
Submitted:
28 November 2025
Posted:
02 December 2025
You are already at the latest version
Abstract
Background: Building on the validation of the Your Memory test for mild cognitive impairment in English speakers, this study adapted and validated the Memory Test for Mild Cognitive Impairment (TYM-MCI) for Spanish-speaking older adults, highlighting its potential for early detection of Alzheimer's disease (AD). Methods: A total of 151 independently functioning adults aged 60 or older (Barthel Index 9-10) completed the TYM-MCI, the Addenbrooke's Cognitive Examination-Revised (ACE-R-Ch), the Mini-Mental State Examination, and the original TYM. Analyses included ROC curves, correlation matrices, and principal component analysis (PCA). Results: The TYM-MCI exhibited strong psychometric properties (Cronbach's α = 0.832; sensitivity = 81.7%; specificity = 47.8%). The optimal cut-off score was ≥ 24.5/30. Scores between 19 and 24.5 suggested probable mild cognitive impairment (MCI). Conclusions: The episodic memory components of this test are key cognitive features that help differentiate the progression of potential cognitive decline related to dementia and are straightforward to administer. Notably, it specifically assesses visual and verbal episodic memory. It can be used alongside other assessments, such as the ACE-R or MMSE, to evaluate cognitive function in older adults. Clinically, it offers a foundation for early assessment and intervention in cases of cognitive decline, aiding in the prevention or delay of MCI or dementia diagnoses.
Keywords:
aged
; alzheimer’s disease
; cognitive dysfunction
; early diagnosis
; memory
; episodic
; mild cognitive impairment
; mini-mental state examination
; neuropsychological tests
1. Introduction
Memory is a fundamental cognitive function that supports an individual’s ability to adapt, which is essential for independence and quality of life, especially in older adults [1,2]. Mnemonic impairment serves as a key indicator of neurocognitive decline that can lead to dementia [3]. This gradual, widespread, and multifactorial brain dysfunction is classified into several subtypes based on etiology, clinical features, disease progression, and associated disorders [4]. In this context, mild cognitive impairment, particularly its amnestic subtype (aMCI), is described as a transitional phase between normal aging and Alzheimer’s disease (AD), initially marked by changes in episodic memory (EM) [5,6,7]. EM, which involves recalling autobiographical events situated in time and space, relies on the hippocampus and neocortical regions [8,9]. Recent studies emphasize that a decline in episodic memory is one of the most sensitive markers of the transition from aMCI to AD, especially for conscious recollection of information [10,11]. AD is a specific type of dementia and is a widespread concern [12]. Clinically, it manifests as progressive memory loss, language difficulties, challenges with abstract thinking, and problem-solving [13,14]. Early detection of these symptoms is essential, as it enables the timely initiation of therapeutic and psychosocial interventions that can slow down disease progression [15,16,17]. Several neuropsychological tests have been validated to evaluate key cognitive domains and detect early signs of MCI or dementia. For instance, the ACE-R-Chile (Addenbrooke’s Cognitive Examination—adapted version) has proven helpful as an initial screening tool for cognitive impairment [18,19]. Likewise, the Test Your Memory (TYM) and its MCI-specific version (TYM-MCI) are brief, sensitive assessments for detecting memory issues; TYM-MCI has demonstrated advantages over other tests, such as the MMSE, in evaluating episodic memory in English-speaking countries [20,21]. Nonetheless, emerging evidence highlights specific diagnostic biomarkers in the prodromal stage that can differentiate individuals progressing toward dementia or other forms of cognitive decline [22,23]. Meanwhile, tools such as the TYM-S and the MMSE are used to screen for memory deficits and other cognitive impairments [22]. The TYM-S contains limited verbal and visual memory components, which could be key indicators of early AD [23,24]. The TYM-MCI version addresses these limitations and aids in diagnosing AD and cognitive impairment, showing high sensitivity among amnestic profiles to exclude dementia and MCI within a normative group [16,25]. It is also helpful in identifying AD or MCI-like symptoms in patients who score well on the MMSE and ACE-R [23], a relevant point for this study. On the other hand, there is very limited evidence on TYM-MCI assessments in Spanish-speaking countries since Brown’s review in 2019 [20]. In Chile in 2017, individuals aged 60 and older, regardless of gender, made up 11.9% of the population [27]. This figure is expected to increase to 18.9% by 2035, with life expectancy around 80 years for men and 86 years for women [27,28]. Therefore, there is an urgent need for validated Spanish tools to detect cognitive decline early, given the rapidly aging population [28,29]. Projections indicate that by 2035, older adults will constitute about 19% of the population, with life expectancy around 80 years for men and 86 years for women [27,28,29,30]. In this demographic context, other factors are also important, such as nutritional status [31], hearing loss [32], and perceived social status within reference groups [33]. Additionally, while imaging has been proven effective for diagnosis, we support the implementation of efficient and accessible diagnostic strategies that allow early intervention, lower healthcare costs, and prevent unnecessary institutionalization [34].
Hence, this study aims to validate and adapt the TYM-MCI for Spanish-speaking populations, assessing its psychometric properties and clinical utility in detecting episodic memory disorders among older adults. The goal is to develop brief, culturally appropriate, evidence-based diagnostic tools that support comprehensive, preventive geriatric care.
2. Materials and Methods
2.1. Design and Sample Population
This research employs a descriptive, non-experimental, cross-sectional design [35]. A total of 151 participants were recruited through a non-probabilistic, purposive sampling method, following the approach of Brown et al. [20]. The sample had a 6% margin of error and a 95% confidence level. Inclusion criteria were: being a native Spanish speaker, living in the Metropolitan Region of Chile; aged 60 or older; without restrictions related to education or gender; possessing sufficient functional literacy to respond to the assessment tools; having maintained functional capacity (maximum score on the Barthel Index); and participating in community organizations for older adults. Exclusion criteria adhered to the provisions of Article 28 of Law No. 20,584 and Article 9, paragraph 5, of Law No. 21,331, both from the Republic of Chile, concerning human rights and mental health protections. Individuals with medical diagnoses or histories of psychiatric, neurological, or neurodegenerative disorders that hindered voluntary and conscious participation, as well as those with sensorimotor or physical limitations impairing their ability to perform assessment tasks, were excluded. The mild cognitive impairment (MCI) group was defined as those with scores between 81 and 91 on the ACE-R-Ch [19]. All procedures received approval from the Scientific Ethics Committee of the Universidad Mayor de Chile (protocol No. 0264, July 13, 2022, and Session 107, September 13, 2023), in compliance with the guidelines of the Declaration of Helsinki concerning research with human subjects [36].
2.2. Instrument
The assessments used include the Addenbrooke’s Cognitive Examination-Revised (ACE-R)—an instrument combining the MMSE that evaluates dementia with high sensitivity. It distinguishes Alzheimer’s disease (AD) from frontotemporal dementia (FTD), assessing temporal and spatial orientation, attention and concentration, memory, verbal fluency, language, and visuospatial skills. The cut-off score for mild cognitive impairment (MCI) is 82–91 out of 100 points. Scores below 81 suggest early AD. Reliability indicators are: reliability = 0.918; sensitivity = 0.917; and specificity = 0.93316 [18,19].
Test Your Memory (TYM-S): A brief assessment covering cognitive domains such as temporal-spatial orientation, autobiographical, semantic, and delayed memory, as well as attention, calculation, phonological and categorical fluency, and visuo-perceptual and visuo-constructive skills. The cut-off for MCI is ≤ 42/50, and for dementia it is < 39. It demonstrates acceptable reliability (α = 0.776), sensitivity (0.857), and specificity (0.690) [22,24].
TYM-MCI (Test Your Memory for Mild Cognitive Impairment): A specialized version designed to detect amnestic MCI and Alzheimer’s disease, focusing on episodic memory (verbal and visual delayed recall), comprehension, delayed recall, recognition, and drawing recall. The cutoff point is ≤13/30. Reported sensitivity is 0.67, with a specificity of 0.66 [20,21].
Mini-Mental State Examination (MMSE): A screening tool that assesses basic cognitive functions such as orientation, memory, attention, calculation, language, and spatial skills [37,38].
Barthel Index: An instrument measuring functional independence in basic daily activities, serving as a supplementary indicator of cognitive integrity and functional autonomy, evaluated in nutritional contexts [39].
2.3. Procedure
The TYM-MCI [21,29] was translated into Spanish using the translation-back-translation method to ensure semantic and conceptual equivalence. It was then reviewed by an expert panel comprising three psychologists experienced in neuropsychology and one professional translator. A rating matrix based on the Aiken V index and a Likert scale was used to assess the relevance, clarity, and consistency of the items within the cognitive domain, with an acceptance threshold of 95% [40]. Testing took place in a quiet 3 x 3-meter room provided by the Communal Union of Older Adults (UCAM) in Melipilla city, Chile. Participants first signed the informed consent and completed the Barthel assessment. Subsequently, the ACE-R-Ch was administered, followed by the TYM and TYM-MCI tests. Researchers supported the older adults during testing, who completed minimal self-administered tasks. In a follow-up session, results were discussed along with suggestions for improving performance or maintaining cognitive strengths.
2.4. Statistical Analysis
The ROC curve, correlation analysis, and Principal Component Analysis (PCA) were performed using R software version 4.2.1. This process allows for the identification of cutoff points for cognitive impairment by calculating sensitivity and specificity for the TYM-MCI [41]. PCA reduces data complexity, facilitating the interpretation of results by revealing underlying variables [42]. The use of parametric statistics depended on the normality analysis, which was conducted using the Kolmogorov-Smirnov (K-S) test. Coefficients for homogeneity and reliability were calculated with Cronbach’s alpha. The cut-off score for estimating cognitive impairment was determined via the ROC curve based on sensitivity and specificity data [41]. Data were analyzed using IBM SPSS version 29.0 and GraphPad Prism 6.0 for descriptive purposes. In summary, the following procedures were applied: a normality test (Kolmogorov-Smirnov) to guide the use of parametric procedures, Cronbach’s alpha to assess internal consistency, ROC curves to identify optimal cutoff points based on diagnostic sensitivity and specificity [41] and PCA to reduce data dimensions and explore latent variables related to cognitive domains, aiding the structural interpretation of the test [42].
3. Results
The principal quantitative findings obtained in the validation and cultural adaptation of the TYM-MCI in Spanish-speaking older adults are presented.
3.1. Descriptive data and Sample Distribution
The Kolmogorov–Smirnov test confirmed normal data distribution for all test measures among the 151 community-dwelling older adults evaluated. Mean scores were ACE-R-Ch = 91.82 (SD = 4.13; p = .15), MMSE = 28.35 (SD = 2.14; p = .32), TYM = 44.19 (SD = 2.69; p = .15), and TYM-MCI = 23.48 (SD = 2.82; p = .0098). Participants’ mean age was 72.9 years (SD = 7.7), with a predominance of women. 30.1% reported having a technical or university education, with average educational level of 11.21 (SD = 2.76) and participated regularly in cognitively stimulating activities, such as reading and community workshops. This is characteristic of highly stimulated adults and contributes to their cognitive reserve [43,44].
3.2. Internal Consistency, Prevalence of Impairment, and ROC Curve of the TYM-MCI
The TYM-MCI demonstrated high internal consistency, with a Cronbach’s alpha of 0.832. ROC curve analysis identified an optimal cutoff score of 24.5 points, with a sensitivity of 81.7% and a specificity of 47.8%. This cutoff offers the best trade-off between false positives and false negatives for detecting MCI46. Among all participants, 89 individuals were classified as having cognitive impairment based on this cutoff, accounting for 58.9% of the sample. The area under the curve (AUC) was 0.641, indicating moderate discriminatory ability (Figure 1 and Table 1).
3.3. Correlation Analysis Between Cognitive Tests
Pearson’s correlation analysis between the different instruments showed that the TYM-MCI has a weak to moderate correlation with the other tests. The strongest Pearson correlation was with the TYM (r = 0.348), followed by the ACE-R (r = 0.254), and then the MMSE (r = 0.186). All correlations were significant at p < .01. These findings suggest that the TYM-MCI assesses somewhat different aspects of cognitive functioning, supporting its additional value in diagnosing MCI. Additionally, there is a moderate correlation between the ACE-R and MMSE tests (r = .54) and ACE-R TYM (r = .58), and a low correlation between MMSE and TYM (r = .32).
3.4. Sensitivity and Specificity by Cognitive Domains
The analysis of diagnostic accuracy indicates that for the episodic memory domain, the TYM-MCI achieved a specificity of 83.1% and an accuracy of 67.5%, although its sensitivity was low at 12.1%. In contrast, the ACE-R demonstrated a more balanced ratio between sensitivity (33.3%) and specificity (80.5%). When assessing global cognitive impairment, the ACE-R achieved an accuracy of 97.4%, with high sensitivity (94.2%) and specificity (100%). The TYM-MCI also showed high specificity (81.7%) but had an intermediate sensitivity (47.8%) (see Table 2).
3.5. Principal Components Analysis (PCA). State Variables
The PCA analysis performed for each of the cognitive tests is shown in the following tables 3 and 4, along with the corresponding figures, which will be indicated.
3.6. PCA Del ACE-R
Three components explain 76.18% of the total variance (Table 3). Orientation and memory cluster in the first dimension, showing a high correlation with the total test score (r = 0.85). Verbal fluency clusters in the second dimension as an independent variable, and language associates with the visuospatial component in the third dimension, although in different directions (Table 4 and Figure 2). The suitability of the five ACE-R items, measured using the Kaiser-Meyer-Olkin (KMO) index, indicates acceptable scores for item 1. Orientation, Concentration, and Attention (0.52); item 2. Memory (0.52) and item 4. Language (0.50). The items with insufficient suitability are: item 3. Verbal Fluency (0.42) and item 5. Visuospatial Skills (0.49). Bartlett’s Test of Sphericity shows a significance R of < 0.01, indicating that the correlation matrix is not an identity matrix.
3.7. PCA of the MMSE
Three components accounted for 83.68% of the variance (Table 3). The overall test showed a high correlation with the first dimension (r = .97). In the second dimension, the language subtest exhibited a strong negative correlation. In contrast, visuospatial construction showed a positive but low association with the total MMSE (Table 4 and Figure 3). The five MMSE items had acceptable KMO values, as indicated by Item 1. Orientation = .66; Item 2. Attention and Concentration = .61; Item 3. Memory = .68; Item 4. Language = .56; and Item 5. Visuoconstruction = .55. Bartlett’s test of sphericity showed a significance level less than R = .01, demonstrating that the correlation matrix is not an identity matrix.
3.8. PCA of the TYM-S
Five components explained 67,65% of the variance (See Table 3). The structure of the TYM-S is dispersed, with a low correlation between the total score and the component factors. Dimension 1 strongly groups items related to lexical similarities (item 6), functional calculation (item 4), delayed recall and semantic memory (item 7), and episodic memory (item 3). These results suggest the emergence of a component related to complex verbal reasoning and active memory processes, possibly linked to verbal cognitive reserve and the executive integration of verbal-semantic content. Dimension 2 groups items on time-spatial orientation (item 1), direct copying (item 2), and the evaluator item (item 11), suggesting a second component more closely linked to simple visual-constructional skills and attentional monitoring or basic execution tasks. Dimension 3 is characterized by a strong positive loading on the semantic memory item (item 5) and significant negative loadings on visual agnosia and tracking (item 8), which could represent an opposite gradient between conceptual retrieval and visual perceptual identification, suggesting a differentiation between visual and semantic processing. Dimension 4 shows a significant loading on visuospatial skills, specifically on the visuospatial skills item (item 9), indicating the emergence of a specific factor linked to complex visuospatial skills that is relatively independent of the other functions. Dimension 5 is notable for its high loadings on functional calculation (item 4) and semantic memory (item 5), components that can be associated with acquired cognitive reserve (arithmetic fluency and cultural knowledge). Dimensions 6 and 7, although with less explanatory weight, contain significant correlations with delayed episodic memory (item 3) and visual components such as agnosia and visuospatial construction, suggesting a diversity of individual strategies for visual and verbal recall. The total TYM score correlates moderately with the first five dimensions (higher in Dim. 2 and Dim. 1), confirming a multifactorial structure of the test, with orientation, similarity, memory, and calculation tasks contributing most to overall performance (Table 4 and Figure 4).
The KMO measures acceptable are Item 1-Time-Space Orientation (0.47), Item 2-Direct Copy to Writing (0.47), Item 3-Episodic Memory (0,66), Item 4-Functional Calculation (0.64), Item 5-Semantic Memory (0,37), Item 6-Similarities (0,62), Item 7-Delayed Recall and Semantic Memory (0.42), Item 8-Visual Gnosis and Tracking (0.57), Item 9-Visuoconstruction and Visuospatial Skills (0,47), Item 10-Deferred Recall (0.64), and Item 11-Evaluator (0.67). The KMO is unacceptable for Semantic Memory, Delayed Recall, and Visuospatial Memory, as well as Visuospatial skills; for the other variables, it is mediocre. Bartlett’s Test of Sphericity has a significance level of less than 0.01, indicating that the correlation matrix is not an identity matrix.
Table 3 shows the correlation between the variables and the eigenvectors, with the total TYM test score as the dependent variable. From this, it is clear that the total TYM score has a very low correlation with the third dimension onward, which shows a high positive correlation with the item Semantic Memory and a high negative correlation with the items Visual Gnosia and Tracking. The correlation with four dimensions is nearly zero, and these four dimensions have a strong correlation with item nine of Visuo-construction. The correlation of TYM with the fifth dimension is low (0.31), and this dimension is highly correlated with Item 4 – Functional Calculation and Item 5 - Semantic Memory.
3.9. PCA of the TYM-MCI
Three components explained 80.4% of the variance (Table 3). The total test score was strongly correlated with the third dimension (r = .93), where visual and verbal episodic memory converge, giving these items structural significance compared to other instruments. Specifically, Dimension 1 exhibits strong positive correlations with the verbal and semantic components, particularly with items 3 and 4. Dimension 2 is strongly related to verbal episodic and delayed recall memory, indicating an independent axis of verbal processing. Dimension 3 is closely aligned with the total test score (.933) and loads significantly on both verbal and visual components, suggesting this dimension represents the integrative factor of overall episodic memory performance. Dimension 4 presents opposite correlations between visual and semantic items, which could indicate a tension between visual versus verbal/semantic encoding (Table 4 y Figure 5).
Figure 4 y 5. Variables PCA graph: (a) Figure 4; Items of TYM test work with structure disperse of variables. Compare with Table 4; (b) Figure 5; Items of TYM-MCI test work independently.
The KMO values are moderate for all variables: 0.55 for Visual Episodic Memory, Visuoconstruction, and Delayed Recall; 0.55 for Episodic Verbal Memory and Delayed Recall; 0.48 for Verbal Episodic Memory, Semantic Memory, and Delayed Recall; and 0.54 for Episodic Visual, Semantic, and Deferred Recall Memory. Bartlett’s Test of Sphericity has a significance of less than 0.01, indicating that the correlation matrix is not an identity matrix. TYM-MCI scores, which shows high positive or negative correlations with some subtests. All of this is new compared to previous tests, which had a weaker relationship with visual items.
4. Discussion
4.1. Global Analyses
The overall results of the TYM-MCI test confirm its effectiveness in assessing episodic memory (EM) performance, as initially reported by Brown et al. (2014) [25]. Its high internal consistency and reliability, compared to other screening tools, likely stem from its ability to focus on a specific cognitive domain using criteria that help detect mental impairment, as shown by ROC curve analysis—a standard method in such validation studies [45]. Visual and verbal EM assessments are predictive markers for diagnosing aMCI and early AD [46,47,48]. Along with limitations in daily living activities, these are essential criteria for early dementia diagnosis [49]. Besides, the Barthel Index scores in this study ranged from 9 to 10 in all participants, indicating preserved functionality—a critical factor in ruling out early functional decline [50]. Such indicators are recommended in clinical practice, as they affect occupational, social, and family performance, consistent with the MMSE’s validation in Chile using the Pfeffer questionnaire [38]. Early cognitive signs include deficits in learning and retaining new information, disorientation in time and space, and significant changes in autobiographical memory, which aid in detecting MCI previous a AD without distortion [47,51]. The specific EM contexts measured by the TYM-MCI differ from those assessed by other tools, improving the accuracy of neuropsychological evaluation [52,53,54].
The optimal cut-off (≥24.5) achieved high sensitivity (81.7%) but moderate specificity (47.8%). This data indicates a strong ability to correctly identify MCI cases (low false negatives), which is clinically important in preventive settings. The low specificity, indicating possible false positives, can be explained, first, by the TYM-MCI’s explicit design to detect subtle EM changes—a domain particularly vulnerable to early impairment [25,54,55]. As a result, it may detect preclinical or subthreshold alterations that broader tests such as the MMSE or ACE-R do not capture, leading to more “positive” results without a formal diagnosis. Second, in a community sample with good education and high functionality, undiagnosed individuals may already show subtle EM deficits detectable by the TYM-MCI [55,56]. From a public health perspective, prioritizing sensitivity reduces the risk of missing at-risk cases, even if secondary confirmatory assessments are needed. The TYM-MCI thus serves as an ideal initial screening tool to be supplemented by more comprehensive neuropsychological batteries. This approach aligns with the ecological variability of EM, observable even in populations without obvious impairment and cognitive reserve [43,56].
The difference between the present current cutoff (24.5) and that proposed by Brown et al. [20,21], (13.1) is due to sociodemographic and cognitive differences in the samples. The original study included patients from the neurology clinic with a high pretest probability of impairment. In contrast, our cohort consisted of functioning, autonomous older adults (Barthel 9–10) engaged in community activities in Chile, with medium to high education and a younger mean age (72 years). This profile suggests greater cognitive reserve, linked to better test performance despite mild impairment [43,56]. In high-reserve populations, baseline performance is higher, requiring stricter cut-offs to detect significant decline [44]. Thus, a higher cut-off is expected in active, non-clinical samples, reflecting appropriate local adaptation [57]. In Chile and Latin America, evaluation of EM remains limited and under-validated despite growing research [58]. Screening tools validated in similar domains include the ACE-R-Ch [19], the MMSE [38], the TYM [24], and the IFS [59]. Correlation analyses show significant associations between most instruments, except for the TYM-MCI, whose lower correlation suggests it measures distinct domains. This reinforces its specificity for EM, especially in differentiating amnestic MCI and AD [20,21].
The TYM-MCI also provides specific features to evaluate verbal and visual episodic memory—key indicators for early diagnosis of amnestic cognitive impairment—through tasks like direct copying and delayed recall [21]. This information provides crucial diagnostic clues and helps distinguish different types of dementia when combined with assessments of daily living skills [4,12,17]. Furthermore, by evaluating amnestic symptoms that affect daily activities, the TYM-MCI conducts assessments under standardized conditions that reflect functional and predictive relationships of ecological validity [60,61]. Clinically, performance tends to decline in routine tasks within family, work, and social settings, which correlates with hippocampal white matter development and organization [62]. Complex event patterns activate hippocampal areas, with familiarity rooted in the perirhinal cortex, which is sensitive to repetition [10]. Palliative strategies, such as distraction-based activities, may stimulate cognition by leveraging episodic memory [63].
4.2. Analysis of the Relationship Between Cognitive Tests Regarding Episodic Memory
Exploratory principal components analysis (PCA) of each test allowed us to evaluate the contribution of TYM-MCI to the assessment of mental impairment. Since each item influences the final test score, this impact is readily observable. We used the individual item scores to determine the overall total score as a supplemental quantitative measure. This approach enables us to analyze the correlations between the original items and their components, and to assess how these variables influence the final score within the observed sample. The importance of the variables in each item varies with the final score, which will be examined more thoroughly using PCA [42].
The correlation of the ACE-R eigenvector variables suggests that the orientation and memory items do not correspond to distinct variables, given their high correlations and the total test score. Therefore, the individual being assessed might be relying on the same cognitive process for these items. The high correlation of the verbal influence item in dimension 2 with other components demonstrates its independence from different items. The language item centers on the visuospatial item in dimension 3, indicating a strong likelihood that performance on the visuospatial task depends on language skills. Understanding instructions may be a key factor in the visuospatial test, which could explain why the clarity of the evaluator’s expression influences performance on the subtest, as evidenced by the correlation between these variables (see Figure 2 and Table 2). Evidence indicates that language affects cognitive reserve, which may be reflected in optimal mental performance, explaining this relationship [43,64,65].
Regarding the MMSE test, the first component (Dim. 1) heavily groups all the classic items of the test, with exceptionally high loadings on the subtests. This test suggests that the first dimension represents a global cognitive function, or general factor (g), that explains a significant portion of MMSE performance. The high correlation with the total MMSE (0.97) supports the view that this test mainly functions as a unidimensional measure of overall cognitive performance (as supported by previous studies [66]). Regarding episodic memory representation, although it shares variance with overall performance, this cognitive process is not confined to dimension one but spans dimensions 1 and 3, distinguishing it from other mental functions. However, the MMSE is limited to immediate word recall and delayed evocation without greater complexity [22,37], and episodic memory assessed here does not significantly influence the overall test score [67]. Conversely, a dissociation between visuospatial and verbal functions has been identified due to contradictory loadings in the PCA analysis. The MMSE is only moderately sensitive and specific for episodic memory, limiting its utility in evaluating older adults. Instead, it is designed as a broad screening tool for cognitive decline, which is why it should be supplemented with the TYM-MCI [21] or the ACE-R [19].
Furthermore, the PCA results for the TYM uncover a complex, partially multidimensional structure, consistent with this instrument being a brief, heterogeneous screening test that includes verbal, visuospatial, and memory components [20,24]. The presence of multiple dimensions suggests that the TYM does not measure a single cognitive construct but rather a set of cognitive subfunctions. This pattern aligns with previous findings indicating that screening tests capture different types of cognitive decline, depending on cognitive reserves, educational background, or neuropsychological aging trajectories [56,67].
However, identifying a separate visuospatial construction component enhances the clinical utility of the TYM in detecting specific deficits, especially in non-amnestic dementias (e.g., frontotemporal dementia or non-amnestic mild cognitive impairment). Additionally, the combination of verbal and visual tasks across domains may reflect the various compensatory strategies older adults employ. Finally, the association of semantic memory with both executive functions and perceptual and visuospatial components emphasizes its role as an integrative link between knowledge and retrieval processes, which is vital during the early stages of mild cognitive impairment [7,15,48].
4.3. Does the TYM-MCI Effectively Assess Episodic Memory Compared to Other Tests?
In summary, it is possible to demonstrate:
a) Concerning the consistency of the factor structure with mixed memory systems, the results show that the tasks included in the TYM-MCI, although mainly designed to evaluate episodic memory, activate multiple systems (verbal, visual, semantic episodic memory, and consolidation processes). This consistency is expected, as episodic memory rarely occurs in isolation and relies on neurocognitive networks that integrate semantics, attention, and multisensory encoding [7,8].
b) An empirical finding of a general episodic memory factor appears in Dimension 3, which shows a high correlation with the total TYM-MCI score (r = 0.933). This high correlation confirms that the test has internal structural coherence, with items converging on a single factor. This consistency indicates that the test effectively synthesizes a strong representation of episodic performance (both verbal and visual) within its total score [22], supporting its internal validity.
c) Furthermore, processing differences between visual and verbal modalities serve as a functional dissociation, as Dimensions 1 and 2 suggest a relative separation between these modalities. Dimension 2, which focuses on verbal recall, is the most independent, while the visual dimension is spread across other dimensions. This variability could be due to individual differences in encoding strategies (dual coding) or to selective impairments in patients with amnestic mild cognitive impairment (aMCI), who often show reduced verbal episodic memory rather than visual memory [16,68].
d) The compensatory gradient, indicated by the opposite signs between visual and verbal items in Dimension 4, may reflect individual compensatory strategies: individuals with difficulties in visual tasks may compensate via the semantic-verbal domain, and vice versa. This finding is clinically significant as it helps outline different cognitive pathways in mild impairment, with implications for personalized rehabilitation [17]. Factor analysis of the TYM-MCI indicates that this tool effectively captures a core aspect of episodic memory, particularly given its combined verbal, visual, and delayed recall components. The high load of the total score on the third dimension, along with the observed dissociations between sensory modalities, suggests that the TYM-MCI is a brief yet well-structured test for detecting mild cognitive impairment, with a particular focus on episodic memory, and is especially sensitive to early and mixed memory issues [20].
5. Conclusions
5.1. General Conclusion
The results of the principal components analysis (PCA) and the comparison with other cognitive screening tools confirm that the TYM-MCI is a sensitive and specific instrument for detecting amnestic-type mild cognitive impairment. It also meets reliability and internal consistency criteria, with a cutoff score of 24.5 in older adults with cognitive reserve. Unlike other general assessments, such as the MMSE or the ACE-R, the TYM-MCI exhibits a clear factor structure focused on episodic memory, encompassing visual, verbal, and semantic components, with a high factor loading on a primary dimension that consolidates this performance. This structural coherence enhances its internal validity as a specialized test.
Furthermore, the functional separation between the visual and verbal modalities suggests that the TYM-MCI can identify compensatory patterns or different cognitive profiles, increasing its clinical usefulness in early diagnosis and planning personalized interventions. In this regard, the TYM-MCI not only effectively distinguishes cases of amnestic-type mild cognitive impairment but also provides indicators of cognitive reserve, encoding strategies, and progression pathways, making it a valuable tool for a comprehensive approach to cognitive deficits in older adults. Therefore, it is recommended to combine it with broader and functional assessments in neuropsychological evaluation protocols for older adults, especially during the early stages of cognitive decline when episodic memory is a key clinical marker. Overall, the psychometric, clinical, and contextual results confirm that the TYM-MCI is a valid, reliable, culturally and educationally appropriate tool for older spanish-speaking adults, with a clear focus on episodic memory as an early indicator of cognitive decline. It is curious that, after the publication of Brown et al. (2019), there are no reports of TYM-MCI use in the Spanish-speaking population, which makes this study relevant, in addition to what has been indicated above.
5.2. Strengths and Limitations of the Study
This study has several strengths. It is one of the few validations of the TYM-MCI specifically conducted in Spanish-speaking older adults, a group for which culturally adapted cognitive screening tools are still limited. Using a functionally independent, community-based sample with medium to high educational levels improves external validity and reflects performance in active aging settings. Applying advanced statistical methods, such as PCA, provides a solid psychometric analysis, helping to clarify the specific role of episodic memory components in the total score. Additionally, the TYM-MCI demonstrated good internal consistency (α = .832) and high sensitivity, supporting its potential as a first-line screening tool for early cognitive decline.
However, some limitations should be acknowledged. The moderate-to-low specificity (47.8%) indicates a risk of false positives, especially among highly educated individuals with greater cognitive reserve, highlighting the need for confirmatory assessments with additional tests. The cross-sectional design limits conclusions regarding predictive validity, emphasizing the necessity for longitudinal studies to assess the test’s ability to monitor progression from MCI to dementia. Lastly, although the sample is representative of active older adults, it may not fully capture rural or low-literacy populations, indicating that additional research is needed in more diverse sociodemographic groups.
Author Contributions
Conceptualization, ABM, VGE, FEG, NMO, PSL, ECM, and ACB; methodology, ABM, HB, DFF, and FAC; software, DFF and FAC; validation, assessed the methodological quality of the studies, CCV, ACB, PSL, VGE, ECM, and HB; formal analysis, FAC, CCV, and HB; investigation, ABM, NMO, ACB, EC, CCV, and HB; writing-original draft preparation, ABM, PSL, ECM, CCV, FEG, and HB; writing, review and editing, HB, VGE, ECM and CCV; project administration ABM and HB. All authors have read and agreed to the published version of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received external funding. i) This work is supported by Funding Universidad Mayor, Chile (ABM, FEG) ii) FONIS SA24I0065 and Interdisciplinary 11340012 to (CCV) iii) Escuela de Enfermería, Facultad de Salud, Universidad Santo Tomás, Chile (HB, ECM, PSL).
Institutional Review Board Statement
All procedures received approval from the Scientific Ethics Committee of the Universidad Mayor de Chile (protocol No. 0264, July 13, 2022, and Session 107, September 13, 2023), in compliance with the guidelines of the Declaration of Helsinki concerning research with human subjects [36].
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study, indicates in protocol No. 0264, July 13, 2022, and Session 107, September 13, 2023.
Data Availability Statement
The data is stored on the authors’ electronic devices or in the Google Drive folder if the authors formally request it.
Acknowledgments
The authors thank and consent to the following institutions: i) Escuela de Psicología and Magíster en Neuropsicología of Universidad Mayor, Chile. ii) Escuela de Enfermería, Facultad de Salud, Universidad Santo Tomás for providing the facilities to develop this study; iii) +SALUD / Centro de Investigación en Prevención y Cuidados de la Salud, Facultad de Salud, Universidad Santo Tomás, Santiago, Chile for technical support and financing; iv) Facultad de Economía y Negocios, Universidad Alberto Hurtado for technical and statistical contribution. Special thanks to the Unión Comunal de Adultos Mayores of Melipilla (UCAM) for making it easier for senior citizens to access services. Thanks to the Grammarly program for its assistance in refining the English wording. In special, to Dr. Carlos Muñoz Neira who incorporate the original idea.
Conflicts of Interest
The authors declare that there are no conflicts of interest. The funders had no role in designing the study; in collecting, analyzing, or interpreting data; in writing the manuscript; or in deciding to publish the results.
References
- Cowan, E.T.; Schapiro, A.C.; Dunsmoor, J.E.; Murty, V.P. Memory consolidation as an adaptive process. Psychonomic bulletin & review 2021, 28, 1796–1810. [Google Scholar] [CrossRef]
- Mehling, W.E.; Scott, T.M.; Duffy, J.; Whitmer, R.A.; Chesney, M.A.; Boscardin, W.J.; Barnes, D.E. Dyadic Group Exercises for Persons with Memory Deficits and Care Partners: Mixed-Method Findings from the Paired Preventing Loss of Independence through Exercise (PLIÉ) Randomized Trial. J Alzheimers Dis. 2020, 78, 1689–1706. [Google Scholar] [CrossRef]
- Mian, M.; Tahiri, J.; Eldin, R.; Altabaa, M.; Sehar, U.; Reddy, P.H. Overlooked cases of mild cognitive impairment: Implications to early Alzheimer’s disease. Ageing Research Reviews 2024, 98, 102335. [Google Scholar] [CrossRef] [PubMed]
- Garre-Olmo. Epidemiology of Alzheimer’s disease and other dementias. Neurology Journal 2018, 66, 377–386. [Google Scholar] [CrossRef]
- Anderson, N.D. State of the science on mild cognitive impairment (MCI). CNS Spectrums 2019, 24, 78–87. [Google Scholar] [CrossRef]
- Ministerio de Salud. Plan nacional de demencia. Ministerio de Salud 2017. https://www.minsal.cl/wp-content/uploads/2017/11/PLAN-DE-DEMENCIA.pdf.
- Mowszowski, L.; Lampit, A.; Walton, C.C.; Naismith, S.L.; Valenzuela, M. The role of memory interventions in mild cognitive impairment: A systematic review. Neuropsychology Review 2022, 32, 1–27. [Google Scholar] [CrossRef]
- Tulving, E. Episodic memory: from mind to brain. Annual Review of Psychology 2002, 53, 1–25. [Google Scholar] [CrossRef]
- Moscovitch, M.; Cabeza, R.; Winocur, G.; Nadel, L. Episodic Memory and Beyond: The Hippocampus and Neocortex in Transformation. Annual Review of Psychology 2016, 67, 105–134. [Google Scholar] [CrossRef]
- Yonelinas, A.; Hawkins, C.; Abovian, A.; Aly, M. The role of recollection, familiarity, and the hippocampus in episodic and working memory. Neuropsychologia 2024, 193, 108777. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, M.; Teng Koh, M. Episodic memory on the path to Alzheimer’s disease. Current Opinion in Neurobiology 2011, 21, 929–934. [Google Scholar] [CrossRef]
- Alzheimer’s Association. 2020 Alzheimer’s disease facts and figures. Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association 2020, 2, 5. [Google Scholar] [CrossRef]
- Dubois, B.; Hampel, H.; Feldman, H.H.; et al. Preclinical Alzheimer’s disease: Definition, natural history, and diagnostic criteria. Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association 2016, 12, 292–323. [Google Scholar] [CrossRef]
- Khan, S.; Barve, K.H.; Kumar, M.S. Recent advancements in pathogenesis, diagnostics and treatment of Alzheimer’s disease. Current Neuropharmacology 2020, 18, 1106–1125. [Google Scholar] [CrossRef]
- Gainotti, G.; Quaranta, D.; Vita, M.G.; Marra, C. Neuropsychological predictors of conversion from mild cognitive impairment to Alzheimer’s disease. Journal of Alzheimer’s Disease: JAD 2014, 38, 481–495. [Google Scholar] [CrossRef]
- Dubois, B.; Feldman, H.H.; Jacova; et al. Advancing research diagnostic criteria for Alzheimer’s disease: the IWG-2 criteria. The Lancet Neurology 2014, 13, 614–629. [Google Scholar] [CrossRef]
- Arvanitakis, Z.; Shah, R.; Bennett, D. Diagnosis and management of dementia: review. Journal of the American Medical Association 2019, 322, 1589–1599, https://pubmed.ncbi.nlm.nih.gov/31638686/. [Google Scholar] [CrossRef]
- Bruno, D.; Slachevsky, A.; Fiorentino, N.; Rueda, D.; Bruno, G.; Tagle, A.; Olavarría, L.; Flores, P.; Lillo, P.; Roca, M.; Torralva, T. Validación argentino-chilena de la versión en español del test Addenbrooke’s Cognitive Examination III para el diagnóstico de demencia. Neurología 2020, 35, 82–88. [Google Scholar] [CrossRef]
- Muñoz-Neira, C.; Ihnen, J.; Flores, P.; Henriquez, F.; Sánchez, M.; Slachevsky, A. Propiedades psicométricas y utilidad diagnóstica del Addenbrooke’s Cognitive Examination-Revised (ACE-R) en una muestra de ancianos chilenos. Revista Médica Chile 2012, 140, 1006–1013. [Google Scholar] [CrossRef]
- Brown, J.; Wiggins, J.; Dawson, K.; Rittman, T.; Rowe, J. Test Your Memory (TYM) and Test Your Memory for Mild Cognitive Impairment (TYM-MCI): a review and update including results of using the TYM test in a general neurology clinic and using a telephone version of the TYM test. Diagnostics 2019, 9, 116. [Google Scholar] [CrossRef]
- Brown, J.; Lansdall, C.; Wiggins, J.; Dawson, K.; Hunter, K.; Rowe, J.; Parker, R. The Test Your Memory for Mild Cognitive Impairment (TYM-MCI). Journal of Neurology, Neurosurgery, and Psychiatry 2017, 88, 1045–1051. [Google Scholar] [CrossRef] [PubMed]
- Van de Zande, E.; Van de Nes, J.; Jansen, I.; Van den Berg, M.; Zwart, A.; Bimmel, D.; Rijkers, G.; Andringa, G. The Test Your Memory (TYM) test outperforms the MMSE in the detection of MCI and dementia. Current Alzheimer Research 2017, 14, 598–607. [Google Scholar] [CrossRef]
- Luna-Lario, P.; Azcárate-Jiménez, L.; Seijas-Gómez, R.; Tirapu-Ustárroz, J. Propuesta de una batería neuropsicológica de evaluación cognitiva para detectar y discriminar deterioro cognitivo leve y demencias. Rev Neurol 2015, 60, 553–561, https://psicogerontologia.org/wp-content/uploads/2015/06/Propuesta-de-bateria-neuropsicologica.pdf. [Google Scholar] [CrossRef]
- Muñoz-Neira, C.; Chaparro, F.; Delgado, C.; Brown, J.; Slachevsky, A. Test Your Memory-Spanish version (TYM-S): a validation study of a self-administered cognitive screening test. International Journal of Geriatric Psychiatry 2014, 29, 730–740. [Google Scholar] [CrossRef]
- Larner, A. Hard-TYM: a pragmatic study. International Journal of Geriatric Psychiatry 2015, 30, 330–331. [Google Scholar] [CrossRef]
- Brown, J.M.; Wiggins, J.; Dong, H.; Harvey, R.; Richardson, F.; Hunter, K.; Dawson, K.; Parker, R.A. The hard Test Your Memory. Evaluation of a short cognitive test to detect mild Alzheimer’s disease and amnestic mild cognitive impairment. International Journal of Geriatric Psychiatry 2014, 29, 272–280. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística. Síntesis de resultados Censo 2017. 2018. http://resultados.censo2017.cl/.
- Servicio Nacional del Adulto Mayor [SENAMA]. Envejecimiento en Chile: evolución y características de las personas mayores. Gobierno de Chile 2022. https://www.senama.gob.cl/storage/docs/Envejecimiento-en-Chile-2022.pdf.
- World Health Organization. Chile [Country overview]. data.who.int 2025. (Accessed on 30 July 2025). Disponible en: https://data.who.int/countries/152.
- Leiva, A.M.; Troncoso-Pantoja, C.; Martínez-Sanguinetti, M.A.; et al. Las personas mayores en Chile: el nuevo desafío social, económico y de salud del siglo XXI. Rev Méd Chile 2020, 148, 799–809. [Google Scholar] [CrossRef]
- Domínguez, L.J.; Veronese, N.; Vernuccio, L.; Catanese, G.; Inzerillo, F.; Salemi, G.; Barbagallo, M. Nutrition, physical activity, and other lifestyle factors in the prevention of cognitive decline and dementia. Nutrients 2021, 13, 4080. [Google Scholar] [CrossRef] [PubMed]
- Yu, R.C.; Pavlou, M.; Schilder, A.G.M.; Bamiou, D.E.; Lewis, G.; Lin, F.R.; Livingston, G.; Proctor, D.; Omar, R.; Costafreda, S.G. Early detection and management of hearing loss to reduce dementia risk in older adults with mild cognitive impairment: findings from the treating auditory impairment and cognition trial (TACT). Age Ageing. 2025, 54(1), afaf004. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Sumerlin, T.S.; Goggins, W.B.; Kwong, E.M.S.; Leung, J.; Yu, B.; Kwok, T.C.Y. Does low subjective social status predict cognitive decline in Chinese older adults? A 4-year longitudinal study from Hong Kong. The American Journal of Geriatric Psychiatry 2021, 29, 1140–1151. [Google Scholar] [CrossRef] [PubMed]
- Dubois, B.; Feldman, H.H.; Jacova, C.; et al. Advancing research diagnostic criteria for Alzheimer’s disease: the IWG-2 criteria. The Lancet Neurology 2014, 13, 614–629. [Google Scholar] [CrossRef]
- Hernández, R.; Fernández, C.; Baptista, M.P. Metodología de la investigación (6ª ed.). McGraw-Hill, 2014.
- World Medical Association. Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Salami, M.; Alinaghipour, A.; Daneshvar, R.; et al. Adapted MMSE and TYM cognitive tests: how much powerful in screening for Alzheimer’s disease in Iranian people. Aging & Mental Health 2020, 24, 1010–1017. [Google Scholar] [CrossRef]
- Quiroga, L.P.; Albala, C.; Klaasen, P.G. Validación de un test de tamizaje para el diagnóstico de demencia asociada a edad, en Chile. Rev Méd Chile 2004, 132, 467–478. [Google Scholar] [CrossRef]
- Fernández-Barrés, S.; García-Barco, M.; Basora, J.; et al. The efficacy of a nutrition education intervention to prevent risk of malnutrition for dependent elderly patients receiving Home Care: A randomized controlled trial. Int J Nurs Stud 2017, 70, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Aiken, L.R. Tests psicológicos y evaluación (11ª ed.). Pearson Educación, 2003.
- Martínez Pérez, J.A.; Pérez Martin, P.S. La curva ROC [ROC curve]. Semergen 2023, 49, 101821. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Fernández, C.; Custodio, N.; Soto-Añari, M. Neuropsychological profile in the preclinical stages of dementia: principal component analysis approach. Dement Neuropsychol 2021, 15, 192–199. [Google Scholar] [CrossRef]
- Toloza Ramírez, D.; Martella, D. Reserva cognitiva y demencias: Limitaciones del efecto protector en el envejecimiento y el deterioro cognitivo. Rev Méd Chile 2019, 147, 1594–1612. [Google Scholar] [CrossRef]
- Madrigal, L.M.J. La estimulación cognitiva en personas adultas mayores. Rev Cúpula 2007, 11, 57–66. [Google Scholar]
- Nahm, F.S. Receiver operating characteristic curve: overview and practical use for clinicians. Korean J Anesthesiol 2022, 75, 25–36. [Google Scholar] [CrossRef]
- Sarazin, M.; Berr, C.; De Rotrou, J.; et al. Amnestic syndrome of the medial temporal type identifies prodromal AD: a longitudinal study. Neurology 2007, 69, 1859–1867. [Google Scholar] [CrossRef] [PubMed]
- Gainotti, G.; Quaranta, D.; Vita, M.G.; Marra, C. Verbal vs. visual memory in Alzheimer’s disease: a meta-analytical review. J Neurol Neurosurg Psychiatry 2014, 85, 1030–1035. [Google Scholar] [CrossRef]
- Chatzikostopoulos, A.; Moraitou, D.; Tsolaki, M.; et al. Episodic Memory in Amnestic Mild Cognitive Impairment (aMCI) and Alzheimer’s Disease Dementia (ADD): Using the “Doors and People” Tool to Differentiate between Early aMCI-Late aMCI-Mild ADD Diagnostic Groups. Diagnostics 2022, 12, 1768. [Google Scholar] [CrossRef]
- Muñoz-Neira, C.; López, O.L.; Riveros, R.; et al. The technology - activities of daily living questionnaire: a version with a technology-related subscale. Dement Geriatr Cogn Disord 2012, 33, 361–371. [Google Scholar] [CrossRef]
- Nakhla, M.Z.; Banuelos, D.; Pagán, C.; et al. Differences between episodic and semantic memory in predicting observation-based activities of daily living in mild cognitive impairment and Alzheimer’s disease. Appl Neuropsychol Adult 2022, 29, 1499–1510. [Google Scholar] [CrossRef]
- El Haj, M.; Colombel, F.; Kapogiannis, D.; Gallouj, K. False memory in Alzheimer’s disease. Behavioural Neurology 2020, 2020, 5284504. [Google Scholar] [CrossRef]
- Dhamoon, M.S.; Cheung, Y.K.; Gutierrez, J.; et al. Functional trajectories, cognition, and subclinical cerebrovascular disease. Stroke 2018, 49, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Soto-Añari, M.; Custodio, N.; Rivera-Fernández, C. Validación de instrumentos breves para deterioro cognitivo en adultos mayores. Rev Chilena de Neuropsicología 2020, 15, 4–12. [Google Scholar] [CrossRef]
- El Haj, M.; Antoine, P.; Amouyel, P.; Lambert, J.; Pasquier, F.; Kapogiannis, D.; Apolipoprotein, E. (APOE) ε4 and episodic memory decline in Alzheimer’s disease: a review. Ageing Res Rev 2016, 27, 15–22. [Google Scholar] [CrossRef]
- Mungas, D.; Fletcher, E.; Gavett, B.E.; et al. Comparison of education and episodic memory as modifiers of brain atrophy effects on cognitive decline: implications for measuring cognitive reserve. J Int Neuropsychol Soc 2021, 27, 401–411. [Google Scholar] [CrossRef]
- Stern, Y. Cognitive reserve. Neuropsychologia 2009, 47, 2015–2028. [Google Scholar] [CrossRef] [PubMed]
- Mollinedo Cardalda, I.; López, A.; Cancela Carral, J.M. The effects of different types of physical exercise on physical and cognitive function in frail institutionalized older adults with mild to moderate cognitive impairment. A randomized controlled trial. Arch Gerontol Geriatr 2019, 83, 223–230. [Google Scholar] [CrossRef]
- Quiñones-Bermúdez, S.; Restrepo de Mejía, F. Evaluación neuropsicológica de la memoria episódica. Edupsykhé Rev Psicol Educ 2023, 20, 24–55. [Google Scholar] [CrossRef]
- Ihnen-Jory, J.I.; Bruna, A.A.; Muñoz-Neira, C.; Chonchol, A.S. Chilean version of the INECO Frontal Screening (IFS-Ch): psychometric properties and diagnostic accuracy. Dement Neuropsychol 2013, 7, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Sbordone, R.J. Ecological validity: some critical issues for the neuropsychologist. In: Sbordone RJ, Long CJ (eds). St. Lucie Press, 1998. [CrossRef]
- García-Molina, A.; Tirapu Ustárroz, J.; Roig Rovira, T. Validez ecológica en la exploración de las funciones ejecutivas. An Psicol 2007, 23, 289–299, https://www.redalyc.org/pdf/167/16723216.pdf. [Google Scholar]
- Femir-Gurtuna, B.; Kurt, E.; Ulasoglu-Yildiz, C.; et al. White-matter changes in early and late stages of mild cognitive impairment. J Clin Neurosci 2020, 78, 181–184. [Google Scholar] [CrossRef]
- Demonty, M.; Coppalle, R.; Bastin, C.; Geurten, M. The use of distraction to improve episodic memory in ageing: a review of methods and theoretical implications. Can J Exp Psychol 2023, 77, 130–144. [Google Scholar] [CrossRef]
- Alantie, S.; Tyrkkö, J.; Makkonen, T.; Renvall, K. Is old age just a number in language skills? Language performance and its relation to age, education, gender, cognitive screening, and dentition in very old Finnish speakers. J Speech Lang Hear Res 2022, 65, 274–291. [Google Scholar] [CrossRef]
- Delgado-Losada, M.L.; Rubio-Valdehita, S.; Lopez-Higes, R.; et al. How cognitive reserve influences older adults’ cognitive state, executive functions and language comprehension: a structural equation model. Arch Gerontol Geriatr 2019, 84, 103891. [Google Scholar] [CrossRef] [PubMed]
- Arévalo-Rodríguez, I.; Smailagic, N.; Roqué IFiguls, M.; Ciapponi, A.; Sánchez-Pérez, E.; Giannakou, A.; Pedraza, O.L.; Bonfill Cosp, X.; Cullum, S. Mini-Mental State Examination (MMSE) for the detection of Alzheimer’s disease and other dementias in people with mild cognitive impairment (MCI). The Cochrane database of systematic reviews 2015, 3, CD010783. [Google Scholar] [CrossRef]
- Brunette, A.M.; Calamia, M.; Black, J.; Tranel, D. Is episodic future thinking important for instrumental activities of daily living? A study in neurological patients and healthy older adults. Arch Clin Neuropsychol 2019, 34, 403–417. [Google Scholar] [CrossRef]
- Didic, M.; Barbeau, E.J.; Felician, O.; et al. Which memory system is impaired first in Alzheimer’s disease? J Alzheimers Dis 2011, 27, 11–22. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
ROC Curve for TYM-MCI.Figure 1. ROC curve for TYM-MCI and Table 1 with curve coordinates TYM-MCI: (a) Graph showing the cut-off point obtained in TYM-MCI Test. See the cut-off point and area under the curve; (b) Specificity and sensitivity values of the TYM-MCI Test according to the ROC curve calculation.
Figure 1.
ROC Curve for TYM-MCI.Figure 1. ROC curve for TYM-MCI and Table 1 with curve coordinates TYM-MCI: (a) Graph showing the cut-off point obtained in TYM-MCI Test. See the cut-off point and area under the curve; (b) Specificity and sensitivity values of the TYM-MCI Test according to the ROC curve calculation.
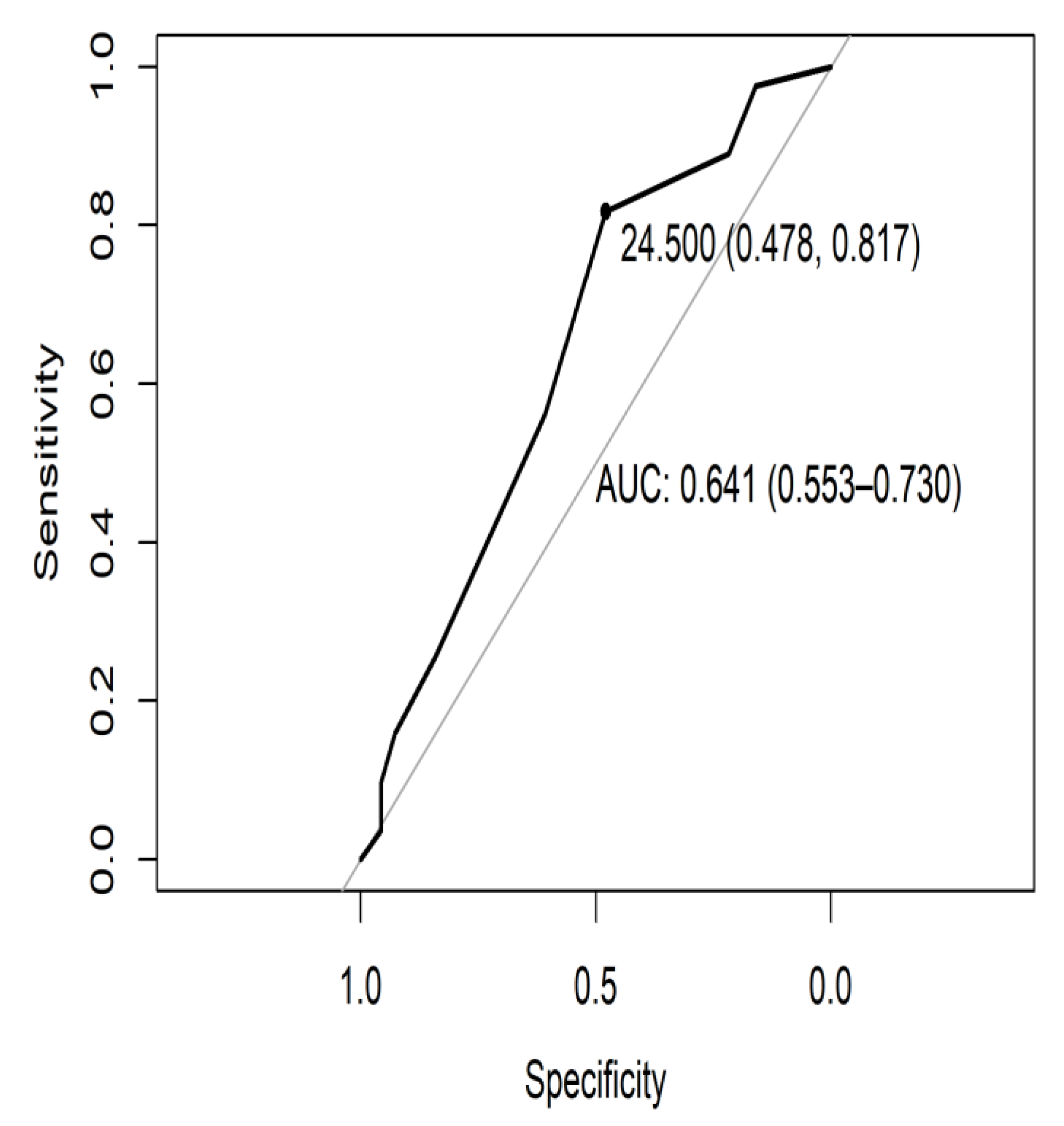
Figure 2.
PCA Graph of variables ACE-R test.
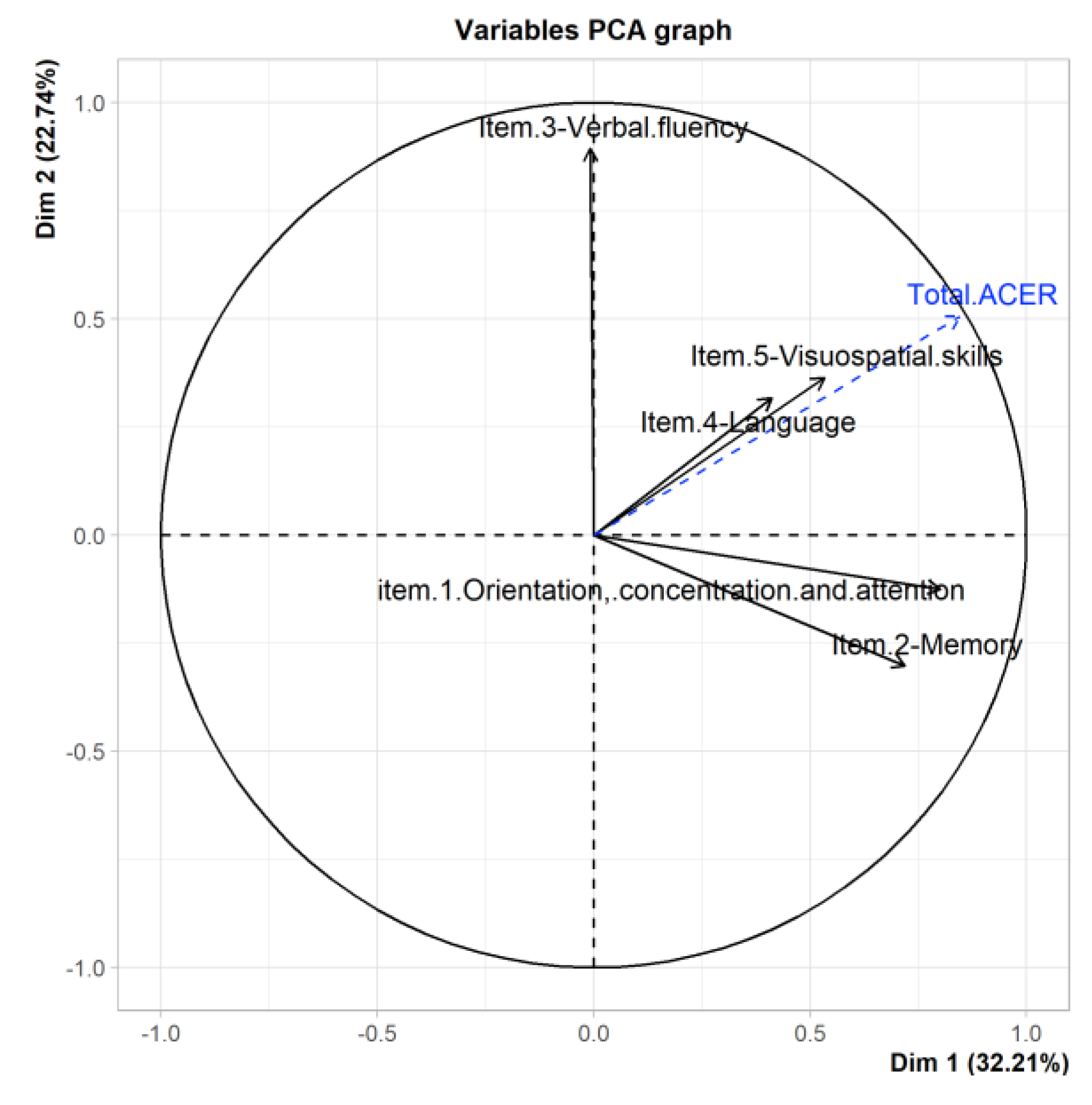
Figure 3.
Graph of variables MMSE test.
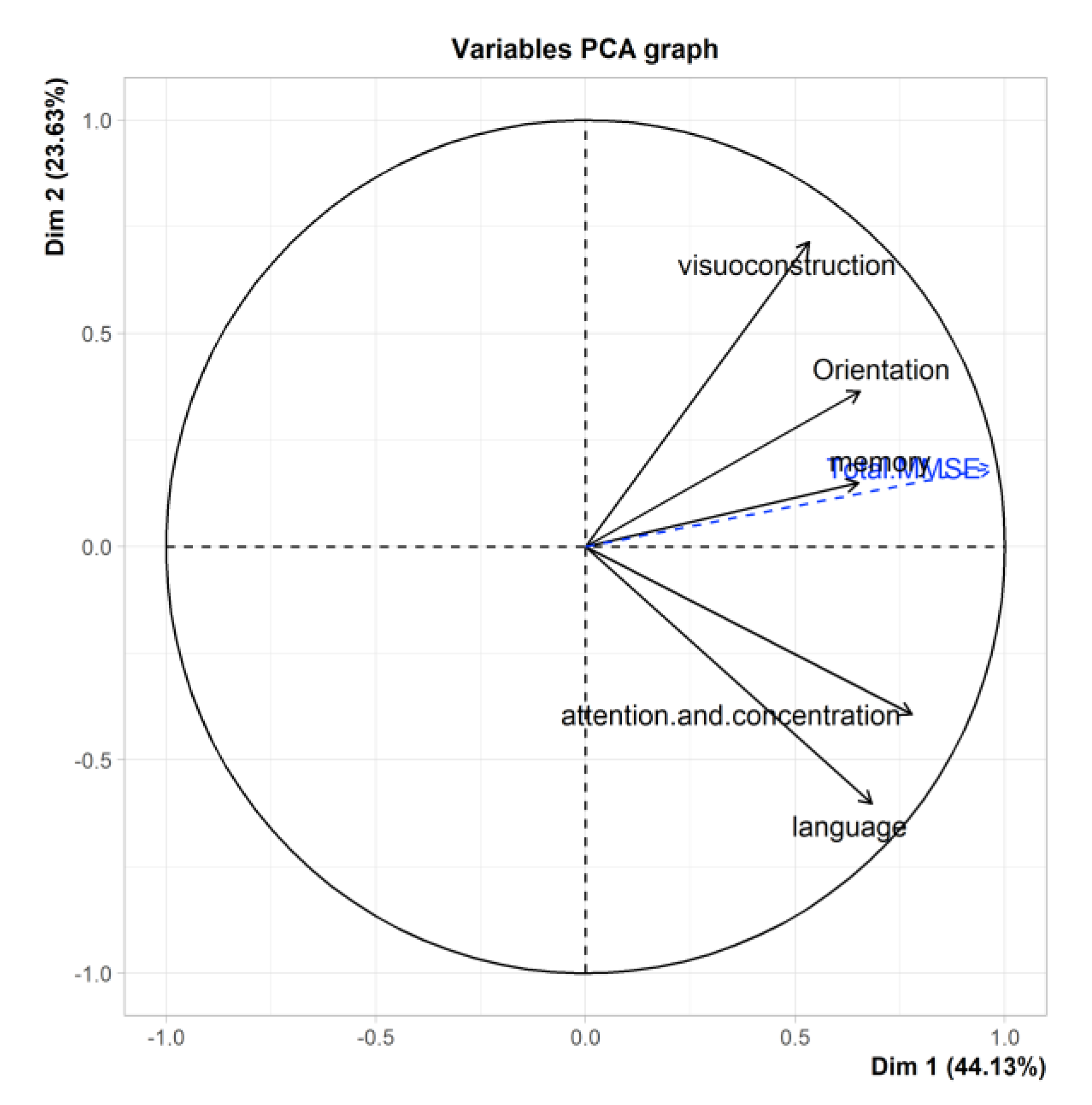
Figure 4.
PCA Graph of variables TYM-S test.
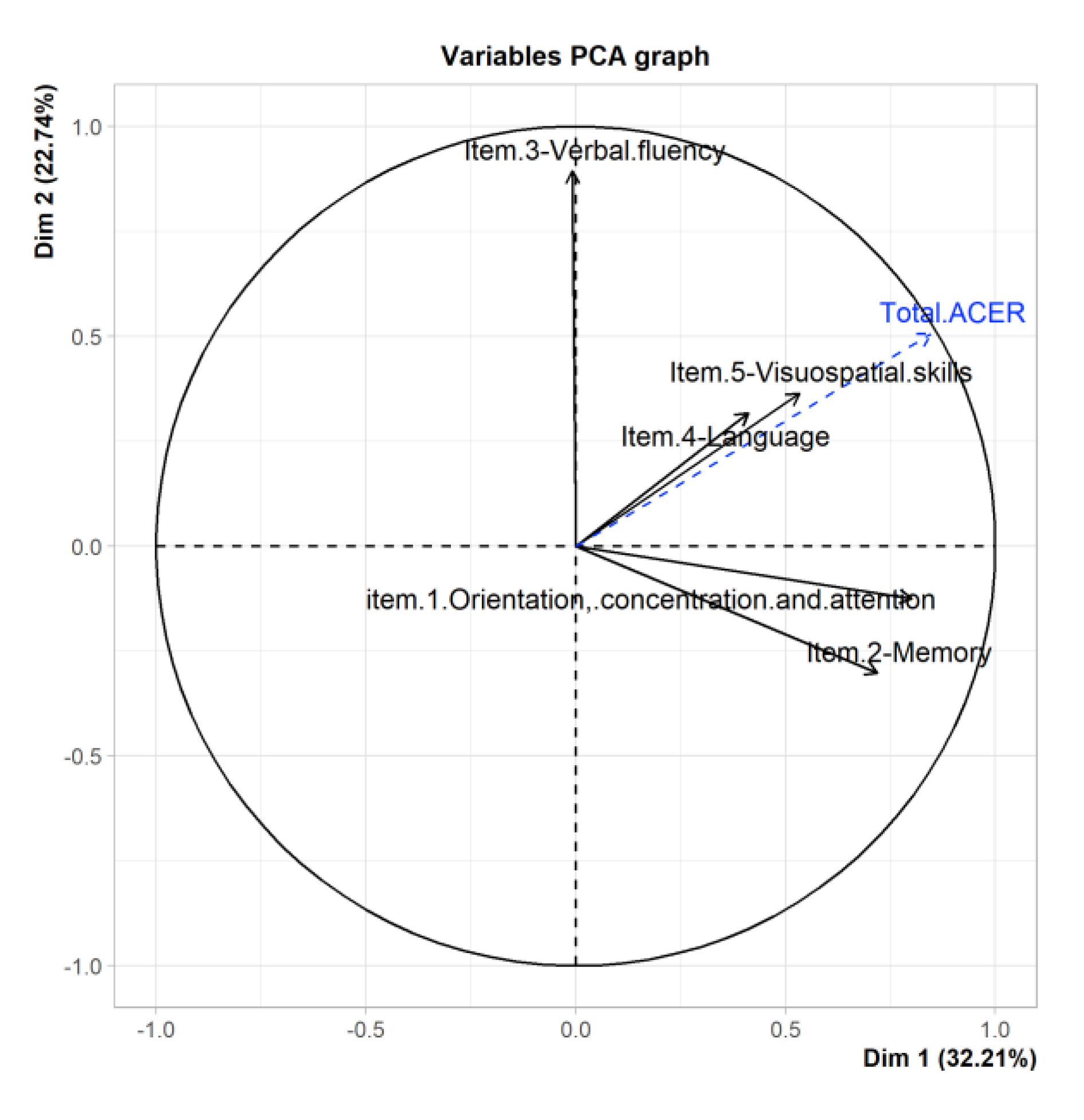
Figure 5.
Graph of variables TYM-MCI test.
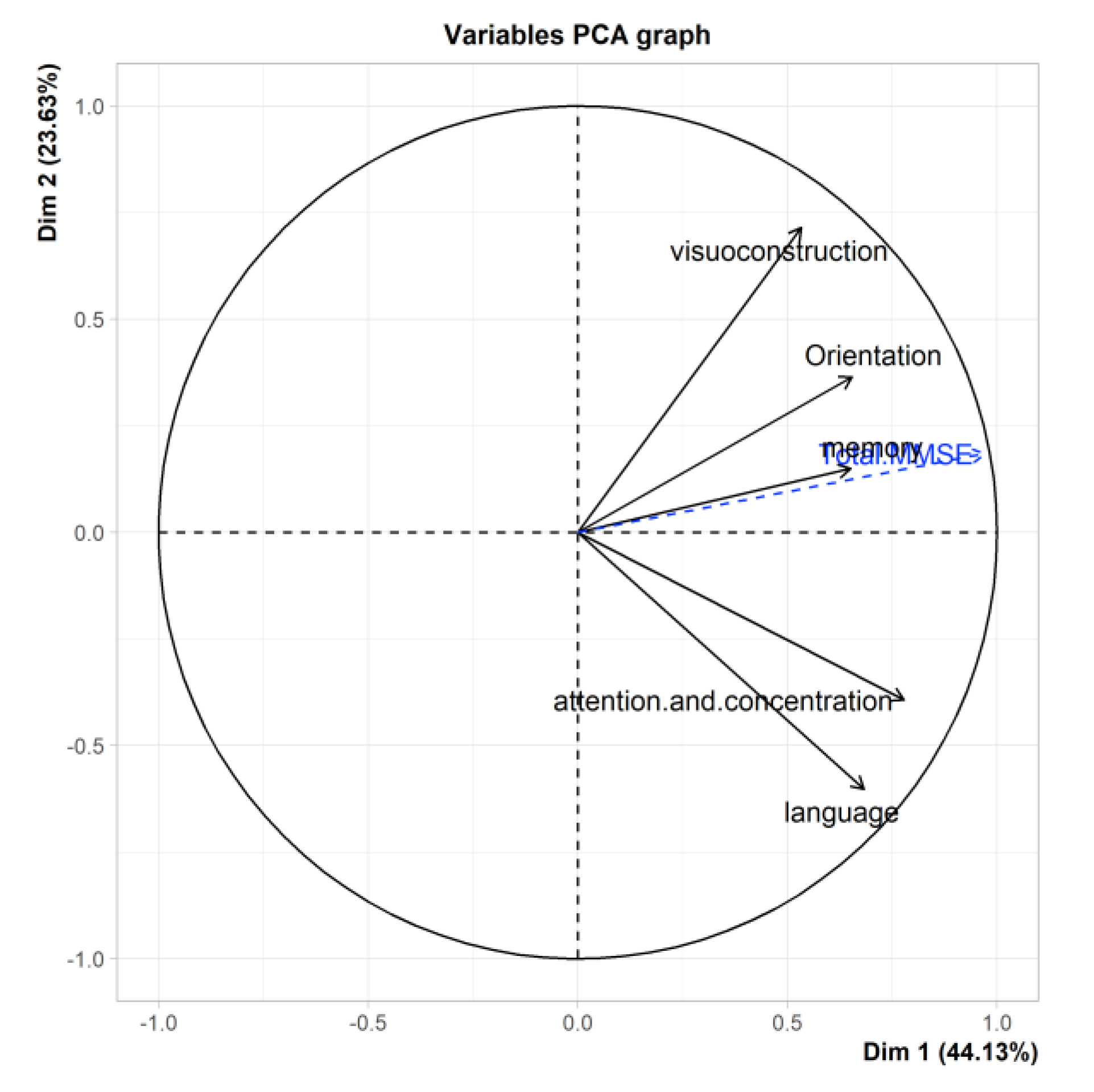

Table 1.
Coordinates TYM-MCI.
| Ptje.* | Sensitivity | Specificity |
|---|---|---|
| 27.5 | 0.976 | 0.159 |
| 26.5 | 0.890 | 0.217 |
| 25.5 | 0.866 | 0.304 |
| 24.5 | 0.817 | 0.478 |
| 23.5 | 0.561 | 0.609 |
| 22.5 | 0.256 | 0.841 |
| 21.5 | 0.159 | 0.928 |
| 20.5 | 0.098 | 0.957 |
| 19.5 | 0.073 | 0.957 |
| 18.5 | 0.037 | 0.957 |
* Positive if greater than or equal to….
Table 2.
Accuracy, Sensitivity and specificity of Cognitive test.
| Episodic Memory | Global Cognitive | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ACER | MMSE | TYM | TYM-MCI | ACER | MMSE | TYM | TYM-MCI | |||
| Accuracy | .702 | .238 | .623 | .675 | Accuracy | .974 | .729 | .828 | .662 | |
| Sensitivity | .333 | .879 | .333 | .121 | Sensitivity | .942 | .841 | .942 | .478 | |
| Specificity | .805 | .059 | .703 | .831 | Specificity | 1.00 | .634 | .732 | .817 | |
Table 3.
Eigenvector components of each test.
| Components of test | Eigenvalue | % Variance | Cumulative % variance |
|---|---|---|---|
| comp 1 ACE R | 1.61 | 32.21 | 32.21 |
| comp 2 ACE R | 1.14 | 22.74 | 54.95 |
| comp 3 ACE R | 1.06 | 21.23 | 76.18 |
| comp 4 ACE R | .674 | 13.49 | 89.66 |
| comp 5 ACE R | .512 | 10.34 | 100.00 |
| comp 1 MMSE | 2.21 | 44.12 | 44.12 |
| comp 2 MMSE | 1.18 | 23.63 | 67.76 |
| comp 3 MMSE | 0.80 | 15.93 | 83.69 |
| comp 4 MMSE | 0.47 | 9.41 | 93.09 |
| comp 5 MMSE | 0.35 | 6.91 | 100.00 |
| comp 1 TYM | 1.95 | 17.71 | 17.71 |
| comp 2 TYM | 1.88 | 17.09 | 34.80 |
| comp 3 TYM | 1.46 | 13.22 | 48.02 |
| comp 4 TYM | 1.12 | 10.18 | 58.21 |
| comp 5 TYM | 1.04 | 9.44 | 67.65 |
| comp 6 TYM | 0.76 | 6.89 | 74.54 |
| comp 7 TYM | 0.68 | 6.15 | 80.69 |
| comp 8 TYM | 0.65 | 5.90 | 86.58 |
| comp 9 TYM | 0.61 | 5.48 | 92.07 |
| comp 10 TYM | 0.56 | 5.09 | 97.16 |
| comp 11 TYM | 0.31 | 2.84 | 100.00 |
| comp 1 TYM-MCI | 1.295 | 32.384 | 32.384 |
| comp 2 TYM-MCI | 1.061 | 26.517 | 58.901 |
| comp 3 TYM-MCI | 0.860 | 21.499 | 80.401 |
| comp 4 TYM-MCI | 0.784 | 19.599 | 100.000 |
Table 4.
Correlations variables eigenvectors cognitive test. Each test projected as the dependent variable.
Table 4.
Correlations variables eigenvectors cognitive test. Each test projected as the dependent variable.
| Sub ítem | Dim.1 | Dim.2 | Dim.3 | Dim.4 | Dim.5 | Dim.6 | Dim.7 |
|---|---|---|---|---|---|---|---|
| Orientation ACE-R | 0.80 | -0.13 | -0.26 | 0.16 | -0.50 | X | X |
| Memory ACE-R | 0.72 | -0.30 | 0.32 | 0.35 | 0.40 | X | X |
| Verbal fluency ACE-R | -0.007 | 0.89 | 0.06 | 0.45 | -0.01 | X | X |
| Language ACE-R | 0.41 | 0.32 | 0.72 | -0.44 | -0.11 | X | X |
| Visuospatial skills ACE-R | 0.53 | 0.36 | -0.60 | -0.36 | 0.30 | X | X |
| Total ACE-R | 0.85 | 0.51 | 0.03 | 0.14 | 0.09 | X | X |
| Orientation MMSE | 0.65 | 0.36 | -0.53 | -0.38 | 0.09 | X | X |
| Attention and concentration MMSE | 0.78 | -0.39 | -0.22 | 0.18 | -0.40 | X | X |
| Memory MMSE | 0.65 | 0.15 | 0.67 | -0.30 | -0.10 | X | X |
| Language MMSE | 0.68 | -0.60 | 0.07 | 0.11 | 0.40 | X | X |
| Visuospatial construction MMSE | 0.53 | 0.71 | 0.07 | 0.44 | 0.08 | X | X |
| Total MMSE | 0.97 | 0.19 | 0.054 | -0.15 | 0.002 | X | X |
| Time-space orientation TYM | 0.42 | 0.64 | -0.31 | 0.15 | 0.21 | -0.16 | -0.12 |
| Direct copy to writing TYM | 0.37 | 0.64 | -0.24 | 0.18 | -0.27 | 0.11 | 0.40 |
| Episodic memory TYM | 0.54 | -0.07 | 0.15 | 0.49 | -0.17 | 0.42 | -0.48 |
| Functional calculation TYM | 0.53 | 0.14 | -0.08 | 0.03 | 0.67 | 0.04 | 0.15 |
| Semantic memory TYM | 0.04 | 0.17 | 0.68 | -0.27 | 0.46 | 0.17 | -0.06 |
| Similarities TYM | 0.62 | -0.32 | 0.04 | -0.28 | -0.07 | -0.41 | -0.12 |
| Delayed recall and semantic memory TYM | 0.58 | -0.24 | 0.39 | -0.29 | -0.29 | 0.30 | 0.36 |
| Visual agnosia and tracking TYM | -0.18 | -0.35 | -0.60 | -0.20 | 0.30 | 0.44 | 0.03 |
| Visuoconstruction and visuospatial skills TYM | -0.23 | -0.17 | 0.46 | 0.66 | 0.20 | -0.13 | 0.25 |
| Deferred recall TYM | -0.50 | 0.54 | 0.14 | -0.07 | -0.08 | 0.19 | 0.005 |
| Evaluator TYM | -0.07 | 0.64 | 0.26 | -0.33 | -0.08 | -0.01 | -0.20 |
| Total TYM | 0.40 | 0.50 | 0.21 | -0.004 | 0.31 | 0.26 | 0.06 |
| Visual episodic memory + visoconstruction + delayed recall |
-0.48 |
-0.57 |
0.65 |
0.10 |
X |
X |
X |
| Episodic verbal memory + delayed recall |
-0.15 |
0.84 |
0.53 |
0.001 |
X |
X |
X |
| Verbal episodic memory + semantic + delayed recall |
0.73 |
-0.06 |
0.21 |
0.65 |
X |
X |
X |
| Episodic visual + semantic + deferred recall |
0.71 |
-0.16 |
0.34 |
-0.60 |
X |
X |
X |
| Total TYM-MCI | 0.12 | -0.30 | 0.93 | 0.16 | X | X | X |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



