Submitted:
30 November 2025
Posted:
01 December 2025
You are already at the latest version
Abstract
Background: Type B aortic dissection management relies on risk stratification, yet evidence-based tool adoption remains inconsistent in NHS. Bridging the gap between Emergency Medicine and Vascular Surgery remains essential for timely diagnosis, optimal risk stratification, and appropriate intervention to improved outcomes and reduced mortality.
Methods: A cross-sectional survey of EM consultants yielded n=173 valid responses from n=33 units across UK. Subgroup analyses was conducted using a Chi-square test (p < 0.05) alongside descriptive analysis. A pooled prevalence analysis of the literature, utilizing a random-effects model at a 95% confidence interval (CI), served as a benchmark for perception analysis. Agreement was evaluated using Bland-Altman analysis, incorporating upper, lower, and overall bias of agreeability.
Results: Access to rapid CTA was 70% (95% CI: 63.3%–76.8%, p < 0.001), while 32% had SOPs for TBAD (95% CI: 25.3%–39.1%), and 26% were aware of any decision tool (95% CI: 20.6%–33.6%). Labetalol as a first-line antihypertensive was more common amongst least experience (p < 0.05). TBAD diagnosis increased 1.6-fold with every 4 years of additional experience (p < 0.05). Perception analysis showed strong agreement for pain (characteristics and location), hypertension, gender, and age with moderate-to-low agreement for other factors with reported bias of bias of 23.58% (-38.20% to 85.36%) (p = 0.02).
Results: The survey suggests a degree of misperception and inconsistency in recognition of most and least prevalence factors for TBAD suspicion and management. This outcome advocates targeted strategies to enhance diagnostic accuracy using tools aligned with NHS resources and QALY frameworks.
Keywords:
cardiovascular disease
; acute aortic syndrome
; aortic dissection
; systematic review
; pooled analysis
; preception analysis
; QALY
; frame work
; awareness
Introduction
Acute aortic dissection (AAD) remains the most common life-threatening condition affecting 3 to 6 per 100000 individuals with incidences exceeding that of ruptured abdominal aortic aneurysms.[1,2] Their presentation continues to pose a significant challenge and chest pain as a constitutional symptom, accounts for millions of visits to the emergency departments (ED). Prompt and accurate diagnosis is essential, as delayed or misdiagnosis occurs in 14-38% of cases, and is associated with 22.7% mortality within the initial 6 hours and 50% at 24 hours. [3,4,5] The International Registry of Acute Aortic Dissection (IRAD) highlighted that approximately 40% of AADs are classified as Type B Aortic Dissection (TBAD).[6] However, the recent collaboration between National Vascular Registry (NVR), Hospital Episode Statistic (HES) and National Institute of Cardiovascular Outcomes Research (NICOR) in England alone stated that amongst n=6994 cases of AAD from 2017 to 2022, 60% were TBAD.[7]
The lack of classical signs and constitutional symptoms in TBAD continues to challenge emergency physicians in their prompt recognition.[8,9] Furthermore, the complex interplay of hemodynamic and anatomical factors, demands a comprehensive and systematic management from their earliest onset to achieve optimal outcome. [10,11,12] The recent report by the UK Healthcare Safety Investigation Branch indicated that AAD impacts approximately 2,500 individuals annually. [13] This report indicated that the low frequency of cases, combined with a lack of robust detection strategies, continues to contribute to mortality and morbidity.
From a surgical perspective, advancements in technology have led to better outcomes, particularly when combined with non-operative management. However, whilst efforts focus on those that are diagnosed and treated, the issue of misdiagnosis or delayed diagnosis has not been evaluated. Given the patient journey begins in the ED, it is essential for Emergency Medicine (EM) consultants to maintain a high index of suspicion to minimize diagnostic delays. [13] Taking aforementioned factors into account, this survey was primarily designed to capture the current perception, knowledge, and awareness of EM Consultants regarding TBAD within the wider NHS. This survey was inclusive of baseline information such as signs, symptoms, diagnostic criteria, management strategies, infrastructure, ongoing care and educational aspects of TBAD. The secondary aim focused on comparison of the current survey results to that of national and international standards, guidelines and policies and, if deemed necessary, recommend refinements to improve prompt diagnosis and raise awareness with an objective methodology.
Methods
Survey Design:
A review of the literature to identify existing scoring, stratification and/or predictive tools that provide insight to relevant data pertaining to signs, symptoms, clinical findings and risk factors was conducted. This was an electronic & systematic search in Medline on predictive and/or risk stratification tools for the diagnosis of Type-B Aortic Dissection (TBAD). The review was focused on those articles that included demographics, signs, symptoms, clinical findings, risk factors and primary biomarkers for their predictive or risk stratification methodology. The search was limited to English language and adults only. (Supplementary data) Data extraction was conducted by two independent reviewers and subjected to inter-rater reliability agreement (Cohen's kappa coefficient). A value greater than 0.8 indicated good agreement, [14,15]. The search outcome served as the foundation for the clinical section of the survey & point of reference for the perception analysis. This survey was a collaborative effort of Vascular Surgery & Emergency Medicine (Supplementary information). This survey was also evaluated in line with the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) (Supplementary Information).
Survey Details
An electronic consultant-based survey was designed. This survey was forward to the administrator of the individual Schools of Emergency Medicine (EM) within the National Healthcare System (NHS) for dissemination. The survey was voluntary, with no obligation or incentives. None of the participants were aware of the contents of the survey. This survey contained no patient data or alteration of routine practice. The authors contribution list contains those that consented to their name and unit with no attribution to the results. The survey was disseminated electronically to EM consultants only within the NHS. The survey comprised of a total of n=19 questionnaire entailing n=63 data points (supplementary data) over a 9-month period. A total of n=173 consultants across Wales, Scotland and England from n=33 units (n=13 district general, n=11 tertiary and n=9 university hospitals) responded. The outcome was automatically recorded on completion with no missing data. This survey comprised of two distinct sections. The initial part focused on experience of individual EM consultants in their practice, prior involvement, approach and knowledge surrounding their (inclusion and/or exclusion) criterion for diagnosis of TBAD, investigation modalities and access to such. Second section evaluated the initial management strategy, speciality disposition, definitive care plan, awareness of clinical scoring systems, standard of operating procedure (SOP) alongside the need for a national risk stratification tool/s and education in TBAD. The final stage of this article includes perception analysis comparing the survey outcome to that of pooled prevalence analysis to the initial search outcome.
Standards Operating Protocol (SOP) & Guidelines:
- Acute Aortic Syndrome (AAS): This term encompasses aortic dissection, penetrating aortic ulcer (PAU), and intramural hematoma (IMH).[16]
- Type B Aortic Dissection (TBAD) & blood pressure management: TBAD is defined as a dissection occurring in the aorta beyond the left subclavian artery, without involving the ascending aorta. Labetalol is the recommended first line antihypertensive for management of hypertension in TBAD.[16]
Statistical Analysis
Prior to the dissemination of the survey, an initial power calculation identified that n=150 consultant responses would be adequate to achieve 80% power at a 95% confidence interval (95% CI), assuming an effect size sufficient to prevent conclusion bias with an estimated proportion of 0.5. A total of n=173 consultants with no missing data from UK (Wales, Scotland and England) & n=33 units (n=13 district general, n=11 tertiary and n=9 university hospitals) responded to this survey. This study employed a cross-sectional survey design to evaluate the experiences, practices, and perceptions of EM consultants in the diagnosis & management of TBAD. The initial data output was subjected to descriptive analysis. This included percentage and count for binary data and complemented by 95% CI for polynomial. Inferential analysis was conducted using the binomial test, an exact test for assessing the statistical significance of deviations from a theoretical expected distribution of binary outcomes, as defined by acknowledged and practiced criteria. This was applicable to: the use of Labetalol (beta-blocker) as a first-line antihypertensive, the presence of Standard Operating Procedures (SOPs), access to rapid CTA and reporting, awareness of decision tools, and the inclusion of TBAD in local educational programs as per guidelines and definitions.[15,16,17,18]
Subgroup Analysis: Initial analysis was complemented by subgroup analysis based on the experience of consultants per year, categorized into three groups: Group-1 (0-4 years), Group-2 (5-10 years), and Group-3 (>10 years), as per questionnaire. The Chi-square test was utilized to assess whether consultants with varying levels of experience responded differently to specific aspects of the survey by comparing observed and expected frequencies within a 95% confidence interval (CI). A probability value (p-value) of less than 0.05 was considered statistically significant.[20]
Pooled and Perception analysis: The extracted data from the primary review of literature on all endpoint of the survey was subjected to a pooled prevalence analysis using a random-effects model at a 95% confidence interval (CI).[21] This analysis served as a benchmark to evaluate respondents' estimated perceptions in the survey. Perception analysis utilized Bland-Altman methodology to evaluate the agreement between survey and pooled outcome. This approach involved assessing the differences between the two outcomes and plotting them against their averages. Systematic bias (mean difference) and limits of agreement, calculated as ±1.96 SD of the differences, were determined. The lower confidence limit (LCL) and upper confidence limit (UCL) were identified to provide thresholds within which most differences would fall.[22] The results were presented using a Bland-Altman plot and radar chart to illustrate the levels of agreeability and any disparities.[23,24]
Results
Primary Outcome: Among 173 consultants, 41% had more than 10 years of experience. Majority reported prior involvement in managing TBAD and considering it as a differential for chest pain. The key clinical signs prompting suspicion were pain severity and location, hypertension, neurological manifestations, and pulse deficits. Risk factors considered included connective tissue disorders, prior aortic surgery, and age. Raised D-Dimer was the most common diagnostic trigger (44%), followed by raised lactate and normal Troponin-T. Labetalol was the preferred first-line antihypertensive, followed by GTN. Cardiothoracic surgery was the most common specialty referral, followed by vascular surgery and internal medicine. Management occurred at tertiary centres in 47% of cases. Implementation of a risk stratification was perceived to be useful by majority of the cohort. Overall, majority indicated that TBAD was included in their educational programs (Table 1).
Subgroup outcome: Access to rapid CTA and reporting was noted in 70% of respondents. However, only 32% reported the presence of SOPs for TBAD and only 26% were aware of any decision tools. The use of Labetalol (beta-blocker) as first-line antihypertensive was more common among those with less experience. The diagnosis of TBAD showed a 1.6-fold increase with every additional 4 years of experience in the ED p < 0.05. Furthermore, there was a 1.3-fold increase in the recognition of murmurs as a clinical prompt and a 2.6-fold increase in the likelihood of initiating a CTA based on a normal ECG for every 4-years increment in experience (Table 2).
Pooled Analysis Outcome: The analysis demonstrated that pain and location were identified as the most predominant factors at 76.4% (95% CI: 72.7%–79.8%), followed by hypertension at 68.6% (95% CI: 61.5%–74.9%), raised D-dimer at 61.8% (95% CI: 54.4%–68.7%), and male gender at 66.5% (95% CI: 44.55%–88.45%). The median age was 64.5 years (95% CI: 61–69 years) and all outcomes are detailed in (Table 3).[25,26,27,28,29,30,31,32,33]
Perception Analysis Outcome: Strong agreement was observed in pain & location and hypertension, with minimal differences clustering near the bias line. Moderate agreement was noted in Raised D-Dimer, Connective Tissue Disorder, and Aortic Surgery, where data points remain within the limits of agreement. Pulse Deficit, Focal Neurology, and Murmur showed lower agreement, with differences nearing the limits of agreement and greater inconsistency. There was bias of 23.58%, with limits of agreement from -38.20% (LCL) to 85.36% (UCL). This was statistically significant (p=0.02) (Figure 1 and Figure 2)
Discussions
The survey reported a higher prevalence inclusive of clinical examination for murmur.[34] Additionally, aortic chromosomal abnormalities (e.g., Turner and Noonan syndromes) and hereditary conditions (e.g., Marfan and Ehlers-Danlos syndromes) are observed in younger populations (<40 years) compared to the general population.[35] Furthermore, cocaine use with incidence of 37% as risk factor is more likely to result in TBAD (48%), exceeding the collective impact of the later risk factors.[36]
The survey demonstrated that majority considered TBAD in the differential diagnosis of chest pain, with a higher threshold to proceed to CTA when raised D-Dimer, elevated lactate, or normal Troponin-T were observed. However, 30% (95% CI: 23.2%–36.7%) lacked rapid access to prompt CT imaging and reporting, despite CT being the most accurate diagnostic modality.[37] This is of concern when misdiagnosis was reported by quarter of the respondents in the survey.
Malperfusion syndrome or so called complicated TBAD is caused by end-organ ischemia due to aortic branch involvement that accounts for 20%–31% of all TBAD cases. [38] Its presentation can resemble transient ischemic attacks (TIA) or manifest as acute limb or organ ischemia. [28] While signs such as pulse deficits, focal neurology, murmurs, nausea, and vomiting may suggest malperfusion, these features are uncommon in uncomplicated TBAD. Furthermore, placing equal emphasis on less consistent signs compared to more common indicators may represent an overestimation.
Upon diagnosis, Labetalol was the preferred first-line antihypertensive, although its preference decreased with increasing experience in practice, despite clear guidelines (Group:1 100% vs. Group: 2: 92.6% vs. Group:3: 86.9%) p < 0.05. Among respondents, 19% (95% CI: 13.9%–25.5%) reported using GTN, despite literature recommending its use only after beta-blockers. This is due to the risk of sympathetic stimulation from direct vasodilation, which can lead to increased dP/dT because of catecholamine release.[39] Furthermore, there was notable lack of SOPs in emergency departments for TBAD. EM consultants were more likely to involve cardiothoracic surgeons and acute physicians rather than vascular surgeons (p = 0.01) as the primary point of reference and management.
The perception analysis revealed some overestimation, which also has two positive implications. Firstly, it suggests a strong awareness of the signs and symptoms amongst consultants in ED. Secondly, overestimation is preferable when predicting risk in clinical settings, especially when the stakes are high.[40] Furthermore, increased clinical experience correlated with a higher rate of TBAD diagnosis. The inclusion of normal ECG as a diagnostic aid in this survey (9%), despite its absence from most stratification scores, aligns with recent evidence that normal ECG are observed in 20-30% of TBAD cases.[41]
Overall, the survey suggests inconsistency and varied perception in TBAD stratification and management. This outcome advocates targeted strategies to enhance diagnostic accuracy using tools aligned with NHS resources and QALY frameworks.[42] Unified local and national educational initiatives should prioritize improving awareness, with a secondary goal of establishing standardized operating procedures (SOPs) that comprehensively cover the entire care pathway, from diagnosis to specialty deposition. Achieving this objective demands a realistic and collaborative approach involving all stakeholders. Furthermore, integrating data and coding systems is essential to gain a better understanding of this complex pathology, which continues to present significant challenges to involved specialties.
Limitations:
While this survey provides valuable insights into current practices and gaps in the management of TBAD, it has several limitations that warrant consideration. First, the survey relies on self-reported data, which may introduce recall bias alongside over or underestimation of data points. Variability in access to resources, such as CTA or its rapid reporting, may also reflect institutional differences rather than broader systemic issues within NHS. Furthermore, the survey does not account for regional disparities in training, experience, or access to multidisciplinary teams, which could influence reported practices.
This survey was based on categorical and numerical data points. A larger number would have enhanced the robustness of the study, enabling more reliable statistical inferences. It is important to note that the analysis depends on the accuracy of participant reporting. Additionally, the inclusion of more detailed categories and parameters would have provided a more comprehensive understanding of TBAD diagnosis or management. Finally, the lack of standardized definitions for some clinical parameters and outcomes, such as "misdiagnosis," may lead to inconsistencies in interpretation.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Funding
The authors have not declared any grant or funding for this survey from any funding agency in the public, commercial of non-for-profit sectors.
Acknowledgments of Survery Contributors
A. Alanood, Abdal Butt, Abdelrahman Abbas, Ajantha Kurukulasuriya, Alain vella, Aleinmar Winthein, Alison Macleod, Ammar Salem, Andy Ashton, Andy Webster, Angelo Giubileo, Angharad Spencer, Anna Bayston, Aszad Aya, B.Vivegananthan, Bianca Ebtehadj, Binu George, Brian Chivima, Catherine Botting, Clare Davies, Clare O'Leary, Dalip Kumar, Daniel Stanciu, David Hartin, David Maltby David Prosser, Donna wade, Ed Barnard, Francoise Sheppard, Georgina Robertson, Gyorgyi Kamaras, Heinrich Hollis, Helen Turner, Hunniya Waseem, Husnain Ali, Jamie Cooper, Jason Louis, Jim Crawfurd, John Lankester, Jonathan Scrimshaw, Kate Russ, Kh Gul Zaman Butt, Kirsten Walthall, Kirsty Challen, Lee Helliwell, Manoj Viegas, Martin Hunt, Mehdi Hassan Teeli, Mike Iacovou, Mohit Arora, Muhammad Sajid, Nadine Darlow, Natalie James, Neil Prater, Oliver Meller-Herbert, Polly Haywood, Rajesh Vasiraju, Ravishankar Prabhakar Shashikala, Rehman Raj, Rengarajan Subramanian, Rishi Rallan, Robert Taylor, Roopa Balasundaram, Sanjoy Bhattacharyya, Sarah Higgins, Sebastian Clark, Shanthi Siva, Sukhbir Singh Bhullar, Syed Masud, Tamer Okasha, Tanya Lindsay, Teifion Davies, Thomas Gaskarth, Victor Nwokocha, William Kent, Wojciech K Sawicki, Yusuf Gali, Zahid Rahman.
Competing interest
None Declared.
Patient consent for publication
Not Applicable.
Ethics Approval
Not Applicable.
Provenance and peer review
Not commissioned: externally peer reviewed.
Data Availability
Data are available upon reasonable request. Any data pertaining to this survey may be obtained in de-identified format from the corresponding author, provided reasonable request is made within an acceptable timeframe.
References
- Olsson C, Thelin S, Stahle E, Ekbom A, Granath F. Thoracic aortic aneurysm and dissection: increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14,000 cases from 1987 to 2002. Circulation. Dec 12 2006;114(24):2611-8. [CrossRef]
- Howard DP, Banerjee A, Fairhead JF, et al. Population-Based Study of Incidence, Risk Factors, Outcome, and Prognosis of Ischemic Peripheral Arterial Events: Implications for Prevention. Circulation. Nov 10 2015;132(19):1805-15. [CrossRef]
- Zhan S, Hong S, Shan-Shan L, et al. Misdiagnosis of aortic dissection: experience of 361 patients. J Clin Hypertens (Greenwich). Apr 2012;14(4):256-60. [CrossRef]
- Hansen MS, Nogareda GJ, Hutchison SJ. Frequency of and inappropriate treatment of misdiagnosis of acute aortic dissection. Am J Cardiol. Mar 15 2007;99(6):852-6. [CrossRef]
- Klompas M. Does this patient have an acute thoracic aortic dissection? JAMA. May 1 2002;287(17):2262-72. [CrossRef]
- Nienaber CA, Clough RE. Management of acute aortic dissection. Lancet. Feb 28 2015;385(9970):800-11. [CrossRef]
- Pherwani A. New data highlight rising incidence of aortic dissection in England. VascularNews. Accessed 25/04/2024, https://vascularnews.com/new-data-highlight-rising-incidence-of-aortic-dissection-in-england/#:~:text=New%20data%20highlight%20rising%20incidence%20of%20aortic%20dissection%20in%20England,-25th%20April%202024&text=“The%20incidence%20of%20acute%20aortic,April%2C%20London%2C%20UK).
- Asha SE, Miers JW. A Systematic Review and Meta-analysis of D-dimer as a Rule-out Test for Suspected Acute Aortic Dissection. Ann Emerg Med. Oct 2015;66(4):368-78. [CrossRef]
- Nazerian P, Morello F, Vanni S, et al. Combined use of aortic dissection detection risk score and D-dimer in the diagnostic workup of suspected acute aortic dissection. Int J Cardiol. Jul 15 2014;175(1):78-82. [CrossRef]
- American College of Emergency Physicians Clinical Policies Subcommittee on Thoracic Aortic D, Diercks DB, Promes SB, et al. Clinical policy: critical issues in the evaluation and management of adult patients with suspected acute nontraumatic thoracic aortic dissection. Ann Emerg Med. Jan 2015;65(1):32-42 e12. [CrossRef]
- Erbel R, Aboyans V, Boileau C, et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur Heart J. Nov 1 2014;35(41):2873-926. [CrossRef]
- Nazerian P, Giachino F, Vanni S, et al. Diagnostic performance of the aortic dissection detection risk score in patients with suspected acute aortic dissection. Eur Heart J Acute Cardiovasc Care. Dec 2014;3(4):373-81. [CrossRef]
- Body HSSI. Delayed recognition of acute aortic dissection. https://www.hssib.org.uk/patient-safety-investigations/delayed-recognition-of-acute-aortic-dissection/investigation-report/.
- McHugh ML. Interrater reliability: the kappa statistic. Biochem Med (Zagreb). 2012;22(3):276-82.
- Barendregt JJ, Doi SA, Lee YY, Norman RE, Vos T. Meta-analysis of prevalence. J Epidemiol Community Health. Nov 1 2013;67(11):974-8. [CrossRef]
- Riambau V, Bockler D, Brunkwall J, et al. Editor's Choice - Management of Descending Thoracic Aorta Diseases: Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. Jan 2017;53(1):4-52. [CrossRef]
- Baliga RR, Nienaber CA, Bossone E, et al. The role of imaging in aortic dissection and related syndromes. JACC Cardiovasc Imaging. Apr 2014;7(4):406-24. [CrossRef]
- Mills AM, Raja AS, Marin JR. Optimizing diagnostic imaging in the emergency department. Acad Emerg Med. May 2015;22(5):625-31. [CrossRef]
- Morello F, Santoro M, Fargion AT, Grifoni S, Nazerian P. Diagnosis and management of acute aortic syndromes in the emergency department. Intern Emerg Med. Jan 2021;16(1):171-181. [CrossRef]
- McHugh ML. The chi-square test of independence. Biochem Med (Zagreb). 2013;23(2):143-9. [CrossRef]
- Blettner M, Sauerbrei W, Schlehofer B, Scheuchenpflug T, Friedenreich C. Traditional reviews, meta-analyses and pooled analyses in epidemiology. International Journal of Epidemiology. 1999;28(1):1-9. [CrossRef]
- Giavarina D. Understanding Bland Altman analysis. Biochem Med (Zagreb). 2015;25(2):141-51. [CrossRef]
- Gerke O. Reporting Standards for a Bland-Altman Agreement Analysis: A Review of Methodological Reviews. Diagnostics (Basel). May 22 2020;10(5). [CrossRef]
- Saary MJ. Radar plots: a useful way for presenting multivariate health care data. J Clin Epidemiol. Apr 2008;61(4):311-7. [CrossRef]
- Suzuki T, Mehta RH, Ince H, et al. Clinical profiles and outcomes of acute type B aortic dissection in the current era: lessons from the International Registry of Aortic Dissection (IRAD). Circulation. Sep 9 2003;108 Suppl 1:II312-7. [CrossRef]
- Morello F, Bima P, Pivetta E, et al. Development and Validation of a Simplified Probability Assessment Score Integrated With Age-Adjusted d-Dimer for Diagnosis of Acute Aortic Syndromes. J Am Heart Assoc. Feb 2 2021;10(3):e018425. [CrossRef]
- Nazerian P, Mueller C, Soeiro AM, et al. Diagnostic Accuracy of the Aortic Dissection Detection Risk Score Plus D-Dimer for Acute Aortic Syndromes: The ADvISED Prospective Multicenter Study. Circulation. Jan 16 2018;137(3):250-258. [CrossRef]
- von Kodolitsch Y, Schwartz AG, Nienaber CA. Clinical prediction of acute aortic dissection. Arch Intern Med. Oct 23 2000;160(19):2977-82. [CrossRef]
- Ohle R, McIsaac S, Van Drusen M, et al. Evaluation of the Canadian Clinical Practice Guidelines Risk Prediction Tool for Acute Aortic Syndrome: The RIPP Score. Emerg Med Int. 2023;2023:6636800. [CrossRef]
- McLatchie R, Reed MJ, Freeman N, et al. Diagnosis of Acute Aortic Syndrome in the Emergency Department (DAShED) study: an observational cohort study of people attending the emergency department with symptoms consistent with acute aortic syndrome. Emerg Med J. Feb 20 2024;41(3):136-144. [CrossRef]
- Matsushita A, Tabata M, Mihara W, et al. Risk score system for late aortic events in patients with uncomplicated type B aortic dissection. J Thorac Cardiovasc Surg. Jun 2020;159(6):2173-2183 e1. [CrossRef]
- Rogers AM, Hermann LK, Booher AM, et al. Sensitivity of the aortic dissection detection risk score, a novel guideline-based tool for identification of acute aortic dissection at initial presentation: results from the international registry of acute aortic dissection. Circulation. May 24 2011;123(20):2213-8. [CrossRef]
- Riambau V, Bockler D, Brunkwall J, et al. Editor's Choice - Management of Descending Thoracic Aorta Diseases: Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. Jan 2017;53(1):4-52. [CrossRef]
- Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. Feb 16 2000;283(7):897-903. [CrossRef]
- Larson EW, Edwards WD. Risk factors for aortic dissection: a necropsy study of 161 cases. Am J Cardiol. Mar 1 1984;53(6):849-55. [CrossRef]
- Eagle KA, Isselbacher EM, DeSanctis RW, Investigators tIRfAD. Cocaine-Related Aortic Dissection in Perspective. Circulation. 2002;105(13):1529-1530. doi:. [CrossRef]
- Wicky S, Wintermark M, Schnyder P, Capasso P, Denys A. Imaging of blunt chest trauma. Eur Radiol. 2000;10(10):1524-38. [CrossRef]
- Cambria RP, Brewster DC, Gertler J, et al. Vascular complications associated with spontaneous aortic dissection. J Vasc Surg. Feb 1988;7(2):199-209.
- Durham CA, Cambria RP, Wang LJ, et al. The natural history of medically managed acute type B aortic dissection. J Vasc Surg. May 2015;61(5):1192-8. [CrossRef]
- Myles PS, Cui J. Using the Bland-Altman method to measure agreement with repeated measures. Br J Anaesth. Sep 2007;99(3):309-11. [CrossRef]
- Liu WT, Lin CS, Tsao TP, et al. A Deep-Learning Algorithm-Enhanced System Integrating Electrocardiograms and Chest X-rays for Diagnosing Aortic Dissection. Can J Cardiol. Feb 2022;38(2):160-168. [CrossRef]
- Thokala P, Goodacre S, Cooper G, et al. Decision analytical modelling of strategies for investigating suspected acute aortic syndrome. Emergency Medicine Journal. 2024:emermed-2024-214222. [CrossRef]
Figure 1.
Bland-Altman Plot demonstrating the degree of agreement between the survey and review of literature.
Figure 1.
Bland-Altman Plot demonstrating the degree of agreement between the survey and review of literature.
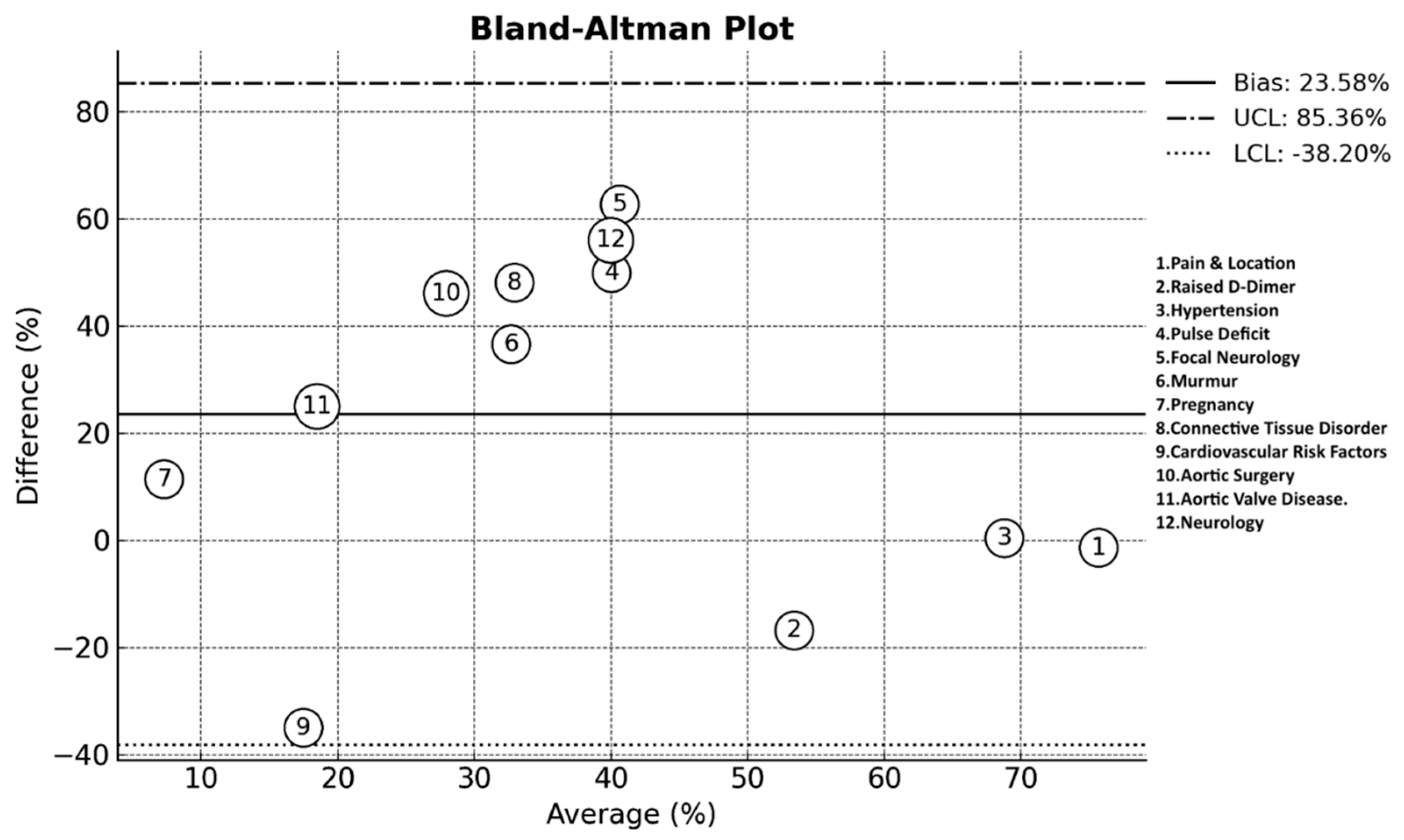
Figure 2.
A Radar Chart illustrating the degree of perception.
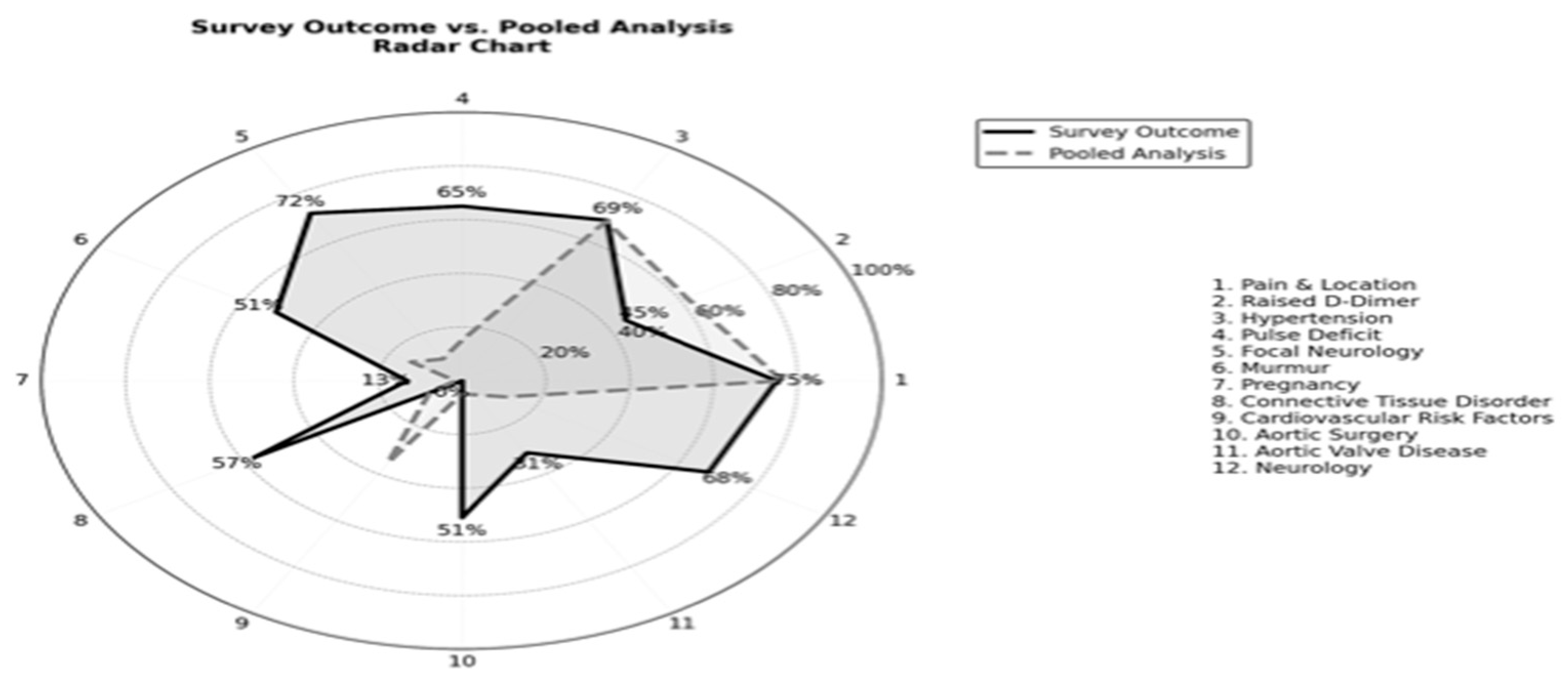

Table 1.
The questionnaire outcome in each respected category. (Non-Binary data presented at 95% Confidence interval).
Table 1.
The questionnaire outcome in each respected category. (Non-Binary data presented at 95% Confidence interval).
| Years Of Experience | Outcome | What Prompts CTA? | Outcome |
| 0-4 | 28% (95% CI: 22.1% - 35.5%) | Normal ECG | 9% (95% CI: 5.4% - 14.5%) |
| 5-10 | 31% (95% CI: 24.8% - 38.5%) | Normal Troponin | 10% (95% CI: 6.2% - 15.8%) |
| >10 | 41% (95% CI: 33.4% - 47.9%) | Raised D-Dimer | 44% (95% CI: 36.9% - 51.6%) |
| Prior Involvement (Yes) | 96% (n=166/173) | Raised Lactate | 25% (95% CI: 19.0% - 31.8%) |
| Prior Diagnosis | None Of the Above | 35% (95% CI: 28.3% - 42.2%) | |
| 0-4 | 49% (95% CI: 41.8% - 56.5%) | All Of the Above | 12% (95% CI: 8.0% - 17.8%) |
| 5-10 | 38% (95% CI: 31.0% - 45.1%) | ||
| >10 | 13% (95% CI: 8.9% - 18.9%) | Rapid CTA & Reporting: (Yes) | 70% (n=122/173) |
| A Differential in Chest Pain? (Yes) | 94% (n=163/173) | First Line Antihypertensive? | |
| Suspecting Symptoms | Labetalol | 88% (95% CI: 82.2% - 91.9%) | |
| Severity and Location of Pain | 75% (95% CI: 67.6% - 80.5%) | GTN | 19% (95% CI: 13.9% - 25.6%) |
| Neurology | 68% (95% CI: 60.3% - 74.2%) | Nitroprusside | 1% (95% CI: 0.3% - 4.1%) |
| Shortness Of Breath | 11% (95% CI: 7.1% - 16.5%) | Hydralazine | 0% (95% CI: 0.0% - 2.2%) |
| Nausea And Vomiting | 6% (95% CI: 3.6% - 11.0%) | I Don’t Start | 2.5% (95% CI: 0.9% - 5.8%) |
| All Of the Above | 25% (95% CI: 19.0% - 31.8%) | Site Management | |
| None Of the Above | 0.5% (95% CI: 0.1% - 2.5%) | Local | 41% (95% CI: 34.0% - 48.5%) |
| Suspecting Clinical Signs | Tertiary Centre | 47% (95% CI: 39.9% - 54.3%) | |
| Hypertension | 69% (95% CI: 61.7% - 75.2%) | Both | 12% (95% CI: 7.8% - 17.7%) |
| Pulse Deficit | 65% (95% CI: 57.7% - 71.6%) | Speciality Management | |
| Focal Neurology | 72% (95% CI: 64.7% - 78.1%) | Internal Medicine | 33% (95% CI: 26.4% - 39.9%) |
| Reduced Air Entry | 0.5% (95% CI: 0.1% - 2.5% | Vascular Surgery | 40% (95% CI: 33.4% - 47.0%) |
| Murmurs | 50% (95% CI: 42.6% - 57.4%) | Cardiothoracic Surgery | 51% (95% CI: 43.6% - 58.2%) |
| All Of the Above | 20% (95% CI: 14.7% - 26.6%) | Decision Tool Awareness? | |
| Risk Factor? | Aortic Dissection Decision Tool | 26% (95% CI: 20.1% - 32.9%) | |
| Age | 48% (95% CI: 40.4% - 55.7%) | ADDR + Age Adjusted D-Dimer | 19% (95% CI: 13.9% - 25.6%) |
| Gender | 30% (95% CI: 23.8% - 37.1%) | ADDR + D-Dimer >500 | 19% (95% CI: 13.9% - 25.6%) |
| Pregnancy | 13% (95% CI: 8.9% - 18.7%) | ADDR + Ascending Aorta > 40 | 1.5% (95% CI: 0.5% - 4.3%) |
| Connective Tissue Disorder | 56% (95% CI: 48.6% - 62.8%) | None Of the Above | 51% (95% CI: 43.6% - 58.2%) |
| Cardiovascular Risk Factors | 0% (95% CI: 0.0% - 2.1%) | All Of the Above | 0.5% (95% CI: 0.1% - 2.5%) |
| Aortic Surgery | 51% (95% CI: 43.6% - 58.2%) | Is Stratification Useful? (Yes) | 85% (n=147/173) |
| Family History of Aortic Valve Disease | 31% (95% CI: 24.6% - 38.3%) | Rate Of Misdiagnosis? | |
| All Of the Above | 39% (95% CI: 31.7% - 46.5%) | 10-29% | 31% (95% CI: 24.6% - 38.3%) |
| In Teaching Programme? (Yes) | 93% (n=161/173) | 30-49% | 39% (95% CI: 31.7% - 46.5%) |
| Is There a SOP (Yes) | 32% (n=55/173) | >50% | 30% (95% CI: 23.5% - 37.3%) |
Table 2.
Comparison of Survey Response per Category per years of experience.
|
Group 1 (0-4 years) |
Group 2 (5-10 years) |
Group 3 (>10 years) |
p-value | |
| How Many Diagnosed (0-4) | 67.35% (95% CI: 54.22% - 80.48%) |
57.41% (95% CI: 44.22% - 70.60%) |
28.99% (95% CI: 18.28% - 39.69%) |
p < 0.001 |
| How Many Diagnosed (5-10) | 26.53% (95% CI: 14.17% - 38.89%) |
33.33% (95% CI: 20.76% - 45.91%) |
50.72% (95% CI: 38.93% - 62.52%) |
p < 0.05 |
| How Many Diagnosed (>10) | 6.12% (95% CI: 0.00% - 12.84%) |
9.26% (95% CI: 1.53% - 16.99%) |
20.29% (95% CI: 10.80% - 29.78%) |
p < 0.05 |
| Murmurs | 48.98% (95% CI: 34.98% - 62.98%) |
37.04% (95% CI: 24.16% - 49.92%) |
65.22% (95% CI: 53.98% - 76.46%) |
p < 0.01 |
| Normal ECG as a Prompt | 4.08% (95% CI: 0.00% - 9.62%) |
1.85% (95% CI: 0.00% - 5.45%) |
17.39% (95% CI: 8.45% - 26.33%) |
p < 0.01 |
|
Rapid CT & Reporting |
59.18% (95% CI: 45.42% - 72.95%) |
64.81% (95% CI: 52.08% - 77.55%) |
82.61% (95% CI: 73.67% - 91.55%) |
p < 0.05 |
| First Line Antihypertensive: Labetalol | 100.00% (95% CI: 100.00% - 100.00%) |
92.59% (95% CI: 85.61% - 99.58%) |
86.96% (95% CI: 79.01% - 94.90%) |
p < 0.05 |
Table 3.
Pooled prevalence analysis at 95% CI.
| ESVS |
Ohle et al. |
Von Kodolitsch et al. |
Lovy et al. |
McLatchie et al. |
Morello et al. |
Rogers et al. |
Nazerian et al. |
Matsushita et al. | Suzuki et al. | Pooled Analysis | |
| Pain & Location | 80% | 81.2% | 79% | 83-89% | 44-86% | - | 72.7-79.3% | - | 44-69% | 86.3-89.2% | 76.4% (95% CI: 72.7% - 79.8%) |
| Neurology | - | - | 20% | - | 8% | 10.2% | - | - | 6% | - | 11.5% (95% CI: 7.6% - 17.0%) |
| Shortness of Breath | - | - | - | - | - | - | - | - | - | - | N/A |
| Nausea/Vomiting | - | - | - | - | - | - | - | - | - | - | N/A |
| Hypertension | - | - | 82% | 82.1% | 31% | 69.4% | - | 55.4% | 73% | 69.1% | 68.6% (95% CI: 61.5% - 74.9%) |
| Pulse deficit | 9% | 5.3% | 38% | - | 1% | 14.3% | 20.3% | 7.9% | - | 21.1% | 15.1% (95% CI: 10.6% - 21.1% |
| Focal neurology | 7% | 10.8% | 13% | - | 5% | 1.41–5.42% | 10.8% | 11.4% | 3% | 4.7% | 9.3% (95% CI: 5.8% - 14.4%) |
| Reduced Air Entry | - | - | - | - | - | - | - | - | - | - | N/A |
| Murmur | - | 4.2% | 28% | - | 0.2% | 2.7% | 23.6% | - | - | - | 14.4% (95% CI: 9.7% - 20.8%) |
| Age | Yes** | 68.5 | 57 | 66 | 55 | 70 | - | 62 | 71 | 64.6 | 64.5 (95%CI: 61- 69 years) |
| Pregnancy | Yes* | - | - | - | 3% | - | - | - | - | 0.2% | 1.6% (95% CI: 1.1% - 4.3%) |
| Connective tissue disorder | 13-22% | 0.2% | - | - | 0.5% | 5% | 4.3% | - | - | 2.9% | 8.9% (95% CI: 5.6% - 14.1%) |
| Cardiovascular risk factors | - | 6% | - | - | - | 42.9% | - | - | 53% | 42% | 35.0% (CI: 10.7% -59.3%) |
| Aortic surgery | - | 0.3% | - | - | 1% | 2% | 2.8% | - | - | 12.3% | 4.9% (95% CI: 2.6% - 9.0%) |
| Aortic Valve Disease | - | 1.5% | - | - | 2% | 14.3% | 11.9% | - | - | - | 6.3% (95% CI: 3.4% - 11.5%) |
| Normal ECG | - | - | - | - | - | - | - | - | - | 31% | N/A |
| Normal Troponin | - | - | - | - | - | - | - | - | - | - | N/A |
| Raised D-Dimer | Yes* | - | - | - | 40% | 18.2–77.8% | Yes* | YES* | 94-97% | Yes* | 61.8% (95% CI: 54.4% - 68.7%) |
| Raised Lactate | Yes* | - | - | - | Yes* | - | - | - | - | - | N/A |
(% Indicates the degree of factor presentation in TBAD - Indicates lack of data. *Highlighted without percentage N/A: meaningful statistical analysis not plausible.). Male: 66.5% (44.55% to 88.45%) Vs. Female: 51.2% (39.1%-62.6%).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



