
Submitted:
24 November 2025
Posted:
25 November 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The successful use of bromhexine hydrochloride (BRH) for COVID-19 prevention led us to apply the same method for flu prevention. The goal of this study is to observe whether BRH could protect people against influenza.This is non-interventional, observational, questionnaire-based survey. General practitioners informed their patients to take BRH 8 mg twice per day for at least 3 weeks if they want. The mean participant age was 58.9 years (95% CI: 57.4–60.5), with a median of 62 years, indicating that the sample predominantly consisted of individuals over 60 years of age.The average number of comorbidities was 0.98, and the mean duration of prophylactic use was 80 days (95% CI: 76.7–83.7). The reported influenza incidence within the sample was 10.6%.Influenza incidence among individuals taking BRH prophylactically was significantly lower compared to national data (36.15%). Longer use was associated with a modest reduction in risk. The number of comorbidities remained the strongest predictor of influenza occurrence. Age had no significant impact among those using BRH prophylactically. The model demonstrated good discriminative ability but limited calibration, and the results should be interpreted cautiously.
Keywords:
influenza
; bromhexine hydrochloride
; TMPRSS2
; Covid‐19
1. Introduction
Over the past 100 years the world has been ravaged by deadly influenza A/H1N1 (1918-1920) and SARS-CoV-2 (2019-) virus pandemics, with death tolls respectively between 17-100 million [1] and 7.1-36.5 million [2]. In addition, two other flu pandemics in the 20th century also claimed millions of lives: 1957–1958 Influenza A/H2N2 pandemic between 1-4 million deaths [3] and 1968-1969 Hong Kong Influenza A/H3N2 pandemic also between 1-4 million deaths [4].
In contrast to the great theoretical progress in unravelling the pathogenetic mechanisms of influenza and COVID-19, there is currently no effective prevention and treatment for the complications of these diseases [5]. In addition to tens of millions of victims, these pandemics also caused enormous financial losses to Humanity.
The best strategy would be to prevent the virus from entering the host cells. This is also the main task of vaccines. For example, probably the biggest killer in human history, smallpox, disappeared from the world's health map thanks to the vaccine. Unfortunately, for a number of reasons, vaccines are not effective enough against either COVID-19 or the flu. COVID-19 vaccines do not appear to be effective against secondary infection. What's more, significantly high number of vaccinated individuals had a secondary encounter and subsequent infection with COVID-19 [6], which is explained by their “high-risk” activities, such as avoiding social distancing, engaging in more-frequent public activities [7].
Another approach is to block the entry of viruses into the cell by inhibiting the proteases responsible for this.
Very interestingly, the main protease responsible for the penetration of SARS-CoV-2 and Influenza is the same - the Transmembrane Protease Serine S1 subtype 2 (TMPRSS2), whose role in these viruses is well established [5,8,9,10,11,12,13,14,15].
To be used prophylactically, a drug must have a favourable safety profile during extended use. BRH is exactly like that! BRH, a well-known inhibitor of TMPRSS2, is derived from Vasicin, a plant-based active ingredient and alkaloid that was developed from the Indian lung herb, Adhatoda vasica [16,17]. This mucolytic cough suppressant, known since 1963, is inexpensive, over the counter, non-invasive, effective, with proven safety, available globally, and well-tolerated. In addition, it has been shown to have anti-inflammatory effects, thus reducing swelling and irritation in the respiratory tract [17,18,19,20,21,22].
We recently published case reports and data analysing 125 people who took BRH prophylactically during the COVID-19 pandemic [18,22]. The effect of BRH is best when given continuously for prophylaxis during peaks of contagion in the wave of COVID-19. Then the probability of infection drops sharply, and if a disease does occur, it proceeds mildly. BRH is also effective when given by inhalation for post-exposure prophylaxis. When COVID-19 manifests itself clinically, the efficacy of BRH drops sharply because the virus is already in the cell. However, BRH inhalations are useful because they limit the spread of the virus and have an anti-inflammatory and possibly antiviral effect [18,19,20,21,22].
The successful use of BRH for COVID-19 prevention led us to apply the same method for flu prevention. The goal of this study is to observe whether BRH could protect people against influenza.
2. Methods and Sample
This is non-interventional, observational, questionnaire-based survey. Information and reasoning of the probable prophylactic effect of BRH against flu was presented in front the general practitioners. Those who agreed to recommend it to their patients were approached. Physicians informed their patients of the experimental study, advised on safety-profile, established an individual treatment plan and duration, applied an informed consent form, scheduled follow-up. The dosing was 2 tablets of 8 mg per day at least 3 weeks before the peak influenza season. Duration was based on individual patient preference, and risk factors. The herbal nature of the medicine reassured people, thus, enabling longer duration of BRH application.
Once the epidemic season subsided (measured as a significant decline in weekly reported cases by the Regional Health Directorate), patients on BRH were asked to report to their physician on key information such as incidence, number of infections, duration of BRH intake. From the patient’s dossier we collected information about the respondents age and comorbidities.
Sample size calculation was based on reported prevalence of acute respiratory infections (ARI) through the national portal for the year 2023 – P = 30%. Sample size formula used was (Z2 x P(1-P))/∆2 – with ∆ (Margin of error) set at 5% and Z = 1.96 for a 95% Confidence interval. A total of 462 questionnaires were collected, of which 407 were valid for analysis. Fifty-five were excluded due to missing data on influenza occurrence or on BRH dosage and duration.
Demographic statistic and logistic regression analyses (enter method) were performed to evaluate the respondents’ characteristics and predictive factors for influenza development.
3. Results
3.1. Demographic Analysis
The mean participant age was 58.9 years (95% CI: 57.4–60.5), with a median of 62 years, indicating that the sample predominantly consisted of individuals over 60 years of age. The average number of comorbidities was 0.98, and the mean duration of prophylactic use was 80 days (95% CI: 76.7–83.7).
The reported influenza incidence within the sample was 10.6%.

Table 1.
Respondents’ demographics.
| Age | Duration of Utilization (Days) | Number of Comborbidities | Self-Reported Incidence | |
| Sample (n) | 405 | 407 | 407 | 407 |
| mean | 58.96 | 80.2 | 0.98 | 10.6% |
| 95% CI | 57.413 - 60.503 | 76.667 - 83.726 | 0.877 - 1.088 | 7.57% - 13.6% |
| Variance | 250.30 | 1312.2962 | 1.1746 | 0.09472 |
| Standard error | 0.7862 | 1.7956 | 0.05372 | 0.01526 |
| Median | 62.000 | 90.000 | 1.000 | 0.000 |
| 95% CI | 60.000 - 63.000 | 90.000 - 90.000 | 1.000 - 1.000 | 0.000 - 0.000 |
| Minimum | 6.000 | 5.000 | 0.000 | 0.000 |
| Maximum | 91.000 | 180.000 | 7.000 | 1.000 |
Several indicators show that the group is heterogenous with a slight prevalence of elderly. The age range spans for 85 years, with a corresponding high variance, as well as the right-side skewness of the sample (Figure 1.) Maximum number of comorbidities observed in a single patient were 7, Subsequent analyses revealed 37 (9%) patients with 3 more comorbidities.
3.2. Comparison with National Incidence
According to data from the National Centre for Infectious and Parasitic Diseases (NCIPD) [23], for 2023, the combined incidence of acute respiratory infections and influenza was 36.15%, whereas the annual influenza incidence in this pilot study was significantly lower (10.6%, p<0.0001).
Even assuming an influenza only incidence of 15% in the general population, the difference remained statistically significant (p=0.0157). Sample and population monthly incidence were 1% and 1.62%, respectively.
These findings suggest a potential prophylactic effect of BRH against influenza infections, despite the inherent limitations of the study.
3.3. Logistic Regression Analysis
Three variables were examined for their influence on influenza occurrence (Table 2):
- -
- Duration of intake (days)
- -
- Number of comorbidities
- -
- Age
The model demonstrated good predictive performance (AUC=0.79).
Two significant predictors were identified (Table 3):
- -
- Number of comorbidities – each additional comorbidity increased the risk of influenza by approximately 92% (OR=1.92; 95% CI: 1.43–2.57; p<0.0001).
- -
- Duration of intake – longer prophylactic use was associated with a slight but statistically significant reduction in risk (OR=0.99; p=0.0378), equivalent to about a 1% lower risk for every 10 additional days of use.
Age showed no independent effect on influenza risk, suggesting that among BRH users, age does not play a significant role—a finding that contrasts with population-level data where age is a known risk factor in the absence of prophylaxis.
The negative correlation for the duration was not influenced by the number of tablets per day,
3.4. Subgroup Analysis (Patients with ≥3 Comorbidities)
Among 37 patients with three or more comorbidities, influenza incidence was 21.6% vs 9.6% in the sample with 2 or less comorbidities (p = 0.04). Mean and median ages in this sample was 68.32, and 63 years, respectively, confirming elderly with comorbidities are more susceptible to influenza.
Influenza rates in this subset were significantly lower than the combined incidence of influenze+ARI in the population (difference 14.55%, p<0.0001), but no significance was observed for the hypothetical incidence of influenza only at 15% in the general population.
4. Discussion
Drug repurposing presents a well-established approach in identifying new uses for established drugs [24,25]. Examples of successful repurposing efforts include methotrexate, valproic acid, aspirin and even thalidomide [26]. Since this approach reduces the high financial burden, and failure rate seen in traditional drug discovery, renewed efforts have been put into finding novel targets for established products. From 2000 to 2018 a continuous growth in repurposing studies has been reported [27], with the trend not subsiding. The COVID-19 pandemic acted as a catalyst for drug repurposing due to the urgency with which new treatments were sought [28]. Although most investigated treatments focused on systemic administration and effect, the lungs represent the primary injury site, with cases of acute lung injury or acute respiratory distress syndrome being observed in many COVID-19 cases [29]. This often-overlooked aspect of adjuvant treatment has led to the inclusion of BRH (ambroxol-derivate of BRH) as a potential prophylactic agent, since it has been shown to inhibit the TMPRSS2. TMPRSS2 has emerged as a key player in viral pathogenesis [30], and a potential target for anti-influenza drug discovery [31]. However, drug repurposing studies of TMPRSS2 inhibitors are few and far between, with the use of BRH in the outpatient setting being very uncommon [32]. Most studies, focusing on the efficacy side of BRH limit the primary or secondary endpoints to the symptomatic relief in patients with bronchitis, as evidenced in the public assessment report [33].
It should not be surprising that prophylactic use has been vastly understudied, since a trial design in such a setting is extremely challenging. Researchers need to account for risk factors, potential issues in sample bias, patient-level factors such as adherence, as well as aim for a larger-than-average sample size, due to the low incidences [34]. Retrospective and self-reported studies such as ours attempt to fill the gap in knowledge, particularly in the absence of well-designed clinical trials, despite the inherent limitations of such trials.
Convinced in the efficacy of this prophylactic approach, our study seems to validate our hypothesis of the potential inhibitory effect of BRH for influenza in patients. Previous studies have demonstrated conclusively the in-vitro efficacy [35,36], and despite being studied for COVID-19 [37,38] BRH’s use in influenza has been overlooked [5].
SARS-CoV-2 and influenza viruses have very similar mechanism of cell penetration, clinical presentations and they are likely to continue co-circulating in the foreseeable future [5,39]. After binding to angiotensin-converting enzyme 2 (ACE2), which serves as a receptor for SARS-CoV-2, the virus spike protein must be cleaved into 2 subunits - SARS-CoV-2-S1, that binds to ACE2, and SARS-CoV-2-S2, which mediates fusion of the viral envelope and host cell membranes [40]. TMPRSS2 is the main protease for proteolytic activation of SARS-CoV-2 [41].
For entering host lung cells IAV binds to α−2,6-Gal sialic acid or α−2,3-Gal sialic acid receptors. Surface proteins of IAV and IBV virus hemagglutinin (HA) is a homotrimer, expressed as precursor, that must be cleaved by host proteinases, where TMPRSS2 plays a primary role. TMPRSS2 activates IAV HA as well as IBV HA [42], although this applies more to IAV [10] where TMPRSS2 is the main protease for monobasic HA cleavage in IAV strains in vivo [43,44,45]. Therefore, TMPRSS2 is a suitable molecular target for the development of anti-influenza drugs [15,42].
SARS-CoV-2 and IAV operate as an “organized crime group”. SARS-CoV-2 Delta variants upregulated α−2-3-linked sialic acid expression, while IAV infection upregulated ACE2 and TMPRSS2. Furthermore, co-infection with SARS-CoV-2 and IAV exacerbated cellular damage compared to infection with either virus alone [46]. Several studies have reported co-infection or sequential infection with SARS-CoV-2 and especially with IAV in COVID-19 patients [47,48,49,50,51,52].
Thus, сo-infection with influenza virus has been linked to an earlier and more severe cytokine storm in patients with severe COVID-19 [53].
The overall proportion of co-infection was estimated to be 0.7%, with a predominance of the IAV (74.4%), as among critically ill COVID-19 patients tended to be higher than that in overall patients [54].
Inhibition of TMPRSS2 by BRH as the Basis for Prevention of COVID-19 and Influenza
BRH showed a higher inhibition effect than camostat, a widely known TMPRSS2 inhibitor [55]
Moreover, TMPRSS2-deficient mice are healthy [56], suggesting that the inhibition of TMPRSS2 may not harm the host.
The FDA-approved expectorant/mucolytic agent and cough suppressant, BRH, is a well-known potent inhibitor of TMPRSS2 with IC50 equal to 0.75 μM [9]. Since epithelisin is expressed primarily in the apical surface of airway epithelial cells, inhibiting pulmonary TMPRSS2 with BRH could represent a prophylactic strategy against the airborne transmission of SARS-CoV2 [57].
It should be noted that the dependence on TMPRSS2 is different for the different subspecies of IAV. It is bigger for H1N1/1918 and H13, while recombinant IAVs carrying H12 or H17 were not affected by TMPRSS2 knockdown [58]. TMPRSS2 activates also the HA in IAV subtypes H2, H3, H5, H6, H8, H10, H11, H14, and H15 [59].
Several trials have been conducted to determine BRH efficacy, however, its usefulness remains controversial [17,20,37,38,60,61,62,63,64].
In our experience, administration of inhaled BRH is beneficial in both outpatient and inpatient settings [19]. This will be more or less effective, but in no case decisive to avoid possible complications. As we have already noted, only inhibition of the hyperactivated NLRP3 inflammasome can save the patient from cytokine storm (CS), multiorgan damage and death [65]. BRH is most effective when given prophylactically over the course of a month during the peak of viral spread or by inhalation as post-exposure prophylaxis [Table 4].
Many hopes were placed on the TMPRSS2 inhibitor Camostat Mesylate (CM), previously used for treatment of pancreatitis and reflux oesophagitis, now for the treatment of COVID-19 [41]. At least 12 prestigious clinical trials have been launched to investigate the effectiveness of CM in COVID-19. Despite high expectations, the results are disappointing [66].
These results can be easily predicted, for the following reasons: SARS-CoV-2 used two distinct routes to enter cells, one fast (˜10 min) (TMPRSS2-mediated virus uptake), and one slower (40–50 min), corresponding to cathepsin L priming (endosomal uptake) [67]. The mean incubation period for COVID-19 onset was estimated to be 5.1 days, and most cases develop symptoms after 14 days [68]. Due to this fact, inhibiting TMPRSS2 after the virus has long since entered the cell, replicated, and infected other cells is doomed to failure. The conclusion is that successful prevention can be expected if TMPRSS2 is inhibited preventively (Table 4).
This means that long-term use of an inhibitor should be safe. BRH is exactly like that! Unlike furin, very little is known about the physiological role of the TMPRSS2 [69], but it is not required for normal development and does not cause pathological changes as demonstrated in TMPRSS2 knockout mice [56]. In addition, BRH may reach in pulmonary and bronchial epithelial cells concentrations 4 to 6-fold higher than those found in the plasma - high enough to inhibit TMPRSS2 [70].
Very recently, cases of elderly women with severe comorbidities were published, who after long-term prophylaxis with BHH, practically did not get sick with COVID-19, although their families became seriously ill [18].
Our study aims in part to be a proof-of-concept, and in part to initiate wider dialogue within the scientific community of the benefits associated with continued use of BRH during peak influenza season, particularly in susceptible populations. Our finding that concurrent use of BRH led to no correlation between age and infection probability indicates a potential use in elderly, who are known to be at a higher risk of complications [71].
A limitation to this is that the influenza statistic was self-reported and not laboratory confirmed. Future research aims to rectify this by requesting country-wide laboratory data through the freedom of information act (FOIA) in Bulgaria.
5. Conclusions
Influenza incidence among individuals taking BRH prophylactically was significantly lower compared to national data. Longer use of BRH was associated with a modest reduction in risk.
The number of comorbidities remained the strongest predictor of influenza occurrence.
Age had no significant impact among those using BRH prophylactically.
The model demonstrated good discriminative ability but limited calibration, and the results should be interpreted cautiously.
Acknowledgments
This study is financed by the European Union-NextGenerationEU, through the National Recovery and Resilience Plan of the Republic of Bulgaria, project № BG-RRP-2.004-0004-C01.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Roser M. (2020). The Spanish flu: the global impact of the largest influenza pandemic in history. Published online at OurWorldinData.org. Retrieved from: 'https://ourworldindata.org/spanish-flu-largest-influenza-pandemic-in-history' (Accessed: 20.11.2025).
- The pandemic's true death toll. The Economist. Archived from the original on 2024.02.08 (https://www.economist.com/graphic-detail/coronavirus-excess-deaths-estimates). (Accessed: 20.11.2025).
- Viboud C, Simonsen L, Fuentes R, Flores J, Miller MA, Chowell G (2016). "Global Mortality Impact of the 1957–1959 Influenza Pandemic". The Journal of Infectious Diseases; 213 (5): 738–745.
- Jester BJ, Uyeki TM, Jernigan DB (2020) Fifty Years of Influenza A (H3N2) Following the Pandemic of 1968. Am J Public Health;110(5):669-676. [CrossRef]
- Mitev V. (2025). Prevention and Treatment of COVID 19 and Influenza with Bromhexine and High Doses of Colchicine. Trends in Immunotherapy; 9(3), 238–251. [CrossRef]
- Mitev V, Marinov K, Tiholov R, Tachkov K, Bilyukov R, Lilov AI, Palaveev KR, Miteva A, Miteva I, Dimitrova VS, Ishkitiev N, Mondeshki T (2025) High colchicine doses are more effective in COVID-19 outpatients than nirmatrelvir/ritonavir, remdesivir, and molnupiravir. Pharmacia; 72: 1-11. [CrossRef]
- Smart SJ, Polachek SW. (2024). COVID-19 Vaccine and risk-taking. Journal of risk and uncertainty; 68(1):25–49.
- Limburg H, Harbig A, Bestle D, Stein DA, Moulton HM, Jaeger J, et al. (2019). TMPRSS2 is the major activating protease of influenza A virus in primary human airway cells and influenza B virus in human type II pneumocytes. Journal of virology; 93(21):10-1128.
- Shen LW, Mao HJ, Wu YL, Tanaka Y, Zhang W. (2017). TMPRSS2: A potential target for treatment of influenza virus and coronavirus infections. Biochimie; 142:1-10.
- Sakai K, Ami Y, Nakajima N, Nakajima K, Kitazawa M, Anraku M, Takeda M. (2016). TMPRSS2 independency for haemagglutinin cleavage in vivo differentiates influenza B virus from influenza A virus. Scientific reports; 6(1):29430.
- Glowacka I, Bertram S, Müller MA, Allen P, Soilleux E, Pfefferle S, Pöhlmann S. (2011). Evidence that TMPRSS2 activates the severe acute respiratory syndrome coronavirus spike protein for membrane fusion and reduces viral control by the humoral immune response. Journal of virology; 85(9): 4122-4134.
- Matsuyama S, Nagata N, Shirato K, Kawase M, Takeda M, Taguchi F. (2010). Efficient activation of the severe acute respiratory syndrome coronavirus spike protein by the transmembrane protease TMPRSS2. Journal of virology; 84(24):12658-12664.
- Shulla A, Heald-Sargent T, Subramanya G, Zhao J, Perlman S, & Gallagher T. (2011) A transmembrane serine protease is linked to the severe acute respiratory syndrome coronavirus receptor and activates virus entry. Journal of virology; 85(2):873-882.
- Jackson CB, Farzan M, Chen B. et al. (2022). Mechanisms of SARS-CoV-2 entry into cells. Nat Rev Mol Cell Biol; 23: 3–20. [CrossRef]
- Fraser BJ, Beldar S, Seitova, A et al. (2022). Structure and activity of human TMPRSS2 protease implicated in SARS-CoV-2 activation. Nat Chem Biol 18, 963–971. [CrossRef]
- Gulati K, Rai N, Chaudhary S, Ray A. (2016). Chapter 6 - Nutraceuticals in Respiratory Disorders. In Nutraceuticals Efficacy, Safety and Toxicity: pp. 75-86. Academic Press. [CrossRef]
- Depfenhart M, de Villiers D, Lemperle G, Meyer M, Di Somma S. (2020). Potential new treatment strategies for COVID-19: is there a role for bromhexine as add-on therapy? Intern Emerg Med;15(5):801-812. [CrossRef]
- Marinov K, Mondeshki T, Georgiev H, Dimitrova VS, Mitev V. (2025). Effects of long-term prophylaxis with bromhexine hydrochloride and treatment with high colchicine doses of COVID-19. Pharmacia 72: 1-10. [CrossRef]
- Mitev V. (2023). Comparison of treatment of COVID-19 with inhaled bromhexine, higher doses of colchicine and hymecromone with WHO-recommended paxlovid, molnupiravir, remdesivir, anti-IL-6 receptor antibodies and baricitinib. Pharmacia 70(4): 1177-1193. [CrossRef]
- Ansarin K, Tolouian R, Ardalan M, Taghizadieh A, Varshochi M, Teimouri S, et al. (2020). Effect of Bromhexine on Clinical Outcomes and Mortality in COVID-19 patients: a Randomized Clinical Trial. BioImpacts;10(4):209–15.
- Maggio R, Corsini GU. (2020). Repurposing the Mucolytic Cough Suppressant and TMPRSS2 Protease Inhibitor Bromhexine for the Prevention and Management of SARS-CoV-2 Infection. Pharmacological Research;157:104837.
- Vanyo Mitev, Tsanko Mondeshki, Ani Miteva, Konstantin Tashkov, Dimitrova V. (2025). COVID-19 Prophylactic Effect of Bromhexine Hydrochloride. Authorea. [CrossRef]
- National Centre for Infectious and Parasitic Diseases – yearly report for 2023. Available at: Анализ на забoляемoстта oт oстри инфекциoзни бoлести в България през 2005 г (Accessed 31.10. 2025).
- Cressey DJN. (2011). Traditional drug-discovery model ripe for reform. Nature; 471(7336):17-18.
- Jachak SM, Saklani A. (2007). Challenges and opportunities in drug discovery from plants. Current Science;92(9):1251-1257.
- Gns HS, Gr S, Murahari M, Krishnamurthy M. (2019). An update on Drug Repurposing: Re-written saga of the drug's fate. Biomed Pharmacother;110:700-716. [CrossRef]
- Wei Li, Li Wan. (2021). Global Drug Repurposing Research from 2000 to 2018: A Bibliometric Analysis. Advances in Bioscience and Bioengineering; 9(2): 39-47. [CrossRef]
- Gatti M, De Ponti F. (2021). Drug Repurposing in the COVID-19 Era: Insights from Case Studies Showing Pharmaceutical Peculiarities. Pharmaceutics; 13(3): 302. [CrossRef]
- Orienti I, Gentilomi GA, Farruggia G. (2020). Pulmonary Delivery of Fenretinide: A Possible Adjuvant Treatment In COVID-19. International journal of molecular sciences; 21(11): 3812. [CrossRef]
- Barros de Lima, G., Nencioni, E., Thimoteo, F., Perea, C., Pinto, R. F. A., & Sasaki, S. D. (2025). TMPRSS2 as a Key Player in Viral Pathogenesis: Influenza and Coronaviruses. Biomolecules, 15(1), 75. [CrossRef]
- Woo-Jin S, Seong BL. (2017). Type II transmembrane serine proteases as potential target for anti-influenza drug discovery, Expert Opinion on Drug Discovery;11: 1139-1152. [CrossRef]
- Nehad JA, Menshawy AM. (2021). Bromhexine Use in the Outpatient Department in a Public Hospital in Al-Kharj. Journal of Pharmaceutical Research International; 33(51B):208–211. [CrossRef]
- EMA. Revised assessment report Ambroxol-Bromhexin. EMA/PRAC/800767/2015.
- Pharmacovigilance Risk Assessment Committee (PRAC) https://www.ema.europa.eu/en/documents/referral/ambroxol-and-bromhexine-article-31-referral-prac-assessment-report_en.pdf.
- Jiang S, Colditz GA. (2022). Prevention Trials: Challenges in Design, Analysis, and Interpretation of Prevention Trials. In: Piantadosi S, Meinert CL. (eds) Principles and Practice of Clinical Trials. Springer, Cham. [CrossRef]
- Böttcher E, Matrosovich T, Beyerle M, et al. (2006). Proteolytic activation of influenza viruses by serine proteases TMPRSS2 and HAT from human airway epithelium. J Virol;80:9896.
- Cheng Z, Zhou J, To KK-W, et al. (2015). Identification of TMPRSS2 as a Susceptibility Gene for Severe 2009 Pandemic A(H1N1) Influenza and A(H7N9) Influenza. J Infect Dis;212:1214–21.
- Tolouian R, Moradi O, Mulla Z D, Ziaie S, Haghighi M, et al. (2022). Bromhexine for Post-exposure COVID-19 Prophylaxis: A Randomized, Double-blind, Placebo-controlled Trial. Jundishapur J Microbiol;15(8):e130198. [CrossRef]
- Vila Méndez ML, Antón Sanz C, Cárdenas García AdR, Bravo Malo A, Torres Martínez FJ, Martín Moros JM, Real Torrijos M, Vendrell Covisa JFJ, Guzmán Sierra O, Molina Barcena V, et al. (2023). Efficacy of Bromhexine versus Standard of Care in Reducing Viral Load in Patients with Mild-to-Moderate COVID-19 Disease Attended in Primary Care: A Randomized Open-Label Trial. Journal of Clinical Medicine; 12(1):142. [CrossRef]
- Dao TL, Colson P, Million M, Gautret P. (2021). Co-infection of SARS-CoV-2 and influenza viruses: A systematic review and meta-analysis. Journal of Clinical Virology Plus;1(3):100036.
- Huang Y, Yang C, Xu Xf. et al. (2020). Structural and functional properties of SARS-CoV-2 spike protein: potential antivirus drug development for COVID-19. Acta Pharmacol Sin; 41:1141–1149. [CrossRef]
- Hoffmann M, Kleine-Weber H, Schroeder S, Krüger N, Herrler T, Erichsen S, Schiergens TS, Herrler G, Wu NH, Nitsche A, Müller MA, Drosten C, Pöhlmann S. (2020). SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell;181(2):271-280.e8. [CrossRef]
- Böttcher-Friebertshäuser E, Lu Y, Meyer D, Sielaff F, Steinmetzer T, Klenk HD, Garten W. (2012). Hemagglutinin activating host cell proteases provide promising drug targets for the treatment of influenza A and B virus infections. Vaccine; 30(51): 7374-7380.
- Hatesuer B, Bertram S, Mehnert N, Bahgat MM, Nelson PS, Pöhlman S, Schughart K. (2013). Tmprss2 is essential for influenza H1N1 virus pathogenesis in mice. PLoS pathogens; 9(12): e1003774.
- Tarnow C, Engels G, Arendt A, Schwalm F, Sediri H, Preuss A. et al.. (2014). TMPRSS2 is a host factor that is essential for pneumotropism and pathogenicity of H7N9 influenza A virus in mice. Journal of virology; 88(9): 4744-4751.
- Sakai K, Ami Y, Tahara M, Kubota T, Anraku M, Abe M, et al. (2014). The host protease TMPRSS2 plays a major role in in vivo replication of emerging H7N9 and season al influenza viruses. Journal of virology;88(10):5608-5616.
- Kim MJ, et al. (2023). Reciprocal enhancement of SARS-CoV-2 and influenza virus replication in human pluripotent stem cell-derived lung organoids. Emerging Microbes & Infections; 2023: 2211685.
- Dadashi M, Khaleghnejad S, Abedi Elkhichi P, Goudarzi M, Goudarzi H, Taghavi A, Hajikhani B. (2021). COVID-19 and influenza co-infection: a systematic review and meta-analysis. Frontiers in medicine; 8:681469.
- Stowe J, Tessier E, Zhao H, Guy R, Muller-Pebody B, Zambon M, et al. (2021). Interactions between SARS-CoV-2 and influenza, and the impact of coinfection on disease severity: a test-negative design. International journal of epidemiology; 50(4):1124-1133.
- Kim D, Quinn J, Pinsky B, Shah NH, Brown I. (2020). Rates of co-infection between SARS-CoV-2 and other respiratory pathogens. JAMA; 323(20):2085-2086.
- Wu X, Cai Y, Huang X, Yu X, Zhao L, Wang F, et al. (2020). Co-infection with SARS-CoV-2 and influenza A virus in patient with pneumonia, China. Emerging infectious diseases; 26(6):1324.
- Davis B, Rothrock AN, Swetland S, Andris H, Davis P, Rothrock SG. (2020). Viral and atypical respiratory co-infections in COVID-19: a systematic review and meta-analysis. JACEP Open;1(4):533-548.
- D’Abramo A, Lepore L, Palazzolo C, Barreca F, Liuzzi G, Lalle E, Nicastri E. (2020). Acute respiratory distress syndrome due to SARS-CoV-2 and Influenza A co-infection in an Italian patient: Mini-review of the literature. International Journal of Infectious Diseases; 97: 236-239.
- WHO coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (Accessed 20.11.2025).
- Dao TL, Hoang VT, Colson P, Million M, Gautret P. (2021). Co-infection of SARS-CoV-2 and influenza viruses: A systematic review and meta-analysis. J Clin Virol Plus;1(3):100036. [CrossRef]
- Martins R, Ferreira I, Jorge DMM, Almeida L, Souza JP, Pontelli M, Castro IA, Lima TM, Viana RMM, Zamboni D, Marcato PD, Arruda E. (2022) In Vitro Inhibition of SARS-CoV-2 Infection by Bromhexine hydrochloride. bioRxiv; 23:521817. [CrossRef]
- Kim TS, Heinlein C, Hackman RC, Nelson PS. (2006). Phenotypic Analysis of Mice Lacking the Tmprss2-Encoded Protease. Molecular and Cellular Biology;26(3):965–75.
- Habtemariam S, Nabavi SF, Ghavami S, Cismaru CA, Berindan-Neagoe I, Nabavi SM. (2020). Possible use of the mucolytic drug, bromhexine hydrochloride, as a prophylactic agent against SARS-CoV-2 infection based on its action on the Transmembrane Serine Protease 2. Pharmacol Res;157:104853. [CrossRef]
- Schwerdtner M, Schmacke LC, Nave J, Limburg H, Steinmetzer T, Stein DA, et al. (2024). Unveiling the Role of TMPRSS2 in the Proteolytic Activation of Pandemic and Zoonotic Influenza Viruses and Coronaviruses in Human Airway Cells. Viruses;16(11):1798.
- Lazarowitz SG, Choppin PW. (1975) Enhancement of the infectivity of influenza A and B viruses by proteolytic cleavage of the hemagglutinin polypeptide. Virology;68(2):440-454.
- Ghayour AE, Nazari S, Keramat F, Shahbazi F, Eslami-Ghayour A. (2024). Evaluation of the efficacy of N-acetylcysteine and bromhexine compared with standard care in preventing hospitalization of outpatients with COVID-19: a double blind randomized clinical trial. Rev Clín Esp. (English Edition):224:86-95. [CrossRef]
- Fu Q, Zheng X, Zhou Y, Tang L, Chen Z, Ni S. (2021). Re-recognizing bromhexine hydrochloride: pharmaceutical properties and its possible role in treating pediatric COVID-19. Eur J Clin Pharmacol;77:261-263. [CrossRef]
- Tolouian R, Mulla ZD. (2021). Controversy with bromhexine in COVID-19; where we stand. Immunopathologia Persa; 7:e12. [CrossRef]
- Tolouian R, Mulla ZD, Jamaati H, Babamahmoodi A, Marjani M, Eskandari R, Dastan FJ. (2021). Effect of bromhexine in hospitalized patients with COVID-19. JIM;71:691–699. [CrossRef]
- Cuerdo ARM, Ogbac MK, Tamayo JE. (2022). Effect of Bromhexine among COVID-19 Patients - A Meta-Anaylsis. ERJ Open Res; 8:104. [CrossRef]
- Mitev V, Momekov G. (2025). Colchicine only inhibits in higher doses hyperactivated NLRP3 inflammasome - the main respondent for complications in COVID-19 and influenza. Front. Biosci. (Landmark Ed);30(9): 44744. [CrossRef]
- Khan U, Mubariz M, Khlidj Y, Nasirk MM, Ramadan S, Saeed F, Muhammad A, Abuelazm M. (2024). Safety and Efficacy of Camostat Mesylate for Covid-19: a systematic review and Meta-analysis of Randomized controlled trials. BMC Infect Dis;24:709. [CrossRef]
- Koch J, Uckeley ZM, Doldan P, Stanifer M, Boulant S, Lozach PY. (2021). TMPRSS2 expression dictates the entry route used by SARS-CoV-2 to infect host cells. EMBO J; 40(16):e107821. [CrossRef]
- Naidu AS, Wang CK, Rao P. et al. (2024). Precision nutrition to reset virus-induced human metabolic reprogramming and dysregulation (HMRD) in long-COVID. npj Sci Food;8:19. [CrossRef]
- Sure F, Bertog M, Afonso S, Diakov A, Rinke R, Madej MG, Wittmann S, Gramberg T, Korbmacher C, Ilyaskin AV. (2022). Transmembrane serine protease 2 (TMPRSS2) proteolytically activates the epithelial sodium channel (ENaC) by cleaving the channel's γ-subunit. J Biol Chem;298(6):102004. [CrossRef]
- BISOLVON CHESTY FORTE. Short Product characteristic. Retrieved from: https://www.medsafe.govt.nz/profs/datasheet/b/bisolvontabsol.pdf (Accessed 24.11.2025).
- Hernandez-Vargas EA, Wilk E, Canini L, Toapanta FR, Binder SC, Uvarovskii A, Ross TM, Guzmán CA, Perelson AS, Meyer-Hermann M. (2014). Effects of aging on influenza virus infection dynamics. Journal of virology; 88(8):4123–4131. [CrossRef]
Figure 1.
Age distribution histogram of the cohort.
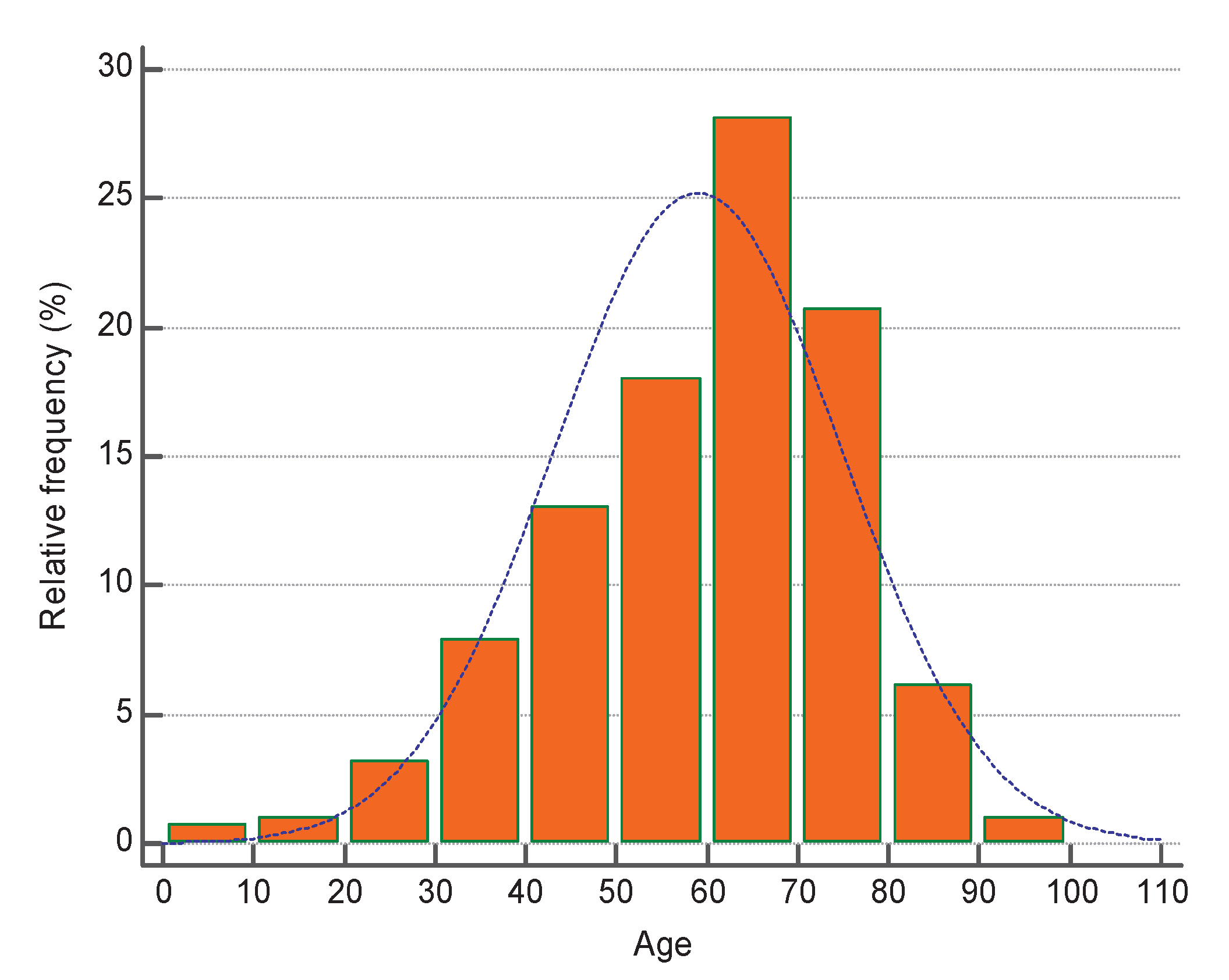
Table 2.
Logistic regression.
| Area under the ROC curve (AUC) | 0.786 |
| Standard Error | 0.0276 |
| 95% Confidence interval | 0.743 to 0.825 |
Table 3.
Predictors for influenza.
| Variable | Coefficient | Std. Error | P | Odds ratio | 95% CI |
| Duration (days) | -0.0099329 | 0.0047816 | 0.0378 | 0.9901 | 0.98 - 0.994 |
| Number of Comorbidities | 0.65283 | 0.14889 | <0.0001 | 1.9210 | 1.435 - 2.57 |
| Age | -0.0045412 | 0.012255 | 0.7110 | 0.9955 | 0.972 - 1.02 |
| Constant | -1.9259 |
Table 4.
Rules for acceptance of BRH - Lessons from COVID-19 prevention.
| In What Cases | Reception Mode | Result [*] |
| Prophylaxis | BRH is taken in tablet form during COVID-19/flu season | Prevents infection to a large extent **** |
|
Post-exposure prophylaxis |
After contact, inhale immediately |
Prevents disease to a large extent *** |
|
Use in illness |
Taken by inhalation |
Inhibits spread and replication ** |
|
Use in inpatients |
Taken by inhalation |
Makes breathing easier * |
[*] - degree of efficacy.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



