
Submitted:
26 November 2025
Posted:
27 November 2025
You are already at the latest version
Abstract
Permanently increasing incidence of chronic diseases is challenging for healthcare worldwide being directly associated with physical inactivity considered an important cause of most chronic diseases. In contrast, physical exercise is proven as a powerful instrument of healthcare to protect individuals against health-to-disease transition and against disease progression. Nonetheless, a number of studies warn against inappropriate high-intensity and/or unaccustomed exercise which exceed an individual physical capacity. Indeed, an extensive cardiac output during prolonged exercise leads to significantly increased cardiac dimensions triggering cardiac complications which may result in arrythmogenic sudden cardiac death.
Remarkable plasticity of mitochondria allows these organelles for sensing and adapting to a variety of stressors and responding to stimuli by molecular signalling, regulating bioenergetics and cellular homeostasis decisive for repair machinery, proliferation and apoptosis, tissue regeneration versus degeneration with whole body outcomes. Mitochondria act as biosensors in human body: they are reactive towards stimuli and protective against health-to-disease transition. For performing this life-important function throughout the life, mitochondria need supportive measures including physical activity considered an essential pillar of the mitochondrial medicine. This article highlights reciprocity between the quality of mitochondrial health and homeostasis on one hand and physical fitness and exercise intervention on the other hand. The proposed novelty relates to monitoring of mitochondrial homeostasis strongly recommended for creating individualised training programmes and monitoring exercise efficacy during and after the programme performed. To this end, patient friendly non-invasive approach is already established utilising tear fluid multi-omics, mitochondria as a vital biosensor and AI-based multi-professional data interpretation.
Keywords:
physical fitness
; natural bodybuilding
; mitochondrial rejuvenation
; individualised health protection
; anti-aging & longevity
; recommended training algorithms
1. Introduction
Permanently increasing incidence of chronic diseases is challenging for healthcare worldwide being directly associated with ageing populations, increasing urbanisation and air pollution, imbalanced multi-factorial stress, suboptimal life-style, behavioural and dietary habits on one hand, and on the other hand with early onset of severe pathologies affecting working-age populations, decreased life quality and premature death in affected subpopulations resulting in high demographic and economic burden to the society.
Physical inactivity is detrimental to health status and considered an important cause of most chronic diseases. In contrast, physical exercise is proven as a powerful instrument of primary healthcare to protect healthy individuals and individuals in suboptimal health conditions [1] against health-to-disease transition for at least 35 chronic conditions including but not restricted to accelerated ageing and sarcopenia of multi-factorial nature, fe/male infertility and complications in pregnancy and post-partum, mood, eating and digestive disorders, diverticulitis, obesity, metabolic syndrome and type 2 diabetes mellitus, a spectrum of cardiovascular impairments, inflammatory disorders, chronic pain, stroke, non-alcoholic fatty liver disease, disorders of musculoskeletal system, cognitive decline, neurodegeneration and cancers [2]. Field-dedicated experts emphasise that human body may rapidly maladapt to physical inactivity resulting in significantly decreased both – total and of good quality years of life, whereas physical exercise demonstrates a capacity to either fully prevent or at least to delay clinically manifested chronic disorders.
Nonetheless, a number of studies warn against intense exercises which exceed an individual physical capacity. Indeed, an extensive cardiac output during prolonged exercise leads to significantly increased cardiac dimensions triggering cardiac complications which may result in arrythmogenic sudden cardiac death (SCD) [3]. The phenomenon is mainly described by investigating high performance athletes: emerging data indicate that long-standing vigorous exercise may lead to multi-faceted adverse effects including electrical changes and structural remodelling in otherwise normal hearts [4]. National statistics for SCD incidence in athletes vary between 0,54 and 6,8 per 100.000 athletes [5,6,7,8,9,10]. The SCD incidence 6,8 per 100.000 athletes was recorded by the English Football Association Cardiac Screening Program; mean age 16 years old of healthy adolescent soccer players [10]. Noteworthy, amongst the risks of SCD, specifically the hypertrophic cardiomyopathy was reported as the leading one in athletes aged below 35 years and the second leading one in athletes older than 35 years [4]. Moreover, in marathon runners specifically the hypertrophic cardiomyopathy (HC) was demonstrated not only the leading risk but also a predictor of the SCD [5]. In general, HC is the most common genetic cardiovascular pathology diagnosed in 1 of 500 individuals and equally distributed between men and women; HC is considered the main cause of SCD in patients younger than 35 years old [4]. Although pathophysiology of HC is complex, imbalanced mitochondrial quality control system, shifted mitochondrial homeostasis and disrupted mitochondrion-related autophagy were demonstrated as crucial for the HC manifestation [11]. Moreover, disrupted mitochondrial fusion was demonstrated to cause cellular hypertrophy in cardiomyocytes which is characteristic for the HC pathomechanisms [12,13]. Contextually, impaired mitochondrial dynamics is a crucial risk factor for HC, poor outcomes of inappropriate physical activities and vigorous exercise potentially leading to SCD, and vice versa: exercise-induced mitochondrial damage may cause pathophysiological heart abnormalities, chronic fatigue and muscle degeneration [14].
Remarkable plasticity of mitochondria allows these organelles for sensing and adapting to a variety of stressors and responding to stimuli by molecular (including SOS) signalling, regulating bioenergetics and cellular homeostasis decisive for repair machinery, proliferation and apoptosis, tissue regeneration vs. degeneration with whole body outcomes. Mitochondria act as biosensors in human body: they are reactive towards stimuli and protective against health-to-disease transition. For performing this life-important function throughout the life, mitochondria need supportive measures including physical activity considered an essential pillar of the mitochondrial medicine [15]. As for any medicine, the optimal prescription is critical based on comprehensive diagnostics and treatments tailored to individualised patient profiles and adapted to actual needs of the patient. This article highlights mitochondrial biosensorics and mitochondria-associated protective measures relevant for sport exercise as the stressor on one hand, and on the other hand non-pharmacological treatment approach. The novelty is focused on 3PM approach integrated into individualised training programmes utilising mitochondrial biosensorics check-up for monitoring physical fitness and exercise intervention adapted to personalised needs of the trained individuals.
2. From Eukaryotic “Powerhouse” to the Life-Orchestrating Biosensors in Humans: The Evolution of Mitochondrial Significance Traced by Exercise
About 2 billion years ago as the Earth was becoming more oxygenated, mitochondria (that time a phototrophic alpha-proteobacterium) has been endocytosed by an ancestral eukaryote for utilising this form of life as the synergetic energy-producing organelle [16,17]. This evolutionary step advanced the host by a significantly enhanced energy supply which allowed for extensive developmental capacities resulted in highly organised life-forms later on reflected in the human evolution. Corresponding competencies evolved through comprehensive physical and mental exercise (long-distance walking, running, hunting etc.) followed by dietary shifts towards nutrients-rich food and technological sophistication accompanied by continuous aerobic organ development recoded for the brain, heart, lung and muscles [18]. In the modern medicine, well-acknowledged determinants of human health and longevity are the overall aerobic capacity of the body reflected in fitness of cardiorespiratory system and skeletal muscles [18]. Indeed, mounting evidence demonstrates that physically active individuals are better protected against cardiovascular and metabolic diseases, neurodegeneration and malignancies; further, they live significantly longer compared to physically inactive ones [19,20]. Consequently, running was suggested as an essential pillar of the longevity (defined as high life expectancy) medicine [21]. Protective effects depend on the quality of mitochondrial health and rejuvenation of mitochondrial population [18]. These effects are systemic and adapted to multi-faceted stimuli. In this way, mitochondria sense intrinsic and environmental stressors, govern physiologic stress response, and orchestrate well-balanced cellular homeostasis, namely life and proliferation versus senescence and death of cells. Contextually, mitochondrial biosensorics is instrumental for monitoring and prediction of both – beneficial and detrimental (including SCD) effects to health of individuals undergoing exercise training programmes.
3. Mitochondrial Health and Rejuvenation as the Hub of Physical Fitness and Vice Versa
Physiologic homeostasis and rejuvenation of mitochondrial population is the hallmark of maintaining the physiologic reserve and sustainable physical and mental fitness which is true for any age categories. In contrast, accelerate ageing is associated with functional decline in mitophagy and autophagy linked to compromised mitochondrial turnover and uncontrolled production of ROS by damaged mitochondria followed by systemic inflammageing and mitochondrial “vicious circle”. The latter is characterised by lowering energy production and increasing ROS over-generation leading to unrepairable damage of subcellular structures resistant to physiologic recycling mechanisms and accumulation of cell debris. These processes are extensively described in the literature for brain, heart and muscles of otherwise healthy individuals from the third life-decade onwards as reviewed elsewhere [18].
Physical activity is the unique scientifically proven non-pharmacologic therapeutic approach capable to rejuvenate mitochondrial population and anti-ageing mechanisms in a holistic way. Aerobic exercise stimulates mitochondrial autophagy, recycling and rejuvenation. However, corresponding effects are highly individual depending on the actual nutrient status and exercise duration [18]. To this end, an inappropriate high-intensity and/or unaccustomed exercise may cause health adverse effects resulting in tissue damage, pro-inflammatory activation and pain. Contextually, the type (e.g. aerobic or resistance exercise training), intensity, frequency and duration of the exercise training – all demand individualised prescription and professional coaching.
Resent study investigating impacts of physical activity on physical function, mitochondrial energetics, ROS production and Ca2+ handling across the adult lifespan in men demonstrated [22]:
- Ageing is associated with minimal or even no changes in mitochondrial respiration and content; moreover, physical activity status was positively associated with quantity and quality of mitochondria throughout the human lifespan.
- In the pooled group of participants (all ages together) mitochondrial respiration was positively correlated with muscle strength and physical function;
- Noteworthy, ageing per se is not associated with increasing H2O2 emission; however, physically active participants demonstrated higher levels of H2O2 emission compared with physically inactive participants; although potential explanation is controversial (increased number of mitochondrial or/and increased oxidative stress by exercise), this fact has to be kept in mind, when the type, intensity and duration is prescribed;
- No impact of ageing on the mitochondrial calcium uptake was recorded; nonetheless, higher calcium uptake was observed in physically active participant compared to inactive ones within the age group > 40 years.
4. Mitochondrial Multiomic Response to Endurance Exercise Training Is Highly Tissue-Specific
Although endurance (also called aerobic) exercise training is generally known to increase ATP-generating capacity, volume, size and number of mitochondria in skeletal muscles, detailed multiomics performed utilising animal models demonstrate tissue-specific patterns of mitochondrial response. This specific response is well interpretable in the context of corresponding organ’s functions on one hand, and on the other hand keeping in mind high mitochondrial plasticity and unique ability to adapt to multi-faceted intrinsic and environmental stimuli promptly reacting towards acute tissue-specific metabolic demands [23]. Indeed,
- The minimal mitochondrial multiomic alterations were reported for the brain, small intestine and spleen. To this end, the brain is a mitochondria-rich organ with high levels of energy consumption at rest; although brain activity increases during exercise, the differential metabolic demand is relatively low;
- In contrast, cardiac and skeletal muscles mitochondria demonstrate highly increased ATP production covering significantly enhanced energy demand during contractions. Contextually, the greatest shifts in multiomic patterns were recorded for skeletal muscles, heart but also for liver, colon, adrenal gland, brown and white adipose tissue and blood reflecting adaptive mitochondrial response towards the endurance training and corresponding demands such as stress modulation, improved bioenergetics, blood flow and signalling and metabolic shifts adapting to repeated bouts of exercise.
- Mitochndrial stress response modulation affects sympathetic adrenal-medullary activation, catecholamine and cortisol levels – all considered adaptive for reducing acute stress [24].
- Hepatic mitochondria are critical for oxidising fat for providing ATP and substrates to fuel TCA cycle flux and gluconeogenesis to maintain glucose levels in blood at rest, fasting and under stress conditions. Endurance training leads to improved mitochondrial qualities even independent from their increasing quantity. Per evidence, multiomic changes linked to the exercise demonstrated opposite regulation patterns compared to those induced by the liver cirrhosis [23].
- Brown adipose tissue is rich in mitochondria which are crucial for a physiologic thermogenesis adapted to the cold stress provocation and maintaining physiologic body temperature. Also for this tissue significantly altered multiomic patterns were recorded after endurance training that is well in consensus with energy preservation mechanisms described for professionally trained athletes.
5. Type, Intensity, Frequency, and Duration of the Exercise Training – All Demand Individualised Prescription Tailored to Individualised Patient Profiling
Physical activity benefits health status in general reducing all-cause mortality in the population, mitigating health risks, protecting individuals against health-to-disease transition (primary care) and delaying clinical manifestation and disease progression in secondary care. However, optimising the balance between exercise and recovery is critical to avoid exercise stress-related detrimental effects and to achieve improved individual outcomes.
Physical activity includes any form of movement resulting in contraction of skeletal muscles and systemically enhanced energy consumption. The measures are quantifiable and controllable by the individually adapted intensity, frequency and duration of the exercise [25]. Field-dedicated professionals provide recommendations towards stratified patient groups summarised below.
5.1. Healthy Adults of All Ages
These evidence-based recommendations are considered appropriate also for patients with certain chronic disorders and disabilities coached and advised by responsible professionals [26]. The recommended programme of regular exercise includes cardiorespiratory, resistance, flexibility and neuro-motor exercise training. Main pool of recommendations comprises
- -
- either the moderate intensity cardiorespiratory training for more than 30 minutes daily on at least 5 days a week (totally >150 minutes weekly), vigorous-intensity cardiorespiratory exercise for more than 20 minutes daily on at least 3 days a week (totally >75 minutes weekly),
- -
- or a combination of moderate- and vigorous-intensity training with a total energy expenditure of 500-1000 MET minutes per week;
- -
- On 2-3 days a week, adults should perform resistance exercise for each of the major muscle group as well as neuro-motor training of balance, agility and coordination;
- -
- Further, for maintaining joint rang of movement a series of flexibility exercise for each the major muscle-tendon groups (60 seconds per exercise) on at least 2 days a week is strongly recommended.
Experts conclude that the recommended exercises far overweight potential risks in most adults. Nonetheless, the entire programme has to be adapted to individualised profiling considering habitual physical activity, health status, exercise responses and stated goals. Further, the experts emphasise the necessity of educational component for individuals undergoing the programme and coaching by professionals. Finally, mitochondria-relevant nutraceuticals protecting health in primary and secondary care are strongly recommended by the field-dedicated international expert groups [27]. The expert emphasise that application of nutraceuticals can be beneficial only if meeting needs at individual level. Contextually, health risk assessment based on individualised patient profiles is crucial for adapting nutraceutical sets and improving individual outcomes in primary and secondary care [27].
5.2. Natural Body Building
Muscle loss mitigation may be achieved by resistance training focused on the natural body building technics described earlier [28].
and summarised below.
- Muscle groups in focus should be trained at least two times a week; certainly the muscle volume benefits from a frequent exercise;
- 3-15 repetitions in the 6-12 range (in total 40-70 repetitions for each of the major muscle group per session) should occur to achieve visible effects; for advanced bodybuilder higher numbers of repetitions are appropriate;
- Rest intervals of 1-3 minutes are adequate;
- Chosen tempo should allow for controlling the muscular load;
- Cardiovascular exercise training is recommended to intensify fat loss;
- High-intensity training demands better recovery;
- Fasted cardiovascular training is not recommended, since being not really beneficial and could be even detrimental.
5.3. Exercise Training in the Overall Management of Obesity in Adults
Due to steadily increasing incidence of overweight individuals worldwide linked to sedentary lifestyle, suboptimal dietary habits on one hand, and on the other hand compromised mitochondrial health and accelerated ageing, extensive professional efforts are dedicated to the affected subpopulations. Following recommendations are presented [29]:
- An aerobic exercise at moderate intensity is strongly recommended for loss in body weight, total fat, visceral fat, intra-hepatic fat, and for improvement in blood pressure;
- On average, the expected weight loss is 2 to 3 kg;
- An exercise training program based specifically on resistance training at moderate-to-high intensity is recommended for preservation of lean mass during weight loss;
- For improved cardiorespiratory fitness and insulin sensitivity, any type of exercise training can be applied, namely either aerobic or resistance as well as a combination of both – aerobic and resistance one; after cardiovascular risk assessment also high-intensity interval training can be considered under professional supervision;
- Specifically for the muscular fitness improvement, an exercise training program based preferentially on resistance training alone (or in combination with aerobic training) is recommended;
- Complementary recommendations consider psychological and energetic aspects, appetite control and bariatric surgery as well as life style and behavioural habits in overall management of overweight and obesity.
5.4. Adapted Exercise Training Benefits Children with Attention Deficits Hyperactivity Disorders (ADHD)
A standard medication is well compatible with physical exercise therapy in the treatment of ADHD. To this end, both acute and chronic exercise training demonstrate beneficial effects mitigating symptoms characteristic for the disease, executive function, cognitive and motor abilities in affected children [30]. Systematic long-term training is strongly recommended following the scientific evidence in the field demonstrating beneficial effects accumulating over time. To this end:
- Aerobic exercise training demonstrates a capacity to positively impact neurotransmitter (serotonin and dopamine amongst others) production and to stimulate blood flow in the brain;
- Perceptual motor exercise and meditation stimulate neuroplasticity improving synaptic cross-communication and strengthening the sensory-motor competencies collectively mitigating attention deficits;
The adapted programme demonstrates well documented improved individual outcomes including moderate to high intensity interval training which combines balanced physical exercise with cognitive tasks [30], both rely on improved mitochondrial functionality and reciprocity of beneficial systemic effects. To this end, preclinical studies concluded interval aerobic training remarkably improves bioenergetics state and mitochondrial dynamics of different brain regions [31]. Thereby, main improvements were observed in the frontal and parietal lobes evidently associated with the location of motor and sensory areas. Therefore, the exercise is recommended as a prophylactic approach against compromised bioenergentics and mitochondrial dysfunction.
5.5. Exercise for Patients with Peripheral Neuropathies (PN)
PN is highly prevalent and heterogeneous cohort of patients affected by diseased peripheral nervous system with debilitating symptoms becoming chronic. Medications currently applied are less effective with non-seldom negative side-effects demonstrated in patients with treated polyneuropathy. Based on the accumulated research data, field dedicated international expert groups strongly recommend a combination of endurance exercise and sensorimotor training for the best pronounced health benefits in this patient cohort [32]. Noteworthy, for achieving best individual outcomes, a detailed stratification is essential. For example, specifically for patients diagnosed with the chemotherapy-induced PN the most effective component in the training programme is the sensorimotor exercise. To this end, mitochondria-based holistic 3PM approach has been recommended as the “game-changer” for individualised rehabilitation programmes exemplified by treated breast cancer survivors [33].
5.6. Exercise Recommendations for Individuals Diagnosed with Multiple Sclerosis (MS)
The field-dedicated expert group strongly recommends resistance and aerobic exercise as the most effective training programme to improve the quality of life, balance, walking ability and endurance and to mitigate chronic fatigue in individuals affected by MS [34].
5.7. Exercise Prescription Tailored to the “Long COVID Syndrome” (LCS) Affected Individuals
Statistics collected in the field demonstrate that at least 25-30% of individuals diseased on SARS-CoV-2” may suffer from the LCS diagnosed, when symptoms and signs last over four weeks after initial diagnosis. Chronic fatigue, brain fog, impaired functional capacity with post-exertional malaise, positional tachycardia out of proportion to level of effort, and exercise intolerance are characteristic for the LCS patient cohort [35]. Further, there are evident similarities between LCS and cardiac deconditioning of multi-factorial nature. Contextually, early return to physical activity in a gradual fashion by adapted training programmes is strongly recommended by several international groups of experts, to mitigate detrimental effects of LCS on the brain, cognition, cardiorespiratory competencies and physical inactivity [36,37,38,39,40,41,42,43].
The recommended exercise protocols account for the cardiac deconditioning, by incorporating low-duration and low-intensity exercise early on in the course of training. Further, the type of exercise is critical, since jogging or running, particularly early on, will be difficult to perform, due to exercise intolerance. Consequently, the exercise prescriptions should consider rather semi/recumbent positioning at early stages (week 1-8) followed by walking and jogging (week 9-12) [35]. The recommended exercises range from pulmonary rehabilitation, low and moderate-intensity aerobic exercise and inspiratory muscle training, and resistance training. For example, objective measurements demonstrate improvements in metrics of LCS severity by utilising 6 min of walking distance, upper and lower extremity strength followed by subjective improvements (e.g. decreased fatigue severity). It is critical to emphasize a graded increase in exercise duration and intensity in the individualised rehabilitation programme to avoid post-exertional malaise and potentially limited adherence to the prescribed training.
6. Individualised Check-Up of the Mitochondrial Biosensorics Is Crucial for Physical Fitness and Exercise Intervention Quality – Concluding Remarks
Physical activity is a unique scientifically proven non-pharmacologic therapeutic approach capable to rejuvenate mitochondrial population and anti-ageing mechanisms in a holistic way. Aerobic exercise stimulates mitochondrial autophagy, recycling and rejuvenation. However, corresponding effects are highly individual depending on the actual nutrient status and exercise duration [18]. To this end, an inappropriate high-intensity and/or unaccustomed exercise may cause health adverse effects resulting in tissue damage, pro-inflammatory activation and pain. Contextually, the type (e.g. aerobic or resistance exercise training), intensity, frequency and duration of the exercise training – all demand individualised prescription and professional coaching utilising AI-based multi-parametric health risk assessment followed by creating training programmes tailored to individualised patient profiles. Contextually, mitochondrial biosensorics (stimuli sensing and stress adaptation) linked to biogenesis, dynamics and autophagy (quality control) is decisive for predictive diagnostics and individualised health protection. Targeting mitochondrial quality control is strongly recommended for adaptability to exercise training in healthy populations including particularly stress-sensitive individuals in suboptimal health conditions (such as Flammer Syndrome Phenotype carriers), treating sarcopenia and coaching exercises in anti-ageing, rehabilitation and rejuvenation programmes as well as optimising training programme to the needs of patient groups suffering from the cardiac deconditioning with and without comorbidities [18,33,44,45,46,47,48,49,50,51,52].
Therefore, an application of the digital health monitoring including records of mitochondrial homeostasis is recommended for creating individualised training programmes and monitoring exercise efficacy during and after the programme performed. To this end, patient friendly non-invasive approach is already established utilising tear fluid multi-omics, mitochondria as a vital biosensor and AI-based multi-professional data interpretation [53].
Finally, mitochondria-relevant nutraceuticals protecting health in primary and secondary care are strongly recommended by the field-dedicated international expert groups [27]. The expert emphasise that application of nutraceuticals can be beneficial only if meeting needs at individual level. Contextually, health risk assessment based on individualised patient profiles is crucial for adapting nutraceutical sets and improving individual outcomes in primary and secondary care [27].
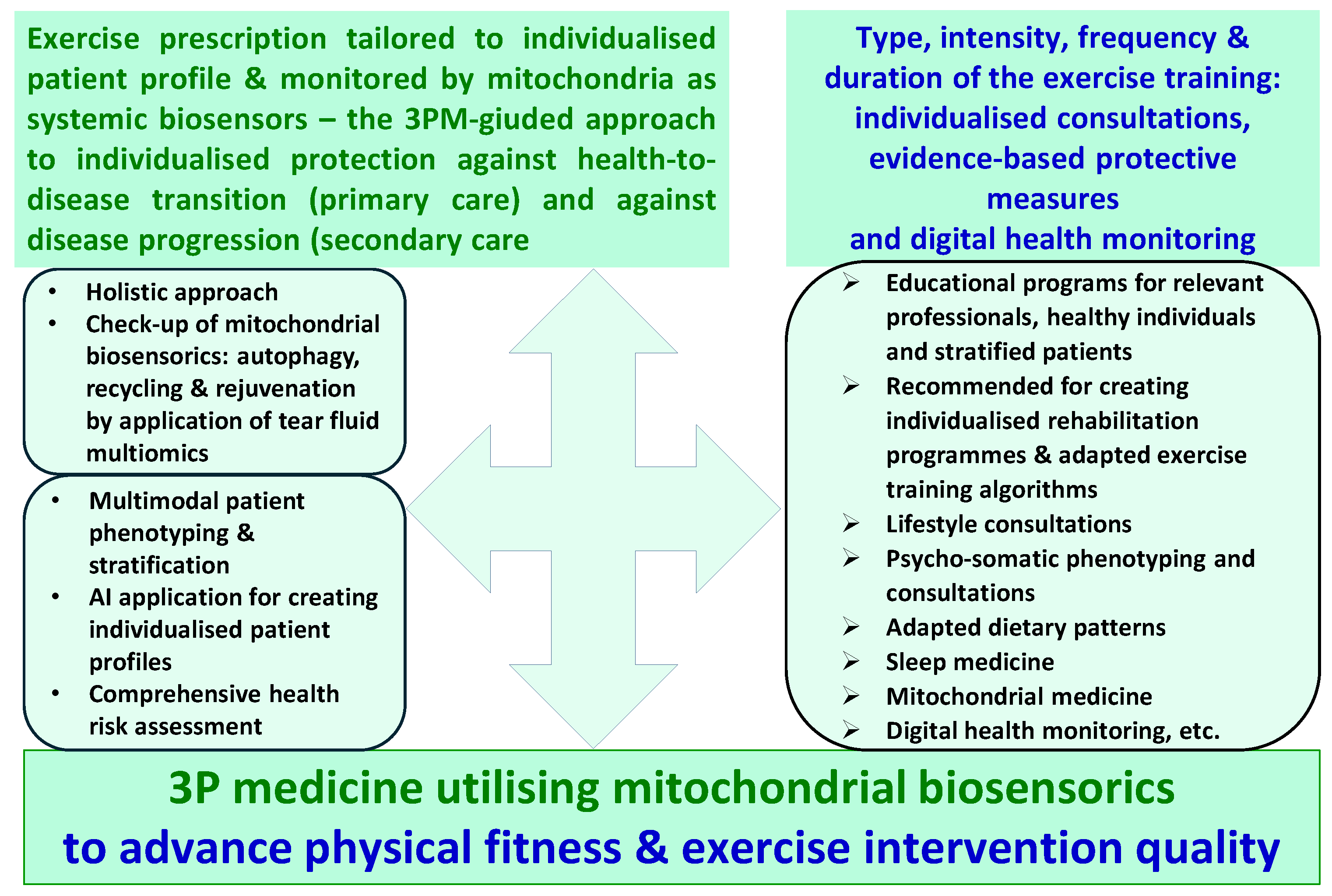
The proposed innovation is summarised by the Figure 1 which includes 3 main pillars, namely
- -
- the goal is to improve physical fitness and to advance exercise intervention quality by the paradigm change from reactive to proactive care implementing concepts of predictive, preventive and personalised (3P) medicine;
- -
- the key instrument is mitochondrial biosensorics as detailed in this article;
- -
- the consequent pathway to achieve the goal is, on a regular basis, to perform mitochondrial biosensorics check-up.
Funding
Not applicable.
Data availability
All the data used in this study are presented in this article.
Consent for publication
Not applicable.
Conflicts of Interest
The author declares no conflict of interest.
Abbreviations
| ADHD | Attention Deficits Hyperactivity Disorders |
| AI | Artificial Intelligence |
| HC | Hypertrophic Cardiomyopathy |
| LCS | Long-COVID Syndrome |
| PN | Peripheral Neuropathies |
| ROS | Reactive Oxygen Species |
| SCD | Sudden Cardiac Death |
References
- Wang W, Yan Y, Guo Z, Hou H, Garcia M, Tan X, Anto EO, Mahara G, Zheng Y, Li B, Kang T, Zhong Z, Wang Y, Guo X, Golubnitschaja O; Suboptimal Health Study Consortium and European Association for Predictive, Preventive and Personalised Medicine. All around suboptimal health - a joint position paper of the Suboptimal Health Study Consortium and European Association for Predictive, Preventive and Personalised Medicine. EPMA J. 2021;12(4):403-433. [CrossRef]
- Booth FW, Roberts CK, Laye MJ. Lack of exercise is a major cause of chronic diseases. Compr Physiol. 2012;2(2):1143-211. [CrossRef]
- Sharma S, Merghani A, Lluis Mont L. Exercise and the heart: the good, the bad, and the ugly. Eur Heart J. 2015;36(23):1445-53. [CrossRef]
- Kochi AN, Vettor G, Dessanai MA, Pizzamiglio F, Tondo C. Sudden Cardiac Death in Athletes: From the Basics to the Practical Work-Up. Medicina (Kaunas). 2021;57(2):168. [CrossRef]
- Kim, J.H.; Malhotra, R.; Chiampas, G.; d’Hemecourt, P.; Troyanos, C.; Cianca, J.; Smith, R.N.; Wang, T.J.; Roberts, W.O. Thompson, P.D.; et al. Cardiac Arrest during Long-Distance Running Races. N. Engl. J. Med. 2012, 366, 130–140;
- Corrado, D.; Basso, C.; Pavei, A.; Michieli, P.; Schiavon, M.T.G. Trends in Sudden Cardiovascular Death in Young Competitive Athletes. JAMA 2006, 296, 1593–1601.
- Maron, B.J.; Gohman, T.E.; Aeppli, D. Prevalence of Sudden Cardiac Death during Competitive Sports Activities in Minnesota High School Athletes. J. Am. Coll. Cardiol. 1998, 32, 1881–1884.
- Steinvil, A.; Chundadze, T.; Zeltser, D.; Rogowski, O.; Halkin, A.; Galily, Y.; Perluk, H.; Viskin, S. Mandatory Electrocardiographic Screening of Athletes to Reduce Their Risk for Sudden Death: Proven Fact or Wishful Thinking? J. Am. Coll. Cardiol. 2011, 57.
- Harmon, K.G.; Asif, I.M.; Maleszewski, J.J.; Owens, D.S.; Prutkin, J.M.; Salerno, J.C.; Zigman, M.L.; Ellenbogen, R.; Rao, A.L.; Ackerman, M.J.; et al. Incidence, Cause, and Comparative Frequency of Sudden Cardiac Death in National Collegiate Athletic Association Athletes a Decade in Review. Circulation 2015, 132, 10–19; 10.
- Malhotra, A.; Dhutia, H.; Finocchiaro, G.; Gati, S.; Beasley, I.; Clift, P.; Cowie, C.; Kenny, A.; Mayet, J.; Oxborough, D.; et al. Outcomes of Cardiac Screening in Adolescent Soccer Players. N. Engl. J. Med. 2018, 379, 524–534.
- Li B, Liu F, Chen X, Chen T, Zhang J, Liu Y, Yao Y, Hu W, Zhang M, Wang B, Liu L, Chen K, Wu Y. FARS2 Deficiency Causes Cardiomyopathy by Disrupting Mitochondrial Homeostasis and the Mitochondrial Quality Control System. Circulation. 2024;149(16):1268-1284. [CrossRef]
- Song M, Franco A, Fleischer JA, Zhang L, Dorn GW 2nd. Abrogating Mitochondrial Dynamics in Mouse Hearts Accelerates Mitochondrial Senescence. Cell Metab. 2017;26(6):872-883.e5. [CrossRef]
- Gustafsson ÅB, Dorn GW 2nd. Evolving and Expanding the Roles of Mitophagy as a Homeostatic and Pathogenic Process. Physiol Rev. 2019;99(1):853-892. [CrossRef]
- Ostojic SM. Exercise-induced mitochondrial dysfunction: a myth or reality? Clin Sci (Lond). 2016 Aug 1;130(16):1407-16. [CrossRef]
- Bishop DJ, Lee MJ, Picard M. Exercise as Mitochondrial Medicine: How Does the Exercise Prescription Affect Mitochondrial Adaptations to Training? Annu Rev Physiol. 2025;87(1):107-129. [CrossRef]
- Kurland CG, Andersson SG. Origin and evolution of the mitochondrial proteome. Microbiol Mol Biol Rev. 2000;64(4):786-820. [CrossRef]
- Holland HD. The oxygenation of the atmosphere and oceans. Philos Trans R Soc Lond B Biol Sci. 2006;361(1470):903-15. [CrossRef]
- Nilsson MI, Tarnopolsky MA. Mitochondria and Aging-The Role of Exercise as a Countermeasure. Biology (Basel). 2019;8(2):40. [CrossRef]
- Kodama S, Saito K, Tanaka S, Maki M, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis JAMA 2009;301(19):2024-35. [CrossRef]
- Reimers CD, Knapp G, Reimers AK. Does physical activity increase life expectancy? A review of the literature. J Aging Res. 2012:2012:243958. [CrossRef]
- Lee DC, Brellenthin AG, Thompson PD, Sui X, Lee IM, Lavie CJ. Running as a Key Lifestyle Medicine for Longevity. Prog Cardiovasc Dis. 2017;60(1):45-55. [CrossRef]
- Cefis M, Marcangeli V, Hammad R, Granet J, Leduc-Gaudet J-P et al. Impact of physical activity on physical function, mitochondrial energetics, ROS production, and Ca2+ handling across the adult lifespan in men Cell Rep Med. 2025;6(2):101968. [CrossRef]
- Amar D, Gay NR, Jimenez-Morales D, Jean Beltran PM, Ramaker ME, Raja AN, Zhao B, Sun Y, Marwaha S, Gaul DA, Hershman SG, Ferrasse A, Xia A, Lanza I, Fernández FM, Montgomery SB, Hevener AL, Ashley EA, Walsh MJ, Sparks LM, Burant CF, Rector RS, Thyfault J, Wheeler MT, Goodpaster BH, Coen PM, Schenk S, Bodine SC, Lindholm ME; MoTrPAC Study Group. The mitochondrial multi-omic response to exercise training across rat tissues. Cell Metab. 2024;36(6):1411-1429.e10. [CrossRef]
- Picard M, McManus MJ, Gray JD, Nasca C, Moffat C et al. Mitochondrial functions modulate neuroendocrine, metabolic, inflammatory, and transcriptional responses to acute psychological stress Proc Natl Acad Sci U S A. 2015;112(48):E6614-23. [CrossRef]
- Miko HC, Zillmann N, Ring-Dimitriou S, Dorner TE, Titze S, Bauer R. Effects of Physical Activity on Health. Gesundheitswesen. 2020;82(S 03):S184-S195. [CrossRef]
- Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee IM, Nieman DC, Swain DP; American College of Sports Medicine. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43(7):1334-59. [CrossRef]
- Golubnitschaja O, Kapinova A, Sargheini N, Bojkova B, Kapalla M, Heinrich L, Gkika E, Kubatka P. Mini-encyclopedia of mitochondria-relevant nutraceuticals protecting health in primary and secondary care-clinically relevant 3PM innovation. EPMA J. 2024;15(2):163-205. [CrossRef]
- Helms ER, Fitschen PJ, Aragon AA, Cronin J, Schoenfeld BJ. Recommendations for natural bodybuilding contest preparation: resistance and cardiovascular training. J Sports Med Phys Fitness. 2015;55(3):164-78.
- Oppert JM, Bellicha A, van Baak MA, Battista F, Beaulieu K, Blundell JE, Carraça EV, Encantado J, Ermolao A, Pramono A, Farpour-Lambert N, Woodward E, Dicker D, Busetto L. Exercise training in the management of overweight and obesity in adults: Synthesis of the evidence and recommendations from the European Association for the Study of Obesity Physical Activity Working Group. Obes Rev. 2021;22 Suppl 4(Suppl 4):e13273. [CrossRef]
- Chan YS, Jang JT, Ho CS. Effects of physical exercise on children with attention deficit hyperactivity disorder. Biomed J. 2022;45(2):265-270. [CrossRef]
- Khodagholi F, Zareh Shahamati S, Maleki Chamgordani M, Mousavi MA, Moslemi M, Salehpour M, Rafiei S, Foolad F. Interval aerobic training improves bioenergetics state and mitochondrial dynamics of different brain regions in restraint stressed rats. Mol Biol Rep. 2021;48(3):2071-2082. [CrossRef]
- Streckmann F, Balke M, Cavaletti G, Toscanelli A, Bloch W, Décard BF, Lehmann HC, Faude O. Exercise and Neuropathy: Systematic Review with Meta-Analysis. Sports Med. 2022;52(5):1043-1065. [CrossRef]
- Pesta M, Mrazova B, Kapalla M, Kulda V, Gkika E, Golubnitschaja O. Mitochondria-based holistic 3PM approach as the 'game-changer' for individualised rehabilitation - the proof-of-principle model by treated breast cancer survivors. EPMA J. 2024;15(4):559-571. [CrossRef]
- Du L, Xi H, Zhang S, Zhou Y, Tao X, Lv Y, Hou X, Yu L. Effects of exercise in people with multiple sclerosis: a systematic review and meta-analysis. Front Public Health. 2024;12:1387658. [CrossRef]
- Edward JA, Peruri A, Rudofker E, Shamapant N, Parker H, Cotter R, Sabin K, Lawley J, Cornwell WK 3rd. Characteristics and Treatment of Exercise Intolerance in Patients With Long COVID. J Cardiopulm Rehabil Prev. 2023;43(6):400-406. [CrossRef]
- Gaffney FA, Nixon JV, Karlsson ES, Campbell W, Dowdey ABC, Blomqvist CG. Cardiovascular deconditioning produced by 20 hours of bedrest with head-down tilt (-5 degrees) in middle-aged healthy men. Am J Cardiol. 1985;56:634-638.
- Gluckman TJ, Bhave NM, Allen LA, et al. 2022 ACC expert consensus decision pathway on cardiovascular sequelae of COVID-19 in adults: myocarditis and other myocardial involvement, post-acute sequelae of SARS-CoV-2 infection, and return to play. J Am Coll Cardiol. 2022;79(17):1717-1756.
- Ormiston CK, Swiatkiewicz I, Taub PR. Postural orthostatic tachycardia syndrome as a sequela of COVID-19. Heart Rhythm. 2022;19(11):1880-1889.
- Rudofker E, Parker H, Cornwell WK III. An exercise prescription as a novel management strategy for treatment of Long COVID. JACC Case Rep. 2022;4(20):1344-1347.
- Rao P, Peritz DC, Systrom D, Lewine K, Cornwell WK III Hsu JJ. Orthostatic and exercise intolerance in recreational and competitive athletes with Long COVID. JACC Case Rep. 2022;4(17):1119-1123.
- Hughes DC, Orchard JW, Partridge EM, La Gerche A, Broderick C. Return to exercise post-COVID-19 infection: a pragmatic approach in mid-2022. J Sci Med Sport. 2022;25(7):544-547.
- Salman D, Vishnubala D, Le Feuvre P, et al. Returning to physical activity after Covid-19. BMJ. 2021;372:m4721.
- Teo WP, Goodwill AM. Can exercise attenuate the negative effects of long COVID syndrome on brain health? Front Immunol. 2022;13:986950.
- Guan Y, Yan Z. Mitochondrial Quality Control. Adv Exp Med Biol. 2025;1478:51-60. [CrossRef]
- Picca A, Calvani R, Leeuwenburgh C, Coelho-Junior HJ, Bernabei R, Landi F, Marzetti E. Targeting mitochondrial quality control for treating sarcopenia: lessons from physical exercise. Expert Opin Ther Targets. 2019;23(2):153-160. [CrossRef]
- Romanello V, Sandri M. Mitochondrial Quality Control and Muscle Mass Maintenance. Front Physiol. 2016;6:422. [CrossRef]
- Oizumi R, Sugimoto Y, Aibara H. The Potential of Exercise on Lifestyle and Skin Function: Narrative Review. JMIR Dermatol. 2024;7:e51962. [CrossRef]
- Zhou Y, Suo W, Zhang X, Liang J, Zhao W, Wang Y, Li H, Ni Q. Targeting mitochondrial quality control for diabetic cardiomyopathy: Therapeutic potential of hypoglycemic drugs. Biomed Pharmacother. 2023;168:115669. [CrossRef]
- Golubnitschaja O. How to use an extensive Flammer syndrome phenotyping for a holistic protection against health-to-disease transition - facts and practical recommendations. EPMA J. 2025;16(3):535-539. [CrossRef]
- Shao Q, Ndzie Noah ML, Golubnitschaja O, Zhan X. Mitochondrial medicine: "from bench to bedside" 3PM-guided concept. EPMA J. 2025;16(2):239-264. [CrossRef]
- Golubnitschaja O, Sargheini N, Bastert J. Mitochondria in cutaneous health, disease, ageing and rejuvenation-the 3PM-guided mitochondria-centric dermatology. EPMA J. 2025;16(1):1-15. [CrossRef]
- Smokovski I, Steinle N, Behnke A, Bhaskar SMM, Grech G, Richter K, Niklewski G, Birkenbihl C, Parini P, Andrews RJ, Bauchner H, Golubnitschaja O. Digital biomarkers: 3PM approach revolutionizing chronic disease management - EPMA 2024 position. EPMA J. 2024;15(2):149-162. [CrossRef]
- 3PMedicon–your risk reducer. https://www.3pmedicon.com/en/scientific-evidence/compromised-mitochondrial-health assessed on September 19th 2025.
Figure 1.
3PM-guided innovation utilising of high quality mitochondrial biosensorics to advance overall management of health-supportive physical activity; protective measures are tailored to individualised patient profiles.
Figure 1.
3PM-guided innovation utilising of high quality mitochondrial biosensorics to advance overall management of health-supportive physical activity; protective measures are tailored to individualised patient profiles.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



