
Submitted:
18 November 2025
Posted:
19 November 2025
You are already at the latest version
Abstract
Objective: To characterize the findings on the ocular surface of patients with cystic fibrosis (CF) and non-cystic fibrosis bronchiectasis (NCFB) and to correlate them with the degree of inflammation and systemic severity. Methods: This work is an observational, cross-sectional study of patients with CF and NCFB. A complete pulmonary evaluation (demographic and clinical data, spirometry, blood sample, computed tomography) and ophthalmological evaluation (visual acuity, biomicroscopy, OSDI test, TBUT test, Schirmer test, and InflammaDry test) were performed. Results: A total of 87 patients were recruited (CF=45, NCFB=42). Both the TBUT test (r=–0.373, p=0.001) and the Schirmer test (r=–0.280, p=0.010) correlated with the degree of systemic inflammation in our sample. Conclusion: Both CF and NCFB can cause a systemic inflammatory state related to altered ocular surface homeostasis, leading to evaporative and hyposecretory dry eye. However, in neither disease does this subclinical alteration translate into severe symptoms or serious ophthalmologic complications for these patients.
Keywords:
ocular surface disease
; bronchiectasis
; cystic fibrosis
; systemic inflammation
; dry eye disease
Introduction
Ocular surface inflammatory disorders encompass a spectrum of conditions characterized by persistent inflammatory activity affecting the ocular surface and leading to a substantial deterioration in patients’ quality of life. Within this spectrum, dry eye disease constitutes a multifactorial disorder defined by the loss of tear film homeostasis and the presence of ocular symptoms, wherein tear film instability and hyperosmolarity, ocular surface inflammation and tissue damage, and neurosensory alterations serve as key etiological drivers [1,2].Systemic diseases and hypersensitivity reactions have been associated with its onset and, if left untreated, it can result in severe inflammatory dry eye, corneal damage, and vision loss [1].
Several pulmonary disorders can entail ocular surface involvement. Specifically, inflammatory dry eye disease (DED) has been linked to lung conditions such as asthma, sarcoidosis, or cystic fibrosis (CF) [2,3,4]. This association might be related to a connection between the lungs and the eyes, since the same immunological imbalance that affects the respiratory mucosa can be found on the ocular surface [2,5].
Non-cystic fibrosis bronchiectasis (NCFB) is defined as a chronic respiratory disease characterized by irreversible, abnormal dilation of the bronchi, most often resulting from recurrent respiratory infections, impaired mucociliary clearance, or underlying inflammatory or immune-mediated conditions [3,6,7]. The clinical syndrome is marked by persistent symptoms, most notably chronic cough with daily mucopurulent sputum production and a tendency toward frequent exacerbation. Common etiologies include prior severe pneumonia, nontuberculous mycobacterial infection, asthma, chronic obstructive pulmonary disease, gastroesophageal reflux disease, primary ciliary dyskinesia, immunodeficiency, autoimmune diseases, and, in a significant proportion of cases, idiopathic causes [8]. Beyond localized airway damage, growing evidence highlights the role of systemic inflammation as a key contributor to disease progression and its extrapulmonary manifestations [8,9,10]
Cystic fibrosis (CF) is a disease caused by variants in a gene that encodes the cystic fibrosis transmembrane conductance regulator (CFTR) protein [11,12]. CFTR plays an essential role in the transport of water, chloride ions, and sodium reabsorption in the epithelial cells of organs with exocrine function. In people with CF, altered mucociliary clearance leads to the development of chronic bronchial infections that generate an exaggerated inflammatory response [13].
CF and NCFB share similar pathophysiological features, most notably chronic airway colonization and a sustained, predominantly neutrophilic inflammatory response, despite differing in etiology. In both conditions, impaired mucociliary clearance leads to mucus retention, which promotes persistent colonization by pathogens such as Haemophilus influenzae and Pseudomonas aeruginosa and drives a vicious cycle of infection, inflammation, and progressive airway damage [1,14,16,17]. Neutrophil-driven inflammation is central to disease progression in both CF and NCFB, with excessive release of neutrophil serine proteases (e.g., neutrophil elastase) and proinflammatory cytokines contributing to tissue injury and airway remodeling [18,19]. This chronic inflammatory state is not limited to the airways, rather systemic inflammation is a recognized feature of both diseases and is associated with worse clinical outcomes and the development of extrapulmonary comorbidities. Elevated systemic inflammatory markers, such as neutrophil elastase and C-reactive protein, correlate with disease severity, frequency of exacerbations, and increased risk of extrapulmonary manifestations [20,21].
Although the exact cause of ocular surface alterations in people with CF and NCFB is not fully understood, it has been shown that in people with CF, the CFTR gene is expressed in the cells of the conjunctiva, cornea, and lacrimal glands, playing a role in tear film homeostasis [22]. The direct dysfunction of this ion channel may contribute to the development of dry eye [23]. In NCFB, although there are no mutations in the CFTR gene, persistent systemic inflammation may also indirectly contribute to ocular dysfunction. Notably, both conditions exhibit local inflammation, which may further support the involvement of the ocular surface as an extrapulmonary manifestation [24].
Some studies correlate certain biomarkers of systemic inflammation with ocular surface involvement, as occurs in Sjogren’s disease or graft-versus-host disease (GVHD) [25,26]. However, the correlation between the level of systemic inflammation in people with CF and NCFB and the appearance and severity of changes in the ocular surface are not well known, therefore, we consider this study important to acquire more knowledge of the inflammatory pathophysiology in these entities.
Understanding these manifestations is critical for early diagnosis and treatment. The development of screening protocols and early diagnosis and treatment may avoid several later complications. The objective of this study is to correlate systemic markers of inflammation in patients with CF and NCFB with the appearance and severity of ocular surface disease.
Methods
Study Design and Population
This work is a cross-sectional observational clinical study approved by the Provincial Ethics and Clinical Research Committee of Málaga (Protocol code: 1760-N-21 and date of approval: October 28, 2021). Only subjects who agreed to participate in the study following informed consent were included. Subject recruitment, data collection, and sample collection were conducted in accordance with the ethical principles of the most recent version of the Declaration of Helsinki and good clinical practice standards [27].
People with CF and NCFB were recruited sequentially and prospectively from the pulmonology unit when they attended their annual visit between October 2021 and April 2022. Other respiratory diseases were excluded. During the visit, pulmonology and analytical studies were performed. Personal data were processed in accordance with Regulation 2016/679 of the European Parliament and of the Council of April 27, 2016. Patients with CF or NCFB over 18 years of age and had stable signs and symptoms of the disease and who had signed the informed consent were included. The exclusion criteria were age younger than 18 years or older than 60 years, absence of clinical stability in the previous three months (hospital admissions, respiratory exacerbations requiring intravenous antibiotic therapy, or weight change >3%), refractive error >5 diopters (D), ocular disease, previous corneal surgery, use of contact lens and use of topical or systemic treatment contributing to the development of DED. People with CF and NCFB were referred to the Ophthalmology Department of the Regional University Hospital of Málaga for a complete ophthalmologic evaluation, and they were always visited by the same ophthalmologist.
Pulmonary Evaluation: Clinical, Functional, Radiological, and Analytical Variables
The pulmonary evaluation included demographic variables (age, sex, marital status). Anthropometric variables such as height (Holtain Limited, Crymych, UK) and weight (SECA, Hamburg, Germany) were measured. Body mass index was calculated. Severity criteria including age of onset of CF and NCFB symptoms and number of respiratory exacerbations in the previous year were recorded in the database. Exacerbations were categorized based on their severity into two groups: mild to moderate, when patients only required oral antibiotics, and severe, when hospitalization or intravenous antibiotics were necessary [28].
On the day of the visit, simple and forced spirometry (Jaeger Oxycon Pro, Erich Jaeger, Germany) were performed [29]. Values were expressed as a percentage of the predicted value in a reference population. The 6-minute walk test (6MWT) was also performed [30]. To assess structural damage, computed tomography was requested and assessed with the modified Bhalla [31] and modified Reiff scales [32].
Blood samples were collected for leukocyte count and acute phase reactants (alpha 1 antitrypsin, C-reactive protein, ferritin, and fibrinogen). The samples were analyzed in the laboratory of the Regional University Hospital of Málaga following Andalusian Health System protocols [33].
Ophthalmologic Evaluation. Anatomical and Functional Variables
Best corrected visual acuity (logMAR scale, Optotype ETDRS CHART 2, Zeiss Meditec AG, Germany), slit lamp evaluation of the anterior and posterior poles (SL 220, Zeiss, Spain), refraction (autorefractometer-keratometer, VISUREF, Zeiss, Spain), and intraocular pressure with an applanation tonometer with slit lamp support (Zeiss, Spain) were determined.
Dry eye disease was assessed per the TFOS DEWS II using a standardized protocol integrating symptoms and objective signs with a validated test [34]. The DED evaluation included the Ocular Surface Disease Index score (OSDI questionnaire, Allergan, USA) [35], Schirmer test type 1 (ST1) with sterile methylcellulose strips (Alcon, Spain), tear break-up time (TBUT), and fluorescein staining with sterile 1% sodium fluorescein strips (Alcon, Spain) to evaluate the ocular surface following the Oxford Grading Scale.
The OSDI uses a scale from 0 to 100 to assess the severity of symptoms related to ocular surface disease. A score above 13 is considered indicative of pathological ocular surface disease, meaning the patient has dry eye symptoms that should be treated. The Oxford Grading Scale is used to assess the severity of ocular surface damage by evaluating staining on the cornea and conjunctiva [36]. After applying fluorescein dye, the ocular surface is examined under cobalt blue light. The Oxford scale consists of five panels of reference images (graded from 0 to 5), each representing increasing severity of punctate epithelial erosions or staining on the ocular surface. The scale ranges from Grade 0 (no staining) to Grade 5 (severe staining), with higher grades indicating more extensive surface damage. TBUT values below 10 seconds and ST1 below 10 mm were considered pathological.
Statistical Analysis
Data were analyzed using the IBM SPSS 26.0 statistical program (IBM Corp., Armonk, NY, USA) for Windows. The results were expressed as percentages for qualitative data and as mean ± standard deviation or medians (interquartile ranges) for quantitative data according to the distribution of the data. The distribution of the data was analyzed using the Kolmogorov-Smirnov test. Categorical variables were analyzed by the chi-square test or Fisher’s exact test and quantitative data by Student’s t-test or the Mann-Whitney U test, as appropriate.
Severity Scores
A total inflammatory score was developed based on the statistical principles of Bonaccio et al. [39] for the Low-grade inflammation score (INFLA-score) in the Moli-sani study. For this purpose, four biomarkers of systemic inflammation (eosinophils, neutrophils, C-reactive protein, and alpha 1-antitrypsin) were selected. Each variable was divided into deciles. The highest deciles received a score of 1 to 4, while the lowest deciles received a score of -4 to -1. The fifth and sixth deciles received a score of 0. The score obtained for each biomarker was added to yield a total inflammatory score.
The pulmonary severity score was calculated using a methodology similar to that used by Bonaccio et al. for the INFLA-score in the Moli-sani study, which is based on specific statistical principles. In particular, for the pulmonary score, five factors were considered: FEV1, Bhalla score, Reiff score, number of exacerbations, and age at diagnosis. Each variable was divided into deciles to stratify the values. For FEV1 and the Bhalla score—indicators where high values correspond to normality and low values indicate disease—the deciles were weighted inversely, assigning negative scores to the lowest deciles and positive scores to the highest deciles. For the other variables (Reiff score, number of exacerbations, and age at diagnosis), the scoring followed the standard scheme, with positive scores for the highest deciles and negative scores for the lowest. The middle deciles (fifth and sixth) received a score of zero. The scores obtained for each factor were added to obtain a total pulmonary severity score that reflects the combination of the patient’s functional, radiological, clinical, and temporal status, maintaining the logic and structure of the initial inflammatory score but adapted to these specific pulmonary indicators.
An exploratory factor analysis was conducted to identify the latent factors underlying the study variables. The five factors considered were FEV1, Bhalla score, Reiff score, number of exacerbations, and age at diagnosis. Subsequently, individual factor scores were calculated using the regression method (REGR factor scores) to estimate the weight of each factor in each subject.
A correlation analysis was performed to evaluate the relationship between the inflammatory score and TBUT as well as between the inflammatory score and the Schirmer test.
Results
A total of 87 patients were recruited (CF=45, NCFB=42), with an average age of 34.5 ± 10.5 years. Patients with CF were younger due to their genetic etiology (CF=33.4 ± 9.7, NCFB=0.5 ± 11.6, p=0.03). The flowchart of patients included and excluded in the study is shown in Figure 1.
Almost half of the patients were men (48.3%) with no differences between groups. The biometric characteristics were balanced in both groups of patients while the age at onset of the disease was lower in the CF group (CF=5.8 ± 11.1, NCFB 15.1±16.0, p=0.03).
All clinical and demographic data are shown in Table 1.
Concerning the ophthalmological examination, 24.2% of patients had alterations in visual quality measured by the OSDI test and 24.1% of patients had some degree of punctate keratopathy (with no differences found between groups, p=0.859). The TBUT test was pathological in 47.1% of patients and was more severe in the CF group (average CF=9, NCFB =12.5). However, regarding ocular surface damage symptoms (such as itching, burning, tearing, or blurred vision, only 26.4% of patients found these findings bothersome or limiting and only 5.7% of cases were defined as chronic.
The InflammaDry test was performed only in the CF group, with a positive MMP9 detection in 60% of the patients. These ophthalmologic characteristics are collected in Table 2.
A correlation was made between the systemic inflammatory score and the findings on the ocular surface. Significant differences were found regarding the detection of evaporative dry eye using TBUT and hyposecretory dry eye using the Schirmer test (Figure 2 and Figure 3), but not with respect to the degree of keratitis measured using the Oxford Grading Scale or the impact on visual quality measured using the OSDI test.
Discussion
This study addresses for the first time the correlation of inflammatory dry eye in a cohort of patients with CF and NCFB. The relationship between systemic inflammatory status in patients with CF and evaporative or aqueous-deficient dry eye has previously been reported in the literature; however, this finding in patients with NCFB has not yet been described [1]. The objective of this study was to understand the pathophysiology of both inflammatory pulmonary entities with ocular surface alterations and to determine whether there are any differences between them.
CF represents a well-defined monogenic disorder caused by mutations in the CFTR gene, leading to defective chloride and bicarbonate transport across epithelial surfaces. In contrast, non–cystic fibrosis bronchiectasis (NCFB) encompasses a highly heterogeneous group of diseases with diverse etiologies, including post-infectious, immunodeficiency-related, autoimmune, and other less frequent causes [40].
Despite these fundamental differences in origin, both CF and the various forms of NCFB ultimately converge on a common pathophysiological cascade.
This shared pathway is characterized by impaired mucociliary clearance, chronic airway colonization and infection, persistent neutrophilic inflammation, oxidative stress, and progressive structural airway damage [41]. Over time, this results in a similar clinical trajectory marked by recurrent exacerbations, increased pulmonary comorbidity, and a sustained systemic inflammatory burden. Because CF and NCFB express the same mechanistic vicious cycle of mucus stasis, infection, and inflammation, differing primarily in their initiating cause, the downstream consequences are comparable across groups.
For this reason, and consistent with prior literature, CF and NCFB could be meaningfully compared when evaluating extra-pulmonary manifestations, including ocular surface alterations, as they share a common pathophysiological framework despite their distinct etiologic origins.
In this patient sample, both groups had similar demographic and clinical characteristics, though patients with CF were somewhat younger due to the genetic nature of their condition, therefore, a longer exposure time to systemic inflammation is assumed. In both entities, systemic inflammation was correlated to symptom severity and therapeutic needs [9].
Dry eye disease is a multifactorial condition of the ocular surface defined by loss of tear film homeostasis and associated ocular symptoms. Although it had previously been classified into two principal subtypes aqueous-deficient dry eye, characterized by impaired lacrimal gland function leading to reduced tear secretion and abnormal Schirmer test values, and evaporative dry eye, primarily driven by intrinsic or extrinsic meibomian gland dysfunction and typically reflected in decreased tear film stability and altered TBUT, this traditional dichotomy is now integrated within a broader etiopathogenic framework centred on tear film instability, hyperosmolarity, ocular surface inflammation and damage, and neurosensory [42].
In recent years, the neutrophil-lymphocyte and platelet-lymphocyte ratios in blood samples have been proposed as biomarkers of the inflammatory conditions of DED, conceptualizing dry eye as a systemic illness [43]. There are some common cytokines released in DED, including IL-4, IL-5, IL-13, IL-1α, IL-1β, IL-17, tumor necrosis factor, and interferon-α, which in turn play an important role in the vicious cycle of inflammation [44].
Regarding systemic inflammation related to CF and NCFB, some phenotypes related to increased eosinophils and neutrophils have been related to disease severity [45,46].
In our cohort, MMP9 detection was positive in 60% of the patients in the CF group. MMP9 appears to play a physiological role in corneal epithelial desquamation. Although MMP9 does not provide information on tear production, increased MMP9 activity in DED may contribute to altered corneal epithelial barrier function, increased corneal epithelial desquamation and corneal surface irregularity. MMP9 levels have been associated with signs of dry eye assessed by the TBUT and Schirmer test and serve as a biomarker of treatment response in DED [47].
In this sample, the TBUT test and the Schirmer test were found to correlate with the degree of inflammation in both groups of patients, which is consistent with other systemic conditions that cause inflammatory dry eye that have previously been reported [48]. This means that the alteration in the epithelial barrier in the tear gland, conjunctival and corneal epithelium, and meibomian glands due to sustained systemic inflammation in CF and NCFB could be the cause of both ophthalmological tests being altered, causing an induced DED.
Neither the degree of keratitis in these patients measured by the Oxford Grading Scale nor quality of life measured by the OSDI scale were statistically significant in this group of patients. This indicates that the ocular surface damage caused by systemic inflammation in patients with CF and NCFB may be subclinical and also that, given the severity of these diseases and the respiratory comorbidities in these patients, the alteration of the ocular surface does not constitute a problem in both groups’ quality of life. The lack of obvious symptoms may partly explain why routine clinical practice for CF and NCFB does not include systematic screening for DED. Moreover, having a thorough review by an ophthalmologist is not common in these patients, so subclinical findings are more easily detected. Even so, early detection is essential, especially before ocular surgery and in particular before corneal refractive or phacorefractive procedures. This is because undiagnosed DED can alter keratometry and corneal topography, intraocular lens (IOL) power calculations, and reduce postoperative visual quality [49]. In these settings, identifying and treating DED preoperatively is key to optimizing outcomes and lowering retreatment rates [50]. Furthermore, new therapies have increased life expectancy in CF, so DED, as a chronic, age-related condition, is likely to become more clinically relevant over time, with more patients needing cataract surgery. This trend further supports systematic preoperative screening and management of DED.
No significant differences were found between the two groups of patients, so CFTR expression cannot be attributed to the pathophysiology of this inflammatory dry eye, as other authors claim, but rather it could be due to the storm of systemic cytokines related to dry eye and which may be altered in these entities [51].
This study has several limitations. First, the sample size obtained was small, given the rarity of CF and the need to match both groups. Given that this study was conducted in individuals with CF, a low-prevalence disease, and at a single center, the number of participants ultimately enrolled was limited. This constraint affects the statistical power of the analysis, as a larger sample would allow for detecting subtler differences and yield more robust and generalizable estimates. Second, the etiology of bronchiectasis was heterogeneous (e.g., post-infectious, immunodeficiencies, allergic bronchopulmonary aspergillosis, primary ciliary dyskinesia, among others). This introduces substantial clinical and biological variability. This heterogeneity may act as a confounder, modulate systemic and ocular inflammatory phenotypes, and limit the direct extrapolation of our findings to populations with bronchiectasis of diverse etiologies. Also MMP-9 has not been measured in this group. Lastly, this is a cross-sectional study with no long-term follow-up.
Regarding its strengths, to the best of our knowledge, this is the first study to correlate systemic inflammation in bronchiectasis (associated or not with CF) with inflammatory dry eye.
In conclusion, both CF and NCFB can cause a systemic inflammatory state related to altered ocular surface homeostasis, leading to evaporative and hyposecretory dry eye. However, in neither disease does this subclinical alteration translate into severe symptoms or serious ophthalmologic complications for these patients. Further studies on the specific involvement of cytokines in the development of dry eye could be useful for increasing understanding of this condition.
Conflicts of Interest
No potential conflict of interest exists. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Quiroga-Garza, M.E.; Ruiz-Lozano, R.E.; Rodriguez-Gutierrez, L.A.; Khodor, A.; Ma, S.; Komai, S.; et al. Lessons Learned From Ocular Graft versus Host Disease: An Ocular Surface Inflammatory Disease of Known Time of Onset. Eye Contact Lens. 2024, 50, 212–21. [Google Scholar] [CrossRef]
- Singh, M.; Deokar, K.; Sinha, B.P.; Keena, M.; Desai, G. Ocular manifestations of common pulmonary diseases: a narrative review. Monaldi Arch Chest Dis Arch Monaldi Mal Torace. 2023, 94. [Google Scholar] [CrossRef]
- Gutiérrez, P.; Jiménez, L.; Martínez, J.; Alba, C.; Girón, M.V.; Olveira, G.; et al. Dry eye disease and morphological changes in the anterior chamber in people with cystic fibrosis. J Cyst Fibros Off J Eur Cyst Fibros Soc. 2025 Jan 7;S1569-1993(24)01860-5.
- Huang, Q.; Zheng, Y.; Zhang, C.; Wang, W.; Liao, T.; Xiao, X.; et al. Association between asthma and dry eye disease: a meta-analysis based on observational studies. BMJ Open. 2021, 11, e045275. [Google Scholar] [CrossRef]
- Allam, V.S.R.R.; Patel, V.K.; De Rubis, G.; Paudel, K.R.; Gupta, G.; Chellappan, D.K.; et al. Exploring the role of the ocular surface in the lung-eye axis: Insights into respiratory disease pathogenesis. Life Sci. 2024 Jul 15;349:122730.
- Choi, H.; McShane, P.J.; Aliberti, S.; Chalmers, J.D. Bronchiectasis management in adults: state of the art and future directions. Eur Respir J. 2024, 63, 2400518. [Google Scholar] [CrossRef]
- Barker, A.F.; Karamooz, E. Non-Cystic Fibrosis Bronchiectasis in Adults: A Review. JAMA. 2025. [Google Scholar]
- Gómez-Olivas JD, Oscullo G, Martínez-García MÁ. Etiology of Bronchiectasis in the World: Data from the Published National and International Registries. J Clin Med. 2023, 12, 5782.
- Doumat, G.; Aksamit, T.R.; Kanj, A.N. Bronchiectasis: A clinical review of inflammation. Respir Med. 2025 Aug;244:108179.
- Wang, X.; Olveira, C.; Girón, R.; García-Clemente, M.; Máiz, L.; Sibila, O.; et al. Blood Neutrophil Counts Define Specific Clusters of Bronchiectasis Patients: A Hint to Differential Clinical Phenotypes. Biomedicines. 2022, 10, 1044. [Google Scholar] [CrossRef]
- HGrasemann y, F. Ratjen, «Cystic Fibrosis», N. Engl. J. Med., vol. 389, n.o 18, pp. 1693-1707, 2023,.
- Mall, M.A.; Burgel, P.R.; Castellani, C.; Davies, J.C.; Salathe, M.; Taylor-Cousar, J.L. Cystic fibrosis. Nat Rev Dis Primer. 2024, 10, 53. [Google Scholar] [CrossRef]
- COlveira «Inflammation Oxidation Biomarkers in Patients with Cystic Fibrosis: The Influence of, A.z.i.t.h.r.o.m.y.c.i.n.; et al. COlveira et al «Inflammation Oxidation Biomarkers in Patients with Cystic Fibrosis: The Influence of, A.z.i.t.h.r.o.m.y.c.i.n.».; Eurasian, J. Med., vol. 49, n.o 2, pp. 118-123, jun. 2017.
- Schäfer, J.; Griese, M.; Chandrasekaran, R.; Chotirmall, S.H.; Hartl, D. Pathogenesis, imaging and clinical characteristics of CF and non-CF bronchiectasis. BMC Pulm Med. 2018, 18, 79. [Google Scholar] [CrossRef]
- Cantin, A.M.; Hartl, D.; Konstan, M.W.; Chmiel, J.F. Inflammation in cystic fibrosis lung disease: Pathogenesis and therapy. J Cyst Fibros Off J Eur Cyst Fibros Soc. 2015, 14, 419–30. [Google Scholar] [CrossRef]
- Wang, X.; Villa, C.; Dobarganes, Y.; Olveira, C.; Girón, R.; García-Clemente, M.; et al. Systemic Inflammatory Biomarkers Define Specific Clusters in Patients with Bronchiectasis: A Large-Cohort Study. Biomedicines. 2022, 10, 225. [Google Scholar] [CrossRef]
- Zarogoulidis, P.; Papanas, N.; Kioumis, I.; Chatzaki, E.; Maltezos, E.; Zarogoulidis, K. Macrolides: from in vitro anti-inflammatory and immunomodulatory properties to clinical practice in respiratory diseases. Eur J Clin Pharmacol. 2012, 68, 479–503. [Google Scholar] [CrossRef]
- Mall, M.A.; Davies, J.C.; Donaldson, S.H.; Jain, R.; Chalmers, J.D.; Shteinberg, M. Neutrophil serine proteases in cystic fibrosis: role in disease pathogenesis and rationale as a therapeutic target. Eur Respir Rev. 2024, 33, 240001. [Google Scholar] [CrossRef]
- Chalmers, J.D.; Metersky, M.; Aliberti, S.; Morgan, L.; Fucile, S.; Lauterio, M.; et al. Neutrophilic inflammation in bronchiectasis. Eur Respir Rev. 2025, 34, 240179. [Google Scholar] [CrossRef]
- Purushothaman, A.K.; Nelson, E.J.R. Role of innate immunity and systemic inflammation in cystic fibrosis disease progression. Heliyon. 2023, 9, e17553. [Google Scholar] [CrossRef]
- Roesch, E.A.; Nichols, D.P.; Chmiel, J.F. Inflammation in cystic fibrosis: An update. Pediatr Pulmonol. 2018 Nov;53(S3):S30–50.
- Felix, C.M.; Lee, S.; Levin, M.H.; Verkman, A.S. Pro-Secretory Activity and Pharmacology in Rabbits of an Aminophenyl-1,3,5-Triazine CFTR Activator for Dry Eye Disorders. Invest Ophthalmol Vis Sci. 2017, 58, :4506–13. [Google Scholar] [CrossRef]
- Giannakouras, P.; Kanakis, M.; Diamantea, F.; Tzetis, M.; Koutsandrea, C.; Papaconstantinou, D.; et al. Ophthalmologic manifestations of adult patients with cystic fibrosis. Eur J Ophthalmol. 2021 Apr 8;11206721211008780.
- Ozarslan Ozcan, D.; Kurtul, B.E.; Ozcan, S.C.; Elbeyli, A. Increased Systemic Immune-Inflammation Index Levels in Patients with Dry Eye Disease. Ocul Immunol Inflamm. 2022, 30, 588–92. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, J.; Liu, X.; Ganesan, K.; Shi, G. Identification of inflammatory markers as indicators for disease progression in primary Sjögren syndrome. Eur Cytokine Netw. 2024, 35, 1–12. [Google Scholar] [CrossRef]
- Alba-Linero, C.; Rodriguez Calvo De Mora, M.; Lavado Valenzuela, R.; Pascual Cascón, M.; Martín Cerezo, A.; Álvarez Pérez, M.; et al. Ocular surface characterization after allogeneic stem cell transplantation: A prospective study in a referral center. Indian J Ophthalmol. 2020, 68. [Google Scholar] [CrossRef]
- World Medical Association, «World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects», JAMA, vol. 310, n.o 20, pp. 2191-2194, nov. 2013,.
- P. T et al., «C-Reactive Protein Concentration in Steady-State Bronchiectasis: Prognostic Value of Future Severe Exacerbations. Data From the Spanish Registry of Bronchiectasis (RIBRON)», Arch. Bronconeumol., vol. 57, n.o 1, ene. 2021.
- J. Roca et al., «Spirometric reference values from a Mediterranean population», Bull. Eur. Physiopathol. Respir., vol. 22, n.o 3, pp. 217-224, 198.
- PAgarwala y, S.H. Salzman, «Six-Minute Walk Test: Clinical Role, Technique, Coding, and Reimbursement», Chest, vol. 157, n.o 3, pp. 603-611, mar. 2020.
- M. Bhalla et al., «Cystic fibrosis: scoring system with thin-section CT», Radiology, vol. 179, n.o 3, pp. 783-788, jun. 1991.
- DB Reiff, A. U. Wells, D. H. Carr, P. J. Cole, y D. M. Hansell, «CT findings in bronchiectasis: limited value in distinguishing between idiopathic and specific types», Am. J. Roentgenol. 1976, vol. 165, n.o 2, pp. 261-267, 1995.
- Directrices para el envío de especímenes a los laboratorios clínicos para el diagnóstico biológico. 2009.
- Wolffsohn, J.S.; Arita, R.; Chalmers, R.; Djalilian, A.; Dogru, M.; Dumbleton, K.; et al. TFOS DEWS II Diagnostic Methodology report. Ocul Surf. 2017, 15, 539–74. [Google Scholar] [CrossRef]
- RM Schiffman, M. D. Christianson, G. Jacobsen, J. D. Hirsch, y B. L. Reis, «Reliability and Validity of the Ocular Surface Disease Index», Arch. Ophthalmol., vol. 118, n.o 5, pp. 615-621, may 2000,.
- AJ Bron, V. E. Evans, y J. A. Smith, «Grading of corneal and conjunctival staining in the context of other dry eye tests», Cornea, vol. 22, n.o 7, pp. 640-650, oct. 2003.
- RSambursky, W.F. Davitt, M. Friedberg, y S. Tauber, «Prospective, multicenter, clinical evaluation of point-of-care matrix metalloproteinase-9 test for confirming dry eye disease», Cornea, vol. 33, n.o 8, pp. 812-818, ago. 2014.
- Messmer, E.M.; von Lindenfels, V.; Garbe, A.; Kampik, A. Matrix Metalloproteinase 9 Testing in Dry Eye Disease Using a Commercially Available Point-of-Care Immunoassay. Ophthalmology. 2016, 123, 2300–8. [Google Scholar] [CrossRef]
- M. Bonaccio et al., «A score of low-grade inflammation and risk of mortality: prospective findings from the Moli-sani study», Haematol. Roma, vol. 101, n.o 11, pp. 1434-1441, 2016.
- Martínez-García, M.A.; Olveira, C.; Máiz, L.; Girón RMa Prados, C.; de la Rosa, D.; et al. Bronchiectasis: A Complex, Heterogeneous Disease. Arch Bronconeumol. 2019, 55, 427–33. [Google Scholar] [CrossRef]
- Garcia-Clemente, M.; de la Rosa, D.; Máiz, L.; Girón, R.; Blanco, M.; Olveira, C.; et al. Impact of Pseudomonas aeruginosa Infection on Patients with Chronic Inflammatory Airway Diseases. J Clin Med. 2020, 9, 3800. [Google Scholar] [CrossRef]
- Craig, J.P.; Nelson, J.D.; Azar, D.T.; Belmonte, C.; Bron, A.J.; Chauhan, S.K.; de Paiva, C.S.; Gomes, J.A.P.; Hammitt, K.M.; Jones, L.; Nichols, J.J.; Nichols, K.K.; Novack, G.D.; Stapleton, F.J.; Willcox, M.D.P.; Wolffsohn, J.S.; Sullivan, D.A. TFOS DEWS II Report Executive Summary. Ocul Surf. 2017, 15, 802–812. [Google Scholar] [CrossRef]
- Alhalwani, A.Y.; Hafez, S.Y.; Alsubaie, N.; Rayani, K.; Alqanawi, Y.; Alkhomri, Z.; Hariri, S.; Jambi, S. Assessment of leukocyte and systemic inflammation index ratios in dyslipidemia patients with dry eye disease: a retrospective case‒control study. Lipids Health Dis. 2024, 23, 179. [Google Scholar] [CrossRef]
- Montero-Iruzubieta, J.; Sanchez Hernandez, M.C.; Dávila, I.; Leceta, A. The Importance of Preventing and Managing Tear Dysfunction Syndrome in Allergic Conjunctivitis and How to Tackle This Problem. J Investig Allergol Clin Immunol. 2023, 33, 439–445. [Google Scholar] [CrossRef]
- Wang, X.; Villa, C.; Dobarganes, Y.; Olveira, C.; Girón, R.; García-Clemente, M.; Máiz, L.; Sibila, O.; Golpe, R.; Menéndez, R.; Rodríguez-López, J.; Prados, C.; Martinez-García, M.A.; Rodriguez, J.L.; de la Rosa, D.; Duran, X.; Garcia-Ojalvo, J.; Barreiro, E. Phenotypic Clustering in Non-Cystic Fibrosis Bronchiectasis Patients: The Role of Eosinophils in Disease Severity. Int J Environ Res Public Health. 2021, 18, 8431. [Google Scholar] [CrossRef]
- Guan, W.J.; Oscullo, G.; He, M.Z.; Xu, D.Y.; Gómez-Olivas, J.D.; Martinez-Garcia, M.A. Significance and Potential Role of Eosinophils in Non-Cystic Fibrosis Bronchiectasis. J Allergy Clin Immunol Pract. 2023, 11, 1089–1099. [Google Scholar] [CrossRef]
- Pinto-Fraga, J.; Enríquez-de-Salamanca, A.; Calonge, M.; González-García, M.J.; López-Miguel, A.; López-de la Rosa, A.; García-Vázquez, C.; Calder, V.; Stern, M.E.; Fernández, I. Severity, therapeutic, and activity tear biomarkers in dry eye disease: An analysis from a phase III clinical trial. Ocul Surf. 2018, 16, 368–376. [Google Scholar] [CrossRef]
- Li, X.; Xu, X.; Li, J.; Huang, Y.; Wang, C.; Zhang, Y.; Zhang, L. Direct and indirect costs of allergic and non-allergic rhinitis to adults in Beijing, China. Clin Transl Allergy. 2022, 12, e12148. [Google Scholar] [CrossRef]
- Sharma, B.; Soni, D.; Saxena, H.; Stevenson, L.J.; Karkhur, S.; Takkar, B.; Vajpayee, R.B. Impact of corneal refractive surgery on the precorneal tear film. Indian J Ophthalmol. 2020, 68, 2804–2812. [Google Scholar] [CrossRef]
- Moshirfar, M.; Brown, A.H.; Sulit, C.A.; Corbin, W.M.; Ronquillo, Y.C.; Hoopes, P.C. Corneal Refractive Surgery Considerations in Patients with Cystic Fibrosis and Cystic Fibrosis Transmembrane Conductance Regulator-Related Disorders. Int Med Case Rep J. 2022 Nov 9;15:647-656.
- Schneider-Futschik, E.K.; Zhu, Y.; Li, D.; Habgood, M.D.; Nguyen, B.N.; Pankonien, I.; Amaral, M.D.; Downie, L.E.; Chinnery, H.R. The role of CFTR in the eye, and the effect of early highly effective modulator treatment for cystic fibrosis on eye health. Prog Retin Eye Res. 2024 Nov;103:101299.
Figure 1.
Flowchart of patients studied. Abbreviations: NCFB, non-cystic fibrosis bronchiectasis; CF, cystic fibrosis; N, sample size; D, diopters; LASIK, laser-assisted in situ keratomileusis; OCT, optical coherence tomography.
Figure 1.
Flowchart of patients studied. Abbreviations: NCFB, non-cystic fibrosis bronchiectasis; CF, cystic fibrosis; N, sample size; D, diopters; LASIK, laser-assisted in situ keratomileusis; OCT, optical coherence tomography.
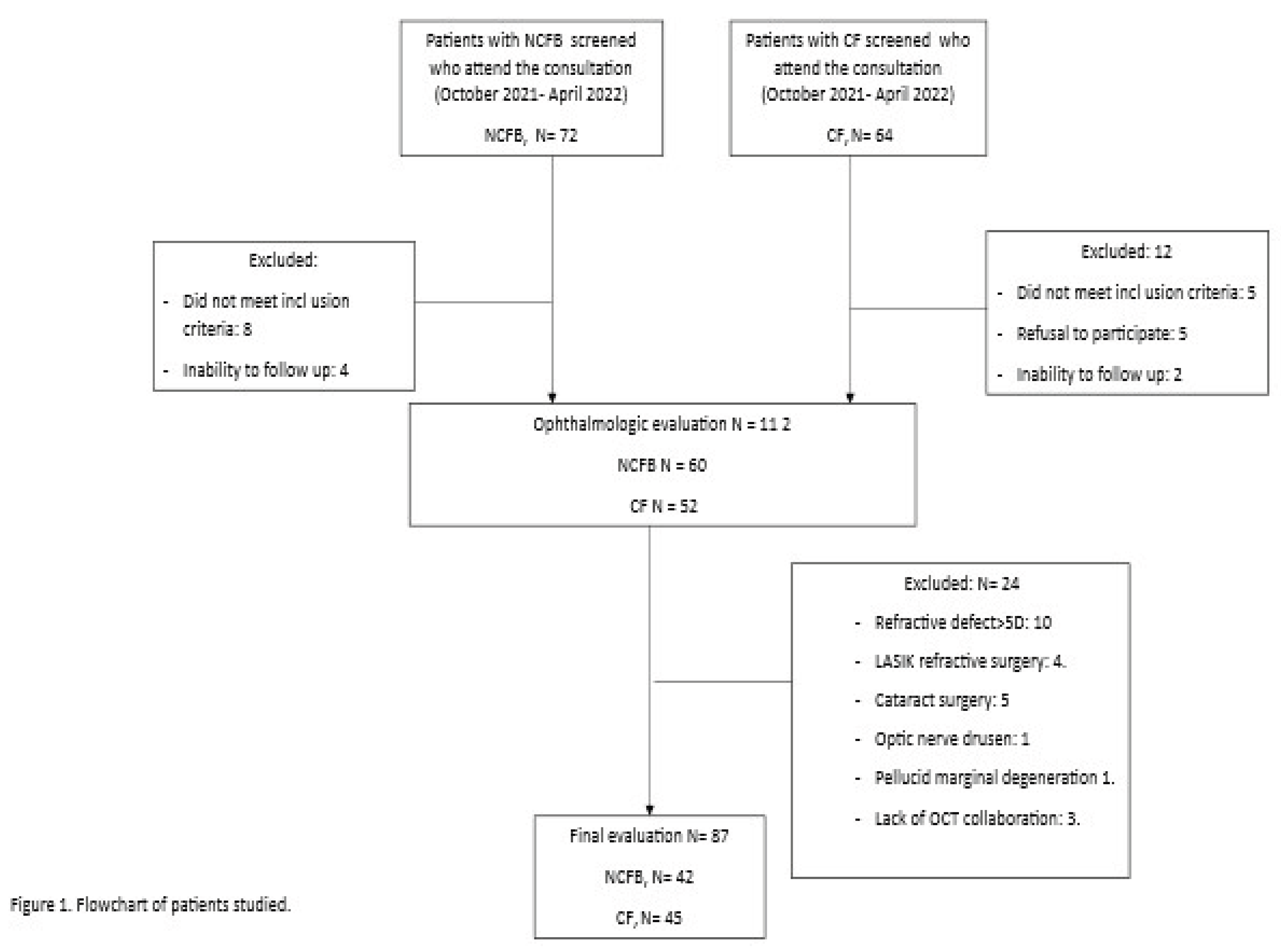
Figure 2.
Correlation between inflammatory score and TBUT.
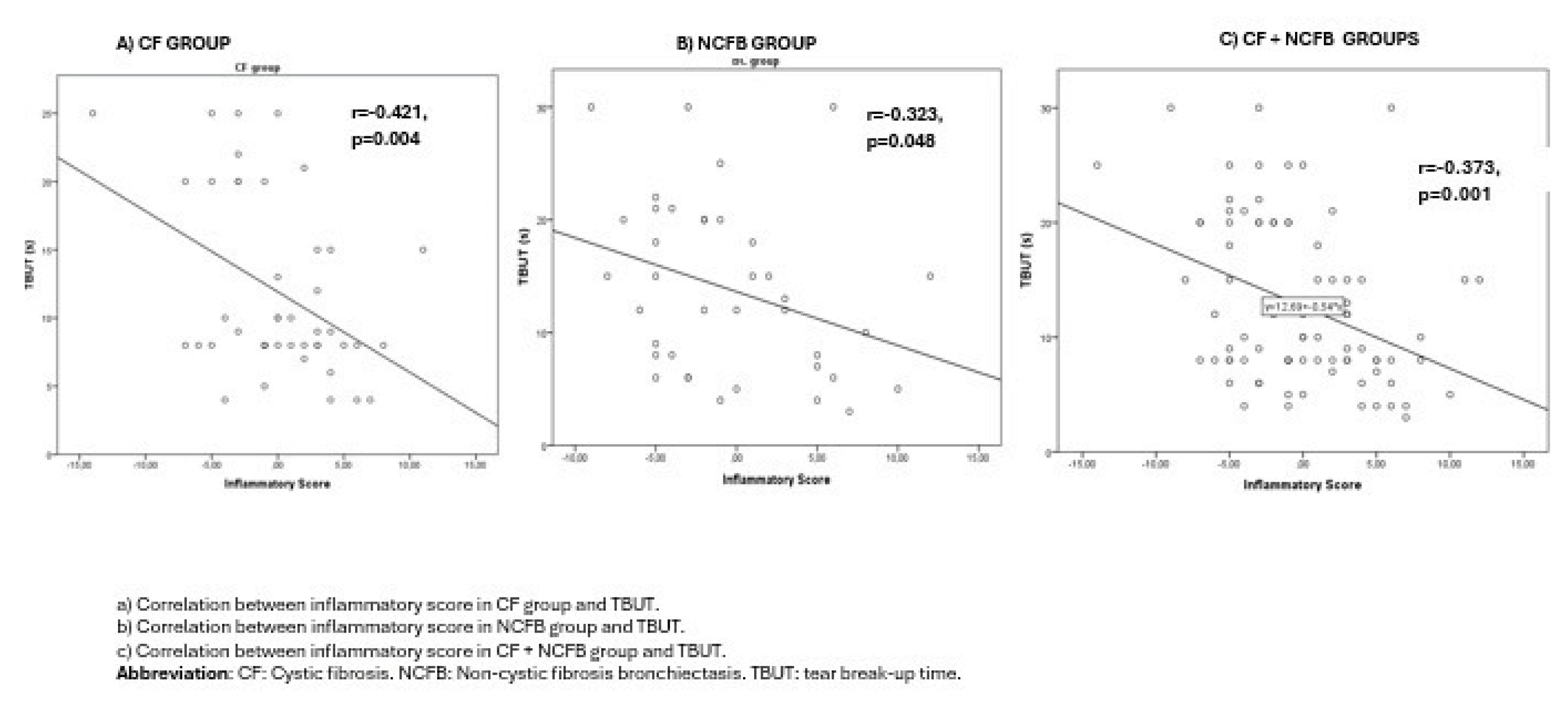
Figure 3.
Correlation between inflammatory score and Schirmer test.
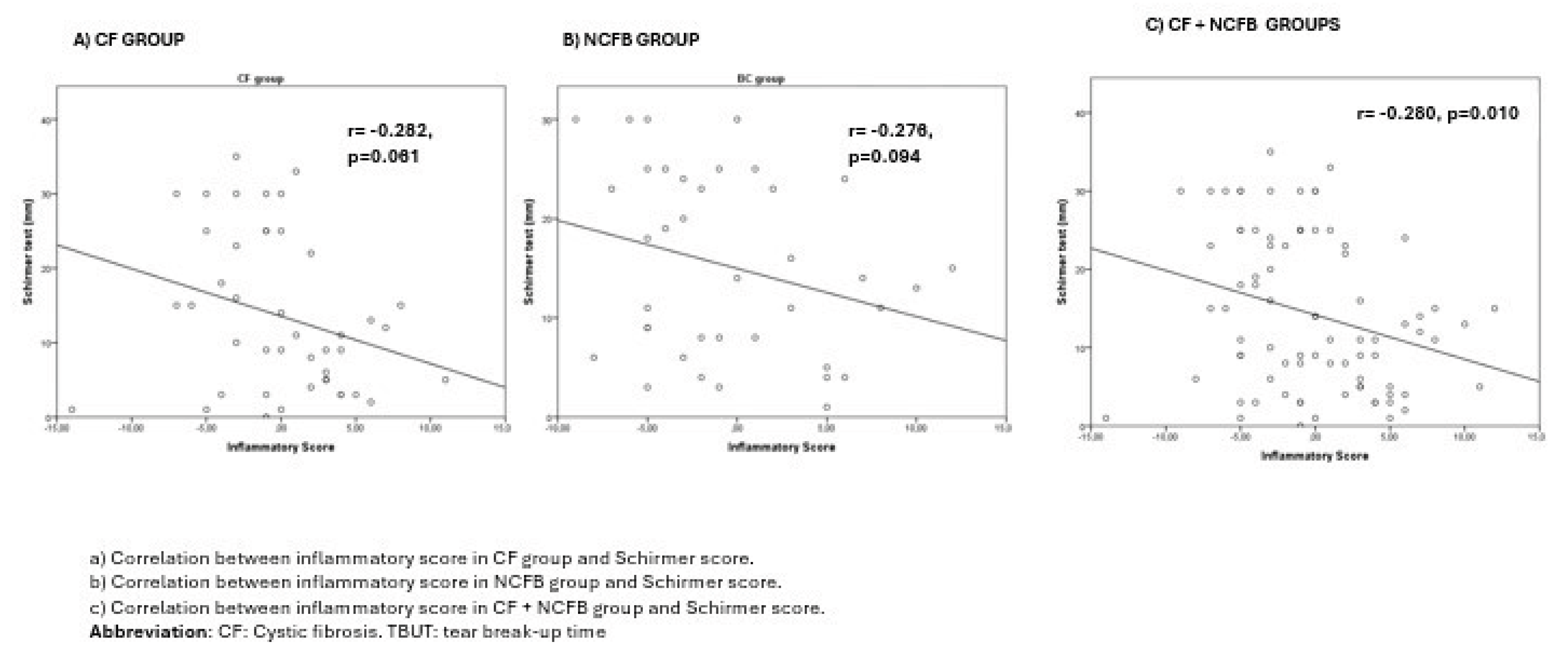

Table 1.
Clinical and demographic data of patients with NCFB and CF.
| All (N=87) | CF (n=45) | NCFB (n=42) |
P value | |||
|---|---|---|---|---|---|---|
| Age (years) | 34.5±10.5 | 33.4±9.7 | 40.5±11.6 | 0.003 | ||
| Gender, M, n (%) | 42 (48.3) | 25 (55.6) | 20 (47.6) | 0.459 | ||
| Height (cm) | 167.2±9.6 | 166.0±9.8 | 168.6±9.4 | 0.223 | ||
| Weight (kg) | 67.2±16.8 | 66.2±19.1 | 68.3±14.1 | 0.556 | ||
| BMI (kg/m2) | 23.8±5.1 | 23.7±5.8 | 24.0±4.4 | 0.741 | ||
| Total exacerbations in the previous year | 1.1±1.4 | 1.3±1.7 | 0.81±0.97 | 0.112 | ||
| Charlson Comorbidity Index, median [IQR] | 1 [1-2] | 1 [1-2] | 1 [1-1] | 0.058 | ||
| Etiology of bronchiectasis, n (%) | - | |||||
|
- | - | 9 (21.4) | |||
|
- | - | 7 (16.7) | |||
|
- | - | 2 (4.8) | |||
|
- | - | 1 (2.4) | |||
|
- | - | 23 (54.8) | |||
|
||||||
|
- | 15 (33.3) | - | - | ||
|
- | 19 (42.2) | - | - | ||
|
- | 11 (24.4) | - | - | ||
|
||||||
|
62.4±24.7 | 56.7±23.4 | 68.5±24.9 | 0.025 | ||
|
70.4±19.3 | 66.5±19.4 | 74.5±18.5 | 0.055 | ||
|
84.9±16.4 | 81.6±15.5 | 88.4±16.8 | 0.053 | ||
|
97.0±1.9 | 96.9±2.0 | 97.2±1.9 | 0.534 | ||
|
94.4±4.5 | 94.0±4.6 | 95.0±4.4 | 0.244 | ||
|
0.0±1.0 | -0.4±1.0 | 0.4±0.8 | <0.001 | ||
|
||||||
|
4.6±4.3 | 5.3±5.0 | 3.8±3.3 | 0.101 | ||
|
16.0±5.4 | 14.8±6.2 | 17.3±4.1 | 0.029 | ||
|
||||||
|
7340.5±2120.2 | 7548±2438 | 7117.7±1717.5 | 0.347 | ||
|
56.8±10.5 | 55.4±12.0 | 58.3±8.5 | 0.197 | ||
|
3.4±2.6 | 3.7±2.8 | 3.1±2.3 | 0.271 | ||
|
51.7±43.1 | 48.2±32.6 | 55.1±51.6 | 0.495 | ||
|
352.0±100.0 | 327.2±90.0 | 368.7±104.4 | 0.144 | ||
|
9.1±14.3 | 9.5±14.1 | 8.6±14.7 | 0.794 | ||
|
134.4±27.8 | 138.3±27.8 | 129.7±27.4 | 0.162 | ||
|
43 (49.4) | 25 (55.6) | 18 (42.9) | 0.236 |
Abbreviations: NCFB: non-cystic fibrosis bronchiectasis; BMI: Body mass index; CFTR: Cystic fibrosis transmembrane conductance regulator; FEV1: Forced expiratory volume in 1 second; FVC: Forced vital capacity; CRP: C-reactive protein. The quantitative data is presented as mean ± standard deviation.
Table 2.
Ophthalmologic characteristics among patients with CF compared to NCFB in dry eye disease.
| All (N=87) | CF (n=45) |
NCFB (n=42) | P value | |
|---|---|---|---|---|
| Age (years) | 34.5±10.5 | 33.4±9.7 | 40.5±11.6 | 0.003 |
| Gender, Male, n (%) | 42 (48.3) | 25 (55.6) | 20 (47.6) | 0.459 |
| Sphere | -0.86±2.17 | -0.90±2.17 | -0.60±2.33 | 0.538 |
| Cylinder | -0.77±0.69 | -0.75±0.69 | -0.78±0.70 | 0.803 |
| Cylinder axis | 88.4±55.2 | 82.8±52.6 | 94.8±58.1 | 0.329 |
| SE | -1.1±2.17 | -1.17±2.16 | -1.10±2.21 | 0.868 |
| BCVA | 1.0±0.05 | 1.01±0.06 | 1.00±0.02 | 0.109 |
| IOP (mmHg) | 17.4±2.6 | 17.6±2.8 | 17.1±2.30 | 0.431 |
| T-BUT<10s, n (%) | 41 (47.1) | 25 (55.6) | 16 (38.1) | 0.103 |
| T-BUT (s) | 10 [8-20] | 9 [8-17.5] | 12.5 [6.75-20] | 0.043 |
| ST1<10, n (%) | 34 (39.1) | 18 (40.0) | 16 (38.1) | 0.856 |
| ST1 (mm) | 14 [8-21] | 11 [4.5-24] | 13,5 [6-23.25] | 0.750 |
| OSDI>13, n (%) | 21 (24.2) | 9 (20.0) | 12 (28.6) | 0.351 |
| Visual symptoms, n (%) | 0.033 | |||
|
59 (67.8) | 26 (57.8) | 33 (78.6) | |
|
23 (26.4) | 14 (31.1) | 9 (21.4) | |
|
5 (5.7) | 5 (11.1) | 0 (0) | |
|
0 (0.0) | 0 (0.0) | 0(0) | |
|
1.32±0.62 | 1.33±0.64 | 1.31±0.60 | 0.859 |
|
21 (24.1) | 11 (24.4) | 10 (23.8) | 0.945 |
|
- | 24 (60) | - | - |
Abbreviations: NCFB: non-cystic fibrosis bronchiectasis; BCVA: best-corrected visual acuity; CF: cystic fibrosis; IOP: intraocular pressure; OSDI: Ocular Surface Disease Index; SE: spherical equivalent; TBUT: tear break-up time; ST: Schirmer test; MMP9: Matrix Metalloproteinase 9. The quantitative data is presented as mean ± standard deviation or medians (interquartile ranges).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



