
Submitted:
22 November 2025
Posted:
27 November 2025
You are already at the latest version
Abstract
Introduction: Presbyopia is a refractive condition characterized by progressive loss of accommodation resulting in loss of visual acuity and is known to affect quality of life. Mainstay treatment modalities for presbyopia include reading spectacles, contact lenses, and a series of surgical techniques. Until recently, pharmacologic treatments were not available. In this paper, we aim to review the role of pilocarpine eye drops in managing presbyopia. Methods: A comprehensive literature search was performed using Medline, EMBASE, and grey literature databases for articles until 01 May 2023. Search terms included “presbyopia”, “presbyopia correction/treatment”, “pilocarpine”, and “pharmacological presbyopia treatment”. All relevant articles from 01 January 2005 to 01 May 2023 and written in the English language were included in the review. Results: The initial search yielded 497 publications, of which 17 met our inclusion criteria and were included in analysis. Pilocarpine, a parasympathomimetic drug, increases the power of accommodation by increasing the lens thickness via the muscarinic receptors on the iris and ciliary muscles. Clinical trials utilizing pilocarpine eye drops in the management of presbyopia have reported positive outcomes in terms of near visual acuity. Pilocarpine HCL ophthalmic 1.25% formulation (Vuity) is currently the only approved pharmacologic treatment option for presbyopia shown to be effective in managing presbyopia. Conclusion: Overall, pilocarpine eye drops appear to be an effective option in improving near visual acuity in presbyopia patients. Long term follow-up data on the use of pilocarpine-based eye drops is not available. With the increase in the number of users overtime following the approval of Vuity, the long-term effects of its prolonged use may be determined. Further research is needed to optimize the concentrations and combinations of pilocarpine and other substances to maximize efficacy and minimize adverse effects.
Keywords:
presbyopia
; pilocarpine
; accommodation
; Vuity
Introduction
Presbyopia is a refractive condition characterized by the progressive loss of accommodation, resulting in an inability to focus on near and distant objects.[1] It affects individuals over the age of 40, with an estimated 25% of the global population, around 1.8 billion people, being affected.[2] Given the increasing world population and the proportionate rise in the elderly population, presbyopia is expected to become one of the most prevalent visual concerns of the 21st century.[1,3]
Treatment options for presbyopia have primarily centred around reading spectacles, contact lenses, and various surgical techniques. Conventional, bifocal, or progressive spectacles can achieve optical correction for presbyopia, but they have limitations such as inadequate vision at intermediate or close distances and the need to align the visual axes in a specific direction for clear near vision.[4] Contact lenses offer an alternative, but age-related changes in the eyes can influence their success, and proper care and hygiene are necessary.[5] Surgical management of presbyopia includes laser ablation techniques like PresbyLASIK, which create multifocality in the cornea, laser ablation with monovision refractive outcomes, and implantable inlays that alter corneal shape to enhance refractive power and near vision.[2] Refractive lens exchange with intraocular lens implants, such as multifocal and trifocal IOLs, can improve both near and distance vision. However, surgical techniques carry various risks depending on the type of surgical procedure and these can include corneal scarring and haze, visual disturbances noted by patient such as glare, halos, and an increased risk of dissatisfaction with presbyopia management outcomes. Many patients still require spectacle corrections postoperatively despite best surgical outcomes.
Pilocarpine, a cholinergic muscarinic receptor agonist, was initially approved by the FDA in 1974 for the treatment of elevated intraocular pressure and glaucoma.[2] Recently, it has been investigated as a potential treatment for presbyopia. Accommodation, the ability to focus on near objects, is driven by parasympathetic stimulation of muscarinic receptors in the iris sphincter muscle and ciliary body, resulting in pupil constriction and ciliary muscle contraction.[2] Topical application of pilocarpine leads to significant shallowing of the anterior chamber depth and thickening of the lens. Studies have shown that pilocarpine administration causes anterior chamber shallowing in elderly individuals, indicating its potential as a non-invasive treatment for presbyopia in this population.[6]
Finding the ideal miotic agent for treating presbyopia involves balancing pupil constriction and ciliary muscle contraction. Pilocarpine can induce these effects, but excessive contraction can impair lens flexibility and distant vision.[2,7] Combining non-steroidal anti-inflammatory drugs (NSAIDs) with pilocarpine reduces the intensity of pupil and ciliary muscle contraction, allowing the lens to adjust for clear vision at all distances.[8] This combination also helps prevent inflammation associated with prolonged pilocarpine use, which can lead to issues such as a fixed pupil, posterior synechiae, and pigment dispersion. Studies have examined other combination with pilocarpine including oxymetazoline, brimonidine, and carbachol.
Pilocarpine-containing eye drops have emerged as a pharmacological treatment for presbyopia, particularly since many patients were left with unsatisfied needs, for whom surgical management was not feasible or inadequate. The efficacy of these eye drops in improving vision has been demonstrated in various studies. VUITY (pilocarpine HCl ophthalmic solution) 1.25% is the first and currently the only FDA-approved eyedrop for treating presbyopia with more concentrated forms such as 2% formulation are usually used for managing glaucoma. A literature review was conducted to investigate the role of pilocarpine eye drops in the management of presbyopia.
Material & Methods
Search Strategy
A literature search for articles relevant to the use of pilocarpine in managing presbyopia was performed using PubMed, EMBASE, and grey literature databases between 01 January 2005 to 01 May 2023. Search terms “presbyopia”, “presbyopia correction/treatment”, “pilocarpine”, and “pharmacological presbyopia treatment” were used. Also, we performed a Google scholar search of the reference list of the included papers to identify further relevant studies. Relevant papers were selected, analyzed, and eventually included in our literature review.
Data Selection/Eligibility and Exclusion Criteria
The initial search identified studies including, observational studies, review articles, survey reports, book chapters, case reports, and original randomized trials. Two reviewers (K.A. and K.G.) independently screened search results for title, abstract, and full-text screening. Studies that were written in English and primarily focused on the use of Pilocarpine eye drops for the treatment of Presbyopia were included in the review.
Research items that were not written in English and did not focus on the use of Pilocarpine eye drops were excluded from this review. Duplicate publications, editorials, blogs, newspapers, news articles, and newsletters were also excluded from our review. Out of the published papers examined, 17 met our inclusion criteria and were included in our review.
Analysis Process
This paper provides a review of research items examining the use of pilocarpine in the pharmacological management of presbyopia. Research items not focusing on pilocarpine were not included in the review. The included research items in this paper were summarized to delineate the composition, results namely visual acuity improvement, and reported effects of pilocarpine eye drops. The included research items were summarized in a table. Studies were also critically reviewed to create an overview and guidance for further research.
Results
Literature Search
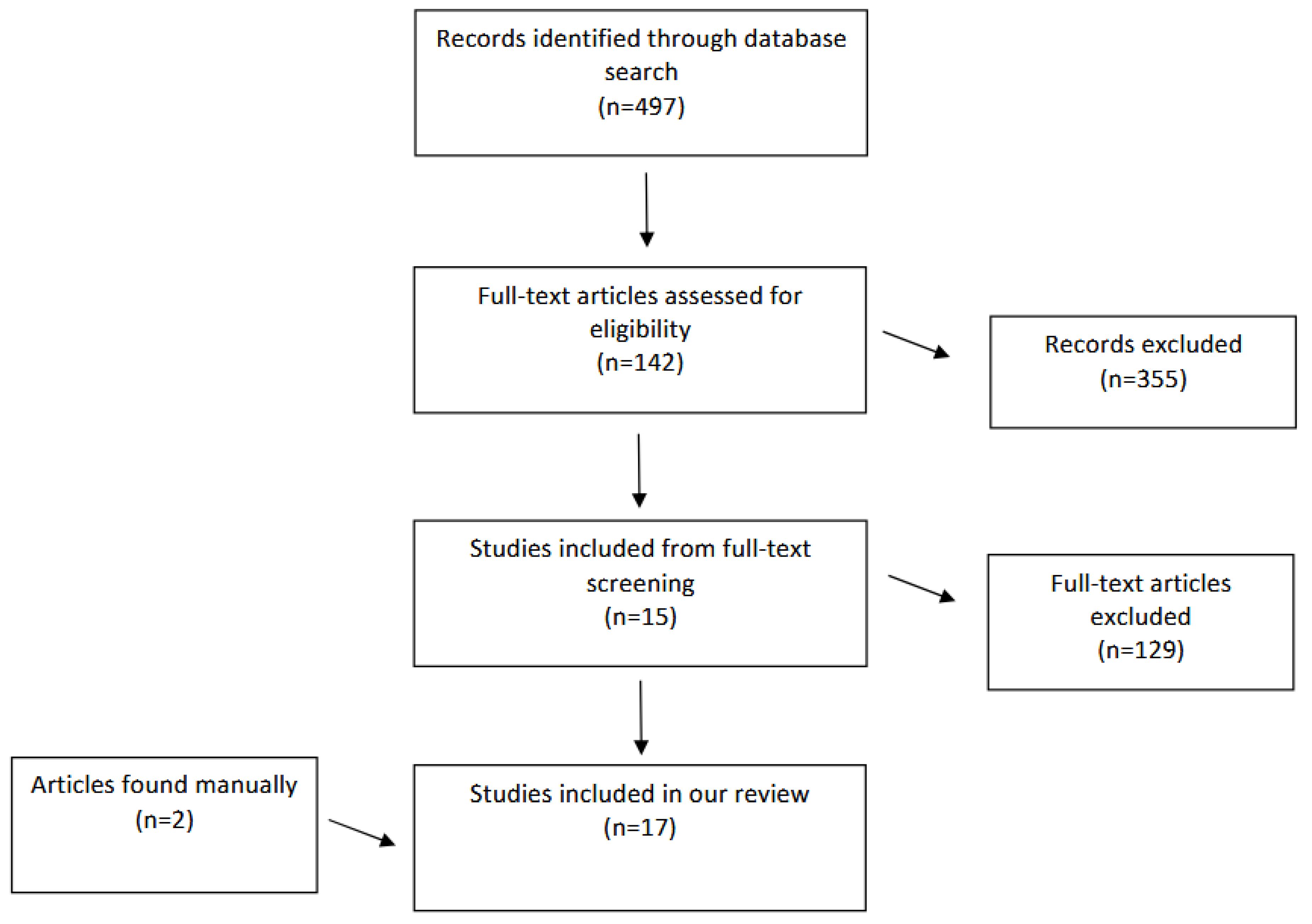
Our search algorithm, “pilocarpine AND (presbyopia OR presbyopia treatment OR presbyopia correction OR pharmacological presbyopia treatment)” yielded 497 publications. Screening of the titles and abstracts by 2 review authors (K.A and K.G.) resulted in the removal of 355 items. The remaining 142 citations underwent a second round of screening of the full text by 2 authors (K.A and K.G.) which resulted in the removal of 129 citations. A total of 15 articles met the inclusion criteria and were included in our review. Two more article was later included in our review via manually looking into the reference lists of all included articles using Google Scholar. A total of 17 papers were included in our analysis. The study selection flow diagram (Figure 1) depicts our research.
Characteristics of Included Studies
Out of the 17 papers included in our review, 4 were non-randomized prospective studies, 7 were randomized control trials, and 6 were case reports/series. All papers examined the use of different composition of eye drops containing different concentration of pilocarpine. Two of the 4 prospective studies examined specialized formulation of pilocarpine named “FOV” tears which is a combination of 0.247% pilocarpine and phenylephrine and “Vuity” which is a formulation of 1.25% pilocarpine. All these studied reported improvement in near vision with minor side effects. Two of the 7 randomized control trials included are phase 2 and two studies are phase 3 clinical trials. Three of the trials did not indicate the phase. One of the trials included a short-term study of 163 participants and an extended study of 151 participants. Three studies were case series, and 3 others were case reports. These studies report improvement in near vision following administration of different formulations of pilocarpine. Two of the case reports describe cases of retinal detachment following pilocarpine administration while one reports a case of vitreomacular traction.
Overall, pilot studies of pilocarpine eye drops demonstrated good tolerance in terms of side effects. Clinical trials revealed a notable improvement in near visual acuity (VA), with a percentage of patients showing improvement ranging from 70.6% to 92.3%. The most reported adverse events were minor ocular discomfort (1-30%) and headache (10-28.1%) in the studied population. Several studies reported on pseudophakic status and improvement in VA. However, the combination of pilocarpine and oxymetazoline was not found to be useful. On the other hand, pilocarpine in combination with NSAIDs showed promising improvement in the management of presbyopia.

Table 1.
Characteristics of the 17 articles included in this review used to investigate the role of pilocarpine eye drops in the management of presbyopia. (NVA; near visual acuity, J; Jaeger).
Table 1.
Characteristics of the 17 articles included in this review used to investigate the role of pilocarpine eye drops in the management of presbyopia. (NVA; near visual acuity, J; Jaeger).
| Studies (year) | Study type | Intervention | Study participants | Results | Adverse effects | Notes | ||
|---|---|---|---|---|---|---|---|---|
| NVA Improvement | % showing improvement | Mean pupil size | ||||||
| Kaufman[9] (2012) | Non-randomized prospective study | Pilocarpine 1% Carbachol 3% Brimonidine 0.2% Placebo (artificial tear) |
12 patients with presbyopia |
Pilocarpine alone: Improvement by 2.3J lines Pilocarpine with brimonidine: Improvement by 3J lines Carbachol: Improvement by 6.3J lines. Carbachol with brimonidine: Improvement by 6.3J lines. |
Minor ocular discomfort by 10-30% of patients including the placebo group | |||
| Benozzi et al[10] (2012) | Non-randomized prospective study | Pilocarpine 1% Diclofenac 0.1% |
100 patients with presbyopia aged 45-50 years | Improvement to J1 | 1% of patients complained of ocular burning and discomfort | The improvement in NVA was maintained for a period of 5 years | ||
| Allergan pharmaceutical[11] (2015) | Phase 2 randomized clinical trial | Pilocarpine (AGN-190584) Oxymetazoline (AGN-199201) |
65 patients with presbyopia with a mean age of 49.2 years | At least 2 lines improvement | In 70.6% of patients using AGN-190584, and 46.7% in patients using AGN-199201. | Eyelid retraction was seen in 26% of patients using oxymetazoline alone. | ||
| Krader and Feinbaum[12] (2015) | Case series | PresbiDrops (pilocarpine (0.247%) | 81 patients with presbyopia in the age group of 42-74 years | Improvement from 0.3J to 0.6J lines. | After treatment with 2 drops, the diameter decreased significantly from 3.77 mm to 2.63 mm. | No serious adverse reactions. 4 patients experience nausea, headache each which spontaneously resolved | ||
| Abdelkader[13] (2015) |
A prospective, double-masked, randomized, placebo-controlled clinical trial | Carbachol 2.25% Brimonidine 0.2% |
48 patients with presbyopia aged between 43 and 56 years | Improvement in all subjects who received carbachol plus brimonidine drops (p < 0.0001) In the >= 50-year-old group, improved significantly from 7.68J to 4.75J at 8 hr (p < 0.0001) In the < 50-year-old group, improved significantly from 6.29J to 4.64J at 8 hr (p < 0.0001) |
In the >=50-year-old group, decreased significantly from 4.77±0.47 mm to 3.48±0.36 mm at 8 hr (P<0.0001) In the < 50-year-old group, decreased significantly from 4.72±0.51 mm to 3.42±0.48 mm at 8 hr (P<0.0001), |
Mild burning (3.3%) in 1 subject Headache (10%) Low luminosity (3.3%) in 1 subject |
||
| Abdelkader and Kaufman[14] (2016) |
A prospective, double-masked, randomized, controlled clinical trial | Carbachol 3% Brimonidine 0.2% |
10 patients with presbyopia aged between 42 and 58 years | Statistically significant improvement was achieved in all subjects who received combined 3% carbachol and 0.2% brimonidine compared with those who received separate forms of carbachol alone or brimonidine alone (P < 0.0001) Improved from 8.6J ± 1.5 before treatment to 2.3J ± 0.5 at 8 h post-treatment (P<0.01) |
Decreased significantly from 4.3 ± 0.5 mm to 2.1 ± 0.3 mm at 8 h post-treatment (P < 0.0001). | None reported | ||
| Abdelkader[15] (2018) |
A prospective, double-masked, randomized, placebo-controlled clinical trial | Carbachol 3% Brimonidine 0.2% |
40 pseudophakic patients with presbyopia aged between 30 and 80 years | In the treatment group, improved significantly from 7.5J ± 1 before treatment to 2.35J ± 0.49 at 8 hours posttreatment (p < 0.0001) | Dropped significantly from 4.1 ± 0.5 mm to 2.5 ± 0.4 mm at eight hours following drops (p < 0.0001). |
None reported | ||
| Vargas et al[16] (2019) | Consecutive, non-randomized, interventional clinical study | FOV Tears: pilocarpine (0.247%) phenylephrine (0.78%) polyethylene glycol (0.09%) nepafenac (0.023%) pheniramine (0.034%) naphazoline (0.003%) |
117 presbyopia patients in the age group of 41 to 60 years were recruited | Improved from 0.35 LogMAR to 0.16 LogMAR at 2 h after use of the eye drop (p = 0.000) | 92.3% of patients |
Decreased significantly under photopic conditions (p = 0.001), from 3.3 mm to 3.05 mm at 2 h after treatment. Also decrease significantly under scotopic conditions (p = 0.000), from 4.9 mm to 3.9 mm at 2 h after treatment |
14 patients (11.9%) complained of headache | |
| Benozzi et al[17] (2021) | Non-randomized case-series retrospective study | Patented formulation: pilocarpine and diclofenac preservative-free eye drops (Benozzi method; US 8.524.758 B2- EP1.938.839 B1) | 148 patients, aged 40 to 60. | At baseline, the NVA for the different groups were between 3J and 8J which was improved to 1J to 2J. | Decrease in light perception (24.6%) Headaches (11.3%) Ocular surface burning (6.6%) Side effects were spontaneously resolved. |
|||
| Price et al[18] (2021) | Two concurrent Phase 2, double-masked, randomized, vehicle-controlled studies, 1 short-term and 1 extended study |
Various concentrations and combinations of Pilocarpine (0%, 0.5% 1.0%, and 1.5%) and oxymetazoline (0%, 0.0125%, 0.05%, and 0.125%). | 163 presbyopia patients were recruited in the short-term study and 151 patients in the extended study. Mean age 48.6 years. | In the short and extended term studies, pilocarpine produced a significant dose response in the average increase of letters (P <0.001). |
All treatment groups had a reduction in diameter | The most common adverse event was headache (<5% when Pilo was dosed alone in the short-term study; up to 28.1% in the High OU group of the extended study) |
A dose response was seen as early as 15 minutes post administration, with peak effect at 1 hour. Peak improvement increased from day 1 to day 14 and was maintained up to day 28. | |
| Waring et al[19] (2022) | Vehicle-controlled, participant- and investigator-masked, randomized, Phase 3 clinical study, GEMINI 1 | AGN-190584, an optimized topical formulation of pilocarpine 1.25% (Vuity) or AGN-190584 formulation vehicle | Individuals with presbyopia, aged 40 to 55. 163 randomized to treatment. 160 randomized to vehicle | The proportion of participants with improvement of 3 or more lines was statistically significantly higher with AGN-190584 treatment compared with vehicle on day 30. | The most common adverse event was headache (23% in treatment group), followed by visual impairment (7% in treatment group). | |||
| Jackson et al[20] (2022) | In Vitro and Clinical Pilot Study | Pilocarpine 1.25% in the proprietary vehicle (Vuity) and a generic 1% Pilocarpine | 5 presbyopia patients aged 26 to 56. | 1 adverse event of brow ache was reported in the Optimized Formulation with 1.25% pilocarpine while 8 adverse events including eye pressure/pain, brow ache, vision blur, stinging, itching, and light sensitivity was reported in the Generic Formulation with 1% pilocarpine. | This study primarily assessed the side effects of the Optimized Formulation compared to Generic. | |||
| Eton et al[21] (2022) | Case Report | Pilocarpine 1.25% | 74 and 68 year old men with pre-existing retinal detachment risk factors | Unilateral retinal detachment occurring within 10 days of initiation of pilocarpine for treatment of presbyopia. | ||||
| Amarikwa et al[22] (2022) | Case Report | Pilocarpine 1.25% | 65 year old woman | Developed vitreomacular traction immediately following first administration of pilocarpine. Follow-up: The associated structural changes and scotoma persisted at follow-up, four weeks later. |
||||
| Al-Khersan et al[23] (2022) | Case Report | Pilocarpine 1.25% | 47 and 46 year old men | 47 year old: Bilateral Retinal detachment following 1 month of pilocarpine 1.25% drop use for presbyopia treatment. 46 year old: Unilateral Retinal detachment following 5 weeks of pilocarpine 1.25% drop use for presbyopia treatment. |
||||
| Vejarano et al[24] (2023) | Case series | FOV Tears: pilocarpine (0.247%) phenylephrine (0.78%) polyethylene glycol (0.09%) nepafenac (0.023%) pheniramine (0.034%) naphazoline (0.003%) |
363 participants with presbyopia aged 40-70 | Mean spherical equivalent (SE) changed significantly (− 0.17 Diopters) after instillation of the FOV Tears formulation (p < 0.001). logMAR NVA improved significantly by nearly two lines (p < 0.01). |
Diameter of the scotopic pupil decreased significantly by 0.97 ± 0.98 mm (p < 0.001) Diameter of the photopic pupil decreased by a non-significant amount (0.07 ± 0.69 mm). |
None mentioned | ||
| Kannarr et al[25] (2023) | Randomized (1:1), vehicle-controlled, double-masked, multicenter, phase 3 study, VIRGO |
Pilocarpine 1.25% (in AGN-190584 vehicle; Vuity) | Individuals with presbyopia, aged 40 to 55. 114 randomized to treatment. 116 randomized to vehicle | The proportion of participants who gained ≥3 lines in NVA on Day 14 was significantly greater with pilocarpine HCl 1.25% BID than vehicle. |
Pilocarpine HCl 1.25% twice daily significantly reduced pupil diameter in nondominant eyes under mesopic conditions (≥1.23 mm) compared to vehicle ( ≤0.08 mm) across all post-dose time points at all visits | Most common adverse reactions reported in >5% of participants were headache and eye irritation | ||
Discussion
Presbyopia is a common eye condition primarily affecting individuals over the age of 40 but can impact people of all age groups. Uncorrected refractive errors are a leading cause of visual impairment and rank second as the cause of blindness in developing nations.[26] Recent studies have examined the effects of managing presbyopia using pilocarpine eye drops, revealing excellent outcomes without significant adverse effects. This pharmacological treatment appears to provide adequate near vision without the need for glasses, particularly for individuals with emmetropia and presbyopia, between the ages of 40 and 60. Surgical options, including corneal refractive procedures and various intraocular lens (IOL) options, offer potential alternatives to glasses, benefiting patients with presbyopia. However, certain limitations restrict the recommendation of these procedures for patients without cataracts and with low refractive error. This age group, typically ranging from 40 to 60 years old, often experiences dissatisfaction with their visual acuity due to the natural decline in accommodation ability with aging.[26,27] As a result, non-surgical approaches utilizing pharmacological eye drops are gaining traction for managing presbyopia among this demographic.
Numerous studies have explored the effectiveness of pilocarpine alone or in combination with other substances for treating presbyopia. Clinical trials evaluated different concentrations of pilocarpine, along with brimonidine, carbachol, diclofenac, phenylephrine, polyethylene glycol, nepafenac, pheniramine, and naphazoline. These investigations sought to enhance near vision and achieve freedom from glasses for patients with presbyopia. The outcomes of these studies have consistently demonstrated positive results, showing significant improvements in visual acuity and depth of focus.
Pilocarpine Formulations and Use of NSAIDs
In the reviewed studies, various formulations of pilocarpine were utilized, including eye drops containing pilocarpine alone or in combination with other substances such as NSAIDs. Some studies also employed patented formulations or proprietary vehicles to improve the effectiveness and tolerability of pilocarpine. These formulations have demonstrated promising outcomes, with fewer adverse events compared to generic formulations.
For instance, Kaufman (2012) compared different concentrations of pilocarpine and brimonidine, pilocarpine alone, and carbachol with or without brimonidine to a placebo.[9] The findings indicate that 1% pilocarpine was the optimal concentration for enhancing near vision. Similarly, Benozzi et al (2012) reported that combining pilocarpine 1% with diclofenac 0.1% restored near vision without causing blurring or inflammation.[10] The addition of NSAIDs alongside pilocarpine was found to enhance the effects of the parasympathomimetic agent by inhibiting prostaglandin synthesis in the anterior uvea.[10] Benozzi et al (2021) also investigated a patented formulation of preservative-free eye drops containing pilocarpine and diclofenac.[17] The recommended dosing regimen involved twice-daily administration, once in the morning upon waking up and again 6 hours later. The study demonstrated a significant improvement in near visual acuity (NVA), although some uncomfortable symptoms like headaches, decreased light perception, and mild burning were reported. In a prospective clinical study conducted by Vargus et al (2019), a combination of pilocarpine 0.247%, phenylephrine 0.78%, polyethylene glycol 0.09%, nepafenac 0.023%, pheniramine 0.034%, and naphazoline 0.003% was used.[16] This formulation, known as FOV Tears, demonstrated improvements in near vision by one or more lines in 92.3% of the 117 presbyopia patients at 2 hours following instillation. Being a case series, its results are limited in their generalizability, and an RCT is required to compare it to placebo, while considering the study's sponsorship by the FOV Tears formulation manufacturers.
Furthermore, Allergan Pharmaceuticals compared low-dose pilocarpine, oxymetazoline, and a combination of both in patients, with pilocarpine exhibiting higher efficacy.[11] Oxymetazoline's vasoconstrictive effect through its α-adrenergic agonistic action led to mydriasis by acting on the iris dilator muscles, thereby reducing the depth of focus and undesired effects in presbyopia treatment. [11] The use of oxymetazoline was likely aimed at mitigating the adverse effects caused by pilocarpine, such as hyperemia, or prolonging the retention of pilocarpine in the eye for slow systemic absorption. Price et al (2021) conducted two Phase 2 studies using different concentrations and combinations of pilocarpine (ranging from 0% to 1.5%) and oxymetazoline (ranging from 0% to 0.125%).[18] The results revealed a notable dose response of pilocarpine in improving NVA, with the optimal concentration range identified between 1.16% and 1.32%. The studies did not show any evidence that oxymetazoline improved outcomes or tolerance and are therefore not recommended in the formulations. Headaches were the most common adverse event, particularly in the high-dose group of the extended study. These findings led to the development of AGN-190584 (Vuity), which employed an optimized concentration of pilocarpine HCl (1.25%) using a proprietary formulation. Subsequently, Phase 3 studies, GEMINI I and II, evaluated its efficacy.
In four of the discussed studies, NSAIDs were combined with parasympathomimetic drugs: diclofenac 0.1% was used in two studies[10,17], and nepafenac 0.023% in the other two.[16,24] Muscarinic stimulation of the anterior uveal tract with parasympathomimetic drops like pilocarpine and carbachol can lead to chronic inflammation, fixed pupil stimulation, posterior synechiae, spasmodic contractions of the iris, pigment dispersion, and myopic shift.[28] Consequently, nonsteroidal anti-inflammatory drugs (NSAIDs) are combined with miotics because NSAIDs have been reported to inhibit cyclooxygenase activity and act as anti-inflammatory agents in the anterior uveal tract, reducing mitosis, spasmodic ciliary contractions, pigment dispersion, and posterior synechiae.[29] Interestingly, none of the mentioned trials, even those without NSAIDs, reported side effects associated with stimulation of the anterior uveal tract. Thus, further evidence is needed to clinically justify the use of NSAIDs alongside pilocarpine.
The variety of combinations and concentrations used underscores the ongoing efforts to optimize the management of presbyopia. However, the limited number of trials exploring specific combinations and the lack of consistent reported results necessitate further research and validation.
Near Visual Acuity Improvements
The primary objective of the reviewed studies was to evaluate the improvement in visual acuity, particularly NVA, in patients with presbyopia. Overall, the findings consistently demonstrated significant improvements in uncorrected NVA following the administration of pilocarpine formulations. These treatments, either using pilocarpine alone or in combination with other substances, resulted in an average improvement of 1 to 2 lines in near vision, indicating their potential to provide spectacle independence for near visual tasks in individuals with emmetropia and presbyopia.
Some studies explored the use of Carbachol as an alternative to pilocarpine as the miotic agent. One study compared different concentrations of pilocarpine, brimonidine, carbachol, and their combinations, showing that 3% carbachol induced a greater improvement in NVA compared to 1% pilocarpine, with a difference of 6.3 lines.[9] However, the small sample size limited the ability to draw definitive conclusions about the relative effectiveness of carbachol and pilocarpine. Other studies investigating the combination of carbachol and brimonidine also reported significant improvements in NVA.[13,14,15] The concentration of carbachol appeared to play a role, with 3% carbachol showing better results than a less concentrated 2.25% formulation over a longer duration.[13,14,15] A study by Abdelkader (2018) investigated the treatment in pseudophakic eyes with drops containing carbachol 3% and brimonidine 0.2%, and the results did not differ from other studies using the same combination in phakic eyes.[15]
A study by Benozzi et al (2012) demonstrated enhancement in accommodation and improvement in near vision over a period of 5 years with the use of pilocarpine 1% and diclofenac 0.1% eye drops administered twice daily.[10] Another case series study by Benozzi et al (2021) observed visual acuity improvement from baseline ranging from J3 to J8 improving to J1 to J2 after administering a patented formulation of preservative-free eye drops containing pilocarpine and diclofenac on a twice-daily schedule.[17]
In a study involving 57 study participants in the age group of 42-74 years with presbyopia, topical eye drops containing 0.247% pilocarpine resulted in a significant decrease in pupil diameter from 3.77mm to 2.63 mm (p < 0.05) and an increase in the mean depth of field from 1.6 D to 2.6 D, leading to improved vision.[12] Another eye drop formulation termed FOV Tears, which included pilocarpine 0.247% along with phenylephrine 0.78%, polyethylene glycol 0.09%, nepafenac 0.023%, pheniramine 0.034%, and naphazoline 0.003%, showed a mean improvement of 0.18 lines in near vision, with 92.3% of patients experiencing an improvement of at least 1 line.[16] Similarly, a case series study by Vejarano et al (2023) involving participants with presbyopia showed significant improvements in mean spherical equivalent and NVA after instilling a similar formulation of "FOV Tears”.[24] Two hours after instillation, significant improvements were observed in mean spherical equivalent (SE) by -0.17 Diopters (p < 0.001) and NVA by nearly two lines (p < 0.01).[24]
Allergan Pharmaceuticals evaluated the utility of pilocarpine and oxymetazoline combination eye drops for the treatment of presbyopia.[11] Their studies indicated that the use of pilocarpine alone resulted in an uncorrected NVA improvement of at least 2 lines in 70.6% of participants, whereas oxymetazoline alone showed improvement in only 46% of patients. Additional studies examining different concentrations of pilocarpine and oxymetazoline confirmed a significant dose-response effect of pilocarpine in improving visual acuity.[18]
Waring et al (2022) conducted the Phase 3 clinical study, GEMINI I to evaluate the effectiveness of AGN-190584 (Vuity), which contains 1.25% pilocarpine, administered once daily for 30 days in individuals aged 40 to 55 with presbyopia.[19] The results showed a significantly higher proportion of participants experiencing an improvement of 3 or more lines in visual acuity compared to the control group. Another recent Phase 3 study named VIRGO evaluated Pilocarpine 1.25% (AGN-190584; Vuity) administered bilaterally, twice daily, for 14 days.[25] The study demonstrated a statistically significant difference in favor of pilocarpine treatment, with a higher proportion of participants gaining ≥3 lines in NVA while maintaining a maximum 5-letter loss in distance visual acuity. This led to FDA approval for twice daily dosing of Vuity.[25]
There were four studies that evaluated whether the effect of pilocarpine treatment was age dependent. In one study involving FOV Tears, younger patients using FOV Tears gained more lines than older patients after administration, possibly due to greater accommodation reserve in younger individuals.[16,30] However, in another study, based on the use of carbachol and brimonidine, improvement in near vision was comparable between groups slightly favouring the <50 years age group.[13] Benozzi et al (2021) study examining pilocarpine and diclofenac formulation showed better near vision improvement in younger age groups with more than 82.3% of the patients aged between 40 and 55 years old achieved J1 with the best effect obtained in the group of patients aged from 40 to 45 years old, where 85.8% of them reached J compared to 77.8% of patients aged between 56 and 60 obtained J1.[17] In contrast, in the VIRGO trial, Vuity (1.25% pilocarpine) drops administered twice daily showed approximately equal percentage of patients aged under 50 years showed improvement in their NVA while on Pilocarpine HCL 1.25% BID to patients over 50 years.[25]
Adverse Effects
The safety profile of pilocarpine-based treatments was generally favorable, with most studies reporting minimal adverse effects. The majority of participants experienced no adverse reactions or only mild and transient symptoms. Commonly reported adverse events included headaches, ocular discomfort, eye irritation, and ocular surface burning. Nausea, blurry distance vision, dryness, burning, stinging, and eyelid retraction were also reported but occurred infrequently and resolved quickly.
In the study by Krader and Feinbaum (2015), topical eye drops containing 0.24% pilocarpine were well-tolerated, with 75% of patients experiencing no adverse reactions.[12] Some patients reported mild and transient adverse events such as nausea, headache, dryness, burning, stinging, and blurry distance vision, which dissipated within a few minutes. Vargus et al (2019) evaluated the safety of FOV Tears, a combination eye drop containing pilocarpine 0.247% along with other substances.[16] A mild headache reaction was reported by 14 participants of 117 total participants, but no severe adverse events were observed.[16]
Allergan Pharmaceuticals compared low-dose pilocarpine, oxymetazoline, and a combination of both in terms of safety and efficacy.[11] Pilocarpine alone was found to be superior to oxymetazoline in improving NVA, and the incidence of adverse reactions, particularly eyelid retraction, was higher in the oxymetazoline group at 26%.[11] However, in another study by Price et al (2021), the most common adverse event reported was headaches, with a frequency of less than 5% when pilocarpine was administered alone in the short-term study, and up to 28.1% in the high dose group of the extended study.[18]
The use of a patented formulation of preservative-free eye drops by Benozzi et al (2021) containing pilocarpine and diclofenac was associated with some uncomfortable symptoms, including a decrease in light perception (24.6%), headaches (11.7%), and ocular surface burning (6.6%).[17] However, all adverse effects resolved without additional treatment, except for ocular surface burning, which was relieved with artificial tears.
In the Phase 3 clinical study, GEMINI I, assessing the effectiveness of Vuity (pilocarpine 1.25%) once daily, headache (23%) was the most commonly reported adverse event, followed by visual impairment (7%).[19] A comparison between an optimized proprietary vehicle formulation (Vuity) and a generic formulation of pilocarpine 1% showed that the optimized formulation had fewer adverse events, including less ocular discomfort, vision blur, and reported symptoms such as eye pressure/pain, brow ache, stinging, itching, and light sensitivity.[20] In the VIRGO trial, which evaluated pilocarpine 1.25% administered twice daily for 14 days, the most common adverse reactions reported were headache and eye irritation.[25] These adverse events were reported by more than 5% of participants.
However, some case reports highlighted the potential risks associated with pilocarpine use, particularly in patients with pre-existing risk factors for retinal detachment.[21,22,23] Several patients treated with pilocarpine 1.25% experienced retinal detachment or vitreomacular traction, requiring urgent surgical intervention. [21,22,23] The case reports emphasized the importance of closely monitoring patients with pre-existing retinal detachment risk factors when using pilocarpine.
In summary, the reviewed studies generally reported minimal adverse effects of pilocarpine-based treatments, with most participants experiencing no adverse reactions or only mild and transient symptoms. Other adverse reactions occurred infrequently and resolved quickly. Monitoring and close follow-up of patients with such risk factors is essential to ensure their safety. Nevertheless, avoidance of these side effects may be related to the different concentrations and compounds in the studied formulations.
Conclusion and Future Steps
Various new pharmaceutical agents are currently under investigation for the treatment of presbyopia, the results of which from the available studies are promising. The reviewed studies provide valuable insights into the potential role of pilocarpine-based treatments in the management of presbyopia. The use of non-surgical options, such as pharmacological eye drops containing pilocarpine, is emerging as a promising approach for addressing the unmet needs of individuals with presbyopia, especially those aged 40 to 60 years. Many of the agents being used are parasympathomimetic, acting on the iris and ciliary muscles to increase the leans thickness and the accommodation for better visual acuity. Pure parasympathetic treatments can result in small pupil diameter and a myopic shift, compromising far distance vision, and muscarinic stimulation can cause several adverse reactions as well. Agents in the form of NSAIDs were proposed as supplements to counteract these actions. The findings suggest that pilocarpine formulations can effectively improve near vision and reduce the dependence on spectacles. There is no doubt that pharmacological treatment of presbyopia is an attractive form of therapy, but further research is needed to optimize the concentrations and combinations of pilocarpine and other substances to maximize efficacy and minimize adverse effects. Ongoing trial need to be implemented to evaluate the effectiveness of pilocarpine eye drops in pseudophakic patients and for uncorrected distance visual acuity indicating the continuous development and exploration of this treatment modality.
Declaration of Conflicting Interests
The Authors declare that there are no conflicts of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Grzybowski, A.; Markeviciute, A.; Zemaitiene, R. A Review of Pharmacological Presbyopia Treatment. Asia-Pacific J. Ophthalmol. 2020, 9, 226–233. [Google Scholar] [CrossRef]
- Glasser, A.; Kaufman, P.L. The mechanism of accommodation in primates. Ophthalmology 1999, 106, 863–872. [Google Scholar] [CrossRef]
- Holden, B.A.; Fricke, T.R.; Ho, S.M.; Wong, R.; Schlenther, G.; Cronjé, S.; Burnett, A.; Papas, E.; Naidoo, K.S.; Frick, K.D. Global Vision Impairment Due to Uncorrected Presbyopia. Arch. Ophthalmol. 2008, 126, 1731–1739. [Google Scholar] [CrossRef]
- Charman, W.N. Developments in the correction of presbyopia I: spectacle and contact lenses. Ophthalmic Physiol. Opt. 2014, 34, 8–29. [Google Scholar] [CrossRef]
- Alió, J.; Balgos, M.T.D.; Vargas, V. Correction of presbyopia: An integrated update for the practical surgeon. Taiwan J. Ophthalmol. 2018, 8, 121–140. [Google Scholar] [CrossRef]
- Wilkie, J.; Drance, S.M.; Schulzer, M. The Effects of Miotics On Anterior-Chamber Depth. Arch. Ophthalmol. 1969, 68, 78–83. [Google Scholar] [CrossRef]
- A Croft, M.; Kaufman, P.L.; Erickson-Lamy, K.; Polansky, J.R. Accommodation and ciliary muscle muscarinic receptors after echothiophate. Invest Ophthalmol Vis Sci. 1991, 32, 3288–97. [Google Scholar]
- Schalnus, R. Topical Nonsteroidal Anti-Inflammatory Therapy in Ophthalmology. Ophthalmologica 2003, 217, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, S. Addressing presbyopia pharmacologically. Ophthalmology Times, https://www.ophthalmologytimes.com/article/addressing-presbyopia-pharmacologically (2012, accessed 23 February 2023).
- Benozzi, J.; Benozzi, G.; Orman, B. Presbyopia: a New Potential Pharmacological Treatment. Med Hypothesis Discov Innov Ophthalmol. 2012, 1, 3–5. [Google Scholar] [PubMed]
- Allergan. Safety and Efficacy of AGN-199201 and AGN-190584 in Patients with Presbyopia. ClinicalTrials.gov Identifier: NCT02197806, https://clinicaltrials.gov/ct2/show/NCT02197806 (2015, accessed 15 March 2023).
- Krader CG, Feinbaum C. Simple solution for presbyopia: topical agent acts by reducing pupil size to increase depth of focus. Ophthalmology Times, https://www.ophthalmologytimes.com/article/simple-solution-presbyopia (2012, accessed 25 February 2023).
- Abdelkader, A. Improved Presbyopic Vision With Miotics. Eye Contact Lens: Sci. Clin. Pr. 2015, 41, 323–327. [Google Scholar] [CrossRef] [PubMed]
- Abdelkader, A.; Kaufman, H.E. Clinical outcomes of combined versus separate carbachol and brimonidine drops in correcting presbyopia. Eye Vis. 2016, 3, 31. [Google Scholar] [CrossRef]
- Abdelkader, A. A novel pharmacological treatment of pseudophakic presbyopia. Int J Ophthalm Res. 2018, 4. [Google Scholar]
- Vargas, V.; Vejarano, F.; Alió, J.L. Near Vision Improvement with the Use of a New Topical Compound for Presbyopia Correction: A Prospective, Consecutive Interventional Non-Comparative Clinical Study. Ophthalmol. Ther. 2019, 8, 31–39. [Google Scholar] [CrossRef]
- Benozzi, G.; Cortina, M.E.; Gimeno, E.; Vantesone, D.L.; Solas, A.E.; Lorda, G.M.; Facal, S.; Leiro, J.; Orman, B. A multicentric study of pharmacological treatment for presbyopia. Graefe's Arch. Clin. Exp. Ophthalmol. 2021, 259, 2441–2450. [Google Scholar] [CrossRef]
- Price, F.W.; Hom, M.; Moshirfar, M.; et al. Combinations of Pilocarpine and Oxymetazoline for the Pharmacological Treatment of Presbyopia: Two Randomized Phase 2 Studies. Ophthalmol Sci. 2021, 1, 100065. [Google Scholar] [CrossRef]
- Waring, G.O.; Price, F.W., Jr; Wirta, D.; et al. Safety and Efficacy of AGN-190584 in Individuals With Presbyopia: The GEMINI 1 Phase 3 Randomized Clinical Trial. JAMA Ophthalmol. 2022, 140, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Jackson, M.A.; Giyanani, J.; Shabaik, Y.; Penzner, J.; Gore, A.V.; Robinson, M.R.; Waring, G.O. In Vitro and In-Eye Comparison of Commercial Pilocarpine Ophthalmic Solution and an Optimized, Reformulated Pilocarpine for Presbyopia Treatment. Ophthalmol. Ther. 2022, 11, 869–879. [Google Scholar] [CrossRef]
- Eton, E.A.; Zhao, P.Y.; Johnson, M.W.; Rao, R.C.; Huvard, M.J. Rhegmatogenous retinal detachment after initiation of pilocarpine hydrochloride ophthalmic solution 1.25% for treatment of presbyopia. Retin. Cases Brief Rep. 2022, 18, 98–100. [Google Scholar] [CrossRef] [PubMed]
- Amarikwa, L.; Michalak, S.M.; Caul, S.; Mruthyunjaya, P.; Rahimy, E. Vitreofoveal Traction Associated With Pilocarpine for Presbyopia. Ophthalmic Surgery, Lasers Imaging Retin. 2022, 53, 410–411. [Google Scholar] [CrossRef] [PubMed]
- Al-Khersan, H.; Flynn, H.W.; Townsend, J.H. Retinal Detachments Associated With Topical Pilocarpine Use for Presbyopia. Arch. Ophthalmol. 2022, 242, 52–55. [Google Scholar] [CrossRef]
- Vejarano, F.; Alió, J.; Iribarren, R.; Lança, C. Non-Miotic Improvement in Binocular Near Vision with a Topical Compound Formula for Presbyopia Correction. Ophthalmol. Ther. 2023, 12, 1013–1024. [Google Scholar] [CrossRef] [PubMed]
- Kannarr, S.; El-Harazi, S.M.; Moshirfar, M.; Lievens, C.; Kim, J.L.; Peace, J.H.; Safyan, E.; Liu, H.; Zheng, S.; Robinson, M.R. Safety and Efficacy of Twice-Daily Pilocarpine HCl in Presbyopia: The Virgo Phase 3, Randomized, Double-Masked, Controlled Study. Arch. Ophthalmol. 2023, 253, 189–200. [Google Scholar] [CrossRef] [PubMed]
- Sheeladevi, S.; Seelam, B.; Nukella, P.B.; Borah, R.R.; Ali, R.; Keay, L. Prevalence of refractive errors, uncorrected refractive error, and presbyopia in adults in India: A systematic review. Indian J. Ophthalmol. 2019, 67, 583. [Google Scholar] [CrossRef]
- Fricke, T.R.; Tahhan, N.; Resnikoff, S.; Papas, E.; Burnett, A.; Ho, S.M.; Naduvilath, T.; Naidoo, K.S. Global Prevalence of Presbyopia and Vision Impairment from Uncorrected Presbyopia: Systematic Review, Meta-analysis, and Modelling. Ophthalmology 2018, 125, 1492–1499. [Google Scholar] [CrossRef] [PubMed]
- Balal S, Gil-Cazorla R, Naroo SA, et al. Refractive surgery’s holy grail. Eyedrops for presbyopia. Myth or medicine? The Ophthalmologist, March 2017, p.18-29.
- Benozzi, G.; Perez, C.; Leiro, J.; Facal, S.; Orman, B. Presbyopia Treatment With Eye Drops: An Eight Year Retrospective Study. 2020, 9, 25.
- Alio, J.L.; Plaza-Puche, A.B.; Férnandez-Buenaga, R.; Pikkel, J.; Maldonado, M. Multifocal intraocular lenses: An overview. Surv. Ophthalmol. 2017, 62, 611–634. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow diagram of study selection.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



