
Submitted:
10 November 2025
Posted:
11 November 2025
You are already at the latest version
Abstract
Background/objectives: Studies evaluating the longitudinal impact (beyond a decade) of Antibiotic stewardship programs (ASP) strategies on the volume/quality of antibiotic prescriptions, as well as impact on antimicrobial resistance are lacking. Since 2008, the ASP at Singapore General Hospital had implemented various strategies in the following phases: 1) initiation; 2) expansion; 3) optimisation; and 4) innovation. In this study, we aim to evaluate the impact of ASP on the volume/quality of antibiotic prescribing and susceptibility trends of clinically significant Gram-negative bacilli (GNB). Methods: We conducted a single-center, retrospective observational study from 2011 to 2024. Antibiotic consumption, appropriateness and susceptibility trends of 6 GNBs to 7 commonly used antibiotics were analysed using Kendall tau test. Results: We demonstrated sustained improvement in appropriateness of 7 broad-spectrum IV antibiotics, accompanied by significant reductions in IV ciprofloxacin, cefepime and, ertapenem use (p < 0.05). Hospital-wide susceptibility of 6 GNBs to all evaluated antibiotics improved significantly (p < 0.05), except for E. coli susceptibility to ertapenem and Enterobacterales susceptibility to ciprofloxacin. Conclusion: An evolving multi-pronged antibiotic stewardship approach improved antibiotic prescribing and GNB susceptibility towards majority of the antibiotics. In a rapidly evolving healthcare landscape, ASPs must remain agile, continually refining priorities and employing innovative strategies.
Keywords:
antibiotic stewardship
; antibiotic appropriateness
; antibiotic consumption
; antibiogram
; gram-negative bacilli susceptibility
; resistance
1. Introduction
Antibiotic stewardship program (ASP) is advocated in all healthcare institutions to combat rising bacteria resistance [1,2]. Globally, ASP implementation has reduced antibiotic consumption and hence, improved Gram-negative bacilli (GNB) susceptibility rates, including P. aeruginosa and ESBL-producing Enterobacterales towards broad-spectrum antibiotics across various healthcare settings [3,4,5,6,7,8,9]. Despite the growing body of literature on ASP, there remains a notable scarcity of longitudinal studies extending beyond a decade evaluating sustained impact of ASP on the volume and quality of antibiotic prescribing, along with antimicrobial susceptibility trends.
At Singapore General Hospital (SGH), an 1800-bedded quaternary care hospital in Singapore, with diverse medical and surgical specialties (including haematology, oncology, and transplant), the ASP team, comprising infectious diseases physicians and clinical pharmacists was officially established in 2008. Since its inception, multi-pronged antibiotic stewardship strategies have evolved over 17 years to address the gaps in prescribing patterns. The growth of the ASP can be mainly categorised into the following 4 phases: 1) initiation; 2) advancement; 3) optimisation; and 4) innovation [Table 1, Figure 1].
1.1. Initiation Phase (2008-2014)
In the initiation phase, our priority was to promote appropriate use of carbapenems (ertapenem/meropenem) and anti-pseudomonal agents (IV ciprofloxacin/ piperacillin-tazobactam) through hospital-wide prospective audit and feedback (PAF). When antibiotics were deemed inappropriate based on institution guidelines, ASP pharmacists/physicians make recommendations to the attending physicians, which included antibiotic discontinuation, de-escalation, escalation, intravenous (IV) to oral switch, dose adjustments, and infectious diseases consult. With PAF, we demonstrated shorter length of stay, lower 14-day re-infection and infection-related readmission rates in cases where ASP recommendations were adopted [10,11,12].
1.2. Advancement Phase (2015-2018)
Next, we leveraged technology to influence antibiotic prescribing. In 2015, computerized decision support system (CDSS) was integrated into the electronic medical records and made mandatory for select broad-spectrum antibiotics. In 2018, entry of treatment duration during electronic prescribing was made compulsory for select antibiotics to enhance physician accountability. Concurrently, we strengthened the visibility and branding of the ASP team, positioning ASP team as collaborative partners in patient care rather than “law enforcers”. For example, ASP pharmacists participated in ward rounds in high antibiotic use departments to engage and support prescribers.
1.3. Optimisation Phase (2019-2023)
Serial in-house studies revealed high prevalence of antibiotic use (~50% of admitted patients received antibiotics, substantially higher than in healthcare systems across Europe and North America (11%-33%)) [13]; and our strategies pivoted. We expanded in scope from solely infection management to include surgical prophylaxis, targeting instances where narrower-spectrum agents may be misused. For example, PAF was expanded to ceftriaxone across surgical wards, accompanied by collaborative efforts with surgical departments to shorten post-surgery prophylaxis [14].
Strong support from hospital senior leadership facilitated key stewardship initiatives, including enhancing analytical capabilities, fostering collaboration between ASP and clinical departments, promoting ASP awareness hospital-wide, and linking antibiotic stewardship metrics to hospital incentives.
1.4. Innovation Phase (2023 Till Current)
In the era of digital transformation, we continued to enhance our digital capacity to advance antibiotic stewardship. In 2023, we launched the first antibiotic mobile application, ABxSG, in Singapore as an antimicrobial stewardship tool that empowers physicians and pharmacists to use antibiotics optimally [15]. Concurrently, we developed an augmented intelligence model to predict the presence of lower respiratory tract infections, which we integrated into our PAF workflow, enabling expansion of our purview to all antibiotics [16]. In the arena of precision medicine, β-lactam therapeutic drug monitoring (TDM) to guide individualised drug dosing for optimal outcomes was introduced for critically ill patients and also to curb resistance emergence [17,18].
1.5. Study Objectives
The primary objective of this study is to evaluate how the evolution of ASP strategies over time has impacted the volume (i.e. consumption) and quality (i.e. appropriateness) of antibiotic prescribing. The secondary objective is to examine the longitudinal susceptibility trends of common Gram-negative bacilli (GNB) over time.
2. Methods
2.1. Data Collection
Data on IV antibiotic consumption was obtained from the hospital data warehouse and converted into defined daily doses per 1,000 inpatient days according to the definitions by the 2024 World Health Organisation (WHO) Anatomical Therapeutic Chemical (ATC) classification system [19]. Appropriate use of antibiotics (i.e. IV ciprofloxacin, ceftriaxone, piperacillin-tazobactam, ertapenem, and meropenem) under PAF were obtained from SGH antimicrobial stewardship electronic audit system. Appropriateness of antibiotic use was evaluated based on antibiotic indication, choice, duration, route, and dose upon antibiotic initiation and discontinuation.
Susceptibility data which was only available from 2011 onwards (and 2014 onwards for carbapenems), was derived from the antibiogram constructed by the institution microbiology laboratory based on definitions by Clinical & Laboratory Standards Institute (CLSI) [20]. The antibiogram was compiled annually using clinical samples and for GNB with ≥30 isolates; including only the first isolate per patient within the same calendar year. The antibiogram of 6 clinically significant GNBs [i.e. Acinetobacter baumannii, Pseudomonas aeruginosa, E. coli, Klebsiella spp. (excluding Klebsiella aerogenes), Enterobacter spp./Klebsiella aerogenes, Citrobacter freundii] towards the commonly used antibiotics (ciprofloxacin, ceftriaxone, amoxicillin-clavulanate, cefepime, piperacillin-tazobactam, ertapenem, and meropenem) was generated. Klebsiella aerogenes was classified alongside with Enterobacter spp. as it was formerly known as Enterobacter aerogenes. Susceptibility was interpreted based on CLSI breakpoints that were recommended for the respective years. Notably, there was a reduction in susceptible breakpoint for piperacillin-tazobactam (≤64/4 to ≤16/4μg/ml) for P. aeruginosa and Enterobacterales (≤16/4 to ≤8/4μg/ml) in 2012 and 2022 respectively [21,22]. Susceptible breakpoint was also reduced for cefepime (≤8 to ≤2μg/ml) towards Enterobacterales in 2014 [23].
2.2. Statistical Analysis
Statistical tests were conducted using SPSS (Version 26.0 Armonk, NY: IBM Corp.). The trend of antibiotic consumption, appropriateness, and susceptibility data over time were analysed using kendall tau test. Continuous data are presented in median (interquartile range), unless stated otherwise.
3. Results
3.1. Antibiotic Consumption
From 2011 to 2024, a significant reduction in consumption was shown for IV ciprofloxacin [11.0 (2011) to 4.9 (2024) DDD/1,000 patient-days], cefepime [41.1 (2011) to 11.9 (2024) DDD/1,000 patient-days], and ertapenem [13.8 (2011) to 7.5 (2024) DDD/1,000 patient-days] (p<0.05). On the contrary, there was a significant increase in consumption of IV amoxicillin-clavulanate [32.9 (2011) to 48.5 (2024) DDD/1,000 patient-days and piperacillin-tazobactam [47.8 (2011) to 82.0 (2024) DDD/1,000 patient-days] (p<0.05) [Table 2, Figure 2]. There were no significant changes in overall trends for ceftriaxone and meropenem consumption.
In the initial phase, following hospital-wide PAF for carbapenems and IV ciprofloxacin/piperacillin-tazobactam in 2011 and 2013 respectively, there was no apparent reduction in consumption of these antibiotics. Ironically, there was a noticeable decline of non-PAF antibiotics, where ceftriaxone and cefepime consumption reduced consistently from 105 to 74.8 DDD/1,000 patient-days and 20.5 to 12.9 DDD patient-days respectively from 2011 to 2015. Interestingly, with the implementation of CDSS and mandatory entry of antibiotic duration in 2015 and 2018 respectively during the advancement phase, meropenem consumption reduced substantially —from 50.2 (2015) to 20.9 (2018) DDD per 1,000 patient-days. This reduction was coupled with an apparent increase in IV co-amoxiclav and piperacillin-tazobactam consumption following 2015 [Figure 2].
During the optimisation/innovation phase, ASP expanded its focus to narrower-spectrum antibiotics, including ciprofloxacin, co-amoxiclav, and ceftriaxone that were often used inappropriately in extended surgical prophylaxis. This approach led to modest reduction in IV ciprofloxacin, while stabilising IV co-amoxiclav and ceftriaxone consumption. The reduction in IV ciprofloxacin could also be attributed to the concurrent decline in susceptibility of E. coli, Klebsiella spp. and Enterobacter spp., rendering it less suitable for culture-directed therapy. Notably, there was a modest reduction in cefepime and ertapenem after 2019, which corresponds to an increase in meropenem consumption thereafter [Figure 2].
3.2. Antibiotic Appropriateness
Overall, there was significant improvement in appropriateness trends of PAF antibiotics; 72% (2013) to 82.6% (2024) for IV ciprofloxacin, 75.9% (2011) to 93.8% (2024) for ertapenem, and 72.2% (2011) to 86.1% (2024) for meropenem. Although not statistically significant, ceftriaxone and piperacillin-tazobactam appropriateness increase from [77.5% (2019) to 82.2% (2024), (p=0.851)] and [67.9% in 2013 to 82.7% in 2024; p = 0.411], respectively [Figure 3].
In the initiation phase, we observed a pronounced improvement in appropriateness of ertapenem [75.9% (2011) to 83.3% (2015)], meropenem [72.7% (2011) to 84.3% (2015)], and piperacillin-tazobactam [72.0% (2013) to 83.5% (2015)] following hospital-wide PAF. With CDSS implementation in 2015 during the advancement phase, there was an appreciable increase in IV ciprofloxacin [75.5% (2015) to 83.2% (2017)] and ertapenem [83.3% (2015) to 90.6% (2017)]. Of note, CDSS provided no recommendations for the empiric use of ertapenem and only limited recommendations for IV ciprofloxacin. Hence, suggesting a possible shift away from empiric use of IV ciprofloxacin/ertapenem to culture-directed prescribing.
During the optimisation/innovation phase, the appropriateness of carbapenems largely remained stable. This prompted the multi-pronged ASP strategies to shift focus from carbapenems to narrower-spectrum antibiotics, along with the expansion of ASP activities from infection management to surgical prophylaxis. This change in focus had led sustained improvements in the appropriate use of ceftriaxone [77.5% (2019) to 82.2% (2024)], IV ciprofloxacin [76.9% (2019) to 82.7% (2024)], and piperacillin-tazobactam [76.7% (2019) to 82.6% (2024)].
3.3. GNB Susceptibility
From 2011 to 2024, hospital-wide susceptibility trends of all six GNBs showed significant increase (p < 0.05), except for E. coli susceptibility to ertapenem and Enterobacterales susceptibility to ciprofloxacin [Table 3 and Figure 4].
A. baumannii and P. aeruginosa, both commonly associated with nosocomial infections, showed a significant increase in susceptibility to ciprofloxacin, cefepime, piperacillin-tazobactam, and meropenem over time (p<0.05). Notably, the most rapid improvement in susceptibility was observed between 2011 and 2016. Susceptibility of E. coli and Klebsiella spp. to ceftriaxone [often used as surrogate for resistance due to extended-spectrum β-lactamase (ESBL)] and cefepime increased significantly (p<0.05) from 2011 to 2024. Enterobacter spp./Klebsiella aerogenes and Citrobacter freundii, which are Enterobacterales that possesses AmpC β-lactamase enzymes, also showed improved susceptibility trends to cefepime, ertapenem, and meropenem (p<0.05). The most rapid improvement in susceptibility of the Enterobacterales was observed after 2018, where it was preceded with a noticeable reduction in ceftriaxone and cefepime consumption from 2011 to 2016.
Interestingly, despite a marked increase in IV amoxicillin-clavulanate and piperacillin-tazobactam consumption, particularly after 2016, E. coli and Klebsiella spp. exhibited a pronounced increase in susceptibility to these antibiotics.
4. Discussion
To date, this is the first study to describe the evolution of antibiotic stewardship strategies over a 17-year period and evaluate their impact on the volume/quality of antibiotic prescribing, and susceptibility trends of commonly seen GNB in a quaternary healthcare institution. We demonstrated sustained improvement in appropriate prescribing of 7 commonly used broad-spectrum IV antibiotics. Additionally, there was an overall reduction in consumption for IV ciprofloxacin, cefepime and ertapenem from 2011 to 2024 (p<0.05), and a steep reduction in ceftriaxone consumption in the initial phase of ASP. Importantly, we demonstrated significant increase in hospital-wide susceptibility trends for all 6 commonly seen GNBs to all 6 β-lactam antibiotics (p < 0.05), except for E. coli susceptibility to ertapenem (which remained stable). Furthermore, susceptibility of A. baumanni and P. aeruginosa to ciprofloxacin improved significantly over time (p<0.05).
Reducing antibiotic consumption to mitigate antimicrobial resistance is a core objective of ASP [1,2]. In the initial phase, ceftriaxone and cefepime consumption declined markedly from 2011 to 2016, after which usage plateaued [Figure 2]. Although PAF targeted carbapenems and piperacillin–tazobactam rather than ceftriaxone then, recommendations for antibiotic cessation when therapy was no longer indicated likely influenced overall prescribing behaviour. This contrasted with pre-PAF practices, where clinicians often preferred antibiotic de-escalation instead of discontinuation. The combination of PAF and rolling out of institutional antibiotic guidelines likely fostered a behavioural shift among prescribers, promoting greater awareness and adherence to judicious use of narrower-spectrum antibiotics.
Interestingly, reductions in cephalosporin consumption coincided with pronounced improvements in A. baumannii susceptibility from 2011 to 2016, consistent with previous evidence linking ceftriaxone use to the selection of multidrug-resistant A. baumannii [24]. A subsequent improvement in Enterobacterales susceptibility to cephalosporins (reflecting declining ESBL prevalence) occurred from 2018 onwards, albeit after a lag of > 3 years following reduced cephalosporin use—an ecological delay similarly reported by Livermore et al. [25]. The persistence of resistance despite reduced selective pressure may be attributable to the efficient horizontal transfer of ESBL-encoding plasmids through conjugation, maintaining resistance within bacterial populations [26]. Furthermore, we postulate that the decline in IV ciprofloxacin use from 2019 contributed to the sustained reduction in ESBL prevalence [27], likely driven by ASP initiatives targeting ciprofloxacin use in surgical prophylaxis and the known reduced susceptibility of Enterobacterales to ciprofloxacin nationally [28]. On the contrary, our data showed improved ciprofloxacin susceptibility in hospital-acquired pathogens such as P. aeruginosa and A. baumannii, supporting judicious use of ciprofloxacin use within the institution for nosocomial infections [29].
Unlike cephalosporins and ciprofloxacin, an association between antibiotic consumption and GNB susceptibility rates was not consistently observed across all antibiotics in our study. Despite increased consumption of IV amoxicillin-clavulanate and piperacillin-tazobactam over time (p<0.05), a trend similarly observed nation-wide [28], there was significant improvement in GNB susceptibility to amoxicillin-clavulanate and piperacillin-tazobactam over time (p<0.05). Similarly, Lee et al. observed that increased piperacillin–tazobactam utilization did not correspond with higher resistance rates in E. coli, suggesting a higher threshold for resistance acquisition [30]. The same study also found no rise in AmpC-β-lactamase producing E. coli or K. pneumoniae. Additionally, Marquet et al. reported that amoxicillin–clavulanate use was protective against third-generation cephalosporin non-susceptibility in K. pneumoniae, supporting its role as a potential alternative to cephalosporins or fluoroquinolones to mitigate resistance [31].
In practice, some degree of the “balloon-squeezing” effect is unavoidable, particularly in quaternary healthcare settings where managing complex and critically ill patients is the norm. At our institution, a reduction in meropenem consumption following implementation of CDSS in 2015 was accompanied by an increased use of IV amoxicillin-clavulanate and piperacillin-tazobactam, likely indicating the effectiveness of CDSS in assisting doctors in choosing narrower-spectrum antibiotics as empiric therapy. Therefore, ASPs should avoid self-penalization based solely on antibiotic usage matrix, recognizing that the rise of consumption of selected antibiotics may be deemed clinically reasonable within acceptable boundaries.
Similarly, following 2019, meropenem consumption increased slowly along with a further reduction in cefepime and ertapenem use. The rise in meropenem was likely influenced by emerging evidence and local experience of cefepime/ertapenem induced neurotoxicity [32,33], which led the ASP team to permit meropenem for infections caused by AmpC- or ESBL-producing Enterobacterales in patients with severe renal impairment. Additionally, the incorporation of evidence supporting higher β-lactam dosing in critically ill or obese patients into our institutional antibiotic guidelines has likely contributed to the increased consumption of not only meropenem but also piperacillin-tazobactam [34,35]. In 2023, β-lactam therapeutic drug monitoring (TDM) was introduced to optimise pharmacokinetic/pharmacodynamic targets with the aim to improve both patient outcomes and suppress emergence of antibiotic resistance [17,18]. Although this coincided with a slight increase in consumption of piperacillin-tazobactam and meropenem in 2023-2024, no deterioration in GNB susceptibility was observed through 2024.
Antibiotic consumption trend may not always align with appropriate prescribing trends, and effective antibiotic stewardship requires balancing evaluation of both indicators. A major achievement of our 17-year ASP has been the sustained improvement in appropriate antibiotic prescribing across all antibiotics evaluated in our study. PAF, which was our cornerstone ASP strategy during the initial phase had led to improved appropriateness of IV ciprofloxacin, piperacillin-tazobactam, and carbapenems. Interestingly, it took 2 years of PAF before carbapenem appropriateness improved. This delayed improvement suggests that building prescriber rapport through ongoing handshake stewardship requires time. Compared to restrictive measures, enabling strategies like PAF allows real-time feedback to prescribers, which provides opportunities to engage, educate, and empower [36].
A coordinated approach with strong senior leadership support is critical for the success and sustainability of ASPs [2]. Provision of financial and manpower resources to develop technology enablers during the optimisation/innovation phase, including CDSS which had driven improvements in carbapenem appropriateness in our study, was also proven effective in other healthcare settings [37,38]. As our ASP matures, real-time surveillance dashboards and analytics have enabled the team to promptly identify prescribing gaps in narrower-spectrum antibiotics. For example, several surgical departments were found to use unnecessarily prolonged antibiotics for surgical prophylaxis. In response, targeted strategies were implemented, including the expansion of PAF to ceftriaxone in surgical departments and collaborations with high-usage teams to optimize antibiotic duration [14]. Furthermore, the launch of an in-house antibiotic mobile application (ABxSg) in 2023, which provides physicians with on-the-go access to antibiotic prescribing guidelines and resources, was designed to promote appropriate antibiotic use across all antibiotics. This strategy had reduced the proportion of hospitalised patients prescribed antibiotics in our institution [15]. Additionally, substantial financial investment supported the development of an augmented intelligence model (AI²D) with an accuracy of 80% in identifying patients at low risk for acute bacterial lower respiratory tract infection. Integration of AI²D into PAF enhanced its effectiveness; antibiotics prescribed to such patients were nearly 4 times more likely to be discontinued within two days compared with cases managed without AI²D [16].
During the advancement phase, significant efforts were directed towards concurrent upskilling of workforce, including supporting clinical pharmacists through national residency programmes and relevant postgraduate studies. Clinically advanced pharmacists are then better equipped to manage complex patients and lead advanced ASP strategies, which strengthened the identity and visibility of ASP team within the hospital. Beyond participating in ward rounds, ASP pharmacists and physicians were actively involved in multiple quality improvement projects, including projects pertaining to diagnostic stewardship with major departments as part of handshake stewardship initiatives. The consistent presence and collaboration of a capable ASP team positioned us as trusted partners in patient care rather than mere “enforcers” of appropriate antibiotic use. This branding improved rapport with prescribers, making them more receptive to ASP recommendations and strategies, thereby contributing to sustained improvements in antibiotic prescribing appropriateness. Notably, appropriate ertapenem and meropenem prescribing increased substantially from 75.9% (2011) to 93.8% (2024) and from 72.7% (2011) to 86.1% (2024) respectively. These results represent an exceptional achievement when compared with reports from hospitals in other parts of Asia, Europe, and North America, where carbapenem appropriateness rates typically range between 50% and 60% [39,40,41].
4.1. Study Limitations
Firstly, in the initial phase, hospital’s electronic system lacked the functionality to capture several critical data types, limiting the ability to comprehensively evaluate the impact of early ASP strategies. For example, complete antibiotic consumption/appropriateness data and carbapenem susceptibility data were not available before 2011 and 2014 respectively. Secondly, susceptibility trends are used as a surrogate measure to assess the impact of the ASP; however, based on the available data, we are unable to distinguish between clinical isolates originating from community-acquired and hospital-acquired infections. Improved susceptibility trends may possibly reflect increased awareness of antibiotic stewardship among community prescribers over time; however, causality cannot be accounted for in our study. This highlights the need to enhance the capabilities of our analytical dashboards to allow segregation of infection origin. Thirdly, although enhanced infection control measures over time likely reduced the spread of drug-resistant organisms, this effect could not be incorporated into our analysis.
5. Conclusion
A multi-pronged ASP approach implemented over 17 years has successfully improved antibiotic prescribing and susceptibility of GNBs towards majority of the antibiotics at our institution. Beyond PAF, technology enablers and handshake stewardship have further advanced our efforts and yielded measurable results. Equally important, is strengthening the visibility and branding of the ASP, with sustained support from hospital leadership, which is critical for long-term success. In a rapidly evolving healthcare landscape, ASPs must remain agile, continually refining priorities and employing innovative strategies. Incorporating diagnostic stewardship alongside advances in rapid diagnostics, immunoprofiling, and machine learning can further enhance judicious use of antibiotics [42,43,44,45,46].
Author Contributions
Conceptualization: Y.P.Z, S.J.C., A.L.H.K., W.H.L.L.; methodology: Y.P.Z., , S.Y.C.L, T.Y.E; formal analysis: Y.P.Z.; data curation: Y.P.Z., W.Y.B, S.Y.C.L, T.Y.E; writing: original draft: Y.P.Z.; review and editing: Y.P.Z., S.J.C., A.L.H.K., W.H.L.L W.Y.B, S.Y.C.L, T.Y.E.; visualization: Y.P.Z.; project administration: Y.P.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was exempted from our institutional ethics board review (SingHealth Institutional Review Board Reference 2022/2560). It was deemed that the activities conducted by the ASP do not require further ethical deliberation because it mainly involves a series of quality improvement initiatives.
Informed Consent Statement
Patient consent was not required as per study exemption from our institutional ethics board review. Deidentified data was used for analysis in this study.
Data Availability Statement
The original contributions presented in this study are included in the article.
Acknowledgments
We would like to express our sincere gratitude to the SGH ASP physicians (Benjamin Cherng, Cherie Gan, Piotr Chlebicki, Siew Yee Thien) and pharmacists (Boon San Teoh, Daphne Yah Chieh Yii, Jia Le Lim, Jun Jie Tan, Kai Chee Hung, Li Wen Loo, Narendran Koomanan, Nathalie Chua, Sarah Tang, Trevina Lee, Yixin Liew) for their support in various ASP strategies. Additionally, we would like to thank the SGH microbiology laboratory for provision of the antibiogram. Lastly, we would like to thank our SingHealth DGCEO Kenneth Kwek, GCDSO Benedict Tan and the Office of Digital Empowerment for their unwavering support.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Barlam TF, Cosgrove SE, Abbo LM, MacDougall C, Schuetz AN, Septimus EJ et al. Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin Infect Dis 2016;62(10):e51–e77. [CrossRef]
- Pollack LA, Srinivasan A. Core elements of hospital antibiotic stewardship programs from the Centers for Disease Control and Prevention. Clin Infect Dis. 2014;59 Suppl 3(Suppl 3):S97-S100. [CrossRef]
- Chua AQ, Kwa A, Tan TY, Legido-Quigley H, Hsu LY. Ten-year narrative review on antimicrobial resistance in Singapore. Singapore Med J 2019; 60(8): 387-396. [CrossRef]
- Ng TM, Ang LW, Heng ST, Kwa A, Wu JE, Seah X et al. Antibiotic utilisation and resistance over the first decade of nationally funded antimicrobial stewardship programmes in Singapore acute-care hospitals. Antimicrobial Resistance & Infection Control 2023; 12: 82. [CrossRef]
- Ababneh MA, Nasser SA, Rababa'h AM. A systematic review of Antimicrobial Stewardship Program implementation in Middle Eastern countries. Int J Infect Dis 2021; 105:746-752. [CrossRef]
- Karanika S, Paudel S, Grigoras C, Kalbasi A, Mylonakis E. Systematic Review and Meta-analysis of Clinical and Economic Outcomes from the Implementation of Hospital-Based Antimicrobial Stewardship Programs. Antimicrob Agents Chemother 2016; Jul 22;60(8):4840-52. [CrossRef]
- Strazzulla A, Adrien V, Houngnandan SR, Devatine S, Bahmed O, Abroug S, et al. Characteristics of Pseudomonas aeruginosa infection in intensive care unit before (2007-2010) and after (2011-2014) the beginning of an antimicrobial stewardship program. Antimicrob Steward Healthc Epidemiol 2024; A29;4(1):e60. [CrossRef]
- Mahmoudi L, Sepasian A, Firouzabadi D, Akbari A. The Impact of an Antibiotic Stewardship Program on the Consumption of Specific Antimicrobials and Their Cost Burden: A Hospital-wide Intervention. Risk Manag Healthc Policy 2020; 23;13:1701-1709. [CrossRef]
- Chrysou K, Zarkotou O, Kalofolia S, Papagiannakopoulou P, Mamali V, Chrysos G, Themeli-Digalaki K, Sypsas N, Tsakris A, Pournaras S. Impact of a 4-year antimicrobial stewardship program implemented in a Greek tertiary hospital. Eur J Clin Microbiol Infect Dis 2022; Jan;41(1):127-132. [CrossRef]
- Liew YX, Lee W, Loh JCZ, Cai Y, Tag S, Lim C et al. Impact of an antimicrobial stewardship programme on patient safety in Singapore General Hospital. Int J Antimicrob Agents 2012; 40: 55-60. [CrossRef]
- Loo L, Liew Y, Lee W, Lee LW, Chlebicki P, Kwa A. Discontinuation of antibiotic therapy within 24 hours of treatment initiation for patients with no clinical evidence of bacterial infection: a 5-year safety and outcome study from Singapore General Hospital Antimicrobial Stewardship Program. Int J Antimicrob Agents 2019; 53: 606-611. [CrossRef]
- Teo J, Kwa AL, Loh J, Chlebicki MP, Lee W. The effect of a whole-system approach in an antimicrobial stewardship programme at the Singapore General Hospital. Eur J Clin Microbiol Infect Dis 2012 Jun;31(6):947-55. [CrossRef]
- Versporten A, Zarb P, Caniaux I, Gros MF, Drapier N, Miller M, Jarlier V, Nathwani D, Goossens H; Global-PPS network. Antimicrobial consumption and resistance in adult hospital inpatients in 53 countries: results of an internet-based global point prevalence survey. Lancet Glob Health 2018; 6(6):e619-e629. [CrossRef]
- Loo LW, Zhou YP, Wang YB, Lee LW, Chung JS. Antimicrobial Stewardship in Cardiac Device Surgery: Impact of Behavioural Change Interventions on Extended Prophylaxis Practices. Antibiotics. 2025; 14(8):754. [CrossRef]
- Lee LW, Lim SYC, Zhou YP, et al. Impact of the ABxSG Mobile Application on Antibiotic Prescribing: An Interrupted Time Series Study. Antibiotics (Basel). 2025;14(9):933. [CrossRef]
- Tang S, Lim JL, Lee LXT, Yii YCD, Zhou YP et al. Augmented intelligence in infectious diseases (AI2D) as an antimicrobial stewardship tool for early antibiotic discontinuation in suspected lower respiratory tract infections [abstract]. Presented at: Congress of the European Society of Clinical Microbiology and Infectious Diseases (ESCMID); April 11-15, 2025; Vienna Austria. Available at: https://registration.escmid.org/AbstractList.aspx?e=30&header=0&preview=1&aig=-1&ai=29130. Accessed on 27 October 2025.
- Sumi CD, Heffernan AJ, Lipman J, Roberts JA, Sime FB. What Antibiotic Exposures Are Required to Suppress the Emergence of Resistance for Gram-Negative Bacteria? A Systematic Review. Clin Pharmacokinet. 2019;58(11):1407-1443. [CrossRef]
- Roberts JA, Paul SK, Akova M, et al. DALI: defining antibiotic levels in intensive care unit patients: are current β-lactam antibiotic doses sufficient for critically ill patients?. Clin Infect Dis. 2014;58(8):1072-1083. [CrossRef]
- WHO Collaborating Centre for Drug Statistics Methodology, ATC classification index with DDDs, 2024. Oslo, Norway 2024.
- CLSI. Analysis and Presentation of Cumulative Antimicrobial Susceptibility Test Data. 5th ed. CLSI guideline M39. Clinical and Laboratory Standards Institute; 2022.
- CLSI. Piperacillin-Tazobactam Breakpoints for Pseudomonas aeruginosa. CLSI rationale document MR15. Clinical and Laboratory Standards Institute; 2024.
- Tamma PD, Harris PN, Mathers AJ, Wenzler E, Humphries RM. Breaking Down the Breakpoints: Rationale for the 2022 Clinical and Laboratory Standards Institute Revised Piperacillin-Tazobactam Breakpoints Against Enterobacterales. Clinical Infect Dis 2023; 77(11):1585-1590. [CrossRef]
- Bork JT, Heil EL, Leekha S, Fowler RC, Hanson ND, Majumdar A, et al. Impact of CLSI and EUCAST Cefepime breakpoint changes on the susceptibility reporting for Enterobacteriaceae. Diagn Microbiol Infect Dis. 2017; Dec;89(4):328-333. [CrossRef]
- Mihalov P, Hodosy J, Koščálová A, et al. Antimicrobial Therapy as a Risk Factor of Multidrug-Resistant Acinetobacter Infection in COVID-19 Patients Admitted to the Intensive Care Unit. Can J Infect Dis Med Microbiol. 2023;2023:4951273. [CrossRef]
- Livermore DM, Hope R, Reynolds R, Blackburn R, Johnson AP, Woodford N. Declining cephalosporin and fluoroquinolone non-susceptibility among bloodstream Enterobacteriaceae from the UK: links to prescribing change? Journal of Antimicrobial Chemotherapy. 2013;68(11):2667-2674. [CrossRef]
- Moosdeen F. The evolution of resistance to cephalosporins. Clin Infect Dis. 1997;24(3):487-493. [CrossRef]
- Aldeyab MA, Harbarth S, Vernaz N, et al. The impact of antibiotic use on the incidence and resistance pattern of extended-spectrum beta-lactamase-producing bacteria in primary and secondary healthcare settings. Br J Clin Pharmacol. 2012;74(1):171-179. [CrossRef]
- Ministry of Health. One health report on antimicrobial utilisation and resistance 2019. Singapore: Ministry of Health Singapore; 2019. Available at https://www.moh.gov.sg/resources-statistics/reports/one-health-report-on-antimicrobial-utilisation-and-resistance-2019. Accessed 21 September 2024.
- Medina Presentado JC, Paciel López D, Berro Castiglioni M, Gerez J. Ceftriaxone and ciprofloxacin restriction in an intensive care unit: less incidence of Acinetobacter spp. and improved susceptibility of Pseudomonas aeruginosa. Rev Panam Salud Publica. 2011;30(6):603-609. [CrossRef]
- Lee J, Oh CE, Choi EH, Lee HJ. The impact of the increased use of piperacillin/tazobactam on the selection of antibiotic resistance among invasive Escherichia coli and Klebsiella pneumoniae isolates. Int J Infect Dis. 2013;17(8):e638-e643. [CrossRef]
- Marquet A, Vibet MA, Caillon J, et al. Is There an Association Between Use of Amoxicillin-Clavulanate and Resistance to Third-Generation Cephalosporins in Klebsiella pneumoniae and Escherichia coli at the Hospital Level?. Microb Drug Resist. 2018;24(7):987-994. [CrossRef]
- Payne LE, Gagnon DJ, Riker RR, et al. Cefepime-induced neurotoxicity: a systematic review. Crit Care. 2017;21(1):276. [CrossRef]
- Wang C, Zhou Y, Zhou Y, Ye C. Ertapenem-Induced Neurotoxicity: A Literature Review of Clinical Characteristics and Treatment Outcomes. Infect Drug Resist. 2023;16:3649-3658. [CrossRef]
- Alobaid AS, Wallis SC, Jarrett P, Starr T, Stuart J, Lassig-Smith M, Mejia JL, Roberts MS, Roger C, Udy AA, Lipman J, Roberts JA. Population Pharmacokinetics of Piperacillin in Nonobese, Obese, and Morbidly Obese Critically Ill Patients. Antimicrob Agents Chemother 2017; Feb 23;61(3):e01276-16. [CrossRef]
- European committee on antimicrobial susceptibility testing. Aminopenicillin breakpoints for Enterobacterales. General Consultation. 2022. https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Consultation/2021/Aminopenicillins_and_Enterobacterales_General_consultation_November_2021.pdf. Accessed on 21 September 2024.
- Davey P, Marwick CA, Scott CL, Charani E, McNeil K, Brown E et al. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database of Systematic Reviews 2017, Issue 2. Art. No.: CD003543. [CrossRef]
- Nachtigall I, Tafelski S, Deja M, Halle E, Grebe MC, Tamarkin A, Rothbart A, Uhrig A, Meyer E, Musial-Bright L, Wernecke KD, Spies C. Long-term effect of computer-assisted decision support for antibiotic treatment in critically ill patients: a prospective 'before/after' cohort study. BMJ Open 2014; Dec 22;4(12):e005370. [CrossRef]
- Paul M, Andreassen S, Tacconelli E, Nielsen AD, Almanasreh N, Frank U, Cauda R, Leibovici L; TREAT Study Group. Improving empirical antibiotic treatment using TREAT, a computerized decision support system: cluster randomized trial. J Antimicrob Chemother 2006; Dec;58(6):1238-45. [CrossRef]
- Poline J, Postaire M, Parize P, et al. Stewardship program on carbapenem prescriptions in a tertiary hospital for adults and children in France: a cohort study. Eur J Clin Microbiol Infect Dis. 2021;40(5):1039-1048. [CrossRef]
- Ishtiaq U, Acosta K, Akabusi C, Noble K, Gujadhur N, Cluzet V. Appropriateness of Empiric Initiation of Meropenem in the Intensive Care Unit as Determined by Internal Medicine Residents. Antimicrob Steward Healthc Epidemiol. 2024;4(1):e185. Published 2024 Oct 24. [CrossRef]
- Zhang D, Cui K, Lu W, et al. Evaluation of carbapenem use in a tertiary hospital: antimicrobial stewardship urgently needed. Antimicrob Resist Infect Control. 2019;8:5. [CrossRef]
- Zakhour J, Haddad SF, Kerbage A, Wertheim H, Tattevin P, Voss A, et al. International Society of Antimicrobial Chemotherapy (ISAC) and the Alliance for the Prudent Use of Antibiotics (APUA). Diagnostic stewardship in infectious diseases: a continuum of antimicrobial stewardship in the fight against antimicrobial resistance. Int J Antimicrob Agents 2023; Jul;62(1):106816. [CrossRef]
- Claeys KC, Trautner BW, Leekha S, Coffey KC, Crnich CJ, Diekema DJ, et al. Optimal Urine Culture Diagnostic Stewardship Practice-Results from an Expert Modified-Delphi Procedure. Clin Infect Dis 2022; Aug 31;75(3):382-389. [CrossRef]
- Pinto-de-Sá, R.; Sousa-Pinto, B.; Costa-de-Oliveira, S. Brave New World of Artificial Intelligence: Its Use in Antimicrobial Stewardship—A Systematic Review. Antibiotics 2024; 13, 307. [CrossRef]
- Tang S, Chang D, Zhi Chin D, Piotr Chlebicki M, Jasmine Chung S, Wei Lee L, et al. 163. Can Machine Learning Guide Antibiotic Initiation for Lower Respiratory Tract Infections? Open Forum Infect Dis 2023;10(Suppl 2):ofad500.236. [CrossRef]
- Hanson KE, Tsalik EL. Host Immune Response Profiling for the Diagnosis of Infectious Diseases. J Infect Dis. Published online August 11, 2025. [CrossRef]
Figure 1.
Antibiotic stewardship strategies implemented at Singapore General Hospital from 2008 to 2024. PAF: Prospective audit feedback. *All ASP strategies listed in the timeline above are ongoing since initiation in the respective year.
Figure 1.
Antibiotic stewardship strategies implemented at Singapore General Hospital from 2008 to 2024. PAF: Prospective audit feedback. *All ASP strategies listed in the timeline above are ongoing since initiation in the respective year.
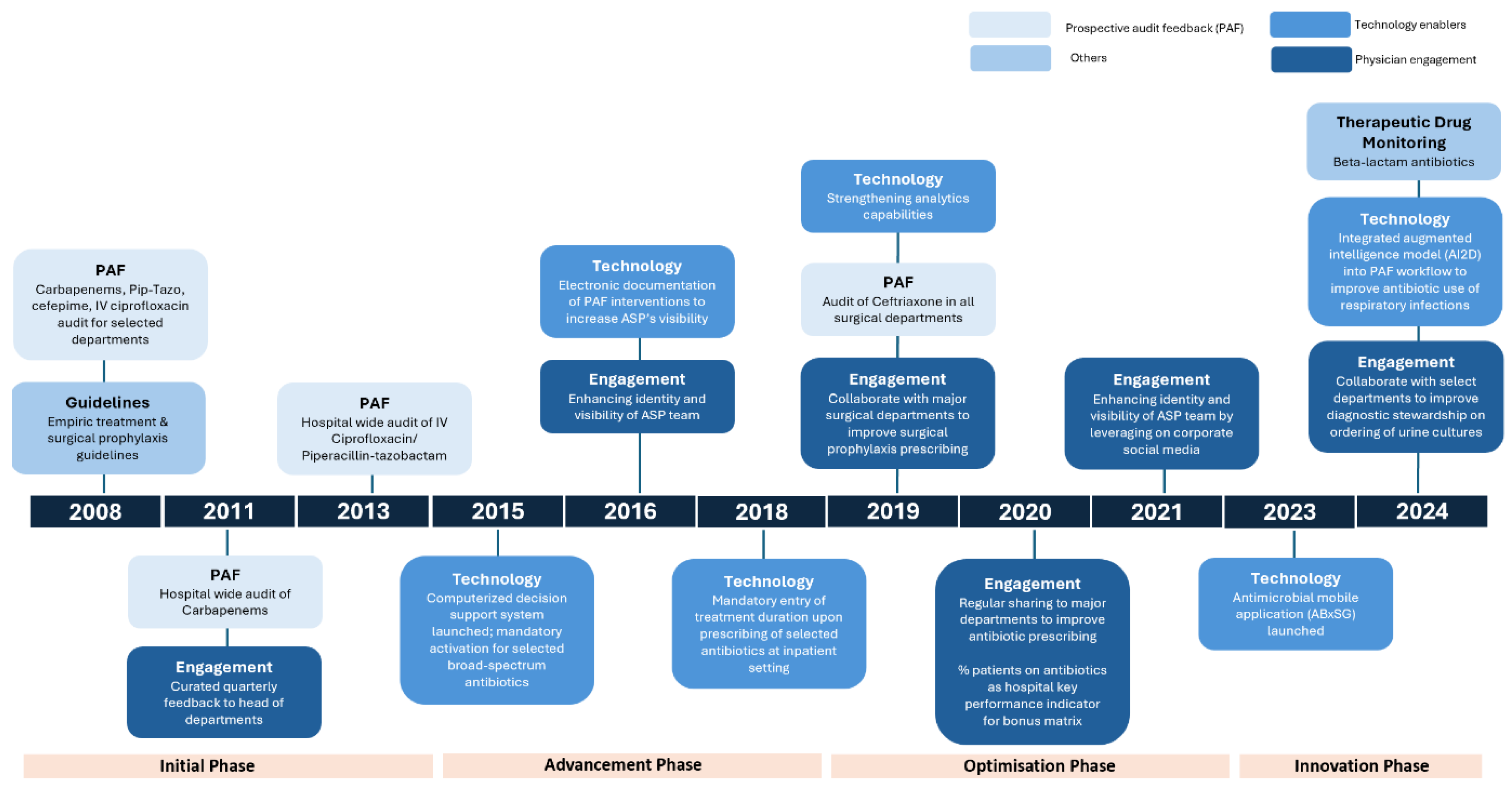
Figure 2.
Consumption of antibiotics (Defined daily doses/10,000 patient days) from 2011 to 2024.
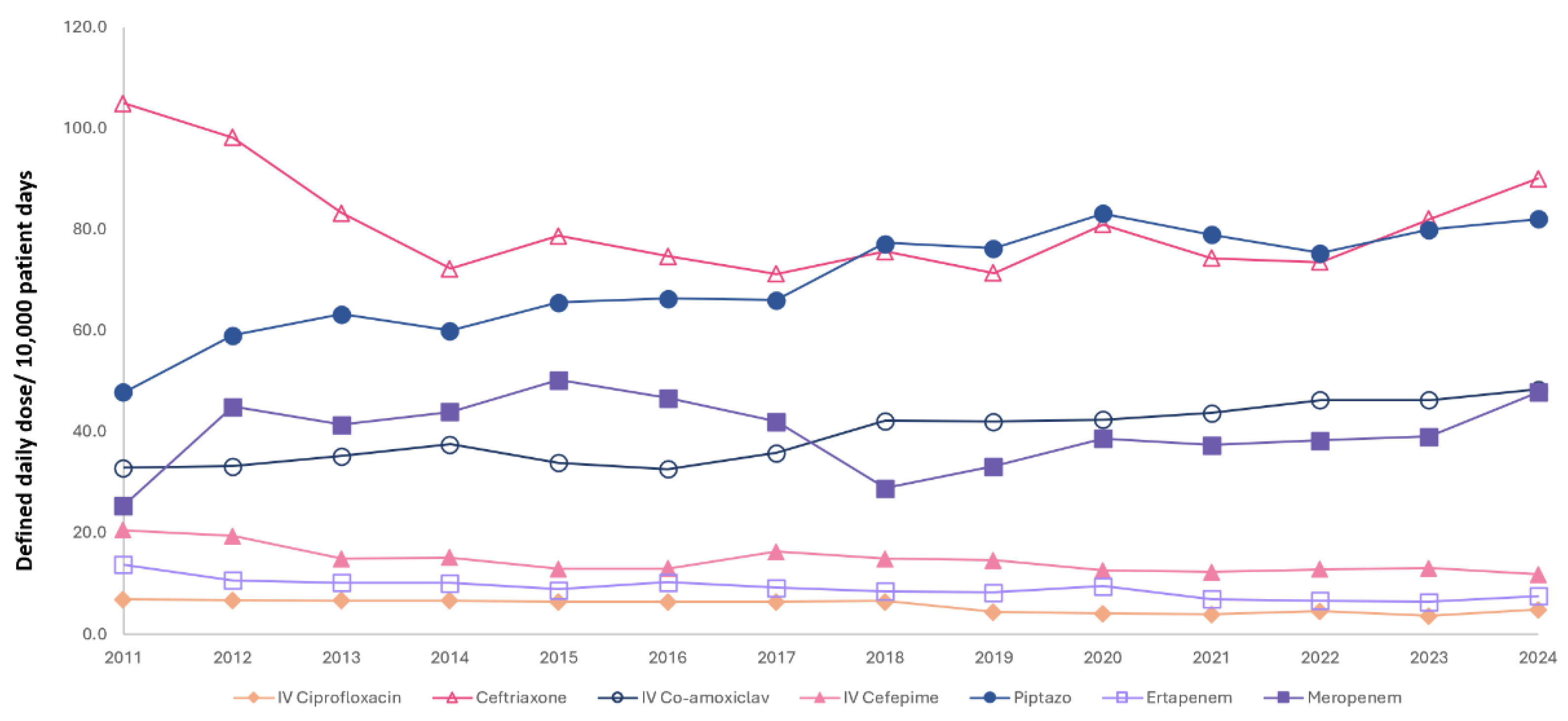
Figure 3.
Appropriateness of PAF Antibiotics (2011 to 2024).
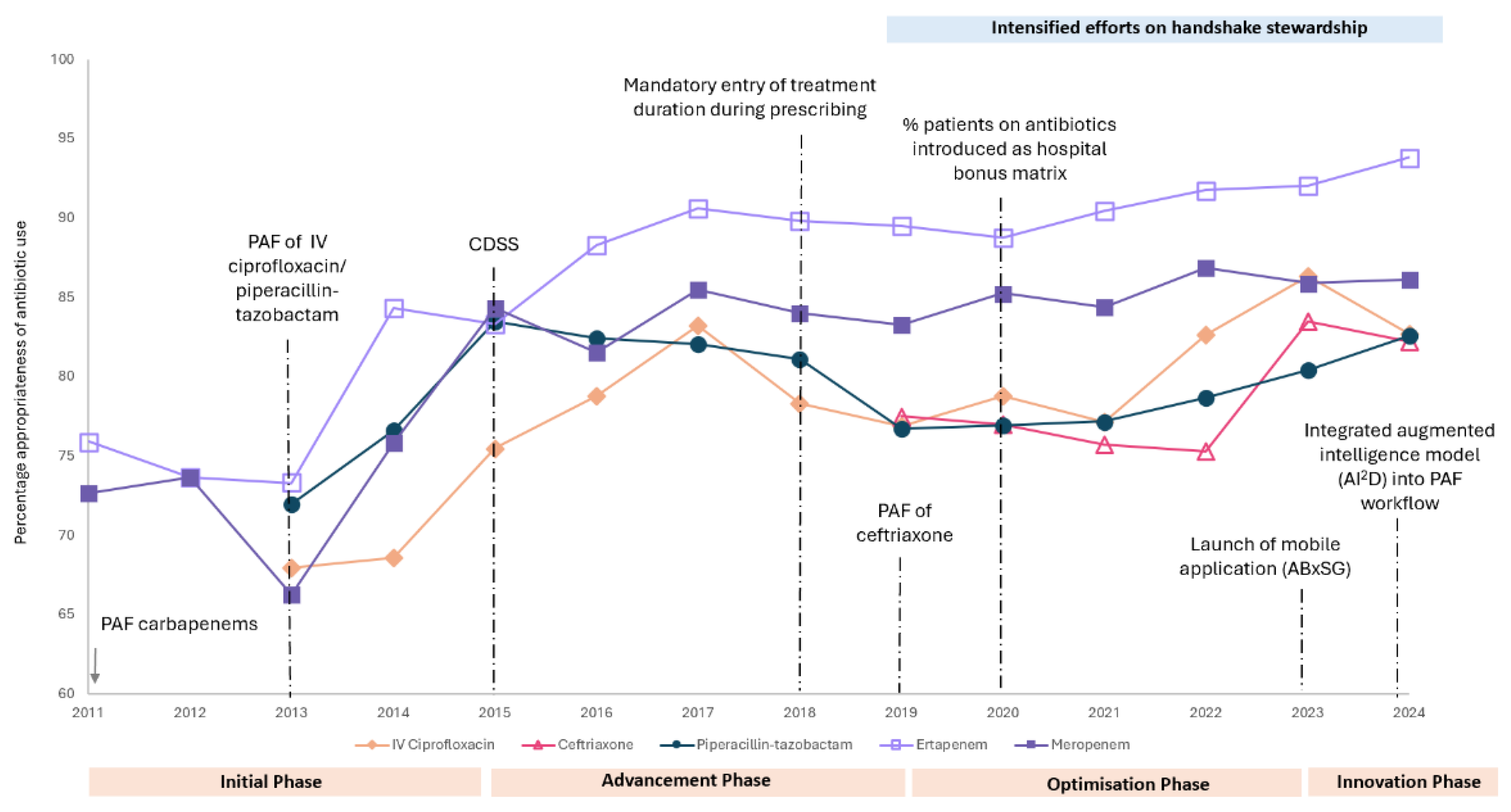
Figure 4.
Hospital-wide susceptibility of 6 Gram-negative bacilli towards 7 antibiotics (from 2011 to 2024). Klebsiella spp. excludes Klebsiella aerogenes. The y-axis for A. baumannii susceptibility data begins at 20%, whereas for other Gram-negative bacilli starts at 50%.
Figure 4.
Hospital-wide susceptibility of 6 Gram-negative bacilli towards 7 antibiotics (from 2011 to 2024). Klebsiella spp. excludes Klebsiella aerogenes. The y-axis for A. baumannii susceptibility data begins at 20%, whereas for other Gram-negative bacilli starts at 50%.
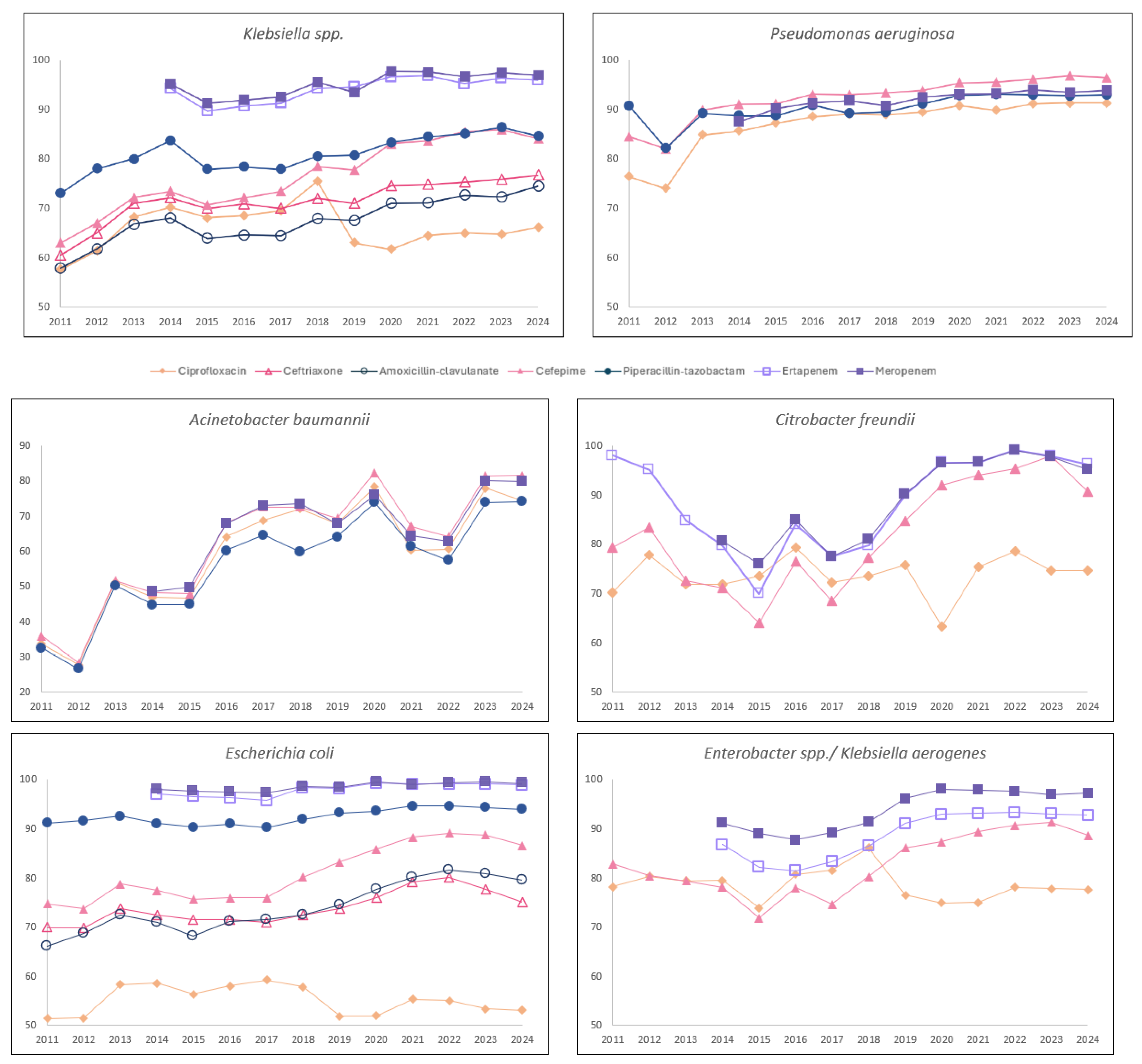

Table 1.
Four phases of Antimicrobial Stewardship Strategies and Corresponding Key Strategies.
| Phase | Approx. Years | Key Stewardship Strategies |
|---|---|---|
| Initiation | 2008-2014 |
|
| Advancement | 2015-2018 |
|
| Optimization | 2019-2023 |
|
| Innovation | 2023-current |
|
Table 2.
Defined daily doses per 10,000 patient days of 7 commonly used antibiotics (2011 to 2024).
| Antibiotic | DDD/1,000 PD (2011) | DDD/1,000 PD (2024) | DDD | Trend (2011-2024) |
Kendall Tau coefficient | p-value |
|---|---|---|---|---|---|---|
| IV Ciprofloxacin | 11.0 | 4.9 | 7.8 (4.4-9.4) | Decreasing | -0.853 | 0.000 |
| Ceftriaxone | 105.0 | 90.0 | 77.2 (73.7-82.9) | Stable | -0.165 | 0.412 |
| IV amoxicillin-clavulanate | 32.9 | 48.5 | 39.8 (34.2-43.4) | Increasing | 0.780 | 0.000 |
| Cefepime | 41.1 | 11.9 | 25.8 (12.8-30.2) | Decreasing | -0.641 | 0.001 |
| Piperacillin-tazobactam | 47.8 | 82.0 | 70.9 (63.8-78.5) | Increasing | 0.780 | 0.000 |
| Ertapenem | 13.8 | 7.5 | 9.0 (7.7-10.2) | Decreasing | -0.751 | 0.000 |
| Meropenem | 38.3 | 47.8 | 40.3 (38.3-44.7) | Stable | -0.011 | 0.956 |
DDD: Defined daily dose; PD: patient days. DDD expressed in median (IQR).
Table 3.
Hospital -wide susceptibility trend of the 10 Gram-negative bacilli towards 7 antibiotics (from 2011 to 2024).
Table 3.
Hospital -wide susceptibility trend of the 10 Gram-negative bacilli towards 7 antibiotics (from 2011 to 2024).
| Gram-negative bacilli | No. of isolates a year | Antibiotic | % Susceptibility (As of 2011 or 2014 for carbapenems) |
% Susceptibility (As of 2024) |
Susceptibility Trend | Kendall Tau coefficient |
p-value |
|---|---|---|---|---|---|---|---|
| Acinetobacter baumannii | 254 (216-378) | Ciprofloxacin | 33.6 | 74.4 | Increasing | 0.58 | <0.01 |
| Cefepime | 35.9 | 81.5 | Increasing | 0.56 | <0.01 | ||
| Piperacillin-tazobactam | 32.4 | 74.1 | Increasing | 0.66 | <0.01 | ||
| Meropenem | 48.5 | 79.8 | Increasing | 0.48 | <0.05 | ||
| Citrobacter freundii | 99 (88-110) | Ciprofloxacin | 70.2 | 74.6 | stable | 0.22 | 0.273 |
| Cefepime | 79.2 | 90.7 | Increasing | 0.53 | <0.05 | ||
| Ertapenem | 79.7 | 96.2 | Increasing | 0.65 | <0.01 | ||
| Meropenem | 80.6 | 99.2 | Increasing | 0.67 | <0.01 | ||
| Enterobacter spp.(including Klebsiella aerogenes) | 805 (747-885) | Ciprofloxacin | 78.2 | 77.6 | Stable | -0.17 | 0.412 |
| Cefepime | 82.8 | 88.6 | Increasing | 0.47 | <0.05 | ||
| Ertapenem | 86.7 | 92.7 | Increasing | 0.60 | <0.05 | ||
| Meropenem | 91.1 | 97.2 | Increasing | 0.52 | <0.05 | ||
| E. Coli | 4282 (3924-4738) | Ciprofloxacin | 51.4 | 53.1 | Stable | -0.10 | 0.622 |
| Ceftriaxone | 69.9 | 75.1 | Increasing | 0.59 | <0.01 | ||
| Amoxicillin-clavulanate | 66.0 | 79.6 | Increasing | 0.77 | <0.01 | ||
| Cefepime | 74.7 | 86.6 | Increasing | 0.73 | <0.01 | ||
| Piperacillin-tazobactam | 91.1 | 93.9 | Increasing | 0.49 | <0.05 | ||
| Ertapenem | 97.0 | 98.9 | Stable | 0.45 | 0.059 | ||
| Meropenem | 97.9 | 99.2 | Increasing | 0.55 | <0.05 | ||
| Klebsiella spp | 2323 (2180-2767) | Ciprofloxacin | 57.6 | 66.1 | Stable | 0.08 | 0.702 |
| Ceftriaxone | 60.5 | 76.7 | Increasing | 0.77 | <0.01 | ||
| Amoxicillin-clavulanate | 57.9 | 74.5 | Increasing | 0.76 | <0.01 | ||
| Cefepime | 63.0 | 84.1 | Increasing | 0.84 | <0.01 | ||
| Piperacillin-tazobactam | 73.0 | 84.6 | Increasing | 0.69 | <0.01 | ||
| Ertapenem | 94.3 | 95.9 | Increasing | 0.62 | <0.01 | ||
| Meropenem | 95.1 | 96.9 | Increasing | 0.53 | <0.05 | ||
|
Pseudomonas aeruginosa |
1522 (1380-1831) | Ciprofloxacin | 76.3 | 91.3 | Increasing | 0.93 | <0.01 |
| Cefepime | 84.5 | 96.4 | Increasing | 0.93 | <0.01 | ||
| Piperacillin-tazobactam | 90.7 | 92.9 | Increasing | 0.65 | <0.01 | ||
| Meropenem | 87.5 | 93.8 | Increasing | 0.86 | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



