Submitted:
18 November 2025
Posted:
18 November 2025
You are already at the latest version
Abstract
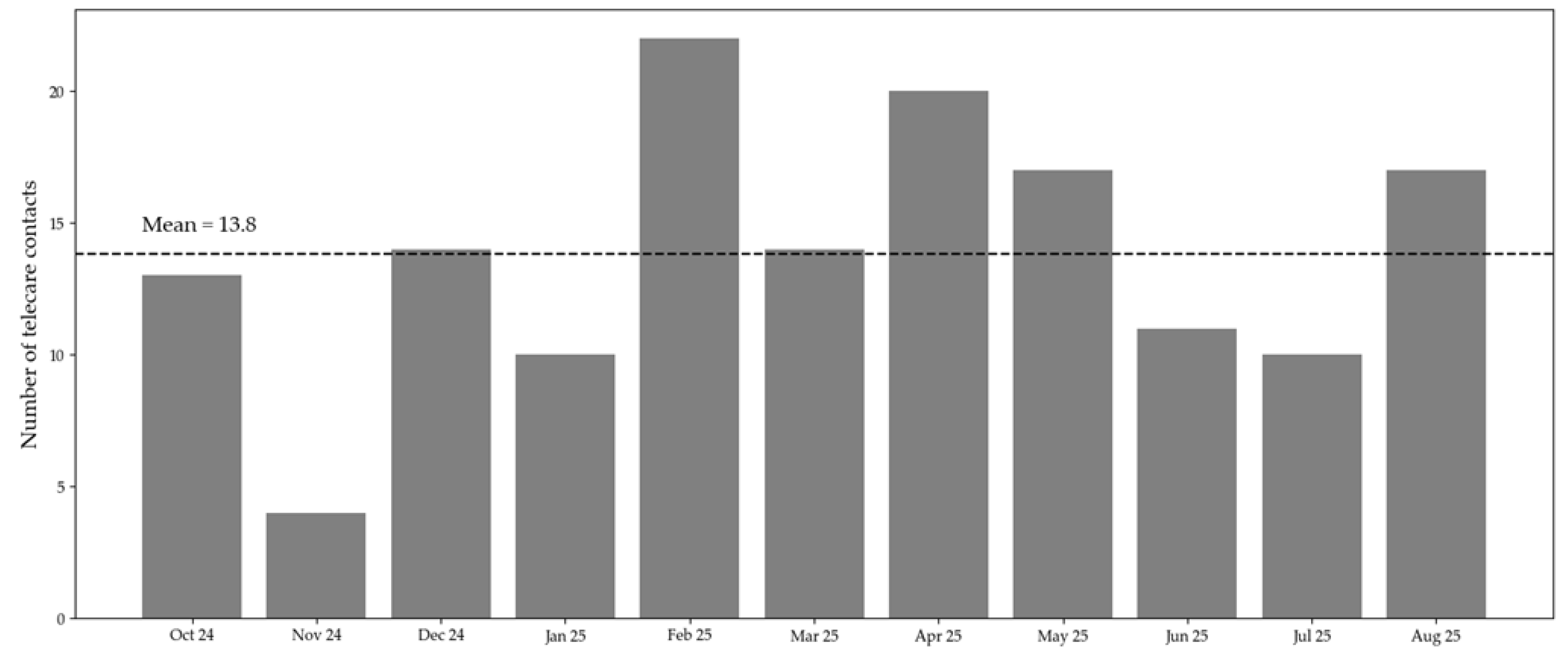
Background: Digital transformation in healthcare has progressed rapidly in hospitals and primary care, while long-term care facilities have often been left behind. The CareConnect project, funded under the German Model Program for Telecare (§ 125a SGB XI), aimed to implement and evaluate a comprehensive telecare system in two nursing homes in Germany, to improve collaboration across sectors, enhance communication between professionals, and strengthen nurses’ digital competencies. Objective: This implementation study examined the feasibility, acceptability, and early adoption of a multiprofessional telecare system in nursing homes, identifying key facilitators, barriers, and perceived effects on interprofessional collaboration and care delivery. Methods: A participatory implementation design was employed over 15 months (June 2024–August 2025), involving a university hospital, two nursing homes (NHs), and four medical practices in an urban region. The intervention consisted of teleconsultations and interdisciplinary case discussions utilizing a certified video platform, combined with diagnostic devices (e.g., otoscopes, dermatoscopes, ECGs). Implementation data included quantitative usage statistics, researcher observations, and user feedback collected during the rollout phase. Data were analyzed descriptively to assess usage patterns, case characteristics, and implementation experiences. Results: A total of 152 documented telecare contacts were conducted with 69 participating residents. Most interactions occurred with general practitioners (48.7%) and dermatologists (23%). Across all contacts, in 79% of cases, there was no need for an in-person visit or transportation. Physicians rated most cases as suitable for digital management, as indicated by a mean of 4.09 (SD = 1.00) on a 5-point Likert scale. Nurses reported improved communication, time savings, and enhanced technical and diagnostic skills. Key challenges included delayed technical integration, interoperability issues, and varying interpretations of data protection requirements across facilities. Conclusions: The CareConnect pilot demonstrates that telecare can effectively improve access to specialized care and strengthen interprofessional collaboration in nursing homes. A participatory, user-centered approach proved crucial for acceptance and sustainability. Future scale-up requires stable technical infrastructures, clear reimbursement pathways, and harmonized legal frameworks.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Implementation Strategy
- 1.
- Needs assessment and co-design: At the beginning, three interdisciplinary workshops were held with nursing staff, physicians, and IT specialists to identify care needs, communication barriers, and expectations regarding telecare and its use cases. The mechanism of change employed was stakeholder engagement, expected to increase acceptability and workflow fit. Based on the workshop findings, the project team developed an initial telecare concept tailored to the organizational routines and technical capabilities of both NHs. The expected outcome was a jointly developed, contextually adapted telecare concept that defined contact types, scheduling structures, and equipment requirements.
- 2.
- Training and technical onboarding: Following the co-design phase, all participating nurses received hands-on training on the use of the telecare system (including the certified video consultation software and additional diagnostic devices like otoscopes, dermatoscopes, and ECGs). The training sessions functioned as multiplier trainings, enabling internal dissemination of skills. Test runs were incorporated to ensure technical readiness and familiarize users with the workflow. The mechanism of change was capacity building, expected to increase digital competence and reduce uncertainty.
- 3.
- Implementation and continuous feedback: During the 11-month implementation phase, teleconsultations and interdisciplinary case discussions were conducted in routine care. The process was accompanied by three structured feedback rounds, in which nursing staff provided input on usability, technical challenges, perceived benefits, and workflow obstacles. Through this iterative refinement, the implementation strategy was adapted to the feedback, where applicable, aiming to achieve the expected outcome of progressively integrating telecare into daily routines.
2.3. Data Sources
- Telecare documentation: The standardized documentation in project-specific spreadsheets completed by physicians after each telecare contact included date of contact, reason for contact, diagnostic instruments used, outcome/treatment decision, and need for re-contact. Furthermore, physicians’ evaluation of the digital suitability of the contact and the technical reliability was measured using a 5-point Likert scale.
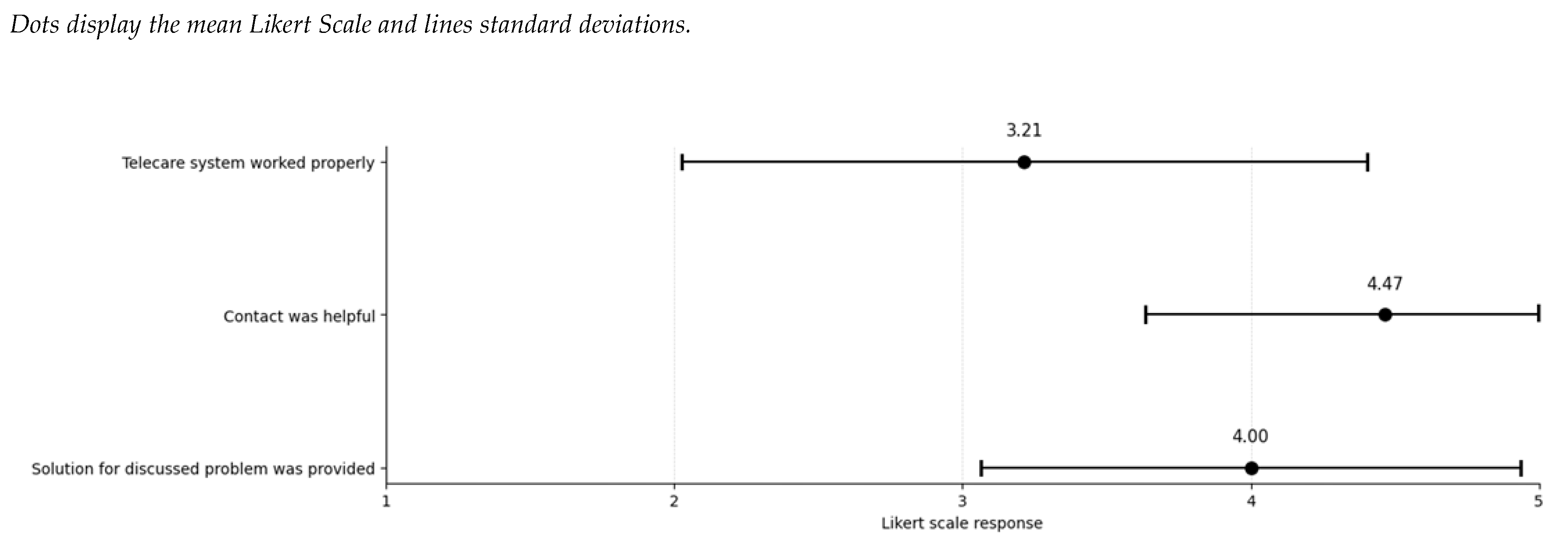
- Structured online nurse survey: This anonymous survey was offered to nurses after every telecare contact from May to August 2025. This survey captured the total frequencies of contacted professionals and the reason for the contact. Nurses’ assessment of the usefulness of the contact, the extent to which the problem could be resolved, and the technical reliability was measured using a 5-point Likert scale.
- Researcher observations: Field notes were taken during workshops, training sessions, test runs, and feedback meetings.
- Semi-structured participant feedback was obtained during regular round-table discussions and short debriefings during the implementation phase.
2.4. Process Evaluation
2.5. Analytical Framework
2.6. Ethical Considerations
3. Results
3.1. Needs Assessment and Co-Design
3.1.1. Contextual Characteristics of Participating Nursing Homes
3.1.2. Workshop Findings
3.2. Training/Onboarding
3.3. Implementation and Continuous Feedback
3.4. Quantitative Results
3.5. Facilitators and Barriers
3.6. Future Needs/ Need for Long-Term Implementation
4. Discussion
4.1. Implications
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CFIR | Consolidated Framework for Implementation Research |
| DNT | Digital nursing technologies |
| ECG | Electrocardiogram |
| EHDS | European Health Data Space |
| GKV | German: Gesetzliche Krankenversicherung |
| NH | Nursing Home |
| SGB | German: Sozialgesetzbuch |
| TI | Telematics Infrastructure |
| WHO | World Health Organization |
| Linear dichroism |
References
- World Health Organization. State of the World’s Nursing 2020: Investing in Education, Jobs and Leadership; 978-92-4-000327-9; World Health Organization: Geneva, 2020.
- Kubek, V. Digitalisierung in der Pflege: Überblick über aktuelle Ansätze. In Digitalisierung in der Pflege: Zur Unterstützung einer besseren Arbeitsorganisation, Kubek, V., Velten, S., Eierdanz, F., Blaudszun-Lahm, A., Eds.; Springer Berlin Heidelberg: Berlin, Heidelberg, 2020; pp. 15-20.
- IGES Institut. Zwischenbericht: Effizienzpotenziale durch digitale Anwendungen in der Pflege; Bundesministerium für Gesundheit: Berlin, 2022.
- Walzer, S.; Armbruster, C.; Mahler, S.; Farin-Glattacker, E.; Kunze, C. Factors Influencing the Implementation and Adoption of Digital Nursing Technologies: Systematic Umbrella Review. J Med Internet Res 2025, 27, e64616. [CrossRef]
- Chua, M.; Lau, X.K.; Ignacio, J. Facilitators and barriers to implementation of telemedicine in nursing homes: A qualitative systematic review and meta-aggregation. Worldviews Evid Based Nurs 2024, 21, 318-329. [CrossRef]
- Boyle, L.D.; Husebo, B.S.; Vislapuu, M. Promotors and barriers to the implementation and adoption of assistive technology and telecare for people with dementia and their caregivers: a systematic review of the literature. BMC Health Services Research 2022, 22. [CrossRef]
- Chiang, K.-F.; Wang, H.-H.; Chien, I.K.; Liou, J.-K.; Hung, C.-L.; Huang, C.-M.; Yang, F.-Y. Healthcare providers’ perceptions of barriers in implementing of home telecare in Taiwan: A qualitative study. International Journal of Medical Informatics 2015, 84, 277-287. [CrossRef]
- Wüller, H.; Koppenburger, A. Digitalisierung in der Pflege. In Systematische Entwicklung von Dienstleistungsinnovationen : Augmented Reality für Pflege und industrielle Wartung, Wiesche, M., Welpe, I.M., Remmers, H., Krcmar, H., Eds.; Springer Fachmedien Wiesbaden: Wiesbaden, 2021; pp. 111-124.
- Kilfoy, A.; Hsu, T.-C.C.; Stockton-Powdrell, C.; Whelan, P.; Chu, C.H.; Jibb, L. An umbrella review on how digital health intervention co-design is conducted and described. npj Digital Medicine 2024, 7, 374. [CrossRef]
- Pinnock, H.; Barwick, M.; Carpenter, C.R.; Eldridge, S.; Grandes, G.; Griffiths, C.J.; Rycroft-Malone, J.; Meissner, P.; Murray, E.; Patel, A.; et al. Standards for Reporting Implementation Studies (StaRI): explanation and elaboration document. BMJ Open 2017, 7, e013318. [CrossRef]
- Damschroder, L.J.; Reardon, C.M.; Widerquist, M.A.O.; Lowery, J. The updated Consolidated Framework for Implementation Research based on user feedback. Implementation Science 2022, 17, 75. [CrossRef]
- Krick, T.; Huter, K.; Domhoff, D.; Schmidt, A.; Rothgang, H.; Wolf-Ostermann, K. Digital technology and nursing care: a scoping review on acceptance, effectiveness and efficiency studies of informal and formal care technologies. BMC Health Services Research 2019, 19. [CrossRef]
- Greenhalgh, T.; Wherton, J.; Papoutsi, C.; Lynch, J.; Hughes, G.; A’Court, C.; Hinder, S.; Fahy, N.; Procter, R.; Shaw, S. Beyond Adoption: A New Framework for Theorizing and Evaluating Nonadoption, Abandonment, and Challenges to the Scale-Up, Spread, and Sustainability of Health and Care Technologies. J Med Internet Res 2017, 19, e367. [CrossRef]
- Stephens, C.E.; Allison, T.A.; Flint, L.A.; David, D.; Wertz, V.; Halifax, E.; Barrientos, P.; Ritchie, C.S. Assessing Technical Feasibility and Acceptability of Telehealth Palliative Care in Nursing Homes. Palliative Medicine Reports 2022, 3, 181-185. [CrossRef]
- Offermann, J.; Wilkowska, W.; Schaar, A.K.; Brokmann, J.C.; Ziefle, M. What Helps to Help? Exploring Influencing Human-, Technology-, and Context-Related Factors on the Adoption Process of Telemedical Applications in Nursing Homes. Springer Nature Switzerland: 2023; pp. 273-295.
- May, C.; Finch, T. Implementing, Embedding, and Integrating Practices: An Outline of Normalization Process Theory. Sociology 2009, 43, 535-554. [CrossRef]
- Federal Ministry of Health. Germany’s Digitalisation Strategy for Health and Care; Federal Ministry of Health: Berlin, 2023.
- Federal Ministry of Health. Telematics Infrastructure (TI): Secure digital networking in the health system. Available online: https://gesund.bund.de/en/telematics-infrastructure (accessed on 14.11.2025).
- European Commission. European Health Data Space (EHDS) – Regulation Proposal; European Commission: Brussels, 2022.
- GKV Spitzenverband. Modellprogramm nach § 125a SGB XI – Telepflege. Available online: https://www.gkv-spitzenverband.de/pflegeversicherung/forschung/modellprogramm_125a_sgb_xi/pflege_modellprojekte_125a.jsp (accessed on.

| Desired telecare contacts | Nursing home A | Nursing home B |
| Infectious Disease Consultations* | yes | |
| Wound specialist | yes | probably |
| Dermatology | yes | |
| Intensive Care | no | yes |
| Dentist | yes | no |
| Neurologist | yes | |
| Opthalmology | yes | |
| Ear-Nose-Throat Medicine | yes | |
| General Practitioner | yes | |
| Anaesthesiologist | no | yes |
| Holiday Consultations | yes | |
| Emergency Department Nurses | probably | |
| Telecare contacts | Nursing home A | Nursing home B |
| Infectious Disease Consultations* | Wednesday 1 pm | Friday 1 pm |
| Dermatology | Wednesday 2 pm | Wednesday 1 pm |
| Intensive Care | Thursday, 2 pm every 2 weeks | - |
| Dentist | - | Thursday, 10 am every 3 weeks |
| General Practitioner | Tuesday | Once a week |
| Anaesthesiologist | Once a week | - |
| Emergency Department Nurses | Wednesday until 7 pm | |
| Holiday Consultations | Official Holidays 4 hours/day | |
| Telecare contact | Total cases | Reason for contact (% of all cases) | Managed completely digital, % of each contact reason | Reason suitable for complete digital contact, Mean Likert Scale (SD*) |
| Infectious disease consultations * | 74 | Respiratory symptoms (35.1%) | 77% | 4.28 (0.83) |
| Wounds/pressure ulcers (29.7%) | 89% | 4.16 (0.69) | ||
| Pain (6.8%) | 75% | 4.0 (0.82) | ||
| Dermatology | 35 | Eczema/dermatitis (28.6%) | 100% | 4.73 (0.47) |
| Pressure ulcers (20%) | 100% | 4.43 (0.53) | ||
| Prurigo (17.1%) | 83.4% | 3.67 (1.37) | ||
| Intensive Care | 28 | Therapy progress assessment (46.4%) | 69% | 4.0 (1.0) |
| Assessment of weaning potential (25%) | 71.4% | 4.67 (0.52) | ||
| Acute deterioration (14.2%) | 75% | 4.25 (0.96) | ||
| Dentist |
15 | Control (46%) | 100% | 4.22 (0.83) |
| Oral cavity assessment (20%) | 66.7% | 3.0 (0.0) | ||
| Dental assessment (13%) | 100% | 3.0 (0.0) | ||
| Emergency department |
3 | Surgical wounds (100%) | 66.6% | 4.0 (1.73) |
| General Practitioners | Missing** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



