
Submitted:
12 November 2025
Posted:
13 November 2025
You are already at the latest version
Abstract
The central venous catheter (CVC) is essential in the management of pediatric patients, allowing the administration of medications, parenteral nutrition, and other treatments. However, its use carries a high risk of central line-associated bloodstream infections (CLABSI) and catheter-related bloodstream infections (CRBSI). Advanced chlorhexidine-impregnated dressings have been developed to reduce bacterial colonization, but their effectiveness in the pediatric population remains uncertain. The aim of this review is to evaluate the effectiveness of chlorhexidine-impregnated dressings compared to standard dressings in reducing CLABSI, CRBSI, and CVC colonization in pediatric patients. Randomized clinical trials published between 2005 and 2021 in PubMed, CINAHL, and Embase, in Italian or English, were selected. Methodological quality was assessed using the Joanna Briggs Institute (JBI) checklist. Relevant data were extracted and summarized in tables. Four studies, including a total of 733 pediatric patients (367 intervention, 366 control), were included. None reported a statistically significant reduction in CLABSI/CRBSI with the use of chlorhexidine-impregnated dressings. However, two studies showed a significant reduction in catheter colonization in the intervention group. Current evidence does not support a superior effect of chlorhexidine-impregnated dressings in preventing CLABSI/CRBSI in pediatric patients, although they may reduce catheter colonization. Randomized trials with larger samples and specific methodologies are needed to clarify the true clinical impact.
Keywords:
central venous catheter
; pediatric patients
; CLABSI/CRBSI
; chlorhexidine
; dressings
1. Introduction
The central venous catheter (CVC) is a device inserted into a large central vein, such as the internal jugular, subclavian, or femoral vein, and positioned so that the distal tip reaches the inferior vena cava, the superior vena cava, or the right atrium [1].
Venous access, essential in both diagnostic and therapeutic settings, allows the safe administration of high-osmolarity drugs, chemotherapeutic agents, antibiotics, analgesics, and other irritant medications, reducing the risk of phlebitis; at the same time, it facilitates total parenteral nutrition (TPN), transfusions, continuous infusions, and the collection and infusion of peripheral stem cells, also helping to decrease the patient’s stress caused by repeated venipunctures [2].
These devices are classified according to several factors:
- duration (short-term or long-term);
- insertion site (subclavian, femoral, jugular, basilic, brachial, cephalic);
- number of lumens (single, double, or triple);
- tip characteristics (open or closed);
- materials used to reduce complications (such as heparin, antibiotic, or silver impregnation) [3];
Furthermore, CVCs are divided into two main categories: tunneled and non-tunneled. Tunneling is a CVC placement technique in which part of the catheter is passed under the skin, creating a subcutaneous tunnel between the venous insertion site and the skin exit site [3]. The tunneling of these devices was introduced to reduce the risk of infectious and mechanical complications. These catheters are particularly suitable for long-term care, that is, for treatment periods requiring venous access maintenance for more than 3 months [2]. In contrast, non-tunneled devices are usually inserted for a short to medium term (from 2–4 weeks to 1–3 months) [4].
Peripherally inserted central catheters (PICC) are introduced through the veins of the upper limbs (usually basilic, brachial, or cephalic), with the tip reaching the cavoatrial junction, passing through the axillary and subclavian veins [5].
Conversely, port-a-caths are central venous catheters completely implanted in the subcutaneous tissue, generally on the anterior chest wall, below the clavicle, and consist of an infusion chamber (port) connected to a catheter. This type of CVC preserves the patient’s body image, and access to this device occurs through a skin puncture with a specific needle (Huber needle) [6].
Obtaining venous access that remains in place for a long time can be particularly difficult, for example, in the pediatric population, due to the anatomy of the veins and the difficulty in palpating them, as well as in patients undergoing prolonged therapies. Even in critical situations, venous access can quickly become difficult. For this reason, having a previously implanted CVC can make the difference, especially when time is a determining factor [7].
The most commonly used device in pediatric intensive care units (PICU) is the CVC. A 2023 study that analyzed CVC insertion data showed that in a pediatric intensive care unit from 2015 to 2020, out of 1200 catheters, 885 of them were CVCs. Of these, 59.5% (526 out of 885 catheters) were inserted in the right internal jugular vein; the remaining part consisted of hemodialysis catheters, which represented 35.6% (315 out of 885 catheters). The average duration of catheter use was 12.22 ± 7.28 days (range 1–41 days) [8].
The most common indications for CVC insertion in pediatric patients identified by this study were: infusion of multiple drugs (28.4%, 341 out of 1200 catheters), extracorporeal treatment (25.4%, 305 out of 1200 catheters), difficult vascular access (25.3%, 304 out of 1200 catheters), bone marrow transplantation (11.3%, 135 out of 1200 catheters), hemodynamic monitoring (5.5%, 66 out of 1200 catheters), total parenteral nutrition (2.3%, 27 out of 1200 catheters) [8].
Central venous catheters were developed around the 1950s and 1960s. Over time, the insertion technique was refined, while aspects related to dressing management received less in-depth attention. The use of central venous catheters (CVCs) spread rapidly as they proved to be an important innovation for the management of many types of patients: critical, oncological, and those requiring long-term therapy. In the early 1960s, attention was mainly focused on the insertion technique and the maintenance of device patency, while care of the insertion site was often neglected or handled superficially. Over time, however, the emergence of infectious complications, particularly CRBSI, prompted the scientific and clinical community to re-evaluate the importance of dressings and insertion site management. It became clear that infection prevention cannot occur without careful and systematic care of the venous access area. The first dressings used were simple, consisting of sterile bandages or gauze, with the purpose of protecting the insertion site. In the 1990s, advanced dressings were introduced, using a transparent film that made the device’s skin insertion site visible without the need to change the dressing. These “new” dressings also allowed for greater adhesiveness and less frequent replacement [9].
Around the 2000s, with the publication of more structured guidelines and protocols for CVC dressing, dressings impregnated with povidone-iodine and/or silver were introduced. From 2010 onward, new-generation dressings were developed, such as those impregnated with chlorhexidine, designed to provide additional antimicrobial protection, help prevent catheter-related infections, reduce bacterial colonization on the skin, and prevent the proliferation of microorganisms [10,11].
Chlorhexidine is a broad-spectrum antiseptic disinfectant used for skin disinfection, effective against a wide range of organisms, including some resistant to antimicrobials [12].
There are several types of chlorhexidine-impregnated dressings, among which the most commonly used are 3M Tegaderm CHG and Biopatch.
The 3M Tegaderm CHG dressing consists of a thin transparent polyurethane film, within which is integrated a transparent gel pad containing 2% chlorhexidine gluconate. The main advantages of this device are the barrier function of the film against external contamination and the antiseptic action of the integrated gel, which acts directly on the skin [13].
Biopatch, on the other hand, is an antimicrobial dressing made of hydrophilic polyurethane foam containing slow-release chlorhexidine gluconate, active for up to 7 days. It has a central slit that facilitates application around the catheter. The absorbent foam not only releases CHG but can also absorb up to 8–10 times its own weight. The use of Biopatch is indicated for the reduction of local infections, central line-associated bloodstream infections (CLABSI), skin colonization, and catheter-related bloodstream infections (CRBSI) in patients with CVCs or arterial catheters. Biopatch remains in contact with the skin and continuously releases chlorhexidine gluconate for 7 days around the catheter insertion site [14].
The frequency of replacement for chlorhexidine-impregnated dressings is seven days or as needed, similar to what is expected for standard dressings [15].
The effectiveness of this dressing in the adult population has been widely tested, with positive outcomes, while in the case of the pediatric population, its use remains controversial and debated due to the limited number of studies conducted exclusively on this target.
Although central vascular access is considered safe and reliable, and dressings are constantly improving, these devices are still associated with bloodstream infections, such as central line-associated bloodstream infections (CLABSI) and catheter-related bloodstream infections (CRBSI) [16], with a CLABSI rate in pediatric hospitals that was 0.924 in 2016, 0.687 in 2019, and 0.808 in 2022 [17].
A higher incidence of CLABSI leads to an increase in antibiotic use, hospital length of stay (which is extended by about 9 days), mortality, and healthcare costs [18].
To address the problem of CLABSI, care bundles have been developed over the years that include several actions for correct catheter management. These actions include skin antisepsis with 2% chlorhexidine, the adoption of barrier precautions, ultrasound-guided venipuncture, catheter tunneling, application of glue at the exit site, sutureless fixation, use of transparent dressings, application of chlorhexidine sponge dressings after 7 days, and the use of needle-free neutral displacement connectors. The adoption of these bundles has led to a significant reduction in the CLABSI rate, which decreased from 15 per 1000 catheter days to 1.5 per 1000 catheter days (p < 0.05), thus contributing to improved patient safety [19].
Starting from these premises, the research question of this review arises, aiming to investigate whether the exclusive use of chlorhexidine dressings, compared to care bundles already established and known for their effectiveness, can reduce the rate of CLABSI and CRBSI in pediatric patients with CVCs.
In the literature, there is a meta-analysis [20] that mainly highlights the effectiveness of chlorhexidine dressings in the adult population; only a minority of the included studies (3 out of 12) focus on effectiveness in the pediatric population. Moreover, the results concerning the effectiveness of chlorhexidine dressings are not consistent across the examined articles.
Therefore, this study focuses exclusively on reviewing the literature regarding the use of chlorhexidine-based dressings in the pediatric population with central venous catheters (CVCs), comparing them with standard dressings in reducing the rate of CLABSI and CRBSI and in preventing catheter colonization, also integrating more recent research to update and expand the available knowledge on the subject.
2. Materials and Methods
2.1. Inclusion Criteria
The studies included in this review met the following criteria: published between 2000 and 2025, in Italian or English, conducted on pediatric patients (<18 years), retrieved from specific databases such as PubMed, CINAHL, and Embase, and addressing the comparison between the use of standard dressings and chlorhexidine-impregnated dressings in relation to the rate of CLABSI, CRBSI, and catheter colonization.
2.2. Exclusion Criteria
The studies excluded from this review met the following criteria: published before 2000, written in languages other than Italian or English, conducted on adult patients (>18 years), not relevant to the research question or not available in full text, and not comparing chlorhexidine-impregnated dressings with standard dressings.

| Inclusion criteria | Exclusion criteria |
|---|---|
|
|
2.3. Research Question
For each database, a search string was formulated and launched based on the following PIO framework. (Table 2):
2.4. Search Strategy
The search was conducted in the EMBASE, MEDLINE, and CINAHL databases on January 14, 2025.
All terms were combined using the Boolean operators “AND” and “OR”.
Some terms were searched using “MESH” terminology, while others were searched as free terms.
Keywords: Central venous catheter, Central intravenous catheter, Short-term central venous catheter, Central venous catheterization, Chlorhexidine, Chlorhexidine dressing, Catheter related bloodstream infection (CRBSI), Central line associated bloodstream infection (CLABSI), child, adolescent, infant, newborn, preschool. (Table 3)
2.5. Time Limits
Studies published from 2000 to 2025
3. Results
3.1. Study Selection
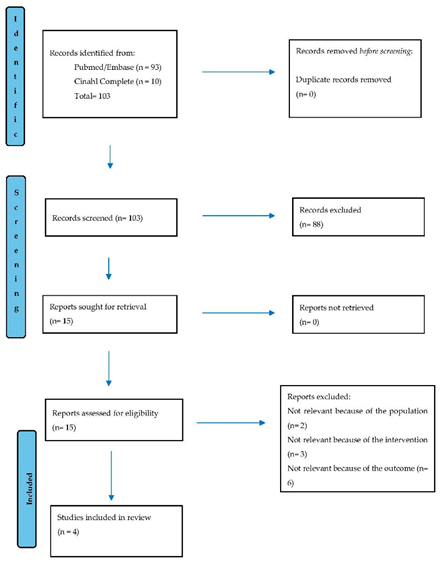
From the database search, 103 bibliographic references were identified, distributed as follows: 11 in Medline, 28 in Embase, 10 in CINAHL, and 54 in Embase/Medline. After reading the titles and abstracts, 88 references were excluded. Subsequently, 15 full-text articles were assessed, distributed as follows: 1 in Medline, 2 in CINAHL, 1 in Embase, and 11 in Embase/Medline. After reviewing the full-texts, a further selection was made, excluding 11 studies due to a lack of relevance to the study objective. Therefore, 4 full-text articles were included. (Table 4)
Table 5.
synoptic table.
|
First Author, Country, Year |
Study Design | Population | Number of Participants | Type of Catheter | Clinical Indication for CVC Insertion | Intervention with Chlorhexidine-Impregnated Dressing | Comparison | Definition of CLABSI/ CRBSI (i) | Definition of Catheter Colonization (ii) | Follow-up | Contraindications | Results |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Muhterem Duyu, Turkey, 2021 | Parallel-group RCT | Pediatric patients admitted to the PICU with a CVC >48h.. Main pathology : Respiratory failure. |
Intervention group Patients 151 M: 57,6 % F: 42,4 % Range:0-18. Control group Patients:156 M: 55,1 % F : 44,9 % Range:0-18. Mean age: 2 years | Non-tunneled short-term CVC | Administration of heparin and antibiotics | Chlorhexidine dressing: Applied 24h after catheterization, changed every 7 days or as needed | Transparent or standard breathable hypoallergenic dressing. | Bacteremia/fungemia with >1 positive blood culture from a peripheral vein, clinical manifestations of infection, and positive semiquantitative (>15CFU/segment) or quantitative (>10^3 CFU/segment) culture of catheter segment. | 15 CFU from catheter tip culture, without clinical signs of infection and without the same microorganism in blood samples, or when the microorganism isolated from blood differs from that on the catheter tip. | 1 year and 7 months | Contact dermatitis : (p = 0,346) Intervention group (7,2%) Control group (4,4%) |
CLABSI/CRBSI (i) : No statistically significant difference between intervention group and control group (9,9% vs 12,8%; p = 0,767). Catheter Colonization (ii) : Chlorhexidine dressing significantly reduces the incidence of catheter colonization (5,9% vs 12,8%; p = 0,041). |
| Nattapong Jintrungruengnij, Thailand, 2020 |
Parallel-group RCT | Patients with CVC or PICC >48h.. Main pathology : Heart disease |
Intervention group. Patients : 92 M: 51 % F: 49 % Range: 0-18 Control group: Patients : 89 M: 66 % F: 34 % Range: 0-18 Mean age: 2,3 years |
Short-term CVC or PICC | Intravenous therapy. | Chlorhexidine dressing: Applied within 72h after catheterization, changed every 7 days or as needed. | Standard transparent dressing. | Patients showing at least one sign or symptom of bloodstream infection (fever, chills, or hypotension not related to another infection site). | >100 CFU from catheter tip cultures using quantitative methods. | 1 year | Local skin reaction : (p = 0,54) Intervention group (7,5%) Control group (6,0%) |
CLABSI/CRBSI (i) : No statistically significant difference between intervention group and control group (7,98 per 1000 days vs 6,74 per 1000 days p= 0,70). Catheter colonization (ii) : No statistically significant difference between intervention group and control group (2,02 per 1000 days vs 3,07 per 1000 days; p= 0,59). |
| Duygu Sönmez Düzkaya, Turkey, 2016 |
Parallel-group RCT | Pediatric patients admitted to the PICU with CVC >72h.. Main pathology : Respiratory failure. |
Intervention group. Patients : 50 M: 60 % F: 40 % Range: 0-18 Control group. Patients : 50 M: 60 %. F: 40 % Range: 0-18 Mean age: 2,1 years |
Short-term CVC | Parental nutrition and blood transfusions | Chlorhexidine dressing: Applied after CVC insertion and changed every 7 days or as needed. | Sterile pad dressing | >15 CFU growth at catheter tip and microorganism isolated from two blood samples showing the same antibiotic resistance pattern as those from the catheter tip. | >15 CFU growth but no clinical infection signs and negative blood cultures, or blood microorganism different from that on catheter tip. | 2 years | Not specified | CLABSI/CRBSI (i) : No statistically significant difference between intervention group and control group (2% vs 10% p = 0,07) Catheter colonization (ii) : No statistically significant difference between intervention group and control group (2% vs 8% p = 0,07) |
| Itzhak Levy, Israel, 2005 |
Parallel-group RCT | Pediatric patients admitted to the cardiac PICU with CVC>48h. Main pathology : Heart disease |
Intervention group: Patients : 74 M: 34 % F: 66 % Range: 0-18 Control group: Patients : 71 M: 39 %. F: 61 %. Range: 0-18 Mean age: 2-5 years |
Non-tunneled short-term CVC | Fluid administration and blood sampling. | Sponge impregnated with chlorhexidine placed at insertion site, covered with transparent polyurethane, replaced in case of mechanical complications, bleeding or infection signs.. | Standard polyurethane dressing. | Bacteremia without isolation of the same organism from both CVC tip and blood | >15 CFU by roll-plate technique, without local or systemic infection signs. | 1 year and 2 months | Erythema at insertion site : Intervention group (5,4%) Control group (1,5%) |
CLABSI/CRBSI (i) : No statistically significant difference between intervention group and control group (5,4% vs 4,2%; p= 1,00) Catheter colonization (ii) : Chlorhexidine dressing significantly reduces the incidence of catheter colonization (14,8% vs 29,5%; p =0,04) |
3.2. JBI Checklist for the Critical Appraisal of Randomized Clinical Trials
THE CRITICAL APPRAISAL OF RANDOMIZED CLINICAL TRIALS
The critical appraisal of randomized clinical trials was conducted by two independent reviewers (GP, AM) using the Joanna Briggs Institute (JBI) tools [21] adapted to the specific study design.
The revised JBI tool for randomized controlled trials (RCTs) consists of 13 items addressing key aspects of study validity, including selection and allocation bias, intervention delivery, outcome assessment, participant retention, and the validity of statistical conclusions. Some specific questions are considered critical for determining the internal validity of an RCT.
For scoring, the following system was applied:
- 2 points if the criterion was met
- 1 point if unclear
- 0 points if not met
The maximum possible score for RCTs was 26. Studies were classified by quality as follows:
- High quality: more than 80% of criteria met
- Moderate quality: 60% to 80% of criteria met
- Low quality: less than 60% of criteria met.
Table 6.
JBI Checklist for the Critical Appraisal of Randomized Clinical Trials.
| Internal validity | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Selection and allocation | Administration of the intervention/exposure | Assessment, detection and measurement of the outcome | Retention of participants | Total score (%) | Validity of the statistical conclusion | ||||||||||||
| Questions | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | ||||
| Duyu et al 2021 | OUTCOME | RESULTS | |||||||||||||||
| CLABSI/CRBSI | 1 year 7 months | YES | YES | YES | NO | NO | YES | YES | YES | YES | YES | 22/26 (84,6) | YES | YES | YES | ||
| Catheter colonization | 1 year 7 months | YES | YES | YES | NO | NO | YES | YES | YES | YES | YES | YES | YES | YES | |||
| Jintrungruengnij et al 2020 | CLABSI/CRBSI | 1 year | YES | YES | YES | NO | NO | YES | YES | YES | YES | YES | 22/26 (84,6) | YES | YES | YES | |
| Catheter colonization | 1 year | YES | YES | YES | NO | NO | YES | YES | YES | YES | YES | YES | YES | YES | |||
| Düzkaya et al 2016 | CLABSI/CRBSI | 2 years | YES | YES | YES | NO | NO | YES | YES | YES | YES | YES | 22/26 (84,6) | YES | YES | YES | |
| Catheter colonization | 2 years | YES | YES | YES | NO | NO | YES | YES | YES | YES | YES | YES | YES | YES | |||
| Levy et al 2005 | CLABSI/CRBSI | 1 year 2 months | YES | NC | YES | NO | NO | YES | YES | YES | YES | YES | 21/26 (80,7) | YES | YES | YES | |
| Catheter colonization | 1 year 2 months | YES | NC | YES | NO | NO | YES | YES | YES | YES | YES | YES | YES | YES | |||
All studies, regardless of their methodological quality, were included in the review.
3.3. Characteristics of the Included Studies
3.4. Characteristics of the Population
The studies recruited a total of 733 patients, of whom 367 were in the intervention group and 366 in the control group, with ages ranging from 0 to 18 years and a prevalence of male patients. The clinical indications for central venous catheter (CVC) placement included: administration of intravenous therapy [22,23,25], parenteral nutrition [24], blood transfusions [24], and repeated venous sampling [25]. In most studies, the population setting was represented by the critical care area [22,24,25], while in others, the setting was not clearly specified [23]. The main diagnoses found among hospitalized patients who received a CVC were respiratory failure [22,24] and cardiac diseases [23,25].
3.5. Characteristics of the Intervention
The nursing intervention adopted in the various studies involved the application of a chlorhexidine-impregnated dressing, with timing varying according to the protocol followed: in some cases, the dressing was applied 24 hours after CVC insertion [22], in others after 72 hours [23], while in additional studies, application occurred immediately after catheter placement [24,25]. The frequency of dressing replacement also varied among studies: in some, it was routinely performed every 7 days [22,23,24], while in others, replacement occurred only as clinically indicated [25]. In all studies considered, both the intervention and the control procedures were performed by nursing staff. The intervention was applied exclusively to the patient, while parents were asked to provide informed consent for participation in the study [22,23,24,25]. The control groups received either a standard transparent polyurethane dressing [23,24,25] or a standard transparent, breathable, hypoallergenic polyurethane dressing [22].
3.6. Outcomes
The outcomes investigated in the studies included in this literature review, consistent with the objective of evaluating the effectiveness of chlorhexidine-impregnated dressings compared to standard ones, concern the rate of CLABSI/CRBSI and the prevention of catheter colonization in pediatric patients with CVCs [22,23,24,25]. Considering the studies that examined respiratory failure as the main condition [22,24], in the study where the clinical indication was the administration of heparin and antibiotics, no statistically significant difference was found in the reduction of CLABSI/CRBSI rates despite the use of chlorhexidine-impregnated dressings [22]. However, a statistically significant reduction in catheter colonization was observed [22]. Conversely, in the study where the clinical indication was the administration of parenteral nutrition and blood transfusions, no statistically significant difference was observed either in the CLABSI/CRBSI rate or in catheter colonization [24].
Regarding the studies that considered cardiac diseases as the main condition [23,25], in the study where the clinical indication was intravenous therapy administration [23], no statistically significant difference was observed with the use of chlorhexidine-impregnated dressings, neither for CLABSI/CRBSI rates nor for catheter colonization [23]. However, in the study where the clinical indication was fluid administration and blood sampling [25], although there was no statistically significant reduction in CLABSI/CRBSI rates, a significant decrease in catheter colonization was reported [25].
The insertion of CVCs, whether short- or long-term, was not associated with a statistically significant reduction in CLABSI/CRBSI incidence, as shown by studies analyzing short-term non-tunneled CVCs [22,25] and those evaluating the use of CVCs or PICCs [23,24]. However, a significant reduction in catheter colonization was observed in the studies involving short-term non-tunneled CVCs [22,25].
In three of the four studies analyzed, catheter colonization was defined as the growth of more than 15 colony-forming units (CFU) on the catheter tip, in the absence of clinical signs of infection and without microorganism isolation from the bloodstream [22,24,25]. In another study, colonization was defined as the growth of more than 100 CFU on the catheter tip [23]. A statistically significant reduction in colonization was observed in two of the three studies using the 15 CFU threshold [22,25]. Conversely, no significant difference was found in one of these studies [24]. Likewise, in the study using the 100 CFU threshold, no statistically significant variation was observed [23].
In 2005, the chlorhexidine dressing consisted of a sponge impregnated with antiseptic solution, applied directly to the insertion site and covered with a transparent polyurethane film. In that context, no significant reduction was observed in the incidence of CLABSI or CRBSI compared to the standard dressing, while a statistically significant reduction in catheter colonization was detected [25]. In later studies conducted between 2016 and 2021, the chlorhexidine dressing was no longer covered with polyurethane [22,23,24]. In these cases, no significant differences emerged in the incidence of CLABSI/CRBSI or in catheter colonization, except for one study that showed a significant reduction in colonization [22].
Standard dressings have also evolved over time. Although they have always been made of polyurethane, in 2005 they consisted of a simple polyurethane dressing [25], whereas by 2021 they had evolved into a more advanced version: transparent, breathable, and hypoallergenic [22]. Despite these technological improvements, the outcomes remained largely unchanged: there was no significant reduction in CLABSI/CRBSI rates [22,23,24,25], while catheter colonization showed a significant decrease [22,25].
Another variable analyzed was the average age of the study population. In three studies involving patients with a mean age between 2 and 2.3 years [22,23,24], no significant differences were found in CLABSI/CRBSI rates; nonetheless, only one study reported a significant reduction in catheter colonization [22]. When the mean age slightly increased, between 2 and 5 years [25], the CLABSI/CRBSI rate remained stable, while catheter colonization significantly decreased.
4. Discussion
The aim of this review was to evaluate the effectiveness of chlorhexidine-impregnated dressings compared to standard dressings in preventing CLABSI, CRBSI, and catheter colonization in pediatric patients with central venous catheters (CVCs).
The results did not show statistically significant differences in the development of CLABSI and CRBSI across the four studies analyzed [22,23,24,25].
A possible explanation for this lack of effectiveness lies in the specificity of the studied population. Unlike the meta-analysis by Wei et al. (2019) [20], in which only 3 out of 12 studies were conducted on pediatric patients, this review focuses exclusively on this age group. The pediatric age can represent a limiting factor, both because of the immaturity of the immune system [26]—especially in very young patients (mean age 2–2.3 years) [22,23,24]—and because of behaviors that compromise the integrity of the dressing, such as restlessness [27].
However, even in the meta-analysis by Wei et al. (2019) [20], the results align with those of this review when only pediatric studies are considered.
Furthermore, the studies cover a time span of 16 years, during which both chlorhexidine-impregnated and standard dressings have evolved [9,28]. The most recent standard dressings offer improved performance in terms of adhesion, breathability, and hypoallergenicity [22], which—together with improved clinical practices—may reduce the additional benefit margin of chlorhexidine-impregnated dressings [19,29]. This may explain the absence of statistically significant differences in effectiveness observed in the studies included in this review [22,23,24,25].
Organizational and methodological variables may also have influenced the results, such as differences in CVC management protocols, staff training, or adherence to guidelines [19], as well as the varying definitions adopted for CLABSI/CRBSI. This latter aspect is particularly important, as stricter or looser thresholds can alter event classification: for example, colonization was defined with a threshold of 15 CFU in some studies [22,24,25], while others used a higher threshold of 100 CFU [23]. The latter study, adopting the higher threshold, did not detect significant differences between groups.
Despite the lack of significant benefits in terms of CLABSI/CRBSI, two of the four included studies [22,25] reported a statistically significant difference in catheter colonization when using chlorhexidine-impregnated dressings.
These findings are consistent with those of Garland et al. (2001) [30], where a similar reduction was observed, although the control group used povidone-iodine disinfection. A possible explanation for this concordance may lie in the homogeneity of the samples, particularly regarding age, with greater susceptibility to bacterial colonization. Moreover, the more sensitive definition of colonization (≥15 CFU) [22,25] likely allowed the detection of minimal microbial growth, increasing the sensitivity of the intervention’s effect. This suggests that catheter colonization may represent a more sensitive indicator of dressing effectiveness in the pediatric population than CLABSI/CRBSI.
This review presents some methodological limitations, including the small number of included studies, variability in outcome definitions, and changes over time in dressings and guidelines, which make direct comparison of results difficult. Furthermore, detailed data on staff compliance and patient comorbidities are lacking. Other limitations concern the search process, such as language restrictions, publication dates, and databases used.
Despite the extensive literature on the use of chlorhexidine-impregnated dressings, the effectiveness of this single intervention in the pediatric population remains uncertain and often insufficient. This is particularly true in critical care contexts, where population- and management-specific factors may influence outcomes. Recent studies highlight the importance of an integrated (bundle) approach combining chlorhexidine-impregnated dressings with other measures, such as ultrasound-guided catheter placement, tunneling, the use of glue to protect the exit site, and staff training programs [19].
This multidimensional strategy has demonstrated greater effectiveness in preventing CLABSI/CRBSI in the pediatric critical care setting and is currently recommended by major international guidelines [31,32,33].
However, the specific characteristics of the pediatric population and the organizational variables of the studies reviewed make it necessary to further investigate the effectiveness of chlorhexidine-impregnated dressings as a standalone intervention in this context. Although an integrated approach is recommended, in pediatric clinical practice chlorhexidine-impregnated dressings are often used as a single measure. Assessing their isolated effectiveness is therefore essential to understand the true contribution of this intervention, identify potential limitations, and guide the optimization of catheter-related infection prevention protocols.
These limitations highlight the need for new, up-to-date randomized controlled clinical trials reflecting current technologies, using standardized definitions and methodologies, and involving larger, age-homogeneous samples to obtain more precise results.
This review also presents several strengths, both methodological and clinical. In particular, it focuses exclusively on the pediatric population, which is inherently more exposed to infection risk [34] and often underrepresented in the literature compared to adults.
The selected studies also highlight the evolution of care practices and materials used, offering an overview that integrates both historical and current aspects.
Unlike other reviews, this one has a specific focus on the comparison between two types of dressings, making the results directly applicable to pediatric clinical practice. The review considered important variables such as patient pathology, the indication for CVC placement, the type of device used, and dressing management. This approach contributes to greater validation of the findings.
Furthermore, the inclusion of an analysis of the different definitions of CLABSI/CRBSI and catheter colonization demonstrates attention to factors influencing data consistency and comparability.
Finally, the topic addressed in this review is directly relevant to nursing practice, and these results can guide evidence-based decision-making regarding dressing selection.
5. Conclusions
The prevention of catheter-related infections is a crucial element not only for ensuring the safety of pediatric patients but also for reducing the costs associated with infectious complications, thereby improving the overall quality of healthcare.
This review highlighted that, in the pediatric population with central venous catheters, chlorhexidine-impregnated dressings are not more effective than standard dressings in reducing CLABSI/CRBSI. However, two studies reported greater effectiveness of chlorhexidine dressings in reducing catheter colonization.
The most recent guidelines recommend an integrated approach based on care bundles that include the use of chlorhexidine dressings as the most effective strategy for preventing CLABSI/CRBSI in pediatric patients [32,33].
In light of current evidence, chlorhexidine dressings cannot be considered a priority preventive strategy when used alone in the pediatric setting. However, their inclusion within a bundle suggests a potential benefit that warrants further investigation.
It is therefore desirable that future research focus on randomized clinical trials specifically targeting the pediatric population, in order to clarify the factors influencing the effectiveness of different dressings, identify subgroups of pediatric patients who may benefit the most, evaluate the impact of dressing duration and replacement frequency, and optimize the composition of preventive bundles to improve their efficacy and safety.
Author Contributions
Conceptualization, G.P., A.Mariani. and S.B..; methodology, G.P.; A.Mariani.; writing—original draft preparation, G.P.; A.Mariani; S.B..; writing—review and editing, A.L.; A.Messina.; supervision, B.M.; L.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CLABSI | Central Line-Associated Bloodstream Infection |
| CRBSI | Catheter-Related Bloodstream Infection |
| CVC | Central Venous Catheter |
References
- Kolikof, J. , Peterson, K., Williams, C., Baker, A.M. ‘Central Venous Catheter Insertion’, in StatPearls. Treasure Island (FL): StatPearls Publishing, 4 February (2025).
- Cellini, M. , Bergadano, A., Crocoli, A., Locatelli, F., Cesaro, S., Putti, M.C., Rondelli, R., Vinti, L., Menna, G., Rizzari, C. ‘Guidelines of the Italian Association of Pediatric Hematology and Oncology for the management of the central venous access devices in pediatric patients with onco-hematological disease’, Journal of Vascular Access, 23(1), (2022) pp. 3–17.
- Cesaro, S. , Caddeo, G. ‘Vascular Access’, in Sureda, A., Corbacioglu, S., Greco, R., Kröger, N., Carreras, E. (eds.), The EBMT Handbook: Hematopoietic Cell Transplantation and Cellular Therapies, 8th ed. Cham (CH): Springer, (2024) pp. 197–201.
- Lee, K. , Ramaswamy, R.S. ‘Intravascular access devices from an interventional radiology perspective: indications, implantation techniques, and optimizing patency’, Transfusion, 58(Suppl 1), (2018) pp. 549–557.
- Cornillon, J. , Martignoles, J.A., Tavernier-Tardy, E., Isnard, F., Thomas, X., Yakoub-Agha, I., Michallet, M., Salles, G., Dhedin, N., Dauriat, G., Garnier, F., Tabrizi, R., Bay, J.O. ‘Prospective evaluation of systematic use of peripherally inserted central catheters (PICC lines) for the home care after allogenic hematopoietic stem cells transplantation’, Supportive Care in Cancer, 25, (2017) pp. 2843–2847.
- Blanco-Guzman, M.O. ‘Implanted vascular access device options: a focus review on safety and outcomes’, Transfusion, 58, (2018) pp. 558–568.
- Lee, M.M. , Anand, S., Loyd, J.W. ‘Saphenous Vein Cutdown’, in StatPearls. Treasure Island (FL): StatPearls Publishing, 4 September (2023).
- Misirlioglu, M. , Yildizdas, D., Yavas, D.P., Ekinci, F., Horoz, O.O., Yontem, A. ‘Central Venous Catheter Insertion for Vascular Access: A 6-year Single-center Experience’, Indian Journal of Critical Care Medicine, 27(10), (2023) pp. 748–753. [CrossRef]
- Ullman, A.J., Cooke, M.L., Mitchell, M., Tran, V., Rickard, C.M., Marsh, N., Mihala, G., Chopra, V., Cheng, A.C. ‘Dressings and securement devices for central venous catheters (CVC)’, Cochrane Database of Systematic Reviews, 2015(9):CD010367 (2015). [CrossRef]
- Arvaniti, K. , Lathyris, D., Clouva-Molyvdas, P., Papaioannou, V., Malachias, S., Rellos, K., Tsolaki, V., Tripodaki, E., Nanas, S., Dimopoulou, I. ‘Comparison of Oligon catheters and chlorhexidine-impregnated sponges with standard multilumen central venous catheters for prevention of associated colonization and infections in intensive care unit patients: a multicenter, randomized, controlled study’, Critical Care Medicine, 40(2), (2012) pp. 420–429.
- Ho, K.M. , Litton, E. ‘Use of chlorhexidine-impregnated dressing to prevent vascular and epidural catheter colonization and infection: a meta-analysis’, Journal of Antimicrobial Chemotherapy, 58(2), (2006) pp. 281–287. [CrossRef]
- Tingley, K. , Lê, M.L. ‘Chlorhexidine Gluconate for Skin Preparation During Catheter Insertion and Surgical Procedures’, Ottawa (ON): Canadian Agency for Drugs and Technologies in Health, August (2021).
- Jenks, M. , Craig, J., Green, W., Hewitt, N., Arber, M., Sims, A. ‘Tegaderm CHG IV Securement Dressing for Central Venous and Arterial Catheter Insertion Sites: A NICE Medical Technology Guidance’, Applied Health Economics and Health Policy, 14(2),(2016) pp. 135–149. [CrossRef]
- Shapiro, J.M. , Bond, E.L., Garman, J.K. ‘Use of a chlorhexidine dressing to reduce microbial colonization of epidural catheters’, Anesthesiology, 73(4), (1990) pp. 625–631. [CrossRef]
- Thokala, P. , Arrowsmith, M., Poku, E., Martyn-St James, M., Anderson, J., Foster, S., Elliott, T., Whitehouse, T. ‘Economic impact of Tegaderm chlorhexidine gluconate (CHG) dressing in critically ill patients’, Journal of Infection Prevention, 17(5), (2016) pp. 216–223. [CrossRef]
- O'Grady, N.P. , Alexander, M., Burns, L.A., Dellinger, E.P., Garland, J., Heard, S.O., Lipsett, P.A., Masur, H., Mermel, L.A., Pearson, M.L., Raad, I., Randolph, A.G., Rupp, M.E., Saint, S. ‘Guidelines for the prevention of intravascular catheter-related infections’, Clinical Infectious Diseases, 52(9), (2011) pp. e162–e193. [CrossRef]
- Prestel, C. , Fike, L., Patel, P., Smith, J., Walker, B. ‘A Review of Pediatric Central Line-Associated Bloodstream Infections Reported to the National Healthcare Safety Network: United States, 2016-2022’, Journal of Pediatric Infectious Diseases Society, 12(9), (2023)pp. 519–521. [CrossRef]
- Nowak, J.E. , Brilli, R.J., Lake, M.R., Gedeit, R.G., Sparling, K.W. ‘Reducing catheter-associated bloodstream infections in the pediatric intensive care unit: Business case for quality improvement’, Pediatric Critical Care Medicine, 11(5), (2010) pp. 579–587. [CrossRef]
- Biasucci, D.G. , Pittiruti, M., Taddei, A., Elia, F., Cogo, P., Cattani, S., Avolio, M., Iorio, R. ‘Targeting zero catheter-related bloodstream infections in pediatric intensive care unit: a retrospective matched case-control study’, Journal of Vascular Access, 19(2), (2018) pp. 119–124. [CrossRef]
- Wei, L. , Li, Y., Li, X., Bian, L., Wen, Z., Li, M. ‘Chlorhexidine-impregnated dressing for the prophylaxis of central venous catheter-related complications: a systematic review and meta-analysis’, BMC Infectious Diseases, 19(1) (2019):429. [CrossRef]
- Aromataris E, Fernandez R, Godfrey C, Holly C, Kahlil H, Tungpunkom P. Summarizing systematic reviews: methodological development, conduct and reporting of an Umbrella review approach. Int J Evid Based Healthc. (2015);13(3):132-40.
- Duyu M, Karakaya Z, Yazici P, Yavuz S, Yersel NM, Tascilar MO, Firat N, Bozkurt O, Caglar Mocan Y. Comparison of chlorhexidine impregnated dressing and standard dressing for the prevention of central-line associated blood stream infection and colonization in critically ill pediatric patients: A randomized controlled trial. Pediatr Int. (2022) Jan;64(1):e15011. [CrossRef] [PubMed]
- Jitrungruengnij N, Anugulruengkitt S, Rattananupong T, Prinyawat M, Jantarabenjakul W, Wacharachaisurapol N, Chatsuwan T, Janewongwirot P, Suchartlikitwong P, Tawan M, Kanchanabutr P, Pancharoen C, Puthanakit T. Efficacy of chlorhexidine patches on central line-associated bloodstream infections in children. Pediatr Int. 2020 Jul;62(7):789-796. [CrossRef] [PubMed]
- Düzkaya DS, Sahiner NC, Uysal G, Yakut T, Çitak A. Chlorhexidine-Impregnated Dressings and Prevention of Catheter-Associated Bloodstream Infections in a Pediatric Intensive Care Unit. Crit Care Nurse. (2016) Dec;36(6):e1-e7. [CrossRef] [PubMed]
- Levy I, Katz J, Solter E, Samra Z, Vidne B, Birk E, Ashkenazi S, Dagan O. Chlorhexidine-impregnated dressing for prevention of colonization of central venous catheters in infants and children: a randomized controlled study. Pediatr Infect Dis J. (2005) Aug;24(8):676-9. [CrossRef] [PubMed]
- Liu, L.P. , Lin, Q.S., Yang, W.Y., Chen, X.J., Liu, F., Chen, X., Ren, Y.Y., Ruan, M., Chen, Y.M., Zhang, L., Zou, Y., Guo, Y., Zhu, X.F. ‘High risk of bloodstream infection of carbapenem-resistant Enterobacteriaceae carriers in neutropenic children with hematological diseases’, Antimicrobial Resistance and Infection Control (2023), 12(1):66. [CrossRef]
- McNamara, S.A. , Hirt, P.A., Weigelt, M.A., Nanda, S., de Bedout, V., Kirsner, R.S., Schachner, L.A. ‘Traditional and advanced therapeutic modalities for wounds in the paediatric population: an evidence-based review’, Journal of Wound Care, 29(6), (2020) pp. 321–334. [CrossRef]
- Centers for Disease Control and Prevention. (2024, 12 April). Updates | Infection Control.
- Xu, H. , Hyun, A., Mihala, G., Rickard, C.M., Cooke, M.L., Lin, F., Mitchell, M., Ullman, A.J. ‘The effectiveness of dressings and securement devices to prevent central venous catheter-associated complications: A systematic review and meta-analysis’, International Journal of Nursing Studies, (2024) 149:104620. [CrossRef]
- Garland, J.S. , Alex, C.P., Mueller, C.D., Hedlund, T.L., Miller, C.A., Reisinger, K.D., Buck, R.K., Stafford, R.R. ‘A randomized trial comparing povidone-iodine to a chlorhexidine gluconate-impregnated dressing for prevention of central venous catheter infections in neonates’, Pediatrics, 107(6), pp. 1431–1 (2001) 436. [CrossRef]
- Pittiruti, M. , Scoppettuolo, G. ‘Raccomandazioni GAVeCeLT 2024 per indicazione, impianto e gestione dei dispositivi per accesso venoso’, Gruppo Aperto di Studio Gli Accessi Venosi Centrali a Lungo Termine (GAVeCeLT). (2024) Documento disponibile online presso IVAS e GAVeCeLT.
- Infusion Nurses Society (INS). Infusion therapy standards of practice. 9th ed. Norwood, MA: Infusion Nurses Society (2024).
- Society for Healthcare Epidemiology of America (SHEA), Infectious Diseases Society of America (IDSA), Association for Professionals in Infection Control and Epidemiology (APIC), Centers for Disease Control and Prevention (CDC). ‘Strategies to prevent central line–associated bloodstream infections in acute-care hospitals: 2022 update’,Infection Control & Hospital Epidemiology, 43(5), (2022) pp. 547–585. [CrossRef]
- Raymond, S. L., Stortz, J. A., Mira, J. C., & Moldawer, L. L. Programmed and environmental determinants driving neonatal susceptibility to infection. Immunological Reviews (2023), 311(1), 82396. [CrossRef]
Table 2.
Research question according to the PIO methodology.
| (P) Population | Pediatric patients with central venous catheter (CVC) |
| (I) Intervention | Use of chlorhexidine-impregnated dressings. |
| (O) Outcome | CLABSI, CRBSI, CVC colonization |
Table 3.
Combination of keywords.
| Database | Search strategy | Results |
|---|---|---|
| Medline/Embase | ('central venous catheter'/exp OR 'axera':ti,ab,kw OR 'broviac':ti,ab,kw OR 'cvp line':ti,ab,kw OR 'careflow (central venous catheter)':ti,ab,kw OR 'cook spectrum (central venous catheter)':ti,ab,kw OR 'groshong':ti,ab,kw OR 'icy (central venous catheter)':ti,ab,kw OR 'logicath':ti,ab,kw OR 'leonard':ti,ab,kw OR 'leonard catheter':ti,ab,kw OR 'orion ii':ti,ab,kw OR 'pediasat':ti,ab,kw OR 'powerline (central venous catheter)':ti,ab,kw OR 'powerwand':ti,ab,kw OR 'pro-line':ti,ab,kw OR 'secalon-t':ti,ab,kw OR 'vortex (central venous catheter)':ti,ab,kw OR 'vortex port':ti,ab,kw OR 'catheter, central venous':ti,ab,kw OR 'central intravenous catheter':ti,ab,kw OR 'central line':ti,ab,kw OR 'central vein catheter':ti,ab,kw OR 'central venous access catheter':ti,ab,kw OR 'central venous access device':ti,ab,kw OR 'central venous catheter':ti,ab,kw OR 'central venous catheter, device':ti,ab,kw OR 'central venous catheterization kit, short-term':ti,ab,kw OR 'central venous catheters':ti,ab,kw OR 'central venous line':ti,ab,kw OR 'cv cath':ti,ab,kw OR 'short-term central venous catheterization kit':ti,ab,kw OR 'central venous catheterization'/exp OR 'catheterisation, central venous':ti,ab,kw OR 'catheterization, central venous':ti,ab,kw OR 'central vein catheterisation':ti,ab,kw OR 'central vein catheterization':ti,ab,kw OR 'central venous catheterisation':ti,ab,kw OR 'central venous catheterization':ti,ab,kw) AND ('chlorhexidine'/exp OR '1, 1 hexamethylenebis [5 (para chlorophenylbiguanide) ]':ti,ab,kw OR '1, 1` hexamethylenebis [5 (4 chlorophenyl) biguanide]':ti,ab,kw OR '1, 1` hexamethylenebis [5 (para chlorophenylbiguanide) ]':ti,ab,kw OR '1, 6 bis (n5 para chlorophenyl n1 diguanido) hexane':ti,ab,kw OR '1, 6 bis [n1 (para chlorophenyl) n5 biguanido] hexane':ti,ab,kw OR '1, 6 di (4` chlorophenyldiguanido) hexane':ti,ab,kw OR 'ay 5312':ti,ab,kw OR 'ay5312':ti,ab,kw OR 'bidex (chlorhexidine)':ti,ab,kw OR 'boston conditioning lotion':ti,ab,kw OR 'chlorhex':ti,ab,kw OR 'chlorhexidin':ti,ab,kw OR 'chlorhexidine':ti,ab,kw OR 'chlorhexidine chlorhydrate':ti,ab,kw OR 'chlorhexidine dihydrochloride':ti,ab,kw OR 'chlorhexidine glutamate':ti,ab,kw OR 'chlorhexidine hydrochloride':ti,ab,kw OR 'chlorohex':ti,ab,kw OR 'chlorohexidine':ti,ab,kw OR 'chlorohexidine acetate':ti,ab,kw OR 'chlorohexydine':ti,ab,kw OR 'clohexidine':ti,ab,kw OR 'clorhexidine':ti,ab,kw OR 'compound 10040':ti,ab,kw OR 'hexamethylene 1, 6 bis [1 (5 para chlorophenyl) biguanide]':ti,ab,kw OR 'lisium':ti,ab,kw OR 'nibitane':ti,ab,kw OR 'nolvasan':ti,ab,kw OR 'nolvascin':ti,ab,kw OR 'rotersept':ti,ab,kw OR 'sterilon':ti,ab,kw OR 'tubilicid':ti,ab,kw OR 'tubulicid':ti,ab,kw OR 'umbipro':ti,ab,kw) AND ('catheter related bloodstream infection'/exp OR 'clabsi (central line associated bloodstream infection)':ti,ab,kw OR 'clabsis (central line associated bloodstream infections)':ti,ab,kw OR 'crbsi (catheter related bloodstream infection)':ti,ab,kw OR 'crbsis (catheter related bloodstream infections)':ti,ab,kw OR 'catheter associated blood stream infection':ti,ab,kw OR 'catheter associated blood stream infections':ti,ab,kw OR 'catheter associated bloodstream infection':ti,ab,kw OR 'catheter associated bloodstream infections':ti,ab,kw OR 'catheter related blood stream infection':ti,ab,kw OR 'catheter related blood stream infections':ti,ab,kw OR 'catheter related bloodstream infection':ti,ab,kw OR 'catheter related bloodstream infections':ti,ab,kw OR 'central line associated bloodstream infection':ti,ab,kw OR 'central line associated bloodstream infections':ti,ab,kw) AND ([adolescent]/lim OR [child]/lim OR [infant]/lim OR [newborn]/lim OR [preschool]/lim OR [school]/lim) | 93 |
| Cinhal | ('central venous catheter'/exp OR 'axera':ti,ab,kw OR 'broviac':ti,ab,kw OR 'cvp line':ti,ab,kw OR 'careflow (central venous catheter)':ti,ab,kw OR 'cook spectrum (central venous catheter)':ti,ab,kw OR 'groshong':ti,ab,kw OR 'icy (central venous catheter)':ti,ab,kw OR 'logicath':ti,ab,kw OR 'leonard':ti,ab,kw OR 'leonard catheter':ti,ab,kw OR 'orion ii':ti,ab,kw OR 'pediasat':ti,ab,kw OR 'powerline (central venous catheter)':ti,ab,kw OR 'powerwand':ti,ab,kw OR 'pro-line':ti,ab,kw OR 'secalon-t':ti,ab,kw OR 'vortex (central venous catheter)':ti,ab,kw OR 'vortex port':ti,ab,kw OR 'catheter, central venous':ti,ab,kw OR 'central intravenous catheter':ti,ab,kw OR 'central line':ti,ab,kw OR 'central vein catheter':ti,ab,kw OR 'central venous access catheter':ti,ab,kw OR 'central venous access device':ti,ab,kw OR 'central venous catheter':ti,ab,kw OR 'central venous catheter, device':ti,ab,kw OR 'central venous catheterization kit, short-term':ti,ab,kw OR 'central venous catheters':ti,ab,kw OR 'central venous line':ti,ab,kw OR 'cv cath':ti,ab,kw OR 'short-term central venous catheterization kit':ti,ab,kw OR 'central venous catheterization'/exp OR 'catheterisation, central venous':ti,ab,kw OR 'catheterization, central venous':ti,ab,kw OR 'central vein catheterisation':ti,ab,kw OR 'central vein catheterization':ti,ab,kw OR 'central venous catheterisation':ti,ab,kw OR 'central venous catheterization':ti,ab,kw) AND ('chlorhexidine'/exp OR '1, 1 hexamethylenebis [5 (para chlorophenylbiguanide) ]':ti,ab,kw OR '1, 1` hexamethylenebis [5 (4 chlorophenyl) biguanide]':ti,ab,kw OR '1, 1` hexamethylenebis [5 (para chlorophenylbiguanide) ]':ti,ab,kw OR '1, 6 bis (n5 para chlorophenyl n1 diguanido) hexane':ti,ab,kw OR '1, 6 bis [n1 (para chlorophenyl) n5 biguanido] hexane':ti,ab,kw OR '1, 6 di (4` chlorophenyldiguanido) hexane':ti,ab,kw OR 'ay 5312':ti,ab,kw OR 'ay5312':ti,ab,kw OR 'bidex (chlorhexidine)':ti,ab,kw OR 'boston conditioning lotion':ti,ab,kw OR 'chlorhex':ti,ab,kw OR 'chlorhexidin':ti,ab,kw OR 'chlorhexidine':ti,ab,kw OR 'chlorhexidine chlorhydrate':ti,ab,kw OR 'chlorhexidine dihydrochloride':ti,ab,kw OR 'chlorhexidine glutamate':ti,ab,kw OR 'chlorhexidine hydrochloride':ti,ab,kw OR 'chlorohex':ti,ab,kw OR 'chlorohexidine':ti,ab,kw OR 'chlorohexidine acetate':ti,ab,kw OR 'chlorohexydine':ti,ab,kw OR 'clohexidine':ti,ab,kw OR 'clorhexidine':ti,ab,kw OR 'compound 10040':ti,ab,kw OR 'hexamethylene 1, 6 bis [1 (5 para chlorophenyl) biguanide]':ti,ab,kw OR 'lisium':ti,ab,kw OR 'nibitane':ti,ab,kw OR 'nolvasan':ti,ab,kw OR 'nolvascin':ti,ab,kw OR 'rotersept':ti,ab,kw OR 'sterilon':ti,ab,kw OR 'tubilicid':ti,ab,kw OR 'tubulicid':ti,ab,kw OR 'umbipro':ti,ab,kw) AND ('catheter related bloodstream infection'/exp OR 'clabsi (central line associated bloodstream infection)':ti,ab,kw OR 'clabsis (central line associated bloodstream infections)':ti,ab,kw OR 'crbsi (catheter related bloodstream infection)':ti,ab,kw OR 'crbsis (catheter related bloodstream infections)':ti,ab,kw OR 'catheter associated blood stream infection':ti,ab,kw OR 'catheter associated blood stream infections':ti,ab,kw OR 'catheter associated bloodstream infection':ti,ab,kw OR 'catheter associated bloodstream infections':ti,ab,kw OR 'catheter related blood stream infection':ti,ab,kw OR 'catheter related blood stream infections':ti,ab,kw OR 'catheter related bloodstream infection':ti,ab,kw OR 'catheter related bloodstream infections':ti,ab,kw OR 'central line associated bloodstream infection':ti,ab,kw OR 'central line associated bloodstream infections':ti,ab,kw) AND ([adolescent]/lim OR [child]/lim OR [infant]/lim OR [newborn]/lim OR [preschool]/lim OR [school]/lim) | 10 |
Table 4.
Study selection process.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



