
Submitted:
22 November 2025
Posted:
24 November 2025
You are already at the latest version
Abstract
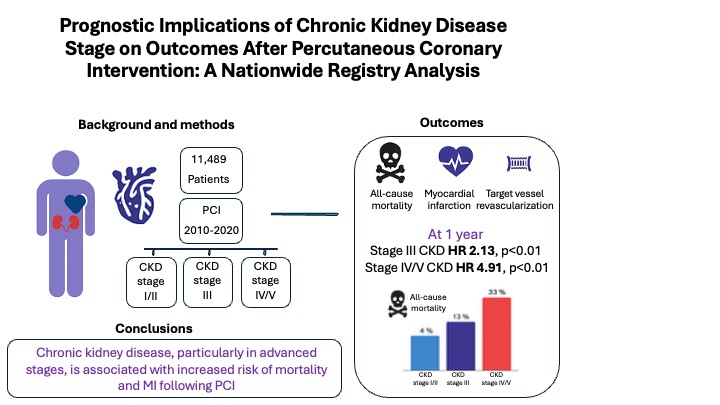
Aims: Chronic kidney disease (CKD) is associated with adverse cardiovascular outcomes, yet the prognostic impact of specific CKD stages following percutaneous coronary intervention (PCI) is not well defined. We assessed the relationship between CKD stage and clinical outcomes after PCI. Methods: We retrospectively analyzed 11,489 patients who underwent PCI between 2010 and 2020. Kidney function was classified as preserved (eGFR≥60 mL/min/1.73 m²), stage III CKD (eGFR 30–59), or stage IV/V CKD (eGFR<30) using the CKD-EPI equation. The primary endpoint was a composite of all-cause mortality, non-fatal myocardial infarction (MI), and target vessel revascularization (TVR) at 1 year; secondary endpoints included individual components and outcomes through 5 years. Associations were evaluated using multivariable Cox regression. Results: Stage III and stage IV/V CKD were present in 18% and 5.6% of patients, respectively. At 1 year, both stage III (HR 2.13, p<0.01) and stage IV/V CKD (HR 4.91, p<0.01) were associated with higher risk of the composite endpoint. Mortality rose sharply with CKD severity (33% in stage IV/V vs. 4% in preserved renal function), and MI risk was significantly higher in stage IV/V CKD. These associations persisted at 5 years. Unadjusted TVR risk was higher in stage IV/V CKD but lost significance after adjustment. Conclusions: CKD, particularly in advanced stages, is independently associated with increased mortality and MI after PCI, with effects persisting long-term. While advanced CKD showed higher unadjusted TVR risk, this was not independent after adjustment. These findings support individualized treatment strategies and extended follow-up in PCI patients with CKD.
Keywords:
Percutaneous coronary intervention
; chronic kidney disease
; myocardial infarction
; target vessel revascularization
1. Introduction
Chronic kidney disease (CKD) is a well-established independent risk factor for adverse cardiovascular outcomes, including coronary artery disease (CAD) [1,2]. The prevalence and severity of CAD increase progressively as kidney function declines, with patients in advanced stages of CKD (stages IV/V) facing particularly high risks of cardiovascular events and mortality compared to those with preserved renal function [3,4]. Despite advances in percutaneous coronary intervention (PCI) techniques, current evidence suggests that individuals with CKD especially those with advanced disease remain at elevated risk for complications such as target vessel revascularization (TVR) and myocardial infarction (MI) following complex PCI [5,6].
Understanding how varying degrees of renal dysfunction affect post-PCI outcomes is essential for optimizing management strategies in this high-risk population. In this study, we aimed to evaluate the incidence of all-cause mortality, TVR and MI following PCI across different stages of CKD.
2. Materials and Methods
2.1. Study Population
We conducted a retrospective analysis of 11,489 patients who underwent PCI between 2010 and 2020 at Rabin Medical Center. CKD was defined using the CKD-EPI equation, categorizing patients into preserved kidney function (eGFR ≥60 mL/min/1.73 m², including CKD stage I/II), CKD stage III (eGFR 30–59 mL/min/1.73 m²) and CKD stage IV/V (eGFR <30 mL/min/1.73 m²), also referred as advanced CKD [7].
2.2. Follow-Up and Outcomes
Patients were followed from the time of PCI until death or up to five years, whichever occurred first. The primary endpoint was a composite of all-cause mortality, non-fatal MI and TVR at one year. Secondary outcomes included each of the components of the primary outcome in separate. Long-term outcomes up to five years were assessed. Mortality data were obtained from the Israeli Ministry of the Interior’s Population Registry.
2.3. Data Collection and Definitions
CKD diagnosis was based on the most recent creatinine level recorded within three months prior to the PCI procedure. eGFR was calculated using the CKD-EPI equation [8]. Patients with an eGFR of 30–59 mL/min/1.73 m² were classified as CKD stage III, those with 15–29 mL/min/1.73 m² as stage IV, and those with eGFR <15 mL/min/1.73 m² or requiring renal replacement therapy as stage V [7].
Baseline comorbidities were recorded according to physician documentation at the time of PCI. Obstructive coronary artery disease was defined as angiographic stenosis ≥70% in a vessel with a a diameter ≥ 2mm, ≥50% in the left main, or a fractional flow reserve (FFR) <0.80. Severe left ventricular dysfunction was defined as an ejection fraction <30% based on the initial echocardiogram during hospitalization [9].
2.4. Statistical Analysis
Continuous variables were presented as means ± standard deviation (SD) or medians with interquartile ranges (IQR), as appropriate. Group comparisons for continuous variables were performed using one-way ANOVA or the Kruskal–Wallis test, depending on data distribution. Categorical variables were reported as counts and percentages and compared using the chi-squared test. For pairwise comparisons between two groups, the chi-squared test was used for categorical variables, and either the Student’s t-test or the Mann–Whitney–Wilcoxon test was applied for continuous variables, based on the normality of the data’s distribution. As a secondary analysis, we performed a competing risk analysis to account for the influence of death on the incidence of TVR and re-MI. The Fine and Gray sub distribution hazard model was used to estimate the cumulative incidence function, treating death as a competing event. Sub distribution hazard ratios (sHRs) and 95% confidence intervals (CIs) were calculated.
All statistical tests were two-sided, and a p-value <0.05 was considered significant. Hazard ratios (HR) are presented with 95% confidence intervals (CI). Kaplan–Meier survival curves were generated, and the log-rank test was used to compare survival rates across groups at one and five years. Cox proportional hazards models were used to assess the association between CKD stage and outcomes (TVR, MI, mortality), adjusting for relevant covariates identified in univariate analyses (p<0.05). All analyses were performed using R (version 4.0.0, RStudio, Vienna, Austria).
3. Results
3.1. Study Population and Strata
Between 2010 and 2020, 11,489 patients underwent PCI at Rabin Medical Center. Among these, 2,708 (23.6%) were identified as having CKD, including 2,063 patients (18%) with stage III CKD and 645 patients (5.6%) with stage IV/V CKD.
The study population was predominantly older adults. The mean age was 72.5 years for patients with CKD stage IV/V , 75.0 years for stage III , and 63.4 years for those with preserved renal function. Approximately one-third of the cohort was female, with lower proportions in earlier CKD stages. Cardiovascular risk factors, including diabetes mellitus, hypertension, smoking, and chronic obstructive pulmonary disease (COPD) were more prevalent with increasing CKD severity. Likewise, prior stroke and peripheral vascular disease were more common in advanced CKD stages (Table 1).
Cardiac conditions such as congestive heart failure and reduced ejection fraction were also more frequent in patients with stage IV/V CKD. Additionally, lipid profiles (total cholesterol and LDL) tended to be lower among patients with advanced CKD.
PCI indications and procedural characteristics differed by CKD stage. The proportion of interventions for acute coronary syndromes decreased from 67.9% in patients with preserved renal function to 55.5% in those with stage IV/V CKD. Left main coronary interventions were more frequent in advanced CKD, while intervention distribution across other coronary territories was similar. Femoral artery access was used more often than radial access in patients with advanced CKD (Table 1).
3.2. Follow-Up and Outcomes
CKD stages III and IV/V were associated with increased rates of the composite outcome including all-cause mortality, non-fatal MI and TVR at 1 year. Patients with CKD stage III were at 2.13 fold risk for mortality, MI or TVR (95% CI 1.9-2.4, p<0.01). This risk increased to 4.91 among patients with CKD stage IV/V (95% CI 4.28-5.63, p<0.01) (Table 2, Figure 1).
All-cause mortality was strongly correlated with declining renal function. One-year mortality was 33% in patients with CKD stage IV/V, compared to 14.1% in patients with CKD stage III and 4% among patients with preserved kidney function. Kaplan–Meier curves depicting mortality by CKD stage are presented in Figure 2.
The increased rates of non-fatal MI were consistent in all CKD stages, with HR of 2.29 (95% CI 1.78–2.95, p<0.01) at stage IV/V and 1.31 (95% CI 1.1–1.6, p<0.01) at stage III CKD. CKD stage IV/V was associated with an increased risk of TVR (HR 1.67, 95% CI 1.07–2.61, p=0.02), whereas this association was not significant for CKD stage III.
The associations of CKD with the composite primary outcome, as well as all-cause mortality and non-fatal MI continued through the five-year follow-up. Patients with advanced CKD had 4.63 fold risk of experiencing death, MI or TVR (95% CI 4.16-5.15) compared to patients with preserved kidney function. This risk was 2.22 fold higher for patients with CKD stage III (95% CI 2.05-2.4).
Five-year mortality was 57% in patients with CKD stage IV/V, compared to 10.5% in patients with preserved kidney function. The hazard ratio for MI at five years was 2.09 (95% CI 1.7–2.57, p<0.001) and 1.29 (95% CI 1.2–1.47, p<0.001) in advanced CKD and at CKD stage III, respectively.
At five years, the risk of TVR in CKD stage IV/V did not reach statistical significance (HR 1.37, 95% CI 0.94–2.02, p=0.104) (Table 2).
3.3. Multivariable and Competing Risk Analysis
After adjustment, stage IV/V remained independently associated with the primary composite outcome at 1 year (HR 3.00, 95% CI 2.58–3.49, p<0.001) and 5 years (HR 2.78, 95% CI 2.48–3.13, p<0.001). The adjusted risk for CKD stage III was 1.46 (95% CI 1.29–1.65, p<0.001) at 1 year and 1.49 (95% CI 1.37–1.63) at 5 years (Table 3).
All-cause mortality remained significantly elevated across CKD stages. In CKD stage IV/V, mortality risk was 4.73-fold higher at 1 year (95% CI 3.90–5.73, p<0.001) and 4.13-fold higher at 5 years (95% CI 3.60–4.73, p<0.001). For CKD stage III, the corresponding HRs were 2.18 (95% CI 1.85–2.58, p<0.001) at 1 year and 2.15 (95% CI 1.93–2.38, p<0.001) at 5 years (Table 4).
The increased risk of MI in CKD stage IV/V remained significant after multivariable adjustment at both 1 and 5 years. However, CKD stage III was not independently associated with increased MI risk (Table 5).
The association between advanced CKD and TVR was attenuated after adjustment, with no independent association observed for either 1-year or 5-year follow-up (Table 6).
Other predictors of increased mortality included older age (≥65 years), female sex, peripheral vascular disease, diabetes, COPD, femoral vs. radial access, and severe left ventricular dysfunction. These findings were consistent in competing risk models (Supplementary Table 1).
4. Discussion
In this large retrospective cohort study, we evaluated the impact of CKD severity on cardiovascular outcomes following PCI. Worsening CKD stage was strongly and consistently associated with adverse outcomes. Advanced CKD (stage IV/V) conferred more than a fourfold higher risk of the composite endpoint of death, MI, or TVR at both 1 and 5 years, while stage III CKD carried approximately a twofold increased risk. Mortality risk rose steeply with declining renal function, reaching 57% at 5 years in stage IV/V. Although MI risk remained elevated in advanced CKD after adjustment, the association with TVR was attenuated and no longer significant.
These results are strongly supported by the literature. Multiple large cohort studies and registries have demonstrated a stepwise increase in mortality and major adverse cardiovascular events (MACE) with worsening CKD stage after PCI, even after multivariable adjustment for confounders [10,11,12,13] . For example, the J-MINUET study found that three-year mortality and MACE rates rise sharply from patients with preserved kidney function to those with moderate and severe CKD, and that CKD stage improved risk prediction models for adverse outcomes [12]. Those findings are also supported by meta-analysis demonstrating that CKD is an independent predictor of mortality and MI after PCI, with risk increasing as eGFR declines [14].
Several pathophysiological mechanisms probably contribute to the poor post-PCI outcomes observed in patients with CKD. Chronic kidney dysfunction is associated with systemic inflammation, oxidative stress, endothelial dysfunction, and as a result accelerated atherosclerosis, increased risk for restenosis or therefore recurrent ischemia [15,16,17]. Additional mechanism is uremia-related platelet dysfunction and impaired drug metabolism that may compromise both procedural success and antiplatelet efficacy [18,19].
The increased rate of femoral access and higher interventional complexity in patients with advanced CKD stages, as seen in our cohort, may further contribute to the increased procedural risk and worse outcomes.
The association between CKD and restenosis or stent thrombosis remains incompletely understood. Much of the existing evidence is based on earlier-generation stent platforms and outdated interventional techniques. The SYNTAX trial, which utilized paclitaxel-eluting stents, reported worse outcomes and higher restenosis rates in patients with eGFR <30 mL/min/1.73 m² or dialysis dependence [20]. However, its five-year follow-up failed to establish a significant link between CKD and TVR [21]. Other trials, including a 2016 Korean study, showed that individuals with advanced CKD experienced higher rates of target lesion failure, even with second-generation drug-eluting stents [5]. In contrast, findings from the HORIZONS-AMI trial indicated no significant association between CKD and TVR at 30 days, 1 year, or 3 years. [14,22]. Furthermore, in that same trial, no difference in TVR rates was observed between bare-metal and drug-eluting stents in CKD patients at 3-year follow-up [22]. In our cohort, the association between CKD and TVR was modest. A statistically significant association was observed at one year in patients with stage IV/V CKD, but this association diminished over time and was no longer significant after adjusting for confounding variables and competing risks. Multivariate analysis revealed that neither stage III nor stage IV/V CKD independently predicted TVR. These findings suggest that MI in this cohort was more likely driven by de novo lesions rather than stent failure. Advanced CKD may serve as a surrogate marker for higher TVR risk, rather than being a direct causal factor.
Our study has several notable strengths that enhance the robustness and relevance of these findings. First, it represents one of the largest and most contemporary real-world cohorts to date evaluating the prognostic impact of CKD stage on PCI outcomes, encompassing over 11,000 patients treated within the last decade. Second, the analysis specifically examined TVR as a distinct endpoint, which has been underreported in prior CKD-PCI research. Importantly, the study reflects current clinical practice in the era of latest-generation drug-eluting stents, advanced interventional techniques, and contemporary pharmacological therapies, thereby providing relevant insights for present-day patient management. The inclusion of both short- and long-term follow-up strengthens the validity of the findings and allows for a comprehensive assessment of temporal trends in risk. Finally, the use of detailed multivariable and competing risk analyses enhances the robustness of the results and supports their applicability to a broad PCI population.
As CKD is becoming a growing global health burden, a substantial proportion of patients undergoing PCI have some degree of renal impairment. Renal dysfunction is independently associated with increased cardio-vascular risk. Whether PCI modifies this risk remains uncertain.
The ISCHEMIA-CKD trial evaluated elective patients with advanced CKD (stages 4–5 or dialysis-dependent) and failed to find benefit of invasive strategy of revascularization (PCI or CABG) over optimal medical therapy. However, interpretation of these results should be cautious, as the trial excluded patients with severe symptoms, left main disease, or systolic heart failure. Additionally, crossover between treatment arms was frequent, and peri-procedural MI rates were higher in the intervention group compared to the conservative treatment group [23,24].
Unlike elective procedures, in the acute setting, PCI remains a necessary and often life-saving intervention unrelated to CKD severity. Data from the SWEDEHEART registry demonstrated improved one-year survival with an early invasive strategy in patients with NSTEMI and CKD stages 2–4, nevertheless, the benefit of invasive strategy declined with progression of the kidney failure and was less evident in stage 5 CKD and in dialysis patients [25]. However, more recent and up to date study have supported invasive management in patients with acute MI in all stages of CKD patients including those on hemodialysis, showing reduced in-hospital mortality [26].
Based on the study results and previous publications, we support a more tailored, risk-adjusted approach in managing patients with CKD undergoing PCI, taking into consideration elective vs emergent intervention, access site and the severity of renal impairment. In elective cases, strategies may include intensified surveillance, optimization of medical therapy, consideration of access site, and possibly earlier involvement of nephrology and multidisciplinary heart-kidney teams. Procedural decisions should balance benefits against long-term survival projections, informed by evidence from the ISCHEMIA-CKD trial, while acknowledging its limitations, and the observed TVR rates from this analysis and earlier studies. In acute presentations, clinicians should refrain from postponing PCI out of concern for potential renal injury, a practice sometimes referred to as “renalism” [27].
Several limitations should be acknowledged. First, this is a retrospective observational study from a single center, and although the cohort is large and multivariable and competing risk analyses were performed, the possibility of residual confounding cannot be excluded. Second, CKD classification relied on eGFR measurements before PCI and did not incorporate albuminuria or proteinuria, potentially underestimating renal dysfunction. Third, we lacked data on medication adherence, contrast volume, and nephroprotective measures, all of which may influence outcomes. Lastly, while follow-up was robust, we could not assess cause-specific mortality, limiting our ability to distinguish between cardiovascular and non-cardiovascular deaths.
5. Conclusions
CKD, particularly in advanced stages, is independently associated with increased mortality and MI after PCI, with effects persisting long-term. While advanced CKD showed higher unadjusted TVR risk, this was not independent after adjustment. These findings support individualized treatment strategies and extended follow-up in PCI patients with CKD.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, Keren Skalsky and Alon Shechter; Methodology, Yeela Talmor-Barkan, Alon Shechter and Amos Levi; Software, Amos Levi; Validation, Yeela Talmor-Barkan, Tsahi T. Lerman and Amos Levi; Formal analysis, Amos Levi; Investigation, Keren Skalsky, Edward Itelman, Tsahi T. Lerman, Assaf Rotmensh, Shapira Yaron, Arthur Shiyovich and Amos Levi; Resources, Tsahi T. Lerman and Ran Kornowski; Data curation, Amos Levi; Writing – original draft, Keren Skalsky; Writing – review & editing, Yeela Talmor-Barkan, Edward Itelman, Tsahi T. Lerman, Assaf Rotmensh, Leor Perl, Alon Shechter, Shapira Yaron, Arthur Shiyovich and Amos Levi; Visualization, Edward Itelman, Tsahi T. Lerman, Assaf Rotmensh, Leor Perl, Shapira Yaron, Arthur Shiyovich and Ran Kornowski; Supervision, Arthur Shiyovich and Ran Kornowski.
Funding
none.
Ethical Approval
The study protocol was priori approved by the institution’s human research committee (Rabin Medical Center Helsinki committee) .
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of interest
none.
References
- Gansevoort RT, Correa-Rotter R, Hemmelgarn BR, Jafar TH, Heerspink HJL, Mann JF, et al. Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms, and prevention. The Lancet [Internet]. 2013 Jul [cited 2025 Jul 16];382(9889):339–52. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0140673613605954.
- Saeed D, Reza T, Shahzad MW, Karim Mandokhail A, Bakht D, Qizilbash FH, et al. Navigating the Crossroads: Understanding the Link Between Chronic Kidney Disease and Cardiovascular Health. Cureus. 2023 Dec;15(12):e51362.
- Fox CS, Matsushita K, Woodward M, Bilo HJ, Chalmers J, Heerspink HJL, et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes: a meta-analysis. The Lancet [Internet]. 2012 Nov [cited 2025 Jul 16];380(9854):1662–73. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0140673612613506.
- Na KY, Kim CW, Song YR, Chin HJ, Chae DW. The Association between Kidney Function, Coronary Artery Disease, and Clinical Outcome in Patients Undergoing Coronary Angiography. J Korean Med Sci [Internet]. 2009 [cited 2025 Jul 16];24(Suppl 1):S87. Available from: https://jkms.org/DOIx.php?id=10.3346/jkms.2009.24.S1.S87.
- Lee JM, Kang J, Lee E, Hwang D, Rhee TM, Park J, et al. Chronic Kidney Disease in the Second-Generation Drug-Eluting Stent Era. JACC Cardiovasc Interv [Internet]. 2016 Oct [cited 2025 Jul 16];9(20):2097–109. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1936879816310895.
- Kwon W, Choi KH, Song YB, Park YH, Lee JM, Lee JY, et al. Intravascular Imaging in Patients With Complex Coronary Lesions and Chronic Kidney Disease. JAMA Netw Open [Internet]. 2023 Nov 29 [cited 2025 Jul 16];6(11):e2345554. Available from: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2812357.
- Levey AS, Eckardt KU, Tsukamoto Y, Levin A, Coresh J, Rossert J, et al. Definition and classification of chronic kidney disease: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int [Internet]. 2005 Jun [cited 2025 Jul 16];67(6):2089–100. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0085253815506984.
- Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009 May 5;150(9):604–12.
- Mitchell C, Rahko PS, Blauwet LA, Canaday B, Finstuen JA, Foster MC, et al. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. J Am Soc Echocardiogr [Internet]. 2019 Jan [cited 2025 Jul 16];32(1):1–64. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0894731718303183.
- Vichova T, Knot J, Ulman J, Maly M, Motovska Z. The impact of stage of chronic kidney disease on the outcomes of diabetics with acute myocardial infarction treated with percutaneous coronary intervention. Int Urol Nephrol [Internet]. 2016 Jul [cited 2025 Jul 23];48(7):1137–43. Available from: http://link.springer.com/10.1007/s11255-016-1260-9.
- Grandjean-Thomsen NL, Marley P, Shadbolt B, Farshid A. Impact of Mild-to-Moderate Chronic Kidney Disease on One Year Outcomes after Percutaneous Coronary Intervention. Nephron [Internet]. 2017 [cited 2025 Jul 23];137(1):23–8. [CrossRef]
- Hashimoto Y, Ozaki Y, Kan S, Nakao K, Kimura K, Ako J, et al. Impact of Chronic Kidney Disease on In-Hospital and 3-Year Clinical Outcomes in Patients With Acute Myocardial Infarction Treated by Contemporary Percutaneous Coronary Intervention and Optimal Medical Therapy ― Insights From the J-MINUET Study ―. Circ J [Internet]. 2021 Sep 24 [cited 2025 Jul 23];85(10):1710–8. Available from: https://www.jstage.jst.go.jp/article/circj/85/10/85_CJ-20-1115/_article.
- Soh RYH, Sia CH, Lau RH, Ho PY, Timothy NYM, Ho JSY, et al. The impact of chronic kidney disease on long-term outcomes following semi-urgent and elective percutaneous coronary intervention. Coron Artery Dis [Internet]. 2021 Sep [cited 2025 Jul 23];32(6):517–25. Available from: https://journals.lww.com/10.1097/MCA.0000000000000980.
- Jiang W, Zhou Y, Chen S, Liu S. Impact of Chronic Kidney Disease on Outcomes of Percutaneous Coronary Intervention in Patients With Diabetes Mellitus: A Systematic Review and Meta-Analysis. Tex Heart Inst J [Internet]. 2023 Jan 1 [cited 2025 Jul 23];50(1). Available from: https://thij.kglmeridian.com/view/journals/thij/50/1/article-e227873.xml.
- Ronco C, Bellasi A, Di Lullo L. Cardiorenal Syndrome: An Overview. Adv Chronic Kidney Dis [Internet]. 2018 Sep [cited 2025 Jul 16];25(5):382–90. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1548559518301204.
- Kumar U, Wettersten N, Garimella PS. Cardiorenal Syndrome: Pathophysiology. Cardiol Clin. 2019 Aug;37(3):251–65.
- Rangaswami J, Bhalla V, Blair JEA, Chang TI, Costa S, Lentine KL, et al. Cardiorenal Syndrome: Classification, Pathophysiology, Diagnosis, and Treatment Strategies: A Scientific Statement From the American Heart Association. Circulation [Internet]. 2019 Apr 16 [cited 2025 Jul 16];139(16). [CrossRef]
- Vasu S, Gruberg L, Brown DL. The impact of advanced chronic kidney disease on in-hospital mortality following percutaneous coronary intervention for acute myocardial infarction. Catheter Cardiovasc Interv Off J Soc Card Angiogr Interv. 2007 Nov 1;70(5):701–5.
- Skalsky K, Shiyovich A, Steinmetz T, Kornowski R. Chronic Renal Failure and Cardiovascular Disease: A Comprehensive Appraisal. J Clin Med [Internet]. 2022 Feb 28 [cited 2025 Jul 16];11(5):1335. Available from: https://www.mdpi.com/2077-0383/11/5/1335.
- Milojevic M, Head SJ, Mack MJ, Mohr FW, Morice MC, Dawkins KD, et al. The impact of chronic kidney disease on outcomes following percutaneous coronary intervention versus coronary artery bypass grafting in patients with complex coronary artery disease: five-year follow-up of the SYNTAX trial. EuroIntervention [Internet]. 2018 May [cited 2025 Jul 17];14(1):102–11. Available from: http://www.pcronline.com/eurointervention/134th_issue/15.
- Milojevic M, Head SJ, Mack MJ, Mohr FW, Morice MC, Dawkins KD, et al. The impact of chronic kidney disease on outcomes following percutaneous coronary intervention versus coronary artery bypass grafting in patients with complex coronary artery disease: five-year follow-up of the SYNTAX trial. EuroIntervention [Internet]. 2018 May [cited 2025 Jul 24];14(1):102–11. Available from: http://www.pcronline.com/eurointervention/134th_issue/15.
- Saltzman AJ, Stone GW, Claessen BE, Narula A, Leon-Reyes S, Weisz G, et al. Long-Term Impact of Chronic Kidney Disease in Patients With ST-Segment Elevation Myocardial Infarction Treated With Primary Percutaneous Coronary Intervention. JACC Cardiovasc Interv [Internet]. 2011 Sep [cited 2025 Jul 24];4(9):1011–9. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1936879811005450.
- Chaitman BR, Cyr DD, Alexander KP, Pracoń R, Bainey KR, Mathew A, et al. Cardiovascular and Renal Implications of Myocardial Infarction in the ISCHEMIA-CKD Trial. Circ Cardiovasc Interv [Internet]. 2022 Aug [cited 2025 Jul 17];15(8). [CrossRef]
- Bangalore S, Maron DJ, O’Brien SM, Fleg JL, Kretov EI, Briguori C, et al. Management of Coronary Disease in Patients with Advanced Kidney Disease. N Engl J Med [Internet]. 2020 Apr 23 [cited 2025 Jul 17];382(17):1608–18. [CrossRef]
- Szummer K, Lundman P, Jacobson SH, Schön S, Lindbäck J, Stenestrand U, et al. Influence of Renal Function on the Effects of Early Revascularization in Non-ST-Elevation Myocardial Infarction: Data From the Swedish Web-System for Enhancement and Development of Evidence-Based Care in Heart Disease Evaluated According to Recommended Therapies (SWEDEHEART). Circulation [Internet]. 2009 Sep 8 [cited 2025 Jul 17];120(10):851–8. [CrossRef]
- Smilowitz NR, Gupta N, Guo Y, Mauricio R, Bangalore S. Management and outcomes of acute myocardial infarction in patients with chronic kidney disease. Int J Cardiol [Internet]. 2017 Jan [cited 2025 Jul 17];227:1–7. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0167527316334726.
- Gaut JP. Time to Abandon Renalism: Patients with Kidney Diseases Deserve More. Clin J Am Soc Nephrol [Internet]. 2023 Apr [cited 2025 Jul 24];18(4):419–20. Available from: https://journals.lww.com/10.2215/CJN.0000000000000127.
Figure 1.
Cumulative incidence of the composite outcome - death, MI and TVR by CKD stage.
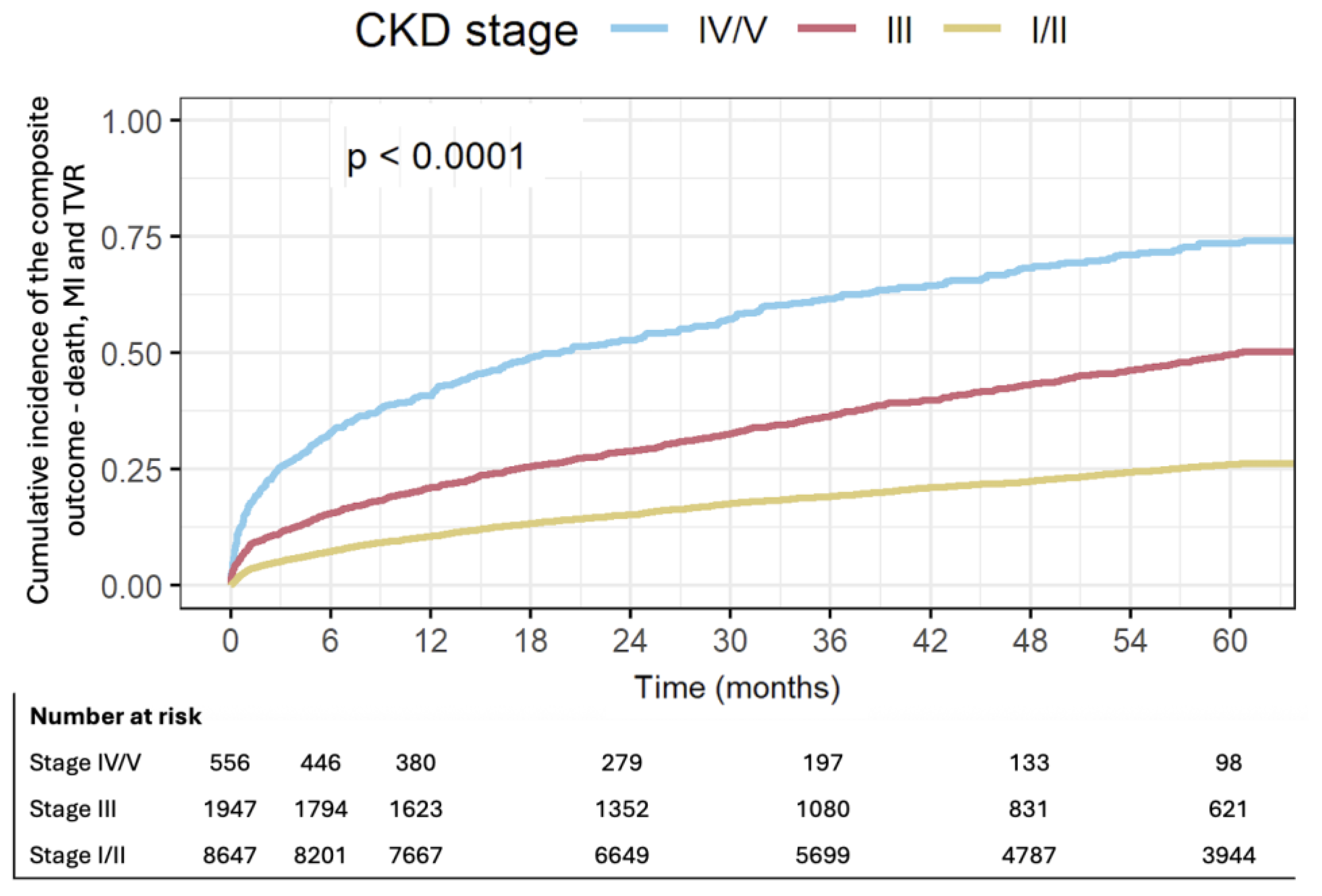
Figure 2.
Cumulative incidence of death by CKD stage.
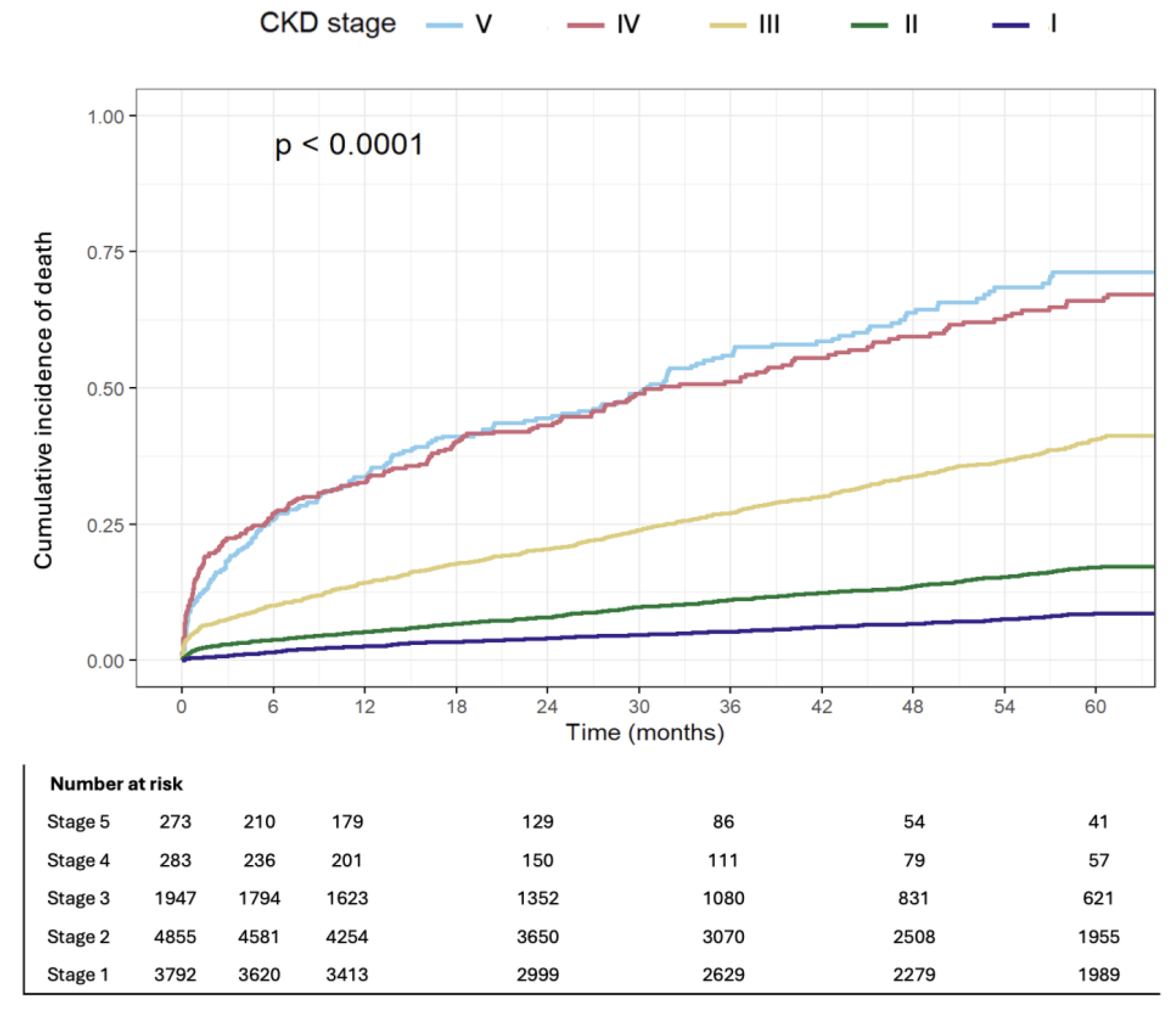

Table 1.
Baseline demographics, clinical history, and procedural characteristics of patients, stratified by CKD stage.
Table 1.
Baseline demographics, clinical history, and procedural characteristics of patients, stratified by CKD stage.
| Stage I/II (n=8781) | Stage III (n=2063) | Stage IV/V (n=645) | P | |
| Demographics | ||||
| age (years) | 63.4 (11.6) | 75 (10.1) | 72.5 (12.9) | 0.000 |
| Female gender (%) | 20.1 | 33.7 | 33 | 0.000 |
| Cardiovascular risk factors | ||||
| DM (%) | 40.8 | 54.9 | 70.7 | 0.000 |
| HTN (%) | 67.2 | 87.6 | 94.4 | 0.000 |
| Smoking History (%) | 38.6 | 22 | 19.2 | 0.000 |
| COPD (%) | 7.6 | 11.8 | 14 | 0.000 |
| PVD (%) | 4.1 | 7.4 | 15.5 | 0.000 |
| Prior Stroke (%) | 5.6 | 10.4 | 14.6 | 0.000 |
| Cardiac diseases | ||||
| Known CHF (%) | 7.7 | 14.9 | 11.6 | 0.000 |
| EF (%) | 54.9 (8.9) | 52.7 (10.3) | 49.9 (11.5) | 0.000 |
| Known Atrial Fibrillation (%) | 4.4 | 7.6 | 8.2 | 0.000 |
| S/P CABG (%) | 9.1 | 15.7 | 18.8 | 0.000 |
| Other diseases | ||||
| Prior Malignancy (%) | 9.7 | 18.2 | 22.2 | 0.000 |
| Active Malignancy (%) | 4 | 5.5 | 2.9 | 0.002 |
| Dementia (%) | 1.5 | 4.7 | 5.1 | 0.000 |
| Blood tests results | ||||
| Total Cholesterol (mg/dL) | 170.8 (44.7) | 156.9 (44.2) | 147.8 (44.3) | 0.000 |
| HDL (mg/dL) | 41.5 (12.4) | 42.8 (13.9) | 39.3 (12.8) | 0.000 |
| LDL (mg/dL) | 99.7 (37.8) | 85.7 (36.5) | 78.2 (35.7) | 0.000 |
| Triglycerides (mg/dL) | 153.7 (106.6) | 143.1 (85.2) | 157.6 (96.2) | 0.001 |
| HbA1C (%) | 6.8 (1.7) | 7.3 (1.8) | 7.2 (1.9) | 0.000 |
| Hgb (g/dL) | 13.7 (1.7) | 12.4 (2) | 10.7 (1.7) | 0.000 |
| MPV (fL) | 8.9 (1.2) | 9.1 (1.3) | 9.2 (1.3) | 0.000 |
| Plt (10^3/µL) | 232.2 (73.7) | 227.5 (86.1) | 221.8 (84.9) | 0.000 |
| Creatinine (mg/dL) | 0.9 (0.2) | 1.4 (0.3) | 4.3 (2.6) | 0.000 |
| Uric Acid (mg/dL) | 5.8 (1.5) | 7.2 (1.9) | 7.7 (2.7) | 0.000 |
| WBC (10^3/µL) | 8.7 (4.7) | 9.2 (9.4) | 8.6 (4.1) | 0.002 |
| Coronary intervention | ||||
| Acute MI (%) | 44.8 | 42.7 | 38 | 0.002 |
| STEMI (%) | 21.4 | 16.5 | 12.9 | 0.000 |
| ACS (excluding MI) (%) | 24 | 21.7 | 18.3 | 0.001 |
| CX_treated (%) | 30.6 | 30.8 | 34.1 | 0.183 |
| LAD_treated (%) | 48.3 | 46.2 | 42.8 | 0.009 |
| RCA_treated (%) | 32.4 | 28.1 | 29.1 | 0.000 |
| LM_treated (%) | 5.3 | 10.5 | 12.6 | 0.000 |
| Graft treated (%) | 2.1 | 5.6 | 5.7 | 0.000 |
| Multivessel PCI (%) | 10.3 | 10.2 | 12.2 | 0.308 |
| CTO treated (%) | 13.6 | 11.9 | 10.4 | 0.012 |
| DES (%) | 76.9 | 72.5 | 73 | 0.000 |
| DEB (%) | 2.9 | 3.3 | 3.3 | 0.494 |
| Radial approach (%) | 64.4 | 51.2 | 40.9 | 0.000 |
Abbreviations: DM – Diabetes Mellitus; HTN – Hypertension; COPD – Chronic Obstructive Pulmonary Disease; PVD – Peripheral Vascular Disease; CHF – Congestive Heart Failure; EF – Ejection Fraction; S/P CABG – Status Post Coronary Artery Bypass Grafting; AF – Atrial Fibrillation; Hx – History of (implied in “Prior Malignancy”, etc.); HDL – High-Density Lipoprotein; LDL – Low-Density Lipoprotein; HgA1C – Hemoglobin A1C; Hgb – Hemoglobin; MPV – Mean Platelet Volume; Plt – Platelets; WBC – White Blood Cells; MI – Myocardial Infarction; STEMI – ST-Elevation Myocardial Infarction; ACS – Acute Coronary Syndrome; CX – Circumflex Artery; LAD – Left Anterior Descending Artery; RCA – Right Coronary Artery; LM – Left Main Artery; Graft – Coronary Artery Bypass Graft; PCI – Percutaneous Coronary Intervention; CTO – Chronic Total Occlusion; DES – Drug-Eluting Stent; DEB – Drug-Eluting Balloon.
Table 2.
All-cause mortality, acute MI and TVR at 1 year and at 5 years in each CKD stage.
| Outcomes | Preserved kidney function (n=8781), % | Stage III (n=2063), % | Stage IV/V (n=645), % | p |
| Mon-fatal MI, TVR and all-cause mortality at 1y | 10.3 | 20.6 | 40.8 | 0.000 |
| All-cause mortality at 1y | 4 | 14.1 | 33 | 0.000 |
| MI at 1y | 5.8 | 7.1 | 10.5 | 0.000 |
| TVR at 1y | 2.4 | 2.3 | 3.3 | 0.387 |
| non-fatal MI and all-cause mortality at 1y | 9.4 | 20.1 | 40.2 | 0.000 |
| All-cause mortality at 5y | 10.5 | 33.3 | 57.2 | 0.000 |
| MI at 5y | 11.1 | 12.6 | 15.2 | 0.002 |
| TVR at 5y | 4.7 | 4.8 | 4.3 | 0.901 |
| Mon-fatal MI and all-cause mortality at 5y | 20.1 | 40.8 | 63.3 | 0.000 |
Abbreviations: MI – Myocardial Infarction; TVR – Target Vessel Revascularization; y- year.
Table 3.
Multivariable analysis for the composite outcome – all-cause mortality, MI and TVR at 1 year and at 5 years.
Table 3.
Multivariable analysis for the composite outcome – all-cause mortality, MI and TVR at 1 year and at 5 years.
| Variable | 1-year HR (95% CI) | p-value | 5-year HR (95% CI) | p-value |
| CKD Stage | ||||
| IV/V | 3.00 (2.58–3.49) | <0.001 | 2.78 (2.48–3.13) | <0.001 |
| III | 1.46 (1.29–1.65) | <0.001 | 1.49 (1.37–1.63) | <0.001 |
| Adjusted Variables | ||||
| Age (per year) | 1.018 (1.014–1.022) | <0.001 | 1.020 (1.017–1.022) | <0.001 |
| Female gender | 1.15 (1.03–1.28) | 0.015 | 1.07 (0.99–1.16) | 0.107 |
| Diabetes mellitus | 1.14 (1.03–1.27) | 0.010 | 1.27 (1.18–1.37) | <0.001 |
| MI or ACS (non-elective PCI) | 1.43 (1.29–1.60) | <0.001 | 1.17 (1.09–1.26) | <0.001 |
| Moderate-to-severe LV dysfunction | 1.76 (1.57–1.96) | <0.001 | 1.64 (1.52–1.78) | <0.001 |
| Atrial fibrillation | 0.92 (0.76–1.13) | 0.432 | 1.08 (0.95–1.23) | 0.218 |
| Peripheral vascular disease | 1.33 (1.09–1.63) | 0.005 | 1.56 (1.35–1.79) | <0.001 |
| COPD | 1.28 (1.10–1.48) | 0.001 | 1.36 (1.23–1.51) | <0.001 |
| Radial approach | 0.64 (0.58–0.70) | <0.001 | 0.76 (0.71–0.82) | <0.001 |
| Prior stroke | 1.23 (1.05–1.44) | 0.012 | 1.25 (1.12–1.40) | <0.001 |
| Congestive heart failure | 1.13 (0.98–1.31) | 0.101 | 1.32 (1.20–1.46) | <0.001 |
Abbreviations: ACS – Acute coronary syndrome; CKD – Chronic kidney disease; CI – Confidence interval; COPD – Chronic obstructive pulmonary disease; HR – Hazard ratio; LV – Left ventricular; MI – Myocardial infarction; PCI – Percutaneous coronary intervention; PVD – Peripheral vascular disease; TVR – Target vessel revascularization.
Table 4.
Multivariable analysis for all-cause mortality at 1 year and at 5 years.
| Variable | 1-year HR (95% CI) | p-value | 5-year HR (95% CI) | p-value |
| CKD Stage | ||||
| IV/V | 4.73 (3.90–5.73) | <0.001 | 4.13 (3.60–4.73) | <0.001 |
| III | 2.18 (1.85–2.58) | <0.001 | 2.15 (1.93–2.38) | <0.001 |
| Adjusted Variables | ||||
| Age (per year) | 1.03 (1.02–1.03) | <0.001 | 1.03 (1.03–1.03) | <0.001 |
| Female gender | 1.29 (1.11–1.49) | <0.001 | 1.20 (1.09–1.32) | <0.001 |
| Diabetes mellitus | 1.01 (0.88–1.16) | 0.913 | 1.20 (1.10–1.32) | <0.001 |
| MI or ACS (non-elective PCI) | 1.17 (1.01–1.35) | 0.032 | 0.97 (0.89–1.07) | 0.536 |
| Moderate-to-severe LV dysfunction | 2.46 (2.13–2.84) | <0.001 | 2.09 (1.90–2.30) | <0.001 |
| Atrial fibrillation | 0.58 (0.42–0.80) | <0.001 | 0.94 (0.80–1.10) | 0.422 |
| Peripheral vascular disease | 1.49 (1.17–1.90) | 0.001 | 1.78 (1.52–2.09) | <0.001 |
| COPD | 1.57 (1.31–1.88) | <0.001 | 1.64 (1.45–1.85) | <0.001 |
| Radial approach | 0.50 (0.44–0.58) | <0.001 | 0.68 (0.62–0.75) | <0.001 |
| Prior stroke | 1.17 (0.95–1.44) | 0.145 | 1.29 (1.13–1.48) | <0.001 |
| Congestive heart failure | 0.65 (0.51–0.83) | <0.001 | 1.06 (0.94–1.21) | 0.355 |
Table 5.
Multivariable analysis for MI at 1 year and at 5 years.
| Variable | MI at 1 year HR (95% CI) | p-value | MI at 5 years HR (95% CI) | p-value |
| CKD Stage | ||||
| IV/V | 1.83 (1.40–2.39) | <0.001 | 1.68 (1.35–2.09) | <0.001 |
| III | 1.06 (0.87–1.29) | 0.578 | 1.08 (0.93–1.26) | 0.292 |
| Adjusted Variables | ||||
| Age (per year) | 1.01 (1.00–1.01) | 0.147 | 1.00 (0.99–1.00) | 0.894 |
| Female gender | 1.02 (0.86–1.21) | 0.828 | 0.95 (0.83–1.08) | 0.407 |
| Diabetes mellitus | 1.31 (1.13–1.53) | <0.001 | 1.42 (1.27–1.59) | <0.001 |
| MI or ACS (non-elective PCI) | 2.02 (1.69–2.42) | <0.001 | 1.65 (1.46–1.87) | <0.001 |
| Moderate-to-severe LV dysfunction | 1.09 (0.91–1.32) | 0.350 | 1.13 (0.99–1.30) | 0.076 |
| Atrial fibrillation | 1.42 (1.11–1.83) | 0.006 | 1.48 (1.23–1.77) | <0.001 |
| Peripheral vascular disease | 1.07 (0.75–1.52) | 0.722 | 1.26 (0.98–1.63) | 0.072 |
| COPD | 0.95 (0.73–1.23) | 0.687 | 1.00 (0.83–1.21) | 0.979 |
| Radial approach | 0.77 (0.66–0.89) | <0.001 | 0.81 (0.73–0.90) | <0.001 |
| Prior stroke | 1.35 (1.07–1.72) | 0.013 | 1.25 (1.04–1.50) | 0.019 |
| Congestive heart failure | 2.00 (1.65–2.42) | <0.001 | 2.04 (1.77–2.35) | <0.001 |
Abbreviations: ACS – Acute coronary syndrome; CKD – Chronic kidney disease; CI – Confidence interval; COPD – Chronic obstructive pulmonary disease; HR – Hazard ratio; LV – Left ventricular; MI – Myocardial infarction; PCI – Percutaneous coronary intervention; PVD – Peripheral vascular disease; TVR – Target vessel revascularization.
Table 6.
Multivariable analysis for TVR at 1 year and at 5 years.
| Variable | 1-yearHR (95% CI) | p-value | 5-yearHR (95% CI) | p-value |
| CKD Stage | ||||
| IV/V | 1.16 (0.73–1.85) | 0.530 | 1.08 (0.73–1.60) | 0.714 |
| III | 0.74 (0.53–1.04) | 0.084 | 0.97 (0.76–1.23) | 0.774 |
| Adjusted Variables | ||||
| Age (per year) | 1.01 (1.00–1.02) | 0.077 | 1.00 (0.99–1.01) | 0.894 |
| Female gender | 0.85 (0.64–1.13) | 0.267 | 0.82 (0.66–1.02) | 0.069 |
| Diabetes mellitus | 1.88 (1.47–2.41) | <0.001 | 1.77 (1.48–2.11) | <0.001 |
| MI or ACS (non-elective PCI) | 1.49 (1.15–1.95) | 0.003 | 1.18 (0.98–1.42) | 0.073 |
| Moderate-to-severe LV dysfunction | 1.22 (0.92–1.63) | 0.169 | 1.06 (0.85–1.33) | 0.589 |
| Atrial fibrillation | 1.14 (0.75–1.75) | 0.534 | 1.40 (1.05–1.88) | 0.022 |
| Peripheral vascular disease | 0.79 (0.42–1.49) | 0.464 | 1.12 (0.74–1.69) | 0.598 |
| COPD | 0.95 (0.64–1.43) | 0.823 | 0.96 (0.71–1.30) | 0.787 |
| Radial approach | 0.81 (0.63–1.02) | 0.077 | 0.93 (0.78–1.10) | 0.382 |
| Prior stroke | 1.58 (1.10–2.26) | 0.012 | 1.44 (1.09–1.90) | 0.010 |
| Congestive heart failure | 2.16 (1.60–2.91) | <0.001 | 1.96 (1.56–2.45) | <0.001 |
Abbreviations: ACS – Acute coronary syndrome; CKD – Chronic kidney disease; CI – Confidence interval; COPD – Chronic obstructive pulmonary disease; HR – Hazard ratio; LV – Left ventricular; MI – Myocardial infarction; PCI – Percutaneous coronary intervention; PVD – Peripheral vascular disease; TVR – Target vessel revascularization.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



