
Submitted:
20 November 2025
Posted:
21 November 2025
You are already at the latest version
Abstract
Drug-resistant epilepsy (DRE) remains a major therapeutic challenge, as a considerable proportion of epilepsy patients fail to achieve seizure control with conventional anti-seizure medications or surgical therapy. Closed-loop systems have emerged as a promising alternative, offering patient-specific, on-demand neuromodulation. Despite notable advances in the academic domain, clinical translation has stagnated, and surgical resection remains the intervention with the highest probability of achieving seizure freedom. In this review, we delineate the principal limitations currently constraining progress in epilepsy neuromodulation and conceptualise these systems as instantiations of the read-write architecture characteristic of brain-computer interfaces. The read component entails the continuous acquisition and analysis of neurophysiological signals to predict or detect imminent seizures. In contrast, the write component involves the delivery of targeted interventions to disrupt epileptiform dynamics and prevent clinical seizure manifestation. We outline the closed-loop processing pipeline, survey the current state of the art, and discuss key methodological and translational challenges, particularly in algorithm validation and long-term reliability. Finally, we address patients’ and caregivers’ perspectives on the acceptance and practical integration of such technologies. This work synthesises current advances in the field and delineates the path toward fully autonomous clinically effective closed-loop neuromodulation as a viable treatment paradigm for DRE, aiming to improve patients’ quality of life.
Keywords:
drug-resistant epilepsy
; seizure prediction
; seizure detection
; closed-loop
; brain-computer interface
1. Introduction
Epilepsy stands as a chronic, noncommunicable neurological disorder affecting approximately 50 million individuals globally, ranking among the most common neurological conditions [1]. It is fundamentally characterised by the recurrent seizures, arising from sudden, excessive electrical discharges within neuronal clusters in the brain. While a single seizure does not constitute epilepsy, a formal diagnosis is established upon experiencing two or more unprovoked seizures [2].
Drug-resistant epilepsy (DRE) is a major clinical challenge [2,3], defined by the ILAE as the failure to achieve sustained seizure freedom after adequate trials of two or more appropriately chosen and tolerated anti-seizure medications (ASMs) [2]. While many patients respond to ASMs, 30–40% develop DRE [4,5], representing a high-risk population [6,7,8]. Risk varies with age and epilepsy type: early-onset epilepsy strongly associates with DRE [9,10,11], whereas adult-onset cases linked to progressive disorders or cortical lesions are also prone to pharmacoresistance [12,13,14,15,16,17,18], with focal epilepsies carrying particularly high risk [19,20,21,22].
DRE imposes significant economic and societal burdens [22,23,24,25], exacerbated by psychiatric comorbidities [26,27] and social marginalisation [28,29]. Families and caregivers experience emotional, financial, and social strain [30,31,32,33,34], and care demands are higher than for pharmacoresponsive patients [35,36,37]. In high-income countries, direct healthcare costs may be 2–10 times higher, up to €9,000 per patient per year [37,38,39], while limited treatment access in low- and middle-income countries worsens socioeconomic impact [40,41].
Resective surgery of the epileptogenic zone remains the most established alternative after ASM failure [42,43], with durable seizure freedom achieved in 50% of focal neocortical and two-thirds of temporal lobe epilepsy patients when the epileptogenic network is accurately identified [44,45,46,47,48,49,50,51].
For patients unsuitable for resection, neuromodulation systems offer complementary strategies [52,53], delivering interventions that prevent generation or disrupt ongoing seizures[54,55].
As of today, only a limited number of neuromodulatory therapies are commercially available and approved in both the European Union and the United States (see Table 1). These include the Responsive Neurostimulation System (RNS) [56], Vagus Nerve Stimulation (VNS) [57,58], Deep Brain Stimulation of the Anterior Thalamus (DBS) [59,60], and External Trigeminal Nerve Stimulation (eTNS). Among them, DBS, eTNS, and the first-generation VNS operate under an Open-Loop System (OLS) architecture (Figure 1A), wherein stimulation parameters are predefined and delivered independently of ongoing neural activity. In contrast, RNS and the latest VNS iterations [61,62] implement a Closed-Loop System (CLS) architecture (Figure 1B), integrating continuous monitoring of brain—or surrogate—signals to predict or detect seizures and deliver temporally precise interventions [63,64,65].
Recent developments have introduced the concept of Adaptive Deep Brain Stimulation (aDBS) [66,67], an evolution of conventional DBS that integrates feedback-driven modulation. Notably, Medtronic’s Percept™ PC, although currently operating as an open-loop device, has the technical capability to operate in a closed-loop framework. Other experimental approaches, such as Repetitive Transcranial Magnetic Stimulation (rTMS) and Transcranial Direct Current Stimulation (tDCS) [68], were initially conceived as OLS modalities but are increasingly being adapted to CLS frameworks [69,70,71]. Collectively, these trends reflect a decisive shift in neuromodulation research towards CLS paradigms, aiming to achieve patient-specific, autonomous, and dynamically responsive therapy. Such systems hold the promise of enhancing efficacy, minimising adverse effects, and optimising long-term therapeutic outcomes.
With respect to their mechanism of action, current evidence supports two forms of stimulus-driven modulation. The first is direct suppression of electrographic seizure patterns (ESPs), wherein triggered electrical stimulation inhibits an ongoing seizure, consistent with the classical understanding of RNS. The second is direct frequency modulation, a recently described phenomenon in which stimulation reshapes the spectral content of ESPs [72]. Notably, in both modalities, the therapeutic benefits of CLS seem to emerge through progressive adaptations within the seizure network, rather than through the immediate termination of individual ictal events, suggesting a potential disease-modifying mechanism [55]. Then, crucially, the therapeutic efficacy of CLS-based neuromodulation depends on constant accurate state detection or prediction, enabling the precise delineation of the temporal window during which patient-specific interventions can effectively be administered. From a technical standpoint, CLS architectures intended for clinical deployment represent a specialised subclass of Brain–Computer Interfaces (BCIs), as they continuously acquire neural signals and translate them into adaptive therapeutic outputs without requiring human supervision or explicit user control.
However, the efficacy of available neuromodulation BCIs in epilepsy remains fundamentally palliative rather than curative [76,77,78,79]. For instance, while RNS achieves significant seizure frequency reductions (50–70%), durable seizure freedom rates remain low (8.7–21.1%) [80,81,82,83]. Similar outcomes are reported for VNS (6.9–11%) [84,85,86] and DBS (1.32–8.9%) [82,83,87,88,89]. It should also be noted that the definition of seizure freedom varies between studies, with many adopting the criterion of no seizures for at least one year. While clinically meaningful, such an interval does not constitute true long-term seizure freedom if relapse subsequently occurs. Nevertheless, these findings underscore that surgical resection of the epileptogenic tissue offers a markedly superior, potentially curative outcome, with long-term seizure-freedom rates of approximately 50–66%, as previously noted.
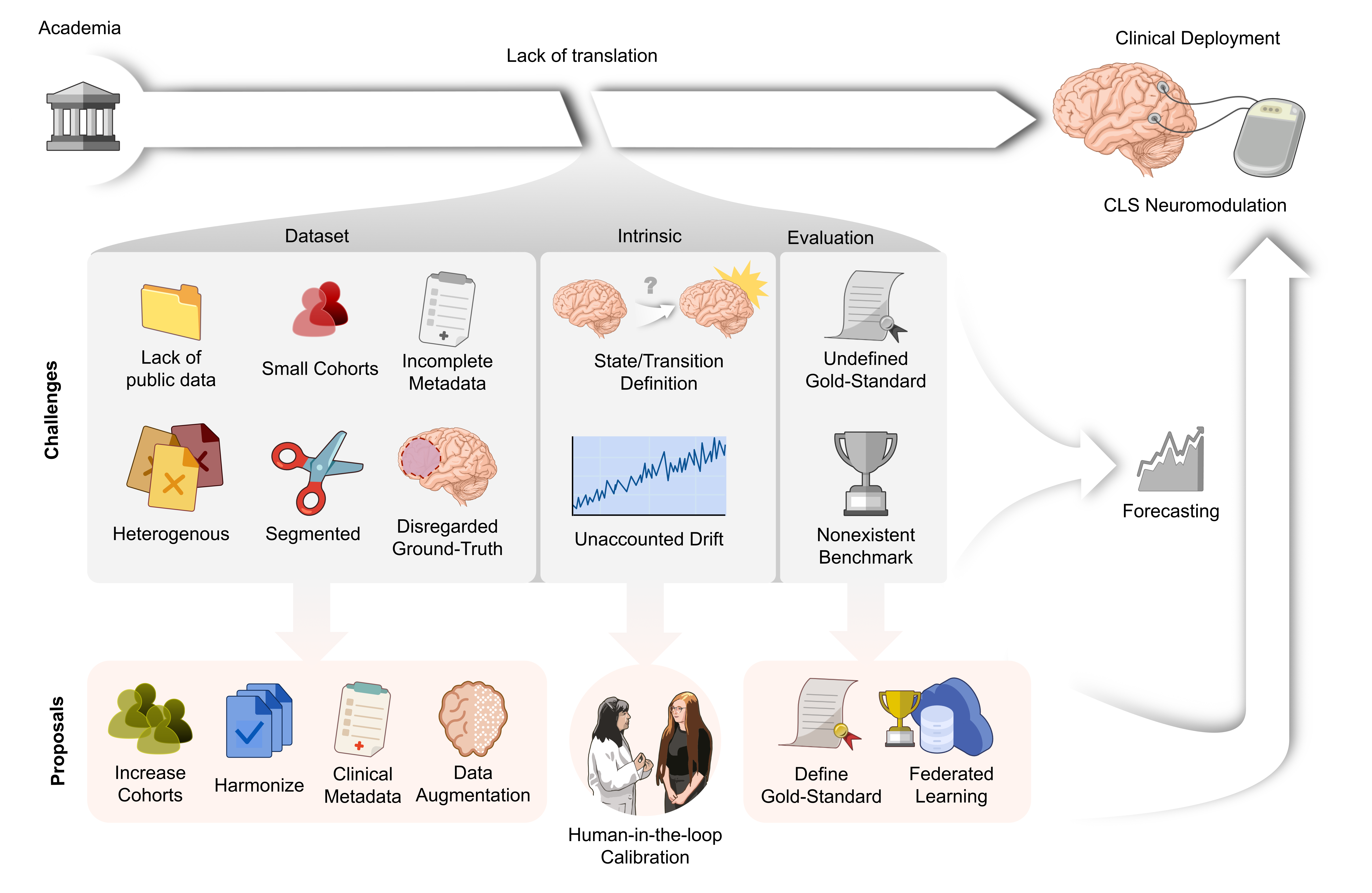
Therefore, the core research problem, and the underlying motivation for this review, is to examine why seizure detection and prediction systems, despite their sophistication and their classification as a type of BCI reacting to precise patterns of brain activity, have failed to reach the durable curative efficacy benchmark often achieved by successful surgical resection. This stagnation indicates that significant fundamental challenges persist within the translational pathway from research to clinical deployment. This review will explore persistent bottlenecks, including data limitations and methodological shortcomings in performance evaluation.
2. The Plateau of Clinically Deployable Devices
To date, the RNS and modern applications of VNS (i.e., AspireSR®) remain the only commercially available CLS devices for epilepsy to have received approval from the US FDA and to be CE-marked in the European Union. Since their approval in 2013 and 2014, respectively, they have stood as the sole clinically established therapies routinely implemented for seizure modulation and prevention in patients with DRE. Although several other CLS systems have advanced to clinical or investigational trials in the intervening years, none has yet achieved regulatory approval.
Given the considerable time elapsed since the introduction of RNS and VNS, it becomes evident that progress in neuromodulation through seizure detection and prediction has advanced more slowly than initially anticipated, especially considering that state-of-the-art algorithms now surpass these systems in performance. Sisterson et al. [90] reported that RNS achieved a mean accuracy of 90.0% (interquartile range 84.3–98.8%, range 63.0–100%), sensitivity of 51.5% (interquartile range 48.7–50.1%, range 0–100%), and specificity of 93.2% (interquartile range 90.6–99.6%, range 64.5–100%). However, they observed substantial inter-patient variability in detector accuracy and noted that results were highly dependent on manually pre-defined thresholds. The authors also cautioned that the device’s limited onboard storage allows only a small fraction of recordings to be retained, such that the derived performance summaries may misrepresent true sensitivity and specificity. Regarding CLS-VNS, Boon et al. [91] reported that multiple detector configurations achieved sensitivities ≥80%, but only for seizures accompanied by heart-rate increases, and that false positive rates ranged from approximately 0.5 to 7.2 events per hour, depending on the tachycardia threshold employed. Similarly, Fisher et al. [92] found that merely 34.8% of recorded seizures were actually treated by the VNS device. Despite these limitations, recent reviews of seizure detection and prediction algorithms demonstrate that numerous contemporary approaches perform on par with, or even exceed, the capabilities of RNS and VNS [54,93,94,95]. Nevertheless, these advances have yet to translate into clinical adoption.This stagnation suggests that fundamental scientific and translational challenges remain unresolved, and that key bottlenecks persist along the pathway from research to clinical application.
Rather than directly addressing the core challenges, the seizure detection and prediction community progressively shifted its emphasis from real-time brain state identification towards more probabilistic or circadian-based forecasting of seizures [96]. In this paradigm, the objective is no longer to classify discrete brain states but instead to estimate the likelihood of a seizure occurring within a given time window. While such forecasts can offer valuable clinical benefits, enabling patients to take safety precautions or find a secure location, they are fundamentally incompatible with a proper BCI architecture. The inherent imprecision of these forecasts makes them unsuitable for defining the sharp limits required to close the therapeutic loop in BCIs, whose core purpose is to provide autonomous and automated therapeutic intervention.
A prominent example of this forecasting approach was the NeuroVista Seizure Advisory System, an implantable device that forecasted seizures based on continuous intracranial EEG (iEEG) recordings [97]. The system transmitted neural data wirelessly from cortical electrodes to an external receiver that generated warnings of impending seizures. In the pivotal Melbourne trial, the device achieved predictive performance above chance in a subset of patients, yielding clinically useful forecasts in approximately half of the cohort. However, for several participants, the system proved ineffective, either failing to generate timely warnings or producing excessive false alarms. These mixed outcomes, combined with practical limitations such as device maintenance requirements and dependence on a handheld receiver, ultimately led to the termination of both the trial and the sponsoring company.
Following the trial’s discontinuation, the collected data were released as part of the Melbourne University AES/MathWorks/NIH Seizure Prediction Challenge on Kaggle. Many community-developed algorithms improved average sensitivity 1.9 times with respect to the original NeuroVista model, particularly in the most challenging patient cases [98]. Building on this achievement, the organisers established the platform Epilepsyecosystem.org, which serves as a collaborative hub for data and algorithm sharing, fostering a crowdsourced approach to advancing seizure prediction research.
Despite these advances, it is noteworthy that the enhanced algorithmic performance did not translate into renewed clinical development of the NeuroVista system. This outcome suggests that, even with substantial methodological progress, the forecasting paradigm alone may be insufficient to address the broader challenge of effective closed-loop seizure control. A likely explanation is that probabilistic forecasting, by definition, cannot specify the precise real-time intervention windows required for a genuine CLS. The effectiveness of such systems hinges on accurately identifying the temporal intervals during which stimulation must be delivered to prevent or interrupt seizure onset. While forecasting may hold potential for patient warning systems or wearable alert devices, this inherent functional limitation may preclude its application as a true epilepsy BCI.
3. Scarcity of Complete Public Datasets
The fundamental prerequisite for the successful development of BCIs is the availability of high-quality, large-scale datasets. It is well established that large datasets are advantageous for training deep learning models as they provide the statistical power required to capture the variability of brain signals both within and across subjects, contexts, and recording environments [99,100]. Such variability is essential to design BCIs that function reliably outside controlled laboratory conditions.
However, dataset quality and relevance are equally important. For instance, early-stage development of novel signal processing methods can often be undertaken successfully using smaller, more focused datasets [101]. Several studies have demonstrated that even relatively small EEG/ECoG datasets can train effective BCI decoders, especially when the recorded features are well-defined and consistent across sessions or subjects [102,103,104]. Nevertheless, when developing robust real-world systems capable of adapting to diverse users and environments, the availability of larger and more heterogeneous datasets becomes critical [105].
Beyond the sheer volume and fidelity of recordings, contemporary BCI development emphasises the adoption of standardised data formats, such as the Brain Imaging Data Structure (BIDS) and its extensions for EEG and MEG, as well as adherence to open data principles [106,107]. Implementing community standards such as BIDS, in combination with containerised BIDS-Apps and standardised preprocessing pipelines, enhances data interoperability, reproducibility, and the portability of analysis workflows across research sites [108,109].
In contrast to these general trends in BCI research, one of the principal obstacles to epilepsy-oriented BCIs is the scarcity of publicly accessible datasets for seizure detection and prediction [110,111]. The existing datasets often lack a consistent format, needing time-consuming harmonisation efforts before any comparative analysis. In some cases, harmonisation is impossible due to incompatible acquisition protocols or incomplete metadata.
The aforementioned NeuroVista clinical trial represents a pivotal, albeit underexploited, milestone. It demonstrated that open data and crowdsourcing can serve as powerful catalysts for biomedical innovation, even in a condition as complex and heterogeneous as epilepsy. Despite this compelling proof of concept, epilepsy research has not fully embraced open-data practices comparable to those driving progress in motor and language BCIs.
3.1. Current Available Datasets
To systematically assess the availability of electrophysiological datasets for epilepsy research, a literature review was conducted using PubMed, IEEE Xplore, and Google Scholar. The search strategy employed the terms [(epilepsy[Title/Abstract]) AND (dataset[Title/Abstract])]. Peer-reviewed publications, institutional repositories, data-sharing platforms (e.g., PhysioNet, Kaggle, EBRAINS), and personal communication with dataset authors were examined to identify relevant resources.
Datasets were included if they met the following criteria: (i) they contained patient-level electrophysiological recordings of seizures; and (ii) they were publicly accessible, either directly or free of charge upon request.
For each identified dataset, the following characteristics were extracted: (1) cohort size (N); (2) age group of participants, categorised as adult or paediatric; (3) recording duration per patient (L); (4) inclusion of DRE patients; (5) availability of information on the resected brain area in cases where surgery had been performed; (6) presence of longitudinal follow-up data when applicable; (7) the neuroimaging or electrophysiological modality used for data acquisition; and (8) the information disclosed in the metadata, if available.
A total of 11 datasets were identified. A summary of the reviewed datasets and their characteristics is presented in Table 2.
Among the available datasets, cohort sizes are generally adequate for academic research (mean = 45.27, SD = 42.11, median = 23), yet remain insufficient for clinical trials. The required sample size in such trials depends on factors including the primary endpoints, expected effect size, and statistical power, which vary considerably across studies. Nevertheless, pivotal (registration) trials typically enroll around 200 participants [122,123]. This requirement may be even higher for Class-III (high-risk) implantable devices, where both safety and efficacy must be demonstrated across heterogeneous populations.
Regarding age groups, five datasets included only adult participants, three included both adult and paediatric patients, and three did not disclose participant’s ages. This distinction is relevant, as age strongly influences both epilepsy prevalence and the probability of developing drug resistance.
Recording duration per patient (L) was highly heterogeneous, ranging from 1 minute to 183.8 days. Notably, six of the eleven datasets provided continuous long-term recordings, whereas the remaining five contained preselected clips.
Most datasets (8/11) focused exclusively on patients with DRE. Only three datasets reported information on resected brain regions following presurgical evaluation. Of these, just two included follow-up data to verify whether surgery was successful, thereby confirming whether the epileptogenic network had been resected or at least impaired.
Regarding recording modalities, four datasets were acquired using scalp EEG, two using SEEG, two using SEEG or ECoG, one combining SEEG and ECoG, one using iEEG, and one employing a multimodal wearable system including behind-the-ear EEG, ECG, EMG, and movement sensors (accelerometer and gyroscope).
The availability of patient-level metadata also varied considerably. Four datasets provided complete anonymised clinical and demographic information; three included no metadata at all; one contained age, sex, and seizure classification; one provided age and sex; one reported only sex; and one included only the putative seizure onset zone (SOZ) as defined by clinical staff.
3.2. Why Is It So Difficult to Find Data?
Strictly speaking, the challenge does not lie in the existence of data but in its availability for sharing. Hospitals with epilepsy monitoring units routinely collect highly valuable long-term recordings of their patients, together with the associated clinical metadata required for research. There is evidence that data are collected and stored but under-utilized due to ethical/regulatory constraints, despite the willingness of many centres and patients to collaborate with researchers [124,125,126].
The principal barrier in many jurisdictions arises from ethical and regulatory constraints. In the European Union, patient information cannot be shared without explicit consent, which must often be obtained anew for each study [127]. Moreover, regulations differ substantially across jurisdictions: data that may be shared or accessed in one country may be subject to strict limitations in another [128]. This represents a significant setback, as vast quantities of clinically rich data remain effectively inaccessible [129]. Nonetheless, these regulatory frameworks play a crucial role in safeguarding patient information and ensuring anonymity [130].
4. Intrinsic Limitations
Having examined the limitations of publicly available datasets, several fundamental questions arise about how these datasets are defined and the assumptions that guide their use. The first pertains to how we conceptualise and delineate brain states, while the second concerns the expectations we hold regarding the dynamical activity of the epileptic brain.
4.1. State Definition
Although the existence of four principal brain states in epilepsy (interictal, preictal, ictal, and postictal) is widely recognised, precise definitions lack. This ambiguity represents a significant limitation for epilepsy-oriented BCIs, as accurate labelling of signal features is critical for successful system development. For instance, in language BCIs, the neural states to be identified are temporally well delineated, typically corresponding to spoken words or their cognitive representations. Similarly, in motor BCIs, the relevant states are clearly defined in time, reflecting the intention to execute a movement. These fields benefit from the ability to interact directly with participants, enabling the precise annotation of event onsets and offsets. Moreover, an extensive body of literature provides empirical evidence concerning the spatiotemporal organisation of language and motor functions in the brain. In contrast, temporal boundaries of epileptogenic brain activity remain imprecise, with multiple theoretical frameworks proposed and no definitive consensus achieved to date.
- The ictal state is the least controversial and the most clearly delineated [131,132]. Clinical experts have established behavioural and pathophysiological criteria that mark the onset and termination of seizures [133]. Minor discrepancies among clinicians are generally acceptable, and the community relies on these timepoint annotations as the de facto ground truth [134,135].
- In contrast, the preictal and postictal states are ambiguous [96,136]. For the preictal state, there is no agreement regarding its temporal onset. Proposed definitions range from minutes to hours, days, or even months before seizure onset [137,138,139,140,141,142]. Its underlying dynamics also remain unclear, both in terms of whether preictal states share common features across individuals with DRE, and whether a single patient experiences seizures preceded by distinct preictal patterns [142,143,144]. Pre-ictal definition relies on the seizure onset, however, it is possible that some preictal states never reach seizure transition due to regulatory brain activity. In these cases, an algorithm might correctly detect the pre-ictal state, but due to the lack of ground truth it would be regarded as a false positive.
- Finally, the interictal state is often defined simply as all remaining periods outside the preictal, ictal, or postictal windows. It is inherently dependent on the delineation of seizure-related states, and consequently liable to error.
4.2. Long-Term Changes in Brain Dynamics
Most existing methods for brain-state classification in DRE assume that brain dynamics remain relatively stable over time. Within this framework, training an algorithm on previously acquired samples is expected to ensure reliable classification of future instances. In practice, this entails developing models on a bounded portion of patient data, with the expectation that their performance will generalise across subsequent periods.
This assumption, however, is at odds with biological reality. Brain dynamics are inherently non-stationary and evolve over time, both in epilepsy and in healthy function. It is well established that neural activity patterns exhibit gradual changes, a phenomenon known as drift [145]. Drift can degrade decoding performance, so BCIs in other domains employ adaptive algorithms to dynamically adjust to changes in neural signals in real time, by continuously updating decoding parameters.
In epilepsy, evidence for non-stationarity is even more compelling. Seizures induce recurrent reorganisation of brain networks, progressively worsening the disorder when left untreated [146,147,148]. Pre-ictal variability in functional connectivity distinguishes seizure types in mesial temporal lobe epilepsy (TLE) [149], and TLE patients exhibit accelerated dynamics and increased temporal instability relative to healthy controls with DRE showing greater temporal variability [150]. This indicates that seizure generation dynamics are drifting rather than remaining stationary. Furthermore, models that adapt to concept drift in EEG over long recordings significantly outperformed static models [151]. Nevertheless, most existing algorithms are designed under the assumption of data stability and consequently underperform when confronted with the evolving nature of real-world data.
5. The Depth-Breadth Dilemma
Broadly speaking, research in seizure detection and prediction has followed two dominant methodological paradigms: (1) patient-independent (or general) algorithms, designed to operate across diverse patient populations, and (2) patient-specific algorithms, tailored to the neurophysiological patterns of individual patients [152,153,154]. Both approaches have merits and limitations, and both continue to be actively explored in the field.
5.1. Breadth: General Paradigm
The breadth-oriented strategy aims to develop a “one-size-fits-all” solution by training models on large, heterogeneous datasets comprising recordings from multiple patients. The goal is to identify generalisable neural features that can signal or predict seizures across individuals. These models are often based on deep learning, designed to operate in previously unseen patients with minimal or no retraining [155,156].
The principal advantage of this approach lies in its scalability. A single validated model could, in principle, be deployed across diverse clinical settings without the need for extensive patient-specific optimisation. Moreover, such models require substantially less data per patient, particularly valuable in cases of infrequent seizures [156,157].
However, epilepsy is profoundly heterogeneous in seizure morphology, onset dynamics, and background activity. General models struggle to capture these patient-specific features, resulting in reduced sensitivity and specificity [158,159,160]. The high degree of inter-patient variability remains a fundamental limitation of the general-oriented paradigm.
5.2. Depth: Patient-Specific Paradigm
In contrast, depth-oriented approaches focus on training algorithms uniquely for each patient. These models learn the individual’s specific electrophysiological “fingerprint” during interictal, preictal, and ictal states, and frequently achieve superior performance in accuracy, sensitivity, and reliability [161,162].
Nevertheless, training such models requires substantial patient-specific data, typically multiple recorded seizures and long interictal/preictal recordings to capture the relevant features and account for variability over time [163]. This limits clinical applicability, especially for patients with infrequent seizures. Moreover, patient-specific models lack generalisability, as a model trained on Patient A generally does not perform well for Patient B.
It is important to emphasise, however, that most current BCI systems prioritise subject-specific strategies rather than adopting a general approach due to inter-individual variability in electrophysiological patterns. Decoding accuracy and system responsiveness are strongly influenced by user-dependent neural characteristics [164,165,166] . Workflows rely on tailoring feature extraction, frequency band selection, and adaptive protocols to the individual [166,167]. Such personalised designs have been consistently shown to improve performance, speed, and reliability across both medical and non-medical BCI applications [168,169].
5.3. Prevailing Trends and Emerging Solutions
Although both paradigms remain under investigation, the field tends to converge on the view that patient-specific algorithms consistently outperform general models.
A hybrid strategy has recently gained traction in the form of transfer learning, which aims to reconcile the advantages of both approaches [163,170,171]. In this paradigm, models are first pre-trained on large, heterogeneous datasets and subsequently fine-tuned using small amounts of patient-specific data. Transfer learning thus offers a pragmatic compromise, enhancing scalability while retaining a degree of personalisation necessary for clinically reliable seizure prediction and detection. Nevertheless, direct subject-specific modelling continues to outperform hybrid methods in many practical scenarios where individual variability exerts a dominant influence on system performance.
6. Methodological Issues in Performance Evaluation
A persistent challenge in the field is the absence of a standardised system for assessing and benchmarking detection and prediction algorithms [172].
The choice of validation strategy determines the performance estimates, as even subtle variations in data segmentation or metric computation can yield markedly different outcomes for the same algorithm [173,174,175]. Most top-performing approaches employ cross-validation (CV) schemes commonly used in machine learning (Figure 2A), in which data are typically divided into an 80/20 train–test split, sometimes combined with k-fold or leave-one-(seizure)-out cross-validation (LOOCV). Shafiezadeh et al. [175] demonstrated the limitations of this framework, showing that random 5-fold CV can inflate performance, improving accuracy by nearly 30% compared with LOOCV. Similarly, Pale et al. [173] reported that algorithms achieved up to a 7% higher F1 score under LOOCV than under time-series cross-validation (Figure 2B), an evaluation strategy that preserves the chronological structure of the data by ensuring that training always precedes testing in time. Both studies highlight that training on excessive or distant data can lead to overestimation of performance and should be avoided. In practice, once deployed, algorithms must contend with patient-specific variability and unseen dynamics not represented in the training set. This methodological disconnect likely contributes to the persistent gap between algorithmic advances and their clinical translation [176].
Although no gold-standard benchmarking system currently exists, some efforts are underway. In seizure detection, one notable initiative is SzCORE (Seizure Community Open-Source Research Evaluation framework for the validation of EEG-based automated seizure detection algorithms) proposed by Jonathan Dan and colleagues [177]. By contrast, in seizure prediction, the definition of a standard validation framework is stagnated by the lack of consensus on preictal state definition [178].
But even in frameworks such as SzCORE, several parameters remain at the discretion of research teams. These include, for example, the permitted overlap between ground-truth and predicted events, the tolerance for onset/offset alignment, and constraints on event duration. While such flexibility permits diverse applications of seizure detection algorithms, it simultaneously undermines comparability across studies. At present, the field lacks a universal method for empirically measuring and directly comparing algorithm quality.
7. Discussion
In this review, we have identified and critically examined the key factors that have hindered the advancement of epilepsy-related BCIs. Building on this analysis, the following discussion presents concrete strategies to overcome these obstacles and accelerate the translation of research outcomes into clinical practice. We also delineate those limitations that, in our assessment, are likely to persist despite current technological and methodological capabilities. We propose reforms in data acquisition and processing, a conceptual reframing of epileptic brain dynamics, and the redesign of epilepsy-oriented BCI systems and evaluation protocols to foster genuine clinical impact.
7.1. Dataset Improvement
7.1.1. Increasing Cohort Sizes
Given the high global prevalence of epilepsy, we argue that existing datasets should be substantially expanded. Enlarging cohort sizes would enhance diversity and statistical representativeness, thereby facilitating the development of models and enabling a more rigorous study of inter-individual variability.
The acquisition of electrophysiological data from patients with DRE, however, is time-consuming and constrained by clinical circumstances, as recordings can only be obtained from hospitalised patients undergoing evaluation. One potential strategy to mitigate the limitation of small cohort sizes is to aggregate data from multiple sources. Yet, as discussed in previous sections, public datasets remain markedly heterogeneous, often to the extent that merging two datasets becomes infeasible, even when similar recording modalities are employed.
Although many hospitals express willingness to share anonymised patient data, stringent regulatory frameworks prohibit the transfer of datasets beyond their hosting institutions without explicit participant consent, particularly within the European Union. These constraints are expected to become even more restrictive in the future. In such contexts, federated learning may offer a promising alternative by enabling collaborative model training without exchanging raw data. Nevertheless, this approach demands rigorous compliance with cybersecurity and data governance standards to ensure its safe and lawful implementation.
In any case, both data aggregation and federated learning depend on the adoption of harmonised standards. Existing and newly generated datasets should conform to interoperable structures that facilitate seamless integration. A set of proposed requirements to support such harmonisation is presented in the following sections.
7.1.2. Mimicking Real-Life Data
Datasets employed in academic research cannot realistically match the scale of those used in clinical trials or real-world practice, as doing so would substantially increase both the time and financial costs of research. Nonetheless, for neuromodulation systems to be effective, they must be trained on data that approximate real-world conditions [179].
The duration of recordings must be sufficient to capture the dynamic nature of brain states. Approximately half of the datasets presented in this review consist of only short segments surrounding seizures. Such restricted windows fail to reflect the broader temporal variability of brain activity, particularly interictal fluctuations. Ideally, datasets should encompass the whole clinical monitoring period, with a minimum duration of 24 hours. Longer recordings are especially valuable, as they permit the study of multiday rhythms and infrequent events that may play a crucial role in seizure generation.
Where continuous long-term acquisition is impractical, it is important to recognise that seizures are relatively rare in real-world settings. Consequently, datasets should reflect this natural imbalance rather than artificially balancing interictal, preictal, and ictal samples. Preserving the natural overrepresentation of interictal periods enables models to extract more meaningful discriminative features of the preictal and ictal states, while also mirroring the event distribution observed in clinical practice.
A complementary strategy to address data scarcity is the use of data augmentation techniques, generating modified variants of existing recordings to artificially diversify datasets. Well established in other BCI domains, such approaches enhance generalisability, improve performance, and reduce overfitting. In the context of EEG, commonly applied augmentation strategies include temporal manipulations (e.g., time-warping, random cropping, or jittering), frequency-domain transformations (e.g., spectral scaling or filtering), and noise-based methods (e.g., Gaussian noise injection or channel dropout). More advanced approaches employ generative models such as variational autoencoders or generative adversarial networks (GANs) to synthesise physiologically plausible signals, increasing dataset diversity.
7.1.3. DRE Focus
Seizure freedom efforts are most clinically relevant when targeted at patients with DRE, for whom current treatments have failed. The mechanisms of seizure generation in DRE are likely to differ from those of drug-responsive patients, thus requiring dedicated investigation.
7.1.4. Metadata
Demographic and clinical metadata are frequently absent or incomplete in publicly accessible datasets, yet are essential for contextualising the electrophysiological recordings and stratifying modelling approaches. For instance, several paediatric epileptic syndromes remit spontaneously with age, so aggregating paediatric and adult recordings introduces confounding variability, biases statistical inference, and may obscure clinically meaningful network patterns.
We therefore advocate for the mandatory inclusion of, at minimum, the following metadata attributes: patient age, sex, ethnicity, epilepsy syndrome, preoperative Engel classification, indication of whether resective surgery was performed, and postoperative Engel outcome at -year follow-up, as multiple studies show that seizure recurrence after epilepsy surgery is concentrated in the first 2-3 years, and that the probability of relapse declines and becomes more stable beyond that period (i.e., after 3-5 years post-surgery) [180,181,182,183,184,185].
In addition, comprehensive access to the structured content of patients’ clinical records would be highly desirable to mitigate unobserved confounders (smoking habits, alcohol consumption, prior brain lesions, comorbid neurological and psychiatric conditions) that may influence neurophysiological dynamics [186,187,188]. Although there are practical barriers due to the unstructured, free-text nature of clinical documentation, large language models (LLMs) offer a promising avenue for automated information extraction. These systems could convert narrative reports into standardised metadata suitable for research workflows. However, such an approach must strictly comply with data protection frameworks (e.g., GDPR, HIPAA) and undergo rigorous validation to ensure both semantic accuracy and reliability before deployment in clinical or research contexts.
7.1.5. The Surgical Resection as an Additional Ground Truth
Epilepsy surgery to remove the pathological tissue is the most common treatment for DRE. Although knowledge of the removed area and postsurgical outcomes is not required for BCI development, it provides a clinical “ground truth” for localising the seizure onset zone and allows researchers to investigate network dynamics within and around the epileptogenic region. Postoperative follow-up at 3 to 5 years indicates whether or not the surgical resection captured the SOZ, as mentioned in the previous section. This is particularly relevant when invasive imaging techniques are employed, targeting a brain area preselected by clinical staff, as clinicians may fail to identify the true SOZ in approximately 50% of cases. Post-resection follow-up, therefore, provides researchers with crucial information on whether the SOZ was indeed captured in the available recordings. Moreover, such data enable a more rigorous sub-selection of relevant signals, for example by restricting analyses to electrodes located within the SOZ.
7.2. Overcoming Intrinsic Limitations
7.2.1. Goal-Oriented State Definition
Given that the definition of the preictal state remains unresolved, two possible strategies can be considered. The first, and most systematic, is to prioritise research aimed at delineating the temporal and physiological boundaries of DRE brain states. Pursuing this path may delay the development of epilepsy BCIs.
Alternatively, BCIs could be developed concurrently by defining brain states in terms of the intended therapeutic goal. For instance, if a system is designed to deliver therapy within five minutes of seizure onset, the preictal state could be defined as the five-minute interval preceding seizure onset. Still, the optimal timing for intervention to effectively prevent a seizure remains unknown. As noted previously, although current neuromodulation systems (RNS, VNS, and DBS) substantially reduce seizure frequency, rates of complete seizure freedom remain low, suggesting that research should also focus on identifying the most effective therapeutic window.
7.2.2. Addressing Brain Drift
Although the challenge of developing BCIs that adapt to drift stems from the limited training data, complementary strategies are required. On the one hand, following the example of other BCIs that employ human-in-the-loop paradigms, epilepsy BCIs could incorporate periodic recalibration informed by feedback from patients, caregivers, or clinicians. Indeed, longitudinal retraining of models improved predictive accuracy in several studies [151,189,190]. On the other hand, research could focus on developing representations of brain network states that are intrinsically robust to temporal variability.
Drift constitutes a critical gap in the field hindering clinical viability, tightly linked to the lack of brain state definitions. Without robust and reproducible criteria to delineate interictal, preictal, ictal, and postictal states, addressing temporal variability in a principled and generalisable manner remains unattainable.
7.3. Performance Evaluation: A Patient-Centric Approach
A persistent methodological limitation in epilepsy-related BCIs arises from validation strategies that neglect temporal dependencies (e.g., random cross-validation or LOOCV) and fail to preserve the natural interictal–preictal–ictal–postictal proportions observed in clinical data (e.g., 80/20 or k-fold partitions). Temporal cross-validation (e.g., time-series splitting) should instead be adopted, as it more accurately reflects real-world deployment on unseen, future data. Complementary to this, Few Sample Learning paradigms, also known as few-shot and one-shot learning [191], may further enhance ecological validity. In this scheme, models are trained on a minimal subset of data (e.g., a single seizure) and tested on the remaining events within the same recording. An optimal design would integrate both principles: train the model on the first available seizure and test sequentially on subsequent seizures (Figure 2C). This approach mitigates temporal leakage, enforces chronological causality, and provides a more realistic estimate of generalisation under non-stationary neural dynamics.
In addition to adopting a universal validation strategy, most appropriate evaluation metrics should be decided for benchmarking algorithms (e.g. accuracy, F1-score, false-positive rate, or detection latency). We propose that evaluation metrics should be redefined based on patient-centred priorities. As these algorithms are ultimately intended to serve individuals with DRE, patients and their caregivers should play an active role in establishing acceptable performance thresholds. This approach resonates with the principles of Participatory Research, which are increasingly being adopted in epilepsy research [192,193,194,195,196]. Although prior surveys and qualitative studies have begun identifying patient priorities, more effort is needed to translate these insights into actionable quantitative benchmarks.
7.3.1. Preferences for Seizure Detection
In the survey conducted by Quiroga et al. [193], it was shown that the most significant concern among patients and their caregivers is the risk of an undetected seizure, or a false negative. A high rate of false negatives compromises safety and a sense of security of seizure detection BCIs. The study also found that acceptable false-positive and false-negative rates should not exceed 25%, and that caregivers expect to be alerted within one minute of seizure onset.
7.3.2. Preferences for Seizure Prediction
Participatory Research may be particularly valuable in the context of seizure prediction, as it directly addresses the two significant challenges discussed previously: the lack of preictal state definition and standardized evaluation frameworks. Engaging patients and caregivers in the research process could help reconcile both issues simultaneously.
Surveys indicate that, regarding seizure prediction devices, the primary priorities for patients with DRE and their caregivers are achieving high predictive accuracy while minimizing false alarms. Although both objectives are essential, there is a slight tendency to prioritise sensitivity to ensure reliable seizure prediction. Patients and caregivers generally prefer short- to medium-length prediction horizons and may accept a modest increase in false-positive alarms if the device demonstrates high sensitivity, as the benefit of a timely warning outweighs the inconvenience. A trade-off may also exist between the desired prediction horizon and achievable accuracy, with users potentially accepting shorter warning times in exchange for more reliable predictions.
Given that the ultimate goal is to improve the lives of people with DRE, we propose that definitions of epilepsy brain states employed in the design of performance evaluation protocols should be grounded in patient needs and preferences.
8. Conclusions
In summary, the “therapeutic loop” framework presents a paradigm shift in the management of drug-resistant epilepsy, moving away from generalized, continuous treatment toward personalized, on-demand intervention. This review has provided a comprehensive analysis of these CLSs, addressing their limitations and proposing actionable steps to bridge the translation gap between research and clinics. While the progress in seizure detection, prediction, and stimulation technologies is promising, significant hurdles remain in achieving widespread clinical translation. The reliability of long-term seizure prediction, the validation of therapeutic efficacy, and the seamless integration of these complex systems into patients’ lives are critical challenges that require further interdisciplinary research. Ultimately, the path toward fully autonomous and effective CLSs depends on a concerted effort to refine the technology, validate its clinical utility, and ensure that the solutions meet the real-world needs of patients and caregivers, thereby holding the potential to significantly improve the quality of life for those affected by DRE.
Author Contributions
Conceptualization, J. MG. and A.P.; formal analysis, J.MG.; investigation, J.MG., A.P., and R.R; writing—original draft preparation, J.MG.; writing—review and editing, J.MG., A.P., K.I., and R.R.; supervision, A.P.; project administration, A.P.; funding acquisition, J.MG. and A.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Agència de Gestió d’Ajuts Universitaris i de Recerca (AGAUR) Generalitat de Catalunya grant number FI-SDUR 20203.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author(s).
Acknowledgments
During the preparation of this manuscript, the author(s) used OpenAI ChatGPT-5 for grammar refinement and language editing. The author(s) reviewed and verified all generated content and accept full responsibility for the final version of the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| ASM | Anti seizure medication |
| aDBS | Adaptive Deep Brain Stimulation |
| BCI | Brain-Computer Interface |
| CLS | Closed-Loop System |
| DBS | Deep Brain Stimulation |
| DRE | Drug Resistant Epilepsy |
| ECoG | Electrocorticography |
| EEG | Electroencephalogram |
| EMG | Electromyography |
| eTNS | External Trigeminal Nerve Stimulation |
| iEEG | Intracranial Electroencephalogram |
| OLS | Open-Loop System |
| RNS | Responsive Neurostimulation System |
| rTMS | Repetitive Transcranial Magnetic Stimulation |
| SD | Standard Deviation |
| SEEG | Stereotactic Electroencephalogram |
| SOZ | Seizure Onset Zone |
| tDCS | Transcranial Direct Current Stimulation |
| VNS | Vagus Nerve Stimulation |
References
- World Health Organization (WHO), International League Against Epilepsy (ILAE), and International Bureau for Epilepsy (IBE). EPILEPSY: A public health imperative, 2019.
- Perucca, E.; Perucca, P.; White, H.S.; Wirrell, E.C. Drug resistance in epilepsy. The Lancet Neurology 2023, 22, 723–734. [CrossRef]
- Kwan, P.; Arzimanoglou, A.; Berg, A.T.; Brodie, M.J.; Hauser, W.A.; Mathern, G.; Moshé, S.L.; Perucca, E.; Wiebe, S.; French, J. Definition of drug resistant epilepsy: Consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia 2009, 51, 1069–1077. [CrossRef]
- Ni, X.J.; Zhong, H.; Liu, Y.X.; Lin, H.W.; Gu, Z.C. Current trends and hotspots in drug-resistant epilepsy research: Insights from a bibliometric analysis. Frontiers in Neurology 2022, 13. [CrossRef]
- Marouf, H.; Mohamed, L.A.; Ftatary, A.E.; Gaber, D.E. Prevalence and risk factors associated with drug-resistant epilepsy in adult epileptic patients. The Egyptian Journal of Neurology Psychiatry and Neurosurgery 2023, 59. [CrossRef]
- Löscher, W.; Potschka, H.; Sisodiya, S.M.; Vezzani, A. Drug resistance in epilepsy: clinical impact, potential mechanisms, and new innovative treatment options. Pharmacological Reviews 2020, 72, 606–638. [CrossRef]
- Rheims, S.; Sperling, M.R.; Ryvlin, P. Drug-resistant epilepsy and mortality—Why and when do neuromodulation and epilepsy surgery reduce overall mortality. Epilepsia 2022, 63, 3020–3036. [CrossRef]
- Ben-Menachem, E.; Schmitz, B.; Kälviäinen, R.; Thomas, R.H.; Klein, P. The burden of chronic drug-refractory focal onset epilepsy: Can it be prevented? Epilepsy & Behavior 2023, 148, 109435. [CrossRef]
- Alare, K.; Ogungbemi, B.; Fagbenro, A.; Adetunji, B.; Owonikoko, O.; Omoniyo, T.; Jagunmolu, H.; Kayode, A.; Afolabi, S. Drug resistance predictive utility of age of onset and cortical imaging abnormalities in epilepsy: a systematic review and meta-analysis. The Egyptian Journal of Neurology Psychiatry and Neurosurgery 2024, 60. [CrossRef]
- Zuo, R.R.; Jin, M.; Sun, S.Z. Etiological analysis of 167 cases of drug-resistant epilepsy in children. The Italian journal of pediatrics 2024, 50. [CrossRef]
- Yildiz, E.P.; Gunes, D.; Bektas, G.; Uzunhan, T.A.; Tatli, B.; Caliskan, M.; Aydinli, N.; Ozmen, M. Predictive factors of drug-resistant epilepsy in children presenting under 2 years of age: experience of a tertiary center in Turkey. Acta Neurologica Belgica 2017, 118, 71–75. [CrossRef]
- Gasparini, S.; Ferlazzo, E.; Sueri, C.; Cianci, V.; Ascoli, M.; Cavalli, S.M.; Beghi, E.; Belcastro, V.; Bianchi, A.; Benna, P.; et al. Hypertension, seizures, and epilepsy: a review on pathophysiology and management. Neurological Sciences 2019, 40, 1775–1783. [CrossRef]
- Lü, Y.; Liu, S.; Yu, W. The causes of new-onset epilepsy and seizures in the elderly. Neuropsychiatric Disease and Treatment 2016, p. 1425. [CrossRef]
- Johnson, E.L.; Krauss, G.L.; Lee, A.K.; Schneider, A.L.C.; Dearborn, J.L.; Kucharska-Newton, A.M.; Huang, J.; Alonso, A.; Gottesman, R.F. Association between midlife risk factors and Late-Onset Epilepsy. JAMA Neurology 2018, 75, 1375. [CrossRef]
- Johnson, E.L.; Krauss, G.L.; Lee, A.K.; Schneider, A.L.; Kucharska-Newton, A.M.; Huang, J.; Jack, C.R.; Gottesman, R.F. Association between white matter hyperintensities, cortical volumes, and late-onset epilepsy. Neurology 2019, 92. [CrossRef]
- Chen, D.Y.; Chen, C.C.; Crawford, J.R.; Wang, S.G. Tumor-related epilepsy: epidemiology, pathogenesis and management. Journal of Neuro-Oncology 2018, 139, 13–21. [CrossRef]
- Sarkis, R.A.; Beers, L.; Farah, E.; Al-Akaidi, M.; Zhang, Y.; Locascio, J.J.; Properzi, M.J.; Schultz, A.P.; Chhatwal, J.P.; Johnson, K.A.; et al. The neurophysiology and seizure outcomes of late onset unexplained epilepsy. Clinical Neurophysiology 2020, 131, 2667–2672. [CrossRef]
- Potschka, H. The aging brain and late onset drug-refractory epilepsies. Seizure 2024. [CrossRef]
- Sultana, B.; Panzini, M.A.; Carpentier, A.V.; Comtois, J.; Rioux, B.; Gore, G.; Bauer, P.R.; Kwon, C.S.; Jetté, N.; Josephson, C.B.; et al. Incidence and prevalence of Drug-Resistant Epilepsy. Neurology 2021, 96, 805–817. [CrossRef]
- Guery, D.; Rheims, S. Clinical Management of Drug Resistant Epilepsy: A review on current strategies. Neuropsychiatric Disease and Treatment 2021, Volume 17, 2229–2242. [CrossRef]
- Poyuran, R.; Mahadevan, A.; Mhatre, R.; Arimappamagan, A.; Sinha, S.; Bharath, R.D.; Rao, M.B.; Saini, J.; Raghavendra, K.; Mundlamuri, R.C.; et al. Neuropathological spectrum of drug resistant epilepsy: 15-years-experience from a tertiary care centre. Journal of Clinical Neuroscience 2021, 91, 226–236. [CrossRef]
- Dalic, L.; Cook, M. Managing drug-resistant epilepsy: challenges and solutions. Neuropsychiatric Disease and Treatment 2016, Volume 12, 2605–2616. [CrossRef]
- Villanueva, V.; Girón, J.; Martín, J.; Hernández-Pastor, L.; Lahuerta, J.; Doz, M.; Cuesta, M.; Lévy-Bachelot, L. Impacto económico y en calidad de vida de la epilepsia resistente en España: estudio ESPERA. Neurología 2012, 28, 195–204. [CrossRef]
- Strzelczyk, A.; Griebel, C.; Lux, W.; Rosenow, F.; Reese, J.P. The Burden of Severely Drug-Refractory Epilepsy: A comparative longitudinal evaluation of mortality, morbidity, resource use, and cost using German health insurance data. Frontiers in Neurology 2017, 8. [CrossRef]
- Tang, F.; Hartz, A.M.S.; Bauer, B. Drug-Resistant epilepsy: multiple hypotheses, few answers. Frontiers in Neurology 2017, 8. [CrossRef]
- Mula, M.; Kanner, A.M.; Jetté, N.; Sander, J.W. Psychiatric comorbidities in people with epilepsy. Neurology Clinical Practice 2020, 11. [CrossRef]
- Malik, N.I.; Fatima, R.; Ullah, I.; Atta, M.; Awan, A.; Nashwan, A.J.; Ahmed, S. Perceived stigma, discrimination and psychological problems among patients with epilepsy. Frontiers in Psychiatry 2022, 13. [CrossRef]
- Yeni, K. Stigma and psychosocial problems in patients with epilepsy. Exploration of neuroscience 2023, 2, 251–263. [CrossRef]
- Arai, Y.; Okanishi, T.; Noma, H.; Kanai, S.; Kawaguchi, T.; Sunada, H.; Fujimoto, A.; Maegaki, Y. Prognostic factors for employment outcomes in patients with a history of childhood-onset drug-resistant epilepsy. Frontiers in Pediatrics 2023, 11. [CrossRef]
- Pokharel, R.; Poudel, P.; Lama, S.; Thapa, K.; Sigdel, R.; Shrestha, E. Burden and Its Predictors among Caregivers of Patient with Epilepsy. Journal of Epilepsy Research 2020, 10, 24–30. [CrossRef]
- Yu, X.; Lim, K.S.; Tang, L.Y.; David, P.; Ong, Z.Q.; Wong, K.Y.; Ji, M. Caregiving burden for adults with epilepsy and coping strategies, a systematic review. Epilepsy & Behavior 2025, 164, 110262. [CrossRef]
- Karakis, I.; Flesler, S.; Ghorpade, S.; Pineda, R.C.; Joshi, K.; Cooper, J.; Patkar, S.; Schulz, A.; Anand, S.B.; Barnes, N. Caregiver burden and healthcare providers perspectives in epilepsy: An observational study in China, Taiwan, and Argentina. Epilepsy & Behavior Reports 2024, 30, 100736. [CrossRef]
- Yu, Z.; Shao, Q.; Hou, K.; Wang, Y.; Sun, X. The experiences of caregivers of children with epilepsy: A meta-synthesis of qualitative research studies. Frontiers in Psychiatry 2022, 13. [CrossRef]
- Berg, A.T.; Kaiser, K.; Dixon-Salazar, T.; Elliot, A.; McNamara, N.; Meskis, M.A.; Golbeck, E.; Tatachar, P.; Laux, L.; Raia, C.; et al. Seizure burden in severe early-life epilepsy: Perspectives from parents. Epilepsia Open 2019, 4, 293–301. [CrossRef]
- Ioannou, P.; Foster, D.L.; Sander, J.W.; Dupont, S.; Gil-Nagel, A.; O’Flaherty, E.D.; Alvarez-Baron, E.; Medjedovic, J. The burden of epilepsy and unmet need in people with focal seizures. Brain and Behavior 2022, 12. [CrossRef]
- Picot, M.; Jaussent, A.; Neveu, D.; Kahane, P.; Crespel, A.; Gelisse, P.; Hirsch, E.; Derambure, P.; Dupont, S.; Landré, E.; et al. Cost-effectiveness analysis of epilepsy surgery in a controlled cohort of adult patients with intractable partial epilepsy: A 5-year follow-up study. Epilepsia 2016, 57, 1669–1679. [CrossRef]
- Toledano, R.; Villanueva, V.; Toledo, M.; Sabaniego, J.; Pérez-Domper, P. Clinical and economic implications of epilepsy management across treatment lines in Spain: a real-life database analysis. Journal of Neurology 2023, 270, 5945–5957. [CrossRef]
- De Zélicourt, M.; De Toffol, B.; Vespignani, H.; Laurendeau, C.; Lévy-Bachelot, L.; Murat, C.; Fagnani, F. Management of focal epilepsy in adults treated with polytherapy in France: The direct cost of drug resistance (ESPERA study). Seizure 2014, 23, 349–356. [CrossRef]
- Pirker, S.; Graef, A.; Gächter, M.; Baumgartner, C. Costs of Epilepsy in Austria: Unemployment as a primary driving factor. Seizure 2021, 89, 24–29. [CrossRef]
- Bäuerle, P.; Schneider, U.; Holtkamp, M.; Gloveli, T.; Dugladze, T. Outlines to Initiate Epilepsy Surgery in Low- and Middle-Income Countries. Journal of Integrative Neuroscience 2022, 21, 134. [CrossRef]
- Allers, K.; Essue, B.M.; Hackett, M.L.; Muhunthan, J.; Anderson, C.S.; Pickles, K.; Scheibe, F.; Jan, S. The economic impact of epilepsy: a systematic review. BMC Neurology 2015, 15. [CrossRef]
- Sabzvari, T.; Iqbal, M.A.; Ranganatha, A.; Daher, J.C.; Freire, I.; Shamsi, S.M.F.; Anthony, O.V.P.; Hingorani, A.G.; Sinha, A.S.; Nazir, Z. A comprehensive review of recent trends in surgical approaches for epilepsy management. Cureus 2024. [CrossRef]
- Gonzalez-Martinez, J.A. Epilepsy surgery in the last 10 years: advancements and controversies. Epiliepsy currents/Epilepsy currents 2025. [CrossRef]
- Winter, F.; Krueger, M.T.; Delev, D.; Theys, T.; Van Roost, D.M.; Fountas, K.; Schijns, O.E.; Roessler, K. Current state of the art of traditional and minimal invasive epilepsy surgery approaches. Brain and Spine 2024, 4, 102755. [CrossRef]
- Bartolomei, F. The epileptogenic network concept: Applications in the SEEG exploration of lesional focal epilepsies. Neurophysiologie Clinique 2024, 54, 103023. [CrossRef]
- Shahabi, H.; Nair, D.R.; Leahy, R.M. Multilayer brain networks can identify the epileptogenic zone and seizure dynamics. eLife 2023, 12. [CrossRef]
- Englot, D.J.; Chang, E.F. Rates and predictors of seizure freedom in resective epilepsy surgery: an update. Neurosurgical Review 2014, 37, 389–405. [CrossRef]
- Jobst, B.C.; Cascino, G.D. Resective Epilepsy Surgery for Drug-Resistant Focal Epilepsy. JAMA 2015, 313, 285. [CrossRef]
- Dash, G.K.; Rathore, C.; Jeyaraj, M.K.; Wattamwar, P.; Sarma, S.P.; Radhakrishnan, K. Predictors of seizure outcome following resective surgery for drug-resistant epilepsy associated with focal gliosis. Journal of neurosurgery 2018, 130, 2071–2079. [CrossRef]
- Hu, X.; Yao, Y.; Zhao, B.; Wang, X.; Li, Z.; Hu, W.; Zhang, C.; Zhang, K. Effective connectivity predicts surgical outcomes in temporal lobe epilepsy: a SEEG study. CNS Neuroscience & Therapeutics 2025, 31. [CrossRef]
- Mir, A.; Jallul, T.; Alotaibi, F.; Amer, F.; Najjar, A.; Alhazmi, R.; Faraidy, M.A.; Alharbi, A.; Aldurayhim, F.; Barnawi, Z.; et al. Outcomes of resective surgery in pediatric patients with drug-resistant epilepsy: A single-center study from the Eastern Mediterranean Region. Epilepsia Open 2023, 8, 930–945. [CrossRef]
- Ghosh, S.; Sinha, J.K.; Ghosh, S.; Sharma, H.; Bhaskar, R.; Narayanan, K.B. A comprehensive review of emerging trends and innovative therapies in epilepsy management. Brain Sciences 2023, 13, 1305. [CrossRef]
- Mushtaq, O.; Grezenko, H.; Rehman, A.; Sher, H.; Sher, Z.; Kaakyire, D.A.; Hanifullah, S.; Dabas, M.; Saleh, G.; Shehryar, A.; et al. Role of Responsive Neurostimulation in Managing Drug-Resistant Epilepsy: A Systematic Review of Clinical outcomes. Cureus 2024. [CrossRef]
- Zhang, X.; Zhang, X.; Huang, Q.; Chen, F. A review of epilepsy detection and prediction methods based on EEG signal processing and deep learning. Frontiers in Neuroscience 2024, 18. [CrossRef]
- Foutz, T.J.; Wong, M. Brain stimulation treatments in epilepsy: Basic mechanisms and clinical advances. Biomedical Journal 2021, 45, 27–37. [CrossRef]
- Bergey, G.K.; Morrell, M.J.; Mizrahi, E.M.; Goldman, A.; King-Stephens, D.; Nair, D.; Srinivasan, S.; Jobst, B.; Gross, R.E.; Shields, D.C.; et al. Long-term treatment with responsive brain stimulation in adults with refractory partial seizures. Neurology 2015, 84, 810–817. [CrossRef]
- Ben-Menachem, E. Vagus-nerve stimulation for the treatment of epilepsy. The Lancet Neurology 2002, 1, 477–482. [CrossRef]
- Hamilton, P.; Soryal, I.; Dhahri, P.; Wimalachandra, W.; Leat, A.; Hughes, D.; Toghill, N.; Hodson, J.; Sawlani, V.; Hayton, T.; et al. Clinical outcomes of VNS therapy with AspireSR® (including cardiac-based seizure detection) at a large complex epilepsy and surgery centre. Seizure 2018, 58, 120–126. [CrossRef]
- Zangiabadi, N.; Ladino, L.D.; Sina, F.; Orozco-Hernández, J.P.; Carter, A.; Téllez-Zenteno, J.F. Deep Brain Stimulation and Drug-Resistant Epilepsy: A Review of the literature. Frontiers in Neurology 2019, 10. [CrossRef]
- Richardson, R.M. Closed-Loop brain stimulation and paradigm shifts in epilepsy surgery. Neurologic Clinics 2022, 40, 355–373. [CrossRef]
- Winston, G.M.; Guadix, S.; Lavieri, M.T.; Uribe-Cardenas, R.; Kocharian, G.; Williams, N.; Sholle, E.; Grinspan, Z.; Hoffman, C.E. Closed-loop vagal nerve stimulation for intractable epilepsy: A single-center experience. Seizure 2021, 88, 95–101. [CrossRef]
- Fisher, B.; DesMarteau, J.A.; Koontz, E.H.; Wilks, S.J.; Melamed, S.E. Responsive vagus Nerve Stimulation for Drug Resistant epilepsy: A review of new features and practical guidance for advanced practice providers. Frontiers in Neurology 2021, 11. [CrossRef]
- Ramgopal, S.; Thome-Souza, S.; Jackson, M.; Kadish, N.E.; Fernández, I.S.; Klehm, J.; Bosl, W.; Reinsberger, C.; Schachter, S.; Loddenkemper, T. Seizure detection, seizure prediction, and closed-loop warning systems in epilepsy. Epilepsy & Behavior 2014, 37, 291–307. [CrossRef]
- Li, Y.; Xu, S.; Wang, Y.; Duan, Y.; Jia, Q.; Xie, J.; Yang, X.; Wang, Y.; Dai, Y.; Yang, G.; et al. Wireless Closed-Loop Optical regulation system for seizure detection and suppression in vivo. Frontiers in Nanotechnology 2022, 4. [CrossRef]
- Sisterson, N.D.; Wozny, T.A.; Kokkinos, V.; Constantino, A.; Richardson, R.M. Closed-Loop Brain Stimulation for Drug-Resistant Epilepsy: Towards an Evidence-Based Approach to Personalized Medicine. Neurotherapeutics 2018, 16, 119–127. [CrossRef]
- Shon, Y.M.; Park, H.R.; Lee, S. Deep Brain Stimulation Therapy for Drug-Resistant Epilepsy: Present and Future Perspectives. Journal of Epilepsy Research 2025, 15, 33–41. [CrossRef]
- Zhong, C.; Yang, K.; Wang, N.; Yang, L.; Yang, Z.; Xu, L.; Wang, J.; Zhang, L. Advancements in Surgical Therapies for Drug-Resistant Epilepsy: A Paradigm Shift towards Precision Care. Neurology and Therapy 2025. [CrossRef]
- Lin, Y.; Wang, Y. Neurostimulation as a promising epilepsy therapy. Epilepsia Open 2017, 2, 371–387. [CrossRef]
- Tervo, A.E.; Nieminen, J.O.; Lioumis, P.; Metsomaa, J.; Souza, V.H.; Sinisalo, H.; Stenroos, M.; Sarvas, J.; Ilmoniemi, R.J. Closed-loop optimization of transcranial magnetic stimulation with electroencephalography feedback. Brain stimulation 2022, 15, 523–531. [CrossRef]
- Qi, Z.; Liu, H.; Jin, F.; Wang, Y.; Lu, X.; Liu, L.; Yang, Z.; Fan, L.; Song, M.; Zuo, N.; et al. A wearable repetitive transcranial magnetic stimulation device. Nature Communications 2025, 16. [CrossRef]
- Leite, J.; Morales-Quezada, L.; Carvalho, S.; Thibaut, A.; Doruk, D.; Chen, C.F.; Schachter, S.C.; Rotenberg, A.; Fregni, F. Surface EEG-Transcranial Direct Current Stimulation (TDCS) Closed-Loop System. International Journal of Neural Systems 2017, 27, 1750026. [CrossRef]
- Kokkinos, V.; Sisterson, N.D.; Wozny, T.A.; Richardson, R.M. Association of Closed-Loop brain stimulation neurophysiological features with seizure control among patients with focal epilepsy. JAMA Neurology 2019, 76, 800. [CrossRef]
- Afra, P.; Adamolekun, B.; Aydemir, S.; Watson, G.D.R. Evolution of the Vagus Nerve Stimulation (VNS) therapy System Technology for Drug-Resistant Epilepsy. Frontiers in Medical Technology 2021, 3. [CrossRef]
- U.S. Food and Drug Administration. Premarket Approval (PMA) — P960009S219. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=p960009s219, 2018. Accessed: 2025-10-14.
- U.S. Food and Drug Administration. Premarket Approval (PMA) — P100026. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P100026, 2013. Accessed: YYYY-MM-DD.
- Ryvlin, P.; Rheims, S.; Hirsch, L.J.; Sokolov, A.; Jehi, L. Neuromodulation in epilepsy: state-of-the-art approved therapies. The Lancet Neurology 2021, 20, 1038–1047. [CrossRef]
- Roa, J.A.; Marcuse, L.; Fields, M.; La Vega-Talbott, M.; Yoo, J.Y.; Wolf, S.M.; McGoldrick, P.; Ghatan, S.; Panov, F. Long-term outcomes after responsive neurostimulation for treatment of refractory epilepsy: a single-center experience of 100 cases. Journal of neurosurgery 2023, 139, 1463–1470. [CrossRef]
- Zawar, I.; Krishnan, B.; Mackow, M.; Alexopoulos, A.; Nair, D.; Punia, V. The Efficacy, Safety, and Outcomes of Brain-responsive Neurostimulation (RNS® System) therapy in older adults. Epilepsia Open 2021, 6, 781–787. [CrossRef]
- Lin, C.; Kim-McManus, O.; Sattar, S.; Rismanchi, N.; Ravindra, V.; Gonda, D.D. 271 A retrospective, chart review study of the efficacy and safety of the RNS system in pediatric populations for medically refractory focal epilepsy. Neurosurgery 2024, 70, 76. [CrossRef]
- Nair, D.R.; Laxer, K.D.; Weber, P.B.; Murro, A.M.; Park, Y.D.; Barkley, G.L.; Smith, B.J.; Gwinn, R.P.; Doherty, M.J.; Noe, K.H.; et al. Nine-year prospective efficacy and safety of brain-responsive neurostimulation for focal epilepsy. Neurology 2020, 95. [CrossRef]
- Razavi, B.; Rao, V.R.; Lin, C.; Bujarski, K.A.; Patra, S.E.; Burdette, D.E.; Geller, E.B.; Brown, M.M.; Johnson, E.A.; Drees, C.; et al. Real-world experience with direct brain-responsive neurostimulation for focal onset seizures. Epilepsia 2020, 61, 1749–1757. [CrossRef]
- Abouelleil, M.; Deshpande, N.; Ali, R. Emerging Trends in Neuromodulation for treatment of Drug-Resistant Epilepsy. Frontiers in Pain Research 2022, 3. [CrossRef]
- Touma, L.; Dansereau, B.; Chan, A.Y.; Jetté, N.; Kwon, C.; Braun, K.P.J.; Friedman, D.; Jehi, L.; Rolston, J.D.; Vadera, S.; et al. Neurostimulation in people with drug-resistant epilepsy: Systematic review and meta-analysis from the ILAE Surgical Therapies Commission. Epilepsia 2022, 63, 1314–1329. [CrossRef]
- Tani, N.; Dibué, M.; Verner, R.; Nishikawa, S.M.; Gordon, C.; Kawai, K.; Kishima, H. One-year seizure freedom and quality of life in patients with drug-resistant epilepsy receiving adjunctive vagus nerve stimulation in Japan. Epilepsia Open 2024. [CrossRef]
- Ghaemi, K.; Elsharkawy, A.E.; Schulz, R.; Hoppe, M.; Polster, T.; Pannek, H.; Ebner, A. Vagus nerve stimulation: Outcome and predictors of seizure freedom in long-term follow-up. Seizure 2010, 19, 264–268. [CrossRef]
- Chen, S.; Yang, X.; Xu, S.; Li, B.; Li, C.; Yang, N.; Yang, X.; Wang, X.; Xu, S.; Zhao, X. Long-term outcome of vagus nerve stimulation therapy in drug-resistant epilepsy: a retrospective single-center study. Frontiers in Neurology 2025, 16. [CrossRef]
- Salanova, V.; Witt, T.; Worth, R.; Henry, T.R.; Gross, R.E.; Nazzaro, J.M.; Labar, D.; Sperling, M.R.; Sharan, A.; Sandok, E.; et al. Long-term efficacy and safety of thalamic stimulation for drug-resistant partial epilepsy. Neurology 2015, 84, 1017–1025. [CrossRef]
- Yan, H.; Wang, X.; Zhang, X.; Qiao, L.; Gao, R.; Ni, D.; Shu, W.; Xu, C.; Ren, L.; Yu, T. Deep brain stimulation for patients with refractory epilepsy: nuclei selection and surgical outcome. Frontiers in Neurology 2023, 14. [CrossRef]
- Li, Q.; Shan, Y.; Wei, P.; Zhao, G. The comparison of DBS and RNS for adult drug-resistant epilepsy: a systematic review and meta-analysis. Frontiers in Human Neuroscience 2024, 18. [CrossRef]
- Sisterson, N.D.; Wozny, T.A.; Kokkinos, V.; Bagic, A.; Urban, A.P.; Richardson, R.M. A rational approach to understanding and evaluating responsive neurostimulation. Neuroinformatics 2020, 18, 365–375. [CrossRef]
- Boon, P.; Vonck, K.; Van Rijckevorsel, K.; Tahry, R.E.; Elger, C.E.; Mullatti, N.; Schulze-Bonhage, A.; Wagner, L.; Diehl, B.; Hamer, H.; et al. A prospective, multicenter study of cardiac-based seizure detection to activate vagus nerve stimulation. Seizure 2015, 32, 52–61. [CrossRef]
- Fisher, R.S.; Afra, P.; Macken, M.; Minecan, D.N.; Bagić, A.; Benbadis, S.R.; Helmers, S.L.; Sinha, S.R.; Slater, J.; Treiman, D.; et al. Automatic vagus Nerve stimulation Triggered by Ictal Tachycardia: Clinical Outcomes and Device Performance—The U.S. E-37 Trial. Neuromodulation Technology at the Neural Interface 2015, 19, 188–195. [CrossRef]
- Kerr, W.T.; McFarlane, K.N.; Pucci, G.F. The present and future of seizure detection, prediction, and forecasting with machine learning, including the future impact on clinical trials. Frontiers in Neurology 2024, 15. [CrossRef]
- Shoka, A.A.E.; Dessouky, M.M.; El-Sayed, A.; Hemdan, E.E.D. EEG seizure detection: concepts, techniques, challenges, and future trends. Multimedia Tools and Applications 2023, 82, 42021–42051. [CrossRef]
- Bai, L.; Litscher, G.; Li, X. Epileptic Seizure Detection Using Machine Learning: A Systematic Review and Meta-Analysis. Brain Sciences 2025, 15, 634. [CrossRef]
- Andrzejak, R.G.; Zaveri, H.P.; Schulze-Bonhage, A.; Leguia, M.G.; Stacey, W.C.; Richardson, M.P.; Kuhlmann, L.; Lehnertz, K. Seizure forecasting: Where do we stand? Epilepsia 2023, 64. [CrossRef]
- Cook, M.J.; O’Brien, T.J.; Berkovic, S.F.; Murphy, M.; Morokoff, A.; Fabinyi, G.; D’Souza, W.; Yerra, R.; Archer, J.; Litewka, L.; et al. Prediction of seizure likelihood with a long-term, implanted seizure advisory system in patients with drug-resistant epilepsy: a first-in-man study. The Lancet Neurology 2013, 12, 563–571. [CrossRef]
- Kuhlmann, L.; Karoly, P.; Freestone, D.R.; Brinkmann, B.H.; Temko, A.; Barachant, A.; Li, F.; Titericz, G.; Lang, B.W.; Lavery, D.; et al. Epilepsyecosystem.org: crowd-sourcing reproducible seizure prediction with long-term human intracranial EEG. Brain 2018. [CrossRef]
- Xu, L.; Xu, M.; Ke, Y.; An, X.; Liu, S.; Ming, D. Cross-Dataset variability problem in EEG decoding with deep learning. Frontiers in Human Neuroscience 2020, 14. [CrossRef]
- Ma, J.; Yang, B.; Qiu, W.; Li, Y.; Gao, S.; Xia, X. A large EEG dataset for studying cross-session variability in motor imagery brain-computer interface. Scientific Data 2022, 9. [CrossRef]
- Tajadini, B.; Seydnejad, S.R.; Rezakhani, S. Short-term epileptic seizures prediction based on cepstrum analysis and signal morphology. BMC Biomedical Engineering 2024, 6. [CrossRef]
- Śliwowski, M.; Martin, M.; Souloumiac, A.; Blanchart, P.; Aksenova, T. Impact of dataset size and long-term ECoG-based BCI usage on deep learning decoders performance. Frontiers in Human Neuroscience 2023, 17. [CrossRef]
- Poziomska, M.; Dovgialo, M.; Olbratowski, P.; Niedbalski, P.; Ogniewski, P.; Zych, J.; Rogala, J.; Żygierewicz, J. Quantity versus Diversity: Influence of Data on Detecting EEG Pathology with Advanced ML Models. Neural Networks 2025, p. 108073. [CrossRef]
- Yang, B.; Rong, F.; Xie, Y.; Li, D.; Zhang, J.; Li, F.; Shi, G.; Gao, X. A multi-day and high-quality EEG dataset for motor imagery brain-computer interface. Scientific Data 2025, 12. [CrossRef]
- Hogan, R.; Mathieson, S.R.; Luca, A.; Ventura, S.; Griffin, S.; Boylan, G.B.; O’Toole, J.M. Scaling convolutional neural networks achieves expert level seizure detection in neonatal EEG. npj Digital Medicine 2025, 8. [CrossRef]
- Niso, G.; Gorgolewski, K.J.; Bock, E.; Brooks, T.L.; Flandin, G.; Gramfort, A.; Henson, R.N.; Jas, M.; Litvak, V.; Moreau, J.T.; et al. MEG-BIDS, the brain imaging data structure extended to magnetoencephalography. Scientific Data 2018, 5. [CrossRef]
- Pernet, C.R.; Appelhoff, S.; Gorgolewski, K.J.; Flandin, G.; Phillips, C.; Delorme, A.; Oostenveld, R. EEG-BIDS, an extension to the brain imaging data structure for electroencephalography. Scientific Data 2019, 6. [CrossRef]
- Gorgolewski, K.J.; Alfaro-Almagro, F.; Auer, T.; Bellec, P.; Capotă, M.; Chakravarty, M.M.; Churchill, N.W.; Cohen, A.L.; Craddock, R.C.; Devenyi, G.A.; et al. BIDS apps: Improving ease of use, accessibility, and reproducibility of neuroimaging data analysis methods. PLoS Computational Biology 2017, 13, e1005209. [CrossRef]
- Meyer, M.; Lamers, D.; Kayhan, E.; Hunnius, S.; Oostenveld, R. Enhancing reproducibility in developmental EEG research: BIDS, cluster-based permutation tests, and effect sizes. Developmental Cognitive Neuroscience 2021, 52, 101036. [CrossRef]
- Wong, S.; Simmons, A.; Rivera-Villicana, J.; Barnett, S.; Sivathamboo, S.; Perucca, P.; Ge, Z.; Kwan, P.; Kuhlmann, L.; Vasa, R.; et al. EEG datasets for seizure detection and prediction— A review. Epilepsia Open 2023, 8, 252–267. [CrossRef]
- Wang, D.X.; Ng, N.; Seger, S.E.; Ekstrom, A.D.; Kriegel, J.L.; Lega, B.C. Machine learning classifiers for electrode selection in the design of closed-loop neuromodulation devices for episodic memory improvement. Cerebral Cortex 2023, 33, 8150–8163. [CrossRef]
- Bernabei, J.M.; Li, A.; Revell, A.Y.; Smith, R.J.; Gunnarsdottir, K.M.; Ong, I.Z.; Davis, K.A.; Sinha, N.; Sarma, S.; Litt, B. "HUP iEEG Epilepsy Dataset", 2022. [CrossRef]
- Nasreddine, W. “Epileptic EEG Dataset” V1. Mendeley Data, 2021. [CrossRef]
- Obeid, I.; Picone, J. The Temple University Hospital EEG data corpus. Frontiers in Neuroscience 2016, 10. [CrossRef]
- Guttag, J. “CHB-MIT Scalp EEG Database” (version 1.0.0). Mendeley Data, 2021. [CrossRef]
- Detti, P. "Siena Scalp EEG Database" (version 1.0.0). PhysioNet, 2020. [CrossRef]
- Fan, X.; Gaspard, N.; Legros, B.; Lucchetti, F.; Ercek, R.; Nonclercq, A. Automated epileptic seizure detection based on break of excitation/inhibition balance. Computers in Biology and Medicine 2019, 107, 30–38. [CrossRef]
- Bhagubai, M.; Chatzichristos, C.; Swinnen, L.; Macea, J.; Zhang, J.; Lagae, L.; Jansen, K.; Schulze-Bonhage, A.; Sales, F.; Mahler, B.; et al. SeizeIT2: Wearable dataset of patients with focal Epilepsy. Scientific Data 2025, 12. [CrossRef]
- Bougou, V.; Vanhoyland, M.; Cleeren, E.; Janssen, P.; Van Paesschen, W.; Theys, T. Mesoscale insights in Epileptic Networks: A Multimodal Intracranial Dataset. Scientific Data 2025, 12. [CrossRef]
- Nejedly, P.; Kremen, V.; Sladky, V.; Cimbalnik, J.; Klimes, P.; Plesinger, F.; Mivalt, F.; Travnicek, V.; Viscor, I.; Pail, M.; et al. Multicenter intracranial EEG dataset for classification of graphoelements and artifactual signals. Scientific Data 2020, 7. [CrossRef]
- Li, A.; Huynh, C.; Fitzgerald, Z.; Cajigas, I.; Brusko, D.; Jagid, J.; Claudio, A.O.; Kanner, A.M.; Hopp, J.; Chen, S.; et al. Neural fragility as an EEG marker of the seizure onset zone. Nature Neuroscience 2021, 24, 1465–1474. [CrossRef]
- Heck, C.N.; King-Stephens, D.; Massey, A.D.; Nair, D.R.; Jobst, B.C.; Barkley, G.L.; Salanova, V.; Cole, A.J.; Smith, M.C.; Gwinn, R.P.; et al. Two-year seizure reduction in adults with medically intractable partial onset epilepsy treated with responsive neurostimulation: Final results of the RNS System Pivotal trial. Epilepsia 2014, 55, 432–441. [CrossRef]
- Almarie, B.; Pacheco-Barrios, K.; Gianlorenco, A.C.; Eltawil, Y.; Sanchez, A.; Fregni, F. Clinical trial design in FDA submissions for neuromodulation devices, 1960-2023: a systematic review and meta-analysis. Expert Review of Medical Devices 2025. [CrossRef]
- Carver, R.B.; Kolberg, M.; Reed, W.; Mikkelsen, O.L.; Kvam, S.; Halgunset, J.; Budin-Ljøsne, I. Toward a more general consent for the use of patients’ biological material and health information for Medical Research—The Patient Perspective. Biopreservation and Biobanking 2025. [CrossRef]
- Köngeter, A.; Schickhardt, C.; Jungkunz, M.; Bergbold, S.; Mehlis, K.; Winkler, E.C. Patients’ willingness to provide their clinical data for research purposes and acceptance of different consent models: findings from a representative survey of patients with cancer. Journal of Medical Internet Research 2022, 24, e37665. [CrossRef]
- Richter, G.; Borzikowsky, C.; Lieb, W.; Schreiber, S.; Krawczak, M.; Buyx, A. Patient views on research use of clinical data without consent: Legal, but also acceptable? European Journal of Human Genetics 2019, 27, 841–847. [CrossRef]
- European Union. Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data, and repealing Directive 95/46/EC (General Data Protection Regulation). https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX%3A32016R0679, 2016. Official Journal of the European Union, L119, 1–88.
- Kaushik, A.; Barcellona, C.; Mandyam, N.K.; Tan, S.Y.; Tromp, J. Challenges and opportunities for data sharing related to Artificial Intelligence (AI) tools in healthcare in low- and middle-income countries: A systematic review and case study from Thailand. (Preprint). Journal of Medical Internet Research 2024, 27, e58338. [CrossRef]
- Beusink, M.; Koetsveld, F.; Van Scheijen, S.; Janssen, T.; Buiter, M.; Schmidt, M.K.; Rebers, S. Health Research with Data in a Time of Privacy: Which Information do Patients Want? Journal of Empirical Research on Human Research Ethics 2023, 18, 304–316. [CrossRef]
- Shlobin, N.A.; Campbell, J.M.; Rosenow, J.M.; Rolston, J.D. Ethical considerations in the surgical and neuromodulatory treatment of epilepsy. Epilepsy & Behavior 2022, 127, 108524. [CrossRef]
- Perucca, P.; Dubeau, F.; Gotman, J. Intracranial electroencephalographic seizure-onset patterns: effect of underlying pathology. Brain 2013, 137, 183–196. [CrossRef]
- Scheffer, I.E.; Berkovic, S.; Capovilla, G.; Connolly, M.B.; French, J.; Guilhoto, L.; Hirsch, E.; Jain, S.; Mathern, G.W.; Moshé, S.L.; et al. ILAE classification of the epilepsies: Position paper of the ILAE Commission for Classification and Terminology. Epilepsia 2017, 58, 512–521. [CrossRef]
- Fisher, R.S.; Cross, J.H.; D’Souza, C.; French, J.A.; Haut, S.R.; Higurashi, N.; Hirsch, E.; Jansen, F.E.; Lagae, L.; Moshé, S.L.; et al. Instruction manual for the ILAE 2017 operational classification of seizure types. Epilepsia 2017, 58, 531–542. [CrossRef]
- Halford, J.; Shiau, D.; Desrochers, J.; Kolls, B.; Dean, B.; Waters, C.; Azar, N.; Haas, K.; Kutluay, E.; Martz, G.; et al. Inter-rater agreement on identification of electrographic seizures and periodic discharges in ICU EEG recordings. Clinical Neurophysiology 2014, 126, 1661–1669. [CrossRef]
- Scheuer, M.L.; Wilson, S.B.; Antony, A.; Ghearing, G.; Urban, A.; Bagić, A.I. Seizure detection: interreader agreement and detection algorithm assessments using a large dataset. Journal of Clinical Neurophysiology 2020, 38, 439–447. [CrossRef]
- Karoly, P.J.; Rao, V.R.; Gregg, N.M.; Worrell, G.A.; Bernard, C.; Cook, M.J.; Baud, M.O. Cycles in epilepsy. Nature Reviews Neurology 2021, 17, 267–284. [CrossRef]
- Litt, B.; Esteller, R.; Echauz, J.; D’Alessandro, M.; Shor, R.; Henry, T.; Pennell, P.; Epstein, C.; Bakay, R.; Dichter, M.; et al. Epileptic seizures may begin hours in advance of clinical onset. Neuron 2001, 30, 51–64. [CrossRef]
- Gregg, N.M.; Attia, T.P.; Nasseri, M.; Joseph, B.; Karoly, P.; Cui, J.; Stirling, R.E.; Viana, P.F.; Richner, T.J.; Nurse, E.S.; et al. Seizure occurrence is linked to multiday cycles in diverse physiological signals. Epilepsia 2023, 64, 1627–1639. [CrossRef]
- Batista, J.; Pinto, M.F.; Tavares, M.; Lopes, F.; Oliveira, A.; Teixeira, C. EEG epilepsy seizure prediction: the post-processing stage as a chronology. Scientific Reports 2024, 14. [CrossRef]
- Baud, M.O.; Kleen, J.K.; Mirro, E.A.; Andrechak, J.C.; King-Stephens, D.; Chang, E.F.; Rao, V.R. Multi-day rhythms modulate seizure risk in epilepsy. Nature Communications 2018, 9. [CrossRef]
- Chang, W.C.; Kudlacek, J.; Jiruska, P.; Jefferys, J.G.R. Transition to Seizure from Cellular, Network, and Dynamical Perspectives; 2024; pp. 196–200. [CrossRef]
- Leal, A.; Curty, J.; Lopes, F.; Pinto, M.F.; Oliveira, A.; Sales, F.; Bianchi, A.M.; Ruano, M.G.; Dourado, A.; Henriques, J.; et al. Unsupervised EEG preictal interval identification in patients with drug-resistant epilepsy. Scientific Reports 2023, 13. [CrossRef]
- Das, A.; Cash, S.S.; Sejnowski, T.J. Heterogeneity of preictal dynamics in human epileptic seizures. IEEE Access 2020, 8, 52738–52748. [CrossRef]
- Bandarabadi, M.; Rasekhi, J.; Teixeira, C.A.; Karami, M.R.; Dourado, A. On the proper selection of preictal period for seizure prediction. Epilepsy & Behavior 2015, 46, 158–166. [CrossRef]
- Driscoll, L.N.; Duncker, L.; Harvey, C.D. Representational drift: Emerging theories for continual learning and experimental future directions. Current Opinion in Neurobiology 2022, 76, 102609. [CrossRef]
- Pitkänen, A.; Sutula, T.P. Is epilepsy a progressive disorder? Prospects for new therapeutic approaches in temporal-lobe epilepsy. The Lancet Neurology 2002, 1, 173–181. [CrossRef]
- Morgan, V.L.; Johnson, G.W.; Cai, L.Y.; Landman, B.A.; Schilling, K.G.; Englot, D.J.; Rogers, B.P.; Chang, C. MRI network progression in mesial temporal lobe epilepsy related to healthy brain architecture. Network Neuroscience 2021, 5, 434–450. [CrossRef]
- Liang, Y.; Chen, C.; Li, F.; Yao, D.; Xu, P.; Yu, L. Altered Functional Connectivity after Epileptic Seizure Revealed by Scalp EEG. Neural Plasticity 2020, 2020, 1–8. [CrossRef]
- Ye, H.; He, C.; Hu, W.; Xiong, K.; Hu, L.; Chen, C.; Xu, S.; Xu, C.; Wang, Y.; Ding, Y.; et al. Pre-ictal fluctuation of EEG functional connectivity discriminates seizure phenotypes in mesial temporal lobe epilepsy. Clinical Neurophysiology 2023, 151, 107–115. [CrossRef]
- Wei, Z.; Wang, X.; Liu, C.; Feng, Y.; Gan, Y.; Shi, Y.; Wang, X.; Liu, Y.; Deng, Y. Microstate-based brain network dynamics distinguishing temporal lobe epilepsy patients: A machine learning approach. NeuroImage 2024, 296, 120683. [CrossRef]
- Pontes, E.D.; Pinto, M.; Lopes, F.; Teixeira, C. Concept-drifts adaptation for machine learning EEG epilepsy seizure prediction. Scientific Reports 2024, 14. [CrossRef]
- Saadoon, Y.A.; Khalil, M.; Battikh, D. Machine and Deep Learning-Based Seizure Prediction: A scoping review on the use of temporal and spectral features. Applied Sciences 2025, 15, 6279. [CrossRef]
- Jemal, I.; Abou-Abbas, L.; Henni, K.; Mitiche, A.; Mezghani, N. Domain adaptation for EEG-based, cross-subject epileptic seizure prediction. Frontiers in Neuroinformatics 2024, 18. [CrossRef]
- Massoud, Y.M.; Abdelzaher, M.; Kuhlmann, L.; Ghany, M.A.A.E. General and patient-specific seizure classification using deep neural networks. Analog Integrated Circuits and Signal Processing 2023, 116, 205–220. [CrossRef]
- Leguia, M.G.; Rao, V.R.; Tcheng, T.K.; Duun-Henriksen, J.; Kjær, T.W.; Proix, T.; Baud, M.O. Learning to generalize seizure forecasts. Epilepsia 2022, 64. [CrossRef]
- Zargar, B.S.; Mollaei, M.R.K.; Ebrahimi, F.; Rasekhi, J. Generalizable epileptic seizures prediction based on deep transfer learning. Cognitive Neurodynamics 2022, 17, 119–131. [CrossRef]
- Nazari, J.; Nasrabadi, A.M.; Menhaj, M.B.; Raiesdana, S. Epilepsy seizure prediction with few-shot learning method. Brain Informatics 2022, 9. [CrossRef]
- Wu, D.; Yang, J.; Sawan, M. Bridging the gap between patient-specific and patient-independent seizure prediction via knowledge distillation. Journal of Neural Engineering 2022, 19, 036035. [CrossRef]
- Orosco, L.; Correa, A.G.; Diez, P.; Laciar, E. Patient non-specific algorithm for seizures detection in scalp EEG. Computers in Biology and Medicine 2016, 71, 128–134. [CrossRef]
- Billeci, L.; Marino, D.; Insana, L.; Vatti, G.; Varanini, M. Patient-specific seizure prediction based on heart rate variability and recurrence quantification analysis. PLoS ONE 2018, 13, e0204339. [CrossRef]
- Saemaldahr, R.; Ilyas, M. Patient-Specific Preictal Pattern-Aware Epileptic Seizure Prediction with Federated Learning. Sensors 2023, 23, 6578. [CrossRef]
- Yang, Y.; Qin, X.; Wen, H.; Li, F.; Lin, X. Patient-specific approach using data fusion and adversarial training for epileptic seizure prediction. Frontiers in Computational Neuroscience 2023, 17. [CrossRef]
- Lopes, F.; Pinto, M.F.; Dourado, A.; Schulze-Bonhage, A.; Dümpelmann, M.; Teixeira, C. Addressing data limitations in seizure prediction through transfer learning. Scientific Reports 2024, 14. [CrossRef]
- Perez-Velasco, S.; Santamaria-Vazquez, E.; Martinez-Cagigal, V.; Marcos-Martinez, D.; Hornero, R. EEGSYM: Overcoming Inter-Subject Variability in Motor Imagery Based BCIs with Deep Learning. IEEE Transactions on Neural Systems and Rehabilitation Engineering 2022, 30, 1766–1775. [CrossRef]
- Kumar, S.; Alawieh, H.; Racz, F.S.; Fakhreddine, R.; Del R Millán, J. Transfer learning promotes acquisition of individual BCI skills. PNAS Nexus 2024, 3. [CrossRef]
- Peterson, V.; Wyser, D.; Lambercy, O.; Spies, R.; Gassert, R. A penalized time-frequency band feature selection and classification procedure for improved motor intention decoding in multichannel EEG. Journal of Neural Engineering 2019, 16, 016019. [CrossRef]
- Wang, J.G.; Shao, H.M.; Yao, Y.; Liu, J.L.; Ma, S.W. A personalized feature extraction and classification method for motor imagery recognition. Mobile Networks and Applications 2021, 26, 1359–1371. [CrossRef]
- Zhong, Y.; Yao, L.; Wang, Y. Enhanced motor imagery decoding by calibration Model-Assisted with Tactile ERD. IEEE Transactions on Neural Systems and Rehabilitation Engineering 2023, 31, 4295–4305. [CrossRef]
- Luo, S.; Angrick, M.; Coogan, C.; Candrea, D.N.; Wyse-Sookoo, K.; Shah, S.; Rabbani, Q.; Milsap, G.W.; Weiss, A.R.; Anderson, W.S.; et al. Stable Decoding from a Speech BCI Enables Control for an Individual with ALS without Recalibration for 3 Months. Advanced Science 2023, 10. [CrossRef]
- Pale, U.; Teijeiro, T.; Rheims, S.; Ryvlin, P.; Atienza, D. Combining general and personal models for epilepsy detection with hyperdimensional computing. Artificial Intelligence in Medicine 2024, 148, 102754. [CrossRef]
- Yan, K.; Luo, X.; Ye, L.; Geng, W.; He, J.; Mu, J.; Hou, X.; Zan, X.; Ma, J.; Li, F.; et al. Automated seizure detection in epilepsy using a novel dynamic temporal-spatial graph attention network. Scientific Reports 2025, 15. [CrossRef]
- Cherian, R.; Kanaga, E.G. Theoretical and methodological analysis of EEG based seizure detection and prediction: An exhaustive review. Journal of Neuroscience Methods 2022, 369, 109483. [CrossRef]
- Pale, U.; Teijeiro, T.; Atienza, D. Importance of methodological choices in data manipulation for validating epileptic seizure detection models. 2022 44th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC) 2023, pp. 1–7. [CrossRef]
- Shah, V.; Golmohammadi, M.; Obeid, I.; Picone, J. Objective Evaluation Metrics for automatic classification of EEG events; 2021; pp. 223–255. [CrossRef]
- Shafiezadeh, S.; Duma, G.M.; Mento, G.; Danieli, A.; Antoniazzi, L.; Del Popolo Cristaldi, F.; Bonanni, P.; Testolin, A. Methodological issues in evaluating machine learning models for EEG seizure prediction: Good Cross-Validation accuracy does not guarantee generalization to new patients. Applied Sciences 2023, 13, 4262. [CrossRef]
- West, J.; Bozorgi, Z.D.; Herron, J.; Chizeck, H.J.; Chambers, J.D.; Li, L. Machine learning seizure prediction: one problematic but accepted practice. Journal of Neural Engineering 2022, 20, 016008. [CrossRef]
- Dan, J.; Pale, U.; Amirshahi, A.; Cappelletti, W.; Ingolfsson, T.M.; Wang, X.; Cossettini, A.; Bernini, A.; Benini, L.; Beniczky, S.; et al. SzCORE: Seizure Community Open-Source Research Evaluation framework for the validation of electroencephalography-based automated seizure detection algorithms. Epilepsia 2024. [CrossRef]
- Carmo, A.S.; Abreu, M.; Baptista, M.F.; De Oliveira Carvalho, M.; Peralta, A.R.; Fred, A.; Bentes, C.; Da Silva, H.P. Automated algorithms for seizure forecast: a systematic review and meta-analysis. Journal of Neurology 2024. [CrossRef]
- Andrade, I.; Teixeira, C.; Pinto, M. On the performance of seizure prediction machine learning methods across different databases: the sample and alarm-based perspectives. Frontiers in Neuroscience 2024, 18. [CrossRef]
- De Tisi, J.; Bell, G.S.; Peacock, J.L.; McEvoy, A.W.; Harkness, W.F.; Sander, J.W.; Duncan, J.S. The long-term outcome of adult epilepsy surgery, patterns of seizure remission, and relapse: a cohort study. The Lancet 2011, 378, 1388–1395. [CrossRef]
- Andrews, J.P.; Gummadavelli, A.; Farooque, P.; Bonito, J.; Arencibia, C.; Blumenfeld, H.; Spencer, D.D. Association of seizure spread with surgical failure in epilepsy. JAMA Neurology 2018, 76, 462. [CrossRef]
- Cohen-Gadol, A.A.; Wilhelmi, B.G.; Collignon, F.; White, J.B.; Britton, J.W.; Cambier, D.M.; Christianson, T.J.H.; Marsh, W.R.; Meyer, F.B.; Cascino, G.D. Long-term outcome of epilepsy surgery among 399 patients with nonlesional seizure foci including mesial temporal lobe sclerosis. Journal of neurosurgery 2006, 104, 513–524. [CrossRef]
- Jin, B.; Wang, J.; Zhou, J.; Wang, S.; Guan, Y.; Chen, S. A longitudinal study of surgical outcome of pharmacoresistant epilepsy caused by focal cortical dysplasia. Journal of Neurology 2016, 263, 2403–2410. [CrossRef]
- Harris, W.B.; Brunette-Clement, T.; Wang, A.; Phillips, H.W.; Von Der Brelie, C.; Weil, A.G.; Fallah, A. Long-term outcomes of pediatric epilepsy surgery: Individual participant data and study level meta-analyses. Seizure 2022, 101, 227–236. [CrossRef]
- Mohan, M.; Keller, S.; Nicolson, A.; Biswas, S.; Smith, D.; Farah, J.O.; Eldridge, P.; Wieshmann, U. The long-term outcomes of epilepsy surgery. PLoS ONE 2018, 13, e0196274. [CrossRef]
- Kang, Y.; Kim, S.; Jung, Y.; Ko, D.S.; Kim, H.W.; Yoon, J.P.; Cho, S.; Song, T.J.; Kim, K.; Son, E.; et al. Exploring the Smoking-Epilepsy Nexus: a systematic review and meta-analysis of observational studies. BMC Medicine 2024, 22. [CrossRef]
- Zhang, Z.; Wang, M.; Yuan, S.; Liu, X. Alcohol, coffee, and milk intake in relation to epilepsy risk. Nutrients 2022, 14, 1153. [CrossRef]
- Bratu, I.; De Clerck, L.; Catenoix, H.; Valton, L.; Aupy, J.; Nica, A.; Rheims, S.; Aubert-Conil, S.; Benoit, J.; Makhalova, J.; et al. Cerebral Cavernous Malformations and Focal Drug-Resistant Epilepsy: Behind a quid pro quo of lesion and Epileptogenic Networks. European Journal of Neurology 2025, 32. [CrossRef]
- Lopes, F.; Leal, A.; Pinto, M.F.; Dourado, A.; Schulze-Bonhage, A.; Dümpelmann, M.; Teixeira, C. Removing artefacts and periodically retraining improve performance of neural network-based seizure prediction models. Scientific Reports 2023, 13. [CrossRef]
- Shafiezadeh, S.; Duma, G.M.; Mento, G.; Danieli, A.; Antoniazzi, L.; Del Popolo Cristaldi, F.; Bonanni, P.; Testolin, A. Calibrating deep learning classifiers for Patient-Independent Electroencephalogram Seizure Forecasting. Sensors 2024, 24, 2863. [CrossRef]
- Lu, J.; Gong, P.; Ye, J.; Zhang, J.; Zhang, C. A survey on machine learning from few samples. Pattern Recognition 2023, 139, 109480. [CrossRef]
- Ferreira, J.; Peixoto, R.; Lopes, L.; Beniczky, S.; Ryvlin, P.; Conde, C.; Claro, J. User involvement in the design and development of medical devices in epilepsy: A systematic review. Epilepsia Open 2024, 9, 2087–2100. [CrossRef]
- Quiroga, D.F.T.; Britton, J.W.; Wirrell, E.C. Patient and caregiver view on seizure detection devices: A survey study. Seizure 2016, 41, 179–181. [CrossRef]
- Hill, C.E.; Vanderboll, K.; Parent, J.M.; Skolarus, L.E.; Zahuranec, D.B. Health priorities and treatment preferences of adults with epilepsy: A narrative literature review with a systematic search. Epilepsy & Behavior 2025, 166, 110359. [CrossRef]
- Grzeskowiak, C.L.; Dumanis, S.B. Seizure Forecasting: patient and caregiver perspectives. Frontiers in Neurology 2021, 12. [CrossRef]
- Janse, S.A.; Dumanis, S.B.; Huwig, T.; Hyman, S.; Fureman, B.E.; Bridges, J.F. Patient and caregiver preferences for the potential benefits and risks of a seizure forecasting device: A best–worst scaling. Epilepsy & Behavior 2019, 96, 183–191. [CrossRef]
Figure 1.
Overview of neurostimulation architectures. (A) Open-Loop System (OLS). Stimulation is administered using predefined settings that operate independently of the patient’s real-time neural state. (B) Closed-Loop System (CLS). The device acquires neural signals (or surrogates thereof), detects candidate windows for intervention, and dynamically modulates its stimulation parameters to deliver precise, adaptive neuromodulation.
Figure 1.
Overview of neurostimulation architectures. (A) Open-Loop System (OLS). Stimulation is administered using predefined settings that operate independently of the patient’s real-time neural state. (B) Closed-Loop System (CLS). The device acquires neural signals (or surrogates thereof), detects candidate windows for intervention, and dynamically modulates its stimulation parameters to deliver precise, adaptive neuromodulation.
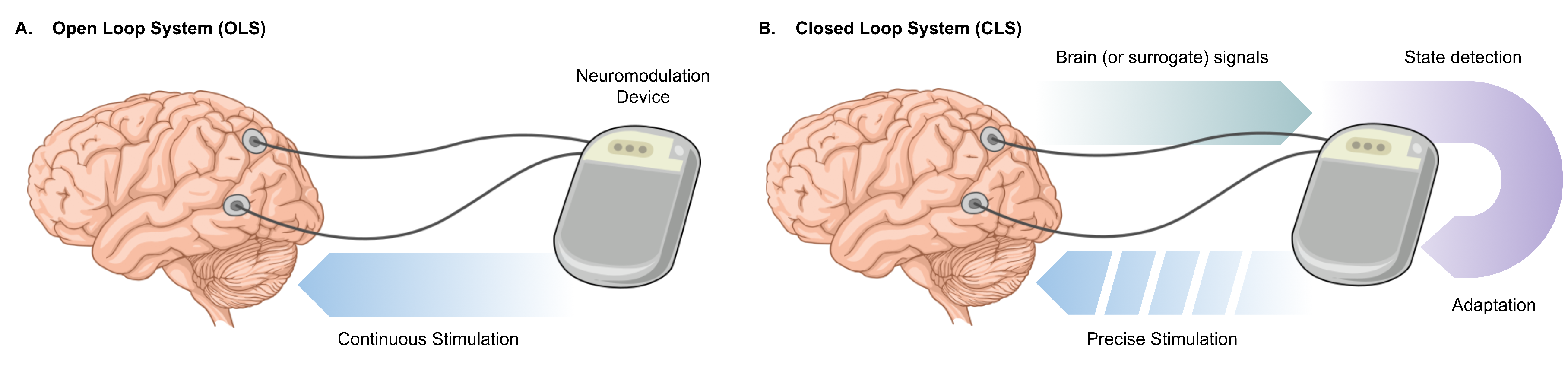
Figure 2.
Schematic representation of performance evaluation techniques. (A) K-fold Cross-Validation. The dataset is partitioned into folds used iteratively for training (orange) and testing (purple). Conventionally, the training set is larger than the test set, and in several folds the training data are chronologically older than the test data (e.g., iterations 1–3). (B) Time-series Cross-Validation. Training sets always precede their corresponding test sets in time, preserving the temporal structure of the data; the training set remains larger than the test set. (C) One-Shot Time-Series Cross-Validation. The training set is restricted to a single (or a small number of) chronologically earlier instances, which always precede the test set, providing a stringent temporally faithful evaluation.
Figure 2.
Schematic representation of performance evaluation techniques. (A) K-fold Cross-Validation. The dataset is partitioned into folds used iteratively for training (orange) and testing (purple). Conventionally, the training set is larger than the test set, and in several folds the training data are chronologically older than the test data (e.g., iterations 1–3). (B) Time-series Cross-Validation. Training sets always precede their corresponding test sets in time, preserving the temporal structure of the data; the training set remains larger than the test set. (C) One-Shot Time-Series Cross-Validation. The training set is restricted to a single (or a small number of) chronologically earlier instances, which always precede the test set, providing a stringent temporally faithful evaluation.
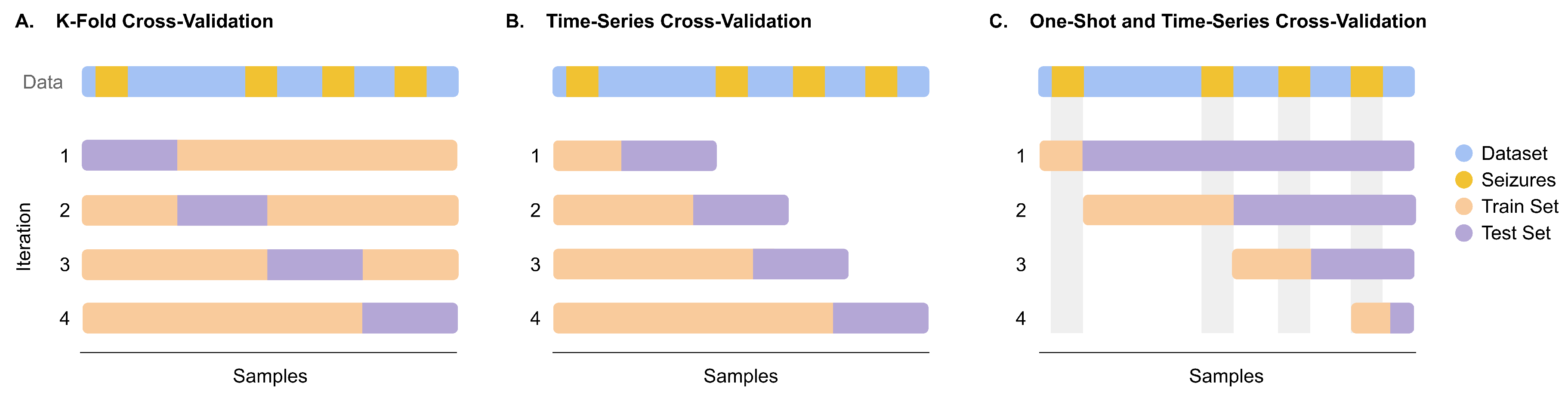

Table 1.
Contemporary neuromodulation systems used for drug-resistant epilepsy.
| System | Architecture | Approval Status | Examples |
|---|---|---|---|
| VNS (conventional) | OLS | Adjunctive therapy (CE 1994 (EU); FDA 1997 (US)) [73] | NeuroCybernetic Prosthesis System |
| VNS (latest) | CLS | Adjunctive therapy (CE 2014 (EU); FDA 2015 (US)) | AspireSR® and SenTiva® |
| DBS | OLS with CLS capability | Adjunctive therapy (CE 2010 (EU); FDA 2018 (US)) [55,74] | Percept™ PC |
| RNS | CLS | Adjunctive therapy (FDA 2013 (US) [75]) | NeuroPace RNS® System |
| eTNS | OLS | Adjunctive therapy (CE 2012 (EU)) | Monarch™ eTNS™ |
| rTMS | OLS and CLS | Investigational | |
| tDC | OLS and CLS | Investigational |
Table 2.
Current publicly available datasets containing human epilepsy data.
| Dataset | N | Age | L | DRE | Resect. | Img. Tech. |
|---|---|---|---|---|---|---|
| NeuroVista Trial Data [97] | 15 | Both | Long-term | Yes | No | iEEG |
| HUP iEEG [112] | 581 | Adult | 25 min | Yes | Yes | ECoG or SEEG |
| Epileptic EEG Dataset [113] | 6 | Unk. | 2h | No | No | EEG |
| TUH EEG Epilepsy Corpus [114] | 100 | Unk. | Long-term | No | No | EEG |
| CHB-MIT Scalp EEG Database [115] | 22 | Both | 9-42 h | Yes | No | EEG |
| Siena Scalp EEG [116] | 14 | Adult | 3.3-24 h | No | No | EEG |
| Xiaoya Fan et al. 2019 [117] | 23 | Unk. | 6-38 h | Yes | No | SEEG |
| SeizeIT2 [118] | 125 | Both | Long-term | Yes | No | Var.2 |
| Mesoscale Insights [119] | 5 | Adult | Unk.3 | Yes | Yes | ECoG & SEEG |
| Petr Nejedly et al. [120] | 39 | Adult | 5.07 h | Yes | No | SEEG |
| Fragility Multi-Center [121] | 91 | Adult | 1 min4 | Yes | Yes | ECoG or SEEG |
1 SEEG was recorded for 38 patients; 2 Behind-the-ear EEG, ECG, EMG, and movement (accelerometer and gyroscope); 3 10 mins before seizure, seizure (undefined length), and 5 mins post seizure; 4 30 seconds before and after the ictal event.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



