
Submitted:
10 November 2025
Posted:
11 November 2025
You are already at the latest version
Abstract
The diagnosis and management of UAD require an integrated, multidisciplinary approach. Diagnostic strategies combine clinical evaluation, imaging (CT), allergy testing, biomarker measurement (such as FeNO, blood eosinophils, IgE), and pulmonary function testing (spirometry, IOS) to phenotype the disease. Therapeutic management is stratified and aims to control inflammation and symptoms in both compartments. Cornerstones include topical corticosteroids (intranasal and inhaled) and saline irrigations. For severe forms, especially T2-high, targeted biologic therapies (anti-IL-5/IL-5R, anti-IL-4R, anti-TSLP) have revolutionized treatment, reducing dependence on oral corticosteroids and the need for surgical interventions (like endoscopic sinus surgery, ESS). Adopting a "treatable traits" approach is emerging as a key strategy for precision medicine in UAD.
Keywords:
United Airway Disease (UAD)
; type 2 inflammation
; biologic therapy
1. Introduction
The concept of united airway disease (UAD) well describes the common nature of inflammatory condition affecting both the upper, with rhinitis and rhinosinusitis, with (CRSwNP) or without nasal polyps (CRSsNP) and lower (e.g., asthma) airways [1]. The unified airway hypothesis postulates that these diseases are not isolated entities but rather manifestations of a single, interconnected inflammatory process [2,3,4,5], with high prevalence of compresence of both entities [6].
The upper and lower airways, though anatomopathological distinct but in anatomic continuity, share histological and functional characteristics, including epithelial lining, mucociliary clearance, and immune cell infiltration patterns. Both segments are exposed to environmental allergens and pollutants, initiating inflammatory responses through similar immunological cascades [7]. The concept of UAD not only enhances understanding of the disease mechanism but also prompts clinicians to re-evaluate compartmentalized treatment strategies. There is growing recognition that, successful management of asthma or rhinitis in isolation, may fall short of delivering optimal patient outcomes. This review aims to synthesize current knowledge on UAD with a focus on pathophysiological mechanisms, diagnostic strategies, therapeutic advancements, and future directions.
Epidemiology and Clinical Burden
UAD is a highly prevalent condition, with prevalence estimate ranging from 10% to 40% [8,9,10]. Epidemiological studies confirm that the deep associations between upper airway disorders and implicated in asthma control, lung function even leading to an increased bronchial hyperreactivity, and reduction of function regardless of smoking status [11]. Furthermore, other studies demonstrate that the prevalence of allergic rhinitis and CRS is growing, particularly in the pediatric population, with rates of allergic rhinitis increasing from 8.4% to almost 20% in the last decade. Therefore, it can be deduced from here that every patient with rhinitis/rhinosinusitis should also be evaluated for the presence of lung diseases (and vice versa) [3,12,13,14].
That frequent coexistence is found principally in severe diseases phenotypes. UAD encompasses a spectrum of diseases, including the usually considered chronic rhinosinusitis, nasal polyposis, and COPD, but also less considered diseases as bronchiectasis all of which contribute to a significant disease burden: the presence of one airway disease often predicts or otherwise precedes the development of another, fueling the paradigm "one airway, one disease" [4,15].
Recent studies show that the concomitant presence of upper airway diseases in patients with bronchiectasis, due to asthma, COPD but also “pure” bronchiectasis syndrome is not only common but also associated with an earlier disorder of the disease, a longer duration and a higher frequency of exacerbations [16,17].
Shared pathogenesis includes eosinophilic or neutrophilic inflammation, mucociliary clearance defects, and allergic factors: allergic sensitization and impaired mucosal defense are important contributors in the pathogenesis of UAD. A recent Mendelian randomization study suggests that pediatric asthma may be a causal risk factor for the development of bronchiectasis and chronic rhinitis, but there is still no certain evidence regarding chronic sinusitis [18].
About the deep link between asthma and rhinosinusitis literature evidence shows that patients with alone upper disease, independently by the presence of a atopic status, improve the development of asthma in their life and viceversa [19]
3. Mechanisms, Endotypes and Phenotypes
The unified airway hypothesis is supported by epidemiological, histoembryological, immunological, and molecular evidence which emphasize the functional and pathophysiological unity of the upper and lower airways.
Epidemiologically about 80% of asthmatic patients suffer from rhinitis, while 10-40% of patients with rhinitis develop asthma [20]. CRS is also linked to difficult-to-control asthma, frequent exacerbations, and poorer respiratory function and, if correctly treated, can lead to improve outcomes for bronchial disease as well [21,22,23,24]. These epidemiological data tend to emphasize how closely connected the airways are and that pathological entities, currently considered distinct, may represent an immunological-inflammatory continuum involving the entire respiratory tree. [2,25,26].
The continuity of the upper and lower airways originates at the embryological level, as both derive from the anterior intestine and closely connected embryonic structures, subsequently they are prone to developing differentiations: pseudostratified mucociliary epithelium with goblet cells, the presence of mucosa-associated lymphoid tissue (MALT), epithelial barrier function, and innate and adaptive immune response patterns [2,27,28,29,30,31].
Type 2 (T2) inflammation is the fulcrum but not the only representation of the pathogenesis of many UAD phenotypes, mainly characterized by eosinophilic infiltration and orchestrated by cells like T helper type 2 (Th2), cytokines such as IL-4, IL-5, and IL-13. These cytokines represent the junction between adaptive immunity and innate immunity, promoting and activating effector cells. Among these, type 2 innate lymphoid cells (ILC2) play an important role, releasing pro-inflammatory mediators in response to epithelial stimuli (mainly represented by IL-33, IL-25, and TSLP) [32], followed by the recruitment of Th2 cells and the intervention of eosinophils, the main effectors of tissue damage and maintenance of the inflammatory cascade [29,33,34].
The modulation of the abovementioned cytokines and cells play a pivotal role in both upper and lower airway inflammation, and their therapeutic targeting has demonstrated clinical benefit across these sites [3,4,5,14,29,35,36].
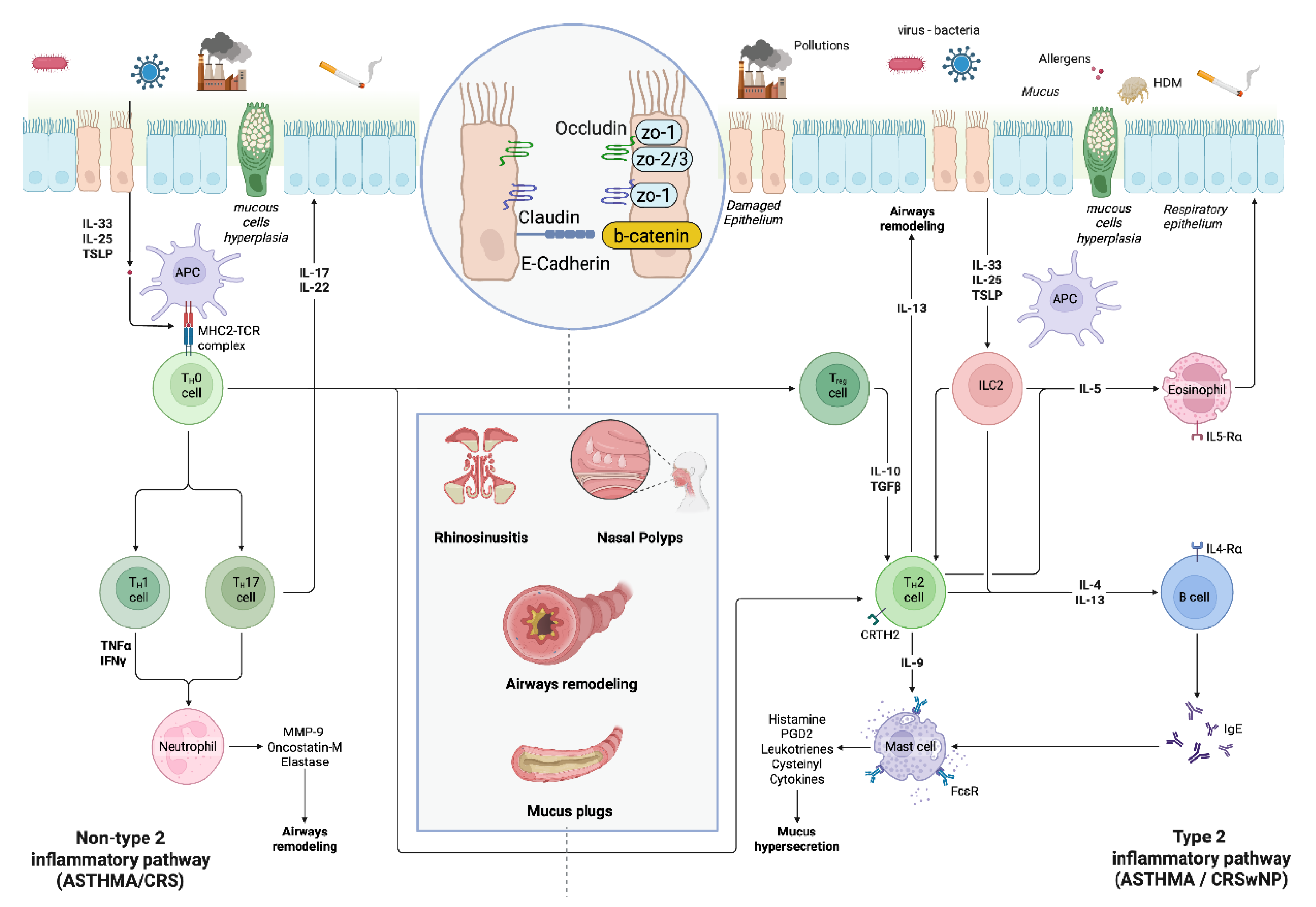
In asthma, as in CRSwNP, the inflammatory pathway is activated by a loss of epithelial barrier integrity, induced by viruses, allergens, or environmental irritants and pollutants. The loss of tight junctions, which causes a loss of cell adhesion (zoonine, claudine, occludine ed E-chaderine), associated with defective mucociliary clearance and antibody deficiency, promotes the penetration of antigens and amplifies the immune response, generating a vicious circle that feeds inflammation and barrier damage (Figure 1). Other inflammatory pathways, including type 1 and type 3 responses, together with epithelial damage, contribute to the heterogeneity of UAD. The airway microbiome, including bacterial and fungal communities, is increasingly recognized as a modulator of airway inflammation and disease expression, although its precise role in UAD pathogenesis remains under investigation. [3,29,37].
MicroRNAs (miRNAs), family of small endogenous non-coding RNA molecules, have emerged as important regulators of gene expression in airway inflammation, but few have been identified that directly link upper and lower airway disease; as an example, specific miRNAs, such as miR-223-3p and miR-155, have been linked to neutrophilic inflammation and immune regulation in asthma and other airway conditions [38]. Although, their clinical utility remains to be established [15].
The distinction between phenotypes (observable clinical manifestations) and endotypes (underlying biological mechanisms) is crucial in precision medicine, for understanding clinical variability and attempt to predict a response to treatment in asthma, rhinitis and CRSwNP.
As previously illustrated, the most representative endotype is the T2, which involves cytokines 4, 5, and 13, as well as eosinophils and class E immunoglobulins (IgE), ILC2, and allarmins; it generally has a good clinical response to corticosteroids (inhalers, intranasal or systemic) and biological therapy targeting one abovementioned mediator (generally antibodies against IL5, IL-5R, IL4R and IL13 or TSLP). Another phenotype is T2 low, which is mainly determined by a neutrophilic or paucigranulocytic inflammatory component and generally occurs in older patients with a higher BMI and a history of smoking. It represents a more difficult endotype, due to a lack of biomarkers and drugs response, both biological and systemic steroids; in these patients [39,40,41,42]. In addition to those described above, there are also other clinical phenotypes, such as exercise-induced asthma, aspirin-exacerbated asthma, and long-standing asthma with fixed obstruction, phenotypes that intersect with those described above, making it even more complex to identify a precise disease phenotype [42,43,44].
About upper airways, rhinitis and CRS can be described different phenotypes depending on the duration and intensity of symptoms, the presence of atopy and comorbidities, as well as the presence or absence of nasal polyps. Type 2 inflammation is well characterized in both (allergic rhinitis) AR and CRS with nasal polyps (CRSwNP), whereas type 1 inflammation is found principally in infectious rhinitis and CRS without nasal polyps (CRSsNP). Finally, can be described also a neurogenic endotype, demonstrated in several forms of non-allergic rhinitis, whereas epithelial barrier dysfunction is shown in AR and CRSwNP, and it seems to be the beginning of developing type 2 inflammation in some patients [45]. Inflammation mechanisms and involved citokines and cells are summarized in Figure 1.
4. Diagnostics tools
Told of the close link between these pathologies, diagnosis and subtyping of UAD require a comprehensive, multidisciplinary approach. Clinical history and physical examination remain crucial, but should be complemented by objective assessments:
- Imaging:
The most common used, both in the field of upper and lower airways are computed tomography (CT) and magnetic resonance imaging (MRI). Crucial for evaluating sinus and lower airway involvement, including detection of parenchymal or structural abnormalities (i.e. emphysema and bronchiectasis) [35].
Moreover, several studies performed in the pediatric setting, show that CT combined with acccurate clinical indices demonstrated high diagnostic accuracy for OSA (Obstructive Sleep Apnea Syndrome) [46].
To accurately assess nasal pathology, an initial endoscopic examination is essential, as it provides direct visualization of the disease and enables the clinician to perform a biopsy if necessary. However, while nasal endoscopy is essential for diagnosis and clinical monitoring, it is limited in its ability to assess the deeper paranasal sinuses, particularly the frontal, sphenoidal, and posterior ethmoidal sinuses. Therefore, imaging is required to obtain a complete evaluation of disease burden. In patients being considered for biologic therapy for severe, uncontrolled CRSwNP, maxillofacial CT without contrast, is particularly valuable because it quantifies disease with imaging evidence, as the Lund-Mackay score and documents the extent of previous surgery via the Amsterdam Classification of Completeness of Endoscopic Sinus Surgery (ACCESS) score—two metrics that help confirm indication and establish a baseline [47,48]
A different and more detailed variant of the Lund-Mackay system is the Zinreich Score, which uses the same anatomical regions but applies a more granular scale, ranging from 0 to 5 for each sinus: 0 = no opacification; 5 = complete opacification. This scoring method offers greater sensitivity in detecting subtle changes over time, making it particularly useful in longitudinal studies or detailed clinical trials. However, due to its complexity, the Zinreich Score is less commonly used in routine clinical practice [49].
In the context of use of biologic therapy, CT must help to exclude alternative diagnoses and detect post-surgical complications such as cerebrospinal fluid (CSF) leaks—reported after FESS. EPOS/EUFOREA 2023 focusing response assessment on endoscopy, symptoms, smell, systemic steroid/salvage surgery needs, and comorbidities, incorporating CT-based measures (e.g., LMS and ACCESS) could provide objective outcome tracking and enhance safety monitoring in severe, uncontrolled type-2 CRSwNP. Emerging radiomics and artificial-intelligence tools may further standardize objective CT evaluation in this setting [47].
Therefore, CT scan remains the better methology for evaluating nasal anatomy and sinonasal disease, together with fibre-optic rhinoscopy, due to its high spatial resolution and capacity to easily delineate bone structures.
On the other hand, magnetic resonance imaging (MRI), plays an important complementary role in discriminating inflammatory tissue, retained secretions in sinus, and neoplastic lesions, due to its better soft tissue contrast.
An interesting and less common use of imaging techniques, particularly CT is the interconnection between upper and lower airway severity of diseases. Ethmoidal sinuses and ostiomeatal complexes are more ofter affected in patients with mild asthma, whereas maxillary, frontal, and sphenoidal sinuses result mostly involved in severe asthma [50].
- b. Allergy and Laboratory Tests:
Skin prick testing, serum specific IgE, and peripheral eosinophil counts help define allergic and eosinophilic phenotypes [2,35].
Diagnosis and management UAD require an integrated approach that includes diagnostic tests to identify different phenotypes, particularly allergic and eosinophilic ones.
Diagnosis of allergies is based on a combined series of clinical, laboratory, and molecular tests.
Skin prick tests and the measurement of specific IgE in the blood remain the most used tests to identify allergic sensitization [51]. Third level tests use modern technologies (ImmunoCAP, microarray, multiplex test) allowing multiple allergens to be evaluated simultaneously. CRD (Component Resolved Diagnosis) tests identify the specific allergenic molecules responsible for the reaction, distinguishing between true and cross-reactive allergens, improving risk stratification and personalization of therapy Cellular functional tests. The Basophil Activation Test (BAT) and the Mast Cell Activation Test (MAT) are in vitro tests that evaluate the cellular response to allergens, useful for monitoring the effectiveness of therapies or in doubtful cases, but not routinarly used to identify a sensibilization
The count of eosinophils principally in in blood but also available in sputum, is a useful biomarker for diagnosis, phenotype detection and therapeutic choice [52]. Eosinophilic airway diseases present heterogeneous phenotypes such as eosinophilic asthma, nasal polyposis, eosinophilic COPD, ABPA, EGPA [53,54,55].
The advantages of the aforementioned methods guarantee, in addition to greater diagnostic accuracy, the possibility of personalizing the therapy with the approach “treatable traits” by identifying and treating specific traits (eosinophilic inflammation, allergic sensitization, etc.) through targeted tests, abandoning the old therapeutic constructs and moving towards more modern precision medicine. The limits linked to complex interpretation, high costs and the need for standardization of procedures remain, but new horizons are opening which will include the need for collaboration between allergists, laboratory workers and clinicians.
- c. Pulmonary Function Testing (PFT):
Spirometry remains a pivotal element for the evaluation of lung function in airway pathologies and can be associated to other simple functional tests to better detect small airway dysfunction and early-stage disease (i.e. IOS, FOT).
in the combination of PFT and other test is crucial for the management of the UAD diseases. In a 2019 study, it sought to determine differences in asthma control (ASTHMA Control Questionnaire ACQ-6), lung function (spirometry), and T2 biomarkers (FeNO and Eos) in relation to the presence of allergic rhinitis in patients with allergic asthma: the result was that subjects with allergic asthma and allergic rhinitis showed much lower predicted FEV1% and predicted FEF25-75% than those with asthma alone, indicating worse lung function and significant type 2 inflammation.
Although spirometry is widely used, it is not completely precise to detect small airway pathology; and the only use of normal spirometry may also not be well correlated with the patient's symptoms. The use of pulse oscillometry (IOS) and forced oscillation technique (FOT) are more sensitive to detect small airway dysfunctionadn appears to be easil. IOS can, for example detect, better than normal spirometry, the presence of small airway disfunction, in patients with normal spirometry values, but remained symptomatic [56]. Spirometry resulted also crucial in the management of severe asthmatic patients, in order to evaluate the concept of clinical remission, requiring usually a stabilization of FEV1 or an improve upper than 80% [57].
- d. Biomarkers:
Fractional exhaled nitric oxide (FeNO) is validated a non-invasive marker of type 2 inflammation [2,35] reflecting IL-4/IL-13 induced processes in the upper and lower airways, particularly the action of IL-13. Elevated FeNO levels are associated with T2 inflammation and, for this reason just in asthma and can help to classify patients as T2-high or T2-low phenotype. Despite its utility, FeNO alone could not be sufficient to completely distinguish airway disease phenotypes, particularly in severe or complex cases. In fact, its levels, as the one of eosinophils may be influenced by factors such as comorbidity, corticosteroid use and environmental exposure, and it may not reliably distinguish all patients with low T2 levels.
Biomarkers used routinely, such as peripheral eosinophilia, total IgE or exhaled nitric oxide, are, even if combined, not completely satisfactory in distinguishing the different phenotypes of type 2 asthma, particularly in the context of severe asthma where the problem of choosing the most effective biological drug arises.
The analysis of sputum inflammatory cells is considered the most specific biomarker in discriminating eosinophilic inflammation in asthma and therefore considered the most reliable in clinical trials and research models. However, it has also demonstrated numerous limitations in clinical applicability. For this reason, therefore, there is the increasing need to identify further biomarkers; recent studies, indeed, have emphasized the potential role of microRNAs and nasal methylome signatures as emerging biomarkers in united airway disease, because their involvement in my inflammatory diseases. Although there is a growing number of studies about the miRNAs’ role in inflammatory diseases of the upper and lower airways, few of them have represented a connection between these two regions [15]. The nasal cellular epigenome can serve as a biomarker of airway pathologies and environmental response. A 2019 study, conducted on 547 children show that nasal DNA methylation is linked to asthma, allergy and airway inflammation. Asthma, IgE and FeNO were found to be associated with the acceleration of nasal epigenetic aging, revealing the nasal epigenome as a sensitive biomarker of airway diseases and [58].
Combining FeNO with other biomarkers such as eosinophilic blood counts, total IgE, transcriptomic or epigenetic markers, would improve diagnostic accuracy, phenotyping, disease monitoring and therapeutic response [59,60].
- e. Histopathology:
The concept of United Airways Diseases (UAD) is also supported by histopathological and molecular evidence: the nasal and bronchial epithelium constitute, indeed, a functional and immunological continuum. Damaged epithelium releases cytokines (TSLP, IL 25, IL 33), that activated dendritic cells and trigger the Th2 and ILC2’s responses along the rhiho-bronchial axis, justifying an integrated diagnostic and therapeutic approach across pulmonology, allergology, and otolaryngology [2,61]. In Th2 high phenotypes, nasal and bronchial tissue show an eosinophilic infiltration, goblet cell hyperplasia with mucus hypersecretion, basement membrane thickening, and signs of epithelial remodeling [62,63]. In contrast, in patients that show bronchiectasis, there is a predominantly neutrophilic inflammation, with epithelial necrosis and destruction of the bronchial wall. In patients with both asthma and bronchiectasis, a mixed eosinophilic-neutrophilic pattern is observed [64].
When the non-invasive biomarkers are inconclusive to detect the underlying inflammatory pattern, tissue biopsy might be performed and may guide the choice between inhaled corticosteroids, antibiotics, or targeted biological therapies [2,35] The Interasma (Global Asthma Association) recommends the reciprocal evaluation of upper and lower airways in patients with rhinitis or rhinosinusitis to ensure timely diagnosis and integrated management [2]. [65,66,67] Other noninvasive tools could be represented by exhaled breath condensate (EBC) and nasal transcriptomic. [4,68].
The UAD approach therefore requires integrated pathways that maximize therapeutic precision, minimize ineffective treatments, and optimize functional outcomes and quality of life.
5. Management Strategies
About pulmonary management, the primary goal should be to ensure good control of symptoms, reduce inflammation, and prevent exacerbations in the aim of reducing the use of OCS. Inhaled corticosteroids represent the cornerstone therapy which should be administered at the lowest effective dose [69]. Diagnosis and monitoring include spirometry with bronchodilator testing, peak expiratory flow diaries, and bronchial provocation tests when indicated [70]. In patients whose condition is poorly controlled despite maximum therapy or who are dependent on steroid treatment, the initiation of biological therapy should be considered, chosen based on biomarkers [71,72,73]. Induced sputum analysis (eosinophilia >3%) [66,74] and non-invasive tools (FeNO, exhaled breath condensate) help distinguish type 2 high inflammation from type 2 low forms [65,68].
On the nasal front, however, it is essential to optimize topical treatment with topical corticosteroids and nasal washes. When medical therapy is insufficient or anatomy restricts drug delivery, endoscopic sinus surgery is indicated.
A stepwise program is obviously necessary, involving a series of progressively more extensive actions for the management and subsequent follow-up of upper and lower respiratory tract diseases, which also includes the assessment and subsequent therapeutic management of associated comorbidities (GERD, bronchiectasis, AERD) [69,70]. Patient education and adherence to therapy are of crucial relevance, as well as the implementation of a structured follow-up program in which patient-reported outcomes (PROs) are evaluated using appropriate validated tools.
6. Multidisciplinary Care:
As previously discussed, the management of UAD should be multidisciplinary and involve different experts for a comprehensive assessment of the upper and lower respiratory tract, combining medical, biological and surgical strategies. The aim of these shared evaluation should be the decreasing of the number of exacerbations, the need of OCS and the revision surgery. The guidelines embrace this cross-airway approach: the GINA 2025 update highlights the impact of comorbid rhinosinusitis/nasal polyposis on asthma control and recommends systematic upper-airway evaluation, while EPOS/EUFOREA 2023 delineates indications and response criteria for biologics in CRSwNP and encourages shared biomarker use and joint follow-up [75]. As evidence of this, in patients with CRSwNP and asthma, the medical and surgical outcome of the nasal condition is closely linked to the severity of the bronchial condition: severe asthma is associated with higher polyp recurrence, more revision surgery, and smaller gains in smell and global symptoms after ESS [76]. On the other hand, treating nasal conditions (with topical or biological therapy) improves asthma symptom control and respiratory function [77].
Treat UAD as one disease expressed in two compartments—co-assess, co-manage, and co-monitor—using guideline-aligned, biomarker-informed, and surgery-enabled strategies tailored to endotype and disease burden. Emerging integrative reviews and translational work continue to validate this unified model [29].
7. Pharmacotherapy:
- Intranasal Corticosteroids and Associations with Antihistamines:
Intranasal corticosteroids (INCS) are first-line therapy for the treatment of allergic rhinitis and chronic rhinosinusitis with nasal polyps (CRSwNP), reducing type-2 inflammation, mucosal edema, polyp size, nasal obstruction, rhinorrhea, and smell impairment, with a positive effect on lower airways [6,7,10]. Administration of these drugs should be started early and maintained long term, seeking to optimize administration through patient education and nasal irrigation [10].
Second-generation nasal steroids are highly effective, maintaining low systemic bioavailability even with prolonged use. Variability in response to this treatment can be attributed to endotypes: non-T2 patients respond well, while those with eosinophilic inflammation may require additional therapies. [2,10].
Advanced delivery systems (steroid-eluting implants, exhalation-delivery sprays) and high-volume, low-pressure steroid irrigation can optimize and improve outcomes, especially on postoperative interventions and polyp regrowth in the immediate healing phase [29,78], with better result in SNOT-22 and endoscopic scores [10]. Even when biologics are introduced, INCS remain the local anti-inflammatory backbone pre- and post-operatively to minimize systemic corticosteroid exposure and maintain disease control over time [1,7,10].
- b. Inhaled Corticosteroids:
ICS are the cornerstone of asthma treatment, as they are essential for reducing airway inflammation. Treatment should be tailored to the patient using biomarkers and respiratory function as indicators, always maintaining the minimum effective treatment. Inhaled steroid therapy has proven to be highly effective, reducing exacerbations by 50% compared to bronchodilator therapy alone. In addition, therapeutic strategies such as MART (maintenance and reliever therapy) with ICS–formoterol offer rapid anti-inflammatory coverage during symptoms and reduce hospitalizations and the use of oral OCS [79,80]. ICS efficacy depends, also, on practical aspects: verification of inhalation technique, use of spacers in patients not able to use MDI, adherence monitoring, and surveillance for local and systemic effects [80]. More often ICS are associated with long acting beta agonists (LABA), to improve bronchodilation. The use of ICS is also effective on the nasal mucosa thanks to systemic diffusion and retrograde mucociliary drainage. [2,36]. Moreover, segmental bronchial provocation studies have shown that inflammation induced in the bronchi can extend to the nasal mucosa, highlighting the bidirectionality of the inflammatory process [81].
- c. Antimuscarinics (LAMA)
In addition to ICS/LABA, in asthmatic patients, the use of LAMA is suggested in GINA and other international guidelines, due to their bronchodilation action and the low anti-inflammatory effect on lower airways [82].
- d. Oral Corticosteroids:
In the treatment of CRSwNP, OCS are reserved for severe flare-ups or cases that are refractory to therapy, after optimization of the latter. The aim of this treatment is to provide rapid relief from symptoms when needed, while limiting cumulative systemic exposure. Although they are effective in reducing the size of polyps and improving symptom control and quality of life, their effect is temporary and wears off within 3-6 months [10]. OCS represent a fundamental therapeutic option in the treatment of asthma exacerbations, increasing bronchodilation and suppressing inflammation, reducing hospitalization and the risk of recurrence [83]. Considering the short- and long-term risks of using these drugs, the guidelines suggest a steroid-sparing approach, resorting to endoscopic surgery or biological drugs in patients who need to undergo a course of OCS twice a year. [10]. Therefore, OCS should be limited to short, carefully timed courses, with shared decision-making and longitudinal monitoring of cumulative exposure.
- e. Antibiotics:
Indicated for acute bacterial exacerbations or chronic infection, particularly in bronchiectasis [11,36]. Up to 85% of sinusitis cases resolve spontaneously within 7-15 days, without the need for antibiotic therapy. This therapy should therefore be reserved for severe cases, with symptoms persisting for more than 10 days, and for patients who show a worsening of symptoms after an initial improvement. According to the 2025 AAO-HNSF guidelines, first-line antibiotics are amoxicillin-clavulanate for 5-10 days, followed by doxycycline or fluoroquinolones for those who are hypersensitive to penicillin. However, the use of macrolides is not recommended due to the high resistance rate of S. pneumoniae. [84,85,86].
In patients with COPD, asthma, and bronchiectasis, the choice of antibiotic therapy should be based on clinical and microbiological evidence to avoid resistance and microbial alterations. In chronic or treatment-resistant forms, endoscopy with targeted cultures can enable the selection of a more precise and effective treatment [17,87,88,89].
In patients with bronchiectasis, chronic infection fuels a cycle of inflammation, colonization, and structural damage, resulting in clinical manifestations. Generally, in the event of an exacerbation, amoxicillin/clavulanate is again the first choice. Infection with Pseudomonas aeruginosa has a poor prognosis and, when detected for the first time, requires eradication with systemic and inhaled therapy (mainly fluoroquinolones), while in cases of chronic colonization, inhaled antibiotic therapy (tobramycin, colistin) is required. In cases where non-tuberculous mycobacteria are isolated, long-term treatment (12 months after sputum negativity) is indicated and requires targeted antibiotic therapy (macrolide + rifampicin + ethambutol) [17,90,91].
In patients with bronchiectasis and sinonasal comorbidities, integrated infection management may improve both respiratory and ENT outcomes.
- f. Biologic Therapies:
The introduction of biologics (Omalizumab, Mepolizumab, Benralizumab, Dupilumab and Tezepelumab) has decisively changed the management of patients with severe asthma, significantly reducing exacerbations and the use of OCS, and improving respiratory function and quality of life, allowing for a personalized approach based on biomarkers (FeNO, eosinophil count, IgE). Biological therapy acts on key cytokines (IL-5, IL-5R, IL-4R, TSLP) that orchestrate the inflammatory response and act on both the upper and lower respiratory tract. [14,36]. Recent studies have confirmed that the efficacy of these biologics extends to the upper airways: Benralizumab and Mepolizumab have demonstrated significant reductions in nasal inflammation and SNOT 22 scores in patients with comorbid CRSwNP [5,14].
For treatment of CRSwNP we should follow the international guidelines Epos Euforea, following the strict conditions for prescription [92] and keep the patients in a strict follow-up during the first Targeted biologics have demonstrated efficacy in both upper and lower airway disease, reducing exacerbations, improving control, and decreasing the need for systemic corticosteroids and surgery. This has been demonstrated during phase III trials [93,94], but also during real life studies [95]. Reviews emphasize that blockade of IL-4/IL-13 and IL-5 pathways not only improves sinonasal outcomes—such as nasal polyp score, congestion, and olfactory function—but also exerts parallel benefits on comorbid asthma, reinforcing the unified airway concept, reducing the use of OCS and the need for EES [96].
- g. Allergen-Specific Immunotherapy:
Specific immunotherapy (AIT) is a targeted therapeutic strategy for patients suffering from allergic rhinitis, chronic rhinosinusitis, and bronchial asthma, associated with documented allergic sensitization and persistent symptoms despite drug therapy. By modulating type 2 inflammation along the nasobronchial axis, AIT improves the symptoms of rhinitis and asthma, reduces bronchial hyperresponsiveness, the use of drugs, and the number of exacerbations, with benefits in terms of quality of life and airway remodeling. [97,98]
Allergen-specific immunotherapy has also been shown to prevent the onset of bronchial asthma and is currently the only therapy that modifies the natural course of the disease. International guidelines also recommend its use in patients with documented sensitization to the allergen, with specific IgE findings, clinically relevant symptoms, and a suboptimal response to conventional therapy, after exclusion of contraindications [2,26,99].
- h. New Targeted Therapies:
In the context of United Airways Diseases (UAD), there is growing interest in other specific therapies for patients who do not respond adequately to conventional treatments. Among these, JAK inhibitors and synthetic peptides represent an emerging therapeutic alternative, capable of reducing inflammation and immune dysregulation along the nasobronchial axis.
Because JAK inhibitors block signaling through the IL-4, IL-5, IL-13, and TSLP cytokines by inhibiting the JAK-STAT pathway, these drugs reduce activation of eosinophils, mast cells, and effector T cells, inhibiting JAK-STAT pathway, essential for activate the signaling of IL-4, IL-5, IL-13, and TSLP cytokines. Agents such as tofacitinib, baricitinib, and ruxolitinib are currently under investigation for severe eosinophilic asthma and chronic rhinosinusitis with nasal polyposis, with promising results in reducing inflammation, improving lung function, and alleviating nasal symptoms, especially in patients with mixed phenotypes or systemic comorbidities [37].
Synthetic peptides and peptidomimetics are emerging as innovative therapies interfering with protein–protein interactions driving immune activation and mucosal inflammation. Among the experimental candidates, antagonists of CXCL10 (eldelumab), anti-TSLP peptides, and mimetics of IL-13Rα1 have demonstrated, in preclinical studies, the ability to reduce eosinophilic infiltrate, mucus secretion, and bronchial hyperreactivity, suggesting benefits for both upper and lower airways [37].
Biomarker discovery and omics technologies in the future will guide personalized use of JAK inhibitors and peptide therapies, thus widening the options for refractory UAD and promoting standards of multidisciplinary care.
- i.
- Surgical Interventions:
ESS is indicated for those patients with CRSwNP who are uncontrolled despite optimized medical therapy, including INCS, short courses of oral corticosteroids and saline irrigation. The principal goals of ESS are to restore sinus ventilation and drainage and to improve the delivery of topical medications, particularly postoperative INCS, with remains the standard of care [7,10]. Beyond an improvement in nasal symptoms, ESS has been shown to improve lower airway outcomes with concomitant asthma, thus supporting the concept of UAD. Patients with eosinophilic CRSwNP and asthma demonstrated a significant reduction in type 2 inflammatory markers after ESS. The blood eosinophils and FeNO levels decreased markedly, while lung function (FEV₁) and asthma control showed improvements [100]. Higher pre-operative tissue eosinophilia and serum periostin have been associated with larger postoperative gains and fewer exacerbations, suggesting a role for biomarkers in prognostication and shared decision-making [101,102].
However, surgical outcomes vary widely between individuals, and polyp recurrence is still frequent, especially in patients with type 2 disease and those with severe asthma. This shows that surgery is just one part of long-term, multidisciplinary management and not a definitive cure [6,7]. When it comes to the extent of surgery, there is no universal consensus on the best approach for chronic rhinosinusitis with nasal polyps (CRSwNP) within the united airway disease framework. Surgical options range from limited and targeted procedures (such as uncinectomy with middle meatal antrostomy, with or without a limited ethmoidectomy), up to complete endoscopic sinus surgery (involving the opening of all paranasal sinus ostia and full ethmoidectomy). The decision depends on factors such as polyp burden, individual anatomy, previous surgeries, and the presence of asthma. However, few studies directly compare limited and complete surgical approaches in terms of lower airway outcomes, so practices can vary significantly between centers [102].
In our experience, when a patient has extensive nasal polyps and all the paranasal sinuses are blocked, we define a complete ESS as opening all the sinus passages — this includes making larger openings in the maxillary, ethmoid (both front and back), frontal, and sphenoid sinuses. The goal is to help restore normal airflow, improve the natural cleaning process, and make it easier for topical treatments to reach all areas. We also often remove part of the middle turbinate to keep the middle nasal passage clear, make aftercare easier, and lower the risk of scar tissue forming [103,104].
The introduction of biologic drugs (targeting IL-4Rα, IL-5/IL-5R, or IgE) has changed the way we decide on treatment. Clinical studies show that, for patients already using nasal steroid sprays, biologics can significantly reduce the need for initial or repeat sinus surgery. They also help shrink polyps, clear up sinus blockages, improve a patient’s sense of smell, and boost overall quality of life. For patients with asthma, these benefits extend to better asthma control. In practice, possible treatment approaches include: (i) starting with biologics in patients who are likely to have a recurrence or have severe asthma alongside their sinus disease; (ii) starting with surgery first if the polyps are so extensive that they block access for topical treatments—then following up with regular nasal steroid sprays and considering biologics if symptoms persist. No matter the path, a common goal is to avoid giving patients too many courses of systemic steroids, which can have serious side effects. [1,7,10].
- j. Non-Pharmacologic Measures:
In the management of chronic rhinosinusitis type 2 with nasal polyposis, several non-pharmacological strategies play a relevant role as important adjuncts for long-term disease control. One of the best-established is nasal saline irrigation. International guidelines [92] recommend its regular use because of its low risk profile, low cost, and ability to improve obstructive symptoms and mucociliary clearance [10]
A Cochrane review confirmed a symptomatic benefit in CRS patients treated with saline irrigation, particularly when delivered as high-volume, low-pressure solutions. Such methods are more effective than standard sprays, including in post-surgical contexts, where they contribute to better endoscopic and radiological outcomes at follow-up [10] In their trial Harvey et al, such as Chakapan Promsopa et al, demonstrated that topical intranasal corticosteroids get better results in controlling symptoms in post-surgical patients [105] and also in non-surgical patients [106].
Other behavioral measures include allergen avoidance and smoking cessation. Continuous exposure to aeroallergens can amplify type 2 inflammation, while cigarette smoke worsens respiratory function and accelerates FEV1 decline. It is important to get a correct nasal irrigation also for getting away allergens from the nose and, in this way, lower the type 2 driven inflammation, lowering also asthma symptoms [10].
Another critical aspect is patient education. Usually, it is important to show the patients the exact method they should use when using nasal irrigation and topical intranasal sprays: if not well explained, if not performed correctly, patients may not benefit from local therapy or may even lose adherence to treatment completely.
8. Precision Medicine and Treatable Traits
The treatable traits (TT) paradigm advocates for the identification and targeted management of specific, modifiable disease mechanisms and risk factors, rather than a syndromic approach. The concept of TT currently represents an emerging paradigm for the management of airway diseases that goes beyond the definition of a single disease, but allows the identification of clinical, behavioral, and pathophysiological aspects on which to act with targeted therapeutic interventions. This approach allows for a multimodal assessment of bronchial asthma, but also its main comorbidities, such as AR, CRS, and CRSwNP, fitting fully within the concept of UADs. [107,108].
9. Research Gaps and Future Directions
Despite advances, significant gaps remain in the understanding and management of UAD. There is a paucity of high-quality studies specifically addressing integrated treatment strategies, optimal use of biomarkers, and long-term outcomes in patients with overlapping airway diseases. Future research priorities include [13,37] elucidation of the molecular and microbial mechanisms linking upper and lower airway inflammation [15,29,37]development and validation of biomarkers for diagnosis, phenotyping, and monitoring response to therapy [13,35,37], evaluation of novel therapeutics, including JAK inhibitors and synthetic peptides, in refractory UAD [37] and implementation of multidisciplinary care models and real-world studies to assess the impact of integrated management on patient outcomes. [2,4,13].
Abbreviations
The following abbreviations are used in this manuscript:
| ABPA | Allergic Bronchopulmonary Aspergillosis |
| ACCESS | Amsterdam Classification of Completeness of Endoscopic Sinus Surgery |
| ACQ-6 | Asthma Control Questionnaire-6 |
| AERD | Aspirin-Exacerbated Respiratory Disease |
| AIT | Allergen-Specific Immunotherapy |
| AR | Allergic Rhinitis |
| BAT | Basophil Activation Test |
| COPD | Chronic Obstructive Pulmonary Disease |
| CRD | Component Resolved Diagnosis |
| CRSsNP | Chronic Rhinosinusitis without Nasal Polyps |
| CRSwNP | Chronic Rhinosinusitis with Nasal Polyps |
| CSF | Cerebrospinal Fluid |
| CT | Computed Tomography |
| EBC | Exhaled Breath Condensate |
| EGPA | Eosinophilic Granulomatosis with Polyangiitis |
| Eos | Eosinophils |
| EPOS/EUFOREA | European Position Paper on Rhinosinusitis and Nasal Polyps / European Forum for Research and Education in Allergy and Airway Diseases |
| ESS | Endoscopic Sinus Surgery |
| FEF25-75% | Forced Expiratory Flow at 25–75% of Vital Capacity |
| FeNO | Fractional exhaled Nitric Oxide |
| FEV1% | Forced Expiratory Volume in 1 second (percentuale del predetto) |
| GERD | Gastroesophageal Reflux Disease |
| GINA | Global Initiative for Asthma |
| ICS | Inhaled Corticosteroids |
| IgE | Immunoglobulins E |
| IL-4, IL-5, IL-13 | Interleukin-4, Interleukin-5, Interleukin-13 (citokines) |
| IL-4R | Interleukin-4 Receptor |
| IL-4Rα | Interleukin-4 Receptor alpha |
| IL-5R | Interleukin-5 Receptor |
| ILC2s | Type 2 Innate Lymphoid Cells |
| INCS | Intranasal Corticosteroids |
| IOS | Impulse Oscillometry (o Spirometria con Tecnica di Oscillazione) |
| JAK | Janus Kinase (inibitori) |
| LABA | Long-Acting Beta Agonist |
| LAMA | Long-Acting Muscarinic Antagonist |
| LMS | Lund-Mackay Score |
| MART | Maintenance and Reliever Therapy |
| MAT | Mast Cell Activation Test |
| MDI | Metered-Dose Inhaler |
| MRI | Magnetic Resonance Imaging |
| OCS | Oral Corticosteroids |
| OSA | Obstructive Sleep Apnea Syndrome |
| PFT | Pulmonary Function Testing |
| PROs | Patient-Reported Outcomes |
| SNOT-22 | Sino-Nasal Outcome Test-22 (score) |
| STAT | Signal Transducer and Activator of Transcription |
| T2 | Type 2 (Inflammation) |
| Th2 | T helper type 2 (cells) |
| TSLP | Thymic Stromal Lymphopoietin (citokine) |
| TT | Treatable Traits |
| UAD | United Airway Disease |
References
- Domínguez-Ortega, J.; Mullol, J.; Álvarez Gutiérrez, F.J.; Miguel-Blanco, C.; Castillo, J.A.; Olaguibel, J.M.; Blanco-Aparicio, M. The Effect of Biologics in Lung Function and Quality of Life of Patients with United Airways Disease: A Systematic Review. The Journal of Allergy and Clinical Immunology: Global 2024, 3. [Google Scholar] [CrossRef]
- Tiotiu, A.; Novakova, P.; Baiardini, I.; Bikov, A.; Chong-Neto, H.; de-Sousa, J.C.; Emelyanov, A.; Heffler, E.; Fogelbach, G.G.; Kowal, K.; et al. Manifesto on United Airways Diseases (UAD): An Interasma (Global Asthma Association - GAA) Document. J Asthma 2022, 59, 639–654. [Google Scholar] [CrossRef]
- Yii, A.C.A.; Tay, T.R.; Choo, X.N.; Koh, M.S.Y.; Tee, A.K.H.; Wang, D.Y. Precision Medicine in United Airways Disease: A “Treatable Traits” Approach. Allergy 2018, 73, 1964–1978. [Google Scholar] [CrossRef]
- Fokkens, W.; Reitsma, S. Unified Airway Disease: A Contemporary Review and Introduction. Otolaryngol Clin North Am 2023, 56, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bachert, C.; Luong, A.U.; Gevaert, P.; Mullol, J.; Smith, S.G.; Silver, J.; Sousa, A.R.; Howarth, P.H.; Benson, V.S.; Mayer, B.; et al. The Unified Airway Hypothesis: Evidence From Specific Intervention With Anti-IL-5 Biologic Therapy. J Allergy Clin Immunol Pract 2023, 11, 2630–2641. [Google Scholar] [CrossRef]
- Laidlaw, T.M.; Mullol, J.; Woessner, K.M.; Amin, N.; Mannent, L.P. Chronic Rhinosinusitis with Nasal Polyps and Asthma. J Allergy Clin Immunol Pract 2021, 9, 1133–1141. [Google Scholar] [CrossRef]
- Hong, H.; Liao, S.; Chen, F.; Yang, Q.; Wang, D.Y. Role of IL-25, IL-33, and TSLP in Triggering United Airway Diseases toward Type 2 Inflammation. Allergy 2020, 75, 2794–2804. [Google Scholar] [CrossRef]
- Bachert, C.; Luong, A.U.; Gevaert, P.; Mullol, J.; Smith, S.G.; Silver, J.; Sousa, A.R.; Howarth, P.H.; Benson, V.S.; Mayer, B.; et al. The Unified Airway Hypothesis: Evidence From Specific Intervention With Anti–IL-5 Biologic Therapy. Journal of Allergy and Clinical Immunology: In Practice 2023, 11, 2630–2641. [Google Scholar] [CrossRef] [PubMed]
- Asano, T.; Takemura, M.; Kanemitsu, Y.; Yokota, M.; Fukumitsu, K.; Takeda, N.; Ichikawa, H.; Hijikata, H.; Uemura, T.; Takakuwa, O.; et al. Combined Measurements of Fractional Exhaled Nitric Oxide and Nasal Nitric Oxide Levels for Assessing Upper Airway Diseases in Asthmatic Patients. Journal of Asthma 2018, 55, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Yii, A.C.A.; Tay, T.R.; Choo, X.N.; Koh, M.S.Y.; Tee, A.K.H.; Wang, D.Y. Precision Medicine in United Airways Disease: A “Treatable Traits” Approach. Allergy: European Journal of Allergy and Clinical Immunology 2018, 73, 1964–1978. [Google Scholar] [CrossRef]
- Relationship of Upper Airways Disorders to FEV1 and Bronchial Hyperresponsiveness in an Epidemiological Study - PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/1426221/ (accessed on 15 October 2025).
- Giombi, F.; Pace, G.M.; Pirola, F.; Cerasuolo, M.; Ferreli, F.; Mercante, G.; Spriano, G.; Canonica, G.W.; Heffler, E.; Ferri, S.; et al. Airways Type-2 Related Disorders: Multiorgan, Systemic or Syndemic Disease? Int J Mol Sci 2024, 25. [Google Scholar] [CrossRef] [PubMed]
- Mullol, J.; Maldonado, M.; Castillo, J.A.; Miguel-Blanco, C.; Dávila, I.; Domínguez-Ortega, J.; Blanco-Aparicio, M. Management of United Airway Disease Focused on Patients With Asthma and Chronic Rhinosinusitis With Nasal Polyps: A Systematic Review. J Allergy Clin Immunol Pract 2022, 10, 2438–2447. [Google Scholar] [CrossRef]
- Mehta, M.P.; Wise, S.K. Unified Airway Disease: Examining Prevalence and Treatment of Upper Airway Eosinophilic Disease with Comorbid Asthma. Otolaryngol Clin North Am 2023, 56, 65–81. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Zhang, X.H.; Callejas-Díaz, B.; Mullol, J. MicroRNA in United Airway Diseases. Int J Mol Sci 2016, 17. [Google Scholar] [CrossRef]
- Shteinberg, M.; Nassrallah, N.; Jrbashyan, J.; Uri, N.; Stein, N.; Adir, Y. Upper Airway Involvement in Bronchiectasis Is Marked by Early Onset and Allergic Features. ERJ Open Res 2018, 4. [Google Scholar] [CrossRef]
- Polverino, E.; Dimakou, K.; Hurst, J.; Martinez-Garcia, M.A.; Miravitlles, M.; Paggiaro, P.; Shteinberg, M.; Aliberti, S.; Chalmers, J.D. The Overlap between Bronchiectasis and Chronic Airway Diseases: State of the Art and Future Directions. Eur Respir J 2018, 52. [Google Scholar] [CrossRef]
- Gao, T.; Cai, Q.; Hu, S.; Zhu, R.; Wang, J. Causal Associations between Pediatric Asthma and United Airways Disease: A Two-Sample Mendelian Randomization Analysis. Front Med (Lausanne) 2024, 11. [Google Scholar] [CrossRef]
- Ryu, G.; Min, C.; Park, B.; Choi, H.G.; Mo, J.H. Bidirectional Association between Asthma and Chronic Rhinosinusitis: Two Longitudinal Follow-up Studies Using a National Sample Cohort. Sci Rep 2020, 10. [Google Scholar] [CrossRef]
- Egan, M.; Bunyavanich, S. Allergic Rhinitis: The “Ghost Diagnosis” in Patients with Asthma. Asthma Res Pract 2015, 1, 8. [Google Scholar] [CrossRef]
- Feng, C.H.; Miller, M.D.; Simon, R.A. The United Allergic Airway: Connections between Allergic Rhinitis, Asthma, and Chronic Sinusitis. Am J Rhinol Allergy 2012, 26, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Passalacqua, G.; Ciprandi, G.; Canonica, G.W. The Nose-Lung Interaction in Allergic Rhinitis and Asthma: United Airways Disease. Curr Opin Allergy Clin Immunol 2001, 1, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Giavina-Bianchi, P.; Vivolo Aun, M.; Takejima, P.; Kalil, J.; Agondi, R.C. United Airway Disease: Current Perspectives. J Asthma Allergy 2016, 9, 93–100. [Google Scholar] [CrossRef]
- Lombardi, C.; Canevari, R.F.; Bagnasco, D.; Bilò, M.B.; Canonica, G.W.; Caruso, C.; Castelnuovo, P.; Cecchi, L.; Calcinoni, O.; Carone, M.; et al. ARIA-Italy Multidisciplinary Consensus on Nasal Polyposis and Biological Treatments: Update 2025. World Allergy Organ J 2025, 18. [Google Scholar] [CrossRef]
- Khan, D.A. Allergic Rhinitis and Asthma: Epidemiology and Common Pathophysiology. Allergy Asthma Proc 2014, 35, 357–361. [Google Scholar] [CrossRef]
- Passalacqua, G.; Canonica, G.W. Treating the Allergic Patient: Think Globally, Treat Globally. Allergy 2002, 57, 876–883. [Google Scholar] [CrossRef]
- Naydenova, K.; Dimitrov, V.; Velikova, T. Immunological and MicroRNA Features of Allergic Rhinitis in the Context of United Airway Disease. Sinusitis 2021, Vol. 5, Pages 45-52 2021, 5, 45–52. [Google Scholar] [CrossRef]
- Nikolić, M.Z.; Sun, D.; Rawlins, E.L. Human Lung Development: Recent Progress and New Challenges. Development (Cambridge) 2018, 145. [Google Scholar] [CrossRef]
- Xu, X.; Yin, J.; Yang, Y.; Liu, H.; Yu, J.; Luo, X.; Zhang, Y.; Song, X. Advances in Co-Pathogenesis of the United Airway Diseases. Respir Med 2024, 225. [Google Scholar] [CrossRef] [PubMed]
- Kanda, A.; Kobayashi, Y.; Asako, M.; Tomoda, K.; Kawauchi, H.; Iwai, H. Regulation of Interaction between the Upper and Lower Airways in United Airway Disease. Med Sci (Basel) 2019, 7. [Google Scholar] [CrossRef] [PubMed]
- Klain, A.; Indolfi, C.; Dinardo, G.; Licari, A.; Cardinale, F.; Caffarelli, C.; Manti, S.; Ricci, G.; Pingitore, G.; Tosca, M.; et al. United Airway Disease. Acta Bio Medica : Atenei Parmensis 2021, 92, e2021526. [Google Scholar] [CrossRef]
- Hong, H.; Liao, S.; Chen, F.; Yang, Q.; Wang, D.Y. Role of IL-25, IL-33, and TSLP in Triggering United Airway Diseases toward Type 2 Inflammation. Allergy 2020, 75, 2794–2804. [Google Scholar] [CrossRef]
- Maspero, J.; Adir, Y.; Al-Ahmad, M.; Celis-Preciado, C.A.; Colodenco, F.D.; Giavina-Bianchi, P.; Lababidi, H.; Ledanois, O.; Mahoub, B.; Perng, D.W.; et al. Type 2 Inflammation in Asthma and Other Airway Diseases. ERJ Open Res 2022, 8. [Google Scholar] [CrossRef]
- Furue, M.; Ulzii, D.; Vu, Y.H.; Tsuji, G.; Kido-Nakahara, M.; Nakahara, T. Pathogenesis of Atopic Dermatitis: Current Paradigm. Iran J Immunol 2019, 16, 97–107. [Google Scholar] [CrossRef]
- Miglani, A.; Lal, D.; Divekar, R.D. Unified Airway Disease: Diagnosis and Subtyping. Otolaryngol Clin North Am 2023, 56, 11–22. [Google Scholar] [CrossRef]
- Shamil, E.; Hopkins, C. Unified Airway Disease: Medical Management. Otolaryngol Clin North Am 2023, 56, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, J.G.; Marino, M.J.; Luong, A.U. Unified Airway Disease: Future Directions. Otolaryngol Clin North Am 2023, 56, 181–195. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.W.Q.; Sim, W.L.; Cheong, J.K.; Kuan, W. Sen; Tran, T.; Lim, H.F. MicroRNAs in Chronic Airway Diseases: Clinical Correlation and Translational Applications. Pharmacol Res 2020, 160. [Google Scholar] [CrossRef]
- Kuruvilla, M.E.; Lee, F.E.H.; Lee, G.B. Understanding Asthma Phenotypes, Endotypes, and Mechanisms of Disease. Clin Rev Allergy Immunol 2019, 56, 219. [Google Scholar] [CrossRef] [PubMed]
- Ricciardolo, F.L.M.; Sprio, A.E.; Baroso, A.; Gallo, F.; Riccardi, E.; Bertolini, F.; Carriero, V.; Arrigo, E.; Ciprandi, G. Characterization of T2-Low and T2-High Asthma Phenotypes in Real-Life. Biomedicines 2021, 9. [Google Scholar] [CrossRef]
- Heaney, L.G.; Perez de Llano, L.; Al-Ahmad, M.; Backer, V.; Busby, J.; Canonica, G.W.; Christoff, G.C.; Cosio, B.G.; FitzGerald, J.M.; Heffler, E.; et al. Eosinophilic and Noneosinophilic Asthma: An Expert Consensus Framework to Characterize Phenotypes in a Global Real-Life Severe Asthma Cohort. Chest 2021, 160, 814–830. [Google Scholar] [CrossRef]
- Chung, K.F.; Dixey, P.; Abubakar-Waziri, H.; Bhavsar, P.; Patel, P.H.; Guo, S.; Ji, Y. Characteristics, Phenotypes, Mechanisms and Management of Severe Asthma. Chin Med J (Engl) 2022, 135, 1141–1155. [Google Scholar] [CrossRef]
- Agache, I. Severe Asthma Phenotypes and Endotypes. Semin Immunol 2019, 46. [Google Scholar] [CrossRef]
- Kaur, R.; Chupp, G. Phenotypes and Endotypes of Adult Asthma: Moving toward Precision Medicine. J Allergy Clin Immunol 2019, 144, 1–12. [Google Scholar] [CrossRef] [PubMed]
- De Greve, G.; Hellings, P.W.; Fokkens, W.J.; Pugin, B.; Steelant, B.; Seys, S.F. Endotype-Driven Treatment in Chronic Upper Airway Diseases. Clin Transl Allergy 2017, 7. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Gu, M.; Zhang, X.; Wen, M.; Li, R.; Wang, Y.; Li, C.; Wang, X.; Yang, R.; Xiao, X. Diagnostic Value of Upper Airway Morphological Data Based on CT Volume Scanning Combined with Clinical Indexes in Children with Obstructive Sleep Apnea Syndrome. Front Med (Lausanne) 2023, 10. [Google Scholar] [CrossRef]
- Bertolini, M.; Bagnasco, D.; Canevari, F.R.M. Should Computed Tomography Be Used in the Evaluation of Biologic Therapies for Severe Chronic Rhinosinusitis with Nasal Polyps? Acta Otorhinolaryngol Ital 2025, 45, 296–298. [Google Scholar] [CrossRef] [PubMed]
- Lund, V.J.; Kennedy, D.W. Staging for Rhinosinusitis. Otolaryngol Head Neck Surg 1997, 117. [Google Scholar] [CrossRef]
- Zinreich, S.J. Imaging for Staging of Rhinosinusitis. Ann Otol Rhinol Laryngol Suppl 2004, 193, 19–23. [Google Scholar] [CrossRef]
- Adapinar, B.; Kurt, E.; Kebapçi, M.; Erginel, M.S. Computed Tomography Evaluation of Paranasal Sinuses in Asthma: Is There a Tendency of Particular Site Involvement? Allergy Asthma Proc 2006, 27, 504–509. [Google Scholar] [CrossRef]
- Ansotegui, I.J.; Melioli, G.; Canonica, G.W.; Caraballo, L.; Villa, E.; Ebisawa, M.; Passalacqua, G.; Savi, E.; Ebo, D.; Gómez, R.M.; et al. IgE Allergy Diagnostics and Other Relevant Tests in Allergy, a World Allergy Organization Position Paper. World Allergy Organ J 2020, 13. [Google Scholar] [CrossRef]
- Carr, T.F.; Berdnikovs, S.; Simon, H.U.; Bochner, B.S.; Rosenwasser, L.J. Eosinophilic Bioactivities in Severe Asthma. World Allergy Organ J 2016, 9. [Google Scholar] [CrossRef]
- Dodig, S.; Čepelak, I. The Potential of Component-Resolved Diagnosis in Laboratory Diagnostics of Allergy. Biochem Med (Zagreb) 2018, 28. [Google Scholar] [CrossRef]
- Hemmings, O.; Kwok, M.; McKendry, R.; Santos, A.F. Basophil Activation Test: Old and New Applications in Allergy. Curr Allergy Asthma Rep 2018, 18. [Google Scholar] [CrossRef]
- Bahri, R.; Custovic, A.; Korosec, P.; Tsoumani, M.; Barron, M.; Wu, J.; Sayers, R.; Weimann, A.; Ruiz-Garcia, M.; Patel, N.; et al. Mast Cell Activation Test in the Diagnosis of Allergic Disease and Anaphylaxis. J Allergy Clin Immunol 2018, 142, 485–496. [Google Scholar] [CrossRef]
- Cottini, M.; Bondi, B.; Bagnasco, D.; Braido, F.; Passalacqua, G.; Licini, A.; Lombardi, C.; Berti, A.; Comberiati, P.; Landi, M.; et al. Impulse Oscillometry Defined Small Airway Dysfunction in Asthmatic Patients with Normal Spirometry: Prevalence, Clinical Associations, and Impact on Asthma Control. Respir Med 2023, 218. [Google Scholar] [CrossRef]
- Canonica, G.W.; Blasi, F.; Carpagnano, G.E.; Guida, G.; Heffler, E.; Paggiaro, P. Journal Pre-Proof SANI Definition of Clinical Remission in Severe Asthma: A Delphi Consensus. I: In Practice The Journal of Allergy and Clinical Immunology, 2023. [Google Scholar] [CrossRef]
- Cardenas, A.; Sordillo, J.E.; Rifas-Shiman, S.L.; Chung, W.; Liang, L.; Coull, B.A.; Hivert, M.F.; Lai, P.S.; Forno, E.; Celedón, J.C.; et al. The Nasal Methylome as a Biomarker of Asthma and Airway Inflammation in Children. Nat Commun 2019, 10. [Google Scholar] [CrossRef]
- Guida, G.; Bagnasco, D.; Carriero, V.; Bertolini, F.; Ricciardolo, F.L.M.; Nicola, S.; Brussino, L.; Nappi, E.; Paoletti, G.; Canonica, G.W.; et al. Critical Evaluation of Asthma Biomarkers in Clinical Practice. Front Med (Lausanne) 2022, 9. [Google Scholar] [CrossRef] [PubMed]
- Cottin, S.; Doyen, V.; Pilette, C. Upper Airway Disease Diagnosis as a Predictive Biomarker of Therapeutic Response to Biologics in Severe Asthma. Front Med (Lausanne) 2023, 10, 1129300. [Google Scholar] [CrossRef] [PubMed]
- Lambrecht, B.N.; Hammad, H. The Airway Epithelium in Asthma. Nat Med 2012, 18, 684–692. [Google Scholar] [CrossRef] [PubMed]
- Jeffery, P.K. Remodeling in Asthma and Chronic Obstructive Lung Disease. Am J Respir Crit Care Med 2001, 164. [Google Scholar] [CrossRef]
- Van Crombruggen, K.; Zhang, N.; Gevaert, P.; Tomassen, P.; Bachert, C. Pathogenesis of Chronic Rhinosinusitis: Inflammation. J Allergy Clin Immunol 2011, 128, 728–732. [Google Scholar] [CrossRef]
- Shoemark, A.; Shteinberg, M.; De Soyza, A.; Haworth, C.S.; Richardson, H.; Gao, Y.; Perea, L.; Dicker, A.J.; Goeminne, P.C.; Cant, E.; et al. Characterization of Eosinophilic Bronchiectasis: A European Multicohort Study. Am J Respir Crit Care Med 2022, 205, 894–902. [Google Scholar] [CrossRef]
- Dweik, R.A.; Boggs, P.B.; Erzurum, S.C.; Irvin, C.G.; Leigh, M.W.; Lundberg, J.O.; Olin, A.C.; Plummer, A.L.; Taylor, D.R. An Official ATS Clinical Practice Guideline: Interpretation of Exhaled Nitric Oxide Levels (FeNO) for Clinical Applications. Am J Respir Crit Care Med 2011, 184, 602. [Google Scholar] [CrossRef]
- Simpson, J.L.; Scott, R.; Boyle, M.J.; Gibson, P.G. Inflammatory Subtypes in Asthma: Assessment and Identification Using Induced Sputum. Respirology 2006, 11, 54–61. [Google Scholar] [CrossRef]
- Long, M.B.; Chotirmall, S.H.; Shteinberg, M.; Chalmers, J.D. Rethinking Bronchiectasis as an Inflammatory Disease. Lancet Respir Med 2024, 12, 901–914. [Google Scholar] [CrossRef]
- Horváth, I.; Hunt, J.; Barnes, P.J.; Alving, K.; Antczak, A.; Baraldi, E.; Becher, G.; van Beurden, W.J.C.; Corradi, M.; Dekhuijzen, R.; et al. Exhaled Breath Condensate: Methodological Recommendations and Unresolved Questions. Eur Respir J 2005, 26, 523–548. [Google Scholar] [CrossRef]
- Holguin, F.; Cardet, J.C.; Chung, K.F.; Diver, S.; Ferreira, D.S.; Fitzpatrick, A.; Gaga, M.; Kellermeyer, L.; Khurana, S.; Knight, S.; et al. Management of Severe Asthma: A European Respiratory Society/American Thoracic Society Guideline. Eur Respir J 2020, 55. [Google Scholar] [CrossRef]
- Reddel, H.K.; Taylor, D.R.; Bateman, E.D.; Boulet, L.P.; Boushey, H.A.; Busse, W.W.; Casale, T.B.; Chanez, P.; Enright, P.L.; Gibson, P.G.; et al. An Official American Thoracic Society/European Respiratory Society Statement: Asthma Control and Exacerbations: Standardizing Endpoints for Clinical Asthma Trials and Clinical Practice. Am J Respir Crit Care Med 2009, 180, 59–99. [Google Scholar] [CrossRef] [PubMed]
- Ortega, H.G.; Liu, M.C.; Pavord, I.D.; Brusselle, G.G.; FitzGerald, J.M.; Chetta, A.; Humbert, M.; Katz, L.E.; Keene, O.N.; Yancey, S.W.; et al. Mepolizumab Treatment in Patients with Severe Eosinophilic Asthma. N Engl J Med 2014, 371, 1198–1207. [Google Scholar] [CrossRef] [PubMed]
- Bleecker, E.R.; FitzGerald, J.M.; Chanez, P.; Papi, A.; Weinstein, S.F.; Barker, P.; Sproule, S.; Gilmartin, G.; Aurivillius, M.; Werkström, V.; et al. Efficacy and Safety of Benralizumab for Patients with Severe Asthma Uncontrolled with High-Dosage Inhaled Corticosteroids and Long-Acting Β2-Agonists (SIROCCO): A Randomised, Multicentre, Placebo-Controlled Phase 3 Trial. Lancet 2016, 388, 2115–2127. [Google Scholar] [CrossRef] [PubMed]
- Menzies-Gow, A.; Corren, J.; Bourdin, A.; Chupp, G.; Israel, E.; Wechsler, M.E.; Brightling, C.E.; Griffiths, J.M.; Hellqvist, Å.; Bowen, K.; et al. Tezepelumab in Adults and Adolescents with Severe, Uncontrolled Asthma. N Engl J Med 2021, 384, 1800–1809. [Google Scholar] [CrossRef]
- Chalmers, J.D.; Aliberti, S.; Blasi, F. Management of Bronchiectasis in Adults. Eur Respir J 2015, 45, 1446–1462. [Google Scholar] [CrossRef]
- Venkatesan, P. 2025 GINA Report for Asthma. Lancet Respir Med 2025, 13, e41–e42. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Yan, M.; Li, C.; Zhao, J.; Liu, Y.; Yang, X.; Zeng, X.; Nie, Z.; Ke, Z.; Zhang, W.; et al. Impact of Asthma Severity on Surgical Outcomes in Patients with Chronic Rhinosinusitis Comorbid with Asthma. Ann Allergy Asthma Immunol 2025, 134, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Gill, A.S.; Alt, J.A.; Detwiller, K.Y.; Rowan, N.R.; Gray, S.T.; Hellings, P.W.; Joshi, S.R.; Lee, J.T.; Soler, Z.M.; Tan, B.K.; et al. Management Paradigms for Chronic Rhinosinusitis in Individuals with Asthma: An Evidence-Based Review with Recommendations. Int Forum Allergy Rhinol 2023, 13, 1758–1782. [Google Scholar] [CrossRef] [PubMed]
- Bertazzoni, G.; Conti, C.; Testa, G.; Pipolo, G.C.; Mattavelli, D.; Piazza, C.; Pianta, L. High Volume Nasal Irrigations with Steroids for Chronic Rhinosinusitis and Allergic Rhinitis. Eur Arch Otorhinolaryngol 2025, 282, 47–62. [Google Scholar] [CrossRef]
- Staples, K.J. In Asthma, Change Is the Only Constant. Am J Respir Crit Care Med 2025, 211, 141–142. [Google Scholar] [CrossRef]
- Daley-Yates, P.; Singh, D.; Igea, J.M.; Macchia, L.; Verma, M.; Berend, N.; Plank, M. Assessing the Effects of Changing Patterns of Inhaled Corticosteroid Dosing and Adherence with Fluticasone Furoate and Budesonide on Asthma Management. Adv Ther 2023, 40, 4042–4059. [Google Scholar] [CrossRef]
- Braunstahl, G.J.; Kleinjan, A.; Overbeek, S.E.; Prins, J.B.; Hoogsteden, H.C.; Fokkens, W.J. Segmental Bronchial Provocation Induces Nasal Inflammation in Allergic Rhinitis Patients. Am J Respir Crit Care Med 2000, 161, 2051–2057. [Google Scholar] [CrossRef]
- Braido, F.; Tiotiu, A.; Guidos-Fogelbach, G.; Baiardini, I.; Cosini, F.; Correia de Sousa, J.; Bikov, A.; Novakova, S.; Labor, M.; Kaidashev, I.; et al. Manifesto on Inhaled Triple Therapy in Asthma: An Interasma (Global Asthma Association–GAA) Document. Journal of Asthma 2022, 59, 2402–2412. [Google Scholar] [CrossRef]
- Chung, L.P.; Upham, J.W.; Bardin, P.G.; Hew, M. Rational Oral Corticosteroid Use in Adult Severe Asthma: A Narrative Review. Respirology 2019, 25, 161. [Google Scholar] [CrossRef]
- Savage, T.J.; Kronman, M.P. Clarifying the Role of Antibiotics in Acute Sinusitis Treatment. Pediatrics 2024, 153. [Google Scholar] [CrossRef]
- JB, A.; MR, J.; MD, P.; PG, A.; MS, B.; JA, H.; WA, C. Antimicrobial Treatment Guidelines for Acute Bacterial Rhinosinusitis. Otolaryngol Head Neck Surg 2004, 130, 1–45. [Google Scholar] [CrossRef]
- Yoon, Y.K.; Park, C.S.; Kim, J.W.; Hwang, K.; Lee, S.Y.; Kim, T.H.; Park, D.Y.; Kim, H.J.; Kim, D.Y.; Lee, H.J.; et al. Guidelines for the Antibiotic Use in Adults with Acute Upper Respiratory Tract Infections. Infect Chemother 2017, 49, 326–352. [Google Scholar] [CrossRef] [PubMed]
- Loperfido, A.; Cavaliere, C.; Begvarfaj, E.; Ciofalo, A.; D’Erme, G.; De Vincentiis, M.; Greco, A.; Millarelli, S.; Bellocchi, G.; Masieri, S. The Impact of Antibiotics and Steroids on the Nasal Microbiome in Patients with Chronic Rhinosinusitis: A Systematic Review According to PICO Criteria. J Pers Med 2023, 13. [Google Scholar] [CrossRef] [PubMed]
- Psaltis, A.J.; Mackenzie, B.W.; Cope, E.K.; Ramakrishnan, V.R. Unraveling the Role of the Microbiome in Chronic Rhinosinusitis. J Allergy Clin Immunol 2022, 149, 1513–1521. [Google Scholar] [CrossRef]
- Polverino, E.; Goeminne, P.C.; McDonnell, M.J.; Aliberti, S.; Marshall, S.E.; Loebinger, M.R.; Murris, M.; Cantón, R.; Torres, A.; Dimakou, K.; et al. European Respiratory Society Guidelines for the Management of Adult Bronchiectasis. Eur Respir J 2017, 50. [Google Scholar] [CrossRef]
- Chalmers, J.D.; Boersma, W.; Lonergan, M.; Jayaram, L.; Crichton, M.L.; Karalus, N.; Taylor, S.L.; Martin, M.L.; Burr, L.D.; Wong, C.; et al. Long-Term Macrolide Antibiotics for the Treatment of Bronchiectasis in Adults: An Individual Participant Data Meta-Analysis. Lancet Respir Med 2019, 7, 845–854. [Google Scholar] [CrossRef]
- Hill, A.T.; Sullivan, A.L.; Chalmers, J.D.; De Soyza, A.; Stuart Elborn, J.; Andres Floto, R.; Grillo, L.; Gruffydd-Jones, K.; Harvey, A.; Haworth, C.S.; et al. British Thoracic Society Guideline for Bronchiectasis in Adults. Thorax 2019, 74. [Google Scholar] [CrossRef]
- Fokkens, W.J.; Viskens, A.S.; Backer, V.; Conti, D.; de Corso, E.; Gevaert, P.; Scadding, G.K.; Wagemann, M.; Sprekelsen, M.B.; Chaker, A.; et al. EPOS/EUFOREA Update on Indication and Evaluation of Biologics in Chronic Rhinosinusitis with Nasal Polyps 2023. Rhinology 2023, 61, 194–202. [Google Scholar] [CrossRef]
- Han, J.K.; Bachert, C.; Fokkens, W.; Desrosiers, M.; Wagenmann, M.; Lee, S.E.; Smith, S.G.; Martin, N.; Mayer, B.; Yancey, S.W.; et al. Mepolizumab for Chronic Rhinosinusitis with Nasal Polyps (SYNAPSE): A Randomised, Double-Blind, Placebo-Controlled, Phase 3 Trial. Lancet Respir Med 2021, 9, 1141–1153. [Google Scholar] [CrossRef] [PubMed]
- Bachert, C.; Han, J.K.; Desrosiers, M.; Hellings, P.W.; Amin, N.; Lee, S.E.; Mullol, J.; Greos, L.S.; Bosso, J. V.; Laidlaw, T.M.; et al. Efficacy and Safety of Dupilumab in Patients with Severe Chronic Rhinosinusitis with Nasal Polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): Results from Two Multicentre, Randomised, Double-Blind, Placebo-Controlled, Parallel-Group Phase 3 Trials. Lancet 2019, 394, 1638–1650. [Google Scholar] [CrossRef]
- Cai, S.; Xu, S.; Zhao, Y.; Zhang, L. Efficacy and Safety of Biologics for Chronic Rhinosinusitis With Nasal Polyps: A Meta-Analysis of Real-World Evidence. Allergy 2025, 80, 1256–1270. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, M.; Okano, M.; Takeuchi, M.; Sunaga, Y.; Orimo, M.; Ishida, M. Reduction of Rescue Treatment With Dupilumab for Chronic Rhinosinusitis With Nasal Polyps in Japan. Laryngoscope 2025, 135, 3093–3103. [Google Scholar] [CrossRef]
- Scadding, G.K.; Kariyawasam, H.H.; Scadding, G.; Mirakian, R.; Buckley, R.J.; Dixon, T.; Durham, S.R.; Farooque, S.; Jones, N.; Leech, S.; et al. BSACI Guideline for the Diagnosis and Management of Allergic and Non-Allergic Rhinitis (Revised Edition 2017; First Edition 2007). Clin Exp Allergy 2017, 47, 856–889. [Google Scholar] [CrossRef] [PubMed]
- Creticos, P.S.; Gunaydin, F.E.; Nolte, H.; Damask, C.; Durham, S.R. Allergen Immunotherapy: The Evidence Supporting the Efficacy and Safety of Subcutaneous Immunotherapy and Sublingual Forms of Immunotherapy for Allergic Rhinitis/Conjunctivitis and Asthma. J Allergy Clin Immunol Pract 2024, 12, 1415–1427. [Google Scholar] [CrossRef]
- Canonica, G.W.; Bachert, C.; Hellings, P.; Ryan, D.; Valovirta, E.; Wickman, M.; De Beaumont, O.; Bousquet, J. Allergen Immunotherapy (AIT): A Prototype of Precision Medicine. World Allergy Organization Journal 2015, 8. [Google Scholar] [CrossRef]
- Hamada, K.; Oishi, K.; Chikumoto, A.; Murakawa, K.; Ohteru, Y.; Matsuda, K.; Uehara, S.; Suetake, R.; Ohata, S.; Murata, Y.; et al. Impact of Sinus Surgery on Type 2 Airway and Systemic Inflammation in Asthma. Journal of Asthma 2021, 58, 750–758. [Google Scholar] [CrossRef]
- Lee, T.J.; Fu, C.H.; Wang, C.H.; Huang, C.C.; Huang, C.C.; Chang, P.H.; Chen, Y.W.; Wu, C.C.; Wu, C.L.; Kuo, H.P. Impact of Chronic Rhinosinusitis on Severe Asthma Patients. PLoS One 2017, 12, e0171047. [Google Scholar] [CrossRef]
- Kanemitsu, Y.; Kurokawa, R.; Ono, J.; Fukumitsu, K.; Takeda, N.; Fukuda, S.; Uemura, T.; Tajiri, T.; Ohkubo, H.; Maeno, K.; et al. Increased Serum Periostin Levels and Eosinophils in Nasal Polyps Are Associated with the Preventive Effect of Endoscopic Sinus Surgery for Asthma Exacerbations in Chronic Rhinosinusitis Patients. Int Arch Allergy Immunol 2020, 181, 862–870. [Google Scholar] [CrossRef]
- Park, M.J.; Fischer, J.L.; Ramakrishnan, V.R.; Welch, K.C.; Kim, D.Y.; Won, T. Bin; Cho, J.H.; Mun, S.J.; Lee, J.T.; Beswick, D.M.; et al. A Systematic Classification of Surgical Approaches for the Sphenoid Sinus: Establishing a Standardized Nomenclature for Endoscopic Sphenoid Sinus Surgery. Clin Exp Otorhinolaryngol 2025, 18, 109–122. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.; Staibano, P.; Snidvongs, K.; Nguyen, T.B.V.; Sommer, D.D. Extent of Endoscopic Sinus Surgery in Chronic Rhinosinusitis: A Systematic Review and Meta-Analysis. Curr Allergy Asthma Rep 2024, 24, 639–650. [Google Scholar] [CrossRef]
- Harvey, R.J.; Snidvongs, K.; Kalish, L.H.; Oakley, G.M.; Sacks, R. Corticosteroid Nasal Irrigations Are More Effective than Simple Sprays in a Randomized Double-Blinded Placebo-Controlled Trial for Chronic Rhinosinusitis after Sinus Surgery. Int Forum Allergy Rhinol 2018, 8, 461–470. [Google Scholar] [CrossRef]
- Promsopa, C.; Quannuy, T.; Chinpairoj, S.; Kirtsreesakul, V.; Prapaisit, U.; Suwanparin, N. A Randomized, Double-Blind Study Comparing Corticosteroid Irrigations and Nasal Sprays for Polyp Size Reduction in CRSwNP. Laryngoscope 2025, 135, 3550–3555. [Google Scholar] [CrossRef]
- Hiles, S.A.; Gibson, P.G.; Agusti, A.; McDonald, V.M. Treatable Traits That Predict Health Status and Treatment Response in Airway Disease. J Allergy Clin Immunol Pract 2021, 9, 1255–1264. [Google Scholar] [CrossRef] [PubMed]
- Agusti, A.; Gibson, P.G.; McDonald, V.M. Treatable Traits in Airway Disease: From Theory to Practice. J Allergy Clin Immunol Pract 2023, 11, 713–723. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Mechanisms of inflammation in upper and lower airways diseases.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



