
Submitted:
17 November 2025
Posted:
17 November 2025
You are already at the latest version
Abstract
Although the estimated TB incidence in Gabon has been declining, there have been challenges with treatment coverage, the HIV status documentation and the treatment outcomes. It is why the National TB Program (PNLT) conducted an innovative data review in Nkembo Health Treatment Center, Libreville, which manages more than 60% of Gabonese TB patients. Objective: since our hypothesis was that the Nkembo treatment center was struggling with the data mismanagement due to the workload, the objective was to assess data quality and identify aspects that need to be addressed to improve data quality, to inform more accurate estimates of disease burden and to improve patient management. Methods: the study used the data reconciliation method. This is a process that involves comparing and aligning data from multiple sources to ensure consistency, accuracy, and integrity. The primary purpose of data reconciliation is to identify and resolve discrepancies or differences between data sets and make them consistent. Using the "TB onion model", analysis identified data mismanagement as a key contributor to underreporting. A data review compared TB registry data with patient folders from January to August 2023. A third data source used was TB medicine registry. The study focused on notified TB cases, HIV status documentation, and TB treatment outcomes. Discrepancies were reconciled, and treatment outcomes re-evaluated. Results: the review significantly improved the programmatic performance concerning the targeted indicators. The number of TB cases increased by 22%, from 2156 to 2623. Documented HIV status increased by 141%, from 730 to 1762. And the successfully treated cases increased by 104%, from 824 to 1678. Discussion: This data reconciliation showed the usefulness of triangulation across data sources to improve completeness of data. Also, current reported data underestimate the number of reported cases, documentation of HIV status, and treatment success. Conclusion and Recommendations: Data reconciliation exercises should be continued in Nkembo and other high-burden facilities. Reviewing data recording procedures and extending data improvement initiatives are crucial for accurate reporting and effective TB management in Gabon.
Keywords:
Tuberculosis
; data quality
; data review
; Gabon
; Nkembo Health Treatment Center
; PNLT
1. Introduction
Tuberculosis (TB), a preventable infectious disease caused by M. tuberculosis, remains a major global health problem in Sub-Saharan Africa region (SSA). Prior to coronavirus disease 2019 (COVID-19) pandemic, TB has been the leading cause of death from a single infectious agent [1]. In addition, a more recent report from the World Health Organization (WHO), covering more than 99% of the world’s population, stipulated that TB ranked second among leading causes of death from a single infectious agent in the year 2022 [2]. Although some regions of the world have achieved substantial reduction of TB burden, the disease morbidity has increased in developing countries. According to the WHO, TB mortality was 1.6 million in 2022, whereas its prevalence was 10.6 million worldwide, with an increase of over 4% as compared with the previous year [3,4].
Because of the HIV pandemic, poverty, the movement of displaced people and the emergence of multi-drug-resistant strains, tuberculosis remains an enormous public health problem in developing countries. Moreover, WHO had identified in most developing countries, HIV pandemics, diabetes, malnutrition, alcoholism, smoking, contact with active TB, extreme poverty and homelessness as common risk factors in relation to TB. Tuberculosis has been identified as an important cause of morbidity and mortality in Gabon [5].
In the Republic of Gabon, TB remains a major public health challenge, with Libreville, the capital town, bearing the heaviest burden in the country. Despite international support by the Global Fund, the Gabonese National Tuberculosis Program (NTP) faces various challenges, including low TB detection and low treatment success rates. In 2022, TB detection rate was 42% and the treatment success rate was 57%. Moreover, the HIV positive rate among TB patients was 29%; however, according to the 2022 national TB program of Gabon (NTP) annual report, only one third of TB patients have undergone HIV testing [6].
The TB response is coordinated by the Minister of Health in Gabon through the National Program of TB management, called PNLT, which was established since 1997. This program is funded by the Government and the Global Fund who has been active since 2004 in the country.
Despite this support, the programme’s performance has been suboptimal on key programme indicators. While the incidence has been slowly declining from 542/100,000 in 2014 to 513/100000 habitants in 2022, the mortality rate has increased from 1974 to 4039 related tuberculosis deaths in the same period [6].
Considering the programmatic performance trends, the treatment coverage declined from 49% in 2019 to 42% in 2022. In the meantime, the treatment success rate declined from 67% in 2019 to 57% in 2022. The proportion of TB patients with a documented HIV status declined from 38% in 2020 to 24% in 2022. At the end of 2022, almost 60% of expected TB cases were not notified, half of confirmed patients were not successfully treated, and the HIV status of more than three quarters was not documented. [4]
According to the tuberculosis global report, the most important risk factors are HIV and malnutrition in Gabon. In fact, the HIV prevalence was 3.6% in general population, and it was estimated at 29% in TB patients. The chronic malnutrition is 17% among children under 5 in the country. [2]
To try understanding the situation, WHO supported the tuberculosis national program to perform periodic data reviews to assess data quality and adopt some data quality improvement strategies.
The country national report stated that 78% of TB patients in Gabon are diagnosed in Libreville and 94% of them are treated by the Nkembo health facility. These data helped to focus the data review on this health facility which has the high burden of patients.
Nkembo health facility is one of the hospital centers in Libreville specialized in tuberculosis management. The offered services are lab, case management, psychosocial support, the HIV lab contributes for the HIV testing of tuberculosis patients, and the administrative support.
The documents used to manage tuberculosis cases are patient folder, lab register, patient register, lab order, appointment card, monthly reports compiled in quarterly report. The patient folder is used to follow-up the confirmed tuberculosis patient. The lab register contents all suspect tuberculosis patients sent by the clinicians with the lab order. Some of the patients are sent by others health facilities clinicians outside Nkembo health facility. All the patients with folders are recorded in the tuberculosis register which is used to prepare the monthly report. At the facility, they have the monthly report for accurate monitoring. After three months, these reports are consolidated in a quarterly report.
The sub performance of tuberculosis management in the country was an indicator that it should be an issue on the reporting system in the big health facility caring more than 70% of patients in the country.
High-burden facilities often face challenges with data completeness, accuracy, and consistency. Facility-level data supports evidence-based planning, including budgeting, staffing, and supply chain management. Regular analysis of core indicators (e.g., case notifications, treatment success rates, HIV co-infection rates) strengthens surveillance. WHO’s standards and benchmarks guide countries in evaluating and improving their TB surveillance systems [7]. This module provides guidance on the analysis and use of routine tuberculosis surveillance data collected at the facility level. The module reviews core facility indicators and analysis, provides suggestions for questions on data quality as well as considerations and limitations for using the data and analysis. Training health workers in data analysis and interpretation is crucial for sustaining improvements.
Objectives
- Perform a data quality reconciliation exercise in the Nkembo health facility in 2023
- Identify the key issues related to the data quality with direct impact on the reporting process
- Formulate the recommendations to improve data recording and reporting in this health facility
2. Methodology
For this review, we used the TB onion change model as described below. This model helps to understand why many tuberculosis cases are not reported at the national level.
TB Onion Model Change of Theory
Figure 1.
The "onion" model: a framework for assessing the fraction of TB cases accounted for in TB notification data, and how this fraction can be increased.
Figure 1.
The "onion" model: a framework for assessing the fraction of TB cases accounted for in TB notification data, and how this fraction can be increased.
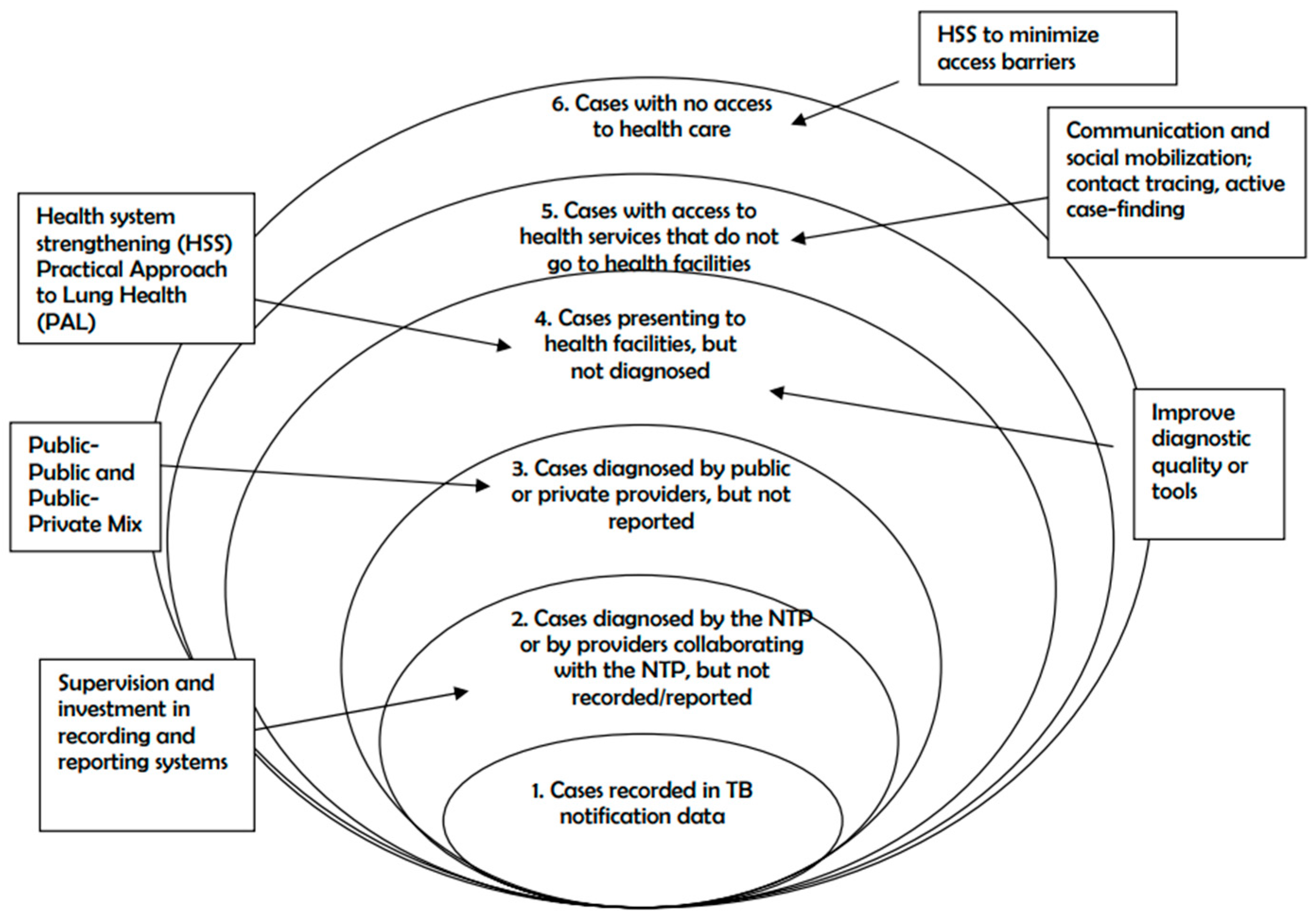
The model shows different situations that occur considering all tuberculosis expected cases.
- There are who don’t have access to the health care. This occurs when the health system minimizes access barriers
- Some others have access, but they don’t go to the health facilities. It is due to the lack of communication and social mobilization
- Some cases arrive to the health facilities, but they are not diagnosed. The services should improve diagnostic quality and tools
- Some others are diagnosed by public or private providers, but they are not reported
- Few only are diagnosed in the public or private providers and are correctly reported
In the current study, the assessment focused on the management of data at the health facility due to the workload. Beyond the underreporting notified cases, the review seized this opportunity to check the HIV status documentation and the treatment result.
Hypothesis
Since the high-burden facilities often face challenges with data completeness, accuracy, and consistency, this was the beacon to formulate the following hypothesis. The individual Informations which are in the patient folders are not fully recorded in the tuberculosis hospital registry. In the same way, all the registry Informations are not recorded in the monthly reports. This last is used to elaborate the hospital report. This situation is contributing to underreporting tuberculosis cases in Nkembo health facility.
Sampling
It was a progressive and an exhaustive sampling covering the period from January until August 2023 when I left Gabon for another appointment. The sampling unit was constituted by the recorded patient. This was also the study unit as well.
Data Collection
It was a cross-sectional study consisting to a desk review of the tuberculosis data recorded in the patient’s registry of the health facility compared with the patient folders.
The variables collected are the number of notified tuberculosis cases, number of tuberculosis cases with known HIV status for the 2023 cohort patients and the number of tuberculosis patients successfully treated at the end-treatment evaluation for the 2022 cohort patients. This last indicator was compared to the other issues that are the number of lost to follow-up patients, the number of deaths, the number of failed patients, and the number of non-evaluated patients.
Data Sources
The sources of data were the monthly reports from the Nkembo Health treatment center, the patient’s registry, and the patient’s folders. The first step was to collect all the patient’s folders in the service archives for the targeted period. Then, we counted again these indicators using folder by folder.
The reconciliation was done in two phases. Firstly, the missing data were reported in the patient’s registry. Secondly the new total number was reported in the report.
In the template, we took the data from the previous report to fill the “before the review” column. In general, these data were the same in the patient’s registry. Then, we filled out the “after review” column” using the reconciled data. The difference between the two columns led to measure the change and the contribution of the data reconciliation exercise.
Data Reconciliation
After comparing data from the quarterly report sent to the National Programme with the data recorded in the registry, some discrepancies were found. And after this step, the individual folders were used to fill out the missing Informations in the tb registry if any. At the end, the data were reconciled between these different sources and treatment outcomes re-evaluated. Data trends before and after the review were analyzed for the variables summarized in Table 1 and Table 2.
Data Analysis
Two templates were used for this review. The first one related to the notified tuberculosis cases and the second one for treatment outcome.
This template helps to compare the notified TB cases and those with known HIV status before and after data review.
This template was used to compare the TB cases successfully treated before and after data review. In the meantime, it helps to analyze the non-favorable issues that could explain the gap if any.
Study Team
The review team was composed by 15 people working for four days. The work was performed after work to avoid service provision disturbance.
They were five from the national program in charge of monitoring and evaluation, two advisors from the regional level, six nurses and data clerks from the Nkembo health treatment center and one from WHO as technical support.
Ethical Consideration
All data used in this study are from TB monitoring and surveillance in Gabon; they are anonymous. Thus, informed consent was not required. Study data consisted in medical records from Nkembo Tuberculosis treatment center located in Libreville.
3. Results
The variables compared include the number of notified tuberculosis cases, number of notified TB cases with known HIV status and the number of successfully treated patients. These were compared for each month, before and after the data reconciliation.
Notified Tuberculosis Cases
Starting by the notified tuberculosis cases, the graph below is presenting the trend from January to August 2023.
Figure 2.
TB cases trend per month before and after the data review, Nkembo Health Treatment Center, PNLT Gabon 2023.
Figure 2.
TB cases trend per month before and after the data review, Nkembo Health Treatment Center, PNLT Gabon 2023.
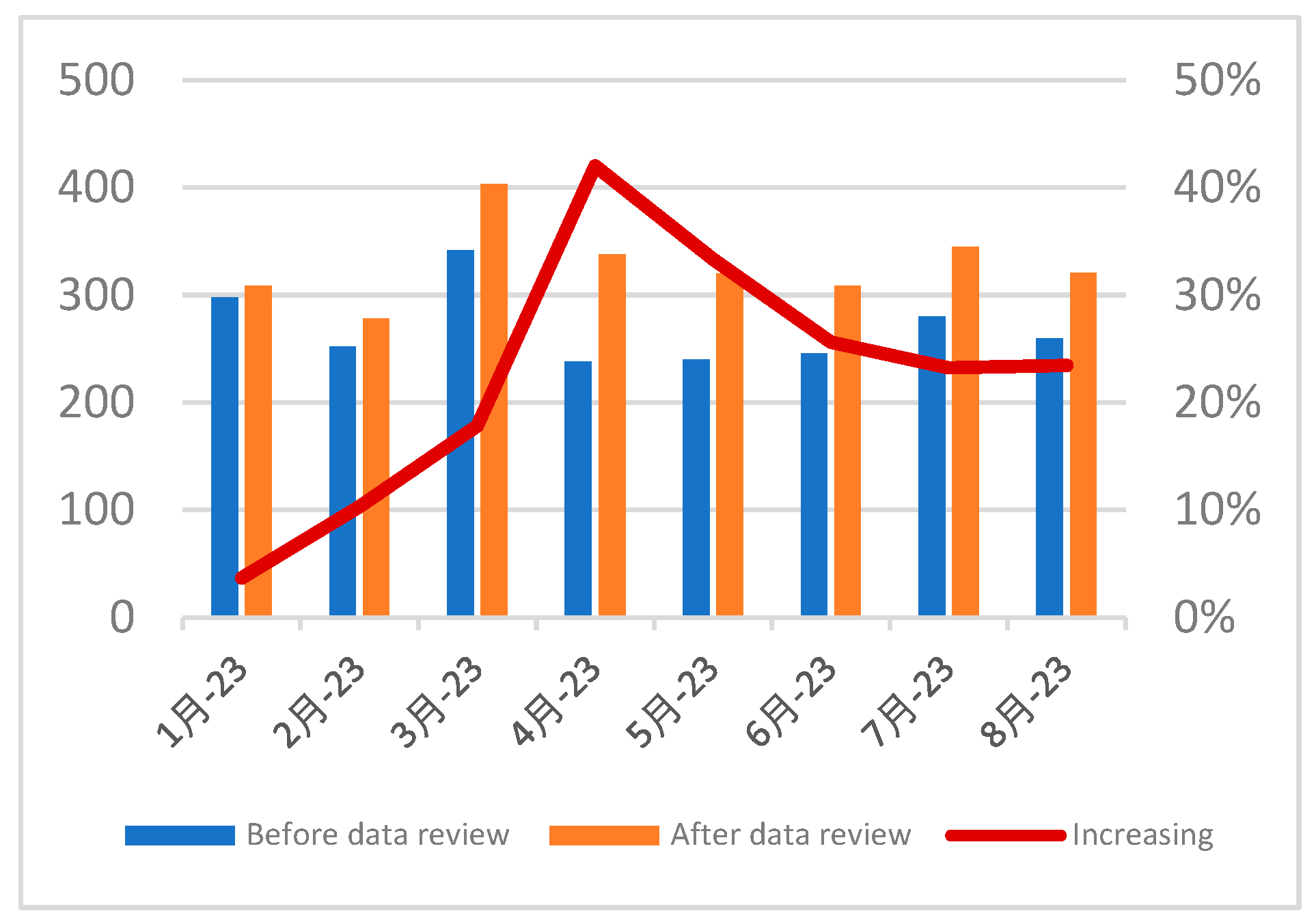
The figure number 2 shows that the notified tuberculosis cases are consistently more after the reconciliation than before for all the months.
For the period January to August 2023, there were 2623 notified TB cases after the review, compared to 2156 recorded before, which represents an increase of 467 cases or 22%.
Notified Tuberculosis Cases with Known HIV Status
Proceeding with the notified tuberculosis cases with known HIV status, the graph below is presenting the trend from January to August 2023.
Figure 3.
Trend of notified tuberculosis cases with known HIV status per month before and after the data review, Nkembo Health Treatment Center, PNLT Gabon 2023.
Figure 3.
Trend of notified tuberculosis cases with known HIV status per month before and after the data review, Nkembo Health Treatment Center, PNLT Gabon 2023.
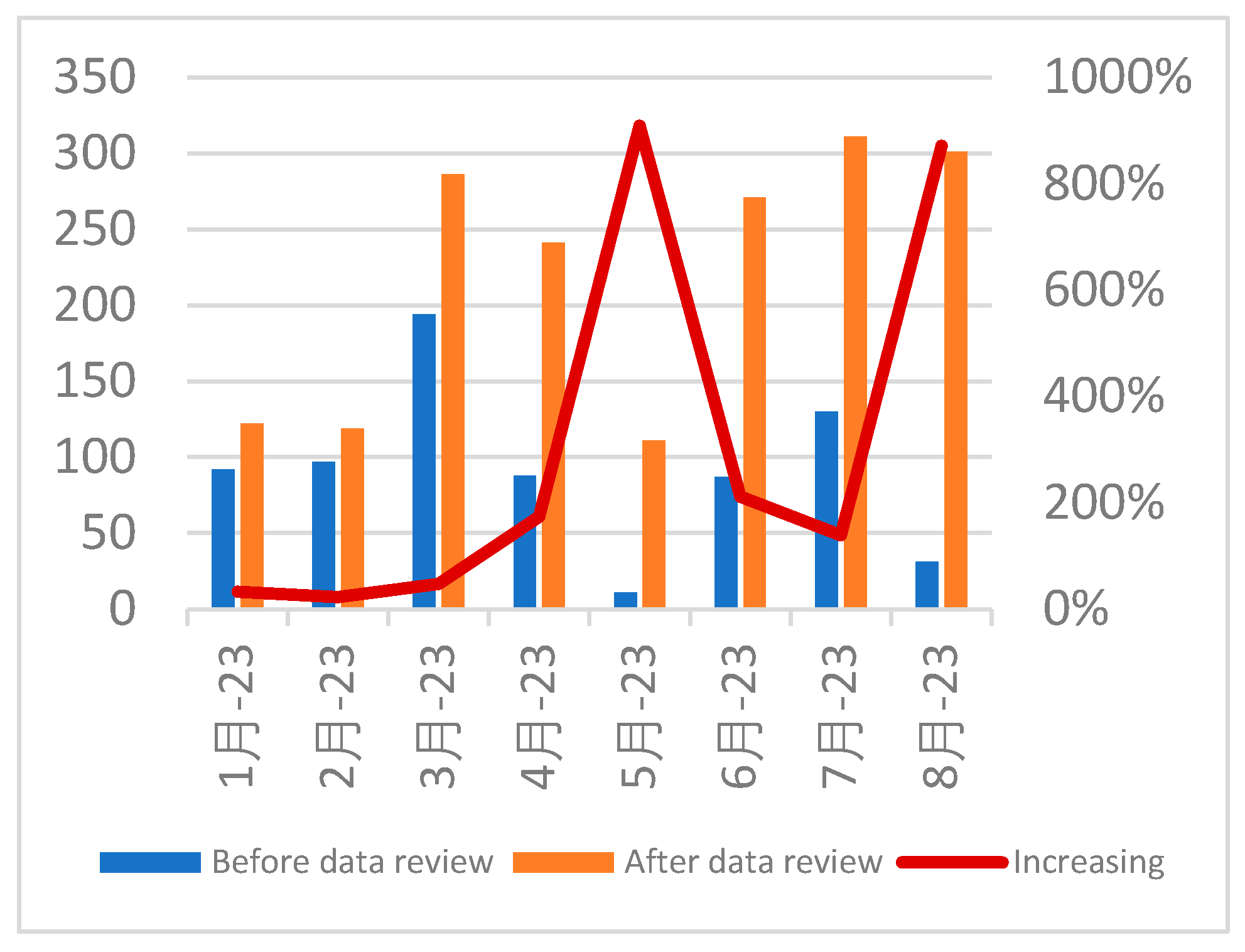
The figure number 3 shows that the proportion of the notified tuberculosis cases with known HIV status was consistently more after the reconciliation than before, for all the months.
For the period January to August 2023, there were 1762 TB cases with known HIV status after the reconciliation, compared to 730 recorded before, which represents an increase of 1032 cases, or 141%.
Trend of Successfully TB Treated Cases
Ending by the successfully treated cases, the graph below is presenting the trend for the patient’s cohort from January to August 2022. They were evaluated one year later in 2023.
Figure 4.
Trend of successfully treated cases per month before and after the data review, Nkembo Health Treatment Center, PNLT Gabon 2022.
Figure 4.
Trend of successfully treated cases per month before and after the data review, Nkembo Health Treatment Center, PNLT Gabon 2022.
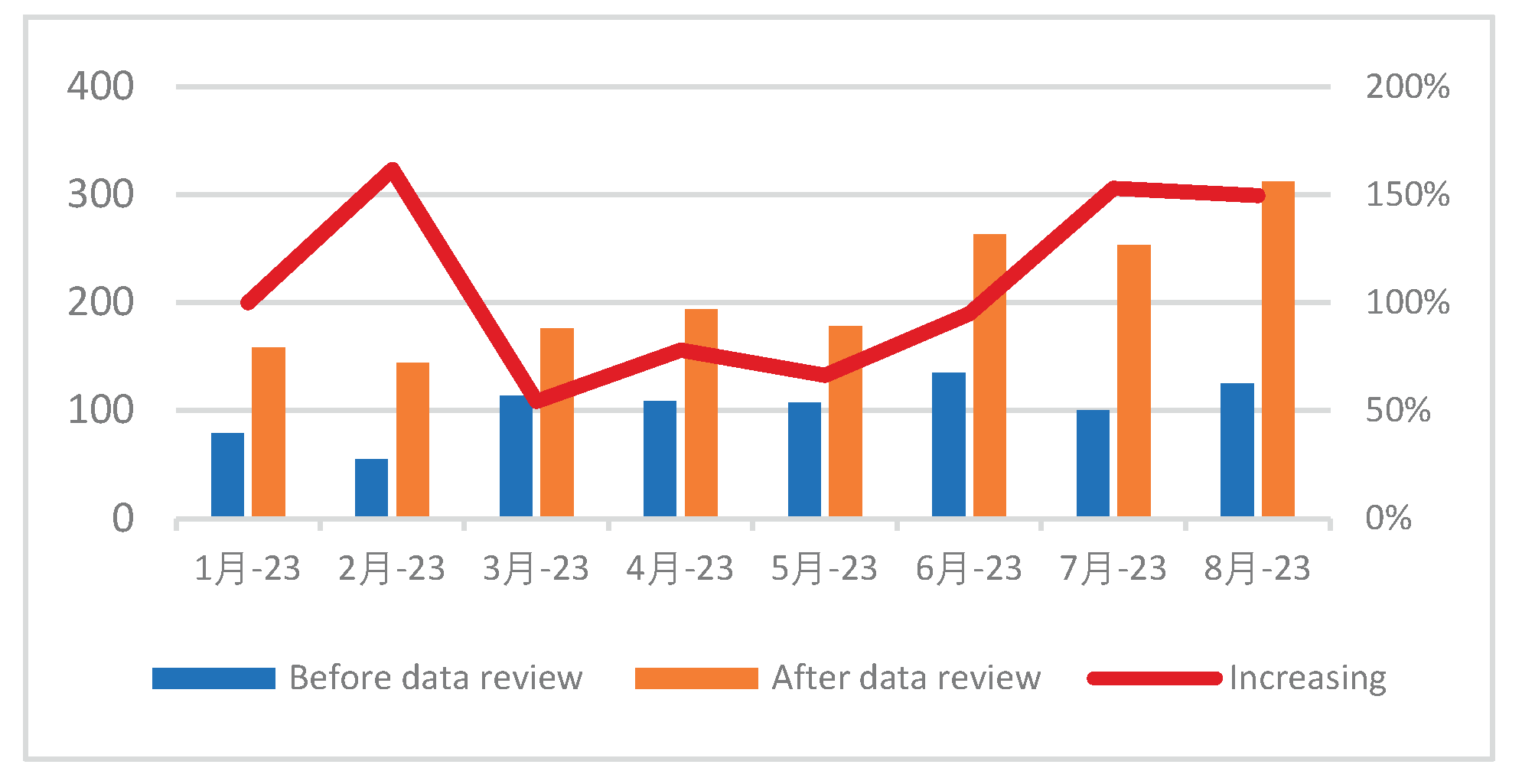
The figure number 4 shows that the TB treatment success number is consistently above after the data reconciliation than before for all the months.
At the end of August 2023, the study finds 1678 TB cases successfully treated after the review, against 824 recorded before, which means 854 supplementary cases and 104% of increasing.
4. Discussions
This section will present first some insights on the onion model and discuss the findings.
Onion Model
For low-income countries, where the numbers of TB cases reported are considered unreliable due to poor access to health services and/or incomplete case notification, until 2015 three main methods were used by the WHO to estimate TB incidence: 1) the annual risk of infection, 2) the Onion Model, and 3) prevalence surveys.
In this review, we considered the onion model which help not only to estimate the cases number, but most importantly to identify accurate strategies to reach those who are missing. From all the tuberculosis cases, the onion model is showing that there are notified cases, cases diagnosed but not notified and undiagnosed cases.
Starting with the number of cases notified by the NTP (the core), each successive layer of the onion represents the percentage of missed cases, i.e., cases diagnosed within the NTP system but not declared, cases diagnosed outside the NTP system and not declared, cases who accessed health services but for whom a diagnosis was lacking, cases with access to health services who did not use them and cases with no access to health services (Figure 1). The various layers are determined to calculate the proportion of incident TB cases missing from TB notification data and to prioritize the programmatic or health system interventions that might be required to address these missed opportunities for TB notification and/or diagnosis. [8]
Nigeria NTP used the onion model in the STOM Project in 2023. STOM means Spot to Tent Onion Model [9]. Through a grant from the USAID-funded Tuberculosis Implementation Framework Agreement (TIFA) project, implemented by JSI Research and Training Institute, KNCV Nigeria implements the Spot to Tent Onion Model of Contact Investigation (STOM) project which employs a systematic approach of TB contact investigation.
The use of the onion model approach was able to increase the contact investigation coverage from 67% to 80%, to boost the community case finding from 8% to 20% and to scale up TB Preventive Therapy (TPT) from 2% to 50% of eligible contacts.
The Current Study Findings
These findings suggest that substantial underreporting occurred prior the data reconciliation. This exercise will significantly improve the national Tb Programme report of 2023 with the Nkembo health treatment center data.
This study demonstrates the need for routine data quality assessments, capacity building and supportive supervision in high-burden settings. It also highlights potential systemic issues contributing to underreporting.
Coming to the onion model, the notified cases represented 42% in 2022, the review showed that 22% can be caught up with the data reconciliation exercise. Considering both, the Gabon tuberculosis program can be able to reach 66% of estimated cases. Where should be reached the 44% still missing?
Beyond the tuberculosis cases diagnosed but not notified by the public sector, there are also many from private sectors and from the NTP or collaborative providers. This situation is critical for this country where the health system is high centralized with many private facilities closer to the communities. It is the case in many countries.
Nigeria conducted an epidemiological review on 9–20 January 2023, its fourth since 2014. The time trend in TB case notifications since 2014 has been fairly stable, at around 50 cases per 100 000 population. Findings from the 2020 epidemiological review suggested that the most important factor for this low level of case notification and the corresponding low levels of treatment coverage (24% in 2018) was the underdiagnosis of people with TB, which in turn was due to issues with the network of primary health care (PHC) facilities. The underdiagnosis was compounded by the underreporting of people with TB, primarily from the private sector and particularly in urban settings.
Among the actions taken, there was the engagement of private providers for diagnosis, treatment and reporting. As results, case notifications increased from 103,018 in 2018 to 285,561 in 2022. And the treatment success rate reached 91%, and 97% of cases had documented HIV status. [10]
The report revealed also other factors contributing to increase the undiagnosed tuberculosis cases:
- The strong stigma attached to tuberculosis patients both among healthcare staff and the population
- The lack of investigation of contact subjects around index cases
- Awareness activities are almost non-existent in healthcare facilities, as well as through the media.
- Missed opportunities for diagnosing tuberculosis cases among people who consult at the hospital without this disease being suspected or diagnosed.
All those factors are limiting the access to the health care for tuberculosis patients. Many countries are in the same situations. It is the case for Gabon.
Data Recvnciliation
The data reconciliation exercise in the routine surveillance helps to fix data discrepancies between different sources of data. It improves the completeness, accuracy, and timeliness of tuberculosis data. It enhances capacity of health workers to manage and use data. It is fostering a better program planning, monitoring, and patient care. The two examples below are showing some benefits.
The Aurum Institute conducted a baseline data reconciliation of drug-resistant TB (DR-TB) records, followed by a data quality improvement process. After the intervention, data completeness for key variables reached 90–100%, and concordance between clinical folders and the electronic database was 100%. This high-quality data supported regulatory submissions and improved patient management. [11]
Kenya’s National TB Program implemented data reconciliation in several counties to assess routine TB service data. The exercise identified gaps in data completeness, accuracy, and timeliness. The findings informed targeted supervision, on-the-job training, and system improvements, resulting in more reliable data for program planning and monitoring. [12]
Strengths and Limitations of the Study
The current exercise is strengthening the need to integrate the tuberculosis data reconciliation in the routine of surveillance, especially in the high burden health facilities. It is known that high-burden facilities often face challenges with data completeness, accuracy, and consistency.
Compared to before review situation, the reconciliation exercise was able to increase the notified cases up to 22%. Similarly, the tuberculosis cases with documented HIV status rose to 141%, and the successfully treated tuberculosis cases lifted to 104%.
The current study is limited by the fact that some individual folders were not fully completed, with some missing information. If this exercise is regularly conducted, the health workers can have the possibility to fill out some missing data.
Suggested directions for future research are delve deeper into the public health implications of these findings. This involves analysis from results quality, the turn-around of patients, the workload of health providers, the quality of archives procedure. All of these can improve the data surveillance of tuberculosis patients in this kind of health facilities.
5. Conclusion and Next Steps
The study shows that the data reconciliation can consistently improve the tuberculosis programmatic data in the health facilities, especially those with a high workload of TB patients to monitor.
Nkembo health treatment center will be able to change the figure of the country at the end of the year in term of TB national report.
This exercise should be sustained in Nkembo and extended to other high-burden facilities to ensure ongoing data accuracy. By implementing these recommendations and utilizing a data-driven approach, Gabon can effectively tackle the TB burden and improve patient outcomes.
The progress to reach the 2030 sustainable development goals can be slowed down if the data quality and data improvement are not considered in the program management.
Data use is part of the precision public health for Africa (PPH4Africa) which is a strategic initiative to end diseases in the Region.
Recommendations for Future Research
Given the findings of the current review and the discussions done, it is recommendable to extend the data reconciliation exercise starting by the health facilities with a high tuberculosis patient burden.
Another point is to explore the contribution of private sector. Also, operational research for tuberculosis screening in the big health facilities will be informative.
In the meantime, the Programme must strengthen sensitization activities, and civil society organizations involvement to fight against stigma in the communities and in the health facilities.
Author Contributions
Conceptualization: Casimir Manzengo, Stredice Manguinga, Ghislaine Nkone; Methodology: Casimir Manzengo, Fleur Lignenguet; Software: Fleur Lignenguet; Validation: Farai Mavungha, Nlandu Roger Ngatu; Formal analysis : Casimir Manzengo, Fleur Lignenguet; Investigation: Casimir Manzengo; Resources: WHO Gabon; Data curation: Stredice Manguinga, Fleur Lignenguet; Writing: Casimir Manzengo, Farai Mavungha, Nlandu Roger Ngatu; Original draft preparation: Casimir Manzengo, Stredice Manguinga, Ghislaine Nkone; Writing—review and editing: Farai Mavungha; Visualization: Casimir Manzengo, Ghislaine Nkone; Supervision: Casimir Manzengo, Ghislaine Nkone; Project administration: Casimir Manzengo. Funding acquisition: Casimir Manzengo
Funding
This research received no external funding
Institutional Review Board Statement
Not applicable” for studies not involving humans or animals
Informed Consent Statement
Not applicable
Data Availability Statement
Data are available in the National Tuberculosis Program, M&E office
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lange C, Dheda K, Chesov D, Mandalakas AM, Udwadia Z, Horsburgh Jr CR. Management of drug-resistant tuberculosis. The Lancet 2019; 394(10202): 953-966. [CrossRef] [PubMed]
- The World Health Organization. Global tuberculosis report 2023. Available from: Global Tuberculosis Report 2023 (who.int).
- Park PG, Fatima M, An T, Moon YE, Woo SK, Youn H et al. Current development of therapeutic vaccines for the treatment of chronic infectious diseases. Clin Exp Vaccine Res. 2024; 13(1): 21-27. [PubMed]
- National tuberculosis program (PNLT). Rapport annuel 2022 (report in French, unpublished).
- J.B.P.A. Agbo Abdul, B.R. Adegbite, M.E.D. Ndanga, J.R. Edoa, R.C. Mevyann, G.R.A.I. Mfoumbi, T. Jean de Dieu, J. Mahoumbou, C.M. Biyogho, S. Jeyaraj, S. Niemann, B. Lell, P.G. Kremsner, A.S. Alabi, A.A. Adegnika, M.P. Grobusch. Resistance patterns among drug-resistant tuberculosis patients and trends-over-time analysis of national surveillance data in Gabon, Central Africa. Infection 2023, 51, 697–704.
- National tuberculosis program (PNLT) Report. Review of the national tuberculosis program (PNLT), 2022 (report in French, unpublished).
- WHO, Guidance on conducting reviews of tuberculosis programmes, 2024.
- WHO, Improving estimation of TB disease burden via systematic assessment of surveillance data, 2021.
- USAID, Spot to Tent Onion Model of Contact Investigation (STOM), Project Final Report, Nigeria 2023.
- WHO, Notable findings from two recent TB epidemiological reviews in the WHO African Region, Global Tuberculosis report, 2023.
- Autorum Institute, DRTB Data Management Support project - Data Quality, The Aurum Institute - The Aurum Institute, 2021.
- National Tuberculosis (TB) Program, Data Quality Assessment: Informed decisions for better management, Data Quality Assessment: Informed decisions for better management – NLTP, 2022.

Table 1.
TB cases notification for the period before and after the data review.
| Before the review | After reconciliation | After the review | |||
| Month 2023 | % | Month-2023 | % | ||
| Number of notified TB cases (cohort 2023) | |||||
| Number of TB cases with known HIV status | |||||
Table 2.
Treatment outcome for the period before and after the data reconciliation (2022 cohort).
| Before the review | After reconciliation | After the review | |||
| Indicator | Month-2022 | % | Month-2022 | % | |
| Number of notified TB cases (cohort 2022) | |||||
| Number of cured patients | |||||
| Number of treatments completed patients | |||||
| Number of lost to follow-up | |||||
| Number of died TB patients | |||||
| Number of failed TB patients | |||||
| Number of non-evaluated patients | |||||
| Successfully treated | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



