Submitted:
08 November 2025
Posted:
12 November 2025
You are already at the latest version
Abstract
Background: Rheumatoid arthritis (RA) is a chronic inflammatory condition affecting joints. It is managed with pharmacological therapies, but it is speculated that dietary intervention may be of significant benefit to patients in helping to manage the condition alongside their medication. This may be mediated through effects on levels of chronic inflammation and thus can influence disease activity. Previous research has indicated the potential of diet to aid in the condition’s management, but a comprehensive review is required to pull together the evidence. Objective: Conduct a systematic review of existing literature on the impact of differing dietary interventions on disease activity and inflammatory status in rheumatoid arthritis patients. Then draw conclusions about the strength of evidence and identify patterns amongst identified papers in a narrative synthesis. Methods: The existing literature was searched according to a pre-determined search strategy, using the databases PubMed, Embase and MEDLINE. Data was then extracted according to a template and results related in a narrative synthesis. Meta-analysis was not conducted. Results: Eight studies, all randomised controlled trials, were included in the review. Outcomes included disease activity score 28 and inflammatory markers such as erythrocyte sedimentation rate and C-reactive protein. Dietary patterns such as an anti-inflammatory diet showed inconclusive evidence with regards to impact on disease outcomes. Strong evidence for the reduction of inflammation and disease activity was demonstrated in studies investigating probiotic supplementation. Conclusion: Results demonstrated the ability of probiotics to have a beneficial impact for RA patients, which may allow healthcare professionals to develop treatment plans and advice including this intervention. However more research should be conducted in different regions and in combination with other interventions to further the understanding of its effects and safety. Other dietary interventions included showed significant associations for some outcomes and not others. Therefore, further research should be conducted to determine whether they are feasible for use in the management of RA patients.
Keywords:
rheumatoid arthritis
; inflammatory arthritis
; arthritis
; diet
; dietary intervention
1. Introduction
2.1. Rheumatoid Arthritis Background and Review Rationale
Rheumatoid arthritis (RA) is a type of chronic inflammatory arthritis characterised by joint pain, swelling and functional disability[5]. It usually presents as a symmetrical polyarthritis[1], meaning it affects multiple joints simultaneously on both sides of the body. It is more prevalent in women[1] and commonly presents in middle age affecting the hands[1], although people of any age can develop RA and it may initiate in other joints[1]. Autoimmune mediated chronic inflammation of the synovial lining of joints and tendon sheaths sustains the condition[6]. It affects 400,000 people in the UK alone[7], and millions more worldwide, causing significant pain and disability for sufferers whilst also presenting a significant burden on healthcare systems (costing the NHS £560 million annually)[8]. Pharmacological interventions have advanced in recent years and decades, becoming the mainstay of treatment for RA[9]. Patients are often prescribed disease modifying anti-rheumatic drugs (DMARDs) such as Methotrexate[9], as a first line, with biologic therapies and corticosteroids as further options[1]. Whilst these interventions have undoubtedly improved patient outcomes, there still exists the downsides of side effects, rigorous monitoring and financial cost of such treatments[1,9]. With this is mind, there has been growing interest in the role that lifestyle plays in the development and severity of chronic autoimmune conditions such as RA.
The aetiology of rheumatoid arthritis is understood to be a combination of genetic susceptibility and environmental factors such as lifestyle[1,10]. Therefore, in recent years a wide range of research has been conducted in order to try and establish to what extent different environmental influences are involved in the pathogenesis of RA and its associated chronic inflammation. One such area of increasing interest is diet. Various studies have explored the effects of specific nutrients, food groups, dietary patterns, and supplementation strategies in modifying the inflammatory response and influencing the course of the disease[4]. Examples such as fibre, pre and probiotic supplementation and fatty acids have received particular attention due to their potential anti-inflammatory effects[11]. The ‘Mediterranean’ diet has been highlighted for similar reasons, being rich in fruits, vegetables, fish and grains[12].
The existing literature therefore contains a variety of interventions, study designs and methodologies to investigate the relationship between diets and disease activity and progression[13]. Previous reviews have addressed the effects of specific dietary interventions on RA, such as the Mediterranean diet[4], and others have addressed effects of diet on specific outcome measures, such as disease activity score or pain. Another review of the literature on this topic is therefore required to investigate a multitude of interventions on both disease activity measures and inflammatory biomarkers to provide a more complete picture of effect on RA. This review aims to pull together the body of knowledge obtained through relevant studies, considering the strengths and limitations of their evidence, in order to draw conclusions about the effectiveness of differing dietary interventions. In addition, this review will discuss any observed gaps in the current literature and the potential clinical implications for any insights ascertained from them. This will allow proposals of further future research to be suggested which will benefit the understanding of nutrition in rheumatoid arthritis generally. This will be of value to healthcare professionals, researchers and sufferers of the condition as such knowledge will help in the development of evidence-based dietary recommendations and strategies to act as adjunctive interventions alongside medication to help best optimise quality of life and wellbeing of patients.
1.2. Aims
The primary aim of the review is to establish if and to what extent different dietary interventions reduce disease activity and inflammatory status in rheumatoid arthritis patients. Other aims include, determining which, if any, inflammatory markers are most affected by dietary intervention and whether there are the same trends in studies using the same, or a similar, intervention.
2.3. Objectives
The primary objective of the review is to determine which dietary interventions are effective, and which are ineffective or less effective, at reducing disease activity and inflammatory status in rheumatoid arthritis patients. This will be achieved through comprehensive analysis of data and findings reported by relevant and eligible studies.
2.4. Hypothesis
Dietary interventions that adopt a general pattern such as the Mediterranean diet or diets excluding various food groups will have a larger effect on disease activity and inflammation than solitary interventions.
3. Methods
3.1. Protocol
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRSIMA) 2020 Checklist provided the basis by which this systematic review was conducted[14].
3.2. Outcomes
The primary outcome was measures of disease activity and inflammation in the body. Scores such as DAS 28 (disease activity score 28) were used, which takes into account the number of swollen and tender joints a patient is experiencing, as can be a useful clinical marker of disease activity[15]. Antibodies such as anti-CCP (anti-cyclic citrullinated peptides) antibodies were also accepted as an outcome measure of disease activity[1]. Secondary outcomes were laboratory markers of inflammation acquired through blood tests. These are considered valid measures of inflammatory status in rheumatoid arthritis patients. These include C-reactive protein (CRP), erythrocyte sedimentation rate (ESR) and inflammatory cytokines such as tumour necrosis factor-alpha and interleukin-6[16].
Other measures of perceived pain and quality of life. Examples include the SF-36 questionnaire[17] which is a survey allowing for quality of life assessment, and using a VAS (visual analogue scale) for pain. Whilst important to consider as potential markers of disease activity, they are not as specific to the aims and objectives of the review as the primary outcomes measured above, and thus were not used in the analysis of results in this review.
3.4. Inclusion Criteria
Studies investigating the impact of dietary interventions on inflammatory status and/or disease progression in rheumatoid arthritis were considered. This includes specific interventions such as supplementation with probiotics, or more general dietary patterns such as the Mediterranean diet. Other criteria included: randomised controlled trial study design, participants with a diagnosis of rheumatoid arthritis based on valid diagnostic criteria[18], studies published in English and not before the year 2013 and outcomes reported that relate to disease activity and/or inflammatory status. For example, inflammatory markers such as C-reactive protein or valid disease activity scores such as DAS 28. Studies were considered if the outcome measures included DAS 28 and at least one inflammatory marker. Joint measures of disease activity inflammation such as DAS 28-ESR and DAS 28-CRP combined scores were accepted as covering both areas. Studies could include patients of any age or gender.
3.5. Exclusion Criteria
Studies not investigating the impact of dietary interventions on rheumatoid arthritis activity, or those that combine a dietary intervention with another unrelated intervention, such as exercise or a pharmacological therapy. Also, reviews, conference abstracts, editorials and letters are excluded alongside study designs other than randomised controlled trial (such as cohort or cross-sectional studies). Studies that recruited rheumatoid arthritis patients that were diagnosed through invalid criteria were also ineligible, as well as those not published in the English language or published before 2013.
3.6. Literature Search Strategy
PubMed, Embase (1974 – present) and MEDLINE (1946 – present) were the databases used for the literature search. They were accessed on 22nd May 2023. Embase and MEDLINE databases were searched simultaneously through Ovid, and PubMed searched separately. A subsequent updated search was not undertaken due to the review being completed within six months of the initial search. The search strategy was put together by the student with the assistance of a supervisor. The PICOS framework[19] formed the basis by which the search strategy was put together (see Figure 1). When searching the databases, relevant terms were identified and combined into the following search string:
(rheumatoid arthritis) AND (diet) AND ((inflammation) OR (inflammatory markers) OR (disease activity))
Filters were applied to the searches. These included only searching for human trials, papers written in the English language and for publications from 2013 to present. De-duplication of search results for Embase and MEDLINE was conducted automatically through Ovid’s software, whereas it was undertaken manually for PubMed.
3.7. Study Selection and Data Extraction
In order to select studies for the review, firstly titles and abstracts of search results were screened. This was performed by the student and a supervisor. Papers that were considered potentially relevant were then sought for retrieval. Screening of the full text was then conducted to determine whether studies were eligible for use in the review. Disagreements were resolved through discussion by the reviewers.
After establishing whether papers sought for retrieval met the inclusion criteria, a final list of papers for use in the review was drawn up. Data extraction was then performed by the student and a supervisor. For papers that had data missing or incomplete, authors were not contacted due to limits on time. The process of data extraction was conducted according to a pre-prepared template (see Appendix 1).
3.8. Risk of Bias Assessment
The Cochrane Risk of Bias Tool 2 (RoB 2) was used to assess risk of bias in the studies[20]. For each paper, five domains of potential bias sources were examined. These were the randomisation process, deviations from intended interventions, missing outcome data, measurement of the outcome and selection of reported result(s). For each domain, a series of ‘signalling questions’ are provided by the RoB 2 tool[20] that are designed to assist in assessing the risk of bias in that area. The questions were answered either ‘yes’, ‘probably yes’, ‘probably no’ or ‘no’. If the answers to all the questions were ‘yes’ in a given domain, then it was judged to be at low risk of bias. If one or more question was answered ‘no’ then it was assigned high risk of bias. If no questions were answered ‘no’, but not all were answered ‘yes’, then unclear risk of bias was given to that domain. Studies containing one or more high risk domain were considered to be at high risk of bias overall, and those that contained unclear risk domains, at moderate risk.
Results
4.1. Study Selection
Eight of the nineteen studies sought for retrieval were included in the review. Therefore, eleven were removed, for which there were several different reasons. Three papers did not report adequate measures of disease activity and inflammation as specified by the inclusion criteria. Three studies considered were published by the same authors, two of which focused on the same intervention. In order to increase heterogeneity in the review, two of the three were excluded. Of the two papers that focused on the same intervention, the older paper was excluded to ensure the most recent evidence was included. The other paper excluded did not report valid outcomes, bringing the total papers excluded for this reason to four. Another seven papers were excluded as they were not randomised controlled trials. Therefore in total eleven papers were excluded, leaving eight for use in the review. The PRISMA flow diagram (Figure 2) summarises the process of study selection[21].
4.2. Study Characteristics
Across the eight trials, a total of 405 participants completed the study periods. Six of the eight studies took the form of a randomised controlled trial, with participants completing one study period in the group they were assigned. Two were randomised crossover trials in which participants took part in both interventions and controls[22,24], with a washout period between. One study sorted participants into three groups[25], with all others using two. The trials took place in four different countries, with a range in geographical location and development. The oldest trial took place in 2013[23] and the most recent in 2022[25], meaning that selected trials ranged across the time period of the literature search. Two studies investigated dietary patterns as their intervention, namely an anti-inflammatory diet[22] and a diet of exclusion (meat, gluten and lactose)[28]. The other six investigated solitary interventions, four of which examined the effect of a single food/nutrient, and two for probiotic supplementation[23,29]. None of the studies took place in hospitals (except for instances of assessment of outcomes – e.g. blood samples for laboratory tests). Five studies specified the level of disease activity of potential participants in the inclusion criteria (four wanted patients with moderate to severe rheumatoid arthritis, and one wanted inactive to moderate). The other three did not state a specific requirement for severity. In addition, five studies used all female participants[23],[24,26,27,28] and even in those that recruited both sexes, males were a small minority. Whilst a greater heterogeneity in this field would have been ideal, the substantial weighting of RA prevalence toward females means the studies would largely be applicable to the patient population as a whole. The key characteristics of the included papers are summarised in Figure 3 .
4.3. Dietary Patterns and Nutrients
The following section address the results of the review with regards to the findings of the included studies. Meta-analysis was considered, however due to the considerable heterogeneity amongst the papers in terms of interventions and outcomes, it was deemed inappropriate as it would lack generalisability.
Anti-Inflammatory Dietary Pattern
One study, Vadell et al (2020) in Sweden, used an anti-inflammatory diet as the intervention for their study[22]. The composition of this diet was similar to the Mediterranean diet. Participants assigned to the intervention group ate fish 3-4 times weekly, legumes, potatoes, whole grain cereals, fruits and low fat dairy products such as yoghurt[22]. They also were provided with juice shots containing Lactobacillus plantarum 299v to be consumed five times weekly[22]. Non-fish meat products were limited to no more than three times a week[22]. The control group ate a typical Swedish diet consisting of the following macronutrient content: 17% protein, 34% fat and 34% carbohydrates[22].
Unadjusted analysis demonstrated a significant decrease in DAS 28-ESR (p=0.012) in the intervention group pre and post diet[22]. The endpoint DAS 28-ESR was also significantly lower in the intervention group when comparing the scores of both groups (p=0.040)[22]. There was a significant decrease in DAS 28-CRP from the intervention (p=0.003)[22], however unlike DAS 28-ESR, the difference in scores between the two groups was not significant (p=0.107)[22]. Also, individual components of the DAS 28-ESR such as ESR and number of tender joints did not show significant differences between the two groups (p=0.155 and 0.565 respectively)[22].
Adjusted analysis was also conducted, using ‘‘a linear mixed model with period, treatment, sequence and baseline value as fixed effects’’. The DAS 28-ESR difference between the two groups was -0.289 (95% confidence interval: -0.652, 0.075) – in other words the intervention group’s score was 0.289 less than the control group[22]. This adjusted analysis difference was not statistically significant (p=0.116)[22]. This study demonstrated the potential of an anti-inflammatory diet to reduce disease activity and inflammation, but not significantly when compared with a typical western diet.
Exclusion of Gluten, Lactose and Red Meat Dietary Pattern
A 2021 study in Italy, Guagnano et al, studied the effect of excluding gluten, lactose and red meat in female patients[28]. The control group maintained a regular, balanced diet. Both groups consumed 1500 calories daily comprised of the following macronutrients: 56% carbohydrates, 16% protein and 28% fats[28]. DAS 28, ESR and hs-CRP were measured before and after the three month study period[28]. The mean DAS 28 did not change in the exclusion group and increased slightly in the control group but this was not statistically significant[28]. Similarly, the ESR in the exclusion group was unchanged (p=0.7535) by the intervention and increased in the control group, again not significantly (p=0.069)[28]. The only significant change was in hs-CRP from 0.7 to 0.5 (p=0.032) in the exclusion group. In the control group the decrease was lesser and non-significant (p=0.306)[28].
Probiotic Supplementation
Two studies investigated the impact of probiotic supplementation. Vaghef-Mehrabany et al observed a significant decrease in DAS 28 in the intervention group, and a significant difference between the two groups (p<0.01) using Lactobacillus casei supplementation[23]. Zamani et al found similar associations, with DAS 28 decreasing significantly by the intervention and between groups also (p<0.001)[29]. This study used Synbiotic capsules, which are a combination of three different bacteria, one of which was L. casei[29]. Both studies were also conducted in Iran[23,29]. Their similar conclusions regarding the disease activity score demonstrates the ability of probiotics to significantly decrease it.
Various inflammatory markers were also measured by the studies. In Zamani et al, the hs-CRP of the placebo group increased significantly (p=0.01)[29], in stark contrast to the Synbiotic group which experienced a statistically significant decrease (p=0.03)[29]. This is similar to Vaghef-Mehrabany et al, which also demonstrated a significant decrease in hs-CRP (p<0.01)[23]. In addition, this study also gathered data on several inflammatory cytokines. Interleukins 10 and 12 (p=0.02, p<0.01, respectively) were decreased significantly by probiotic supplementation, as well as TNF-alpha (p<0.01)[23]. Interleukin 1-beta and interleukin 6 were not changed significantly by the intervention[23].
Blue Mussel
One study, Lindqvist et al (2018), conducted in Sweden investigated the impact of Blue Mussel meat on disease activity[24]. Thirteen different types of dishes were prepared and given to participants to be mixed with meat[24]. The total amount of dishes given to participants over the course of an intervention period was 119[24]. The meat in the intervention group was 75g of Blue Mussel meat and in the control group this was either chicken (80%) or ham or beef meatballs (20%)[24]. The macronutrient proportions of accompanying dishes before meat was added by participants was as follows: 13.5g protein, 20.4g fat, 51.0g carbohydrates, 5.5g fibre[24].
DAS 28 score and inflammatory markers were measured before and after study periods. A DAS 28-CRP combined score was also calculated. For inflammatory markers alone, namely CRP and ESR, the mean decrease was greater in the blue mussel group, however these associations were not significant, with p values of 0.106 and 0.952 respectively[24]. Similarly, mean change in DAS 28 was insignificant between groups (p=0.200)[24]. The only significant association was mean change in DAS 28-CRP, decreasing by 0.50 in the blue mussel group and 0.19 in the control group, yielding a p value of 0.048[24].
Flaxseed
Ghaseminasab-Parizi et al in Iran divided participants into three groups to compare the effects of an anti-inflammatory diet with flaxseed, a regular regional diet with flaxseed and finally a regular diet with wheat[25]. The amount of flaxseed given in the first two groups was 30g daily[25]. The anti-inflammatory diet consisted of consuming fish two to three times weekly and five to six servings of vegetables daily (including legumes). Red meat was limited to three times weekly[25].
Measurements of ESR, CRP and anti-CCP antibodies resulted in non-significant changes between the different groups[25]. In measurements of DAS 28-ESR score, mean decreases after study periods were noted in all three groups. The greatest decrease was -0.87 in the regular diet and flaxseed group and was significant (p=0.001)[25]. In the anti-inflammatory diet/flaxseed group it was -0.48 and wheat group was -0.24[25]. These were insignificant decreases however with p values of 0.057 and 0.110 respectively[25].
Garlic
One study, Moosavian et al in Iran (2020), examined the effects of garlic supplementation[26]. Participants were equally split into two groups (35 in each), one placebo group and one garlic intervention group[26]. Participants in the latter were given two 500mg garlic powder capsules equivalent to 2.5g of fresh garlic[26]. These were taken after lunch with a glass of water. The placebo group did the same however their capsules were 500mg of starch instead[26].
In analysis of mean DAS 28 score, participants in the garlic group experienced a decreased of 0.80 (which was significant; p<0.001) whereas the placebo group decreased by only 0.07 (p=0.651)[26]. The difference between endpoints of the two groups was significant (p<0.001) in analysis of covariance in adjusted model[26]. The co-variants used were age, duration of RA, BMI and energy intake). With regards to inflammatory markers, non-significant changes in both groups were observed for ESR[26]. For CRP, the garlic group decreased significantly (p=0.021) in contrast to the placebo group (p=0.154)[26]. Lastly, TNF-alpha exhibited a similar pattern to CRP with only the garlic group decreasing significantly (p<0.001)[26]. The difference in endpoints between groups was significant for CRP and TNF-alpha (p=0.018 and p<0.001 respectively[26].
Cranberry Juice
A 2019 Brazillian study, Thimotea et al, investigated cranberry juice supplementation[27]. 38 participants were involved, 20 in the intervention group and 18 in the control group[27]. 500ml of cranberry juice per day was consumed by the former for 90 days[27]. Changes in ESR and CRP were non-significant when comparing baseline and endpoint values within each group[27]. Differences in the endpoints between the two groups was also not significant[27]. The DAS 28 median of the groups yielded a significant decrease in the cranberry group from 3.48 at baseline to 2.99 after the study period (p=0.048)[27]. The control group decrease was far smaller (-0.07) and non-significant[27]. The only other significant association was reduction in level of anti-CCP antibodies in the cranberry group (-0.65, p=0.034)[27].
4.4. Safety and Adverse Events
Five studies did not report specific adverse events occurring during the trial. Vadell et al (2020), investigating an anti-inflammatory diet pattern, reported gastrointestinal upset in 29% of participants in the intervention group (compared to 8.7% in the control group)[22]. Constipation, bloating and acid reflux was also reported by some participants in the control group (specific figures were not provided)[22]. Lindqvist et al (2018), reported two teeth injuries from small pieces of blue mussel shell in the intervention group[24]. Guagnano et al (2021) reported non-specific gastrointestinal complaints in 3 participants in their study investigating a diet of excluding lactose, gluten and red meat[28]. Therefore, overall the dietary interventions trialled by papers in this review were largely very well tolerated and safe with a small number of adverse events. It appeared that dietary pattern changes, encompassing range of food groups, had a higher occurrence of adverse complaints from participants than individual nutrient studies.
4.5. Risk of Bias
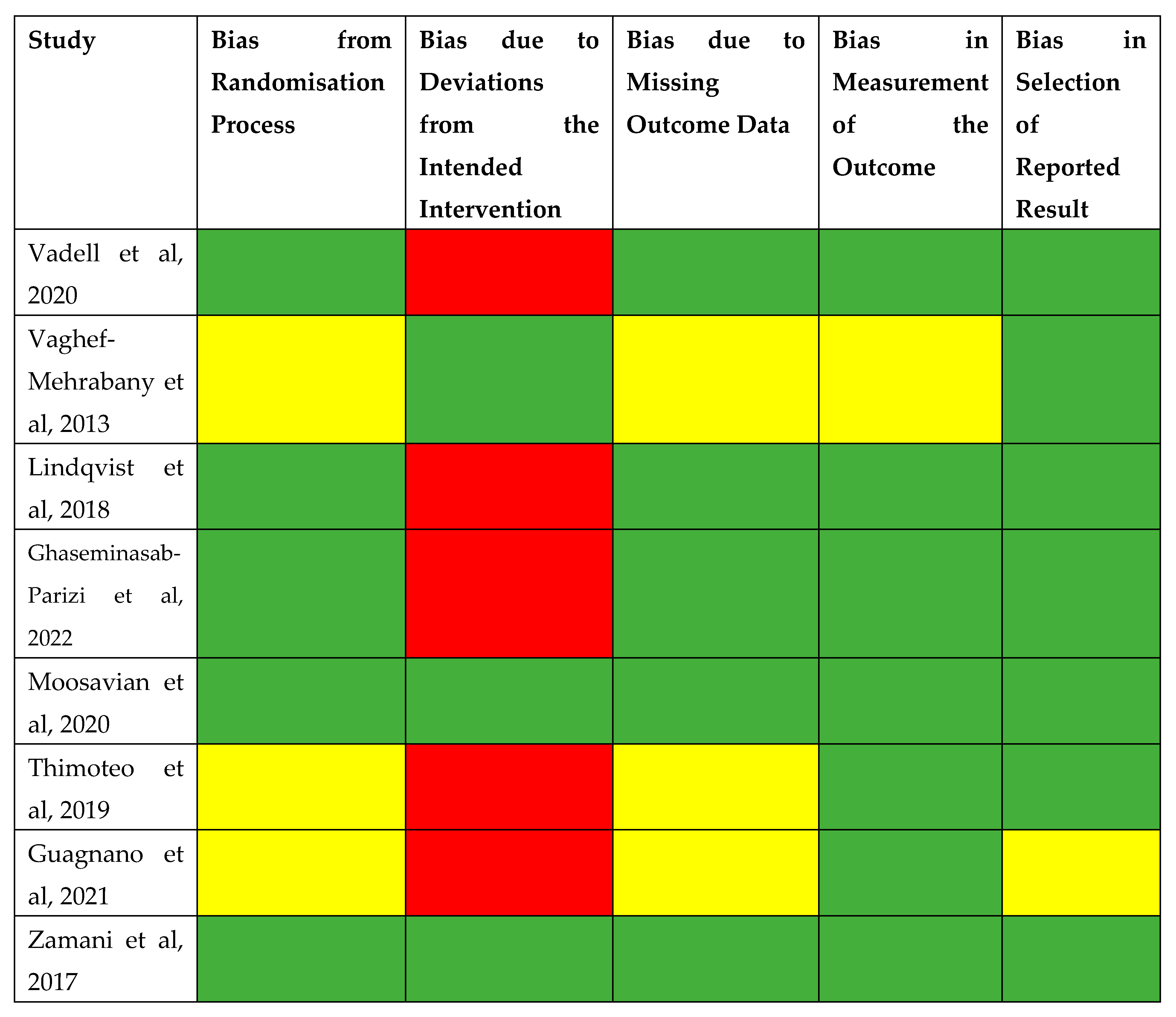
The results of the risk of bias assessment are summarised in Figure 4. Overall, two studies were judged to be at low risk of bias, one was at moderate risk and five were at high risk of bias. For the randomisation process, three studies were given unclear risk of bias due to the method of randomisation not being outlined. Five studies were at high risk of bias in the deviations from intended intervention domain, due to participants being aware of their assigned intervention during the study. Three studies were at unclear risk of bias for missing outcome data. Two studies reported data for all the outcomes but lacked completeness due to missing p values when stating whether associations were significant. One study reported some outcomes graphically without tabular data, making interpretation difficult. One study had unclear bias in measurement of outcome due to stating that ideally repeated measurements would have been taken but was limited due to funding issues. One study had unclear risk of bias in selection of reported results due to a high dropout rate amongst participants.
5. Discussion
5.1. Main Findings
The initial hypothesis for this review predicted that dietary patterns would have a greater beneficial effect on disease activity than solitary interventions with single foods or nutrients. This was shown to be an unfounded hypothesis in this review. Three studies involved investigating dietary patterns (one anti-inflammatory diet study, one exclusion diet and one study combining an anti-inflammatory diet with flaxseed). In each of these, disease activity scores were not decreased significantly[22,25,28]. The studies were conducted across three different countries (Sweden, Italy, Iran) and two of the three involved male patients[22,25], which is it not always the case in rheumatoid arthritis studies. Therefore, the results cover a wide range of demographics of RA sufferers. To conclude, some effect was obtained from these interventions, but they were not shown to be significantly better than a ‘typical’ diet of participants. More research is required on the effect of dietary patterns such as the Mediterranean diet to determine the most effective composition and administration for the best outcomes.
The strongest evidence obtained in this review was for probiotic supplementation. Both studies that investigated this found reductions in disease activity scores and differences in endpoints between study groups that were strongly statistically significant with low p values[23,29]. Vaghef-Mehrabany et al also investigated cytokines and found significant reductions in several pro-inflammatory interleukins[23]. This is in addition to significant reductions in hs-CRP in the intervention groups of both studies[23,29]. The significance of this reduction is highlighted by Zamani et al finding a contrasting increase in hs-CRP in the placebo group[29]. The evidence for the effectiveness of probiotics is also strengthened by the fact that Lactobacillus casei was included in the interventions of both studies[23,29], allowing for valid comparison. Also, both studies were conducted in Iran, reducing the amount of heterogeneity between them further. Overall therefore, supplementing with probiotics was shown to have a statistically significant benefit on both disease activity score and inflammatory markers for rheumatoid arthritis patients, when compared with controls.
Some benefit on disease activity was found from consuming single food interventions such as blue mussel meat[24] and cranberry juice[27]. However, the evidence for these was weaker with insignificant reductions in some of the outcome measures found, especially inflammatory markers such as ESR and CRP[24,27]. Stronger evidence was obtained for garlic consumption as this study accounted for covariance in analysis and found significant reductions in DAS 28 score[26]. However, once more effect on inflammatory markers was limited. Therefore, the impact of single food interventions requires further research to determine the potential of reducing inflammatory markers, as this review demonstrated some effect but limited scope of them to do so.
5.2. Strengths and Limitations
The strengths of this review include the fact that a comprehensive search strategy was adhered to in order to identify the most suitable papers. This, and data extraction, were conducted by two reviewers in order to ensure to reduce chance of human error in the search process. In addition, the Cochrane risk of bias tool was used to evaluate potential sources of bias in the papers. This tool is a widely recognised framework used by many reviews and thus was a suitable method to rigorously check for bias[20]. Also, the review examined several different dietary patterns and nutrient supplementations ensuring that it comprehensively addresses the research question at hand and allows for comparison and contrast between a variety of different interventions. Lastly, all the papers were used are randomised controlled trials ensuring a higher quality of evidence than other study designs.
This review also suffers from some limitations. Firstly, as RA is a disease affecting mostly women, many studies have difficulty recruiting male participants and this review includes five studies that use exclusively female participants. Whilst patients with RA are majority female, it would have been ideal to include more studies that accurately reflect the gender split of RA, with some male participants being included, so that the review is more applicable to patient populations. On a similar note, some of the studies occurred in the same countries as other studies. This risks the results being skewed to geographical regions and ideally a wider spread of nations and regions would have been included. Lastly, due to a large variety of interventions investigated and outcomes measured, there was significant heterogeneity between the studies which prevented pooling of data for meta-analysis that would have strengthened the review.
5.3. Relevance to Clinical Practice and Future Research
This review demonstrated a variety of potential interventions that have the ability to decrease disease activity and inflammation in rheumatoid arthritis. The most effective interventions were probiotic supplements[23,29] and garlic[26], which may have direct implications for formulation of potential future dietary advice for patients, as these would be quick and easy interventions for healthcare professionals to recommend. It is also of note that both these interventions were administered via capsule in these studies[23,26,29]. This was a very rapid and non-disruptive administrative method for participants, in contrast to implementing a new dietary pattern which is more time consuming and may present challenges to participants who are usually used to eating a different composition of foods. The effectiveness of capsules over dietary patterns may be related to this relative ease of compliance. This should be taken into account by clinical practitioners looking to develop effective methods to implement dietary changes.
Of the studies investigating probiotics, both were conducted in Iran, and one used all female participants[23,29]. Therefore, whilst the studies produced strong evidence for the use of probiotics in RA patients, further research should be conducted in different regions and with more male participants to increase the generalisability of this conclusion. In addition, the combination of probiotics with other interventions should be considered by future researchers to determine whether the effect is altered by the influence of other dietary factors.
Appendix
Appendix 1 – Part A: Data Extraction Template
| Study Information | Title |
| Authors | |
| Year & Country | |
| Journal | |
| Study Design | |
| Study Objective | |
| Funding Source | |
| Population | Number of Participants |
| Demographic | |
| Diagnostic Criteria for RA | |
| Inclusion Criteria | |
| Exclusion Criteria | |
| Methods | Setting |
| Duration | |
| Dietary Intervention | |
| Control | |
| Randomisation | |
| Blinding | |
| Assessment of Compliance | |
| Outcome Measures | |
| Assessment of Disease Activity | |
| Assessment of Inflammatory Status | |
| Follow Up Period | |
| Results | Disease Activity Score 28 |
| Inflammatory Markers | |
| Secondary Outcomes | |
| Adverse Events | |
| Conclusion | Key Findings |
| Strengths | |
| Limitations | |
| Implications |
References
- Watchman, T. (no date) Rheumatoid arthritis, Zero To Finals. Available at: https://zerotofinals.com/medicine/rheumatology/ra/.
- Gioia C, Lucchino B, Tarsitano MG, Iannuccelli C, Di Franco M. Dietary Habits and Nutrition in Rheumatoid Arthritis: Can Diet Influence Disease Development and Clinical Manifestations? Nutrients. 2020 May 18;12(5):1456. [CrossRef] [PubMed] [PubMed Central]
- Wong SH, Lord JM. Factors underlying chronic inflammation in rheumatoid arthritis (Nov/Dec 2004) Arch Immunol Ther Exp (Warsz).52(6):379-88. [PubMed]
- Winkvist A, Bärebring L, Gjertsson I, Ellegård L, Lindqvist HM. A randomized controlled cross-over trial investigating the effect of anti-inflammatory diet on disease activity and quality of life in rheumatoid arthritis: the Anti-inflammatory Diet In Rheumatoid Arthritis (ADIRA) study protocol. Nutr J. 2018 Apr 20;17(1):44. [CrossRef] [PubMed] [PubMed Central]
- NHS, Rheumatoid Arthritis (08/03/2023). Available at: https://www.nhs.uk/conditions/rheumatoid-arthritis/.
- Johns Hopkins Arthritis Center, Rheumatoid Arthritis Pathophysioloy (2019). Available at: https://www.hopkinsarthritis.org/arthritis-info/rheumatoid-arthritis/ra-pathophysiology-2/.
- Rheumatoid arthritis (RA) [Internet]. Versus Arthritis. (2022Oct15). Available from: https://www.versusarthritis.org/about-arthritis/conditions/rheumatoid-arthritis/.
- Services for people with rheumatoid arthritis - national audit office (NAO) report [Internet]. National Audit Office (NAO). 2022 (2022Oct19). Available from: https://www.nao.org.uk/reports/services-for-people-with-rheumatoid-arthritis/#:~:text=The%20estimated%20cost%20to%20the,%C2%A31.8%20billion%20a%20year.&text=Rheumatoid%20arthritis%20costs%20the%20NHS%20an%20estimated%20%C2%A3560%20million%20annually.
- Arthrits Foundation, DMARDs (no date) Available at: https://www.arthritis.org/drug-guide/dmards/dmards.
- Johns Hopkins Arthritis Center, Rheumatoid Arthritis Pathophysioloy (2019). Available at: https://www.hopkinsarthritis.org/arthritis-info/rheumatoid-arthritis/ra-pathophysiology-2/.
- Ferro M, Charneca S, Dourado E, Guerreiro CS, Fonseca JE. Probiotic Supplementation for Rheumatoid Arthritis: A Promising Adjuvant Therapy in the Gut Microbiome Era. Front Pharmacol. 2021 Jul 23;12:711788. [CrossRef] [PubMed] [PubMed Central]
- Davis C, Bryan J, Hodgson J, Murphy K. Definition of the Mediterranean Diet; a Literature Review. Nutrients. 2015 Nov 5;7(11):9139-53. [CrossRef] [PubMed] [PubMed Central]
- Philippou E, Petersson SD, Rodomar C, Nikiphorou E. Rheumatoid arthritis and dietary interventions: systematic review of clinical trials. Nutr Rev. (09/03.2021);79(4):410-428. [CrossRef] [PubMed]
- BMJ (OPEN ACCESS) Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. [CrossRef]
- van Riel, PL. The development of the disease activity score (DAS) and the disease activity score using 28 joint counts (DAS28). Clin Exp Rheumatol. 2014 Sep-Oct;32(5 Suppl 85):S-65-74. [PubMed]
- Ansar W, Ghosh S. Inflammation and Inflammatory Diseases, Markers, and Mediators: Role of CRP in Some Inflammatory Diseases. Biology of C Reactive Protein in Health and Disease. 2016 Mar 24:67–107. [CrossRef] [PubMed Central]
- Lins L, Carvalho FM. SF-36 total score as a single measure of health-related quality of life: Scoping review. SAGE Open Med. 2016 Oct 4;4:2050312116671725. [CrossRef] [PubMed] [PubMed Central]
- Jonathan Kay , Katherine S. Upchurch, ACR/EULAR 2010 rheumatoid arthritis classification criteria, Rheumatology, Volume 51, Issue suppl_6, December 2012, Pages vi5–vi9. [CrossRef]
- Eriksen MB, Frandsen TF. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: a systematic review. J Med Libr Assoc. 2018 Oct;106(4):420-431. [CrossRef] [PubMed] [PubMed Central]
- Higgins JPT, Savović J, Page MJ, Elbers RG, Sterne JAC. Chapter 8: Assessing risk of bias in a randomized trial. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.4 (updated August 2023). Cochrane, 2023. Available from www.training.cochrane.org/handbook.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. [CrossRef]
- Vadell AKE, Bärebring L, Hulander E, Gjertsson I, Lindqvist HM, Winkvist A. Anti-inflammatory Diet In Rheumatoid Arthritis (ADIRA)-a randomized, controlled crossover trial indicating effects on disease activity. Am J Clin Nutr. 2020 Jun 1;111(6):1203-1213. [CrossRef] [PubMed] [PubMed Central]
- Vaghef-Mehrabany E, Alipour B, Homayouni-Rad A, Sharif SK, Asghari-Jafarabadi M, Zavvari S. Probiotic supplementation improves inflammatory status in patients with rheumatoid arthritis. Nutrition. 2014 Apr;30(4):430-5. [CrossRef] [PubMed]
- Lindqvist HM, Gjertsson I, Eneljung T, Winkvist A. Influence of Blue Mussel (Mytilus edulis) Intake on Disease Activity in Female Patients with Rheumatoid Arthritis: The MIRA Randomized Cross-Over Dietary Intervention. Nutrients. 2018 Apr 13;10(4):481. [CrossRef] [PubMed] [PubMed Central]
- Ghaseminasab-Parizi M, Nazarinia MA, Akhlaghi M. The effect of flaxseed with or without anti-inflammatory diet in patients with rheumatoid arthritis, a randomized controlled trial. Eur J Nutr. 2022 Apr;61(3):1377-1389. [CrossRef] [PubMed]
- Moosavian SP, Paknahad Z, Habibagahi Z, Maracy M. The effects of garlic (Allium sativum) supplementation on inflammatory biomarkers, fatigue, and clinical symptoms in patients with active rheumatoid arthritis: A randomized, double-blind, placebo-controlled trial. Phytother Res. 2020 Nov;34(11):2953-2962. [CrossRef] [PubMed]
- Thimóteo NSB, Iryioda TMV, Alfieri DF, Rego BEF, Scavuzzi BM, Fatel E, Lozovoy MAB, Simão ANC, Dichi I. Cranberry juice decreases disease activity in women with rheumatoid arthritis. Nutrition. 2019 Apr;60:112-117. [CrossRef] [PubMed]
- Guagnano MT, D'Angelo C, Caniglia D, Di Giovanni P, Celletti E, Sabatini E, Speranza L, Bucci M, Cipollone F, Paganelli R. Improvement of Inflammation and Pain after Three Months' Exclusion Diet in Rheumatoid Arthritis Patients. Nutrients. 2021 Oct 9;13(10):3535. [CrossRef] [PubMed] [PubMed Central]
- Zamani B, Farshbaf S, Golkar HR, Bahmani F, Asemi Z. Synbiotic supplementation and the effects on clinical and metabolic responses in patients with rheumatoid arthritis: a randomised, double-blind, placebo-controlled trial. Br J Nutr. 2017 Apr;117(8):1095-1102. [CrossRef] [PubMed]
Figure 1.
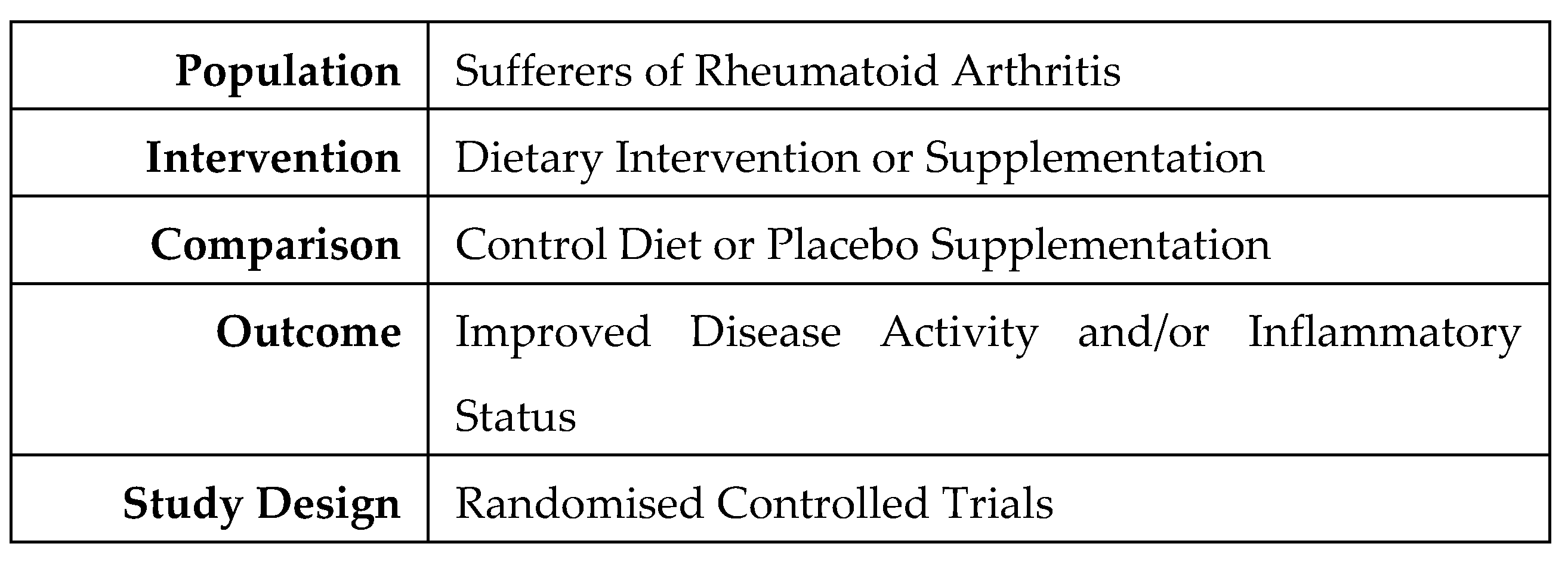
Figure 2.
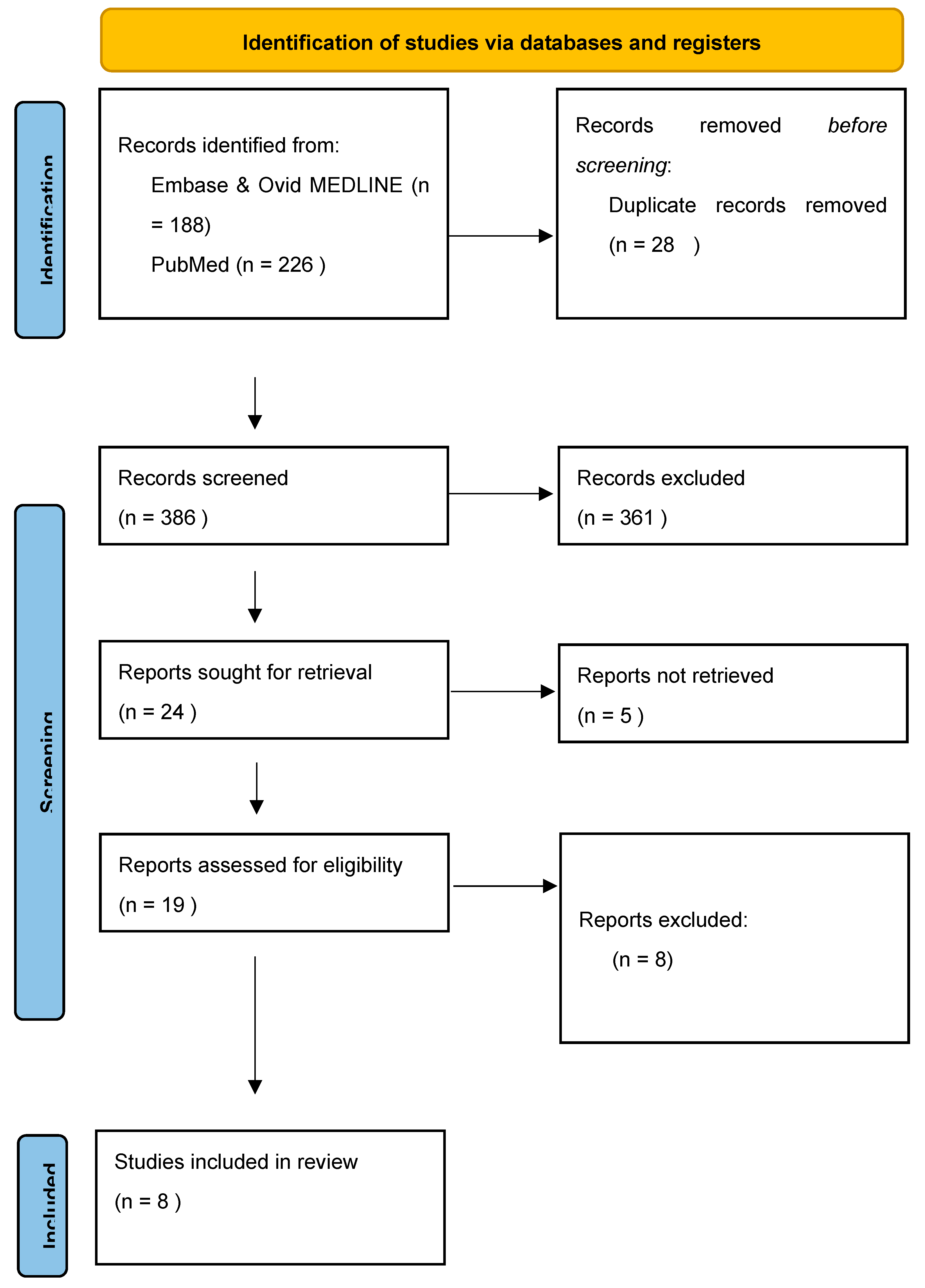
Figure 3.
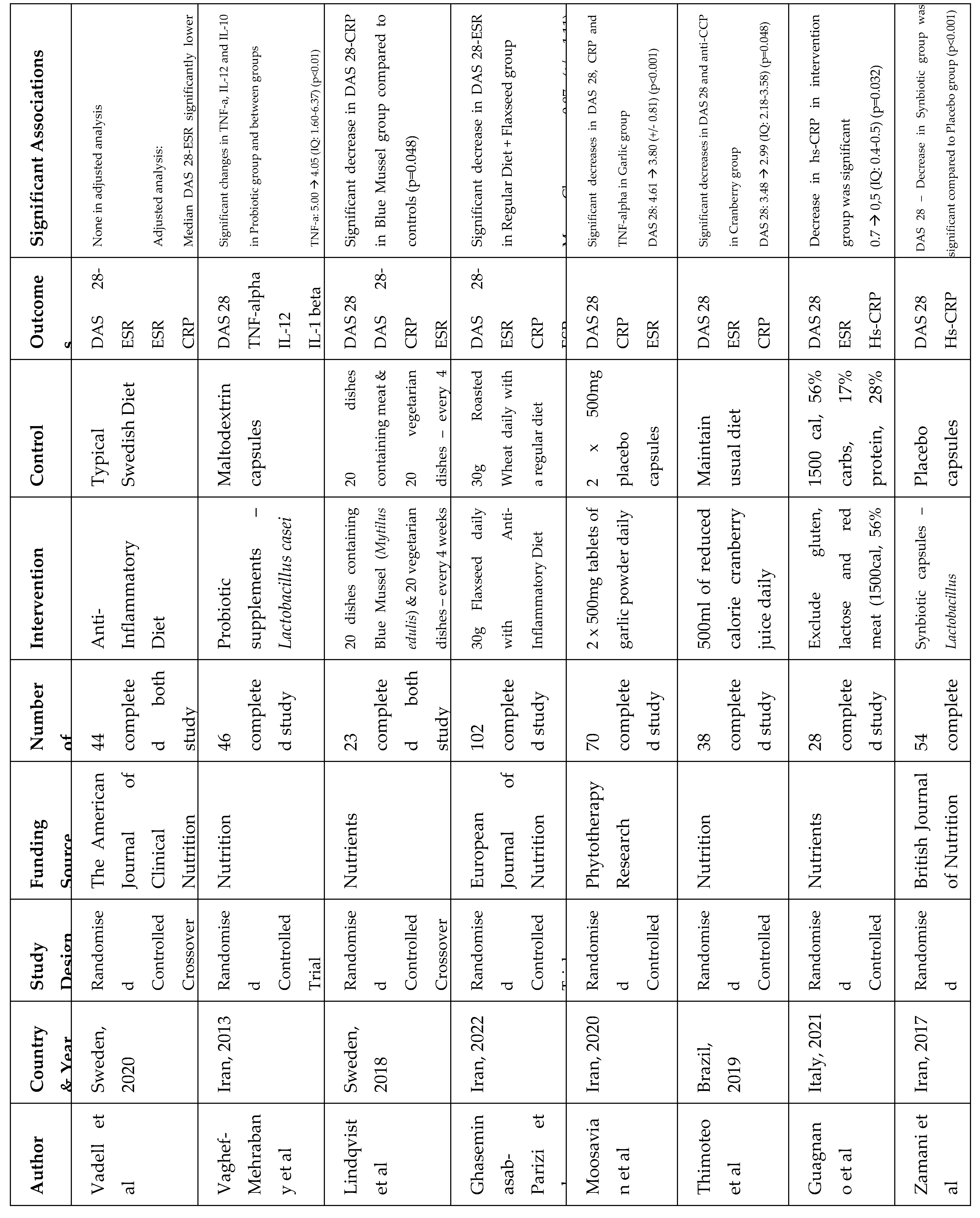
Figure 4.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



