
Submitted:
28 November 2025
Posted:
01 December 2025
You are already at the latest version
Abstract
Metastases to the pancreas (PM), although rare, have been increasingly identified in recent years, especially among high-volume pancreatic centers. They are often asymptomatic and incidentally detected during follow-up examinations, even several years after the treatment of the primary tumor. In this scenario, endoscopic ultrasound (EUS) has emerged as a crucial diagnostic tool for PM, being capable of providing a detailed morphological characterization and safe and effective tissue acquisition for cytohistological examination. The aim of our study was to extensively review the current evidence concerning the role of EUS in the diagnosis of PM, specifically focusing on their morphological features, contrast-enhancement patterns, and tissue acquisition techniques.
Keywords:
pancreatic metastases
; EUS
; EUS-TA
; CH-EUS
1. Introduction
Metastases to the pancreas (PM) are relatively uncommon conditions, representing approximately 2–5% of all pancreatic malignancies in surgical and oncologic series, and up to 15% among autopsy studies [1,2,3]. Given PM commonly mimic primary pancreatic ductal adenocarcinoma (PDAC) in clinical presentation and cross-sectional imaging, a definitive diagnosis is imperative, as management and prognosis differ substantially [4,5,6]. Since its advent [7,8,9], endoscopic ultrasound (EUS) has gradually emerged as the cornerstone for the characterization of solid pancreatic lesions, being capable of providing unmatched spatial resolution for pancreatic parenchyma and enabling simultaneous tissue acquisition for cyto-histological diagnosis [10,11].
EUS-guided tissue acquisition (EUS-TA), including fine-needle aspiration (FNA) and fine-needle biopsy (FNB), is essential for the definitive cytohistological diagnosis of PM. Indeed, EUS-TA has been shown to be associated with high diagnostic accuracy rates and negligible adverse events rates for solid pancreatic lesions, including PM [12,13,14,15,16,17,18].
In recent years, contrast-enhanced EUS (CH-EUS) has further refined lesion characterization by accurately visualizing microvascular perfusion patterns [19]. Anyway, although CH-EUS enhances diagnostic confidence, tissue confirmation remains mandatory, as contrast patterns may overlap with neuroendocrine tumors and atypical PDAC [20,21].
Accurate diagnosis of PM is crucial, having a direct impact on their subsequent management. For instance, patients with isolated metastases may benefit from surgical resection with long-term survival, while the recognition of disseminated disease prevents unnecessary surgery and guides systemic therapy [22,23,24].
Given the increasing detection of PM in the era of long-term cancer survivorship and the key role played by EUS in this scenario, a comprehensive understanding of EUS morphology, CH-EUS patterns, and tissue-acquisition strategies is essential. Our narrative review aimed to summarize and discuss the current evidence regarding the role of EUS in diagnosing PM, specifically focusing on their morphological features, CH-EUS patterns, tissue acquisition techniques, and their clinical implications.
2. Literature Search
We performed a comprehensive literature search in the PubMed/MEDLINE, Google Scholar and Embase databases up to September 2025 in order to identify relevant studies investigating the role of EUS in the diagnosis of PM.
The search included combinations of Medical Subject Headings (MeSH) and free-text terms related to pancreas, metastases, EUS, and tissue acquisition techniques.
The medical search strategy used the terms “pancreas,” “pancreatic,” “metastases,” “metastatic,” “secondary tumor,” “solid lesions”, “endoscopic ultrasound,” “endoscopic ultrasonography,” “EUS,” “endosonography,” “fine-needle aspiration,” “fine-needle biopsy,” “FNA,” “FNB,” “contrast-enhanced endoscopic ultrasound,” and “CH-EUS” in various combinations, using the Boolean operators AND, OR, and NOT. The search was limited to English-language human studies. Additional relevant articles were carefully identified by manual screening of the reference lists of retrieved publications and pertinent reviews. Meeting abstracts, individual case reports, case series (<5 cases), review articles, position papers, editorials, commentaries, and book chapters were excluded from our review.
3. Role of Endoscopic Ultrasound in Pancreatic Metastases
A total of 26 studies were included in the final analysis [4,5,10,12,13,14,15,16,20,22,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40]. All were retrospective in nature. Three were case series [10,32,36], sixteen were single-center studies [4,5,13,14,15,20,25,27,28,29,30,31,33,35,37,38], and seven were multicenter studies [12,16,22,26,34,39,40]. The main characteristics of the included studies are summarized in Table 1 and Table 2.
3.1. Population Characteristics
The median age at diagnosis of PM ranged from 57 to 72 years, with a slight male predominance [4,5,12,13,14,15,16,20,22,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40]. The largest included studies identified PM in approximately 1–6% of pancreatic masses sampled [5,10,13,14,15,20,26,27,28,30,34,38,39,40]. Most patients were asymptomatic or presented with non-specific symptoms such as abdominal pain, weight loss, or jaundice [12,14,15,16,25,27,30,35,39]. In several series, over two-thirds of cases were incidentally detected during oncologic follow-up imaging [16,27,30,36]. Notably, a long-time interval between the diagnosis of the primary tumor and the detection of PM, up to 25 years, was reported, especially among patients affected by renal cell carcinoma (RCC) [16,25,26,28]. Interestingly, Betes et al. noted that PM from lung carcinoma had a significantly shorter latency time than those from RCC [14]. Synchronous presentations, in which the PM was discovered concurrently with or shortly after the primary tumor, were observed in 10–30% of cases [15,16,25].
3.2. Primary Tumors
RCC consistently emerged as the predominant source of PM, accounting for 17–65% of cases among the included studies [5,10,15,16,22,25,26,27,28,29,33,36,40]. Other common primaries included lung carcinoma (8-38%), colorectal adenocarcinoma (4-18%), breast carcinoma (4-18%), melanoma (3-14%), and sarcomas or lymphomas (each 1-10%) [4,5,10,12,13,14,15,16,20,22,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39]. Less common primaries reported include gastric adenocarcinoma, hepatocellular carcinoma, prostate, thyroid, and gynecologic tumors [13,14,15,31,39]. The recent multicenter study by Cui et al. added valuable histopathologic detail, emphasizing the wide spectrum of tumors potentially metastasizing to the pancreas. Indeed, epithelial neoplasms represented 73% of cases, most often RCC, lung adenocarcinoma, and Müllerian-type carcinomas, while non-epithelial metastases originated from hematologic malignancies, sarcomas, and melanoma [34].
3.3. Size, Localization and Focality
Mean lesion size ranged from 15 to 42 mm, with extremes from a few millimeters to over 13 cm [4,10,12,13,14,15,16,20,25,27,28,30,31,33,34,37,38,39]. Lesions were distributed throughout the gland, with a slight predilection for the pancreatic head (17– 83%), followed by the body (9–73%) and the tail (7–27%) [4,5,12,14,15,16,20,25,26,27,28,29,30,31,32,33,34,37,38,39,40]. Multifocality was observed in approximately 10–25% of cases, particularly in RCC metastases [13,25,27,36,39].
3.4. Endoscopic Ultrasound Morphological Features
EUS provides a detailed morphological characterization of PM. PM are typically described as well-demarcated, hypoechoic, and homogeneous lesions, often oval or round in shape [4,10,12,15,16,20,22,25,27,30,31,35,37,39]. As compared to PDAC, which is typically irregular and hypoechoic with poorly defined borders, PM exhibit a clearer interface with surrounding parenchyma (marginal hypoechoic zone, MHZ) [31]. While PDAC is mostly hypovascular, PM frequently appear hypervascular [10,15,16,20]. Notably, pancreatic duct dilatation and parenchymal atrophy, hallmarks of PDAC, were uncommon in metastases, even when lesions were located within the head [31,33]. These features, together with well-defined margins, should promptly raise suspicion for a secondary rather than a primary pancreatic tumor. Aversano et al. [15] recently proposed a composite set of EUS features for PM, noting that the combination of hypoechoic echogenicity, hyper or moderate vascularity, oval or roundish shape with well-defined margins, and hardness on elastography was strongly associated with secondary lesions. Nevertheless, they emphasized that EUS morphology alone is insufficient to differentiate PM from pancreatic neuroendocrine tumors or some solid pseudopapillary neoplasms, underscoring the final need for histologic confirmation.
EUS morphological features of PM are illustrated in Figure 1.
3.5. Contrast-Enhanced Endoscopic Ultrasound Features
CH-EUS has a well-known added value to the evaluation of pancreatic masses and, consequently, of PM, providing valuable information on their vascularity. Studies assessing CH-EUS in PM reported that the majority of metastatic lesions, especially from RCC, display hyperenhancement in the arterial phase [20,37], followed by rapid washout [20]. This vascular pattern contrasts sharply with the hypoenhancement typically observed in PDAC, which reflects its desmoplastic and hypovascular stroma [20]. In the study from Fusaroli et al. [37], hypervascularity was a consistent feature of RCC metastases, while hypovascular or hypo- or isoenhancing patterns were more common in PM from colorectal or breast carcinoma, concluding that the finding of a hyperenhancing lesion in a patient with a previous cancer history, especially if renal or hematological, should prompt EUS-TA.
The CH-EUS behavior of solid pancreatic lesions is illustrated in Figure 2.
3.6. Diagnostic Yield and Final Diagnostic Method
EUS-TA (EUS-FNA/B) is universally regarded as the cornerstone of diagnosis for PM [12,14,15,25]. Early experience from Fritscher-Ravens et al. [4] reported a EUS-FNA sensitivity at 88% with near-perfect specificity and negligible complication rates. Following single-center and multicenter studies [25,29,30,38,39] confirmed accuracy of 85–92%, with diagnostic material obtained in over 90% of cases. More recent studies [15,16,34] consistently exceed 90–95% diagnostic yield, mainly due to EUS-FNB availability, larger-gauge systems, and improved cell-block preparation. Where described, the median number of needle passes through the lesion ranged from 2 to 3 [15,16,25,27,28,31,33,35,39] The addition of immunohistochemistry (IHC) is critical to determine the primary origin, especially in patients with prior malignancies or ambiguous morphology [16,34]. In 2025, Cui et al. [34] showed the morphological overlap between PM and PDAC, emphasizing that EUS-FNB specimens are sufficient for extended IHC and even molecular testing, thereby confirming the current shift from cytology to histology-based diagnosis. Currently, EUS-FNB is the preferred modality for EUS-TA in most centers when PM is suspected, as it provides more intact tissue cores, allowing for cell block preparation, immunostaining, and molecular comparison with prior specimens [15,16].
3.7. Treatment and Outcomes
Management of PM should be patient-tailored and specifically guided by the primary tumor type, disease burden, and patient performance status in a multidisciplinary approach. Surgery should be considered whenever a potentially curative resection is feasible, particularly in RCC, with a reported good long-term survival after pancreatectomy in several studies [14,22,28,38]. Conversely, non-surgical strategies such as systemic anticancer therapy, stereotactic radiotherapy, or endoscopic palliation, is generally applied in disseminated disease [4,15,27]. Prognosis is poor especially in small-cell lung or breast cancer PM, matching that of the metastatic primary.
4. Discussion and Conclusions
Over the past decades, EUS has redefined the diagnostic approach to PM, converting a historically post-surgical or autoptic finding into a clinically feasible diagnosis [1,2]. Although PM currently represent only 1–6% of pancreatic malignancies in large EUS series [5,10,13,14,15,20,26,27,28,30,34,38,39,40], the growing population of long-term cancer survivors has increased their recognition. RCC emerged as the most common primary tumor originating PM, representing 17-65% of all diagnosis [5,10,15,16,22,25,26,27,28,29,33,36,40]. This evidence has remained stable over time, reflecting the prolonged survival of RCC patients and the tumor’s particular tropism for the pancreatic tissue [41]. Early reports like Fritscher-Ravens et al. [4], Mesa et al. [5] and DeWitt et al. [12] demonstrated the feasibility of EUS-FNA, but subsequent studies have consolidated its role as the first-line diagnostic tool. Large series and multicenter studies have confirmed a diagnostic accuracy exceeding 90%, with negligible complication rates [25,29,30,39,40]. EUS-FNB has been progressively integrated to FNA, enabling more tissue to be sampled and a major feasibility and accuracy of IHC and molecular comparison with the primary tumor. In the recent studies by Spadaccini et al. [16] and Cui et al. [34], EUS-FNB provided sufficient tissue for extended immunophenotyping, marking a shift from cytology to histology-based diagnosis. These data align with those from previous literature findings, which have underscored the pivotal role of IHC in confirming the metastatic nature of pancreatic lesions and differentiating them from PDAC, when morphology alone was insufficient [27,40]. Advanced imaging techniques have also provided a significant contribution to the characterization of these lesions. In particular, CH-EUS allowed a real-time functional study, enabling a more accurate assessment of vascularity. Several studies have shown that most PM, especially those from RCC, display hyperenhancement in the arterial phase, contrasting with the hypovascular pattern of PDAC [20,37]. Fusaroli et al. [37] and Teodorescu et al. [20] confirmed that CH-EUS increases diagnostic confidence but cannot replace tissue confirmation, as hypovascular metastases from colorectal or breast carcinoma remain a frequent source of false negatives. These findings emphasize that the strength of EUS lies not only in morphology but also in its capability to integrate vascular and cytologic information during a single procedure. From a clinical standpoint, EUS-based diagnosis directly influences management strategies. The detection of a secondary tumor to the pancreas rather than primary pancreatic tumor significantly alters prognosis and treatment [24,42]. A multidisciplinary team approach is crucial for the proper diagnosis and treatment of PM. Endosonographers, radiologists, pathologists, oncologists and surgeons should deeply cooperate to interpret imaging and histological findings in the context of the patient’s history. Despite the marked progress achieved, current evidence is limited by the retrospective nature of all the included studies, their relatively small sample size, and heterogeneity in reporting. Only a few studies have prospectively compared FNA and FNB or standardized CH-EUS descriptors [20,43,44,45,46].
Artificial intelligence (AI) is also emerging as an ancillary technique in EUS especially after the introduction of Convolutional Neural Network (CNN) technology which have completely revolutionized image classification. In fact, CNN automatically learn hierarchical features from images, allowing for more accurate and robust classification results and high-performance prediction, allowing real-time lesion characterization, segmentation, and classification [47]. There is a scan of literature evidence about the detection of PM with AI. In particular, Kuwahara et al. published a retrospective study about the application of CNN using EfficientNetV2-L (22 000 images generated from 933 patients), able to differentiate PDAC from other benign and malignant lesions, including PM, achieving an accuracy of 91.0%, sensitivity of 94% and specificity of 82% [48].
In conclusion, EUS with EUS-TA currently represents the mainstay for the accurate diagnosis of PM, combining a very high accuracy with minimal morbidity. Furthermore, its combination with CH-EUS and modern EUS-FNB devices allow precision in both macroscopic and microscopic characterization, enabling more tailored therapeutic decisions. Future large multicentric prospective studies should aim to harmonize reporting standards, validate quantitative perfusion and elastographic metrics, and explore molecular profiling from EUS-FNB cores as a platform for personalized oncology.
Author Contributions
Conceptualization, M.R., A.M. and M.A.; resources, M.R., A.M., M.A., F.P.Z., R.F., D.S. and S.C.; writing—original draft preparation, M.R., A.M., M.A. and F.P.Z.; writing—review and editing, M.R., A.M., M.A., F.P.Z., R.F., D.S., S.C. and L.B.; visualization, M.R., A.M., M.A., and L.B.; supervision, F.R., C.M., R.D.M., G.S., L.B. and G.L.; project administration, A.M. and G.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| PM | Metastases to the pancreas |
| EUS | Endoscopic ultrasound |
| PDAC | Primary pancreatic ductal adenocarcinoma |
| EUS-TA | EUS-guided tissue acquisition |
| FNA | Fine-needle aspiration |
| FNB | Fine-needle biopsy |
| CH-EUS | Contrast-enhanced EUS |
| MeSH | Medical Subject Headings |
| RCC | Renal cell carcinoma |
| MHZ | Marginal hypoechoic zone |
| IHC | Immunohistochemistry |
| AI | Artificial Intelligence |
| CNN | Convolutional Neural Network |
References
- Adsay, N. V.; Andea, A.; Basturk, O.; Kilinc, N.; Nassar, H.; Cheng, JeanetteD. Secondary Tumors of the Pancreas: An Analysis of a Surgical and Autopsy Database and Review of the Literature. Virchows Archiv 2004, 444 (6). [CrossRef]
- Nakamura, E.; Shimizu, M.; Itoh, T.; Manabe, T. Secondary Tumors of the Pancreas: Clinicopathological Study of 103 Autopsy Cases of Japanese Patients. Pathol Int 2001, 51(9), 686–690. [Google Scholar] [CrossRef]
- David, O.; Green, L.; Reddy, V.; Kluskens, L.; Bitterman, P.; Attal, H.; Prinz, R.; Gattuso, P. Pancreatic Masses: A Multi-Institutional Study of 364 Fine-Needle Aspiration Biopsies with Histopathologic Correlation. Diagn Cytopathol 1998, 19(6), 423–427. [Google Scholar] [CrossRef]
- Fritscher-Ravens, A.; Sriram, P. V. J.; Krause, C.; Atay, Z.; Jaeckle, S.; Thonke, F.; Brand, B.; Bohnacker, S.; Soehendra, N. Detection of Pancreatic Metastases by EUS-Guided Fine-Needle Aspiration. Gastrointest Endosc 2001, 53(1), 65–70. [Google Scholar] [CrossRef]
- Mesa, H.; Stelow, E. B.; Stanley, M. W.; Mallery, S.; Lai, R.; Bardales, R. H. Diagnosis of Nonprimary Pancreatic Neoplasms by Endoscopic Ultrasound-guided Fine-needle Aspiration. Diagn Cytopathol 2004, 31(5), 313–318. [Google Scholar] [CrossRef]
- Triantopoulou, C.; Kolliakou, E.; Karoumpalis, I.; Yarmenitis, S.; Dervenis, C. Metastatic Disease to the Pancreas: An Imaging Challenge. Insights Imaging 2012, 3(2), 165–172. [Google Scholar] [CrossRef]
- Strohm, W. D.; Phillip, J.; Hagenmüller, F.; Classen, M. Ultrasonic Tomography by Means of an Ultrasonic Fiberendoscope. Endoscopy 1980, 12(05), 241–244. [Google Scholar] [CrossRef] [PubMed]
- Vilmann, P.; Jacobsen, G. K.; Henriksen, F. W.; Hancke, S. Endoscopic Ultrasonography with Guided Fine Needle Aspiration Biopsy in Pancreatic Disease. Gastrointest Endosc 1992, 38(2), 172–173. [Google Scholar] [CrossRef] [PubMed]
- Wiersema, M. J.; Hawes, R. H.; Tao, L.-C.; Wiersema, L. M.; Kopecky, K. K.; Rex, D. K.; Kumar, S.; Lehman, G. A. Endoscopic Ultrasonography as an Adjunct to Fine Needle Aspiration Cytology of the Upper and Lower Gastrointestinal Tract. Gastrointest Endosc 1992, 38(1), 35–39. [Google Scholar] [CrossRef]
- Palazzo, L.; Borotto, E.; Cellier, C.; Roseau, G.; Chaussade, S.; Couturier, D.; Paolaggi, J. A. Endosonographic Features of Pancreatic Metastases. Gastrointest Endosc 1996, 44(4), 433–436. [Google Scholar] [CrossRef]
- Pouw, R. E.; Barret, M.; Biermann, K.; Bisschops, R.; Czakó, L.; Gecse, K. B.; de Hertogh, G.; Hucl, T.; Iacucci, M.; Jansen, M.; Rutter, M.; Savarino, E.; Spaander, M. C. W.; Schmidt, P. T.; Vieth, M.; Dinis-Ribeiro, M.; van Hooft, J. E. Endoscopic Tissue Sampling – Part 1: Upper Gastrointestinal and Hepatopancreatobiliary Tracts. European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2021, 53 (11), 1174–1188. [CrossRef]
- DeWitt, J.; Jowell, P.; LeBlanc, J.; McHenry, L.; McGreevy, K.; Cramer, H.; Volmar, K.; Sherman, S.; Gress, F. EUS-Guided FNA of Pancreatic Metastases: A Multicenter Experience. Gastrointest Endosc 2005, 61(6), 689–696. [Google Scholar] [CrossRef] [PubMed]
- Smith, A. L.; Odronic, S. I.; Springer, B. S.; Reynolds, J. P. Solid Tumor Metastases to the Pancreas Diagnosed by FNA: A Single-institution Experience and Review of the Literature. Cancer Cytopathol 2015, 123(6), 347–355. [Google Scholar] [CrossRef]
- Betés, M.; González Vázquez, S.; Bojórquez, A.; Lozano, M. D.; Echeveste, J. I.; García Albarrán, L.; Muñoz Navas, M.; Súbtil, J. C. Metastatic Tumors in the Pancreas: The Role of Endoscopic Ultrasound-Guided Fine-Needle Aspiration. Revista Española de Enfermedades Digestivas 2019, 111. [CrossRef]
- Aversano, A.; Lissandrini, L.; Macor, D.; Carbone, M.; Cassarano, S.; Marino, M.; Giuffrè, M.; De Pellegrin, A.; Terrosu, G.; Berretti, D. The Role of Endoscopic Ultrasonography (EUS) in Metastatic Tumors in the Pancreas: 10 Years of Experience from a Single High-Volume Center. Diagnostics 2024, 14(12), 1250. [Google Scholar] [CrossRef]
- Spadaccini, M.; Conti Bellocchi, M. C.; Mangiavillano, B.; Fantin, A.; Rahal, D.; Manfrin, E.; Gavazzi, F.; Bozzarelli, S.; Crinò, S. F.; Terrin, M.; Di Leo, M.; Bonifacio, C.; Facciorusso, A.; Realdon, S.; Cristofori, C.; Auriemma, F.; Fugazza, A.; Frulloni, L.; Hassan, C.; Repici, A.; Carrara, S. Secondary Tumors of the Pancreas: A Multicenter Analysis of Clinicopathological and Endosonographic Features. J Clin Med 2023, 12(8), 2829. [Google Scholar] [CrossRef]
- Masuda, S.; Koizumi, K.; Shionoya, K.; Jinushi, R.; Makazu, M.; Nishino, T.; Kimura, K.; Sumida, C.; Kubota, J.; Ichita, C.; Sasaki, A.; Kobayashi, M.; Kako, M.; Haruki, U. Comprehensive Review on Endoscopic Ultrasound-Guided Tissue Acquisition Techniques for Solid Pancreatic Tumor. World J Gastroenterol 2023, 29(12), 1863–1874. [Google Scholar] [CrossRef]
- Hewitt, M. J.; McPhail, M. J. W.; Possamai, L.; Dhar, A.; Vlavianos, P.; Monahan, K. J. EUS-Guided FNA for Diagnosis of Solid Pancreatic Neoplasms: A Meta-Analysis. Gastrointest Endosc 2012, 75(2), 319–331. [Google Scholar] [CrossRef] [PubMed]
- Fusaroli, P.; Napoleon, B.; Gincul, R.; Lefort, C.; Palazzo, L.; Palazzo, M.; Kitano, M.; Minaga, K.; Caletti, G.; Lisotti, A. The Clinical Impact of Ultrasound Contrast Agents in EUS: A Systematic Review According to the Levels of Evidence. Gastrointest Endosc 2016, 84 (4), 587-596.e10. [CrossRef]
- Teodorescu, C.; Bolboaca, S. D.; Rusu, I.; Pojoga, C.; Seicean, R.; Mosteanu, O.; Sparchez, Z.; Seicean, A. Contrast Enhanced Endoscopic Ultrasound in the Diagnosis of Pancreatic Metastases. Med Ultrason 2022. [CrossRef] [PubMed]
- Kitano, M.; Kamata, K.; Imai, H.; Miyata, T.; Yasukawa, S.; Yanagisawa, A.; Kudo, M. Contrast-enhanced Harmonic Endoscopic Ultrasonography for Pancreatobiliary Diseases. Digestive Endoscopy 2015, 27 (S1), 60–67. [Google Scholar] [CrossRef]
- Moussa, A.; Mitry, E.; Hammel, P.; Sauvanet, A.; Nassif, T.; Palazzo, L.; Malka, D.; Delchier, J.-C.; Buffet, C.; Chaussade, S.; Aparicio, T.; Lasser, P.; Rougier, P.; Lesur, G. Pancreatic Metastases: A Multicentric Study of 22 Patients. Gastroenterol Clin Biol 2004, 28(10), 872–876. [Google Scholar] [CrossRef]
- Ballarin, R. Pancreatic Metastases from Renal Cell Carcinoma: The State of the Art. World J Gastroenterol 2011, 17(43), 4747. [Google Scholar] [CrossRef]
- Reddy, S.; Edil, B. H.; Cameron, J. L.; Pawlik, T. M.; Herman, J. M.; Gilson, M. M.; Campbell, K. A.; Schulick, R. D.; Ahuja, N.; Wolfgang, C. L. Pancreatic Resection of Isolated Metastases from Nonpancreatic Primary Cancers. Ann Surg Oncol 2008, 15(11), 3199–3206. [Google Scholar] [CrossRef]
- El Hajj, I. I.; LeBlanc, J. K.; Sherman, S.; Al-Haddad, M. A.; Cote, G. A.; McHenry, L.; DeWitt, J. M. Endoscopic Ultrasound–Guided Biopsy of Pancreatic Metastases. Pancreas 2013, 42(3), 524–530. [Google Scholar] [CrossRef] [PubMed]
- Waters, L.; Si, Q.; Caraway, N.; Mody, D.; Staerkel, G.; Sneige, N. Secondary Tumors of the Pancreas Diagnosed by Endoscopic Ultrasound-guided Fine-needle Aspiration: A 10-year Experience. Diagn Cytopathol 2014, 42(9), 738–743. [Google Scholar] [CrossRef]
- Sekulic, M.; Amin, K.; Mettler, T.; Miller, L. K.; Mallery, S.; Stewart, J. Pancreatic Involvement by Metastasizing Neoplasms as Determined by Endoscopic Ultrasound-guided Fine Needle Aspiration: A Clinicopathologic Characterization. Diagn Cytopathol 2017, 45(5), 418–425. [Google Scholar] [CrossRef]
- Raymond, S. L. T.; Yugawa, D.; Chang, K. H. F.; Ena, B.; Tauchi-Nishi, P. S. Metastatic Neoplasms to the Pancreas Diagnosed by Fine-needle Aspiration/Biopsy Cytology: A 15-year Retrospective Analysis. Diagn Cytopathol 2017, 45(9), 771–783. [Google Scholar] [CrossRef]
- Hou, Y.; Shen, R.; Tonkovich, D.; Li, Z. Endoscopic Ultrasound-Guided Fine-Needle Aspiration Diagnosis of Secondary Tumors Involving Pancreas: An Institution’s Experience. J Am Soc Cytopathol 2018, 7(5), 261–267. [Google Scholar] [CrossRef]
- Atiq, M.; Bhutani, M. S.; Ross, W. A.; Raju, G. S.; Gong, Y.; Tamm, E. P.; Javle, M.; Wang, X.; Lee, J. H. Role of Endoscopic Ultrasonography in Evaluation of Metastatic Lesions to the Pancreas. Pancreas 2013, 42(3), 516–523. [Google Scholar] [CrossRef]
- Hijioka, S.; Matsuo, K.; Mizuno, N.; Hara, K.; Mekky, M. A.; Vikram, B.; Hosoda, W.; Yatabe, Y.; Shimizu, Y.; Kondo, S.; Tajika, M.; Niwa, Y.; Tamada, K.; Yamao, K. Role of Endoscopic Ultrasound and Endoscopic Ultrasound-Guided Fine-Needle Aspiration in Diagnosing Metastasis to the Pancreas: A Tertiary Center Experience. Pancreatology 2011, 11(4), 390–398. [Google Scholar] [CrossRef]
- Pan, B.; Lee, Y.; Rodriguez, T.; Lee, J.; Saif, M. W. Secondary Tumors of the Pancreas: A Case Series. Anticancer Res 2012, 32(4), 1449–1452. [Google Scholar]
- Abdallah, M. A.; Bohy, K.; Singal, A.; Xie, C.; Patel, B.; Nelson, M. E.; Bleeker, J.; Askeland, R.; Abdullah, A.; Aloreidi, K.; Atiq, M. Metastatic Tumors to the Pancreas: Balancing Clinical Impression with Cytology Findings. Ann Hepatobiliary Pancreat Surg 2022, 26(1), 91–97. [Google Scholar] [CrossRef] [PubMed]
- Cui, M.; Amed, M.; Reid, M. D.; Xue, Y. Secondary Pancreatic Tumors in Endoscopic Ultrasound-Guided Fine-Needle Biopsy: Clinicopathologic Characteristics and Morphological Diagnostic Challenges. Hum Pathol 2025, 161, 105869. [Google Scholar] [CrossRef] [PubMed]
- Béchade, D.; Palazzo, L.; Fabre, M.; Algayres, J.-P. EUS-Guided FNA of Pancreatic Metastasis from Renal Cell Carcinoma. Gastrointest Endosc 2003, 58(5), 784–788. [Google Scholar] [CrossRef]
- Ioakim, K. J.; Sydney, G. I.; Michaelides, C.; Sepsa, A.; Psarras, K.; Tsiotos, G. G.; Salla, C.; Nikas, I. P. Evaluation of Metastases to the Pancreas with Fine Needle Aspiration: A Case Series from a Single Centre with Review of the Literature. Cytopathology 2020, 31(2), 96–105. [Google Scholar] [CrossRef]
- Fusaroli, P.; D’Ercole, M. C.; De Giorgio, R.; Serrani, M.; Caletti, G. Contrast Harmonic Endoscopic Ultrasonography in the Characterization of Pancreatic Metastases (With Video). Pancreas 2014, 43(4), 584–587. [Google Scholar] [CrossRef]
- Alomari, A. K.; Ustun, B.; Aslanian, H. R.; Ge, X.; Chhieng, D.; Cai, G. Endoscopic Ultrasound-Guided Fine-Needle Aspiration Diagnosis of Secondary Tumors Involving the Pancreas: An Institution’s Experience. Cytojournal 2016, 13, 1. [Google Scholar] [CrossRef]
- Ardengh, J. C.; Lopes, C. V.; Kemp, R.; Venco, F.; de Lima-Filho, E. R.; dos Santos, J. S. Accuracy of Endoscopic Ultrasound-Guided Fine-Needle Aspiration in the Suspicion of Pancreatic Metastases. BMC Gastroenterol 2013, 13(1), 63. [Google Scholar] [CrossRef] [PubMed]
- Layfield, L. J.; Hirschowitz, S. L.; Adler, D. G. Metastatic Disease to the Pancreas Documented by Endoscopic Ultrasound Guided Fine-needle Aspiration: A Seven-year Experience. Diagn Cytopathol 2012, 40(3), 228–233. [Google Scholar] [CrossRef]
- Sellner, F.; Thalhammer, S.; Klimpfinger, M. Tumour Evolution and Seed and Soil Mechanism in Pancreatic Metastases of Renal Cell Carcinoma. Cancers (Basel) 2021, 13(6), 1342. [Google Scholar] [CrossRef] [PubMed]
- Sperti, C.; Pozza, G.; Brazzale, A. R.; Buratin, A.; Moletta, L.; Beltrame, V.; Valmasoni, M. Metastatic Tumors to the Pancreas: A Systematic Review and Meta-Analysis. Minerva Chir 2016, 71(5), 337–344. [Google Scholar] [PubMed]
- van Riet, P. A.; Erler, N. S.; Bruno, M. J.; Cahen, D. L. Comparison of Fine-Needle Aspiration and Fine-Needle Biopsy Devices for Endoscopic Ultrasound-Guided Sampling of Solid Lesions: A Systemic Review and Meta-Analysis. Endoscopy 2021, 53(04), 411–423. [Google Scholar] [CrossRef]
- Kandel, P.; Nassar, A.; Gomez, V.; Raimondo, M.; Woodward, T. A.; Crook, J. E.; Fares, N. S.; Wallace, M. B. Comparison of Endoscopic Ultrasound-Guided Fine-Needle Biopsy versus Fine-Needle Aspiration for Genomic Profiling and DNA Yield in Pancreatic Cancer: A Randomized Crossover Trial. Endoscopy 2021, 53(04), 376–382. [Google Scholar] [CrossRef]
- Otsuka, Y.; Kamata, K.; Kudo, M. Contrast-Enhanced Harmonic Endoscopic Ultrasound-Guided Puncture for the Patients with Pancreatic Masses. Diagnostics 2023, 13(6), 1039. [Google Scholar] [CrossRef] [PubMed]
- Itonaga, M.; Kitano, M.; Kojima, F.; Hatamaru, K.; Yamashita, Y.; Tamura, T.; Nuta, J.; Kawaji, Y.; Shimokawa, T.; Tanioka, K.; Murata, S. The Usefulness of EUS-FNA with Contrast-enhanced Harmonic Imaging of Solid Pancreatic Lesions: A Prospective Study. J Gastroenterol Hepatol 2020, 35(12), 2273–2280. [Google Scholar] [CrossRef] [PubMed]
- Tacelli, M.; Lauri, G.; Tabacelia, D.; Tieranu, C.G.; Arcidiacono, P.G.; Săftoiu, A. Integrating artificial intelligence with endoscopic ultrasound in the early detection of bilio-pancreatic lesions: Current advances and future prospects. Best Pract Res Clin Gastroenterol. 2025 Feb;74:101975. [CrossRef]
- Kuwahara, T.; Hara, K.; Mizuno, N.; Haba, S.; Okuno, N.; Kuraishi, Y.; Fumihara, D.; Yanaidani, T.; Ishikawa, S.; Yasuda, T.; et al. Artificial intelligence using deep learning analysis of endoscopic ultrasonography images for the differential diagnosis of pancreatic masses. Endoscopy. 2023 Feb;55(2):140-149. [CrossRef]
Figure 1.
Endoscopic ultrasound features of pancreatic metastases. A-B: From renal cell carcinoma (solid, round, well-defined hypoechoic lesions). C: From hepatocellular carcinoma (bilocular hypoechoic lesion). D: From Lymphoma (nodular, hypo-isoechoic lesion with a relatively well-defined boundary).
Figure 1.
Endoscopic ultrasound features of pancreatic metastases. A-B: From renal cell carcinoma (solid, round, well-defined hypoechoic lesions). C: From hepatocellular carcinoma (bilocular hypoechoic lesion). D: From Lymphoma (nodular, hypo-isoechoic lesion with a relatively well-defined boundary).
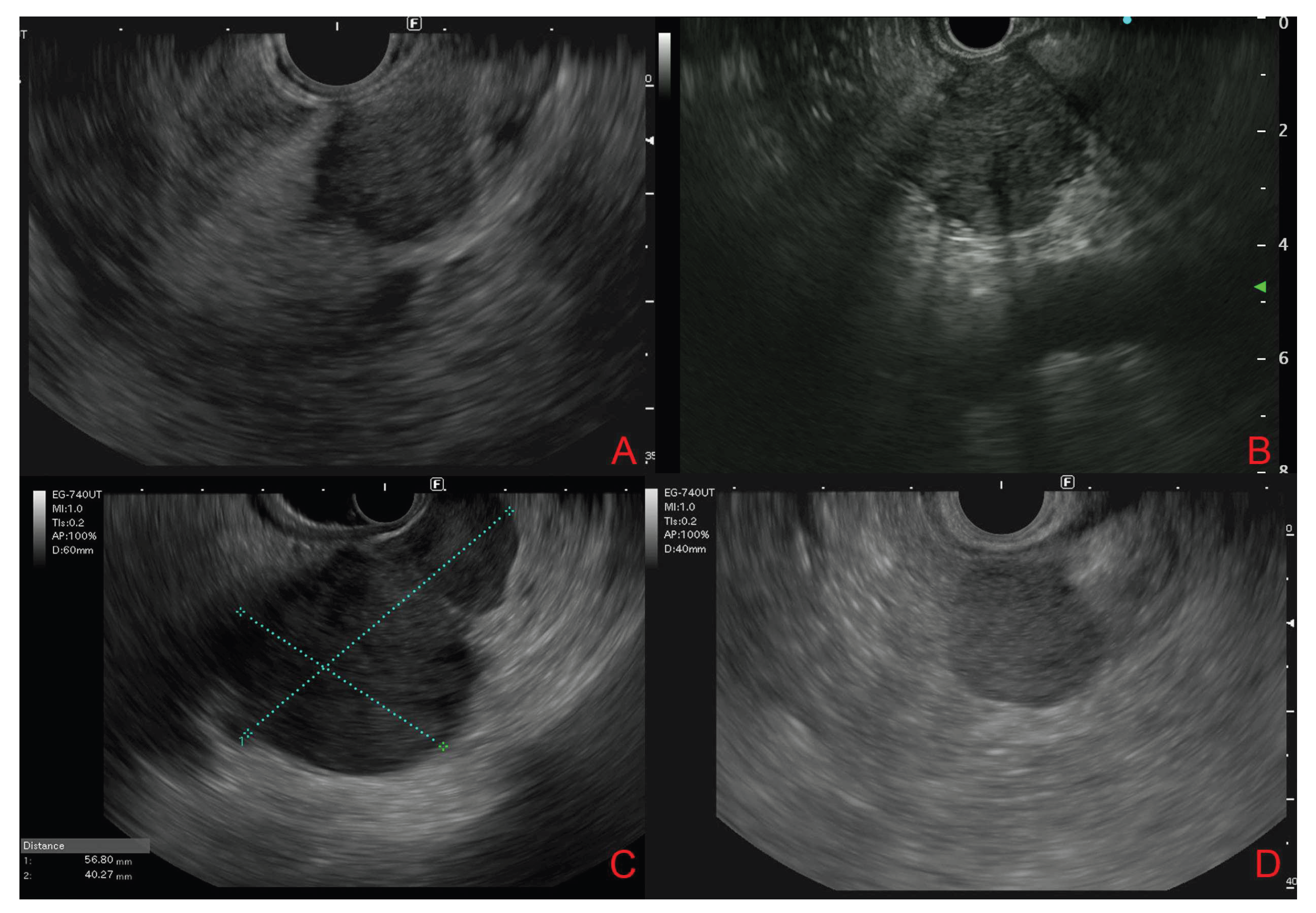
Figure 2.
Contrast-enhanced endoscopic ultrasound behavior of solid pancreatic lesions. A-B: Adenocarcinoma (hypoechoic lesion with ipo-enhancement). C-D: Neuroendocrine tumor (hyper-enhancement in arterial phase). E-F: Pancreatic metastasis from renal cell carcinoma (arterial hyperenhancement with heterogeneous distribution).
Figure 2.
Contrast-enhanced endoscopic ultrasound behavior of solid pancreatic lesions. A-B: Adenocarcinoma (hypoechoic lesion with ipo-enhancement). C-D: Neuroendocrine tumor (hyper-enhancement in arterial phase). E-F: Pancreatic metastasis from renal cell carcinoma (arterial hyperenhancement with heterogeneous distribution).
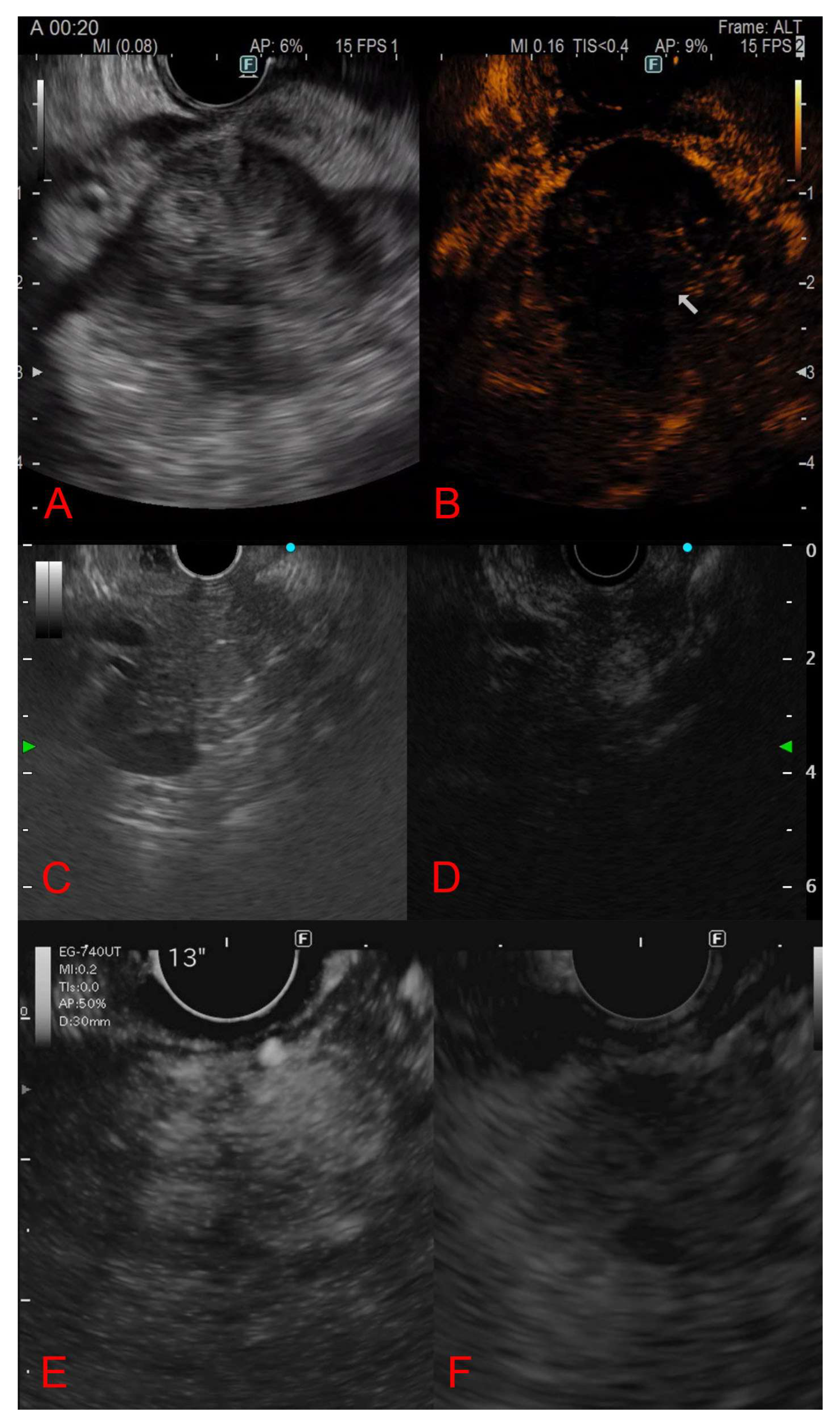

Table 1.
Characteristics and demographics of the included studies.
| Reference | Study design | Country | Study type | Enrollment period | Patients, n | Mean age (range), years | Sex male, % |
|---|---|---|---|---|---|---|---|
| Palazzo et al. [10] | Retrospective | France | Monocentric | 1989-1993 | 7 | 57 (38-77) | 42.9% |
| Fritscher-Ravens et al. [4] | Retrospective | Germany | Monocentric | - | 12 | 61 (34-78) | 33.3% |
| Bechade et al. [35] | Retrospective | France | Monocentric | 1999-2002 | 11 | 65.5 (56-82) | 72.7% |
| Mesa et al. [5] | Retrospective | USA | Monocentric | 2000-2002 | 11 | - | - |
| Moussa et al.[22] | Retrospective | France | Multicentric |
1990-2000 | 22 | 61 (35-76) | 45.5% |
| DeWitt et al.[12] | Retrospective | USA | Multicentric | 1998-2004 | 24 | 60 (33-83) | 62.5% |
| Layfield et al. [40] | Retrospective | USA | Multicentric | 2002-2010 | 17 | 60.9 (15-80) | 88.2% |
| Hijoka et al. [31] | Retrospective | Japan | Monocentric | 1997-2010 | 28 | 59.8 (20-72) | 46.4% |
| Pan et al. [32] | Retrospective | USA | Monocentric | 2010-2012 | 6 | 66.5 (59-73) | 83.3% |
| Ardengh et al. [39] | Retrospective | Brazil | Multicentric | 1997-2010 | 37 | 60.3 (26–84) | 70.3% |
| El Hajj et al. [25] | Retrospective | USA | Monocentric | 1998-2010 | 49 | 63 (30-83) | 46.9% |
| Atiq et al. [30] | Retrospective | USA | Monocentric | 2005-2009 | 23 | 63 | 43.5% |
| Fusaroli et al.[37] | Retrospective | Italy | Monocentric | 2008-2011 | 11 | 66 (42- 82) | 27.3% |
| Waters et al. [26] | Retrospective | USA | Multicentric | 2002-2012 | 66 | 63 (40-89) | 57.6% |
| Smith et al. [13] | Retrospective | USA | Monocentric | 2000-2014 | 22 | 71 (59-83) | 59.1% |
| Alomari et al. [38] | Retrospective | USA | Monocentric | 2005-2012 | 31 | 66 (49-86) | 61.3% |
| Raymond et al. [28] | Retrospective | USA | Monocentric | 2000-2014 | 16 | (43-84) | 68.8% |
| Sekulic et al. [27] | Retrospective | USA | Monocentric | 2006-2016 | 25 | 64 (53-71) (median, IQR) | 52% |
| Hou et al. [29] | Retrospective | USA | Monocentric | 2008-2016 | 30 | 61.2 (25-82) | 60% |
| Betes et al. [14] | Retrospective | Spain | Monocentric | 2004-2016 | 44 | 58 ± 11.7 | 63.6% |
| Ioakim et al. [36] | Retrospective | Greece | Monocentric | 2013-2018 | 7 | 66.9 (56-76) | 71.4% |
| Abdallah et al. [33] | Retrospective | USA | Monocentric | 2011-2017 | 8 | 68.38 ± 10.56 | 50% |
| Teodorescu et al. [20] | Retrospective | Romania | Monocentric | 2012-2020 | 20 | 62 (56–66)(median, IQR) | 50% |
| Spadaccini et al. [16] | Retrospective | Italy | Multicentric | 2010-2021 | 116 | 66.7 (26-86) | 59.5% |
| Aversano et al. [15] | Retrospective | Italy | Monocentric | 2013-2023 | 41 | 71.53 (30-85) | 61% |
| Cui et al. [34] | Retrospective | USA | Multicentric | 2015-2023 | 62 | 66 (42-87) | 46.8% |
Table 2.
Clinicopathological and endoscopic ultrasound features of the included studies.
| Reference | Lesions, n | Primaries (Kidney/Lung/Colon/Breast/ other) |
Mean lesion size (range), mm |
Location (head (uncinate, neck)/body/ tail/multiple) |
Focality (monofocal/multifocal) |
EUS morphology | CH-EUS pattern | Final diagnosis |
|---|---|---|---|---|---|---|---|---|
| Palazzo et al. [10] | 16 | 4/0/0/0/3 | 40 (15-60) | 5/0/1/0 | 6/1 | Isoechoic moderately hypoechoic, homogeneous, rounded and well delineated and associated with peripheral intensification or no attenuation. Hypervascular. |
- | Pre-FNA era, focus on morphology (6 surgery, 1 CT biopsy) |
| Fritscher-Ravens et al. [4] | 12 | 3/1/1/2/4 | 28 (18-40) |
10/2/0/0 | - | Hypoechoic (2); Hypoechoic and inhomogeneus (10) |
- | EUS-FNA |
| Bechade et al. [35] | 29 | 11/0/0/0/0 | - | 5/1/0/5 | 5/6 | Rounded, solid, well-defined, homogeneous, hypoechoic, or isoechoic lesions, with peripheral enhancement of the US beam |
- | EUS-FNA (9/11) |
| Mesa et al. [5] | 11 | 1/4/1/2/3 | - | 6/3/1/1 | - | - | - | |
| Moussa et al.[22] | 31 | 10/4/4/2/2 | - | - | 14/3 | Hypoechogenic (9), well-limited borders (6), posterior enhancement (3), hyperechogenic aspect (1), homogeneous aspect (1) |
- | EUS-FNA (N = 6), CT-guided biopsy (N = 2), ultrasound-guided biopsy (N = 3), duodenoscopy (N = 3) |
| DeWitt et al.[12] | 29 | 10/4/2/0/8 | 36,13 (16-70) |
15/5/3/1 | 22/2 | Borders: poorly defined in 13 (54%); well defined in 11 (46%). Hypoechoic 20 (83%); 1 metastatic RCC hyperechoic; 1 anechoic; 2 mixed hypoechoic/ anechoic 2 lesions. |
- | EUS-FNA |
| Layfield et al. [40] | 17 | 8/2/0/0/9 | - | 6/4/0/4 | - | - | - | EUS-FNA |
| Hijoka et al. [31] | 38 | 7/6/1/2/12 | 34.4 (13-90) | 9/13/3/3 | 23/5 | Regular borders in 18 (64.2%), clear boundary in 26 (92.8%), homogeneous internal echoic pattern in 14 (50.0%). Cystic components in 8 (28.5%), MHZ in 10 (35.7%); calcifications in 3 (10.7%). Distal MPD dilation in 10 (35.7%), distal parenchymal atrophy in 3 (10.7%). |
-- | 22 (78,5%) EUS-FNA; 12 (42.8%) surgical resection |
| Pan et al. [32] | 6 | 2/2/1/1/0 | - | 1/3/1/1 | 5/1 | - | - | - |
| Ardengh et al. [39] | 37 | 5/6/4/3/17 | 42 (12-127) | 22/9/4/0/2 | 34/3 | Hypoechoic (34), with well- defined borders (23) and heterogeneous (22) |
- | EUS-FNA (Final diagnosis in 94% of cases) |
| El Hajj et al. [25] | 72 | 21/8/4/3/13 | 34 (4-80) |
34/8/7/0 | 38/11 | Hypoechoic 39 (80%); mixed hypoechoic/anechoic 7 (14%), hyperechoic 2 (4%); anechoic in 1 (2%). Regular borders in 27 (55%), irregular in 22 (45%). |
- | EUS-FNA |
| Atiq et al. [30] | 23 | 4/4/4/0/11 | 39.1 (16-90) | 10/8/4/1 |
18/5 | Solitary pancreatic lesion in 18 (78.3%). Hypoechoic in 16 (69.6%), anechoic in 2 (8.7%), mixed echogenicity in 5 (21.7%). |
- | 21 EUS-FNA; 1 CT FNA; 1 clinical course |
| Fusaroli et al.[37] | 11 | 3/0/2/2/4 | 29.7 (10-50) |
2/8/0/0/1 | 11/0 | Hypoechoic with homogeneous in echotexture (10). Regular margins (9). Irregular margins in breast cancer metastasis. |
Hypoenhancing with heterogeneous pattern 4; Hypoenhancing with homogeneous pattern 2; Hyperenhancing with homogeneous pattern 4 (RCC); Isoenhancing with heterogeneous pattern 1. |
EUS-FNA and surgical |
| Waters et al. [26] | 66 | 27/9/5/6/19 | - |
30/15/17/1 | 65/1 | - | - | All EUS-FNA |
| Smith et al. [13] | 22 | 14/1/2/0/5 | 37 (15-65) | - | 16/6 | - | - | All EUS-FNA |
| Alomari et al. [38] | 31 | 8/7/2/2/12 | 43 (11- 100) |
13/3/2/13 | 17/14 | - | - | EUS -FNA (Final diagnoses in 94% of cases) |
| Raymond et al. [28] | 16 | 3/6/2/0/5 | 42 (12- 109) | 7/5/4/0 | 15/1 | - | - | EUS FNA 8; CT FNA 3; CT CNB 5; |
| Sekulic et al. [27] | 25 | 10/2/4/1/8 | 15 (9.5- 26) (median, IQR) | 17/11/9/7 | 18/7 | Hypoechoic, heterogeneous, and with variably defined borders |
- | EUS-FNA |
| Hou et al. [29] | 30 | 11/5/2/2/10 | - | 12/7/8/2 | - | - | - | EUS-FNA (93.3% accuracy) |
| Betes et al. [14] | 44 | 12/10/5/1/16 | 28.63 ± 19.4 | 22/8/7/7 | 34/10 | - | - | EUS-FNA |
| Ioakim et al. [36] | 10 | 3/1/1/0/2 | - | - | - | All lesions, except one that showed a mixed solid and cystic morphology, appeared solid. |
- | EUS-FNA |
| Abdallah et al. [33] | 12 | 5/1/0/1/1 | 31.88 ± 25.85 | 3/2/2/0 | 6/2 | - | - | EUS-FNA |
| Teodorescu et al. [20] | 20 | 6/5/3/1/5 |
30 (22–36) (median, IQR) |
12/2/6/0 | 14/6 | Hypoechoic and hypervascularized in 11 (55%) |
Arterial hyperenhancement in 11 (55%); hypoenhancement in 9 |
EUS-FNA |
| Spadaccini et al. [16] | 205 | 75/7/9/7/18 | 25.4 ± 15.2 | 137/50/49/0 | 59/57 | Hypoechoic (95), hypervascular (60), with a heterogeneous pattern (54), well-defined borders (52) |
- | 82 EUS-FNB; 12 EUS-FNA; 15 surgery. |
| Aversano et al. [15] | 41 | 18/4/4/2/13 | 30 (IQR 27) | 17/7/5/12 | 26/15 | Hypoechoic (97.56%), oval-shaped (54.66%), well-defined borders (60.98%), predominantly hypervascular. |
- | 35 EUS-FNA/B; 2 surgery; 3 clinical history and appearances |
| Cui et al. [34] | 62 | 11/9/2/3/37 | 34 (6-130) | 26/13/13/10 | 46/16 | - | - | EUS-FNB |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



