
Submitted:
07 November 2025
Posted:
10 November 2025
You are already at the latest version
Abstract
Cancer is one of the biggest health burdens for women in the Middle East and North Africa (MENA), with the incidence of breast, cervical and colorectal cancer on the rise. Although preventive measures such as the HPV vaccination and population-based screening are available, access to them remains very unequal. Women in rural, low-income and refugee communities face additional barriers, cultural stigmatisation, low health literacy, gender norms and fragile health systems, leading to delayed diagnoses and poorer outcomes. This review summarises the results of 724 peer-reviewed publications to assess the current situation of cancer screening in MENA and Mediterranean countries. The studies were categorised along four dimensions: Cancer type (breast, cervical, colorectal), behavioural constructs (awareness, uptake, education), population vulnerability (e.g. migrants, refugees, low literacy groups) and geographical context (indigenous MENA population vs. diaspora communities). The results show large inequalities in access and participation due to fragmented policies, socio-cultural resistance and infrastructure gaps. Nevertheless, promising approaches are emerging: community-led outreach, mobile screening programmes, AI-assisted triage and culturally appropriate digital health interventions. Comparisons between the local and diaspora populations make it clear that systemic and cultural barriers persist even in well-equipped facilities. Closing the screening gap requires a culturally sensitive, digitally enabled and policy aligned approach. Key priorities include engaging religious and community leaders, promoting men's engagement in women’s health and securing sustainable funding. With coordinated action across all sectors, MENA countries can build inclusive screening programmes that reach vulnerable women and reduce preventable cancer mortality.
Keywords:
cancer screening
; MENA region
; cervical cancer
; breast cancer
; colorectal cancer
; health disparities
; refugees
; immigrant health
; health literacy
; culturally adapted interventions
; AI in screening
; digital health
; early detection
; public health policy
1. Introduction
Cancer continues to be a major public health challenge worldwide, with the burden increasing particularly among women in low- and middle-income countries. In the Middle East and North Africa (MENA) region, the burden of cancer in women has increased in parallel with demographic and lifestyle changes and new reproductive patterns. Recent global cancer statistics show that breast, cervical, and colorectal cancers are leading causes of morbidity and mortality among women in the MENA region, reflecting global trends but with distinct regional differences in screening, prevention, and early detection [ 1]. Breast cancer remains the most common cancer and the leading cause of cancer-related deaths among women in the MENA region. Rising incidence is attributed to delayed childbirth, lower parity, and limited access to screening programs. Despite the initiation of national screening programs in many countries, disparities in coverage, awareness, and follow-up persist, particularly in rural and conflict-affected areas. Research on refugee and immigrant populations highlights the increased vulnerability of women from MENA countries living in host nations, where cultural and linguistic barriers hinder their participation in standard screening programs [2].
Cervical cancer is becoming more common in the MENA region, even though it is largely preventable through human papillomavirus (HPV) vaccination and regular Pap tests. This increase is due to insufficient use of these preventive measures in the past. Countries such as Algeria and Lebanon have developed cost-effective models demonstrating that HPV vaccination is a sound public health investment. However, implementation remains limited because of cultural sensitivities, vaccine hesitancy, and unreliable health infrastructure. Public awareness of HPV and cervical cancer remains low, which is particularly concerning among adolescents and young women, who are a key target group for vaccination programs [3,4].
Colorectal cancer (CRC), once considered a disease primarily affecting older adults in high-income countries, is becoming increasingly common among younger populations in MENA countries. Limited public awareness, lack of structured screening programs, and the stigma associated with gastrointestinal symptoms hinder timely diagnosis and negatively impact treatment outcomes. Fecal occult blood testing (FOBT), colonoscopy, and risk stratification tools are not always accessible, and targeted interventions are needed to increase awareness and improve screening among the general public [5,6].
Overall, while some MENA countries have made progress in developing cancer control strategies and implementing screening programs, the region continues to face systemic barriers, including staff shortages, fragmented data systems, gender inequalities in access to healthcare, and continued political instability in certain areas. In addition, regional disparities between urban and rural populations and between indigenous and displaced populations highlight the urgent need for a contextualized approach to cancer prevention and screening. To ensure that this review is based on comprehensive and representative evidence, we systematically analyzed a corpus of 724 peer-reviewed publications addressing cancer prevention, education and early detection in vulnerable populations in the Mediterranean, North Africa and the Middle East (MENA). The search strategy combined several dimensions: (1) cancer type breast, cervical and colorectal cancer; (2) behavioral constructs such as screening uptake, awareness, education, invitation strategies; (3) population vulnerability, targeting migrants, low-income communities, ethnic minorities and individuals with low health literacy; and (4) geographical relevance, limiting the results to studies covering the Mediterranean, Southern Europe, North Africa or the Middle East.
Within this pool of literature, breast cancer proved to be the most comprehensively studied cancer type with 272 studies, followed by colorectal cancer with 118 studies and cervical cancer with 92 studies. Despite these differences, all three cancer types were well represented, providing comparative insights into cancer-specific screening pathways. Importantly, a substantial number of studies were conducted in MENA countries, including 64 on cervical cancer, 87 on breast cancer and 40 on colorectal cancer. These studies cover a wide range of contexts, from urban hospitals in Lebanon and Morocco to outreach programs in Algeria and Jordan.
The dataset also included a subset of studies looking at refugee and displaced populations (n=9), reflecting the increased vulnerability of these groups to exclusion from preventive health services. In addition, many studies (n=472) were conducted in Western contexts, particularly in the United States, and focused on MENA immigrant and Arab diaspora communities. These diaspora-focused studies provided important insights into how cultural, linguistic, and systemic barriers persist even in well-resourced healthcare settings. Their inclusion provides a valuable contrast to the challenges at home and illuminates how both structural and socio-cultural determinants operate across borders.
This diverse and geographically stratified evidence base not only justifies the scope of this review, but also enables a comparative analysis of barriers, interventions and outcomes for indigenous and immigrant MENA populations and for different cancer types. The following synthesis builds on this extensive literature and aims to identify both common challenges and context-specific opportunities to improve screening and uptake of cancer screening in these underrepresented groups. Drawn from 724 peer-reviewed publications, the keyword coincidence map provides a multidimensional overview of the scientific landscape addressing cancer prevention, early detection and health inequalities in Mediterranean and MENA populations. This visual representation shows the main thematic structures and links between disciplines from nutritional epidemiology to molecular oncology and health policy.
A densely populated cluster centered on the concept of the “Mediterranean diet” lies at the heart of the network. This concept is emerging as a key link in research on reducing cancer risk. Its prominence and extensive connections to terms such as “coronary heart disease,” “inflammation,” “mortality,” and “pattern” indicate a shared interest in diet as a modifiable risk factor for various non-communicable diseases, including cancer. Additional links to “food intake frequency questionnaire,” “cohort study,” and “validation” demonstrate that the methodology relies on nutritional assessment and long-term population research.
A large portion of the map, anchored by this core, focuses on breast cancer. This area is frequently associated with terms like “risk,” “expression,” “mutation,” “BRCA,” and “gene.” Here, genetic susceptibility, biomarker profiling, and tumor biology intersect in translational and clinical research. The terms “apoptosis,” “in vitro,” “activation,” and “antioxidant” highlight the significant laboratory component of the literature, particularly experimental studies investigating the anti-cancer effects of bioactive compounds (such as oleic acid, hydroxytyrosol, phenols, and olive oil) found in the Mediterranean diet.
In contrast, the cervical cancer cluster appears in the lower left corner of the map, representing the area of public health and implementation science in the literature. Key terms include “HPV,” “awareness,” “Pap smear,” “acceptance,” and “screening,” along with country-specific terms like “Lebanon,” “Tunisia,” and “Middle East.” This cluster reflects substantial efforts to understand and increase cervical cancer screening rates among vulnerable and traditionally underserved populations. Connections to terms such as “attitudes,” “education,” “adolescents,” and “self-efficacy” underscore the importance of psychosocial and behavioral factors in determining screening uptake among women in the MENA region. The map also displays a socio-political layer, featuring terms such as “barriers,” “policy,” “access,” “services,” and “health literacy,” which indicate systemic and structural issues. The terms “women,” “population,” “impact,” and “refugee” are closely linked, reflecting increasing research on disparities in healthcare access between immigrant and indigenous populations. This intersectional space underscores the importance of gender, migration status, and socioeconomic vulnerability in determining who benefits from screening initiatives. The close proximity of epidemiology, public health, and biomarker-related clusters further demonstrates the field’s shift toward more integrated and translational approaches. Additionally, terms like “machine learning,” “systems biology,” and “methylation” highlight growing interest in computational and omics-based methods for early disease detection and personalized screening models.
The co-occurrence map reveals extensive interconnected research. It highlights the prevalence of breast and cervical cancer in screening, the central role of diet and lifestyle in prevention strategies, and the urgent need for culturally sensitive, accessible, and policy-driven interventions, particularly for at-risk populations in the MENA and Mediterranean regions. The spatial distribution of terms illustrates the increasing integration of biomedical, behavioral, and systemic domains in advancing equitable cancer prevention. This review summarizes evidence on screening behaviors, barriers, and intervention strategies in MENA countries, focusing on breast, cervical, and colorectal cancer. By linking regional epidemiological data with findings from studies on immigrants and refugees, we aim to develop targeted, culturally sensitive public health strategies and inform future research and policy initiatives for cancer prevention.
Figure 1.
Co-occurrence network of keywords in peer-reviewed literature on cancer prevention, screening, and Mediterranean health determinants (n = 724 studies).
Figure 1.
Co-occurrence network of keywords in peer-reviewed literature on cancer prevention, screening, and Mediterranean health determinants (n = 724 studies).
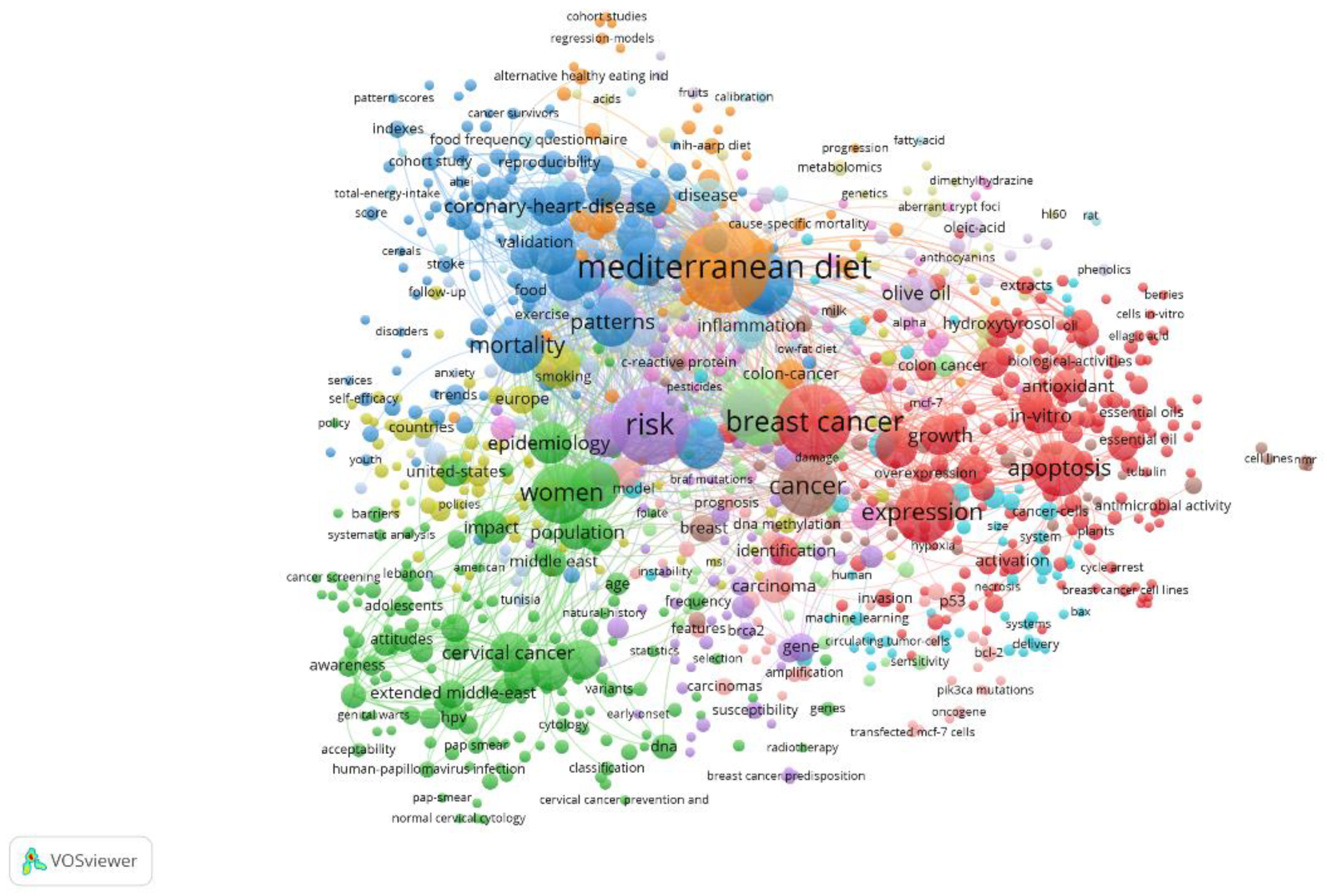
This figure visualizes the thematic landscape of the included literature, generated through a VOSviewer analysis of co-occurring keywords from 724 peer-reviewed publications. Nodes represent keywords, while their size reflects the frequency of occurrence. The proximity and thickness of lines indicate the strength of co-occurrence relationships between concepts.
The Importance of Early Detection and Prevention
Early detection and prevention are generally recognized as cornerstones of effective cancer control. In the context of the MENA region, these strategies are particularly important given the increasing burden of cancer and the systemic challenges that delay diagnosis and treatment. Cancers such as breast, cervical and colorectal cancers are highly detectable at an early stage, and when detected at an early stage, patient outcomes improve significantly while treatment costs and morbidity decrease substantially[7].
Screening programs such as mammography for breast cancer, Pap smears and HPV testing for cervical cancer, and fecal occult blood tests or colonoscopy for colorectal cancer have been shown to reduce mortality through early detection of precancerous lesions or asymptomatic disease. Prevention through vaccination, especially in the case of HPV-related cervical cancer, holds great potential for change[8]. The World Health Organization’s Global Strategy to Eliminate Cervical Cancer as a Public Health Problem targets 90% of girls to be fully vaccinated with the HPV vaccine by the age of 15. However, in many MENA countries, national HPV vaccination programs continue to be implemented inconsistently or not at all. Despite model studies demonstrating the cost-effectiveness of such measures, uptake is low, even in pilot programs, due to the hesitant attitude towards the vaccine and the lack of political prioritization[9,10,11,12,13].
From a public health perspective, investment in prevention and early detection provides significant benefits, both in lives saved and reduced healthcare costs. Efforts to promote culturally appropriate health education, patient navigation, and community engagement have shown promise in increasing screening rates and immunization coverage among both indigenous and diaspora populations of MENA countries [14]. Digital health technologies and artificial intelligence also offer new ways to assess and counsel individuals about their risks, especially in underserved or conflict-affected areas. Making services available to the MENA population is not sufficient; it is also necessary to build trust, cultural competence, and health literacy among the target groups. This is particularly important for vulnerable groups, such as refugees and immigrants, who may have limited access to healthcare and maintain traditional health beliefs. A shift toward evidence-based, inclusive, and sustained investment in preventive oncology in MENA countries could significantly improve cancer-related outcomes in the region.
2. HPV and Cervical Cancer in the MENA Population
Knowledge Gaps, Vaccine Introduction and Cost-Effectiveness Models
Cervical cancer remains one of the most preventable but still neglected cancers among women in the MENA region. Although it is largely due to persistent infection with high-risk types of human papillomavirus (HPV), the region lags behind global benchmarks in both awareness and prevention. The studies included in this review consistently point to profound gaps in knowledge among adolescents, young women and even healthcare professionals regarding HPV transmission, the link between HPV and cervical cancer, and the existence and purpose of the HPV vaccine[15,16,17].
A study of female college students in Lebanon found that only 42% had heard of HPV, and even fewer knew it was linked to cervical cancer. In Algeria and Jordan, where misconceptions about HPV and the vaccine were common, similar knowledge gaps were observed. Healthcare providers were hesitant to recommend the vaccine because they lacked sufficient information and were uncomfortable discussing sexually transmitted infections in general. As a result, very few people in the MENA region are vaccinated. Most countries do not include HPV vaccination in their national immunization programs. Pilot programs exist, but they are limited to private health facilities or donor-funded initiatives. For example, in Lebanon, fewer than 10% of teenage girls have been vaccinated due to high costs and insufficient public funding. Studies of refugees in the US and Europe found even lower vaccination rates, with cultural barriers and lack of provider recommendations cited as the main reasons [18,19,20].
Despite these challenges, cost-effectiveness models offer compelling support for national implementation. A study examining the introduction of the HPV vaccine in Algeria concluded that vaccinating 10-year-old girls could be highly cost-effective, with incremental cost-effectiveness ratios (ICERs) well below WHO-recommended thresholds. These models suggest that HPV vaccination, if delivered efficiently, could significantly and cost-effectively reduce the burden of cervical cancer, especially when combined with screening measures such as Pap smears or HPV DNA testing[21,22].
School-based vaccination strategies, peer education and physician-led communication campaigns have been suggested as culturally acceptable approaches to improve uptake. However, few countries have implemented such measures nationwide. This implementation gap reflects a lack of prioritization in the public health agenda, although it is well justified from an epidemiological and economic perspective[23].
To address cervical cancer caused by HPV in the MENA region, a multi-pronged approach is necessary. This should include raising awareness, overcoming cultural barriers, and incorporating the HPV vaccine into national immunization programs. To reduce preventable deaths among women in the MENA region, cost-effective and culturally appropriate solutions based on local data and public engagement in health issuesare essential [24,25,26,27,28]. Given the low uptake and high prevalence of cervical cancer, prioritizing HPV vaccination in regional public health initiatives is imperative. School-based vaccination programs for girls aged 9 to 14, tailored to local cultural contexts and supported by educational resources for parents and teachers, offer a feasible and effective strategy to mitigate the long-term impact of cancer.
3. Disparities and Indicators in Screening
3.1. Cultural, Socioeconomic, and Systemic Influences
In the MENA region, cancer screening remains underutilized, especially for breast, cervical, and colorectal cancers. This underuse results not only from limited resources and infrastructure but also from deeply rooted cultural beliefs, socioeconomic disparities, and systemic barriers within the healthcare system. Understanding these multifactorial predictors is crucial for designing interventions that increase screening rates among MENA women and reduce avoidable cancer deaths [29].
3.1.1. Cultural Elements
Cultural beliefs and norms related to modesty, fatalism, and gender roles significantly influence screening behaviors. In many MENA countries, women are hesitant to undergo screening, particularly pelvic examinations or mammography, due to feelings of shame, the need for male physician consent, or fear of social stigma. Studies in Jordan and Lebanon show that religious and cultural sensitivities hinder women’s participation in cervical and breast cancer screening programs. Cultural norms also remain a major barrier to obtaining Pap smears and mammograms among MENA immigrants in Western countries, including the United States, especially when services lack linguistic or cultural appropriateness [30].
3.1.2. Socioeconomic Indicators
Socioeconomic status, including educational attainment, income, and employment, is a significant predictor of screening participation. Women with low levels of education are consistently less likely to seek screening due to low health literacy, limited awareness of cancer risks, and reduced ability to navigate healthcare systems. In Lebanon and Algeria, research has shown that low-income women are markedly underrepresented in structured screening programs. Concerns about cost, especially for women without insurance or access to public healthcare, often lead them to delay or forgo screening altogether [31,32].
3.1.3. Barriers in the System
Even when individuals are aware of the issue and want to participate, systemic problems within the health system create additional challenges. These include insufficient primary care infrastructure, lack of national screening programs, irregular or opportunistic screening methods, and inadequate follow-up systems.
Healthcare providers also present a significant barrier. In the MENA region, many doctors do not routinely recommend screening unless patients request it. This missed opportunity for early detection is often due to limited time, insufficient training, and discomfort discussing cancer risks with patients. Long wait times, long distances to clinics, and a shortage of female healthcare providers further reduce screening rates among women. Refugees and displaced individuals, who often live in underserved or unstable areas, face additional obstacles, including legal and financial exclusion from national health systems [33]. These factors frequently interact and reinforce one another. For example, a woman with a low income may have difficulty accessing a clinic, and even if she does, she may encounter a provider who lacks training in culturally sensitive communication, making her less likely to seek follow-up care. This intersectional perspective highlights the need for comprehensive, multilevel approaches that address individual, community, and health system determinants [34].
3.2. Immigrant vs. Native MENA Population
Geographic context further complicates differences in cancer screening among the MENA population. Immigrants in host countries face distinct obstacles compared to women in their countries of origin. While both groups share cultural norms and potential knowledge gaps, immigrant women from MENA countries often encounter additional challenges related to migration status, navigating unfamiliar healthcare systems, and socio-political marginalization.
For example, studies of Arab-American and MENA immigrant women in the US show they are much less likely to be screened for cervical and breast cancer than the general population. Some reasons for this gap include limited English proficiency and lack of translated materials, distrust or unfamiliarity with Western healthcare systems, lower likelihood of receiving a doctor’s recommendation, fear of stigma – especially regarding HPV and sexually transmitted infections – and stress from immigration and competing survival priorities.
Insurance coverage is also a significant issue. Many MENA migrants in host countries lack access to healthcare, particularly those who are temporary, undocumented, or refugees. Even when services are theoretically available, cultural insensitivity and the scarcity of female or Arabic-speaking healthcare providers can discourage utilization.
Women in MENA countries, by contrast, often face a different set of challenges. These are primarily due to weak health systems, irregular screening practices, and political instability. For example, cervical screening in Lebanon and Algeria is often sporadic rather than systematic, and many rural clinics lack the staff or resources to perform Pap smears or follow-up biopsies. National screening programs, where they exist, are frequently underfunded and inconsistently implemented.
Interestingly, some immigrant MENA groups in high-income countries report greater exposure to public health messages and increased awareness, despite poorer socioeconomic conditions. However, this does not always translate into higher screening rates due to persistent structural and cultural barriers. This duality underscores the need for context-sensitive strategies that address the diverse realities of MENA women based on their environment. For immigrant patients, culturally appropriate patient navigation, interpreter services, and participation in public health programs are essential. For the indigenous population, priorities include strengthening primary care, educating healthcare providers, and institutionalizing screening through national campaigns and educational initiatives in schools.
Importantly, men’s involvement in women’s health decisions should not be overlooked. In many MENA households, men play an important role in granting permission for medical visits or allocating family resources. Engaging men through targeted awareness campaigns and their participation in community-based initiatives could improve support for women’s participation in screening programmes and counter patriarchal barriers.
Figure 2.
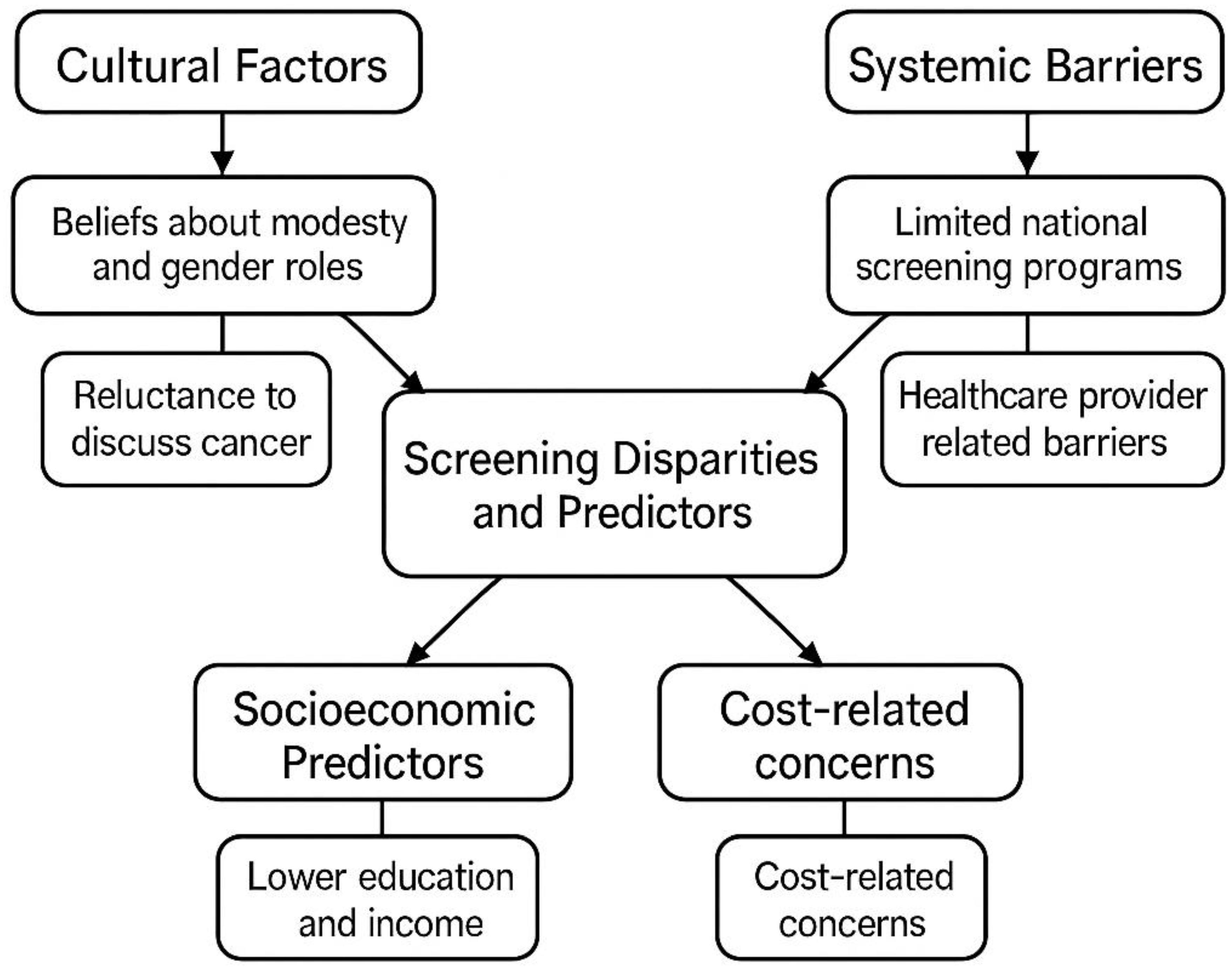
Conceptual diagram illustrating the main factors contributing to cancer screening inequalities and predictors in the MENA and Mediterranean populations. The framework highlights four main areas: cultural factors (e.g., beliefs about modesty, reluctance to talk about cancer), systemic barriers (e.g., limited national infrastructure for cancer screening and challenges related to care providers), socioeconomic predictors (e.g., lower income and education levels), and cost-related concerns. These interrelated elements combine to determine inequalities in awareness, access and participation in screening programs for breast, cervical and colorectal cancer.
Figure 2.
Conceptual diagram illustrating the main factors contributing to cancer screening inequalities and predictors in the MENA and Mediterranean populations. The framework highlights four main areas: cultural factors (e.g., beliefs about modesty, reluctance to talk about cancer), systemic barriers (e.g., limited national infrastructure for cancer screening and challenges related to care providers), socioeconomic predictors (e.g., lower income and education levels), and cost-related concerns. These interrelated elements combine to determine inequalities in awareness, access and participation in screening programs for breast, cervical and colorectal cancer.
4. Culturally Adapted Interventions
4.1. Case Studies of Tailored Navigation and Education Programs
Cultural stigma, rooted in ideas about modesty, sexuality, and fatalism, continues to prevent people in some MENA countries from getting screened. Low health literacy and taboos around discussing cancer or reproductive health often worsen this stigma. To address these issues, it is necessary not only to improve access to information but also to adapt messages to align with cultural values such as family well-being and religious teachings about caring for one’s health. To improve cancer screening for underserved populations, such as women from the MENA region, it is essential to ensure that services are accessible and culturally relevant. Culturally appropriate interventions are increasingly recognized as effective strategies to reduce disparities in screening uptake. These approaches focus on tailoring messages, access methods, and care delivery to the sociocultural and linguistic needs of target populations. The following models and case studies demonstrate how culturally appropriate education, patient navigation, and community engagement have successfully increased cancer screening rates among people in MENA countries and other marginalized groups.
4.2. Health Literacy and Culturally Sensitive Education
One of the most reliable indicators that people will not get screened is a lack of health knowledge. Culturally sensitive education programs aim to clarify and contextualize health information, often using visual aids, narrative accounts, and linguistically appropriate content. Balamou et al. (2023) [35] launched a tailored health education program in France for underserved migrant women facing low literacy and language barriers [36]. The initiative significantly improved understanding of screening recommendations for breast, cervical, and colorectal cancer by using images and simpler language. In Portugal, Gama et al. (2024) applied a health literacy framework to develop educational events for African and Brazilian migrant women in Lisbon, resulting in increased awareness of cervical cancer and greater willingness to participate in screening [37].
Hamdiui et al. (2022) developed a culturally appropriate video intervention for Turkish and Moroccan-Dutch women in the Netherlands. The video incorporated religious sensitivity, language adaptation, and trusted community voices. This approach increased positive attitudes toward cervical cancer screening and trust in public health systems. These case studies show that health education is most effective when it takes into account cultural values, religious beliefs, and preferred communication methods. Culturally appropriate framing, such as emphasizing family well-being or religious compatibility, can increase engagement, especially in MENA countries and among Muslim-majority populations [38].
4.3. Patient Navigation and Language Mediation
Patient navigation strategies provide logistical and emotional support to help people through complex or unfamiliar medical procedures. They are particularly effective with immigrant who have limited familiarity with the system.
In Italy, Palazzi et al. (2016) used telephone-based call-back systems combined with language mediation in the city of Cesena. This program successfully improved migrant women’s participation in cervical cancer screening by bridging communication gaps and easing administrative challenges [39]. In Spain, several programs in Barcelona [40] have shown that personalized invitation letters, telephone follow-ups and the involvement of community mediators increase rates of cervical and breast cancer screening in neighborhoods with a high proportion of migrants [41].
The Marseille study by Piana et al. (2007) went a step further by offering free screening and holding information sessions in the community to build trust and reduce anxiety. The inclusion of culturally relevant facilitators and peer speakers created a safe environment for discussion, which in turn encouraged participation[42].
In each of these cases, navigation efforts were more effective when they combined practical support (scheduling, reminders) with cultural mediation and emotional reassurance, especially in communities where health care is perceived as intimidating or inaccessible.
4.4. Peer Educator and Community-Led Models
Community involvement is essential for sustainable behavior change. Interventions in which local women are trained as peer educators or community health workers have proven to be particularly effective in promoting cancer prevention.
In Lorraine, France, Cambon et al. introduced a participatory, peer-led program targeting precarious women from immigrant communities. These peer educators, who often have the same cultural background as the target group, fostered trust and credibility so that the message was better received. Similarly, in Marseille, Legendre et al. (2024) [43] used trained health mediators from local communities to provide targeted education. This strategy led to increased uptake of breast, cervical and colorectal cancer screening, especially among women with limited education or health literacy. Such bottom-up models empower communities, increase local capacity and reinforce shared norms around screening. They also counteract the historical mistrust of medicine that is widespread among migrants and refugees. In addition to peer educators, the involvement of local religious leaders and trusted community influencers can further increase the uptake and reach of cancer prevention interventions. In many MENA communities, imams, spiritual leaders and respected elders play a critical role in shaping health behaviours and social norms. Training these individuals to deliver culturally sensitive health messages in mosques, at community gatherings or via social media could strengthen advocacy and reduce stigma, particularly around issues such as HPV vaccination and cervical screening.
4.5. Integration into Primary Care and Support at System Level
Cultural adaptation alone is not enough if it is not integrated into the wider healthcare system. Effective interventions need to fit into primary care workflows, leverage relationships with providers and ensure continuity of care.
In a French cluster-randomized controlled trial, Durand et al. (2021) trained GPs to provide visual educational materials tailored to adults with low literacy skills. This simple, scalable intervention led to a significant increase in colorectal cancer screening rates in the intervention clinics. Importantly, GPs were perceived as a credible and accessible source of health advice, especially in populations that previously lacked confidence in the medical system [44]. The success of this approach underscores the need to train healthcare professionals in cultural competence and to develop standardized tools to facilitate risk communication, motivational interviewing, and shared decision making among diverse patient populations.
Taken together, these case studies provide tangible evidence that culturally appropriate interventions, when implemented at multiple levels and with community involvement, can significantly reduce cancer screening disparities in MENA and other vulnerable populations. Education, navigation and community participation, when embedded in primary care and public health infrastructures, are not only effective but also necessary to achieve equitable cancer prevention outcomes. Policy makers and practitioners need to prioritize these strategies in national screening programs, especially in areas of high ethnic diversity, migration and social exclusion[45].
5. Challenges in the Implementation of Health Policy
Although the burden of cancer is increasingly recognized in MENA countries, the translation of evidence into effective, equitable screening programs remains uneven. Numerous structural, systemic and political challenges have hampered the development and implementation of national screening strategies for breast, cervical and colorectal cancer. These challenges are exacerbated by competing health priorities, conflict-related instability and underfunded health systems[46].
5.1. Infrastructural and Systemic Gaps
Basic health infrastructure remains a fundamental barrier to cancer prevention in much of the MENA region. While some high-income countries such as the Gulf States have the resources to implement advanced screening programs, lower and middle-income countries often lack essential components such as:
- Trained primary care providers and gynecologists
- Laboratory services for cytology or HPV DNA testing
- Colposcopy and biopsy follow-up services
- Electronic data systems for screening reminders and follow-up
A review of cervical cancer screening services in Algeria and Jordan, for example, found that many public facilities are limited to opportunistic Pap testing, with no standardized protocols or follow-up pathways. Screening is often not integrated into routine primary care, and rural clinics in particular are not adequately equipped to provide early detection and referral.
Even in urban areas where services do exist, the fragmentation of care between public, private and NGO-run services leads to inefficiencies and missed opportunities. The lack of centralized data makes monitoring and quality control at the national level difficult. These gaps are particularly acute in conflict zones, where both healthcare infrastructure and data systems are often lacking. There is an urgent need for disaggregated, country-specific data, especially in fragile situations, in order to take customised action. Without reliable epidemiological and service delivery data, planning and evaluating cancer screening programmes remains a challenge in many parts of the MENA region.
5.2. Access to Healthcare and Equal Opportunities
Geographic, economic and social barriers prevent many women, especially those in rural or marginalized urban communities, from accessing preventive health care. Out-of-pocket costs, transportation barriers and lack of paid time off from work disproportionately affect low-income women. In some countries, screening is not covered by general health plans, leaving many women to rely on sporadic NGO programs or private providers.
In addition, refugees and displaced persons - a growing population group in conflict areas such as Lebanon, Jordan and Palestine - are often left out of state health provision altogether. Their access to preventive services is highly dependent on external assistance and is often not continuous or comprehensive.
Social factors, such as women’s lack of autonomy in health decisions and the stigmatization of cancer, further inhibit the uptake of screening. Cultural taboos around pelvic exams and fear of cancer diagnoses were cited as psychological barriers to screening uptake, even in facilities where services are physically available.
5.3. Political Instability and Competing Health Priorities
Many MENA countries have delayed investing in public health due to political and economic challenges. Chronic underfunding, civil unrest, and shifting donor priorities often result in cancer screening being postponed in favor of more urgent issues such as maternal and child health, infectious diseases, and emergency care.
For example, the recent economic collapse in Lebanon has significantly affected public health services, making it difficult to sustain screening programs. In areas like Syria, Iraq, and parts of Libya where conflict persists, basic medical care has ceased, and cancer screening is nearly nonexistent. Even in more stable countries, health ministries may prioritize diseases with more immediate short-term impacts or those that attract greater international donor interest [47]. Although there is evidence that HPV vaccination and cervical cancer screening are cost-effective, policymakers are often slow to implement changes. Progress is hindered by a lack of political will, poor coordination between ministries (such as health and education), and weak advocacy platforms [48,49].
Implementing cancer screening policies in the MENA region is extremely challenging due to infrastructure problems, unequal access, and political fragmentation. To address these gaps, regional strategies should prioritize:
- Integrating screening into routine primary care
- Expanding services in rural areas
- Ensuring long-term funding and policy stability
- Collaborating across sectors to align health, education, and community development
Without these measures, even the most effective interventions will struggle to significantly reduce cancer disparities in MENA countries.
6. Possibilities and Future Directions
6.1. AI-Supported Education, Digital Health Literacy and Policy Recommendations
While cancer prevention in the MENA region faces numerous systemic and socio-cultural barriers, there are some promising opportunities at the intersection of technology, health education and policy reform. By leveraging innovations in artificial intelligence (AI), digital communication platforms, and evidence-based policymaking, MENA countries can create scalable, culturally sensitive solutions to improve cancer screening, particularly among women and underserved groups[50,51].
6.2. AI-Powered Outreach and Risk Stratification
Artificial intelligence (AI) and machine learning (ML) offer significant potential for personalizing cancer screening strategies and optimizing resource allocation in low-resource settings. AI-driven models can help:
- Identify high-risk individuals using electronic health records or self-reported data with minimal input
- Automate reminder systems tailored to language, literacy or screening history
- Prediction of non-compliance and suggestions for personalized nudges or navigator support
In high-income MENA countries (e.g. UAE, Saudi Arabia), innovative digital health ecosystems are already exploring AI applications in public health. Extending these tools to screening algorithms and culturally adapted chatbot interfaces (in Arabic, Tamazight, etc.) could help bridge the gap between awareness and participation, especially among digitally connected youth and urban women.
However, equal treatment must be ensured: prediction algorithms must be transparent, must not contain biases against minorities or migrants, and must be embedded in a framework that protects privacy. Investment in open, region-specific datasets and collaboration between health authorities and data scientists will be critical to the utility of AI in real-world screening programs in MENA countries.
6.3. Digital Health Literacy and Mobile Health Interventions
Cell phones are widely used across the MENA region, including in resource-poor and refugee settings. This presents a great opportunity for mobile health (mHealth) interventions to support cancer prevention[52,53]. Examples include:
- SMS-based appointment reminders and health alerts
- Video education via WhatsApp in local dialects
- QR codes that lead to visual explanations of Pap smears or mammograms
- Teleconsultation apps with culturally competent providers
Improving digital health literacy, i.e. the ability to access, understand and act on digital health information, is critical. Community-based training initiatives, school-based digital health programs for youth, and partnerships with women’s cooperatives or mosques can play a central role in bridging the digital divide[53]. Digital tools must also be developed together with the target groups to ensure their usability, relevance and trust. Pilot projects in Lebanon and Morocco have shown that visual and voice-activated mobile applications can support informed screening decisions even in populations with low literacy levels.
6.4. Suggestions for Policies to Support Fair and Long-Term Growth
Policy changes are necessary for sustained improvements in access to and use of screening. Based on the evidence summarized in this review, the following policy recommendations are proposed for MENA governments and stakeholders:
1. Integrate screening for cervical, breast, and colorectal cancer into maternal and child health services.
- Leverage vaccination campaigns (such as HPV) to coordinate with other interventions.
2. Launch cost-effective national HPV vaccination programs. Use school-based models to reach girls before puberty. Seek support from Gavi or WHO for vaccine procurement and distribution.
3. Institutionalize community health workers and mediators.
- Train culturally competent navigators to serve in clinics, refugee centers, and community settings.
- Provide certification, fair compensation, and digital tools to expand their reach.
4. Ensure providers receive training that is both gender-sensitive and culturally sensitive. This will address provider bias and ensure patients are treated with respect and understanding. Incorporate cross-cultural communication skills into medical and nursing education.
5. Strengthen data systems and evaluation frameworks. - Use AI and digital registries to monitor participation, follow-up, and outcomes. - Disaggregate reports by gender, location, and migration status.
6. Promote cross-border collaboration and knowledge sharing by establishing regional consortia (such as the Maghreb-Eastern Med Cancer Screening Network) and facilitating the exchange of best practices, digital tools, and joint procurement agreements.
7. Ensure sustainable funding mechanisms for cancer screening programs.
- Allocate long-term budget lines in national health plans.
- Explore public-private partnerships and international donor engagement to maintain program continuity, especially in low-income and conflict-affected countries.
Combining new technologies with cultural sensitivity and a practical public health approach is essential for cancer prevention in MENA countries. By adopting AI, building digital health capacity, and developing inclusive policy frameworks, MENA countries can close persistent gaps in cancer screening and set an example for others in advancing global health equity. Political will, sustained investment, and collaboration are all critical to achieving this transformation.
7. Conclusions
Deep-seated structural, economic, and socio-cultural obstacles continue to impede cancer prevention and screening in the MENA region. Although effective tools such as HPV vaccines, mammograms, and fecal occult blood tests exist, their use remains limited, especially among vulnerable groups like migrants, low-income women, and displaced people. Fragmented implementation of screening programs, low awareness, and poor coordination between ministries continue to slow progress. However, the review indicates promising ways forward. Culturally appropriate interventions, including peer navigator models, multilingual communication strategies, school-based education, and policy advocacy, have been shown to increase participation. Additionally, integrating digital platforms and artificial intelligence into early detection strategies offers scalable and cost-effective solutions, particularly in settings with limited resources or political instability.
To close existing gaps, a combination of evidence-based policy, community empowerment, and new technologies is required. Public health, education, civil society, and digital health stakeholders must collaborate to build a robust screening infrastructure, ensure equitable access, and adapt strategies to the diverse cultural and socio-economic contexts of the MENA region. Only through such comprehensive efforts can all women, regardless of background or income, access life-saving cancer screening services.
Author Contributions
Conceptualization: RV, Investigation: SG, OFM., MMA, RV. Writing-original draft: R. Writing-review and editing: all authors. Supervision: RV.
Funding Information
This article is based upon work from COST Action Medi-CaSE (CA23151) https://www.cost.eu/actions/ Action CA23151) funded by COST (European Cooperation in Science and Technology; www.cost.eu). This work was also financed by national funds through FCT - Fundação para a Ciência e Tecnologia, I.P., within the scope of the Cardiovascular R&D Center (UIDB/00051/2020 and UIDP/00051/2020) and RISE (LA/P/0053/2020), for funding Institute of Biomedicine (iBiMED) (UIDB/04501/2020, POCI-01-0145-FEDER-007628).
Data Availability Statement
None.
Acknowledgments
We thank all medical professionals who are associated with our practice.
Declaration of Competing Interest
The authors declare no conflicts of interest.
AI Disclosure Statement
All images included in this work were created using Canva® under human supervision, with manual editing and review to ensure accuracy and consistency. Editing in English was supported by the InstaText® tool, with all suggestions carefully reviewed and approved by the authors.
References
- Zahwe, M.; Bendahhou, K.; Eser, S.; Mukherji, D.; Fouad, H.; Fadhil, I.; Soerjomataram, I.; Znaor, A. Current and future burden of female breast cancer in the Middle East and North Africa region using estimates from GLOBOCAN 2022. International journal of cancer 2025, 156, 2320–2329. [Google Scholar] [CrossRef]
- Arnold, M.; Morgan, E.; Rumgay, H.; Mafra, A.; Singh, D.; Laversanne, M.; Vignat, J.; Gralow, J.R.; Cardoso, F.; Siesling, S.; et al. Current and future burden of breast cancer: Global statistics for 2020 and 2040. Breast 2022, 66, 15–23. [Google Scholar] [CrossRef]
- Carlos, R.C.; Dempsey, A.F.; Patel, D.A.; Dalton, V.K. Cervical cancer prevention through human papillomavirus vaccination: using the “teachable moment” for educational interventions. Obstet Gynecol 2010, 115, 834–838. [Google Scholar] [CrossRef]
- Vincent, S.C.; Al Yaquobi, S.; Al Hashmi, A. A Systematic Review of Knowledge, Attitudes, and Factors Influencing HPV Vaccine Acceptance Among Adolescents, Parents, Teachers, and Healthcare Professionals in the Middle East and North Africa (MENA) Region. Cureus 2024, 16, e60293. [Google Scholar] [CrossRef]
- Shamseddine, A.; Chehade, L.; Al Mahmasani, L.; Charafeddine, M. Colorectal Cancer Screening in the Middle East: What, Why, Who, When, and How? American Society of Clinical Oncology educational book. American Society of Clinical Oncology. Annual Meeting 2023, 43, e390520. [Google Scholar] [CrossRef] [PubMed]
- Balata, G.F.; Azzam, H.N. Synopsis of colorectal cancer: prevalence, symptoms, screening, staging, risk factors, and treatment. The Egyptian Journal of Internal Medicine 2025, 37, 4. [Google Scholar] [CrossRef]
- Pace, L.E.; Shulman, L.N. Breast Cancer in Sub-Saharan Africa: Challenges and Opportunities to Reduce Mortality. The oncologist 2016, 21, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Gorina, Y.; Elgaddal, N. Patterns of Mammography, Pap Smear, and Colorectal Cancer Screening Services Among Women Aged 45 and Over. Natl Health Stat Report 2021, 1–18. [Google Scholar]
- Chiumento, A.; Hosny, W.; Gaber, E.; Emadeldin, M.; El Barabry, W.; Hamoda, H.M.; Alonge, O. Exploring the acceptability of a WHO school-based mental health program in Egypt: A qualitative study. SSM-Ment. Health 2022, 2, 12. [Google Scholar] [CrossRef]
- Adigüzel, F.I.; Adigüzel, C.; Seyfettinoglu, S.; Hürriyetoglu, S.; Kazgan, H.; Yilmaz, E.S.S.; Yücel, O.; Baser, E. HPV awareness and HPV vaccine acceptance among women who apply to the gynecology outpatient clinics at a tertiary referral hospital in the south Mediterranean region of Turkey. Med. J. Bakirkoy 2016, 12, 136–139. [Google Scholar] [CrossRef]
- Cervantes-Amat, M.; López-Abente, G.; Aragonés, N.; Pollán, M.; Pastor-Barriuso, R.; Pérez-Gómez, B. The end of the decline in cervical cancer mortality in Spain: trends across the period 1981-2012. BMC cancer 2015, 15, 9. [Google Scholar] [CrossRef]
- Mansori, K.; Khazaei, S.; Khosravi Shadmani, F.; Hanis, S.M.; Jenabi, E.; Soheylizad, M.; Sani, M.; Ayubi, E. Global Inequalities in Cervical Cancer Incidence and Mortality. Middle East J. Cancer 2018, 9, 235–242. [Google Scholar]
- Zhang, X.X.; Zeng, Q.L.; Cai, W.W.; Ruan, W.Q. Trends of cervical cancer at global, regional, and national level: data from the Global Burden of Disease study 2019. Bmc Public Health 2021, 21, 10. [Google Scholar] [CrossRef]
- Caron, R.M.; Noel, K.; Reed, R.N.; Sibel, J.; Smith, H.J. Health Promotion, Health Protection, and Disease Prevention: Challenges and Opportunities in a Dynamic Landscape. AJPM Focus 2024, 3, 100167. [Google Scholar] [CrossRef] [PubMed]
- Al-Awadhi, R.; Chehadeh, W.; Jaragh, M.; Al-Shaheen, A.; Sharma, P.; Kapila, K. Distribution of human papillomavirus among women with abnormal cervical cytology in Kuwait. Diagn. Cytopathol. 2013, 41, 107–114. [Google Scholar] [CrossRef]
- Baddal, B.; Oktay, M.N.; Bostanci, A.; Yenen, M.C. Prevalence and genotype screening of human papillomavirus among women attending a private hospital in Northern Cyprus: an 11-year retrospective study. BMC Womens Health 2023, 23, 8. [Google Scholar] [CrossRef] [PubMed]
- Dom-Chima, N.; Ajang, Y.A.; Dom-Chima, C.I.; Biswas-Fiss, E.; Aminu, M.; Biswas, S.B. Human papillomavirus spectrum of HPV-infected women in Nigeria: an analysis by next-generation sequencing and type-specific PCR. Virol. J. 2023, 20, 11. [Google Scholar] [CrossRef]
- Elmi, A.A.; Bansal, D.; Acharya, A.; Skariah, S.; Dargham, S.R.; Abu-Raddad, L.J.; Mohamed-Nady, N.; Amuna, P.; Al-Thani, A.A.J.; Sultan, A.A. Human Papillomavirus (HPV) Infection: Molecular Epidemiology, Genotyping, Seroprevalence and Associated Risk Factors among Arab Women in Qatar. PloS one 2017, 12, 14. [Google Scholar] [CrossRef] [PubMed]
- Ayash, C.; Raad, N.; Finik, J.; Attia, N.; Nourredine, S.; Aragones, A.; Gany, F. Arab American Mothers’ HPV Vaccination Knowledge and Beliefs. J. Community Health 2022, 47, 716–725. [Google Scholar] [CrossRef]
- Finan, R.R.; Chemaitelly, H.; Racoubian, E.; Aimagambetova, G.; Almawi, W.Y. Genetic diversity of human papillomavirus (HPV) as specified by the detection method, gender, and year of sampling: a retrospective cross-sectional study. Arch. Gynecol. Obstet. 2023, 307, 1469–1479. [Google Scholar] [CrossRef]
- Drolet, M.; Laprise, J.-F.; Boily, M.-C.; Franco, E.; Brisson, M. Potential cost-effectiveness of the nonavalent human papillomavirus (HPV) vaccine. International journal of cancer. Journal international du cancer 2014, 134. [Google Scholar] [CrossRef]
- Sanders, G.D.; Taira, A.V. Cost-effectiveness of a potential vaccine for human papillomavirus. Emerg Infect Dis 2003, 9, 37–48. [Google Scholar] [CrossRef]
- Gobbo, E.L.S.; Hanson, C.; Abunnaja, K.S.S.; van Wees, S.H. Do peer-based education interventions effectively improve vaccination acceptance? a systematic review. BMC Public Health 2023, 23, 1354. [Google Scholar] [CrossRef] [PubMed]
- Martínez, A.C.; Balbino, J.E.; Lemgruber, A.; Ruiz, E.M.; Lima, A.O.D.; Mochón, L.G.; Lessa, F. Adoption of the HPV vaccine: a case study of three emerging countries. J. Comp. Eff. Res. 2017, 6, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Bennacef, A.C.; Khodja, A.A.; Abou-Bekr, F.A.; Ndao, T.; Holl, R.; Bencina, G. Costs and Resource Use Among Patients with Cervical Cancer, Cervical Intraepithelial Neoplasia, and Genital Warts in Algeria. J. Health Econ. Outcome. Res. 2022, 9, 31–38. [Google Scholar] [CrossRef]
- Bencina, G.; Ugrekhelidze, D.; Shoel, H.; Oliver, E.; Meiwald, A.; Hughes, R.; Eiden, A.; Weston, G. The indirect costs of vaccine-preventable cancer mortality in the Middle East and North Africa (MENA). J. Med. Econ. 2024, 27, 1036–1045. [Google Scholar] [CrossRef]
- Cheema, S.; Abraham, A.; Maisonneuve, P.; Jithesh, A.; Chaabna, K.; al Janahi, R.; Sarker, S.; Hussain, A.; Rao, S.; Lowenfels, A.B.; et al. HPV infection and vaccination: a cross-sectional study of knowledge, perception, and attitude to vaccine uptake among university students in Qatar. Bmc Public Health 2024, 24, 13. [Google Scholar] [CrossRef]
- Mahmoud, I.; Al Eid, M.M.A.; Mohamed, M.A.; Aladwani, A.J.; El Amin, N. Human papillomavirus vaccination and Pap test uptake, awareness, and barriers among young adults in Gulf Cooperation Council countries: A comparative cross-sectional survey. J. Infect. Public Health 2024, 17, 7. [Google Scholar] [CrossRef] [PubMed]
- Pierz, A.J.; Randall, T.C.; Castle, P.E.; Adedimeji, A.; Ingabire, C.; Kubwimana, G.; Uwinkindi, F.; Hagenimana, M.; Businge, L.; Musabyimana, F.; et al. A scoping review: Facilitators and barriers of cervical cancer screening and early diagnosis of breast cancer in Sub-Saharan African health settings. Gynecol Oncol Rep 2020, 33, 100605. [Google Scholar] [CrossRef]
- Afsah, Y.R.; Kaneko, N. Barriers to cervical cancer screening faced by immigrant Muslim women: a systematic scoping review. BMC Public Health 2023, 23, 2375. [Google Scholar] [CrossRef]
- Kim, J.J.; Sharma, M.; O’Shea, M.; Sweet, S.; Diaz, M.; Sancho-Garnier, H.; Seoud, M. Model-Based Impact and Cost-Effectiveness of Cervical Cancer Prevention in the Extended Middle East and North Africa (EMENA). Vaccine 2013, 31, G65–G77. [Google Scholar] [CrossRef]
- Bhattacharjee, N.V.; Schumacher, A.E.; Aali, A.; Abate, Y.H.; Abbasgholizadeh, R.; Abbasian, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd ElHafeez, S.; Abd-Elsalam, S.; et al. Global fertility in 204 countries and territories, 1950-2021, with forecasts to 2100: a comprehensive demographic analysis for the Global Burden of Disease Study 2021. Lancet 2024, 403, 2057–2099. [Google Scholar] [CrossRef]
- Makhlouf, S.M.; Ahmed, S.; Mulvey, M.; Bennett, M.I. Attitudes, Knowledge, and Perceived Barriers Towards Cancer Pain Management Among Healthcare Professionals in Libya: a National Multicenter Survey. J Cancer Educ 2023, 38, 789–797. [Google Scholar] [CrossRef]
- Soled, D. Language and Cultural Discordance: Barriers to Improved Patient Care and Understanding. J Patient Exp 2020, 7, 830–832. [Google Scholar] [CrossRef]
- Balamou, C.; Rodrigue-Moulinie, C.; Rahmani, S.; de Jesus, M. Optimizing cancer screening rates in populations with low literacy in France: Results of a mixed-methods cancer educational intervention study. Cancer Research, Statistics, and Treatment 2023, 6, 365–375. [Google Scholar] [CrossRef]
- de jesus, M.; Rodrigue, C.; Rahmani, S.; Balamou, C. Addressing Cancer Screening Inequities by Promoting Cancer Prevention Knowledge, Awareness, Self-Efficacy, and Screening Uptake Among Low-Income and Illiterate Immigrant Women in France. Int. J. Public Health 2021, 66. [Google Scholar] [CrossRef]
- Silva, J.; Gama, A.; Fronteira, I.; Marques, P.; Dias, S. Knowledge and attitudes towards cervical cancer and screening among migrant women: a qualitative study in Portugal. BMJ open 2024, 14, e082538. [Google Scholar] [CrossRef]
- Hamdiui, N.; Stein, M.L.; van Steenbergen, J.; Crutzen, R.; Bouman, M.; Khan, A.; Çetin, M.N.; Timen, A.; van den Muijsenbergh, M. Evaluation of a Web-Based Culturally Sensitive Educational Video to Facilitate Informed Cervical Cancer Screening Decisions Among Turkish- and Moroccan-Dutch Women Aged 30 to 60 Years: Randomized Intervention Study. Journal of medical Internet research 2022, 24, e35962. [Google Scholar] [CrossRef] [PubMed]
- Comparetto, C.; Epifani, C.; Manca, M.C.; Lachheb, A.; Bravi, S.; Cipriani, F.; Bellomo, F.; Olivieri, S.; Fiaschi, C.; Marco, L.; et al. Uptake of cervical cancer screening among the migrant population of Prato Province, Italy. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics 2016, 136. [Google Scholar] [CrossRef] [PubMed]
- Travier, N.; Vidal, C.; Garcia, M.; Benito, L.; Medina, P.; Moreno, V. Communication Channels Used by Women to Contact a Population-Based Breast Cancer Screening Program in Catalonia, Spain. J Med Syst 2019, 43, 244. [Google Scholar] [CrossRef] [PubMed]
- Ricardo-Rodrigues, I.; Jiménez-García, R.; Hernández-Barrera, V.; Carrasco-Garrido, P.; Jiménez-Trujillo, I.; López de Andrés, A. Social disparities in access to breast and cervical cancer screening by women living in Spain. Public Health 2015, 129, 881–888. [Google Scholar] [CrossRef]
- Piana, A.; Sotgiu, G.; Castiglia, P.; Pischedda, S.; Cocuzza, C.; Capobianco, G.; Marras, V.; Dessole, S.; Muresu, E. Prevalence and type distribution of human papillomavirus infection in women from North Sardinia, Italy. BMC Public Health 2011, 11, 785. [Google Scholar] [CrossRef]
- Sande, C.M.; Yang, G.; Mohamed, A.; Legendre, B.L.; Pion, D.; Ferro, S.L.; Grimm, K.; Elenitoba-Johnson, K.S.J. High-resolution melting assay for rapid, simultaneous detection of JAK2, MPL and CALR variants. Journal of clinical pathology 2024, 77, 639–644. [Google Scholar] [CrossRef]
- Durand, M.A.; Lamouroux, A.; Redmond, N.M.; Rotily, M.; Bourmaud, A.; Schott, A.M.; Auger-Aubin, I.; Frachon, A.; Exbrayat, C.; Balamou, C.; et al. Impact of a health literacy intervention combining general practitioner training and a consumer facing intervention to improve colorectal cancer screening in underserved areas: protocol for a multicentric cluster randomized controlled trial. BMC Public Health 2021, 21, 1684. [Google Scholar] [CrossRef] [PubMed]
- Kale, S.; Hirani, S.; Vardhan, S.; Mishra, A.; Ghode, D.B.; Prasad, R.; Wanjari, M. Addressing Cancer Disparities Through Community Engagement: Lessons and Best Practices. Cureus 2023, 15, e43445. [Google Scholar] [CrossRef]
- Priaulx, J.; Turnbull, E.; Heijnsdijk, E.; Csanadi, M.; Senore, C.; Koning, H.; McKee, M. The influence of health systems on breast, cervical and colorectal cancer screening: an overview of systematic reviews using health systems and implementation research frameworks. Journal of Health Services Research & Policy 2019, 25, 135581961984231. [Google Scholar] [CrossRef]
- Basha, L.; Ahmed, H.; Hamze, M.; Ali, A.A.; Alahdab, F.; Marzouk, M.; Sullivan, R.; Abbara, A. Cancer and Syria in conflict: a systematic review. BMC cancer 2024, 24, 1537. [Google Scholar] [CrossRef]
- Abdelaziz, M.N.; Hefnawy, A.; Azzam, H.; Reisha, O.; Hamdy, O. Knowledge and attitude among Egyptian medical students regarding the role of human papillomavirus vaccine in prevention of oropharyngeal cancer: a questionnaire-based observational study. Scientific reports 2025, 15, 3767. [Google Scholar] [CrossRef] [PubMed]
- Jaafar, I.; Atallah, D.; Mirza, F.; Abu Musa, A.; El-Kak, F.; Seoud, M. Determinants of Human Papillomavirus Vaccine recommendation among Middle Eastern and Lebanese Healthcare Providers. Clinical Epidemiology and Global Health 2022, 17, 101092. [Google Scholar] [CrossRef]
- Tun, H.M.; Rahman, H.A.; Naing, L.; Malik, O.A. Artificial intelligence utilization in cancer screening program across ASEAN: a scoping review. BMC cancer 2025, 25, 703. [Google Scholar] [CrossRef]
- Eisemann, N.; Bunk, S.; Mukama, T.; Baltus, H.; Elsner, S.A.; Gomille, T.; Hecht, G.; Heywang-Köbrunner, S.; Rathmann, R.; Siegmann-Luz, K.; et al. Nationwide real-world implementation of AI for cancer detection in population-based mammography screening. Nature medicine 2025, 31, 917–924. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.R.; Egemen, D.; Befano, B.; Rodriguez, A.C.; Jeronimo, J.; Desai, K.; Teran, C.; Alfaro, K.; Fokom-Domgue, J.; Charoenkwan, K.; et al. Assessing generalizability of an AI-based visual test for cervical cancer screening. PLOS Digital Health 2024, 3, e0000364. [Google Scholar] [CrossRef] [PubMed]
- Adapa, K.; Gupta, A.; Singh, S.; Kaur, H.; Trikha, A.; Sharma, A.; Rahul, K. A real world evaluation of an innovative artificial intelligence tool for population-level breast cancer screening. NPJ digital medicine 2025, 8, 2. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



