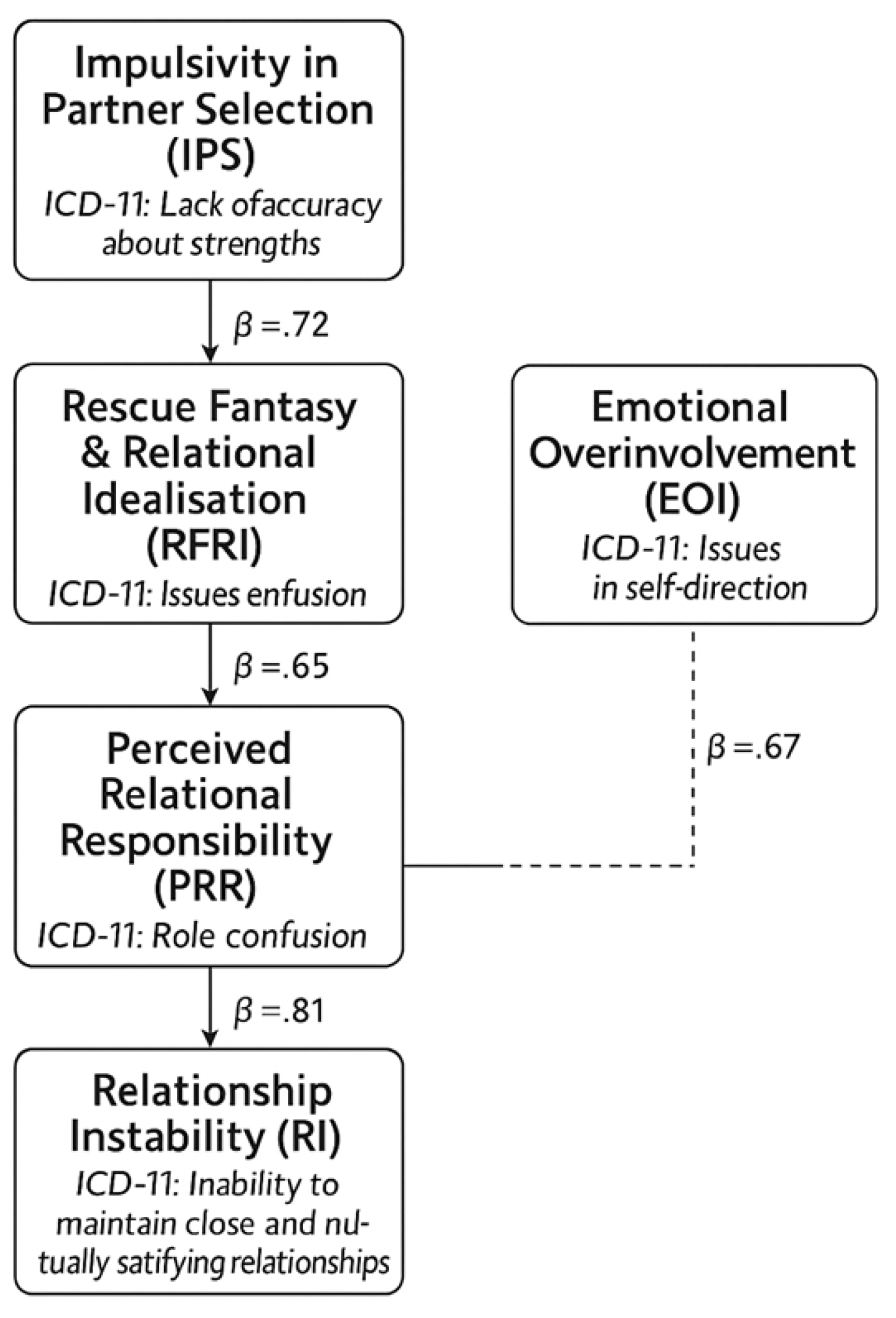

Table 1.
Borsboom et al. (2021) Theory construction stages and our naturalistic findings (see [65]).
Table 1.
Borsboom et al. (2021) Theory construction stages and our naturalistic findings (see [65]).
| Step [65] | Our phenomenological observations and grounded theory |
|---|---|
| Identify empirical phenomena | Women with BPD who are HIV-negative engaged in unprotected and consensual sexual relationships with HIV-positive male partners. |
| Formulating a prototheory through abductive reasoning | HIV sexual transmission and contagion are not always accidental, as shown by our observations in HIV-serodiscordant couples. |
| Formalize theory and phenomena | Women diagnosed with BPD who are HIV-negative and engage in consensual, unprotected sexual relationships with partners who have HIV/AIDS often report experiences of childhood trauma and abuse. |
| Checking explanatory adequacy | Disruptions in early attachment during childhood can lead to changed health behaviors throughout a person’s lifespan. |
| Assessing the overall worth of the theory | By triangulating naturalistic observations with targeted surveys, women with BPD report that early parenting attachment characterized by abusive parents is linked to decreased health prevention from childhood to adulthood, along with inverse relationships to socioeconomic variables. Notably, women with higher education and wealth exhibit fewer protective behaviors in HIV serodiscordant |
Table 2.
Descriptive characteristics of health behaviors in 175 HIV-discordant couples. Data regarding the frequency (from ‘0% to 100%’) of condom use during sexual encounters at risk of HIV transmission. Condom use frequency by sociodemographic characteristics, Outcome is the frequency of condom use during sexual encounters at risk of HIV transmission.
Table 2.
Descriptive characteristics of health behaviors in 175 HIV-discordant couples. Data regarding the frequency (from ‘0% to 100%’) of condom use during sexual encounters at risk of HIV transmission. Condom use frequency by sociodemographic characteristics, Outcome is the frequency of condom use during sexual encounters at risk of HIV transmission.
| Characteristic | Group Comparison | Condom Use (%) | 95% CI | p-value |
|---|---|---|---|---|
| Male partner education | Elementary/Middle vs. High School/University | 86% vs. 58% | [79.9–92.1] vs. [49.9–66.1] | p < 0.001 |
| Female partner education | Same/Higher vs. Lower than male partner | 60% vs. 90% | [51.4–68.6] vs. [83.9–96.1] | p < 0.001 |
| Samos Syndrome background | Disadvantaged vs. Middle-high social class | 87% vs. 59% | [80.6–93.4] vs. [50.1–67.9] | p < 0.001 |
| Relationship with parents | Poor/problematic vs. Good | 40% vs. 83% | [30.6–49.4] vs. [75.4–90.6] | p < 0.001 |
Table 3.
Reinterpreted pathways linking sociodemographic factors to Samos Syndrome and condom use behavior in HIV-serodiscordant couples.
Table 3.
Reinterpreted pathways linking sociodemographic factors to Samos Syndrome and condom use behavior in HIV-serodiscordant couples.
| Pathway | Empirical Support | Behavioral Implication | Beta Coefficient (β) |
|---|---|---|---|
| Male low education → Female higher education | Condom use is higher (86%) when the male is less educated | May foster protective behavior but trigger Samos’ tension due to status incongruence | +0.62 |
| Female higher education → Samos Syndrome | Condom use is lower (60%) when a female is more educated | Reflects agency but may evoke relational dissonance and internalized inferiority | +0.71 |
| Social disadvantage → Samos Syndrome | 87% of female partners with Samos come from disadvantaged families | Core antecedent of the syndrome; fosters vulnerability and relational hypovigilance | +0.68 |
| Poor parental relationship in both partners → Samos Syndrome | Condom use drops to 40% with poor parental bonds | Weak relational templates during childhood in both partners impair trust (increased compliance to unhealthy behaviours) and health behaviour adherence (reduced health behaviours of prevention during infectious diseases) | +0.52 |
| Good parental relationship → Samos Syndrome | Condom use rises to 83% with secure parental bonds | A positive parental bond during childhood predicts increased health behaviors in adulthood. Good parental bonding is a protective factor and a buffers against syndrome emergence | −0.49 |
Table 4.
Thematic constructs and variables definitions.
| Construct Label | Description | ICD-10 Reference | Variable Type | Endogenous/Dependent (EN) or Exogenous/Independent (EX) |
|---|---|---|---|---|
| Partner Complexity Attraction (PCA) | Attraction to partners with health/behavioral difficulties | F60.3 (BPD – instability in relationships) | Binary / Ordinal (0=no attraction; 1=attraction) / partner (0=low level of difficultis; 1=medium level; 2=high level of difficulties). | Ex |
| Low Self-Esteem (LSE) | Self-deprecating beliefs, emotional dependence | F60.3 / F60.31 | Ordinal (0=very low self-esteem; 1=medium level of low self-esteem; 2=high level of low self-esteem) | Ex |
| Unprotected Intimacy (UPI) | Engagement in unprotected sex despite known risk | Z72.51 / F60.3 | Binary (0=protected; 1=unprotected) | En |
| Trauma History (TH) | Childhood abuse, violence, neglect | Z61.4 / F43.1 | Binary | Ex |
| Self-Blame and Guilt (SBG) | Internalized responsibility for relationship failure | F60.3 / F33.2 | Ordinal | En |
| Suicidal Ideation (SI) | Thoughts of self-harm or suicide | R45.81 / F32.3 | Binary | En |
| Accommodation of Risk (AR) | Compliance with harmful partner requests | F60.3 / Z72.51 | Ordinal | En |
| HIV Infection Outcome (HIV+) | Seroconversion following relationship dynamics | B20 / Z21 | Binary | En |
Table 5.
Thematic constructs and variables definitions.
| Construct Label | Description | ICD-10 Reference | Variable Type | Endogenous/Dependent (En) or Exogenous/Independent (Ex) |
|---|---|---|---|---|
| Risk-Taking Sexual Behaviour (RTSB) | Engaging in sexual activity despite known health risks | Z72.51 / F60.3 | Ordinal (0−2) | En |
| Awareness of Risk (ARW) | Cognitive recognition of health/social consequences | Z72.6 / F60.3 | Ordinal (0−2) | En |
| Impulsivity (IMP) | Acting without foresight or planning | F60.3 / F91.0 | Ordinal (0−2) | E |
| Trauma History (TH) | Childhood abuse, neglect, or violence | Z61.4 / F43.1 | Binary (0=no trauma; 1 = trauma) | Ex |
| Low Mood (LM) | Depressive symptoms or affective instability | F32.0 / F60.3 | Ordinal (0−2) | Ex |
| Unprotected Intimacy (UPI) | Sexual contact without protection despite HIV risk | Z72.51 / B20 | Binary (0 = protected, 1 = unprotected) | En |
| Guilt and Regret (GR) | Psychological consequences post-risk | F60.3 / F33.2 | Ordinal (0–2) | En |
Table 6.
Thematic constructs and variables definitions.
| Construct Label | Description | ICD-10 Reference | Variable Type | Endogenous/Independent (En) or Exogenous/Dependent (Ex) |
|---|---|---|---|---|
| Boundary Erosion (BER) | Difficulty maintaining professional/personal boundaries | F60.3 / Z73.2 | Ordinal (0–2) | Ex |
| Romantic Counter-Transference (RCT) | Emotional overinvolvement with clients due to perceived suffering | F60.3 / Z60.4 | Ordinal (0–2) | Ex |
| Rescue Fantasy (RF) | Compulsion to help or “save” vulnerable partners | F60.3 / Z73.1 | Ordinal (0–2) | Ex |
| Impaired Risk Appraisal (IRA) | Underestimation of relational danger or exploitation | F60.3 / Z72.6 | Ordinal (0–2) | Ex |
| Trauma History (TH) | Childhood abuse, neglect, or relational trauma | Z61.4 / F43.1 | Binary (0=absent; 1=present) | En |
| Low Mood (LM) | Depressive symptoms or affective instability | F32.0 / F60.3 | Ordinal (0–2) | En |
| Relationship Entrapment (RE) | Inability to exit harmful or exploitative relationships | F60.3 / Z63.5 | Ordinal (0–2) | Ex |
Table 7.
Illustrative beta coefficients.
| Pathway | β Coefficient | Interpretation |
|---|---|---|
| IPS → RFRI | 0.72 | Strong link between impulsivity and idealisation of vulnerable partners |
| RFRI → PRR | 0.65 | Idealisation fosters a sense of responsibility for partner outcomes |
| PRR → RI | 0.58 | Perceived responsibility contributes to relational instability |
| RI → HRE | 0.81 | Relationship instability strongly predicts health risk exposure |
| EOI → RI | 0.67 | Emotional overinvolvement in care settings leads to role confusion |
| RI → HRE (from EOI pathway) | 0.81 | Same endpoint: unstable relationships increase vulnerability to health risks |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



