
Submitted:
24 November 2025
Posted:
25 November 2025
You are already at the latest version
Abstract
This study aims to identify target group, professionals, mechanisms, and outcomes of nature-based health interventions (NBHIs) for people with mild to moderate anxiety, depression, and/or stress. A Delphi-based study was conducted to explore core components of NBHIs. Thirteen researchers with expertise related to the target group responded in Round 1, and eleven in Round 2. Respondents rated statements on a 7-point Likert scale and prioritised core components regarding target group, professionals, mechanisms, and outcomes. A thematic analysis was applied to synthesise qualitative responses.Consensus was achieved on 12 of 21 items across four domains: target group, professionals, mechanisms, and outcomes. Highest agreement concerned core mechanisms (nature interaction, social community, and physical activity), outcome priorities (mental wellbeing and quality of life), and professional competencies. Greater variation was observed regarding group composition and team delivery. Analysis of qualitative expert responses highlighted four key themes: (1) Balancing Group Composition, (2) Adapting Competencies to Context, (3) Core Mechanisms for Change, and (4) Weighing Perspectives in Outcome Selection.By setting out guiding principles for a programme theory, the study lays the foundation for the design and implementation of context-adapted NBHIs. The study underscores the complexity of developing and evaluating NBHIs, highlighting the need to approach them as complex interventions and contributing to a paradigm shift towards a new era of a bio-psycho-social health perspective.
Keywords:
nature-based health interventions
; programme theory
; mental health
; anxiety
; depression
; stress
; Delphi
1. Introduction
People with mild to moderate anxiety, depression, and/or stress experience complex and often long-term challenges that considerably interfere with daily functioning and diminish quality of life [1,2]. This presents a significant challenge as it places substantial demands on healthcare resources, often exceeding available capacity [3,4]. Additionally, existing treatment options may not be adequately tailored to meet their specific needs [5], highlighting the necessity for more sustainable and scalable interventions.
In recent years, there has been increasing academic and societal attention on the positive impact of nature on mental health [6]. Research indicates that natural environments can reduce physiological stress responses, restore attentional capacity, and foster a sense of connectedness and meaning - particularly for individuals experiencing psychological distress [7,8,9,10,11,12]. Central to this development is the understanding that nature is not merely a passive backdrop but an active therapeutic agent that interacts with psychological processes. These central findings build on two distinct theoretical frameworks developed in the late 20th century: the Stress Reduction Theory (Ulrich, 1991), which draws on an evolutionary perspective to explain how natural environments elicit immediate affective responses such as perceived safety and reduced stress; and the Attention Restoration Theory (Kaplan & Kaplan, 1989), which identifies four key environmental qualities—being away, extent, fascination, and compatibility—as essential for restoring depleted attentional capacities [13,14]. This recognition has led to a broader integration of nature-based health interventions (NBHIs) in public healthcare services, emphasising the importance of integrating green spaces and nature-based activities in programmes for mental health and well-being [15,16,17].
However, to develop relevant and sustainable context adapted NBHIs for people with mild to moderate anxiety, depression, and/or stress, there is a need for the design of a systematically developed framework that specifically addresses this target group [18,19]. Furthermore, interventions in natural environments are highly complex efforts, which need careful considerations both in the development phase, as well as in the evaluation. One way to work with such demanding interventions, is by using a complex intervention framework such as the Medical Research Counsil (MRC) framework [18], which highlight the need for a programme theory to develop and evaluate public health efforts. An often-central feat to programme theory is assessing mechanisms of change for interventions, which are often based on theory or practical knowledge. The MRC framework highlights the need to identify core aspects related to the target group (can we mix the target group), the professionals (which therapeutic competencies are necessary), and the underlying mechanisms (what are the active components) in NBHIs. Additionally, the MRC emphasises the selection of relevant measurement tools, as current assessments rely on a wide range of different outcomes (how do we measure the effect) [19].
Nature Impact, a national research project in Denmark, explores how NBHIs impact people experiencing mild to moderate anxiety, depression, and/or stress within a structured healthcare context. Nature Impact seeks to inform the design of context adapted, evidence-based NBHIs that are feasible and can be effectively implemented into structured healthcare and therapeutic settings.
As part of this broader initiative, the present Delphi-based study aims to identify target group, professionals, mechanisms, and outcomes of NBHIs for people with mild to moderate anxiety, depression, and/or stress. The findings will inform the development of a programme theory adapted to the Danish healthcare context, forming the basis for the design and feasibility testing of context adapted NBHIs in Denmark.
2. Materials and Methods
Design
To gather structured insights and achieve reliable consensus on the target group, professionals, mechanisms and outcomes informing the development of design principles and implementation of NBHIs, a Delphi approach was selected [21]. The Delphi method is a systematic, iterative process, in which selected experts respond to multiple rounds of questions, with each round informed by anonymised feedback from the previous one [22]. To deepen understanding and nuance the interpretation of responses, open-ended questions were included alongside closed items.
A two-round modified Delphi technique was applied to address the study aim. The exploratory function of the first round in a traditional three-round Delphi survey - typically used to generate key issues - had already been fulfilled through preparatory work conducted as part of the Nature Impact research project, which provided a robust scientific foundation for the Delphi process. This made it possible to formulate the initial statements in advance, thereby streamlining the two Delphi rounds and ensuring a robust basis for expert evaluation.
Preparatory Work for the Delphi Development
The Delphi process was informed by a preparatory phase aimed at creating a strong conceptual and empirical basis for identifying key themes and developing the questionnaire content. This phase combined two overall complementary approaches: a systematic literature review investigating the effect of participation in NBHIs [19], and three online stakeholder dialogue meetings [23,24] with key stakeholders (n=28). Together, these steps provided both evidence-based knowledge and practice-informed perspectives, forming part of the broader scientific foundation for the Nature Impact project (Figure 1).
The systematic literature review examined the available knowledge on the effect of NBHIs in people with a diagnosis of mild to moderate anxiety and/or depression, and/or experiencing mild to severe stress, focusing on intervention design, population characteristics, and outcome measures [19]. It highlighted significant variation in reported effects and identified 45 different instruments used to measure mental health-related outcomes [19]. These findings guided the selection of topics, proposed mechanisms, and outcome measures to be assessed in the Delphi rounds.
In parallel, three online stakeholder dialogue meetings were conducted to explore practical and experiential perspectives [24]. Respondents (N=28) were recruited through purposive sampling informed by stakeholder analysis with inspiration from participatory mapping [25]. The sample included people with lived experience (n=3), project practice partners (n=8), general practitioners (n=2), representatives from the Danish Nature Agency (n=3), NGOs (n=3), and private nature-health stakeholders (n=9).
The discussions in the online stakeholder dialogue meetings explored the relationship between nature and mental health, mechanisms of change in NBHIs, and the complexities of target group composition, and professional competencies required, particularly in relation to different healthcare settings. Respondents also reflected on contrasts between interventions delivered within the structured healthcare system and those rooted in the voluntary sector, noting distinct organisational logics and structural conditions - without promoting one model over another. The stakeholder dialogue meetings, which did not directly include representatives from volunteer organizations, supported the decision to anchor the intervention framework within the formal healthcare system, although this may have constrained the diversity of perspectives informing the decision. They also emphasised the need to clarify interdisciplinary roles, relevant competencies, and organisational responsibilities critical for long-term implementation. Combined with insights from the systematic literature review, and the stakeholder dialogue meetings, findings directly informed the structure and content of the Delphi questionnaire.
Recruitment
Purposive sampling was used to invite experts with a minimum of five years of experience researching mental health, anxiety, depression and/or stress in Denmark to participate in the study. Expertise was defined as holding a research-related position (associate professor or professor) and having substantial research experience with the target population. To ensure consistency, we selected a homogeneous group representing only researchers, while aiming for variation in educational backgrounds and research fields, including public health, clinical psychology, general practice, psychiatry, rehabilitation, and mental health services. Our goal was to recruit 10–15 respondents. Seventeen researchers were invited via email informing about the project aim and methods and thus being able to respond to any questions prior to data generation and ensure that respondents could keep the planned timing. Of the total 17 researchers invited, 13 responded in the first Delphi round, and 11 continued their response into the second (Table 1). Respondents were leading researchers representing a broad range of professional backgrounds and academic disciplines (Table 1).
Data Generation
Data was generated through two online survey rounds using the platform SurveyXact. Personalised links ensured that only respondents completing the first round were invited to the second round. Each round was open for 14 days, with a reminder email sent after seven days to non-respondents. Data collection took place from 25 September 2024 to 13 November 2024.
Delphi Survey – Round 1
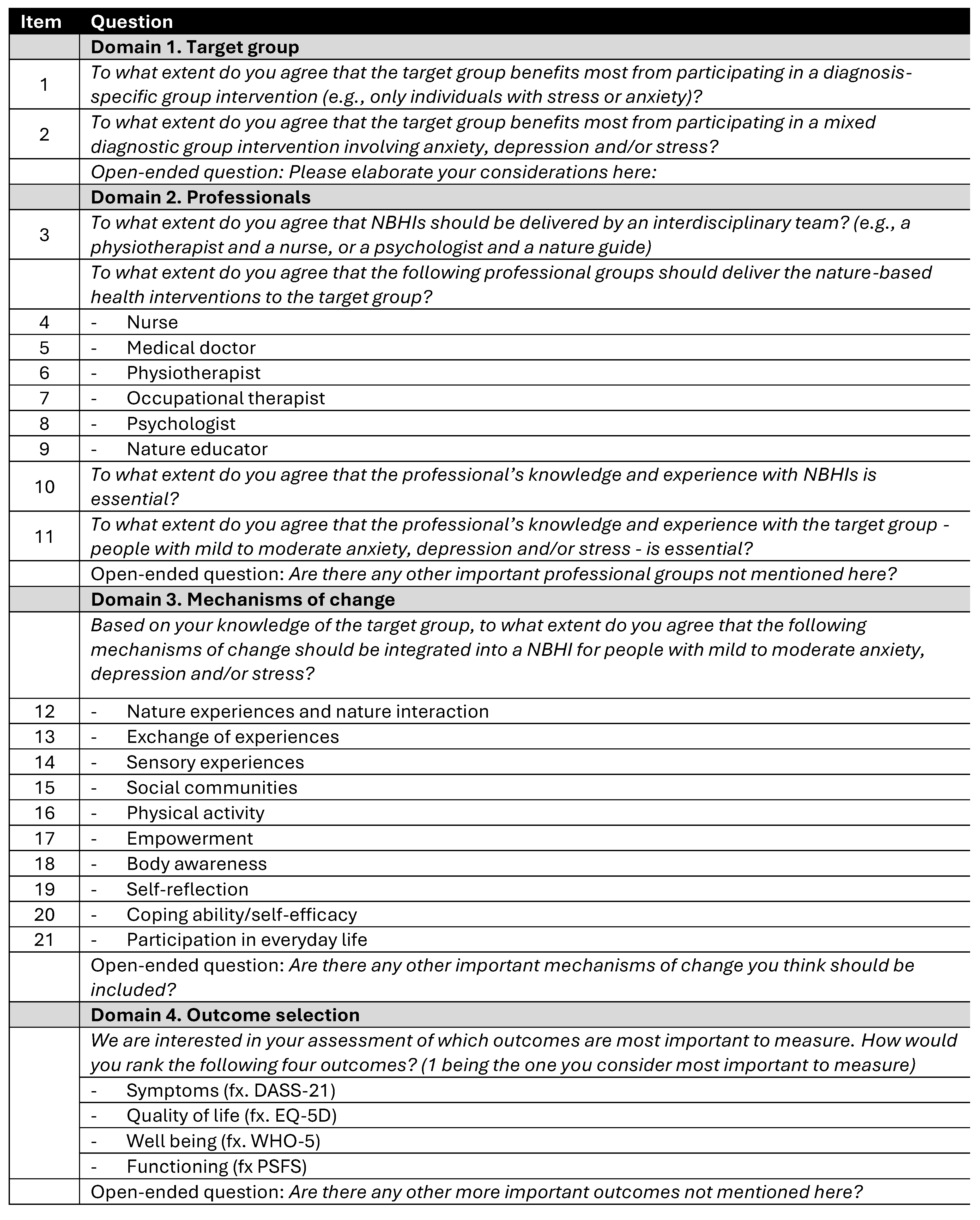
Prior to completing the survey, respondents (N=13) provided informed consent for participation and data handling. The survey included 21 items divided into four domains related to group composition, professionals, mechanisms, and outcomes for an evidence-based NBHI targeting people with mild to moderate anxiety, depression and/or stress (Appendix A). Example of an item was “To what extent do you agree that nature-based health interventions should be delivered by an interdisciplinary team?”. Respondents rated statements on a 7-point Likert scale (from “strongly disagree” to “strongly agree”). To determine consensus, a dual criterion was applied: first, a mean score of ≥ 5.0 was considered indicative of overall agreement; second, consensus was more stringently defined as ≥ 70% of respondents selecting one of the three highest categories (5, 6, or 7), corresponding to “somewhat agree,” “agree,” or “strongly agree.” This dual approach integrates both central tendency and distribution of responses and is consistent with methodological conventions in Delphi research [26]. Additionally, a ranking task was included, asking respondents to prioritise the following outcomes: symptoms, quality of life, mental well-being, and functioning. Each respondent assigned a unique rank order (1 = most relevant), enabling identification of relative outcome priorities across the group. Based on insights from the preparatory phase, nature connectedness had already been selected as a key outcome and was therefore excluded from the ranking exercise.
Each thematic section ended with an open-ended text field, allowing respondents to elaborate and provide additional input. For instance, respondents could suggest additional mechanisms; suggestions mentioned by more than one respondent were reviewed and, if relevant, included in the second round.
Delphi Survey – Round 2
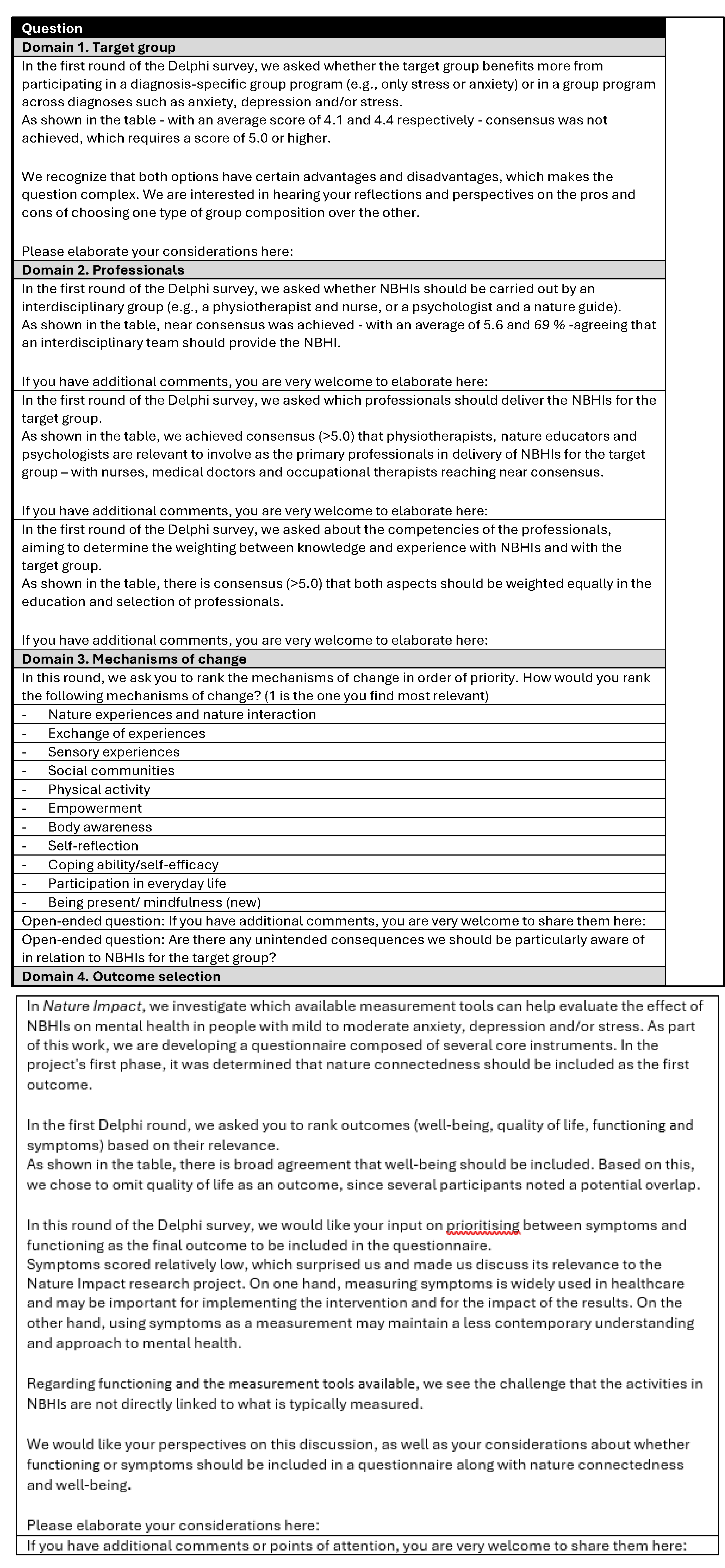
Following the first round, the research team summarised and synthetised all responses and comments, revising the second-round questionnaire for improved clarity and precision based on respondent feedback. Therefore, in round two, we adopted a more exploratory approach, encouraging respondents (N=11) to elaborate on their responses from round one (Appendix B). The aim was to collect more nuanced and detailed feedback. Results from the first round were presented visually using bar charts to aid interpretation. Selected domains were included for further prioritisation in the second round, while items that had already reached consensus were presented for information only and not reassessed. In response to comments in Round 1, an open-ended question was added in Round 2 to examine possible adverse effects. As in the first round, respondents were invited to elaborate on their responses through open-text comment fields linked to each question.
Analysis
Delphi Survey – Round 1 and 2
The analysis was conducted in two phases. First, a descriptive analysis of the quantitative data from both Delphi rounds was performed to identify levels of consensus and prioritisation patterns.
Subsequently, the open-ended responses were analysed qualitatively guided by Reflexive Thematic Analysis as outlined by Braun and Clarke [27,28]. Data from both rounds were integrated and explored through an iterative, reflective process, moving from familiarisation and inductive coding and progressing through theme development, refinement, and naming of themes. Throughout the process, ongoing dialogue within the research team supported coherence, analytical depth, and interpretive rigor. The final themes were structured into a narrative reflecting pattern of meaning aligned with the study aim.
3. Results
Across both rounds, respondents evaluated and prioritised questions related to group composition, team formats and competencies, mechanisms of change and outcome selection. The quantitative part of the Delphi process offered insights into where expert consensus existed - and where divergence remains - on key considerations for developing NBHIs for people with mild to moderate anxiety, depression, and/or stress. Table 2 illustrates how consensus was reached in 12 out of 21 items in total, with 9 items reflecting divergence in the field.
No consensus was reached regarding the optimal group composition for NBHIs. When asked whether respondents with mild to moderate anxiety, depression, and/or stress benefit most from diagnosis-specific groups, the mean score was 4.1. For cross-diagnostic groups, the mean score was slightly higher at 4.4. Only 46% of respondents agreed (5–7) on each statement, indicating divergent expert opinions.
Respondents were asked whether NBHIs should be delivered by an interdisciplinary team. While the item did not formally meet the predefined threshold for consensus (≥70% agreement in categories 5–7), responses strongly indicated support for interdisciplinary delivery of NBHIs. The mean score was 5.6, and 69% of respondents expressed agreement, placing it just below the consensus cut-off. Respondents expressed a clear preference for including health-related and nature-specific competencies in the delivery of NBHIs. In relation to identifying relevant professional backgrounds, physiotherapists reached full consensus with 100% agreement, followed by nature educators (84%) and psychologists (77%), all exceeding the predefined consensus threshold. While nurses (68%), medical doctors (69%), and occupational therapists (61%) did not reach formal consensus, their inclusion still received moderate support.
There was strong consensus that professional expertise is essential in delivering NBHIs, but respondents clearly distinguished between types of knowledge. The highest agreement was found for professionals’ knowledge and experience with the target group - people with mild to moderate stress, anxiety, and/or depression (mean 6.5; 92% agreement). Slightly lower, though still at consensus level, was the emphasis on knowledge of NBHIs themselves (mean 6.3; 77% agreement).
Regarding mechanisms of change necessary for NBHIs, respondents reached consensus on seven out of ten proposed items. The most highly endorsed mechanisms were participation in everyday life (mean 6.3; 100% agreement), social communities (6.6: 92% agreement), and nature experiences and interaction (6.3; 84% agreement), Based on respondents’ feedback in Round 1, mindfulness/presence was added as an additional mechanism and included in the prioritisation exercise in Round 2. Respondents were asked to rank the mechanisms in order of perceived relevance (1 = most relevant) as illustrated in Table 3.
This approach produced a clear hierarchy: when asked to prioritise mechanisms directly against one another, respondents appeared to reconsider their initial ratings. In contrast to Round 1, where participation in everyday life received the highest level of consensus (100%), it was ranked lowest in Round 2. While participation in everyday life remains broadly endorsed as a desirable outcome, it was perceived as less central to the mechanisms of change in NBHIs than more immediate processes such as nature interaction and social communities. The most highly prioritised mechanisms in Round 2 were nature experiences and interaction, social communities, and physical activity, all of which had reached consensus in the first round.
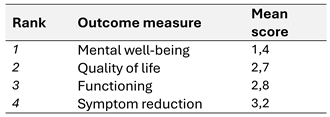
Finally, respondents were asked to prioritise relevant outcomes for evaluating NBHIs. As this approach was only to gather inputs not consensus, a clear pattern of prioritisation emerged (1 = most relevant) (Table 4).
Respondents were asked to rank four outcome domains in order of importance for evaluating NBHIs (1 = most important). Mental well-being was ranked highest (mean 1.4), followed by quality of life (2.7), functioning (2.8), and symptom reduction (3.2). Although the exercise did not seek to establish consensus, the resulting order indicates shared preferences regarding outcome focus on the evaluation of NBHIs in Denmark.
Together, these findings provide a structured overview of where expert agreement converges and where complexity remains. The results offer a quantitative foundation for the more nuanced, qualitative perspectives explored in the following four themes.
Key Insights Through Open-Ended Questions
Additional to the consensus seeking questionnaire, the open-ended questions generated rich insights into key considerations for designing and evaluating NBHIs targeting people with mild to moderate anxiety, depression, and/or stress, and four main themes were identified: Balancing Group Composition, Adapting Competencies to Context, Core Mechanisms for Change, and Weighing Perspectives in Outcome Selection. Together, these themes reflect areas of both consensus and nuanced deliberation, providing a foundation for the development of evidence-informed, context-adapted NBHIs.
Balancing Group Composition
While the quantitative findings showed no clear consensus on group composition, respondents’ qualitative responses shed light on underlying reasoning. A modest preference for cross-diagnostic groups was explained through recognition of shared experiences, high comorbidity, and symptom overlap between anxiety, depression, and stress - factors that challenge rigid diagnostic separation. Mixed groups were described as more reflective of daily practice complexity and as enabling peer mirroring, emotional validation and feelings of normalisation.
Several respondents noted that the natural environment itself may facilitate a transdiagnostic process, where diagnostic labels become less salient in favour of shared experiences such as calm and connection. Mixed diagnostic formats were also seen to support broader personal development, whereas diagnosis-specific groups could risk reinforcing problem-focused identities.
However, respondents emphasised that the optimal group composition should align with the intervention’s structure and target group. For individuals with severe symptoms or where diagnosis-specific psychoeducation is central, targeted groups may be more appropriate. In the absence of definitive evidence favouring one model, practical factors, such as group size and resources, were also cited as important.
Adapting Competencies to Context
Although respondents generally supported the idea of interdisciplinary teams in NBHIs, views also reflected variation and context sensitivity. Qualitative insights underscored that team structure should remain flexible and shaped by the intervention’s goals, target group, and how nature is integrated. Rather than prescribing fixed professional roles, respondents highlighted the importance of combining psychological, physical, and nature-based expertise, adapted to the specific focus and setting of the intervention.
Many noted that physical activity, sensory engagement or psychoeducation require different professional profiles, and that team structure should reflect what is needed for the context adapted NBHI. While physiotherapists and psychologists were preferred, professional roles like nurses and medical doctors were seen as important contributors in planning and consultation, helping to integrate NBHIs within the broader healthcare system. Respondents also emphasised that working in nature can benefit practitioners themselves, potentially enhancing job satisfaction and sustainability. Calls to broaden the definition of NBHIs included suggestions to involve less conventional professionals, such as anthropologists or philosophers, to support existential and holistic perspectives.
There was strong agreement that professionals should possess both knowledge of NBHIs and insight into the target group. Respondents underlined the need for professionals who can sensitively navigate psychological vulnerability while engaging with nature in a credible way. The depth of nature-related competencies required depends on whether nature is used as a setting or an active therapeutic tool.
Core Mechanisms for Change
Respondents described nature experience and interaction, social community participation, and physical activity as interrelated processes central to NBHIs. These mechanisms reflect the embodied and relational dimensions of NBHIs and were seen as foundational for enhancing therapeutic outcomes, particularly by fostering connection, safety and movement.
At the same time, respondents stressed that the mechanisms do not operate in isolation. Many were described as overlapping or mutually reinforcing - such as empowerment and self-efficacy, or nature interaction and sensory engagement - making strict ranking being inadequate to capture their interdependence. The ranking approach was therefore seen less as a fixed hierarchy and more as a reflective dialogue about emphasis, context and sequencing.
Respondents also pointed to the importance of individual variability. Mechanisms like body awareness or mindfulness, while potentially beneficial, were described as distressing for some individuals, particularly those with trauma histories or heightened internal stress. Several called for greater attention to unintended effects and “competing mediators,” urging a shift from asking what works? to what works for whom, and under what conditions? Risks such as emotional overload, accessibility barriers, or post-programme isolation were viewed not as flaws in NBHIs, but as context-dependent outcomes requiring careful consideration.
In summary, respondents broadly agreed that NBHIs should actively incorporate nature interaction, social communities, and physical activity as core therapeutic mechanisms. These were seen as central not only due to their inherent value, but also because they reflect what NBHIs can uniquely offer. At the same time, respondents emphasised that mechanisms must be matched to the needs, capacities, and preferences of individuals. Rather than prescribing fixed components, interventions should be designed with professional sensitivity, allowing for flexibility, responsiveness, and attention to potential unintended effects.
Weighing Perspectives in Outcome Selection
The selection of outcomes for evaluating NBHIs generated both agreement and thoughtful divergence. Respondents ranked mental well-being as the most relevant outcome, with symptom reduction ranked lowest. Thus, round 1 reflected a shared preference for positive, rehabilitation-oriented measures over narrower, clinical symptom metrics. However, in round 2, when asked to reflect more deeply on the choice between everyday functioning and symptoms, more nuanced perspectives emerged.
Many respondents viewed everyday functioning as a more holistic and person-centred outcome, particularly relevant in rehabilitation or preventive contexts. It was seen to better reflect how people manage and live with their symptoms, rather than simply tracking their presence. Conversely, others emphasised the continued relevance of symptom measures, especially for demonstrating clinical effectiveness, enabling comparability with other studies, and meeting research and policy standards. While not the most person-centred, symptoms were viewed as strategically important for gaining recognition within the structured health care system. Patient Reported Outcome Measures were highlighted as a possible bridge between subjective experience and standardised metrics. Respondents broadly supported a focus on well-being, everyday functioning, and quality of life, while also acknowledging the strategic value of symptom tracking in implementation and research.
4. Discussion
Findings from this Delphi study demonstrate that while expert consensus was achieved on several core elements of NBHIs, including target groups, professional competencies, mechanisms of change, and relevant outcomes, there was no uniform agreement on how these elements should be operationalised. Notably, perspectives on group composition and team delivery varied considerably, indicating that such structural and organisational aspects are highly context dependent.
This need for flexibility is consistent with a growing body of literature describing the field as fragmented and lacking in conceptual coherence. As White et al. (2023) argue, the current proliferation of terms, practices, and theoretical traditions creates challenges for the cumulative development and evaluation of NBHIs [29]. A recent systematic review of reviews identified thirteen overlapping categories within the field, including forest therapy, wilderness-based interventions, care farming, blue space interventions, nature play, horticulture, and green exercise, each with its own conceptual lineage, setting, and health logic [30]. This breadth reflects the field's richness but also presents a challenge when developing practice, evaluation, and policy implementation frameworks. NBHIs are inherently complex and diverse, and full standardisation is neither possible nor desirable [18,31].
Building on this premise, the present Delphi study contributes to shaping a flexible and integrative structure. Rather than prescribing fixed formats, it identifies central considerations across four interrelated domains: the people participating in NBHIs, the professionals delivering them, the mechanisms of change involved in NBHIs, and the outcomes used to evaluate impact. These domains do not constitute a rigid model but offer a spectrum of best-practice principles to support local adaptation while maintaining theoretical and practical coherence. The following discussion examines each domain in turn and contextualises the findings within the broader literature.
Discussing the Target Group, Professionals, Mechanisms, and Outcomes
Complex interventions like NBHIs developed for the benefit of the target group, begin with the people involved and the considerations surrounding group composition. In this study, respondents generally supported mixed groups, arguing that anxiety, depression and/or stress are related conditions and thus respondents may benefit from shared processes of reflection, activity and connection. This perspective aligns with recent evidence highlighting the high comorbidity and diagnostic fluidity between these conditions, particularly in primary care [32]. While stress is not a clinical diagnosis per se, it often co-occurs with subclinical or diagnosed anxiety and depression, creating blurred clinical boundaries that challenge categorical approaches [33]. These conditions are also dynamically interrelated: severe stress may exacerbate anxiety and depressive symptoms, while untreated anxiety or depression can increase stress levels.
At the same time, open-ended responses acknowledged that diagnosis-specific groups may be appropriate in certain contexts, such as when addressing acute psychological vulnerability, trauma, or distinct therapeutic requirements. This reinforces the importance of clarifying the intended target group and symptom severity [30,33]. For NBHIs employing a mixed-group format, respondents should be experiencing mild to moderate levels of anxiety, depression and/or stress, with more severe or acute conditions considered a contraindication. This approach reflects a broader shift in mental health and rehabilitation toward need-based, context-sensitive practices rather than strict diagnostic segmentation [34].
The diversity of mental health experiences not only calls for careful consideration of who participates in NBHIs but also informs the composition of professional teams and the competencies required for effective delivery. Findings from this study suggest that NBHIs are best supported through interdisciplinary collaboration, bringing together diverse professional perspectives across disciplines during both planning and implementation. This underscores the need for health professionals who not only draw on their disciplinary expertise but also navigate psychological, physical, and environmental dimensions of health [35].
The findings of this study suggest a prioritisation of psychological, physical, and nature-based competencies in NBHI delivery. Population-specific insight was regarded as the most critical foundation, with nature experience and intervention knowledge seen as essential in combination. This points to the need for professionals who can integrate a deep understanding of the mental health context of respondents with specialised knowledge of nature-based intervention approaches. As described by Bloomfield (2017) [36], a facilitator of NBHIs should be able to speak (at least) two different ‘languages’: the language of healthcare and practice, and the language of nature and environmental engagement. When nature is not merely the setting but the active medium of change, this dual fluency becomes essential, as facilitators must possess the capacity to translate nature experiences into therapeutic value [37,38].
In development, promotion and delivery of effective NBHIs health professionals play a key role [38]. However, a lack of training and confidence in delivering interventions outside conventional clinical settings remains a recognised barrier, particularly regarding the targeted and therapeutic use of natural environments [31,39,40,41]. This underscores the need for strategic investment in upskilling, ensuring that the competencies required to deliver NBHIs are not assumed but actively cultivated through education, guidelines, and organisational support, as also concluded by Stanhope et al. (2023) [42].
Ultimately, the relevance of professional competencies cannot be separated from the mechanisms that drive change in NBHIs. Identifying the factors that influence the effectiveness of these interventions in promoting health and wellbeing remains a key research need [40]. In this Delphi study, three core mechanisms of change reached consensus and were ranked as most important: (1) nature experience and interaction, (2) social community, and (3) physical activity. Together, these mechanisms reflect an embodied and relational understanding of how NBHIs support mental health. This multi-faceted approach distinguishes NBHIs from treatment as usual for individuals with mild to moderate anxiety, depression, and/or stress, where interventions are typically pharmacological or non-pharmacological treatments others than NBHIs, especially regarding depression [43]. By contrast, NBHIs integrate sensory, social, and physical dimensions of experience, aligning therapeutic processes with the environments in which people live and recover. However, a striking drop between Round 1 and 2 in priorisation of ‘participation in everyday life’ was seen and may reflect a distinction between what is valued in principle and what is seen as a primary therapeutic driver. These shifts indicate that while a wide range of mechanisms were seen as relevant when rated individually, forced prioritisation revealed a clearer preference for relational, embodied, and environmental elements as core drivers of change in NBHIs.
The three mechanisms identified in this study also correspond with three of the eleven key moderating and mediating factors influencing the effectiveness of NBIs for overall health and wellbeing, as identified by Kaleta et al. (2023)[30]. Each of these mechanisms is well supported in existing research, offering valuable insights into their individual contributions to health and wellbeing. Interacting and connecting with nature has, over the past decade, developed into an established and impactful research field, with a growing body of consistent evidence demonstrating its effectiveness as a pathway for promoting mental wellbeing [17,19,40,44,45,46]. A related yet distinct line of evidence concerns the role of physical activity. Nature not only facilitates engagement in movement but can also enhance both its amount and intensity, which is why activity is an inherent element of many NBHIs [47,48]. In particular, green exercise interventions have been shown to effectively enhance mental wellbeing [49]. The social dimension of NBHIs is likewise highlighted in both this Delphi study and the wider literature, where group-based settings are found to enhance outcomes [30,36]. Positive social communities and supportive interactions within NBHIs may reduce hopelessness and improve self-worth among people experiencing depression [48].
A key contribution of this Delphi study is the recognition that these mechanisms of change operate in concert, forming interrelated, multi-sensory, affective, and social pathways to mental health and wellbeing. In the context of NBHIs for people with mild to moderate anxiety, depression, and/or stress, the findings further underscore the importance of designing interventions where nature plays a primary therapeutic role [30]. Collectively, these mechanisms signal a shift away from narrow, symptom-oriented models toward a biopsychosocial paradigm in which body, place, and relations are central to promoting mental wellbeing.
While the core mechanisms describe how change is facilitated, the outcomes reflect what that change aims to achieve. The study findings reveal a constructive tension between person-centred relevance and clinical legitimacy, underscoring the need to weigh more perspectives in outcome selection. In the field of NBHIs, there is no single or definitive answer as to which outcomes should be prioritised [30,40,50]. A recent review by Jessen et al. (2025) on the effects of NBHIs for individuals with anxiety, depression and/or stress identified 45 distinct outcome measures, illustrating the diverse ways in which contact with nature influences mental health and wellbeing [19]. This Delphi study contributes by clarifying key considerations for selecting and framing outcomes in this context.
The findings reveal both convergence and constructive divergence in respondents’ views on relevant outcomes for NBHIs. A strong preference for mental well-being over symptom reduction reflects a broader shift toward positive, rehabilitation and recovery-oriented outcomes [34]. At the same time, the debate around everyday functioning versus symptom improvement illustrates the layered complexity of outcome selection [51]. This duality underscores the ongoing tension between clinically legitimised metrics and outcomes that resonate with lived experience. Patient-reported outcome measures were identified as a potential bridge between these domains, combining subjective perspectives with the rigour of standardised assessment.
At a broader level, this tension illustrates the challenges of translating interventions from a biomedical framework into biopsychosocial practice settings [18,52]. The biomedical tradition in mental health research has historically privileged symptom reduction as the primary indicator of success [52]. However, when interventions are situated in outdoor, relational, and dynamic environments, such measures become increasingly insufficient [18]. Respondents implicitly recognised this shift, often emphasising outcomes related to well-being, quality of life, and everyday functioning, dimensions more consistent with a biopsychosocial orientation. Notably, even those who advocated for maintaining symptom measures did so not in opposition to holistic outcomes, but in acknowledgment of the institutional structures that continue to privilege biomedical legitimacy [52].
Collectively, the discussions of target group, professionals, mechanisms, and outcomes in NBHIs highlight a field in transition, moving toward more integrative and context-sensitive understandings of intervention design [53]. This momentum naturally connects to broader developments in health research methodology, particularly the increasing recognition of complexity in intervention science [18].
Towards a New Era in Nature-Based Health Interventions
There is a growing recognition of the necessity to conceptualise public health interventions as complex interventions, as articulated in the 2021 update of the MRC framework [18]. This approach acknowledges the complexity of such interventions, which involve interacting components, dynamic contexts, and non-linear causality. NBHIs is an example of such interventions operating within diverse systems and targeting multiple outcomes, challenging the linear and standardized assumptions of traditional biomedical models.
The MRC framework provides a valuable lens through which to address these complexities inherent to the NBHIs, encouraging researchers and practitioners to consider not only what works, but how, for whom, under what circumstances, and why. By framing NBHIs as complex, the MRC framework highlights the importance of theory-informed design, iterative development through co-production and stakeholder engagement, and contextual sensitivity. It also emphasises the need for mixed-methods/multimethod approaches that capture both measurable outcomes and the nuanced processes through which change occurs [18]. This is particularly relevant in nature-based settings, where individual experiences of nature, the role of facilitators, group dynamics, seasonal and environmental variability, and place-based meanings all contribute to the intervention's effects [54]. Furthermore, this perspective acknowledges the challenges of implementation and scalability. NBHIs often rely on cross-sector collaboration and are shaped by local resources, values, and infrastructures [55]. Thereby, findings from this Delphi-based study support the assumption that the MRC framework is particularly well-suited for guiding the development and evaluation of NBHIs. Recognising and acknowledging NBHIs as complex interventions highlights the need for new approaches to their development and evaluation—marking a shift towards a new era in NBHIs [53].
Methodological Considerations
This study applied a modified two-round Delphi design [20,21], preceded by a preparatory phase consisting of a systematic literature review and stakeholder dialogue meetings [24]. This approach strengthened content validity by grounding the questionnaire in both empirical evidence and practice-based insights [56]. The inclusion of open-ended questions alongside Likert-scaled items enabled both structured prioritisation and deeper interpretive input, crucial in a field characterised by interdisciplinary perspectives and conceptual ambiguity [20].
The combined use of descriptive statistics and Reflexive Thematic Analysis may be viewed as unconventional from a traditional Delphi perspective. However, this integrative approach was chosen to balance numerical consensus with interpretive depth, aligning with the complex and interdisciplinary nature of NBHIs, and reflected in the richness and nuance of respondents’ responses.
The expert panel was relatively homogeneous, comprising senior mental health researchers with limited direct experience in nature-based practices [20]. This focused expertise enhanced internal consistency but may have narrowed the range of perspectives on nature-specific competencies and mechanisms, limiting transferability to broader practice settings [57].
With benefits to both human well-being and pro-nature conservation behaviors, nature connectedness is emerging as an important psychological construct for a sustainable future [10]. In this study, the selection of a nature connection outcome scale was decided prior to the Delphi process to ensure theoretical alignment [30,58], yet this also introduced a potential bias by predefining one outcome as central.
Overall, these methodological choices ensured clinical coherence but may have constrained the inclusion of practice-based or experiential knowledge. The findings are thus most transferable to structured healthcare settings and should be interpreted within this disciplinary context.
5. Conclusions
This study identified key considerations regarding the target group, professionals, underlying mechanisms, and anticipated outcomes that are essential for developing effective NBHIs targeting people with mild to moderate anxiety, depression, and/or stress. Consensus was achieved on key elements for developing NBHIs, including core mechanisms (nature interaction, social community, physical activity), priority outcomes (mental wellbeing, quality of life), and required professional competencies. Greater variation in areas such as group composition and team delivery underscored the need for flexible, context-sensitive approaches. Expert insights highlighted the importance of balancing group heterogeneity, tailoring competencies to local contexts, focusing on core mechanisms for change, and selecting outcomes that capture both holistic wellbeing and clinically relevant improvements. By synthesising expert perspectives through a structured Delphi process, the study provides a comprehensive overview of the elements that should inform intervention design, delivery, and evaluation. These insights contribute to the ongoing advancement of evidence-based practice by bridging conceptual understanding with practical guidance for healthcare professionals, researchers, and policymakers. Furthermore, the study highlights the complexity inherent in the development and evaluation of NBHIs, underscoring the importance of approaching these as complex interventions. By embracing this complexity, rather than seeking to reduce it, NBHIs can be understood and assessed within a broader bio-psycho-social framework. This perspective not only reflects the multifaceted nature of human–nature interactions but also signifies a potential shift from a predominantly biomedical paradigm towards a more integrative understanding of mental health and wellbeing.
In addition, the findings establish guiding principles that can inform the development of a robust programme theory for NBHIs. Such a framework not only clarifies how and why these interventions may work but also facilitates the adaptation of NBHIs to diverse contexts within the Danish healthcare system. By laying a foundation for context adaptive design and implementation, this study supports the integration of NBHIs into mental health care pathways and underscores their potential as complementary approaches to conventional treatments. Future research should build upon these principles to test and refine intervention models, evaluate their effectiveness in real-world settings, and explore long-term impacts on healthcare delivery and patient outcomes.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, LSM, DVP, and NHJ; methodology, LSM, KR, LJN, DVP, and NHJ; software, LSM, and LJN; validation, LSM, DVP, and NHJ; formal analysis, LSM, and NHJ; investigation, LSM, KR, DVP, and NHJ; resources, LSM, and LJN; data curation, LSM, and LJN; writing—original draft preparation, LSM, and NHJ; writing—review and editing, LSM, KR, LJN, DVP, and NHJ; visualization, LSM, LJN, and NHJ; supervision, LSM, and NHJ; project administration, LSM; funding acquisition, LSM, DVP, and NHJ. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the 15th of June Foundation, grant number 2023-0651. The funders had no role in the design of the study, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
Institutional Review Board Statement
According to Danish law, health science questionnaire surveys (and interview) studies that do not involve human biological material (section 14(2) of the Danish Act on Committees), shall not be reported to Ethics Committee or Institutional Review Board approval.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study may be available on request from the corresponding author due to privacy of the respondents.
Acknowledgments
We thank the respondents for sharing their comprehensive knowledge and important thoughts. Furthermore, we thank Peter Lübben for graphic support with Figure 1. During the preparation of this manuscript, the authors used ChatGPT, version 4.0, as a source of inspiration to enhance the readability and clarity of the language in the paper. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
NBHI Nature-based health intervention
MRC Medical Research Counsil
Appendix A.
Items, Ranking and Open-Ended Questions Delphi Round 1
Appendix B.
Ranking and Open-Ended Questions Delphi Round 2
References
- Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2133-61. [CrossRef]
- Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry. 2022;9(2):137-50. [CrossRef]
- National Institute of Public Health [Statens Institut for Folkesundhed]. The Burden of Disease in Denmark – Risk Factors 2022 [Sygdomsbyrden i Danmark – Risikofaktorer 2022]. 2023.
- National Institute of Public Health [Statens Institut for Folkesundhed]. The Burden of Disease in Denmark – Diseases 2022 [Sygdomsbyrden i Danmark – Sygdomme 2022]. 2023.
- Moeller SB, Gbyl K, Hjorthøj C, Andreasen M, Austin SF, Buchholtz PE, et al. Treatment of difficult-to-treat depression - clinical guideline for selected interventions. Nord J Psychiatry. 2022;76(3):177-88. [CrossRef]
- Jimenez MP, DeVille NV, Elliott EG, Schiff JE, Wilt GE, Hart JE, et al. Associations between Nature Exposure and Health: A Review of the Evidence. Int J Environ Res Public Health. 2021;18(9). [CrossRef]
- Franco LS, Shanahan DF, Fuller RA. A Review of the Benefits of Nature Experiences: More Than Meets the Eye. Int J Environ Res Public Health. 2017;14(8). [CrossRef]
- Coventry PA, Brown JE, Pervin J, Brabyn S, Pateman R, Breedvelt J, et al. Nature-based outdoor activities for mental and physical health: Systematic review and meta-analysis. SSM Popul Health. 2021;16:100934. [CrossRef]
- Zelenski JD, RL; Capaldi, CA. Cooperation is in our nature: Nature exposure may promote cooperative and environmentally sustainable behavior. Journal of Environmental Psychology. 2015;42:24-31.
- Martin L WM, Hunt A, Richardson M, Pahl S, Burt J. Nature contact, nature connectedness and associations with health, wellbeing and pro-environmental behaviours. Journal of Environmental Psychology. 2020;Volume 68, 20, 101389. 20 April.
- Hartig T, Mitchell R, de Vries S, Frumkin H. Nature and health. Annu Rev Public Health. 2014;35:207-28. [CrossRef]
- Bratman GN, Anderson CB, Berman MG, Cochran B, de Vries S, Flanders J, et al. Nature and mental health: An ecosystem service perspective. Sci Adv. 2019;5(7):eaax0903. [CrossRef]
- Berman MG, Jonides J, Kaplan S. The cognitive benefits of interacting with nature. Psychol Sci. 2008;19(12):1207-12. [CrossRef]
- Ulrich RS SR, Losito BD, Fiorito E, Miles MA, Zelson M. Stress Recovery During Exposure to Natural and Urban Environments. Journal of Environmental Psychology. 1991;11: 201-230.
- Paredes-Céspedes DM, Vélez N, Parada-López A, Toloza-Pérez YG, Téllez EM, Portilla C, et al. The Effects of Nature Exposure Therapies on Stress, Depression, and Anxiety Levels: A Systematic Review. Eur J Investig Health Psychol Educ. 2024;14(3):609-22. [CrossRef]
- Nguyen PY, Astell-Burt T, Rahimi-Ardabili H, Feng X. Effect of nature prescriptions on cardiometabolic and mental health, and physical activity: a systematic review. Lancet Planet Health. 2023;7(4):e313-e28. [CrossRef]
- Silva A, Matos M, Gonçalves M. Nature and human well-being: a systematic review of empirical evidence from nature-based interventions. J Envir Plan Man. 2023;67(14).
- Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. BMJ. 2021;374:n2061. [CrossRef]
- Jessen NH, Løvschall C, Skejø SD, Madsen LSS, Corazon SS, Maribo T, et al. Effect of nature-based health interventions for individuals diagnosed with anxiety, depression and/or experiencing stress-a systematic review and meta-analysis. BMJ Open. 2025;15(7):e098598. [CrossRef]
- Trevelyan EG, Robinson N. Delphi methodology in health research: how to do it? European Journal of Integrative Medicine. 2015;7(4):423-8.
- Becker GE, Roberts T. Do we agree? Using a Delphi technique to develop consensus on skills of hand expression. J Hum Lact. 2009;25(2):220-5. [CrossRef]
- Rowe, G. The Delphi technique as a forecasting tool: Issues and analysis. Int J Forecasting. 1999;15 (4):353-5.
- Krueger RA Casey, MA. Focus groups: A practical guide for applied research (5th ed.). SAGE Publications. 2014.
- Coghlan D, Brydon-Miller M. Multi-Stakeholder Dialogue. The SAGE Encyclopedia of Action Research. Sage Research Methods.
- Denwood T, Huck JJ, Lindley S. Participatory Mapping: A Systematic Review and Open Science Framework for Future Research. Annals of the American Association of Geographers 2021.
- Jünger S, Payne SA, Brine J, Radbruch L, Brearley SG. Guidance on Conducting and REporting DElphi Studies (CREDES) in palliative care: Recommendations based on a methodological systematic review. Palliat Med. 2017;31(8):684-706. [CrossRef]
- Clarke V, Braun V. Successful Qualitative Research: A Practical Guide for Beginners. SAGE. 2013.
- Braun V, Clarke V. Using thematic analysis in psychology. Qualitative Research in Psychology. 2008. 2008. [CrossRef]
- White MP, Hartig T, Martin L, Pahl S, van den Berg AE, Wells NM, et al. Nature-based biopsychosocial resilience: An integrative theoretical framework for research on nature and health. Environ Int. 2023;181:108234. [CrossRef]
- Kaleta B, Campbell S, O'Keeffe J, Burke J. Nature-based interventions: a systematic review of reviews. Front Psychol. 2025;16:1625294. [CrossRef]
- McCluskey A, Middleton S. Delivering an evidence-based outdoor journey intervention to people with stroke: barriers and enablers experienced by community rehabilitation teams. BMC Health Serv Res. 2010;10:18. [CrossRef]
- Christensen, KS. Validating the 15-item stress anxiety depression scale (SAD-15) using Rasch analysis. J Psychosom Res. 2025;197:112349. [CrossRef]
- Feng G, Xu X, Lei J. Tracking perceived stress, anxiety, and depression in daily life: a double-downward spiral process. Front Psychol. 2023;14:1114332. [CrossRef]
- Slade, M. Measuring recovery in mental health services. Isr J Psychiatry Relat Sci. 2010;47(3):206-12.
- World Health Organization. WHO Rehabilitation competency framework. Geneva; 2020. https://www.who. 14 November 5431.
- Bloomfield, D. What makes nature-based interventions for mental health successful? BJPsych Int. 2017;14(4):82-5. [CrossRef]
- Vibholm AP, Christensen JR, Pallesen H. Occupational therapists and physiotherapists experiences of using nature-based rehabilitation. Physiother Theory Pract. 2023;39(3):529-39. [CrossRef]
- Tambyah R, Olcoń K, Allan J, Destry P, Astell-Burt T. Mental health clinicians' perceptions of nature-based interventions within community mental health services: evidence from Australia. BMC Health Serv Res. 2022;22(1):841. [CrossRef]
- Wolsko C Hoyt, K. Employing the restorative capacity of nature: Pathways to practicing ecotherapy among mental health professionals. Ecopsychology. 2012;4(1):10-24. [CrossRef]
- Shanahan DF, Astell-Burt T, Barber EA, Brymer E, Cox DTC, Dean J, et al. Nature-Based Interventions for Improving Health and Wellbeing: The Purpose, the People and the Outcomes. Sports (Basel). 2019;7(6). [CrossRef]
- Madsen LS, Nielsen CV, Oliffe JL, Handberg C. Navigating a Middle Ground - Exploring Health Professionals' Experiences and Perceptions of Providing Rehabilitation in Outdoor Community Settings. Qual Health Res. 2021;31(1):41-53. [CrossRef]
- Stanhope J, Foley K, Butler M, Boddy J, Clanchy K, George E, et al. Australian allied health professionals' perspectives on current practice, benefits, challenges, and opportunities in nature-based approaches. Health Place. 2025;93:103430. [CrossRef]
- Gartlehner G, Wagner G, Matyas N, Titscher V, Greimel J, Lux L, et al. Pharmacological and non-pharmacological treatments for major depressive disorder: review of systematic reviews. BMJ Open. 2017;7(6):e014912. [CrossRef]
- Passmore HA, Mangat A, Dhanoa T, Schmitt MT, Mackay CML, Richardson M, Howell AJ, Lutz PK. Enhancing personal and planetary wellbeing: A comparative study of the "3 Good Things" and "3 Good Things in Nature" interventions. International Journal of Wellbeing. 2025;15(4):1–28.
- Capaldi CA, Passmore HA, Nisbet EK, Zelenski J M, Dopko RL. Flourishing in nature: A review of the benefits of connecting with nature and its application as a wellbeing intervention. International Journal of Wellbeing. 2015;5(4), 1-16. [CrossRef]
- McMahan EA, Estes D. The effect of contact with natural environments on positive and negative affect: A meta-analysis. The Journal of Positive Psychology. 2015;10(6):507–19. [CrossRef]
- Gladwell VF, Brown DK, Wood C, Sandercock GR, Barton JL. The great outdoors: how a green exercise environment can benefit all. Extrem Physiol Med. 2013;2(1):3. [CrossRef]
- Rosa CD, Chaves, T. S., Collado, S., Larson, L. R., Profice, C. C. The Effect of Nature-Based Adventure Interventions on Depression: A Systematic Review. Environ Behav. 2023. [CrossRef]
- Rogerson M, Wood C, Pretty J, Schoenmakers P, Bloomfield D, Barton J. Regular Doses of Nature: The Efficacy of Green Exercise Interventions for Mental Wellbeing. International Journal of Environmental Research and Public Health. 2020;17:1526. [CrossRef]
- Reis AC, Gray T, Mann J, Mallinson J, Katnoria M, Seach W, Peel N. Measuring nature-based health interventions: A rapid review of instrumentation and outcomes. International Journal of Environmental Research and Public Health. 2023;20(21), 7043. [CrossRef]
- Jacob S, Munro I, Taylor BJ, Griffiths D. Mental health recovery: A review of the peer-reviewed published literature. Collegian. 2017;24(1):53-61. [CrossRef]
- Farre A, Rapley T. The New Old (and Old New) Medical Model: Four Decades Navigating the Biomedical and Psychosocial Understandings of Health and Illness. Healthcare (Basel). 2017;5(4). [CrossRef]
- Sterckx A, Delbaere B, De Blust G, Spacova I, Samson R, Remmen R, et al. Quality criteria of nature-based interventions in healthcare facilities: a scoping review. Front Public Health. 2023;11:1327108. [CrossRef]
- Harries B, Chalmin-Pui LS, Gatersleben B, Griffiths A, Ratcliffe E. Noticing nature: The role of environmental awareness in promoting well-being. British Ecological Society. 2025. [CrossRef]
- Madsen LS, Poulsen DV, Sørensen TB, Vibholm P, Mygind O, Maribo T. Increasing Engagement with the Outdoors – A Green Paper on Nature as a Resource in Health Promotion Efforts, 1st Edition [Vi skal mere ud – Grønbog om naturen som ressource i sundhedsindsatser, 1. udgave]. Rehabilitation Forum Denmark [Rehabiliteringsforum Danmark]. Aarhus. 2022.
- Estremera ML, Mendoza-Sarmiento MA. Content validity and reliability of questionnaires: trends, prospects and innovation in the digital research epoch. ASEAN Innovative and Transformative Education Journal. 2024. [CrossRef]
- Baker J, Lovell K, Harris N. How expert are the experts? An exploration of the concept of 'expert' within Delphi panel techniques. Nurse Res. 2006;14(1):59-70. [CrossRef]
- Keenan R, Lumber R, Richardson M, Sheffield D. Three good things in nature: a nature-based positive psychological intervention to improve mood and well-being for depression and anxiety. J Public Ment Health. 2021;20(4):243-50. [CrossRef]
Figure 1.
Illustration of the full development and involvement phases of the Nature Impact project informed by a co-production approach – including the scientific foundation forming the preparatory work of the Delphi process.
Figure 1.
Illustration of the full development and involvement phases of the Nature Impact project informed by a co-production approach – including the scientific foundation forming the preparatory work of the Delphi process.
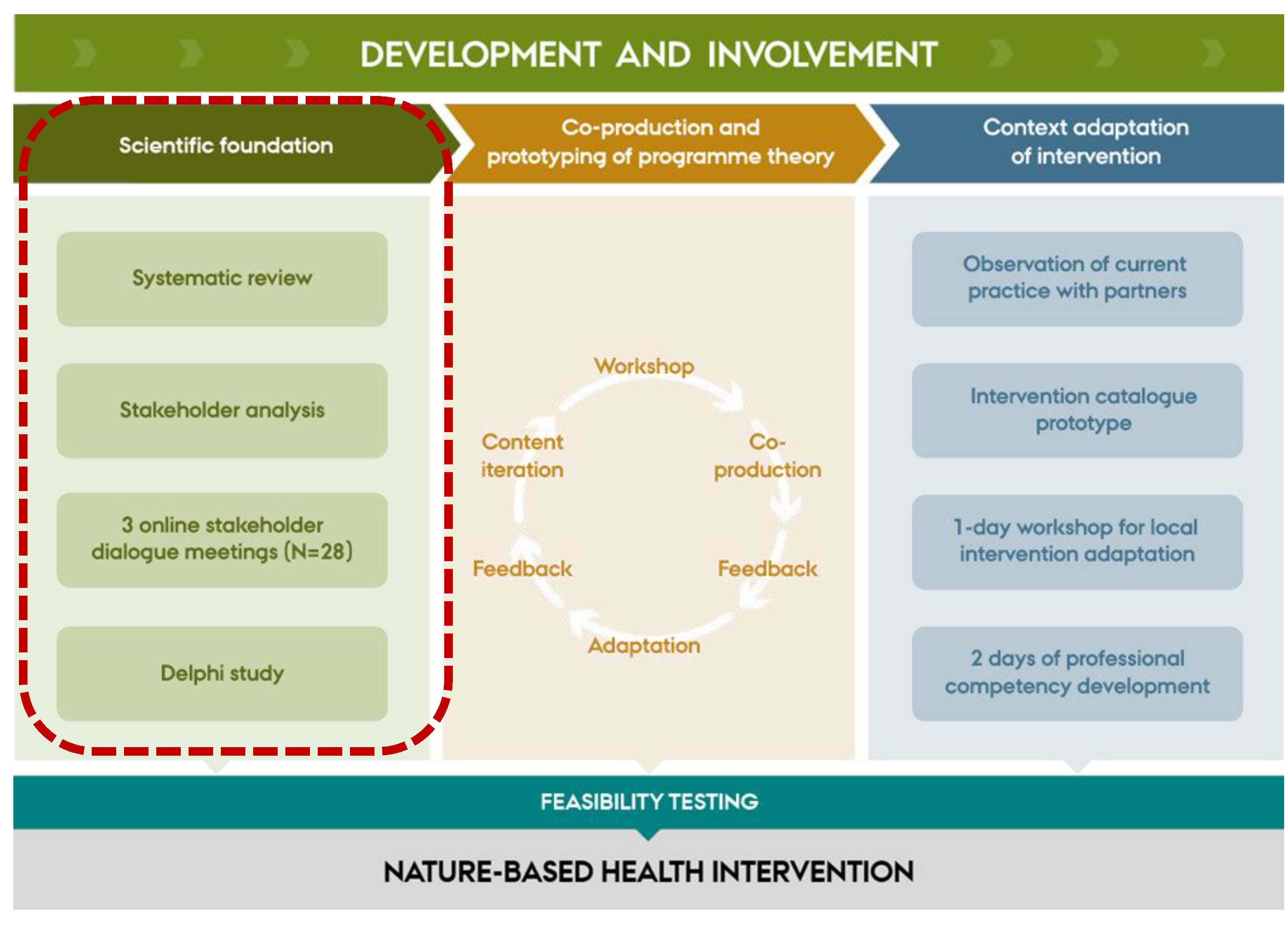

Table 1.
Sociodemographic of respondents Round 1 and 2.
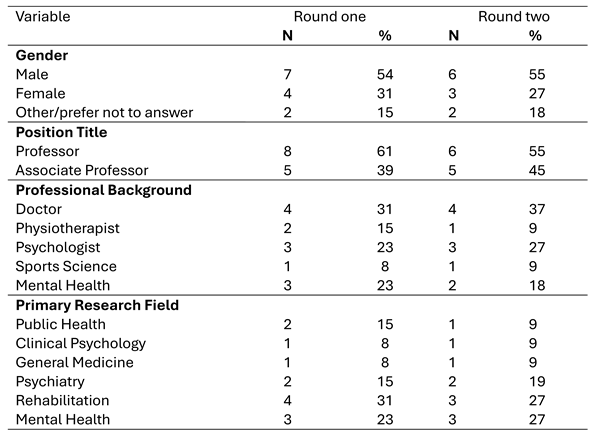
Table 2.
Expert agreement on key aspects of NBHIs (delphi round 1).
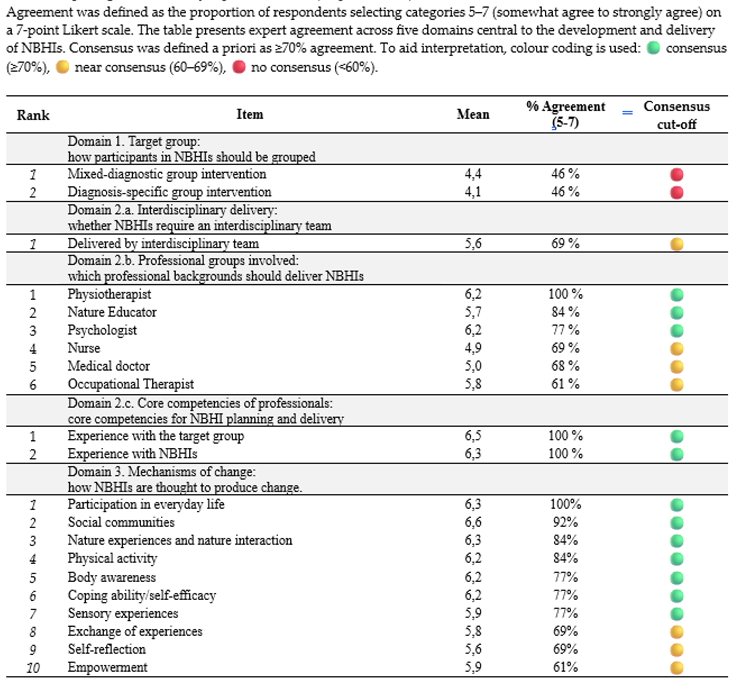
Table 3.
Comparative Ranking of Mechanisms of Change Across Delphi Rounds. The table presents a comparison of mean ranks assigned by respondents in Round 2 with the relative position of each mechanism in Round 1. Lower mean values in Round 2 indicate higher perceived relevance (1 = most relevant). The table illustrates how prioritisation shifted between rounds.
Table 3.
Comparative Ranking of Mechanisms of Change Across Delphi Rounds. The table presents a comparison of mean ranks assigned by respondents in Round 2 with the relative position of each mechanism in Round 1. Lower mean values in Round 2 indicate higher perceived relevance (1 = most relevant). The table illustrates how prioritisation shifted between rounds.
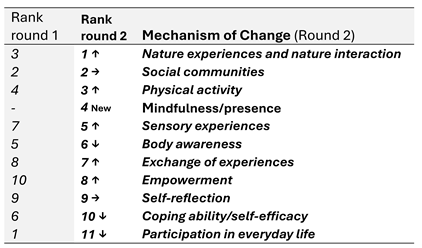
Table 4.
Prioritisation of Outcomes for Evaluating NBHIs. The table shows the outcomes ranked by respondents in order of perceived relevance. Lower mean scores indicate higher prioritisation.
Table 4.
Prioritisation of Outcomes for Evaluating NBHIs. The table shows the outcomes ranked by respondents in order of perceived relevance. Lower mean scores indicate higher prioritisation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



