Submitted:
11 November 2025
Posted:
17 November 2025
You are already at the latest version
Abstract
This study examines how religious and spiritual identities relate to depression and anxiety at baseline and longitudinally. Using data from the Family Foundations of Youth Development Project, which sampled parent-child dyads from the Western United States, we investigated how mental health relates to the conjunction of spirituality and religiosity (S/R), the lack of either, or one separate from the other. At baseline, children identifying as “Spiritual but not Religious” (SBNR) reported the highest levels of anxiety and depression, whereas children who identified as “Religious and Spiritual” (RAS) exhibited the lowest levels of depression. The difference between RAS identity and the SBNR identity was significant across all baseline scales, with SBNR individuals demonstrating greater pathology. Among parents, the "religious but not spiritual RBNS group” was more depressed than the RAS group, and both RBNS and SBNR parents were more anxious than the “not religious, nor spiritual” (NRNS) parents. Longitudinally, SBNR children uniquely showed significant decreases in their depression levels, and no increases in their anxiety levels, likely reflecting a ceiling effect given their initially high symptoms. Regarding adults, all groups except RBNS decreased in depressive symptoms over time. This study highlights the nuanced relationship between psychological well-being and S/R. It offers possible interpretations, intending to alleviate suffering and encourage flourishing by identifying risk and protective factors.
Keywords:
depression
; anxiety
; mental health
; religion
; religiosity
; spiritual
; spirituality
; latter-day saint
; parent
; child
; adolescent
1. Introduction
Current narratives in Western modern psychology (especially pop psychology) regarding religiosity and spirituality appear ambivalent and, at times, contradictory. On the one hand, several media outlets have reported on the social media saturation of messages and personal anecdotes of individuals deconstructing their faith (Harber 2024; Koukl 2022; Wells 2025), which does appear to be happening at rising rates (Burge 2021). Of those disconnecting from religion, many cite the dangers of religious groupthink, religious shame, or religious extremism as detriments to mental health and reasons for leaving religion (Smith 2025). Simultaneously, research regarding religion and spirituality has found numerous benefits of religion, including the benefits of meaning-making, positive emotions derived from spirituality, and spiritual practices such as mindfulness, meditation, etc. (Koenig et al. 2023).
It also appears increasingly common for individuals to consider themselves “spiritual” absent any religious affiliation, with 22% of U.S. adults regarding themselves as “spiritual but not religious”(Pew Research Center 2023). As King has noted: “There is… an increasing trend in the West for religion to be seen as negative while spirituality acquires increasing social approval. By being ‘spiritual,’ one is separating oneself from religion with its negative associations of power, dependence, and clergy, while holding on to something that is seen as good” (King 2014, 114). Given the societal shifting of how individuals connect with religion and spirituality, as well as the, on average, mental health benefits of both, a question that emerges is how this shift relates to mental health for adolescents and young adults. This is a crucial question given the rapidly increasing rates of mental health disorders. According to the Center for Disease Control, depression rates in adolescents and adults over the age of 12 increased from 8.2 to 13.1% from 2013-2014 to August 2021 to August 2023 (Brody and Hughes 2025). In 2023, 20.3% of adolescents ages 12-17 had a current diagnosis of a mental or behavioral health condition; anxiety being the most common (16.1%). These rates also increased 35% (from 15.0% to 20.3%) between 2016 and 2023, anxiety rising 61% (Sappenfield et al., n.d.).
The purpose of the current study is to longitudinally examine how those who belong to various spiritual and religious categories compare in their well-being (depression and anxiety). We compare individuals who identify as spiritual but not religious (SBNR), religious and spiritual (RAS), religious but not spiritual (RBNS), and neither spiritual nor religious (NSNR). The aim of doing so is to better understand possible contemporary implications of shifting connections to both religion and spirituality.
Mental Health and Religion/Spirituality
In the current study, we narrowed the scope of “mental health” to anxiety and depression: Generalized Anxiety Disorder (GAD) and Major Depressive Disorder (MDD). The relationship between these and mental health has been substantially studied, providing a large literature base for the current study. For the purposes of this review, we use Rosmarin and Koenig’s (2020) definition of spirituality as: “any way of relating to that which is perceived to be sacred” (xix), or “a set of individual beliefs, practices, and ways of being that are intended to assist in attaining union with, or experience of, the divine or transcendent”(Koenig et al. 2023, 11). Religiosity is defined as: “institutionalized or culture-bound ways of relating to that which is perceived to be sacred,” or “the phenomenon wherein a system of beliefs and practices unite adherents into a community with a shared vision for attaining union with, or the experience of, the divine or transcendent” (Koenig et al. 2023, 10; Rosmarin and Koenig 2020, xix).This is commonly connected with a religious affiliation and institutionalized religious practices such as church attendance It also includes private religious behaviors (Koenig et al. 2023; Rosmarin and Koenig 2020). The conversation on the relationship between R/S and mental health remains highly ambiguous as the results of the studies offer various and sometimes contradictory results. Additionally, a vast majority of the research examines R/S as a whole, rather than differentiating religiosity and spirituality as separate constructs, something which will be addressed in our current study.
Depression
Rates of Major Depressive Disorder (MDD), which is characterized by the existence of at least one 2-week depressive episode demonstrating five or more depressive symptoms (American Psychiatric Association 2022), are estimated to have a 12-month prevalence of 10.1% and a lifetime prevalence of 20.6% (Hasin et al. 2018). Recently, adolescents appear to be hit especially hard by this mental health crisis, with rates growing amongst youth aged 12-17 (Weinberger et al. 2018; Wilson and Dumornay 2022). The depression prevalence rates for adolescents aged 12-19 is 19.2% (Brody and Hughes 2025). As of 2021, according to the National Institute of Mental Health (NIMH), it was estimated that 14.5 million adults in the US had a major depressive episode within the year (National Institute of Mental Health 2022). Considering this mental health epidemic, researchers, clinicians, and family and friends alike have devoted many resources to discovering the underlying causes, preventative measures, and treatment options for depressive disorders. Given that religion and spirituality are often integral parts of an individual’s mental, emotional, and social worlds, the interplay of religiosity/spirituality and depression has increasingly become a focus of study.
Depression and R/S
Cross-sectional and Longitudinal Research. Several meta-analyses and systematic reviews on the relationship between depression and R/S were examined. One systematic review found that, of the most meticulous studies, 67% found a negative association between S/R and depression, with only 7% of the studies finding a positive association (Bonelli et al. 2012). When exclusively analyzing high-quality studies, of 148 publications, 68% found that higher religious involvement was associated with less depression (Koenig et al. 2012; Rosmarin and Koenig 2020). In sum, with few exceptions, higher religiosity and spirituality seem to be related to lower levels of depression. A more recent overview, from the third edition of the Handbook of Religion and Health (2023), summarizes research from the first two editions, finding that 61% of the 444 studies on the relationship between religion, spirituality, and depression reported less depression among those who were more religious, 6% found more depression, and 33% found no association. Although nearly 80% of these studies were cross-sectional, longitudinal studies yield similar results (Koenig et al. 2023). For example, a rigorous, longitudinal study that employed a sample of 48,984 women found that after up to 12 years of follow-up, consistent attendance at religious services was associated with a 30% decrease in depressive incidents (Li et al. 2016).
Randomized Controlled Trials/Clinical Integration. In addition to cross-sectional and longitudinal studies, randomized controlled trials have also been used to examine the connection between depression and R/S. For example, in a study performed by Razali and colleagues, 100 Muslim patients diagnosed with MDD and 103 diagnosed with GAD at a university clinic were assigned to either a control group receiving antidepressants and supportive psychotherapy, or a group that supplemented this therapy with additional religious-sociocultural psychotherapy: Cognitive behavioral therapy (CBT) based on the Holy Qur’an and Hadith. After 11 total sessions and 4 measurements of depression levels throughout, results found no difference between the two groups at the baseline, yet significant differences at 4 weeks and 12 weeks, but no significant difference at 26 weeks. Thus, although those who received the religious-sociocultural psychotherapy improved faster, both groups improved equally (Razali et al. 1998).
Similarly, in a randomized controlled trial by Ford and Garzon (2017), 78 Christian college students were assigned to either Christian-accommodative Mindfulness Training (CMT) or conventional mindfulness training (MT). They participated in 3 weeks of treatment consisting of psychoeducational group sessions and daily application of the learned mindfulness techniques. After the treatment, the Depression, Anxiety, and Stress scale (DASS) revealed significant differences, both within and between groups, with the CMT group having lower DASS scores. The study found that subjects were more compliant with CMT, which supports the idea that individuals prefer therapy that is religiously aligned with their own religious views (Ford and Garzon 2017). Representing the benefits of a third religion incorporated into treatment, Foley and colleagues (2010) studied 115 randomly selected patients in Australia. The patients were assigned to either Buddhist-based MBCT (Mindfulness-Based Cognitive Therapy) or a wait-listed control group. The experimental group participated in 8 weekly two-hour sessions focused on mindfulness, meditated for one hour per day, and attended an additional full-day treatment session. Their depressive symptoms were assessed blindly pre-treatment and post-treatment; the intervention group was also assessed 3 months later. Results found no significant differences between the groups at the baseline measurement, and a post-treatment significant decrease in depressive symptoms for the intervention group as compared to the control group. The benefits of the treatment remained in the 3-month post-treatment follow-up (Foley et al. 2010; Koenig et al. 2023, 84). These clinical trials all support the conclusion that religious and spiritually integrated psychotherapy is at least as, if not more effective, than control therapies such as CBT and MT.
Anxiety
Research findings on the relationship between R/S and anxiety are somewhat more nuanced and qualified than for the relationship between R/S and depression. Here, “anxiety” will refer to both the emotion broadly (an intense prevalence of fear or worry over a future event) as well as the clinical diagnosis of generalized anxiety disorder (GAD), which constitutes excessive anxiety with multiple focuses for at least a 6-month period (American Psychiatric Association 2022). For GAD, “The intensity, duration, or frequency of the anxiety and worry is out of proportion to the actual likelihood or impact of the anticipated event. The individual finds it difficult to control the worry and to keep worrisome thoughts from interfering with attention to tasks at hand (American Psychiatric Association 2022, 251).” As there are many other anxiety disorders comorbid with GAD, aspects of these disorders, such as panic attacks or social anxiety, may also be present when discussing “anxiety.” According to the National Institute for Mental Health (NIMH), it is estimated that 31.3% of adults living in the United States experience an anxiety disorder in their lifetime, with 5.7% experiencing GAD (American Psychiatric Association 2022; National Institute of Mental Health 2021). Rates of both anxiety and depression are also increasing, with 15.6% of adults experiencing anxiety symptoms in 2019 and 18.2% in 2022 (Terlizzi and Zablotsky 2024).
Providing an overall summary of the relationship between R/S and anxiety, the handbook of Spirituality, Religion, and Mental Health states, “Generally speaking, positive cognitive or emotional aspects of S/R life are consistently associated with less anxiety, whereas negative internal facets of S/R are associated with more anxiety, and effect sizes [are] moderate to large”(Rosmarin and Koenig 2020, 42). Frequently repeated in the literature is the idea that “S/R afflicts the comforted and comforts the afflicted” meaning that S/R can be both a comfort or a stressor depending on the individual’s affect, experiences, and personality (Rosmarin and Koenig 2020, 44). Thus, findings on the relationship between anxiety and R/S are more mixed than findings on the relationship between depression and R/S. The 2023 edition of The Handbook of Religion and Health summarizes the previous editions, stating that 299 quantitative studies were identified that examined the relationship between religiosity and anxiety. Within these studies, 49% discovered less anxiety among the more religious (an inverse relationship), 11% reported the opposite, and 40% reported no association or complex results (Koenig et al. 2023, 131).
Anxiety and R/S
Cross-sectional/Longitudinal Research. Several studies find spirituality and religiosity related to less anxiety. For example, according to Ellison et al. (2009), Jansen et al. (2010), Koenig et al. (1993), Ng et al. (2017), and Schieman et al. (2006), religious event attendances have been connected to fewer anxiety symptoms. Furthermore, Ellison et al.’s (2009) US-based study reported that church attendance was associated with slightly less anxiety. This was also found in Chen et al.’s (2020) analysis of the data of 9,862 young adults across 3 years and 68,376 individuals across 12 years, which found that at least weekly religious service attendance predicted slightly lower anxiety levels across time (Chen et al. 2020). Besides religious service attendance, R/S practices also yielded significant results. For example, multiple studies have found negative associations between anxiety and prayer (Ai et al. 2005; 2007; Dehghani et al. 2012; Rosmarin et al. 2009).
However, other studies found religion related to greater anxiety. For example, Peterman et al.’s (2014) longitudinal work found that those attending religious services and belonging to religious youth groups had slightly but significantly greater anxiety over a three to four year period. Additionally, other studies have found prayer associated with greater anxiety (Byrd and Boe 2001; Sternthal et al. 2010).
Randomized Controlled Trials/Clinical Integration. Due to the complex and sometimes contradictory results of cross-sectional and longitudinal studies, it is also important to look at randomized controlled trials (RCTs) that have provided additional evidence on the effectiveness (or lack thereof) of religiously and spiritually integrated clinical interventions on alleviating anxiety. According to Captari et al. (2018), a meta-analysis of 97 studies using a total of 7,181 patients found that psychotherapy, which was adapted to S/R beliefs and values, was as effective at reducing psychological distress when compared with untreated controls or conventional treatments. Similarly, Koszycki et al.’s (2010) study found that spiritually integrated treatment was just as effective as CBT at reducing the somatic and psychic symptoms of GAD. In Rosmarin et al.’s (2010) study of 125 Jewish individuals, it was found that a spiritually integrated treatment was effective at reducing anxiety symptoms, and Paukert et al.’s (2009) study found that patients with GAD who received spiritually integrated treatment were found to have a reduction of symptoms at a faster rate as compared with those who were administered traditional treatment (CBT). Furthermore, Wachholtz and Pargament (2005, 2008) found that in contrast with patients who practiced secular meditation or relaxation exercises, individuals who employed spiritual meditation, such as repeating the phrase “God is good” daily for a 30-day period, reported less anxiety after the experiment (Wachholtz and Pargament 2008, 351, 358). A randomized controlled trial by Boelens et al. (2009, 2012) found that six 1-hour prayer sessions weekly were associated with reduced anxiety. This reduction persisted both 1 month and 1 year following the final prayer session and was not found in the control condition. Especially as compared to cross-sectional studies regarding anxiety, research on clinical interventions utilizing R/S seems to be both empirical and optimistic.
Additionally, Nikfarjam et al. (2018) randomly assigned 72 patients with anxiety to either a religious intervention or a usual care control group. The usual care control group received drug treatment, including benzodiazepines and selective serotonin reuptake inhibitors (SSRIs). The intervention group received the usual drug treatment with the addition of the group religious intervention. The religious intervention incorporated Qadar, as well as the Qur’an and religious texts. Results suggested that after the 2 months of intervention, the religiously-integrated treatment group showed greater reduction in symptoms than the usual treatment group (Koenig et al. 2023). In sum, the Handbook of Religion and Health (2023) found that of the 24 RCTs identified by Koenig et al., most (18) concluded that religious-based interventions were related to benefits above those of control groups. Only two reported no effect, and only one found religious intervention was related to increased mental health difficulties (anxiety associated with “spiritual direction”), specifically amongst alcoholics. Some of these studies have been detailed previously, as they overlapped with other available meta-analyses.
Mechanisms of R/S on Mental Well-Being
Various factors have been examined as possibly underpinning the relationship between R/S and both depression and anxiety. These factors include the benefits of social support, and specifically religious social support (Cipriani et al. 2018; Vicente et al. 2018), the connection between R/S and positive psychology via R/S’s production of positive emotions, including love, awe, trust/faith, compassion, gratitude, forgiveness, and hope (Cloninger 2006; Koenig et al. 2014; Rosmarin and Koenig 2020; Vaillant 2013), R/S’s promotion of healthy behaviors, leading to decreased substance abuse (Moreira-Almeida et al. 2006), and R/S’s assembly of a sense of coherence and meaning-making through a R/S worldview, something that is evidenced to be especially supportive during life adversities (Pargament et al. 2004; Pargament and Lomax 2013). At the same time, there are aspects of R/S that may relate positively to mental health difficulties. For example, negative religious coping is related to poorer mental health; thus, the relationship between R/S and anxiety is commonly caveat-ed by the type of religious coping the individual utilizes (Aggarwal et al. 2023).
Spiritual but not Religious
While much of the research groups the concepts of “spirituality” and “religiosity” as a single entity, it is increasingly essential to differentiate these concepts, as it has become increasingly popular to identify as “spiritual but not religious” (King 2014). Additionally, some research describes separate, and sometimes even opposite effects, of these on mental health. King’s (2014) study, for example, found that those who were at the highest risk for common mental disorders (depression and anxiety) held a spiritual life view devoid of the context of religious practices. King further explained, “Our conclusions from this study were that neither a religious nor spiritual life-view was protective against major depression. In contrast, it appeared that those with a spiritual life-view had an elevated risk (2014, 110).” Additionally, King also did not find any significant advantage to a religious life-view on mental health (King 2014). Further emphasizing the possible differing influences of spirituality and religiosity, an analysis of data from interviews with 7,403 patients of the third English National Psychiatric Morbidity study compared the various indicators of mental well-being across differing R/S identities. It indicated that individuals who possessed a spiritual understanding of life, absent a religious framework, had worse mental health than those with neither (those who were religious were “broadly similar”). The spiritual individuals were more likely than those who had neither a spiritual nor religious understanding to have GAD, phobia, or any neurotic disorder, as well as take psychotropic medication, and abuse recreational drugs (King et al. 2013, 71). King’s research is also supported by Vitorino et al’s (2018) work that examines the mental health outcomes (quality of life, depressive symptoms, anxiety, optimism, and happiness) of 1,046 Brazilian adults with varying R/S identities: those with both high R/S, high religiosity and low spirituality, vice versa, or low levels of both. The low religiousness, high spirituality group was associated with better social and environmental quality of life outcomes but also associated with more anxiety- a result that is upheld by the previously discussed literature. Lower levels of both R/S were associated with worse outcomes, suggesting that having high levels of R/S may cultivate better mental well-being than having one without the other or none. What's more, the high religiosity group demonstrated better self-perception of quality of life, optimism, and happiness as compared with the high spirituality and low R/S groups, representing that religious practices may be more vital to mental health than high levels of spirituality (Vitorino et al. 2018). These studies are of particular interest and importance to the conversation regarding the effects on mental health of R/S due to its emphasis on the possible dissimilarity of the effects of the various identities.
Current Study
Concerning the overall effects of R/S on mental well-being, it is important to note that the relationship between mental health and religion may be bidirectional. As previously cited, Li and colleagues (2016) also found in their work that women who were depressed were less likely to attend religious services four years later (Li et al. 2016). Thus, the need for further longitudinal research is particularly strong. Especially in the case of anxiety, it appears difficult to establish temporal precedence: which came first, the anxiety, or the decreased participation in spiritual and religious practices?
Consequently, more research still needs to be devoted to investigating the effects of various combinations of religion and spirituality on anxiety and depression. While a meager few studies do differentiate religion and spirituality- such as King (2014)- a majority of the current literature groups the constructs together instead of examining them as separate entities (Khan 2019; Koenig 2008). The necessity of their distinction is increasingly relevant as religious identities have become more fluid, ranging from those who participate in orthodox organized religion to those who practice private meditation and pondering. In addition, as stated, it has become progressively popular for individuals to identify as “spiritual but not religious” (King 2014). Furthermore, a majority of the studies, as evidenced by those previously mentioned, examine the effects of R/S on the mental wellness of adults; research examining adolescents is extremely sparse.
To address this gap, our research presents a longitudinal study of adolescents in the Western United States: Utah, Arizona, and California. The present study compares the depression and anxiety levels of a large sample of parents and their adolescent to young adult children, who self-identify as either “spiritual but not religious”, “religious but not spiritual”, both, or neither, examining their mental health across a span of eight years. We refer to these groups as, respectively: SBNR, RBNS, RAS, and NSNR. Data are from an ongoing longitudinal study, The Family Foundations of Youth Development Project, which examines a variety of subjects such as faith, parenting, suicidal ideation, risky behavior, body image, family processes, mental health, etc. This specific question over who has the edge on mental wellness between the aforementioned groups is investigated, and our data presented, in an effort to better inform the public, allowing for the dissemination of accurate narratives, and to assist clinicians and researchers as they work to become more multiculturally aware of the relationship between R/S and mental health to best tailor therapeutic/clinical care. Our research aims to determine how the mental health of children and their parents is affected by the conjunction of spirituality and religiosity together, the lack of either, religiosity in the absence of spirituality, or spirituality in the absence of religiosity. Based on the previous literature, we hypothesize that:
- Those who identify as both religious and spiritual (RAS) will have the best mental health (i.e., the lowest levels of depression and anxiety) as compared with those who are Spiritual but not Religious (SBNR), Religious but not Spiritual (RBNS), or Neither Spiritual nor Religious (NSNR).
- Those who are neither religious nor spiritual (NRNS) will have the worst mental health.
- Those who identify as either religious but not spiritual (RBNS), or spiritual but not religious (SBNR) will demonstrate levels of mental health between their two counterparts.
- Identifying as Spiritual but not Religious may be detrimental to mental well-being.
2. Results
2.1. Demographics
In 2020 (baseline year), children were an average age of 16.2 (SD = 1.2), and parents were an average age of 47.3 (SD = 5.9). Thirty-nine percent lived in Utah, 30% lived in Arizona, and 31% lived in California. For the children, most identified as white (76.7%), with 8.2% identifying as Hispanic, and 2.4% as Black or African American, with the others from various other racial/ethnic backgrounds. Regarding household income, 10.2% made $45,000 or less, with 32.6% making between $45,000 and $100,000, and the rest (57.2%) making over $100,000.
2.2. Baseline Depression/Anxiety Levels
Table 1 contains levels of depression and anxiety in 2020 (baseline) for both parents and adolescents. Superscripts indicate differences in R/S groups at p < .05. For child depression, the SBNR group had significantly higher levels of depression than each of the other groups, and the RAS group had significantly lower levels of depression than every other group. Regarding parents’ depression, the RAS group had significantly lower depression than RBNS and SBNR, with no other differences found. For child anxiety, the SBNR group had significantly higher levels of anxiety compared with all other groups, with no other significant difference. For the parents’ anxiety, RAS was significantly lower than SBNR and RBNS. The RBNS and SBNR also had significantly higher anxiety than the NRNS.
2.3. Child Depression Over Time
Measurement invariance tests found child depression to be invariant across time, allowing for the specification of a growth curve model (analysis details available from the second author). Table 2 displays regression coefficients for all multilevel growth curve models. Figure 1 displays child depression trajectories across time. RAS and SBNR 2020 levels of child depression were significantly different from all groups. The SBNR group had higher levels of depression, and the RAS group, lower. NRNS and RBNS groupings were not significantly different from each other. None of the groups significantly changed in their depression over time except SBRN, which significantly decreased over time at a rate of -.0312 (p=0.000), being slightly less (though not significantly different from) the RBNS in 2024. It may be that given SBRN began at the highest level of depression, therefore, they had little room to decrease so the decrease may represent a ceiling effect.
2.4. Child Anxiety Over Time
Measurement invariance tests found child anxiety to be invariant across time, allowing for the specification of a growth curve model. Figure 2 displays child anxiety across time. The SBNR group had the highest baseline anxiety, which was significantly higher than every other baseline child anxiety grouping. All other baseline levels were not significantly different from each other. RBNS, NRNR, and RAS individuals’ anxiety levels significantly increased over time at rates of .0494 (p=.001), .0497 (p=.000), and .0158 (p=.017), respectively. SBNR anxiety did not significantly change over time, starting high and remaining high. Similar to child depression, the RBNS grouping was slightly, though non-significantly, higher in anxiety than SBRN in 2024.
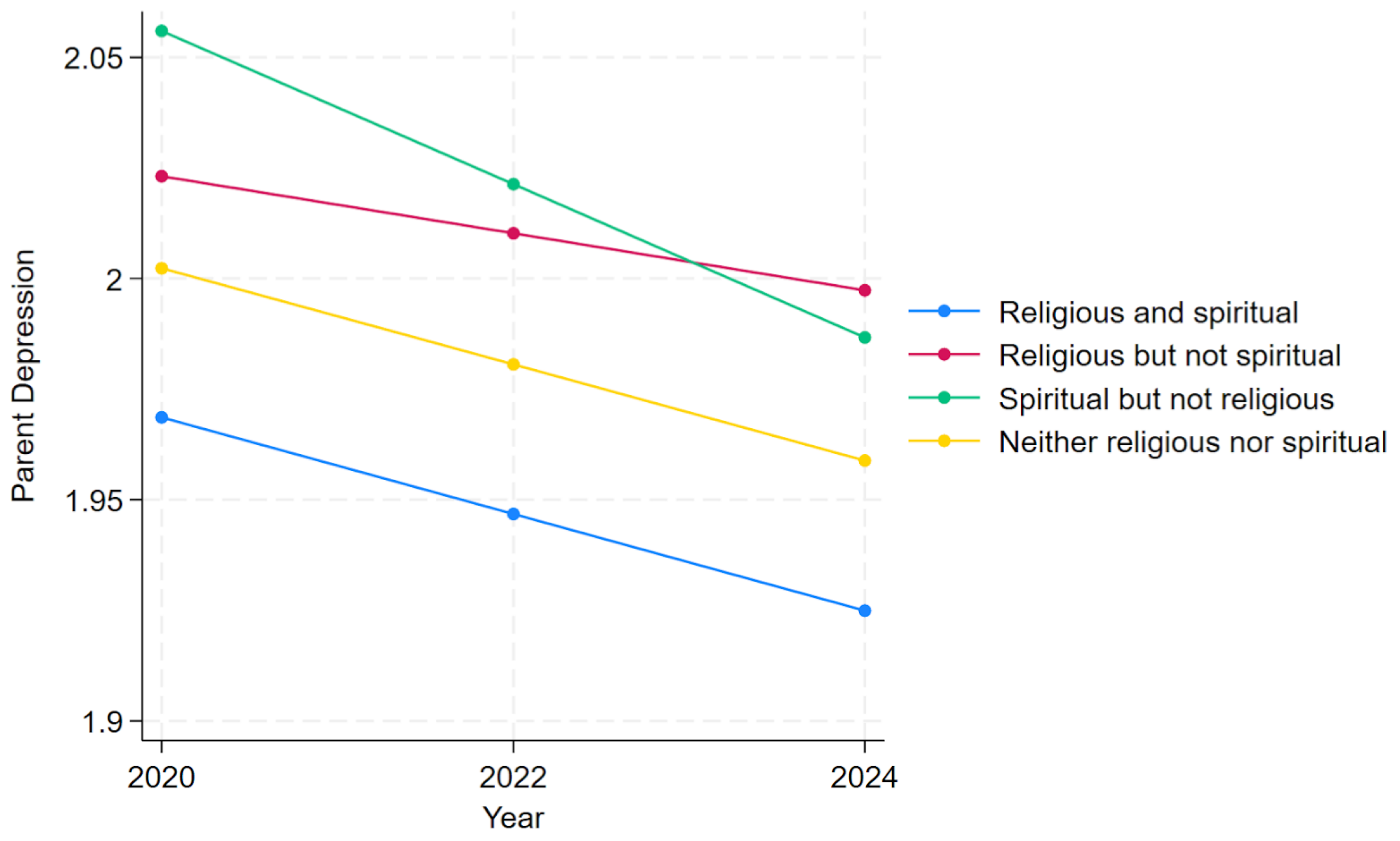
2.5. Parent Depression Over Time
Measurement invariance tests found parent depression to be invariant across time, allowing for the specification of a growth curve model. Parent depression across time is depicted in Figure 3. At baseline, the SBRN and RBNS groupings had significantly higher levels of depression than the RAS group; no other significant differences between categories were found. RAS, SBNR, and NRNS depression significantly decreased over time at a respective rate of -.0218 (p=.000), -.0347 (p=.000), and -.0217 (p=.014). Only RBNS did not significantly change across time. As with previous analyses, although SBNR were highest in 2020 (baseline), by 2024, SBNR were lower than RBNS, though this difference was not significant.
2.6. Parent Anxiety Over Time
Measurement invariance tests found parent anxiety to be variant across time. Given the underlying structure of this variable changes across time, it was inappropriate to specify a growth curve model. We therefore do not examine parent anxiety over time.
Figure 1.
Child depression over time by religious and spiritual groups based on a multilevel growth model.
Figure 1.
Child depression over time by religious and spiritual groups based on a multilevel growth model.
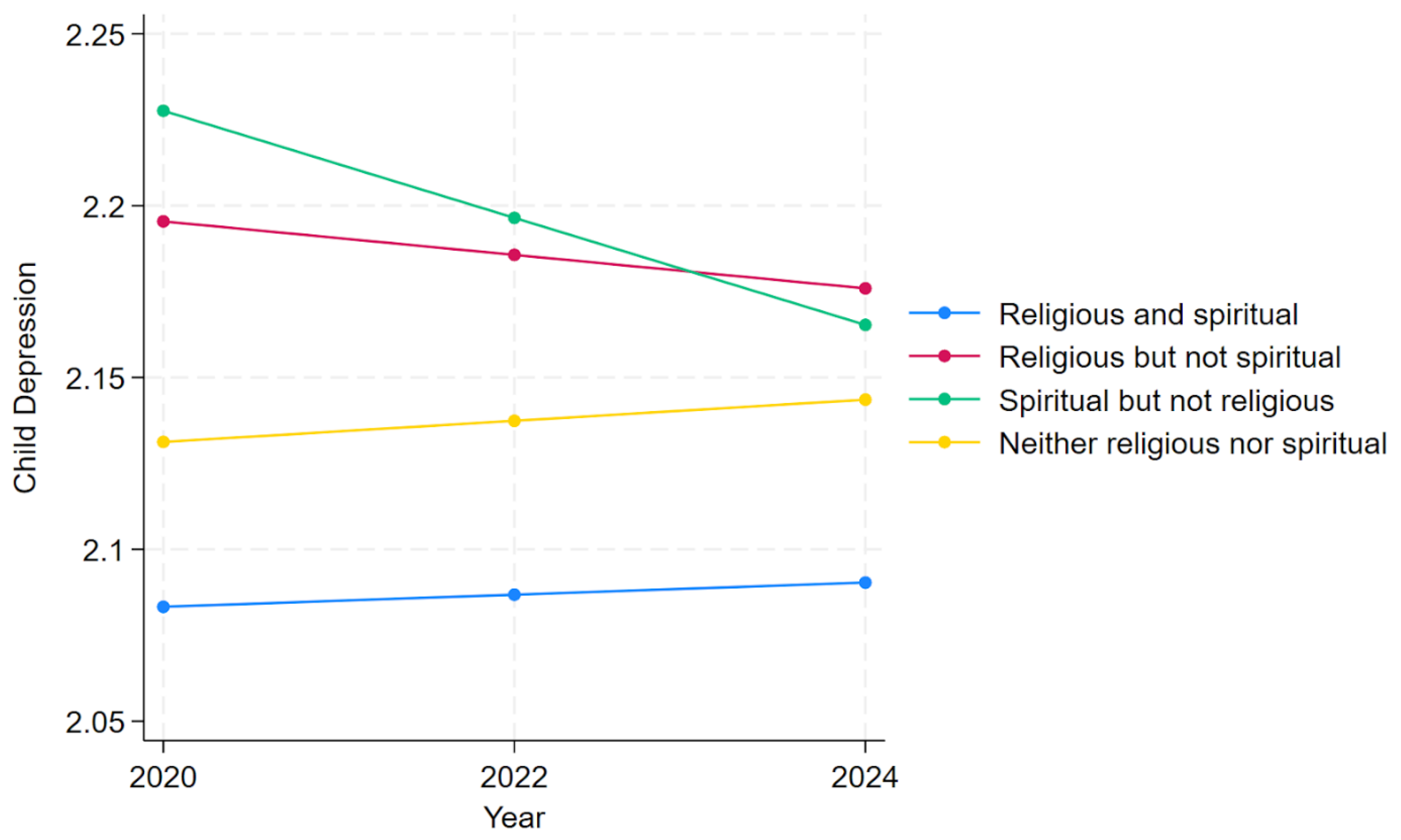
Figure 2.
Child anxiety over time by religious and spiritual groups based on a multilevel growth model.
Figure 2.
Child anxiety over time by religious and spiritual groups based on a multilevel growth model.
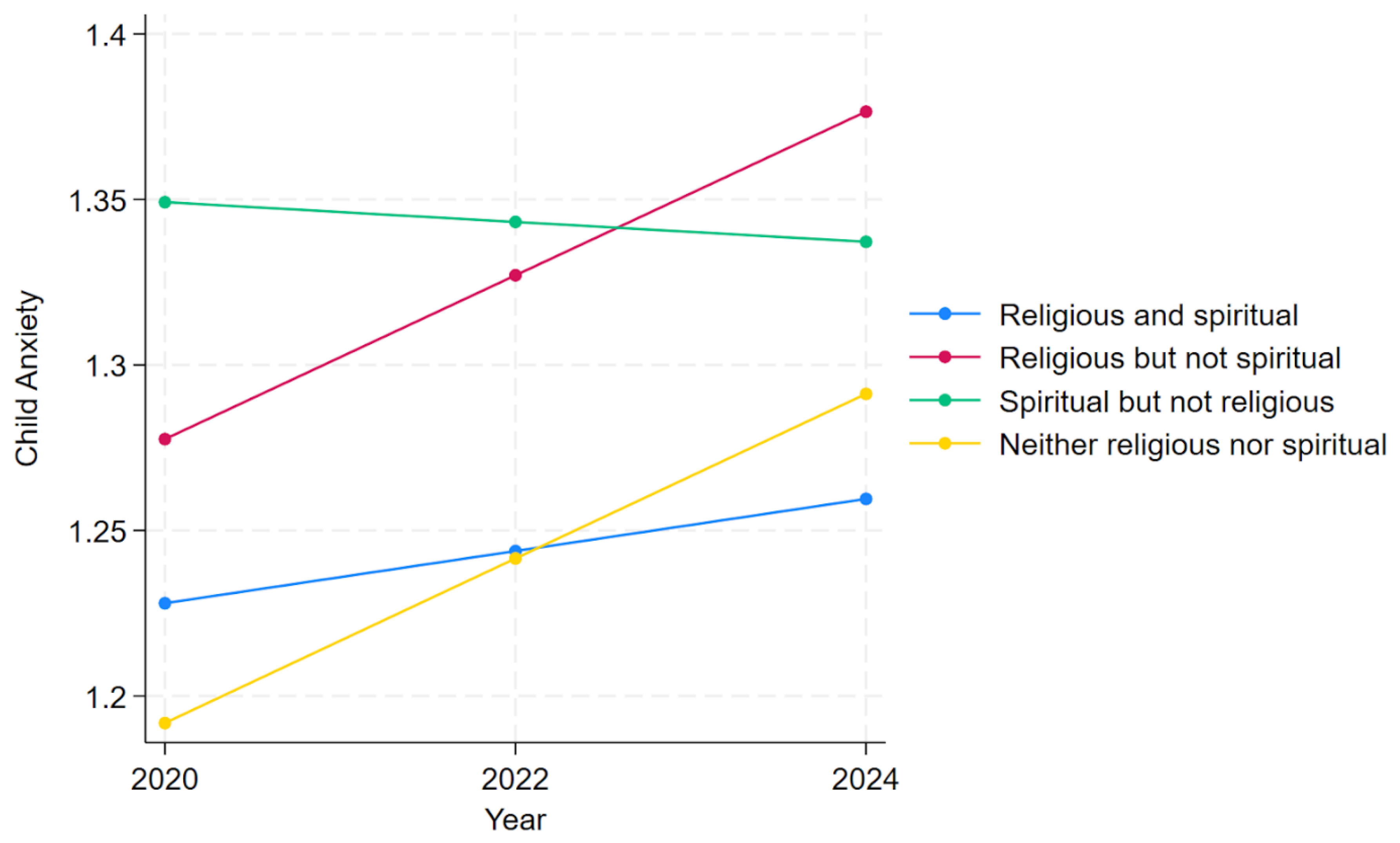
Figure 3.
Parent depression over time by religious and spiritual groups based on a multilevel growth model.
Figure 3.
Parent depression over time by religious and spiritual groups based on a multilevel growth model.
3. Discussion
It is apparent that at each of the child baseline levels, individuals who identified as SBNR had the highest levels of anxiety and depression (the worst mental health). Concerning children’s depression, it was significant that individuals who identified as RAS had the lowest levels of depression (the overall best mental health). The difference between these two groupings, specifically, was significant across every baseline scale. Additionally, for children’s depression, both of these groupings were significantly different from the RBNS and the NRNS groupings (with RAS having lower depression levels, and SBNR having higher). Especially regarding children’s depression, these findings were consistent with the literature and portions of our hypothesis (Bonelli et al. 2012; Koenig et al. 2012; 2023; Rosmarin and Koenig 2020). Also consistent with the literature, our findings on anxiety, both at baseline and across time, were much more nuanced (Chen et al. 2020; Peterman et al. 2014). Although one cannot infer causation, nor a specific linear direction (it is possible that either SBNR individuals have the worst mental health, or those with the worst mental health identify as SBNR), these findings teach us that there is a possible association between this identity and higher levels of anxiety and depression. A possible explanation may be that a yearning for connection with a higher power, devoid of the structure, doctrines, or social support of organized religious practices, may leave a person feeling confused and downhearted: looking for transcendent connection without direction, having questions without faith claims to answer. While the baseline mental health levels of this grouping were significantly worse than the RAS grouping, and significantly worse than all other groupings for children, this was the only group for children to significantly decrease in their depression levels across time, and the only group to not significantly increase in their anxiety levels across time. Although this may represent a possible regression to the mean, this association may also lead to the conclusion that increased spirituality (even, or specifically, lacking religiosity) may improve the mental health of adolescents. As Wave 3 data was gathered in 2020, the impacts of the COVID-19 pandemic may have resulted in the higher baseline depression levels, which, as for adults, generally decreased over time. This could be especially true for the SBNR individuals, as it may represent those who were unable to practice their religion at the time the baseline levels were measured due to social distancing and church closures. The general increase in anxiety across time may also represent the stresses related to a post-COVID reintegration into society. Future research should be done to examine these relationships while controlling for the effects of the pandemic. As for the adults, each group of adults got significantly less depressed over time, except those who identified as RBNS. A possible explanation for this trend could be that adults may be particularly affected by the cognitive dissonance that may result from participating in religious practices without internalizing them spiritually.
Limitations/Future Research
Our study did not examine grouping shifts- individuals may not belong to the same groupings each year, thus future research should examine the mental health changes that accompany shifts in R/S identities (for example, conversion, apostasy, or deconversion). Furthermore, our study only examined the main effect of R/S on anxiety. This is essential to acknowledge, as a large portion of the scientific literature regarding the relationship between R/S and anxiety is mediated by religious coping. Positive religious coping involves using religious and spiritual beliefs to create meaning and find comfort through difficulties. In Christianity, for example, this may look like relying on a belief that Jesus Christ has experienced one’s pain and can help one persevere through and learn from difficulties. Positive religious coping has been shown to predict a significant decline in anxiety symptoms amongst psychiatric patients (Rosmarin et al. 2013). An aspect of positive religious coping is positive beliefs about, and a positive attachment style to, God (or the subject of one’s worship more broadly). Viewing God as benevolent, merciful, and loving has been associated with decreased anxiety and depression, as well as fewer worries, fears, social apprehensions, paranoias, and obsessions/compulsions (Flannelly et al. 2010; Schaefer and Gorsuch 1991; Silton et al. 2014). Indeed, a common theme in the literature is that positive religious coping can function as a protective factor against, and can help alleviate, anxiety.
Negative Religious Coping, however, is frequently found to have a negative relationship with mental health. Negative religious coping (NRC) involves negative religious beliefs: specifically, anger, fear, or feelings of abandonment towards God. These negative religious beliefs, especially the belief that one will be punished for sins, seem to generate greater anxiety (Chapman and Steger 2010; Ellison et al. 2009; Ramirez et al. 2012; Sherman et al. 2009; Trenholm et al. 1998). A longitudinal study by Peterman et al. (2014) found that those who increased their religious attendance over time were more likely to experience increased anxiety, while low religious attendance was associated with decreased anxiety symptoms comparatively. However, self-reported guilt mediated this relationship. Again, it appears that the primary element of negative religious coping is negative beliefs about, or a negative attachment style to, God. Silton et al.’s (2014), McConnell et al.’s (2006), and Rosmarin et al.’s (2009, 2010) work support the notion that mistrust in God, or a perception of one’s deity as malevolent, is associated with greater stress, worry, and anxiety across multiple religious traditions.
It can be seen that one’s view of their god is essential in determining the effect that their religion has on their mental well-being: the more secure one’s attachment style to God is, the less distress and anxiety they experience. With this in mind, a limitation of our current study is that we exclusively studied the main effect of R/S categories on depression and anxiety and did not measure religious coping.
Additionally, as is evidenced by the literature, randomized clinical trials generally, and with greater certainty, as compared with cross-sectional research, uphold that religious and spiritually incorporated psychotherapy yields positive effects on participants’ mental well-being, with religious individuals preferring interventions with greater relevance to their religious beliefs (Ford and Garzon 2017). This evidence has steered the psychological conversation toward a discussion on the logistics of integrating R/S practices into therapeutic treatments, as well as the cultivation of an alliance between clinicians and ecclesiastical leaders (Rosmarin and Koenig 2020).
Finally, as our participants were derived from only three states, the sample demographics, especially for race/ethnicity, are generally homogeneous, and many individuals belong to The Church of Jesus Christ of Latter-day Saints. Future research should obtain and examine more diverse demographics, as researchers, clinicians, and concerned citizens work to improve the mental health of our society.
4. Materials and Methods
Sample
Participants were taken from waves 3, 4, and 5 of the Family Foundations of Youth Development Project: a longitudinal study that began in 2016, which surveys and interviews parent-child dyads via random sampling from Utah, Arizona, and California (see foundations.byu.edu for more information). At wave 3, 1,666 observations (n=1,666) on anxiety and depression were obtained from the participating children, and 1,693 observations on depression (n=1,693), and 1,605 on anxiety (n=1,605) from the parents. The final sample size, which also incorporated waves 4 and 5, was 1,618 child observations and 1,671 parent observations.
Measures
Child Anxiety was measured with the Spence Anxiety Scale (Burns 1989). This six-item questionnaire asked participants to rate themselves on a Likert scale of 1 = never to 4 = always. They were asked how often they experienced various anxiety symptoms, prompted by items such as “I worry about things” and “I feel afraid.” Across waves, Cronbach’s alpha for this scale ranged from .87 to .88
Parent Anxiety was measured with the Burns Anxiety Scale (Burns 1989). This was also a six-item questionnaire, but rather asked participants “How much have you experienced the following in the last week?” and instructed them to rate themselves on a Likert scale of 1= Not at all to 4= A lot. Items of which the parents rated their weekly experience included “Anxiety, nervousness, or worry” and “sudden unexpected panic spells.” Across waves, Cronbach’s alpha for this scale ranged from .80 to .86.
Child and Parent Depression was measured with the CESD-10 (Björgvinsson et al. 2013). This 10-item measure asked participants “How often have you felt this way during the PAST WEEK?” and provided a 4-category Likert scale that ranged from 1=rarely or none of the time (less than 1 day) to 4=Most or all of the time (5-7 days). Items included questions such as “I felt everything I did was an effort” and “I felt lonely.” Across waves and across parents and children, Cronbach’s alpha for this scale ranged from .81 to .84.
Religious/Spiritual Groupings were measured with Smith and Denton’s (2005) scale, which asks participants to select which of the following best describes themselves: “religious and spiritual,” “religious but not spiritual,” “spiritual but not religious,” or “neither religious nor spiritual.”
Analysis Plan
All analyses were conducted in Stata 19. Depression and anxiety across time were generated using latent variables with effects coding, thus reducing measurement error and preserving the scale for longitudinal analyses (Little 2024). We initially compared baseline (2020) levels for both adolescents and parents across religious/spiritual groupings. A multilevel growth curve model was then specified (the command “mixed” in Stata) with “year” treated as a continuous predictor. Year 2020 was coded 0, 2022 was coded 1, and 2024 was coded 2. The year variable interacted with a nominal variable indicating religious/spiritual groupings to test whether baseline and trajectory of depression/anxiety differed by religious/spiritual groups. Important to testing growth over time is first determining whether the construct is invariant across time (Widaman et al. 2010). If a construct is not invariant across time, it is inappropriate to use growth curve models. Finally, in the growth curve models, we controlled for participant sex (male, female), family income, family state (Arizona, California, or Utah), and race.
5. Conclusions
Religion and spirituality are found to be impactful to humans worldwide, and thus, must be psychologically and representatively studied. With the recent increase in those who are spiritual but not religious, it is important to better understand how this may relate to well-being. Our study added to the existing literature by examining the depression and anxiety levels of adolescents and their parents who belong to various R/S categories both at the baseline and across time. We found that those with a spiritual life view devoid of a religious background demonstrated significantly higher levels of anxiety and depression when compared with those who identified as both religious and spiritual, with children who identified as RAS exhibiting the lowest levels of depression. The difference between these two groupings, RAS and SBNR, was significant across every baseline category. The SBNR group was the only category of children to show a significant decrease in depression levels, and the only group not to increase in anxiety levels across time. Each R/S identity amongst adults significantly decreased in their depression levels across time, except the RBNS category. As we have contributed to this ongoing conversation, we call upon additional researchers to continue this important pursuit as we work to heal and strengthen the mental well-being of our adolescents, and our society as a whole.
Author Contributions
Conceptualization, Clevenger. A. and Dyer. W.J .; methodology, Dyer. W. J.; software, Dyer. W. J.; validation, Dyer. W. J.; formal analysis, Dyer. W. J.; investigation, Clevenger. A. and Dyer. W. J.; resources, Dyer. W. J.; data curation, Dyer. W. J.; writing—original draft preparation, Clevenger. A.; writing—review and editing, Dyer. W. J. and Clevenger. A.; visualization, Dyer W. J. and Clevenger, A.; supervision, Dyer. W. J.; project administration, Dyer. W. J.; funding acquisition, Dyer. W. J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of BRIGHAM YOUNG UNIVERSITY, IRB 2021-342-BYU.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study
Data Availability Statement
The data are available based on an application to the study’s authors.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| SBNR | Spiritual but Not Religious |
| RBNS | Religious but Not Spiritual |
| RAS | Religious and Spiritual |
| NRNS R/S |
Neither Religious nor Spiritual Religiosity/Spirituality |
References
- Aggarwal, S., J. Wright, A. Morgan, G. Patton, and N. Reavley. 2023. “Religiosity and Spirituality in the Prevention and Management of Depression and Anxiety in Young People: A Systematic Review and Meta-Analysis.” BMC Psychiatry 23 (1).
- Ai, A. L., C. Peterson, T. N. Tice, B. Huang, W. Rodgers, and S. F. Bolling. 2007. “The Influence of Prayer Coping on Mental Health among Cardiac Surgery Patients: The Role of Optimism and Acute Distress.” Journal of Health Psychology 12 (4): 580–96. [CrossRef]
- Ai, A. L., T. N. Tice, C. Peterson, and B. Huang. 2005. “Prayers, Spiritual Support, and Positive Attitudes in Coping with the September 11 National Crisis.” Journal of Personality 73 (3): 763–91. [CrossRef]
- American Psychiatric Association. 2022. Diagnostic and Statistical Manual of Mental Disorders. Edited by text rev.; DSM-5-TR 5th. American Psychiatric Association. [CrossRef]
- Björgvinsson, T., S. J. Kertz, J. S. Bigda-Peyton, K. L. McCoy, and I. M. Aderka. 2013. “Psychometric Properties of the CES-D-10 in a Psychiatric Sample.” Assessment 20: 429–36.
- Boelens, P. A., R. R. Reeves, W. H. Replogle, and H. G. Koenig. 2009. “A Randomized Trial of the Effect of Prayer on Depression and Anxiety.” International Journal of Psychiatry in Medicine 39 (4): 377–92. [CrossRef]
- Boelens, P. A., R. R. Reeves, W. H. Replogle, and H. G. Koenig. 2012. “The Effect of Prayer on Depression and Anxiety: Maintenance of Positive Influence One Year after Prayer Intervention.” International Journal of Psychiatry in Medicine 43 (1): 85–98. [CrossRef]
- Bonelli, R., R. E. Dew, H. G. Koenig, D. H. Rosmarin, and S. Vasegh. 2012. “Religious and Spiritual Factors in Depression: Review and Integration of the Research.” Depression Research and Treatment 2012: 96286. [CrossRef]
- Brody, Debra, and Jeffery Hughes. 2025. Prevalence of Depression in Adolescents and Adults: United States, August 2021–August 2023. National Center for Health Statistics (U.S.). [CrossRef]
- Burge, Ryan P. 2021. The Nones: Where They Came From, Who They Are, and Where They Are Going. Fortress Press. [CrossRef]
- Burns, D. D. 1989. The Feeling Good Handbook. William Morrow & Co.
- Byrd, K. R., and A. Boe. 2001. “The Correspondence between Attachment Dimensions and Prayer in College Students.” International Journal for the Psychology of Religion 11 (1): 9–24. [CrossRef]
- Captari, L. E., J. N. Hook, W. Hoyt, D. E. Davis, S. E. McElroy-Heltzel, and E. L. Worthington Jr. 2018. “Integrating Clients’ Religion and Spirituality within Psychotherapy: A Comprehensive Meta-Analysis.” Journal of Clinical Psychology 74 (11): 1938–51. [CrossRef]
- Chapman, L. K., and M. F. Steger. 2010. “Race and Religion: Differential Prediction of Anxiety Symptoms by Religious Coping in African American and European American Young Adults.” Depression and Anxiety 27 (3): 316–22. [CrossRef]
- Chen, Ying, Eric S Kim, and Tyler J VanderWeele. 2020. “Religious-Service Attendance and Subsequent Health and Well-Being throughout Adulthood: Evidence from Three Prospective Cohorts.” International Journal of Epidemiology 49 (6): 2030–40. [CrossRef]
- Cipriani, Andrea, Toshi A Furukawa, Georgia Salanti, et al. 2018. “Comparative Efficacy and Acceptability of 21 Antidepressant Drugs for the Acute Treatment of Adults with Major Depressive Disorder: A Systematic Review and Network Meta-Analysis.” The Lancet 391 (10128): 1357–66. [CrossRef]
- Cloninger, C. R. 2006. “The Science of Well-Being: An Integrated Approach to Mental Health and Its Disorders.” World Psychiatry 5 (2): 71–76.
- Dehghani, K. H., R. A. Zare, Z. Pourmovahed, H. Dehghani, A. Zarezadeh, and Z. Namjou. 2012. “The Effect of Prayer on Level of Anxiety in Mothers of Children with Cancer.” [Journal Not Specified].
- Ellison, C. G., A. M. Burdette, and T. D. Hill. 2009. “Blessed Assurance: Religion, Anxiety, and Tranquility among US Adults.” Social Science Research 38 (3): 656–67. [CrossRef]
- Flannelly, K. J., K. Galek, C. G. Ellison, and H. G. Koenig. 2010. “Beliefs about God, Psychiatric Symptoms, and Evolutionary Psychiatry.” Journal of Religion and Health 49 (2): 246–61. [CrossRef]
- Foley, E., A. Baillie, M. Huxter, M. Price, and E. Sinclair. 2010. “Mindfulness-Based Cognitive Therapy for Individuals Whose Lives Have Been Affected by Cancer: A Randomized Controlled Trial.” Journal of Consulting and Clinical Psychology 78 (1): 72–79. [CrossRef]
- Ford, K., and F. Garzon. 2017. “Research Note: A Randomized Investigation of Evangelical Christian Accommodative Mindfulness.” Spirituality in Clinical Practice 4 (2): 92–92.
- Harber, Ian. 2024. “TikTok: Now Serving Deconstruction.” Endeavor With Us, September 4. https://www.endeavorwithus.com/deconstructing-faith-on-tiktok.
- Hasin, D. S., A. L. Sarvet, and J. L. Meyers. 2018. “Epidemiology of Adult DSM-5 Major Depressive Disorder and Its Specifiers in the United States.” JAMA Psychiatry 75 (4): 336–46. [CrossRef]
- Jansen, K., R. Motley, and J. Hovey. 2010. “Anxiety, Depression and Students’ Religiosity.” Mental Health, Religion & Culture 13 (3): 267–71. [CrossRef]
- Khan, I. J. 2019. “Spirituality and Religion: Relevance and Assessment in the Clinical Setting.” Current Psychiatry Research and Reviews 15 (2): 80–87.
- King, M. 2014. “The Challenge of Research into Religion and Spirituality Keynote1Keynote1.” Journal for the Study of Spirituality 4 (2): 106–20. [CrossRef]
- King, Michael, Louise Marston, Sally McManus, Terry Brugha, Howard Meltzer, and Paul Bebbington. 2013. “Religion, Spirituality and Mental Health: Results from a National Study of English Households.” British Journal of Psychiatry 202 (1): 68–73. [CrossRef]
- Koenig, H. G., L. S. Berk, N. S. Daher, et al. 2014. “Religious Involvement Is Associated with Greater Purpose, Optimism, Generosity and Gratitude in Persons with Major Depression and Chronic Medical Illness.” Journal of Psychosomatic Research 77 (2): 135–43. [CrossRef]
- Koenig, H. G., L. K. George, D. G. Blazer, and J. T. Pritchett. 1993. “The Relationship between Religion and Anxiety in a Sample of Community-Dwelling Older Adults.” Journal of Geriatric Psychiatry 26 (1): 65–93.
- Koenig, H. G., D. E. King, and V. B. Carson. 2012. Handbook of Religion and Health. Oxford University Press.
- Koenig, H. G., T. VanderWeele, and J. R. Peteet. 2023. Handbook of Religion and Health. Edited by 3. Oxford University Press.
- Koenig, Harold G. 2008. “Concerns About Measuring ‘Spirituality’ in Research.” Journal of Nervous & Mental Disease 196 (5): 349–55. [CrossRef]
- Koszycki, D., K. Raab, F. Aldosary, and J. Bradwejn. 2010. “A Multifaith Spiritually Based Intervention for Generalized Anxiety Disorder: A Pilot Randomized Trial.” Journal of Clinical Psychology 66 (4): 430–41. [CrossRef]
- Koukl, Greg. 2022. “Social Media Has Amplified Deconstruction.” Stand to Reason, November 14. https://www.str.org/w/social-media-has-amplified-deconstruction.
- Li, S., O. I. Okereke, S. C. Chang, I. Kawachi, and T. J. VanderWeele. 2016. “Religious Service Attendance and Lower Depression among Women: A Prospective Cohort Study.” Annals of Behavioral Medicine 50 (6): 876–84. [CrossRef]
- Little, Todd D. 2024. Longitudinal Structural Equation Modeling. Guilford Publications.
- McConnell, K. M., K. I. Pargament, C. G. Ellison, and K. J. Flannelly. 2006. “Examining the Links between Spiritual Struggles and Symptoms of Psychopathology in a National Sample.” Journal of Clinical Psychology 62 (12): 1469–84. [CrossRef]
- Moreira-Almeida, A., F. L. Neto, and H. G. Koenig. 2006. “Religiousness and Mental Health: A Review.” Revista Brasileira de Psiquiatria 28 (3): 242–50. [CrossRef]
- National Institute of Mental Health. 2021. “Anxiety Disorders.” National Institute of Mental Health, June. https://www.nimh.nih.gov/health/statistics/anxiety-disorders.
- National Institute of Mental Health. 2022. “Major Depression.” National Institute of Mental Health, June. https://www.nimh.nih.gov/health/statistics/major-depression.
- Ng, G. C., S. Mohamed, A. H. Sulaiman, and N. Z. Zainal. 2017. “Anxiety and Depression in Cancer Patients: The Association with Religiosity and Religious Coping.” Journal of Religion and Health 56 (2): 575–90. [CrossRef]
- Nikfarjam, M., K. Solati, S. Heidari Soureshjani, et al. 2018. “Effect of Group Religious Intervention on Spiritual Health and Reduction of Symptoms in Patients with Anxiety.” Journal of Clinical and Diagnostic Research 12 (11): VC06–9. [CrossRef]
- Pargament, K. I., H. G. Koenig, N. Tarakeshwar, and J. Hahn. 2004. “Religious Coping Methods as Predictors of Psychological, Physical and Spiritual Outcomes among Medically Ill Elderly Patients: A Two-Year Longitudinal Study.” Journal of Health Psychology 9 (6): 713–30. [CrossRef]
- Pargament, K. I., and J. W. Lomax. 2013. “Understanding and Addressing Religion among People with Mental Illness.” World Psychiatry 12 (1): 26–32. [CrossRef]
- Paukert, A. L., L. Phillips, J. A. Cully, S. M. Loboprabhu, J. W. Lomax, and M. A. Stanley. 2009. “Integration of Religion into Cognitive-Behavioral Therapy for Geriatric Anxiety and Depression.” Journal of Psychiatric Practice 15 (2): 103–12. [CrossRef]
- Peterman, J., D. R. LaBelle, and L. Steinberg. 2014. “Devoutly Anxious: The Relationship between Anxiety and Religiosity in Adolescence.” Psychology of Religion and Spirituality 6 (2): 113–22. [CrossRef]
- Pew Research Center. 2023. Spirituality among Americans. Religion & Public Life Project. Pew Research Center. https://www.pewresearch.org/religion/2023/12/07/spirituality-among-americans/.
- Ramirez, S. P., D. S. Macêdo, P. M. Sales, et al. 2012. “The Relationship between Religious Coping, Psychological Distress and Quality of Life in Hemodialysis Patients.” Journal of Psychosomatic Research 72 (2): 129–35. [CrossRef]
- Razali, S. M., C. I. Hasanah, K. Aminah, and M. Subramaniam. 1998. “Religious—Sociocultural Psychotherapy in Patients with Anxiety and Depression.” Australian and New Zealand Journal of Psychiatry 32 (6): 867–72.
- Rosmarin, D. H., J. S. Bigda-Peyton, D. Öngur, K. I. Pargament, and T. Björgvinsson. 2013. “Religious Coping among Psychotic Patients: Relevance to Suicidality and Treatment Outcomes.” Psychiatry Research 210 (1): 182–87. [CrossRef]
- Rosmarin, D. H., and H. G. Koenig. 2020. Handbook of Spirituality, Religion, and Mental Health. Edited by 2. Academic Press.
- Rosmarin, D. H., E. J. Krumrei, and G. Andersson. 2009. “Religion as a Predictor of Psychological Distress in Two Religious Communities.” Cognitive Behaviour Therapy 38 (1): 54–64. [CrossRef]
- Rosmarin, D. H., K. I. Pargament, S. Pirutinsky, and A. Mahoney. 2010. “A Randomized Controlled Evaluation of a Spiritually Integrated Treatment for Subclinical Anxiety in the Jewish Community, Delivered via the Internet.” Journal of Anxiety Disorders 24 (7): 799–808. [CrossRef]
- Sappenfield, Olivia, Cinthyia Alberto, Jessica Minnaert, Julie Donney, Lydie Lebrun-Harris, and Reem Ghandour. n.d. Adolescent Mental and Behavioral Health, 2023. National Survey of Children’s Health Data Briefs [Internet]. Health Resources & Services Administration. Accessed October 18, 2025. https://www.ncbi.nlm.nih.gov/books/NBK608531/.
- Schaefer, C. A., and R. L. Gorsuch. 1991. “Psychological Adjustment and Religiousness: The Multivariate Belief-Motivation Theory of Religiousness.” Journal for the Scientific Study of Religion 30 (4): 448–61. [CrossRef]
- Schieman, S., T. Pudrovska, L. I. Pearlin, and C. G. Ellison. 2006. “The Sense of Divine Control and Psychological Distress: Variations across Race and Socioeconomic Status.” Journal for the Scientific Study of Religion 45 (4): 529–49. [CrossRef]
- Sherman, A. C., T. G. Plante, S. Simonton, U. Latif, and E. J. Anaissie. 2009. “Prospective Study of Religious Coping among Patients Undergoing Autologous Stem Cell Transplantation.” Journal of Behavioral Medicine 32 (1): 118–28. [CrossRef]
- Silton, N. R., K. J. Flannelly, K. Galek, and C. G. Ellison. 2014. “Beliefs about God and Mental Health among American Adults.” Journal of Religion and Health 53 (5): 1285–96. [CrossRef]
- Smith, Christian. 2025. Why Religion Went Obsolete. Oxford University Press.
- Sternthal, M. J., D. R. Williams, M. A. Musick, and A. C. Buck. 2010. “Depression, Anxiety, and Religious Life: A Search for Mediators.” Journal of Health and Social Behavior 51 (3): 343–59. [CrossRef]
- Terlizzi, E. P., and B. Zablotsky. 2024. Symptoms of Anxiety and Depression Among Adults: United States, 2019 and 2022. National Health Statistics Reports, no. 213. [CrossRef]
- Trenholm, P., J. Trent, and W. C. Compton. 1998. “Negative Religious Conflict as a Predictor of Panic Disorder.” Journal of Clinical Psychology 54 (1): 59–65. [CrossRef]
- Vaillant, G. E. 2013. “Psychiatry, Religion, Positive Emotions and Spirituality.” Asian Journal of Psychiatry 6 (6): 590–94. [CrossRef]
- Vicente, A. R. T., E. Castro-Costa, J. d. O. A. Firmo, M. F. Lima-Costa, and A. I. d. Loyoola Filho. 2018. “Religiousness, Social Support and the Use of Antidepressants among the Elderly: A Population-Based Study.” Ciencia & Saude Coletive 23 (3): 963–71. [CrossRef]
- Vitorino, Luciano Magalhães, Giancarlo Lucchetti, Frederico Camelo Leão, Homero Vallada, and Mario Fernando Prieto Peres. 2018. “The Association between Spirituality and Religiousness and Mental Health.” Scientific Reports 8 (1): 17233. [CrossRef]
- Wachholtz, A. B., and K. I. Pargament. 2005. “Is Spirituality a Critical Ingredient of Meditation? Comparing the Effects of Spiritual Meditation, Secular Meditation, and Relaxation on Spiritual, Psychological, Cardiac, and Pain Outcomes.” Journal of Behavioral Medicine 28 (4): 369–84. [CrossRef]
- Wachholtz, A. B., and K. I. Pargament. 2008. “Migraines and Meditation: Does Spirituality Matter?” Journal of Behavioral Medicine 31 (4): 351–66. [CrossRef]
- Weinberger, A. H., M. Gbedemah, A. M. Martinez, D. Nash, S. Galea, and R. D. Goodwin. 2018. “Trends in Depression Prevalence in the USA from 2005 to 2015: Widening Disparities in Vulnerable Groups.” Psychological Medicine 48 (8): 1308–15. [CrossRef]
- Wells, Georgia. 2025. “‘Exmo’ Influencers Mount a TikTok War against the Mormon Church: The Church Is Facing a 21st-Century Reckoning, Driven by Social Media—and It Is Racing to Counter the Narrative.” The Wall Street Journal, September 2. https://www.wsj.com/tech/ex-mormon-tiktok-creators-e9a5b00e.
- Widaman, Keith F., Emilio Ferrer, and Rand D. Conger. 2010. “Factorial Invariance Within Longitudinal Structural Equation Models: Measuring the Same Construct Across Time.” Child Development Perspectives 4 (1): 10–18. [CrossRef]
- Wilson, Sylia, and Nathalie M. Dumornay. 2022. “Rising Rates of Adolescent Depression in the United States: Challenges and Opportunities in the 2020s.” Journal of Adolescent Health 70 (3): 354–55. [CrossRef]

Table 1.
Mental Health across religious/spiritual categories in 2020.
| Child Depression | Child Anxiety | Parent Depression | Parent Anxiety | |
| Religious and spiritual (RAS) | 2.07All | 1.22SBNR | 1.93RBNS,SBNR | 1.52RBNS,SBNR |
| Religious but not spiritual (RBNS) | 2.17RAS,SBNR | 1.23SBNR | 2.01RAS | 1.64RAS,NRNS |
| Spiritual but not religious (SBNR) | 2.24All | 1.37All | 1.99RAS | 1.61RAS,NRNS |
| Neither religious nor spiritual (NRNS) | 2.13RAS,SBNR | 1.17SBNR | 1.97 | 1.50RBNS,SBNR |
1Note: Superscripts indicate which categories are significantly different. For example, for child depression, the religious but not spiritual group (RBNS) is significantly higher than the religious and spiritual group, but significantly lower than the spiritual but not religious group.
Table 2.
Multilevel growth curve results across depression and anxiety.
| Child Depression | Child Anxiety | Parent Depression | |
| b(se) | b(se) | b(se) | |
| R/S Groupingsa | |||
| Religious but not spiritual (RBNS) | 0.13(.03)*** | 0.02(.05) | 0.05(.04) |
| Spiritual but not religious (SBNR) | 0.18(.03)*** | 0.14(.05)** | 0.10(.02)*** |
| Neither religious nor spiritual (NRNS) | 0.05(.03) | -0.07(.05) | 0.03(.03) |
| Survey Wave | 0.00(.00) | 0.02(.01)* | -0.02(.00)*** |
| R/S Identification X Wavea | |||
| Religious but not spiritual (RBNS) | -0.01(.01) | 0.03(.02) | 0.01(.01) |
| Spiritual but not religious (SBNR) | -0.03(.01)*** | -0.02(.02) | -0.01(.01)* |
| Neither religious nor spiritual (NRNS) | 0.00(.01) | 0.03(.02)* | 0.00(.01) |
| Male | -0.10(.01)*** | -0.34(.02)*** | -0.01(.02) |
| Income | 0.00(.00)* | 0.00(.00) | -0.01(.00)*** |
| Family Statec | |||
| Arizona | -0.02(.02) | -0.04(.03) | 0.00(.01) |
| California | -0.03(.02) | -0.05(.03) | 0.00(.01) |
| White d | -0.02(.02) | -0.04(.03) | 0.02(.02) |
| Constant | 2.20(.03)*** | 1.45(.04)*** | 2.08(.02)*** |
Religious and Spiritual were the comparison group. b Female was the comparison group. c Utah was the comparison group.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



