
Submitted:
12 November 2025
Posted:
17 November 2025
You are already at the latest version
Abstract
Takotsubo cardiomyopathy (TCM), also known as stress cardiomyopathy or "broken heart syndrome," is a transient form of acute heart failure that mimics acute coronary syndrome (ACS) but typically occurs without obstructive coronary artery disease. Though once considered rare, TCM is increasingly recognized in clinical practice, particularly among postmenopausal women. Despite its rising incidence, significant knowledge gaps remain in its pathophysiology, diagnosis, management, and long-term outcomes. A contemporary understanding of TCM is critical for clinicians to accurately differentiate it from other acute cardiac conditions and provide patient-centered care. This narrative review synthesizes the current literature on TCM, with a focus on evolving theories of pathophysiology, including catecholamine surge and neurocardiac axis dysfunction, alongside emerging diagnostic strategies which may implicate microvascular involvement. We examine the expanding role of cardiac imaging modalities and biomarker profiles in differentiating TCM from ACS, as well as current best practices in acute and long-term management.
Keywords:
takotsubo cardiomyopathy
; broken heart syndrome
; heart failure
1. Introduction
| “And I will give you a new heart, and a new spirit I will put within in you. |
| And I will remove the heart of stone from your flesh, |
| And give you a heart of flesh.” |
| (Holy Bible, English Standard Version, Ezekiel 36:26) |
Takotsubo cardiomyopathy (TCM), also known as stress induced cardiomyopathy or “broken heart syndrome”, is an acute, reversible cardiomyopathy that most commonly affects postmenopausal women [1,2,3], with mortality more than double in men [4], and is typically precipitated by intense emotional or physical stress [5]. First described in Japan in case reports in the early 1990s [6,7] and then later in a multicenter study [5], the syndrome derives its name from the resemblance of the left ventricular silhouette to a “takotsubo”, a traditional Japanese octopus (tako-) pot (-tsubo) trap with a narrow neck and round base. Although its clinical features often mimic those of ST-elevation myocardial infarction (STEMI) [1], coronary angiography in TCM often reveals no significant coronary obstruction. However, co-existing coronary artery disease may still be present in some patients. In this review, we provide an update on the pathophysiology, diagnosis, and management of TCM.
2. Pathophysiology
Catecholamine surge, inducing regional wall remodeling and motion abnormalities, is a central hypothesis in TCM pathogenesis. Triggered by acute stress, patients with TCM exhibit a rapid surge of plasma catecholamines, epinephrine, norepinephrine, and dopamine, with levels reported to be two to three fold higher than those with myocardial infarction [8] and up to 34 times normal values [9]. Rodent models of TCM have successfully replicated its key features using synthetic sympathomimetics [10,11,12], and case reports of TCM associated with pheochromocytoma further support the role of excess catecholamines in its pathogenesis [13,14,15,16]. Moreover, TCM patients receiving catecholamine therapy have been reported to have increased short- and long-term mortality [17,18]. Excess catecholamines are thought to exert direct toxic effects on cardiomyocytes [19,20,21] through alterations in calcium handling [22,23,24,25], disruption in mitochondrial functioning [26,27], and an increase in oxidative stress [28]. Likely due to its higher relative proportion of β-adrenergic receptors relative to the basal segments, the apex of the left ventricle is more susceptible to catecholamine-induced dysfunction [29,30]. This heterogeneous receptor distribution explains the characteristic apical ballooning seen in the majority of TCM cases.
Emerging evidence suggests that the transient myocardial dysfunction characteristic of TCM may also be driven by complex neurocardiac interactions [31]. Multimodal neuroimaging across different phases of TCM, including fMRI, PET, structural MRI, and diffusion tensor imaging, has revealed a dynamic and temporally evolving pattern of brain abnormalities. In the acute phase (within days of diagnosis), patients exhibit markedly increased amygdala metabolic activity, which significantly subsides within one month, consistent with acute hyperactivation of limbic stress-regulatory circuits [32]. Concurrently, acute structural and functional changes include reduced limbic volumes, particularly within the hippocampus, alongside increased cortical thickness in regions such as the insula and thalamus. These alterations are accompanied by enhanced structural connectivity and a mixed pattern of hyper- and hypoconnectivity in networks governing emotion and autonomic regulation [33]. In the chronic phase, the brain-heart axis appears to undergo further remodeling. One study examining patients approximately one-year post-event reported widespread reductions in resting-state functional connectivity across sympathetic, parasympathetic, and default mode networks, suggesting persistent network disruption [34]. In contrast, a separate study conducted nearly three years post-event found increased resting-state and stress-induced functional connectivity in core limbic and central autonomic structures, including the hippocampus, insula, and anterior cingulate cortex [35]. Though seemingly contradictory, these findings likely reflect a time-dependent trajectory—from early disintegration of regulatory networks to later-stage compensatory or maladaptive hyperconnectivity—underscoring the evolving and dynamic nature of brain-heart dysregulation in TCM.
TCM represents a striking convergence of emotional stress, neurohormonal activation, and myocardial vulnerability. The hallmark transient ventricular dysfunction is thought to result from a surge in catecholamines, modulated by regional variability in adrenergic receptor density. However, growing evidence suggests that persistent alterations in central neural circuits, particularly those involved in stress regulation and autonomic control, may extend beyond the acute cardiac event. Continued investigation into the brain–heart axis holds promise not only for elucidating individual susceptibility but also for informing targeted neurocardiac, and potentially psychiatric, interventions aimed at prevention and recovery.
3. Clinical Presentation
TCM typically presents with acute chest pain, dyspnea, syncope, or dizziness, with chest pain being the most common symptom (>75%), often making it clinically indistinguishable from acute coronary syndrome (ACS) [1,36]. Patients may have a history of recent emotional or physical stressors, which are commonly negative, such as grief, conflict, or illness, however in some cases TCM can also be triggered by intense positive experiences. As such, a detailed history may assist with diagnosis. Serious complications include ventricular arrhythmias (such as ventricular tachycardia and ventricular fibrillation), bradyarrhythmia’s, sudden cardiac arrest, significant mitral regurgitation, and ventricular free wall rupture [37]. Patients may also co-present with overlapping features of both ACS and TCM, and in some cases, an ACS event itself can act as a physical stressor that triggers TCM [37,38]. Coronary angiography may reveal a culprit lesion, but the degree and pattern of wall motion abnormalities often appear disproportionate to the severity of coronary disease or the distribution of epicardial coronary involvement [36,39]. Another important differential diagnosis is myocarditis which can present with acute chest pain and heart failure symptoms, typically showing global systolic dysfunction with occasional regional involvement.
4. Assessment, Technology, and Diagnosis
Given the overlap in clinical presentation among TCM, ACS, and heart failure, physical examination findings can also appear similar. Common findings include respiratory distress, rales on auscultation, hypotension, tachycardia, cool extremities, and murmurs due to left ventricular outflow tract obstruction (LVOTO) or acute mitral regurgitation [40]. The differential diagnosis of acute chest pain is broad and includes both cardiovascular and non-cardiovascular causes. Cardiovascular etiologies include myocardial infarction with non-obstructive coronary arteries (MINOCA) and acute aortic syndromes. Non-cardiac causes include pulmonary embolism, pneumothorax, and esophageal rupture. In cases of MINOCA, the underlying mechanisms are typically coronary vasospasm, microvascular dysfunction, or spontaneous coronary artery dissection.
Diagnosing TCM can be challenging as it closely mimics ACS on ECG and biomarker testing [1]. Troponin is elevated in about 87% of TCM cases, though typically to a lesser degree than in ACS, while BNP levels are elevated in over 82%, often more significantly [1,40,41]. Many TCM patients also have incidental, non-obstructive coronary artery disease (CAD), which may not be related to the acute event [36,39]. In stable patients with low suspicion of ACS or suspected recurrent TCM, coronary CT angiography can serve as a valuable non-invasive diagnostic tool. Its role in this setting is to evaluate the epicardial coronary arteries and effectively rule out high-grade stenosis, obstructive CAD, pulmonary embolism, or acute aortic syndromes [39,40,42]. However, the overlap in presentation between TCM and ACS can lead to underdiagnosis of ACS in patients presumed to have TCM. Studies suggest that patients with TCM who do not undergo angiography may have higher mortality rates compared to those who do, highlighting the importance of a thorough diagnostic approach (Figure 1) [43,44].
For patients with TCM, as with anyone presenting with chest pain, ECG is a crucial component of the initial diagnostic evaluation. Common ECG findings in TCM include ST-segment elevation, T-wave inversion, and QT interval prolongation, the latter of which may increase the risk of malignant arrhythmias such as torsade’s de pointes, discussed further in the arrhythmia section of TCM complications [40]. Although ECG abnormalities are frequently present, their sensitivity for diagnosis remains limited [45]. While several studies have proposed ECG criteria to differentiate TCM from ACS, data remains insufficient due to small sample sizes and heterogenous study designs [45]. However, certain features can aid in differentiation. For example, ST-segment depression, commonly observed in ACS, occurs significantly less often in TCM, a distinction incorporated into the InterTAK Diagnostic Score [45]. This scoring system combines clinical variables, such as emotional or physical triggers and neurologic disorders, with ECG findings to improve diagnostic accuracy and help distinguish TCM from ACS [40,46]. While no single ECG characteristic definitively identifies TCM, the overall pattern of ECG changes alongside clinical context provides valuable clues in diagnosis.
Cardiac imaging is essential for the diagnosis of TCM. Ventriculography provides a definitive diagnosis by confirming the characteristic wall motion abnormalities and associated myocardial edema. [39]. Importantly, the absence of late gadolinium enhancement (LGE) on cMRI helps distinguish TCM from ACS and myocarditis [39,40,42,47,48]. Cardiac MRI is also valuable in identifying complications such as left ventricular thrombus or right ventricular involvement, which have prognostic implications [39,42,48]. Echocardiography provides visualization of left ventricular shape, allowing the identification of classic apical dysfunction as well as TCM variants (Figure 2). It also plays a critical role in detecting severe complications: including LVOTO/ejection fraction, valvular dysfunction, right ventricular involvement, thrombus formation, and ventricular wall rupture.
Nuclear imaging has not yet been validated for diagnosing TCM, but it is increasingly used to evaluate perfusion defects and assess wall motion abnormalities. While the role of microvascular dysfunction in TCM remains unclear, it has been proposed as a potential contributor to the syndrome’s pathophysiology. In this context, nuclear techniques such as positron emission tomography (PET) and single-photon emission computed tomography (SPECT) show promise, though their use remains largely limited to research settings [49]. The clinical utility of perfusion assessment in TCM is still debated, as studies have reported increased perfusion while others have shown decreased perfusion. [50,51]. Notably, some investigations in patients with TCM have observed increased tracer uptake in basal myocardial segments, possibly reflecting heightened metabolic demand or compensatory remodeling in response to apical dysfunction [50,52]. There have been varying results with regards to both increased and normal perfusion of the left ventricle that are akinetic in patients with TCM. It is unclear whether these differences in perfusion reflect a continuum of impaired perfusion to quick recovery, distinct phenotypes of the same disease, or possibly other conditions manifesting as TCM [52]. Looking ahead, microvascular evaluation using nuclear imaging could provide valuable prognostic insights in the acute phase of TCM, potentially helping predict ejection fraction, the number of akinetic segments on echocardiography, and the extent of perfusion defects [53].
TCM can be difficult to distinguish from ACS at initial presentation, so patients should be promptly transferred to a cardiology facility with imaging capabilities and a cardiac catheterization lab [40]. Initial management typically follows ACS protocols, including aspirin, a P2Y12 inhibitor, and heparin, with intensive care required for those in cardiogenic shock or post-cardiac arrest [40]. Continuous ECG monitoring is essential, as prolonged QT intervals can lead to torsades de pointes, or the development of AV block. Management is complicated by the lack of high-quality randomized controlled trials in TCM. Retrospective data suggest that angiotensin-converting enzyme inhibitors (ACEi) or angiotensin receptor blockers (ARBs) may improve one-year survival, while beta-blockers have not consistently shown a survival benefit [40,54]. Although some observational studies suggest potential long-term benefit from beta-blockers, particularly in reducing mortality, their effect on recurrence remains unclear, and the observational nature of these studies limits generalizability [54,55].
Treatment of heart failure in TCM depends on congestion and hemodynamics. It’s crucial to assess for LVOTO via transthoracic echocardiography [39,56]. For patients with pulmonary congestion, indicated by dyspnea, orthopnea, and crackles, diuretics are helpful to reduce congestion. In hemodynamically stable patients, beta blockers can be used to manage hypertension and may be especially helpful in LVOTO by reducing hypercontractility and relieving obstruction [57,58].
5. Complications
The most common complication of TCM is acute heart failure (Table 1) [40]. Cardiogenic shock is often associated with LVOTO, acute mitral regurgitation, or right ventricular involvement, each of which can contribute to hemodynamic instability. Arrhythmias, including ventricular arrhythmias, asystole, and bradyarrhythmias, are also frequently reported. Patients with an apical ballooning pattern are at risk for developing a left ventricular thrombus. Notably, the combination of apical ballooning and elevated troponin levels confers a significantly higher risk than apical ballooning alone [59]. In rare cases, ventricular free wall rupture may occur, which can be fatal if not promptly recognized and managed [37,60].
5.1. Acute Heart Failure/Cardiogenic Shock
Systolic heart failure is the most common acute complication of TCM, with risk factors including advanced age, reduced left ventricular ejection fraction (LVEF), and elevated troponin levels [61]. Severe cases may require supportive interventions like mechanical ventilation, inotropes, or an intra-aortic balloon pump (IABP), especially when complications such as pulmonary edema, mitral regurgitation, or LVOTO arise [37].
Management of cardiogenic shock in TCM is largely determined by the presence of LVOTO [56]. While inotropes are often used to increase cardiac output, they can worsen LVOTO by enhancing contractility, which paradoxically exacerbates the shock [57,58]. In such cases, vasopressors like phenylephrine may be preferred to support blood pressure. Rate-controlling agents, such as beta-blockers, help improve ventricular filling time and reduce obstruction [57,58]. Serial echocardiograms are crucial for monitoring LVOTO progression, and if patients fail to respond to medical therapy, advanced interventions like IABP, Impella, or Extracorporeal Membrane Oxygenation (ECMO) should be considered to manage refractory shock.
5.2. Hemodynamic Complications
- Left ventricular outflow tract obstruction (LVOTO)
In the acute phase of TCM, a dynamic LVOTO can develop due to basal hypercontractility and apical stunning, often leading to systolic anterior motion of the mitral valve and resultant mitral regurgitation. Tethering of the mitral valve due to acute left ventricular failure has been reported as a mechanism of mitral regurgitation in patients with TCM [62]. This complication occurs in approximately 10–25% of patients and significantly impairs left ventricular systolic function [61]. These cases are often the most challenging to manage, as both LVOTO and mitral regurgitation further compromise cardiac output. Diagnosis is typically confirmed with Doppler echocardiography. Inotropes and nitrates may worsen the obstruction, while beta-blockers can help reduce it [57,58].
- Valvular dysfunction
Acute mitral regurgitation affects patients with TCM and is associated with more severe outcomes, including reduced LVEF and an increased risk of heart failure or cardiogenic shock. Prevalence has been estimated at 19-25% with one study showing 21% [63]. This condition is commonly caused by systolic anterior motion of the mitral valve, often in conjunction with LVOTO, or by apical tethering of the mitral valve apparatus [62]. Mitral regurgitation typically improves as left ventricular function recovers.
- Right ventricular involvement
RV predominant TCM is a rare subtype characterized by acute RV failure and cardiogenic shock, with imaging showing RV wall motion abnormalities and preserved LV function [64]. It is reported in approximately 11–50% of cases. Management is primarily supportive and may require inotropes or mechanical ventilation. RV involvement has been associated with worse clinical outcomes, including heart failure, cardiac arrest, and prolonged hospitalization [65]. It is also linked to higher rates of intensive care unit admission and increased mortality [37,39,65,66].
- Thrombus formation
Thrombus formation in the akinetic ventricular apex occurs in approximately 1.3–8% of patients with TCM and can lead to serious complications such as stroke or systemic arterial embolism [1,61,67]. Thrombi most commonly develop between 2 and 5 days after symptom onset, typically during the period of persistent left ventricular dysfunction. However, thrombi may also form up to 14 days later, even after apparent recovery of LV function [59]. The role of prophylactic anticoagulation in high-risk TCM remains unclear but may be warranted in selected patients. A 3-month course of oral anticoagulation can be considered in individuals with apical ballooning and elevated troponin levels, as they are at increased risk for LV thrombus formation [59]. Although no randomized studies have compared vitamin K antagonists (VKAs), such as warfarin, to direct oral anticoagulants (DOACs) in this context, DOACs are generally preferred due to their ease of use. Recent guidelines support DOACs as a non-inferior alternative to VKAs in managing thromboembolic risk [68].
- Arrhythmias
The role of beta-blockers in treating TCM remains uncertain, particularly in patients presenting with arrhythmias. While acute arrhythmia management generally follows standard protocols, caution is advised with medications that prolong the QT interval, as over half of TCM patients present with QT prolongation [1,40]. Although TCM is often perceived as a benign condition, it carries significant proarrhythmic risk [69]. Malignant arrhythmias may include ventricular tachycardia, ventricular fibrillation, asystole, high-grade AV block, and sick sinus syndrome [69,70,71]. Life threatening arrhythmias constituted 4.2% of cases [70,72], with atrial fibrillation being the most commonly observed arrhythmia [37,70].
Implantable cardioverter-defibrillator (ICD) placement may be considered for patients with life-threatening arrhythmias; however, given the typically reversible nature of TCM-related ECG and ventricular dysfunction, long-term benefit remains unproven. As such, ICD and wearable cardioverter-defibrillator use should be evaluated on a case-by-case basis, guided by clinical judgment and patient-specific risk factors. Key considerations for ICD implantation include the presence of life-threatening arrhythmias at presentation, such as ventricular tachyarrhythmias or cardiac arrest, as well as persistent long-QT that increases risk of sudden cardiac death despite optimal medical therapy. Similarly, decisions regarding pacemaker placement are influenced by symptomatic bradyarrhythmia, high-grade AV block, or hemodynamic instability, which may necessitate temporary pacing support [70,71,72,73].
- Ventricular free wall rupture
Mechanical complications of TCM, though rare, can be severe and include ventricular free wall rupture or interventricular septal wall rupture. They typically occur in older females, many of whom have a history of hypertension. Some theories to explain this include postmenopausal hormonal changes and anatomical factors such as smaller left ventricular chamber sizes at baseline [60]. While the prognosis remains poor without prompt surgical treatment, timely intervention can significantly improve survival outcomes [74,75]. This complication emphasizes the importance of heightened clinical vigilance and prompt intervention in the management of TCM, particularly in patients presenting with severe manifestations.
6. Takotsubo Variants
- Apical
The apical variant of TCM (Figure 2) is the most common form, accounting for 81.7% of cases, followed by the midventricular type (14.6%). Basal and focal types occur less frequently, representing approximately 2.2% and 1.5% of cases, respectively [1]. Although rare, other variants such as global hypokinesia, biventricular dysfunction, and isolated RV involvement have been reported. These atypical presentations can be associated with severe hemodynamic instability and cardiogenic shock. As most existing literature focuses on the apical form, the less common variants of TCM warrant further discussion, especially given their unique clinical associations and implications for prognosis.
The apical variant is most frequently observed in TCM triggered by emotional stress, or primary TCM, where no clear precipitating factor is identified [76]. In contrast, midventricular and basal variants are more often associated with physical stressors, such as acute medical conditions, surgical procedures, or neurological events, and are therefore categorized as secondary TCM [76]. Of these, the midventricular form has been more commonly linked to surgery, while the basal variant is frequently observed in patients with neurological disorders. Patients with secondary TCM tend to experience longer hospital stays and a higher incidence of in-hospital complications, including more severe heart failure and a greater frequency of ventricular arrhythmias. Early mortality is also increased in cases triggered by secondary causes, whereas patients with primary TCM typically have a more favorable prognosis [76]. Notably, individuals with TCM secondary to neurological conditions have shown worse long-term survival, likely due to the additive effects of both TCM and the underlying neurological disorder [76].
- Midventricular
The midventricular ballooning pattern is characterized by reduced or absent contraction in the middle portion of the LV, while the apex and base of the LV retain normal function [77]. This pattern shares similarities with the well-known apical ballooning, particularly in its strong female predominance [77]. Midventricular ballooning is thought to be a variant of apical ballooning, and long-term follow-up has shown that patients generally experience no recurrence or significant long-term complications [77]. Like the apical variant, the management of mid-ventricular TCM necessitates careful evaluation for LVOTO and valvular abnormalities. This assessment is especially critical in hemodynamically unstable patients, as it plays a key role in guiding appropriate treatment strategies.
- Basal (reverse or inverted Takotsubo)
Patients with the basal variant of TCM, also referred to as the reverse or inverted variant, as it presents with basal hypocontractility and apical hypercontractility. This is the opposite pattern that is seen in the classic apical form, and these patients tend to be significantly younger than those with apical or midventricular variants [78]. Despite presenting with a lower initial LVEF, individuals with the basal variant tended to experience more rapid recovery [78]. The basal form has also been observed in patients with neurological injuries, including intracranial hemorrhage, multiple sclerosis, and serotonin syndrome [79]. Regional differences in catecholamine sensitivity are driven by higher β-adrenergic receptor density at the apex and greater sympathetic nerve density at the base [29,30]. This leads to predominant norepinephrine stimulation at the base and epinephrine effects at the apex during acute stress, which may help explain the development of basal versus apical TCM variants.
7. Prognosis
TCM has a mortality rate similar to acute myocardial infarction, with in-hospital mortality ranging from 2-5% [1,2,3,37]. Poor outcomes are associated with factors such as acute neurologic or psychiatric conditions, elevated troponin levels, age over 75, and admission LVEF <45% [61,80]. Men tend to experience worse clinical outcomes than women, with higher incidences of cardiogenic shock, ventricular arrhythmias, cardiac arrest, and respiratory failure requiring ventilation. In contrast, women are more likely to experience acute systolic heart failure [81].
The type of trigger appears to influence both the clinical presentation and prognosis of TCM, ranging from acute neurological events to surgical stressors, such as following kidney transplant [82]. Physical stressors are more commonly identified as triggers in men, whereas emotional stress is more frequently reported in women. Notably, neurologically triggered TCM is associated with the poorest outcomes, while emotionally induced cases tend to have a more favorable prognosis [76]. There are disparities in outcomes between men and women, which may be explained by the predominance of physical triggers in men, particularly severe neurological events, which are linked to more complicated clinical courses and higher mortality [83]. Interestingly, episodes of severe hypoxia have emerged as a particularly detrimental trigger, with associated worsened outcomes [84]. Perhaps this is related to the sympathetic responses to hypoxia which, through activation of peripheral chemoreceptors, may amplify the overall catecholaminergic drive. Furthermore, patients with secondary TCM exhibit higher mortality, increased rates of major adverse cardiovascular events and more frequent hospital readmissions [76,85]. These findings suggest that the underlying trigger in secondary TCM plays a significant role in the poor prognosis observed.
Although there are no formal guidelines regarding the timing of repeat echocardiography to assess LVEF, reassessment is commonly performed around 4 to 6 weeks post-discharge. Follow-up imaging showed normalization of LVEF by 60 days after admission [1]. Patients with a history of TCM have been found to have a twofold increased risk of hospitalization for any cause compared to the general population, with a particularly elevated risk for cardiovascular events such as acute myocardial infarction, heart failure, and arrhythmias. However, when compared to individuals recovering from acute myocardial infarction, those with TCM tend to experience lower rates of hospital readmission [86].
The recurrence rate of TCM has been estimated to range from 1.5% to 9.6% [87,88,89,90]. Currently, there are no randomized controlled trials evaluating the efficacy of pharmacologic therapies, such as beta-blockers or ACEi/ARBs, in preventing recurrence [54,55]. While some studies suggest that beta-blockers may reduce mortality, they have not demonstrated a significant effect on recurrence rates. The risk factors for recurrence remain poorly defined, and it is unclear whether recurrent episodes are associated with an increased risk of future cardiovascular events or mortality. Interestingly, up to one-third of patients present with a different variant of TCM during recurrence compared to their initial episode [87,88,91]. One theory suggests that regions affected in the initial event may develop a form of localized myocardial adaptation, making them less susceptible to involvement in future episodes. This may explain the variation in regional patterns seen in recurrent cases, although the underlying mechanisms remain unknown.
8. Limitations
Understanding and managing TCM is limited by the absence of randomized controlled trials, with most evidence based on retrospective and observational studies. The condition’s variable clinical presentation, including fewer common variants, and uncertain pathophysiology further complicate diagnosis and treatment. The diverse triggers of TCM, such as emotional, neurological, or physical stress, result in heterogenous patient populations, creating challenges in understanding the disease’s full spectrum and tailoring management to individual cases. Diagnosis is also challenging because TCM mimics other acute life-threatening conditions such as ACS or myocarditis, increasing the risk of misdiagnosis or delayed treatment. Additionally, long-term outcomes including the effectiveness of therapies such as beta-blockers remain unclear. This lack of high-quality data hinders the development of standardized treatment and follow-up strategies, highlighting the need for prospective research.
9. Conclusion
Management of TCM often mirrors that of ACS, given the similar clinical presentation and the necessity of excluding alternative diagnoses such as myocarditis [40]. Although no randomized controlled trials have established guideline-directed therapy for TCM, observational studies suggest a potential survival benefit with ACEi or ARBs, whereas beta-blockers have not demonstrated consistent efficacy [54,55,92]. Management should be individualized based on the patient’s acute presentation, with treatment guided by hemodynamic status, electrocardiographic findings, and the presence of pulmonary congestion, low-output states, or cardiogenic shock. Additionally, clinicians should consider thromboembolic risk and initiate prophylactic anticoagulation in patients with significant left ventricular dysfunction or pronounced apical ballooning.
Author Contributions
F.D.K. and B.V.R.; writing—original draft preparation, F.D.K. and B.V.R.; writing—review and editing, F.D.K. and B.V.R.; supervision – B.V.R; authors have read and agreed to the published version of the manuscript.
Acknowledgments
The authors would like to acknowledge Sai Nimmagadda, for feedback on the first draft of this publication and continued support.
Conflicts of Interest
None.
References
- Templin, C.; Ghadri, J.R.; Diekmann, J.; Napp, L.C.; Bataiosu, D.R.; Jaguszewski, M.; Cammann, V.L.; Sarcon, A.; Geyer, V.; Neumann, C.A.; et al. Clinical Features and Outcomes of Takotsubo (Stress) Cardiomyopathy. New England Journal of Medicine 2015, 373, 929–938. [Google Scholar] [CrossRef]
- Khalid, N.; Sareen, P.; Ahmad, S.A.; Chhabra, L. Takotsubo syndrome: The past, the present and the future. World J Cardiol 2019, 11, 213–216. [Google Scholar] [CrossRef] [PubMed]
- Kuo, B.T.; Choubey, R.; Novaro, G.M. Reduced estrogen in menopause may predispose women to takotsubo cardiomyopathy. Gender Medicine 2010, 7, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Movahed, M.R.; Javanmardi, E.; Hashemzadeh, M. High Mortality and Complications in Patients Admitted With Takotsubo Cardiomyopathy With More Than Double Mortality in Men Without Improvement in Outcome Over the Years. Journal of the American Heart Association 2025, 0, e037219. [Google Scholar] [CrossRef] [PubMed]
- Tsuchihashi, K.; Ueshima, K.; Uchida, T.; Oh-mura, N.; Kimura, K.; Owa, M.; Yoshiyama, M.; Miyazaki, S.; Haze, K.; Ogawa, H.; et al. Transient left ventricular apical ballooning without coronary artery stenosis: a novel heart syndrome mimicking acute myocardial infarction. Journal of the American College of Cardiology 2001, 38, 11–18. [Google Scholar] [CrossRef]
- Sato, H. Tako-tsubo-like left ventricular dysfunction due to multivessel coronary spasm. Clinical aspect of myocardial injury: from ischemia to heart failure 1990, 56–64. [Google Scholar]
- Dote, K.; Sato, H.; Tateishi, H.; Uchida, T.; Ishihara, M. [Myocardial stunning due to simultaneous multivessel coronary spasms: a review of 5 cases]. J Cardiol 1991, 21, 203–214. [Google Scholar]
- Wittstein, I.S.; Thiemann, D.R.; Lima, J.A.C.; Baughman, K.L.; Schulman, S.P.; Gerstenblith, G.; Wu, K.C.; Rade, J.J.; Bivalacqua, T.J.; Champion, H.C. Neurohumoral Features of Myocardial Stunning Due to Sudden Emotional Stress. New England Journal of Medicine 2005, 352, 539–548. [Google Scholar] [CrossRef]
- Goldstein, D.S.; Eisenhofer, G.; Kopin, I.J. Sources and significance of plasma levels of catechols and their metabolites in humans. J Pharmacol Exp Ther 2003, 305, 800–811. [Google Scholar] [CrossRef]
- Zulfaj, E.; Nejat, A.; Haamid, A.; Espinosa, A.; Elmahdy, A.; Pylova, T.; Jha, S.; Redfors, B.; Omerovic, E. Temperature and repeated catecholamine surges modulate regional wall motion abnormalities in a rodent takotsubo syndrome model. Scientific Reports 2025, 15. [Google Scholar] [CrossRef]
- Zulfaj, E.; Nejat, A.; Espinosa, A.S.; Hussain, S.; Haamid, A.; Soliman, A.E.; Kakaei, Y.; Jha, A.; Redfors, B.; Omerovic, E. Development of a small animal model replicating core characteristics of takotsubo syndrome in humans. European Heart Journal Open 2024, 4. [Google Scholar] [CrossRef]
- Redfors, B.; Ali, A.; Shao, Y.; Lundgren, J.; Gan, L.-M.; Omerovic, E. Different catecholamines induce different patterns of takotsubo-like cardiac dysfunction in an apparently afterload dependent manner. International Journal of Cardiology 2014, 174, 330–336. [Google Scholar] [CrossRef]
- Aw, A.; de Jong, M.C.; Varghese, S.; Lee, J.; Foo, R.; Parameswaran, R. A systematic cohort review of pheochromocytoma-induced typical versus atypical Takotsubo cardiomyopathy. International Journal of Cardiology 2023, 371, 287–292. [Google Scholar] [CrossRef]
- Kiamanesh, O.; Vu, E.N.; Webber, D.L.; Lau, E.; Kapeluto, J.E.; Stuart, H.; Wood, D.A.; Wong, G.C. Pheochromocytoma-Induced Takotsubo Syndrome Treated With Extracorporeal Membrane Oxygenation. JACC: Case Reports 2019, 1, 85–90. [Google Scholar] [CrossRef]
- Chiang, Y.L.; Chen, P.C.; Lee, C.C.; Chua, S.K. Adrenal pheochromocytoma presenting with Takotsubo-pattern cardiomyopathy and acute heart failure: A case report and literature review. Medicine (Baltimore) 2016, 95, e4846. [Google Scholar] [CrossRef]
- Sahar, T.; Khan, A.A.; Shabbir, R.W. Takotsubo syndrome with underlying pheochromocytoma. J Geriatr Cardiol 2021, 18, 1068–1070. [Google Scholar] [CrossRef] [PubMed]
- Ansari, U.; El-Battrawy, I.; Fastner, C.; Behnes, M.; Sattler, K.; Huseynov, A.; Baumann, S.; Tülümen, E.; Borggrefe, M.; Akin, I. Clinical outcomes associated with catecholamine use in patients diagnosed with Takotsubo cardiomyopathy. BMC Cardiovascular Disorders 2018, 18. [Google Scholar] [CrossRef] [PubMed]
- Terasaki, S.; Kanaoka, K.; Nakai, M.; Sumita, Y.; Onoue, K.; Soeda, T.; Watanabe, M.; Miyamoto, Y.; Saito, Y. Outcomes of catecholamine and/or mechanical support in Takotsubo syndrome. Heart 2022, 108, 1467–1473. [Google Scholar] [CrossRef] [PubMed]
- Dhalla, N.S. Formation of Aminochrome Leads to Cardiac Dysfunction and Sudden Cardiac Death. Circulation Research 2018, 123, 409–411. [Google Scholar] [CrossRef]
- Ganguly, P.K.; Dhalla, K.S.; Shao, Q.; Beamish, R.E.; Dhalla, N.S. Differential changes in sympathetic activity in left and right ventricles in congestive heart failure after myocardial infarction. Am Heart J 1997, 133, 340–345. [Google Scholar] [CrossRef]
- Ganguly, P. Oxidative Products of Catecholamines During Heightened Sympathetic Activity Due to Congestive Heart Failure: Possible Role of Antioxidants. International Journal of General Medicine 2024, 17, 919–923. [Google Scholar] [CrossRef] [PubMed]
- Krizanova, O.; Myslivecek, J.; Tillinger, A.; Jurkovicova, D.; Kubovcakova, L. Adrenergic and calcium modulation of the heart in stress: From molecular biology to function. Stress 2007, 10, 173–184. [Google Scholar] [CrossRef]
- Opie, L.H.; Walpoth, B.; Barsacchi, R. Calcium and catecholamines: relevance to cardiomyopathies and significance in therapeutic strategies. J Mol Cell Cardiol 1985, 17 Suppl 2, 21–34. [Google Scholar] [CrossRef]
- Strange, P.G. Signaling mechanisms of GPCR ligands. Curr Opin Drug Discov Devel 2008, 11, 196–202. [Google Scholar] [PubMed]
- Yang, B.; Wang, S.-Q.; Yang, H.-Q. β-adrenergic regulation of Ca<sup>2+</sup> signaling in heart cells. Biophysics Reports 2024, 10, 1. [Google Scholar] [CrossRef]
- Izem-Meziane, M.; Djerdjouri, B.; Rimbaud, S.; Caffin, F.; Fortin, D.; Garnier, A.; Veksler, V.; Joubert, F.; Ventura-Clapier, R. Catecholamine-induced cardiac mitochondrial dysfunction and mPTP opening: protective effect of curcumin. Am J Physiol Heart Circ Physiol 2012, 302, H665–674. [Google Scholar] [CrossRef]
- Abele, N.; Münz, F.; Zink, F.; Gröger, M.; Hoffmann, A.; Wolfschmitt, E.-M.; Hogg, M.; Calzia, E.; Waller, C.; Radermacher, P.; et al. Relation of Plasma Catecholamine Concentrations and Myocardial Mitochondrial Respiratory Activity in Anesthetized and Mechanically Ventilated, Cardiovascular Healthy Swine. International Journal of Molecular Sciences 2023, 24, 17293. [Google Scholar] [CrossRef]
- Pop, R.M.; Boarescu, P.-M.; Bocsan, C.I.; Gherman, M.L.; Chedea, V.S.; Jianu, E.-M.; Roșian, Ș.H.; Boarescu, I.; Ranga, F.; Tomoiagă, L.L.; et al. Anti-Inflammatory and Antioxidant Effects of White Grape Pomace Polyphenols on Isoproterenol-Induced Myocardial Infarction. International Journal of Molecular Sciences 2025, 26, 2035. [Google Scholar] [CrossRef]
- Mori, H.; Ishikawa, S.; Kojima, S.; Hayashi, J.; Watanabe, Y.; Hoffman, J.I.; Okino, H. Increased responsiveness of left ventricular apical myocardium to adrenergic stimuli. Cardiovasc Res 1993, 27, 192–198. [Google Scholar] [CrossRef]
- Paur, H.; Wright, P.T.; Sikkel, M.B.; Tranter, M.H.; Mansfield, C.; O’Gara, P.; Stuckey, D.J.; Nikolaev, V.O.; Diakonov, I.; Pannell, L.; et al. High Levels of Circulating Epinephrine Trigger Apical Cardiodepression in a β<sub>2</sub>-Adrenergic Receptor/G<sub>i</sub>–Dependent Manner. Circulation 2012, 126, 697–706. [Google Scholar] [CrossRef]
- Markousis-Mavrogenis, G.; Pepe, A.; Bacopoulou, F.; Lupi, A.; Quaia, E.; Chrousos, G.P.; Mavrogeni, S.I. Combined Brain–Heart Imaging in Takotsubo Syndrome: Towards a Holistic Patient Assessment. Journal of Clinical Medicine 2024, 13, 2991. [Google Scholar] [CrossRef]
- Suzuki, H.; Takanami, K.; Takase, K.; Shimokawa, H.; Yasuda, S. Reversible increase in stress-associated neurobiological activity in the acute phase of Takotsubo syndrome; a brain 18F-FDG-PET study. International Journal of Cardiology 2021, 344, 31–33. [Google Scholar] [CrossRef]
- Khan, H.; Gamble, D.T.; Rudd, A.; Mezincescu, A.M.; Abbas, H.; Noman, A.; Stewart, A.; Horgan, G.; Krishnadas, R.; Williams, C.; et al. Structural and Functional Brain Changes in Acute Takotsubo Syndrome. JACC: Heart Failure 2023, 11, 307–317. [Google Scholar] [CrossRef]
- Templin, C.; Hänggi, J.; Klein, C.; Topka, M.S.; Hiestand, T.; Levinson, R.A.; Jurisic, S.; Lüscher, T.F.; Ghadri, J.-R.; Jäncke, L. Altered limbic and autonomic processing supports brain-heart axis in Takotsubo syndrome. European Heart Journal 2019, 40, 1183–1187. [Google Scholar] [CrossRef]
- Silva, A.R.; Magalhães, R.; Arantes, C.; Moreira, P.S.; Rodrigues, M.; Marques, P.; Marques, J.; Sousa, N.; Pereira, V.H. Brain functional connectivity is altered in patients with Takotsubo Syndrome. Scientific Reports 2019, 9. [Google Scholar] [CrossRef] [PubMed]
- Kurisu, S.; Inoue, I.; Kawagoe, T.; Ishihara, M.; Shimatani, Y.; Nakama, Y.; Maruhashi, T.; Kagawa, E.; Dai, K.; Matsushita, J.; et al. Prevalence of incidental coronary artery disease in tako-tsubo cardiomyopathy. Coronary Artery Disease 2009, 20, 214–218. [Google Scholar] [CrossRef] [PubMed]
- Schneider, B.; Athanasiadis, A.; Schwab, J.; Pistner, W.; Gottwald, U.; Schoeller, R.; Toepel, W.; Winter, K.-D.; Stellbrink, C.; Müller-Honold, T.; et al. Complications in the clinical course of tako-tsubo cardiomyopathy. International Journal of Cardiology 2014, 176, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Honda, S.; Noguchi, M.; Sakai, C.; Harimoto, K.; Kawasaki, T. Takotsubo cardiomyopathy induced by acute coronary syndrome: A case report. J Cardiol Cases 2023, 28, 133–136. [Google Scholar] [CrossRef]
- Bossone, E.; Lyon, A.; Citro, R.; Athanasiadis, A.; Meimoun, P.; Parodi, G.; Cimarelli, S.; Omerovic, E.; Ferrara, F.; Limongelli, G.; et al. Takotsubo cardiomyopathy: an integrated multi-imaging approach. European Heart Journal - Cardiovascular Imaging 2013, 15, 366–377. [Google Scholar] [CrossRef]
- Ghadri, J.-R.; Wittstein, I.S.; Prasad, A.; Sharkey, S.; Dote, K.; Akashi, Y.J.; Cammann, V.L.; Crea, F.; Galiuto, L.; Desmet, W.; et al. International Expert Consensus Document on Takotsubo Syndrome (Part I): Clinical Characteristics, Diagnostic Criteria, and Pathophysiology. European Heart Journal 2018, 39, 2032–2046. [Google Scholar] [CrossRef]
- Stähli, B.E.; Schindler, M.; Schweiger, V.; Cammann, V.L.; Szawan, K.A.; Niederseer, D.; Würdinger, M.; Schönberger, A.; Schönberger, M.; Koleva, I.; et al. Cardiac troponin elevation and mortality in takotsubo syndrome: New insights from the international takotsubo registry. European Journal of Clinical Investigation 2024, 54. [Google Scholar] [CrossRef]
- Paraschiv, C.; Paduraru, L.; Balanescu, S. An Extensive Review on Imaging Diagnosis Methods in Takotsubo Syndrome. Reviews in Cardiovascular Medicine 2023, 24, 300. [Google Scholar] [CrossRef]
- Misumida, N.; Ogunbayo, G.O.; Kim, S.M.; Abdel-Latif, A.; Ziada, K.M.; Sorrell, V.L. Clinical Outcome of Takotsubo Cardiomyopathy Diagnosed With or Without Coronary Angiography. Angiology 2018, 70, 56–61. [Google Scholar] [CrossRef]
- Matsuo, S.; Nakajima, K.; Kinuya, S.; Yamagishi, M. Diagnostic utility of 123I-BMIPP imaging in patients with Takotsubo cardiomyopathy. Journal of Cardiology 2014, 64, 49–56. [Google Scholar] [CrossRef]
- Frangieh, A.H.; Obeid, S.; Ghadri, J.R.; Imori, Y.; D’Ascenzo, F.; Kovac, M.; Ruschitzka, F.; Lüscher, T.F.; Duru, F.; Templin, C.; et al. ECG Criteria to Differentiate Between Takotsubo (Stress) Cardiomyopathy and Myocardial Infarction. Journal of the American Heart Association 2016, 5, e003418. [Google Scholar] [CrossRef]
- Ghadri, J.-R.; Wittstein, I.S.; Prasad, A.; Sharkey, S.; Dote, K.; Akashi, Y.J.; Cammann, V.L.; Crea, F.; Galiuto, L.; Desmet, W.; et al. International Expert Consensus Document on Takotsubo Syndrome (Part II): Diagnostic Workup, Outcome, and Management. European Heart Journal 2018, 39, 2047–2062. [Google Scholar] [CrossRef] [PubMed]
- Eitel, I.; von Knobelsdorff-Brenkenhoff, F.; Bernhardt, P.; Carbone, I.; Muellerleile, K.; Aldrovandi, A.; Francone, M.; Desch, S.; Gutberlet, M.; Strohm, O.; et al. Clinical Characteristics and Cardiovascular Magnetic Resonance Findings in Stress (Takotsubo) Cardiomyopathy. JAMA 2011, 306. [Google Scholar] [CrossRef]
- Zghyer, F.; Botheju, W.S.P.; Kiss, J.E.; Michos, E.D.; Corretti, M.C.; Mukherjee, M.; Hays, A.G. Cardiovascular Imaging in Stress Cardiomyopathy (Takotsubo Syndrome). Frontiers in Cardiovascular Medicine 2022, 8. [Google Scholar] [CrossRef] [PubMed]
- Amicone, S.; Impellizzeri, A.; Tattilo, F.P.; Ryabenko, K.; Asta, C.; Belà, R.; Suma, N.; Canton, L.; Fedele, D.; Bertolini, D.; et al. Noninvasive Assessment in Takotsubo Syndrome: A Diagnostic Challenge. Echocardiography 2024, 41. [Google Scholar] [CrossRef]
- Nayar, J.; John, K.; Philip, A.; George, L.; George, A.; Lal, A.; Mishra, A. A Review of Nuclear Imaging in Takotsubo Cardiomyopathy. Life 2022, 12, 1476. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.L.; Horne, B.D.; Le, V.T.; Bair, T.L.; Min, D.B.; Minder, C.M.; Dhar, R.; Mason, S.; Muhlestein, J.B.; Knowlton, K.U. Spectrum of radionuclide perfusion study abnormalities in takotsubo cardiomyopathy. Journal of Nuclear Cardiology 2022, 29, 1034–1046. [Google Scholar] [CrossRef]
- Christensen, T.E.; Ahtarovski, K.A.; Bang, L.E.; Holmvang, L.; Søholm, H.; Ghotbi, A.A.; Andersson, H.; Vejlstrup, N.; Ihlemann, N.; Engstrøm, T.; et al. Basal hyperaemia is the primary abnormality of perfusion in Takotsubo cardiomyopathy: a quantitative cardiac perfusion positron emission tomography study. European Heart Journal – Cardiovascular Imaging 2015, 16, 1162–1169. [Google Scholar] [CrossRef]
- Kobylecka, M.; Budnik, M.; Kochanowski, J.; Piątkowski, R.; Wojtera, K.; Chojnowski, M.; Peller, M.; Fronczewska-Wieniawska, K.; Mazurek, T.; Mączewska, J.; et al. Diagnostic utility of hybrid single photon emission computed tomography/computed tomography imaging in patients with Takotsubo syndrome. Journal of Cardiovascular Medicine 2019, 20. [Google Scholar] [CrossRef]
- Fazio, G.; Pizzuto, C.; Barbaro, G.; Sutera, L.; Incalcaterra, E.; Evola, G.; Azzarelli, S.; Palecek, T.; Di Gesaro, G.; Cascio, C.; et al. Chronic pharmacological treatment in takotsubo cardiomyopathy. International Journal of Cardiology 2008, 127, 121–123. [Google Scholar] [CrossRef] [PubMed]
- Raposeiras-Roubin, S.; Santoro, F.; Arcari, L.; Vazirani, R.; Novo, G.; Uribarri, A.; Enrica, M.; Lopez-Pais, J.; Guerra, F.; Alfonso, F.; et al. Beta-Blockers and Long-Term Mortality in Takotsubo Syndrome: Results of the Multicenter GEIST Registry. JACC: Heart Failure 2025, 13, 815–825. [Google Scholar] [CrossRef] [PubMed]
- El Mahmoud, R.; Mansencal, N.; Pilliére, R.; Leyer, F.; Abbou, N.; Michaud, P.; Nallet, O.; Digne, F.; Lacombe, P.; Cattan, S.; et al. Prevalence and characteristics of left ventricular outflow tract obstruction in Tako-Tsubo syndrome. American Heart Journal 2008, 156, 543–548. [Google Scholar] [CrossRef]
- Yoshioka, T.; Hashimoto, A.; Tsuchihashi, K.; Nagao, K.; Kyuma, M.; Ooiwa, H.; Nozawa, A.; Shimoshige, S.; Eguchi, M.; Wakabayashi, T.; et al. Clinical implications of midventricular obstruction and intravenous propranolol use in transient left ventricular apical ballooning (Tako-tsubo cardiomyopathy). American Heart Journal 2008, 155, 526.e521–526.e527. [Google Scholar] [CrossRef] [PubMed]
- Santoro, F.; Ieva, R.; Ferraretti, A.; Fanelli, M.; Musaico, F.; Tarantino, N.; Martino, L.D.; Gennaro, L.D.; Caldarola, P.; Biase, M.D.; et al. Hemodynamic Effects, Safety, and Feasibility of Intravenous Esmolol Infusion During Takotsubo Cardiomyopathy With Left Ventricular Outflow Tract Obstruction: Results From A Multicenter Registry. Cardiovascular Therapeutics 2016, 34, 161–166. [Google Scholar] [CrossRef]
- Santoro, F.; Stiermaier, T.; Tarantino, N.; De Gennaro, L.; Moeller, C.; Guastafierro, F.; Marchetti, M.F.; Montisci, R.; Carapelle, E.; Graf, T.; et al. Left Ventricular Thrombi in Takotsubo Syndrome: Incidence, Predictors, and Management: Results From the GEIST (German Italian Stress Cardiomyopathy) Registry. Journal of the American Heart Association 2017, 6. [Google Scholar] [CrossRef]
- Kumar, S.; Kaushik, S.; Nautiyal, A.; Choudhary, S.K.; Kayastha, B.L.; Mostow, N.; Lazar, J.M. Cardiac Rupture in Takotsubo Cardiomyopathy: A Systematic Review. Clinical Cardiology 2011, 34, 672–676. [Google Scholar] [CrossRef]
- Lyon, A.R.; Bossone, E.; Schneider, B.; Sechtem, U.; Citro, R.; Underwood, S.R.; Sheppard, M.N.; Figtree, G.A.; Parodi, G.; Akashi, Y.J.; et al. Current state of knowledge on Takotsubo syndrome: a Position Statement from the Taskforce on Takotsubo Syndrome of the Heart Failure Association of the European Society of Cardiology. European Journal of Heart Failure 2016, 18, 8–27. [Google Scholar] [CrossRef]
- Bouabdallaoui, N.; Wang, Z.; Lecomte, M.; Ennezat, P.V.; Blanchard, D. Acute mitral regurgitation in Takotsubo cardiomyopathy. European Heart Journal: Acute Cardiovascular Care 2015, 4, 197–199. [Google Scholar] [CrossRef]
- Citro, R.; Rigo, F.; D’Andrea, A.; Ciampi, Q.; Parodi, G.; Provenza, G.; Piccolo, R.; Mirra, M.; Zito, C.; Giudice, R.; et al. Echocardiographic Correlates of Acute Heart Failure, Cardiogenic Shock, and In-Hospital Mortality in Tako-Tsubo Cardiomyopathy. JACC: Cardiovascular Imaging 2014, 7, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, H.; Akiba, H.; Inagawa, H.; Okada, Y. Isolated right ventricular takotsubo cardiomyopathy presenting as acute right ventricular failure: A case report. Heliyon 2023, 9, e17607. [Google Scholar] [CrossRef]
- Kagiyama, N.; Okura, H.; Tamada, T.; Imai, K.; Yamada, R.; Kume, T.; Hayashida, A.; Neishi, Y.; Kawamoto, T.; Yoshida, K. Impact of right ventricular involvement on the prognosis of takotsubo cardiomyopathy. European Heart Journal – Cardiovascular Imaging 2016, 17, 210–216. [Google Scholar] [CrossRef]
- El-Battrawy, I.; Santoro, F.; Stiermaier, T.; Möller, C.; Guastafierro, F.; Novo, G.; Novo, S.; Mariano, E.; Romeo, F.; Romeo, F.; et al. Incidence and Clinical Impact of Right Ventricular Involvement (Biventricular Ballooning) in Takotsubo Syndrome: Results From the GEIST Registry. Chest 2021, 160, 1433–1441. [Google Scholar] [CrossRef]
- Kurisu, S.; Inoue, I.; Kawagoe, T.; Ishihara, M.; Shimatani, Y.; Nakama, Y.; Maruhashi, T.; Kagawa, E.; Dai, K. Incidence and treatment of left ventricular apical thrombosis in Tako-tsubo cardiomyopathy. International Journal of Cardiology 2011, 146, e58–e60. [Google Scholar] [CrossRef] [PubMed]
- Levine, G.N.; Mcevoy, J.W.; Fang, J.C.; Ibeh, C.; Mccarthy, C.P.; Misra, A.; Shah, Z.I.; Shenoy, C.; Spinler, S.A.; Vallurupalli, S.; et al. Management of Patients at Risk for and With Left Ventricular Thrombus: A Scientific Statement From the American Heart Association. Circulation 2022, 146. [Google Scholar] [CrossRef] [PubMed]
- Isogai, T.; Matsui, H.; Tanaka, H.; Makito, K.; Fushimi, K.; Yasunaga, H. Incidence, management, and prognostic impact of arrhythmias in patients with Takotsubo syndrome: a nationwide retrospective cohort study. European Heart Journal: Acute Cardiovascular Care 2023, 12, 834–846. [Google Scholar] [CrossRef]
- Pant, S.; Deshmukh, A.; Mehta, K.; Badheka, A.O.; Tuliani, T.; Patel, N.J.; Dabhadkar, K.; Prasad, A.; Paydak, H. Burden of arrhythmias in patients with Takotsubo Cardiomyopathy (Apical Ballooning Syndrome). International Journal of Cardiology 2013, 170, 64–68. [Google Scholar] [CrossRef]
- El-Battrawy, I.; Lang, S.; Ansari, U.; Tülümen, E.; Schramm, K.; Fastner, C.; Zhou, X.; Hoffmann, U.; Borggrefe, M.; Akin, I. Prevalence of malignant arrhythmia and sudden cardiac death in takotsubo syndrome and its management. EP Europace 2018, 20, 843–850. [Google Scholar] [CrossRef]
- Brown, K.H.; Trohman, R.G.; Madias, C. Arrhythmias in Takotsubo cardiomyopathy. Cardiac Electrophysiology Clinics 2015, 7. [Google Scholar] [CrossRef]
- Stiermaier, T.; Rommel, K.-P.; Eitel, C.; Möller, C.; Graf, T.; Desch, S.; Thiele, H.; Eitel, I. Management of arrhythmias in patients with Takotsubo cardiomyopathy: Is the implantation of permanent devices necessary? Heart Rhythm 2016, 13. [Google Scholar] [CrossRef]
- Jaguszewski, M.; Fijalkowski, M.; Nowak, R.; Czapiewski, P.; Ghadri, J.-R.; Templin, C.; Rynkiewicz, A. Ventricular rupture in Takotsubo cardiomyopathy. European Heart Journal 2012, 33, 1027–1027. [Google Scholar] [CrossRef]
- Iskander, M.; Abugroun, A.; Shehata, K.; Iskander, F.; Iskander, A. Takotsubo Cardiomyopathy-Induced Cardiac Free Wall Rupture: A Case Report and Review of Literature. Cardiology Research 2018, 9, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Uribarri, A.; Núñez-Gil, I.J.; Conty, D.A.; Vedia, O.; Almendro-Delia, M.; Duran Cambra, A.; Martin-Garcia, A.C.; Barrionuevo-Sánchez, M.; Martínez-Sellés, M.; Raposeiras-Roubín, S.; et al. Short- and Long-Term Prognosis of Patients With Takotsubo Syndrome Based on Different Triggers: Importance of the Physical Nature. J Am Heart Assoc 2019, 8, e013701. [Google Scholar] [CrossRef] [PubMed]
- Hurst, R.T.; Askew, J.W.; Reuss, C.S.; Lee, R.W.; Sweeney, J.P.; Fortuin, F.D.; Oh, J.K.; Tajik, A.J. Transient Midventricular Ballooning Syndrome: A New Variant. Journal of the American College of Cardiology 2006, 48, 579–583. [Google Scholar] [CrossRef]
- Ramaraj, R.; Movahed, M.R. Reverse or Inverted Takotsubo Cardiomyopathy (Reverse Left Ventricular Apical Ballooning Syndrome) Presents at a Younger Age Compared With the Mid or Apical Variant and Is Always Associated With Triggering Stress. Congestive Heart Failure 2010, 16, 284–286. [Google Scholar] [CrossRef]
- Awad, H.H.; McNeal, A.R.; Goyal, H. Reverse Takotsubo cardiomyopathy: a comprehensive review. Ann Transl Med 2018, 6, 460. [Google Scholar] [CrossRef] [PubMed]
- Citro, R.; Rigo, F.; Previtali, M.; Ciampi, Q.; Canterin, F.A.; Provenza, G.; Giudice, R.; Patella, M.M.; Vriz, O.; Mehta, R.; et al. Differences in Clinical Features and In-Hospital Outcomes of Older Adults with Tako-Tsubo Cardiomyopathy. Journal of the American Geriatrics Society 2012, 60, 93–98. [Google Scholar] [CrossRef]
- Brinjikji, W.; El-Sayed, A.M.; Salka, S. In-hospital mortality among patients with takotsubo cardiomyopathy: A study of the National Inpatient Sample 2008 to 2009. American Heart Journal 2012, 164, 215–221. [Google Scholar] [CrossRef]
- Eslami, V.; Nazari, R.; Senobari, N.; Alirezaei, A.; Akbari, T.; Nasrollahizadeh, A.; Ebrahimi, P.; Ahmed, R.; Khan, S.Q.; Shahid, F. Stress-Induced Cardiomyopathy Following Kidney Transplant. JACC: Case Reports 2025, 30, 103863. [Google Scholar] [CrossRef]
- Abusnina, W.; Elhouderi, E.; Walters, R.W.; Al-Abdouh, A.; Mostafa, M.R.; Liu, J.L.; Mazozy, R.; Mhanna, M.; Ben-Dor, I.; Dufani, J.; et al. Sex Differences in the Clinical Outcomes of Patients With Takotsubo Stress Cardiomyopathy: A Meta-Analysis of Observational Studies. The American Journal of Cardiology 2024, 211, 316–325. [Google Scholar] [CrossRef]
- Li, P.; Wang, Y.; Liang, J.; Zuo, X.; Li, Q.; Sherif, A.A.; Zhang, J.; Xu, Y.; Huang, Z.; Dong, M.; et al. Takotsubo syndrome and respiratory diseases: a systematic review. European Heart Journal Open 2022, 2. [Google Scholar] [CrossRef]
- Núñez-Gil, I.J.; Almendro-Delia, M.; Andrés, M.; Sionis, A.; Martin, A.; Bastante, T.; Córdoba-Soriano, J.G.; Linares, J.A.; González Sucarrats, S.; Sánchez-Grande-Flecha, A.; et al. Secondary forms of Takotsubo cardiomyopathy: A whole different prognosis. European Heart Journal: Acute Cardiovascular Care 2016, 5, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Rudd, A.E.; Horgan, G.W.; McGowan, J.; Sood, A.; McGeoch, R.; Irving, J.; Watt, J.; Leslie, S.J.; Petrie, M.C.; Lang, C.C.; et al. Morbidity After Takotsubo Syndrome: A Report From the Scottish Takotsubo Registry. Annals of Internal Medicine 2025, 178, 754–757. [Google Scholar] [CrossRef] [PubMed]
- Looi, J.-L.; Easton, A.; Webster, M.; To, A.; Lee, M.; Kerr, A.J. Recurrent Takotsubo Syndrome: How Frequent, and How Does It Present? Heart, Lung and Circulation 2024, 33, 1117–1122. [Google Scholar] [CrossRef] [PubMed]
- Saito, Y.; Watanabe, T.; Ishigaki, T.; Toyoshima, M.; Katawaki, W.; Toshima, T.; Takahashi, T.; Yamanaka, T.; Watanabe, M. Recurrent Takotsubo Syndrome Presenting with Different Ballooning Patterns and Electrocardiographic Abnormalities. Internal Medicine 2023, 62, 2977–2980. [Google Scholar] [CrossRef]
- El-Battrawy, I.; Santoro, F.; Stiermaier, T.; Möller, C.; Guastafierro, F.; Novo, G.; Novo, S.; Mariano, E.; Romeo, F.; Romeo, F.; et al. Incidence and Clinical Impact of Recurrent Takotsubo Syndrome: Results From the GEIST Registry. Journal of the American Heart Association 2019, 8. [Google Scholar] [CrossRef]
- Singh, K.; Carson, K.; Usmani, Z.; Sawhney, G.; Shah, R.; Horowitz, J. Systematic review and meta-analysis of incidence and correlates of recurrence of takotsubo cardiomyopathy. International Journal of Cardiology 2014, 174, 696–701. [Google Scholar] [CrossRef]
- Ghadri, J.R.; Jaguszewski, M.; Corti, R.; Lüscher, T.F.; Templin, C. Different wall motion patterns of three consecutive episodes of takotsubo cardiomyopathy in the same patient. International Journal of Cardiology 2012, 160, e25–e27. [Google Scholar] [CrossRef] [PubMed]
- Raposeiras-Roubín, S.; Núñez-Gil, I.J.; Jamhour, K.; Abu-Assi, E.; Conty, D.A.; Vedia, O.; Almendro-Delia, M.; Sionis, A.; Martin-Garcia, A.C.; Corbí-Pascual, M.; et al. Long-term prognostic impact of beta-blockers in patients with Takotsubo syndrome: Results from the RETAKO Registry. Revista Portuguesa de Cardiologia 2023, 42, 237–246. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Clinical Approach to the Diagnosis of Takotsubo Cardiomyopathy. Abbreviations: ACS: acute coronary syndrome, CAD: coronary artery disease, CCTA: coronary computer tomography angiography, cMRI: cardiac magnetic resonance imaging, EKG: electrocardiogram, GRACE: global registry of acute coronary events, LGE: late gadolinium enhancement, LVOTO: left ventricular outflow tract obstruction, RV: right ventricle, TCM: takotsubo cardiomyopathy, TIMI: thrombolysis in myocardial infarction, TTE: transthoracic echocardiogram.
Figure 1.
Clinical Approach to the Diagnosis of Takotsubo Cardiomyopathy. Abbreviations: ACS: acute coronary syndrome, CAD: coronary artery disease, CCTA: coronary computer tomography angiography, cMRI: cardiac magnetic resonance imaging, EKG: electrocardiogram, GRACE: global registry of acute coronary events, LGE: late gadolinium enhancement, LVOTO: left ventricular outflow tract obstruction, RV: right ventricle, TCM: takotsubo cardiomyopathy, TIMI: thrombolysis in myocardial infarction, TTE: transthoracic echocardiogram.
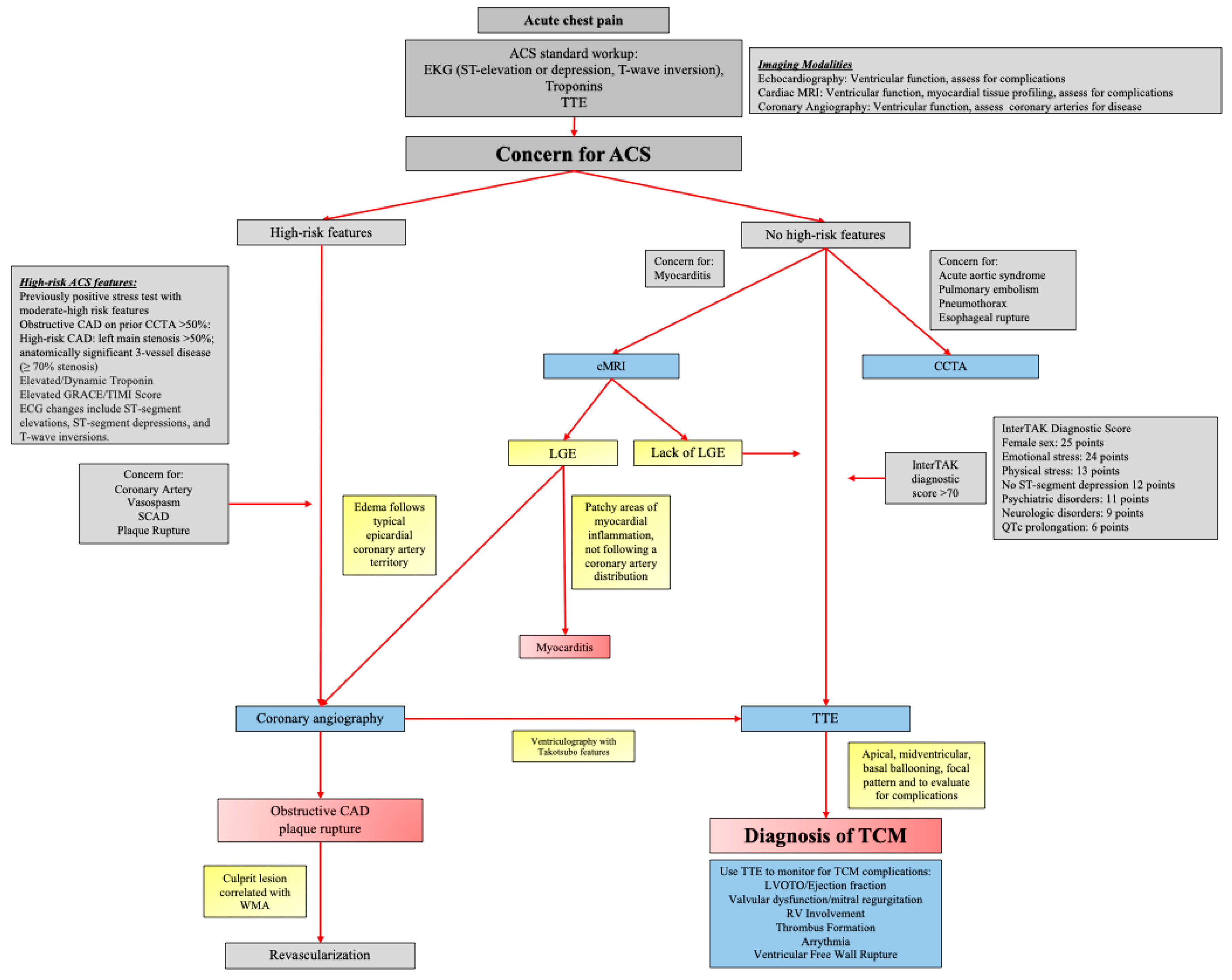
Figure 2.
Structural Variants of Takotsubo Cardiomyopathy: Apical, Midventricular, Basal, and Focal Patterns.
Figure 2.
Structural Variants of Takotsubo Cardiomyopathy: Apical, Midventricular, Basal, and Focal Patterns.
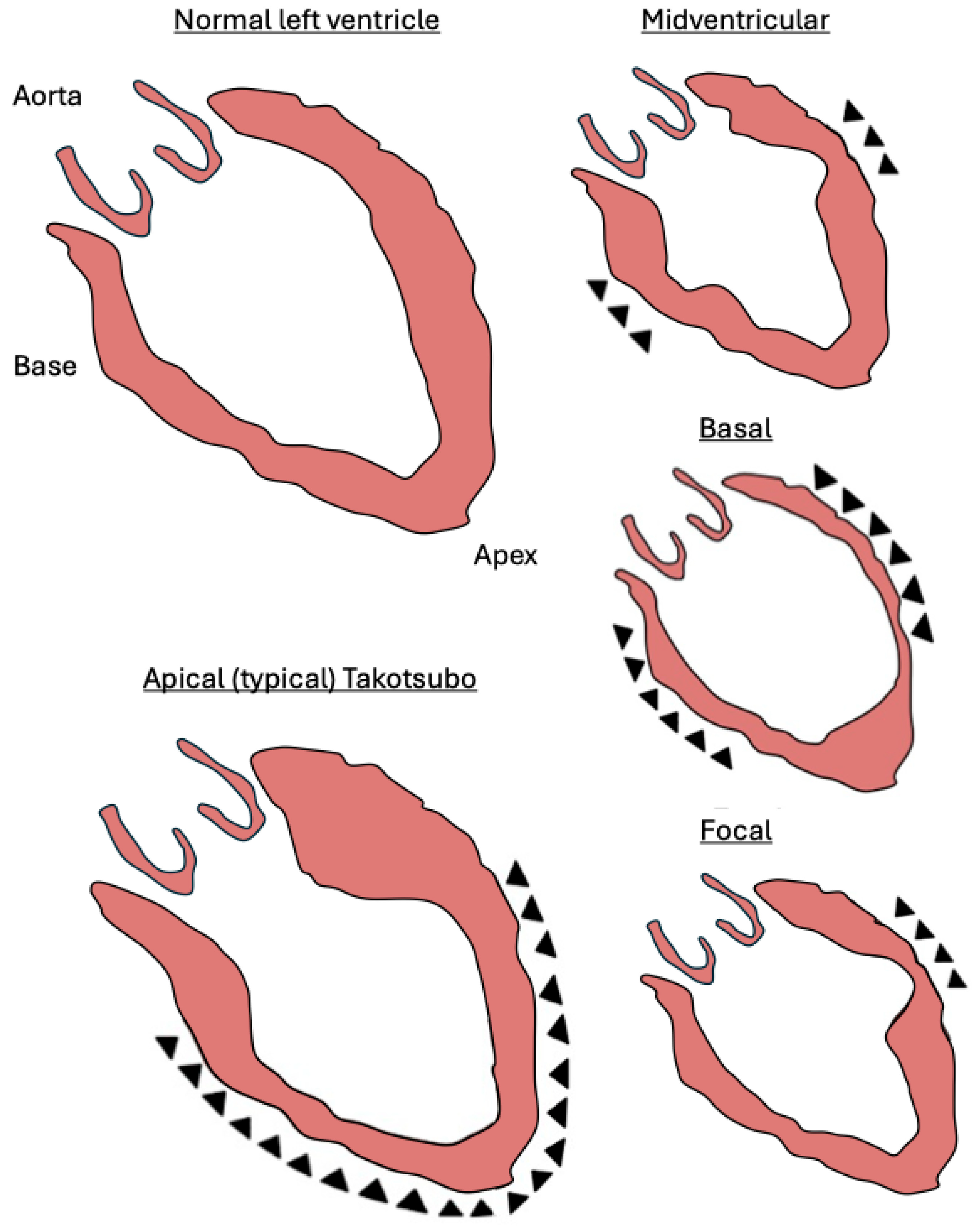

Table 1.
Frequency, diagnosis, timing, presentation, and management of complications associated with Takotsubo cardiomyopathy. Abbreviations: AFib: atrial fibrillation, CXR: chest x-ray, EKG: electrocardiogram, ICD: implantable cardioverter-defibrillator, LV: left ventricle, LVOTO: left ventricular outflow tract obstruction, MR: mitral regurgitation, MRI: magnetic resonance imaging, RV: right ventricle, SCA: sudden cardiac arrest, VF: ventricular fibrillation, VT: ventricular tachycardia.
Table 1.
Frequency, diagnosis, timing, presentation, and management of complications associated with Takotsubo cardiomyopathy. Abbreviations: AFib: atrial fibrillation, CXR: chest x-ray, EKG: electrocardiogram, ICD: implantable cardioverter-defibrillator, LV: left ventricle, LVOTO: left ventricular outflow tract obstruction, MR: mitral regurgitation, MRI: magnetic resonance imaging, RV: right ventricle, SCA: sudden cardiac arrest, VF: ventricular fibrillation, VT: ventricular tachycardia.
| Complication | Frequency | Diagnostic Clues | Onset Timing | Clinical Presentation | Management |
|---|---|---|---|---|---|
| Acute Heart failure | 12-45% | CXR, echo, clinical exam | Acute | Dyspnea, pulmonary edema | Diuretics, oxygen, supportive therapy |
| LVOTO | 10-25% | Echo, hypotension, low cardiac output | Acute | Hypotension. systolic murmur | Inotropes, vasopressors, mechanical support if needed |
| Cardiogenic Shock | 6-20% | Echo with Doppler, hypotension | Acute | Hypotension, systolic murmur, poor perfusion | Beta-blockers, avoid inotropes, |
| Valvular Dysfunction | 19-25% | Echo (MR), auscultation | Acute | Dyspnea, murmur | Afterload reduction, manage MR supportively |
| RV Involvement | 11-34% | Echo, RV dilation or dysfunction | Acute | Hypotension, right-sided heart failure signs | Supportive care, monitor RV function |
| LV Thrombus | 1.3–8% | Echo, cardiac MRI | Subacute | Stroke or embolic signs | Anticoagulation, imaging surveillance |
| Arrhythmias: VT, VF and SCA, atrial fibrillation, bradyarrhythmias | AFib: 5-15% VT/VFs:4-9% Bradyarrhythmias: 2-5% |
EKG, telemetry | Acute | Palpitations, syncope, arrest | Rate/rhythm control, defibrillation if unstable, ICD in certain patients |
| Ventricular Free Wall Rupture | <1% | Echo, pericardial effusion | Acute | Sudden cardiovascular collapse, tamponade | Emergency pericardiocentesis, surgery |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



