Submitted:
06 November 2025
Posted:
07 November 2025
You are already at the latest version
Abstract
Background/Objectives: Acute heart failure (AHF) is a heterogeneous clinical syndrome, and prognosis varies depending on the ejection fraction phenotype. Although the N-terminal pro–B-type natriuretic peptide (NT-proBNP) remains the benchmark biomarker, conventional echocardiographic measures such as the tricuspid annular plane systolic excursion (TAPSE), the right ventricular to right atrial pressure gradient (RV–RA gradient), and the left ventricular outflow tract velocity–time integral (LVOT VTI) provide only partial prognostic information.We previously proposed the Virtue Index, defined as the ratio between the RV–RA gradient and the product of TAPSE and LVOT VTI, reflecting the interaction between right and left ventricular performance. The present study aimed to assess the clinical and prognostic behavior of the index in a cohort of patients with AHF and to determine whether its performance differs between reduced and preserved ejection fraction phenotypes. Methods: We retrospectively analyzed 222 patients admitted with a diagnosis of AHF. Complete echocardiographic data for Virtue Index calculation were available in 168 patients (99 [59%] with heart failure with reduced ejection fraction [HFrEF] and 69 [41%] with heart failure with preserved ejection fraction [HFpEF]). Patients with mid-range ejection fraction (40–49%) or incomplete echocardiographic parameters were excluded from subgroup analyses but retained for descriptive statistics where applicable. Correlation with NT-proBNP was evaluated using Spearman rank testing with bootstrap confidence intervals. Prognostic performance for in-hospital mortality was analyzed using ROC curves, area under the curve (AUC) with bootstrap intervals, and pairwise DeLong comparisons. Results: In the HFpEF subgroup, the index correlated moderately with NT-proBNP (ρ = 0.38, 95% CI 0.13–0.58, p = 0.002) and demonstrated fair prognostic discrimination (AUC 0.704, 95% CI 0.53–0.85), comparable to the RV–RA gradient (AUC 0.724) and higher than TAPSE (AUC 0.637) or LVOT VTI (AUC 0.669). In contrast, in HFrEF, the index showed a weak, non-significant correlation with NT-proBNP (ρ = 0.19, p = 0.06) and modest predictive accuracy (AUC 0.584, 95% CI 0.36–0.79), while LVOT VTI achieved the best discrimination (AUC 0.700). NT-proBNP remained superior in both subgroups (AUC 0.744 in HFrEF, 0.838 in HFpEF). Conclusions: The Virtue Index reflects integrated haemodynamic function and may demonstrate a phenotype-dependent prognostic role in AHF. In our study, its value was more evident in HFpEF, whereas in HFrEF traditional parameters, especially LVOT VTI, remained stronger predictors. Although NT-proBNP consistently outperformed Virtue, the index may complement biomarker assessment by providing rapid, bedside risk stratification of short-term mortality.
Keywords:
acute heart failure
; echocardiography
; prognosis
; Virtue Index
; NT-proBNP
; ventricular coupling
1. Introduction
Acute heart failure (AHF) remains one of the most common cardiovascular emergencies, responsible for millions of hospital admissions each year and associated with high short-term mortality and rehospitalization rates [1,2]. The underlying mechanisms leading to this unfavorable outcome are complex, involving abrupt shifts in preload and afterload, neurohormonal activation, and variable contributions from both ventricles [3,4]. Importantly, prognosis is not uniform across phenotypes: patients with HFrEF differ in clinical course and outcomes from those with HFpEF [5,6].
Early risk stratification is essential to guide management decisions but remains challenging in routine practice. Clinical assessment alone has limited prognostic accuracy [7], and although biomarkers such as NT-proBNP are powerful diagnostic and prognostic tools [8,9,10], their availability may be delayed or restricted in some clinical contexts. Echocardiography provides immediate, bedside information and is central to the evaluation of both left and right ventricular function [11,12]. In routine clinical practice, echocardiographic evaluation in acute settings primarily focuses on left ventricular function, while right ventricular assessment may be more challenging and, at times, overlooked due to technical or time constraints. However, right ventricular performance plays a crucial role in determining outcomes in AHF. This rationale supports the development of a simple, rapid, and feasible index capable of simultaneously evaluating both ventricles at the bedside.
Several echocardiographic parameters have been linked to outcomes in AHF. The left ventricular outflow tract velocity–time integral (LVOT VTI), reflecting forward stroke volume, has shown prognostic relevance in both chronic and acute settings [13,14]. On the right side, tricuspid annular plane systolic excursion (TAPSE) and the tricuspid regurgitation–derived pressure gradient are established indices of right ventricular systolic performance and pulmonary pressures [15,16,17,18]. However, each parameter reflects only a limited dimension of cardiac function. Emerging evidence highlights the importance of ventricular interdependence, whereby right- and left-sided haemodynamics are dynamically coupled, influencing both symptoms and outcomes [19].
To capture this interaction, we proposed a new tool - the Virtue index ,defined as the ratio of the right ventricular to right atrial pressure gradient (RV–RA gradient) to the product of TAPSE and LVOT VTI [20]. Early findings suggested that this composite measure may offer incremental prognostic information by integrating right ventricle (RV) load, longitudinal systolic function, and left ventricle (LV) forward flow. Nonetheless, validation remains limited, and it is not clear whether its prognostic value is consistent across phenotypes defined by ejection fraction.
2. Materials and Methods
2.1. Study Design and Patient Population
We conducted a retrospective analysis including patients admitted with AHF between January 2024 and June 2025 at St. Pantelimon Clinical Emergency Hospital in Bucharest, Romania. The diagnosis of AHF was established in accordance with the 2021 European Society of Cardiology (ESC) Guidelines for the management of acute and chronic heart failure [21]. Patients with missing echocardiographic parameters necessary for the calculation of the Virtue Index were excluded from the analysis. The final study cohort consisted of 222 patients, among whom 99 presented with reduced ejection fraction (HFrEF, <40%) and 69 with preserved ejection fraction (HFpEF, ≥50%), whereas individuals with mid-range ejection fraction values (40–49%) were not included.
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Emergency Clinical Hospital “Sf. Pantelimon”, Bucharest (Approval No. 77 / 09.09.2024).
The flow of patient selection is illustrated in Figure 1.
2.2. Echocardiographic Assessment
Comprehensive transthoracic echocardiography was performed within the first hours after hospital admission, following standard acquisition protocols and current recommendations for chamber quantification [22] and diastolic function assessment [23]. All echocardiographic examinations were performed by experienced cardiologists certified in echocardiography, using the same General Electric Vivid E95 ultrasound system. The following parameters were assessed: left ventricular ejection fraction (LVEF) by Simpson’s biplane method, tricuspid annular plane systolic excursion (TAPSE) measured in the apical four-chamber view using M-mode [24], left ventricular outflow tract velocity–time integral (LVOT VTI) obtained by pulsed-wave Doppler in the apical five-chamber view [13,14], and the right ventricular-to-right atrial systolic pressure gradient (RV–RA gradient) derived from the peak velocity of tricuspid regurgitation using the modified Bernoulli equation [24].
The Virtue Index was calculated as:
This index was previously proposed as an integrative marker reflecting the interaction between right ventricular systolic load, longitudinal contractile function, and left ventricular forward flow [20]. In the present study, the same formula was applied to all patients to explore its prognostic significance across different ejection fraction phenotypes.
2.3. Biomarker Measurement
Blood samples were obtained at admission, prior to initiation of intravenous therapy. Plasma NT-proBNP concentrations were measured using an electrochemiluminescent immunoassay (Elecsys® proBNP II, Roche Diagnostics, Mannheim, Germany) according to the manufacturer’s instructions. Results were expressed in pg/mL. NT-proBNP was selected as a comparator biomarker due to its well-established diagnostic and prognostic significance in AHF, as demonstrated in several pivotal studies [25,26,27].
2.4. Outcomes
The primary objective of the study was to evaluate the prognostic performance of the Virtue Index for in-hospital all-cause mortality.
Secondary analyses included assessment of the relationship between the Virtue Index and NT-proBNP at admission and comparison of its discriminative ability with conventional echocardiographic parameters (TAPSE, RV–RA gradient , and LVOT VTI.
2.5. Statistical Analysis
Continuous variables were expressed as mean ± standard deviation or median (interquartile range), as appropriate. Comparisons between groups used the Student t-test for normally distributed data [28] or the Mann–Whitney U test for non-normally distributed variables [29]. Categorical variables were compared with the χ² test.
Associations between the Virtue Index and NT-proBNP were evaluated using Spearman’s rank correlation coefficient, with 1,000 bootstrap replicates to obtain 95% confidence intervals. Prognostic performance for in-hospital mortality was assessed with receiver operating characteristic (ROC) analysis and area under the curve (AUC), with bootstrap confidence intervals. Pairwise comparisons of AUC values were performed using DeLong’s test for correlated ROC curves [30].
All statistical tests were two-tailed, and a p-value <0.05 was considered significant. Analyses were performed using R (version 4.3.2) and Python (version 3.10).
Generative artificial intelligence tools (ChatGPT, OpenAI, San Francisco, CA, USA) were used for figure generation and minor linguistic adjustments to improve text clarity and readability.
3. Results
3.1. Baseline Characteristics
Baseline demographic, clinical, and laboratory characteristics were compared between patients with reduced (HFrEF) and preserved ejection fraction (HFpEF). Detailed results are presented in Table 1.
Patients with HFpEF were significantly older than those with HFrEF (77.6 ± 9.6 vs. 65.9 ± 14.9 years, p < 0.001) and were more frequently female (72.5% vs. 33.3%, p < 0.001). Smoking was considerably less common in the HFpEF group (8.7% vs. 36.4%, p < 0.001). Hypertension was more prevalent in HFpEF (95.7% vs. 82.8%, p = 0.017), while dyslipidaemia showed a similar prevalence across groups (94.2% vs. 94.9%, p = 0.83). Obesity (24.6% vs. 30.3%, p = 0.46) and diabetes mellitus (37.7% vs. 41.4%, p = 0.63) did not differ significantly between groups. Valvular heart disease was slightly more common in HFrEF (80.8% vs. 73.9%, p = 0.29).
Hemodynamic parameters were broadly comparable, with no significant difference in systolic blood pressure (143 ± 31 in HFrEF vs. 142 ± 31 mmHg in HFpEF, p = 0.83), while diastolic pressure was slightly higher in HFrEF (87 ± 17 vs. 81 ± 17 mmHg, p = 0.02). Median NT-proBNP levels were numerically higher in HFrEF (8453 [4957–21121] pg/mL) than in HFpEF (6537 [2180–24554] pg/mL), though the difference was not statistically significant (p = 0.41).
Echocardiographic findings were consistent with the expected phenotypic pattern. TAPSE values were similar between groups (20 ± 10 mm vs. 21 ± 7 mm, p = 0.41), whereas LVOT VTI was markedly lower in HFrEF (14 ± 4 cm vs. 21 ± 7 cm, p < 0.001). As anticipated, LVEF differed profoundly (28 ± 7% vs. 60 ± 7%, p < 0.001). The RV–RA gradient was significantly higher in HFpEF (21 [17–24] mmHg) compared with HFrEF (17 [14–22] mmHg, p < 0.001), reflecting greater pulmonary pressure load.
The Virtue Index, reflecting the integrated right–left ventricular interaction, was significantly higher in HFrEF than in HFpEF [0.135 (0.069–0.215) vs. 0.075 (0.049–0.110), p < 0.001], consistent with the more pronounced systolic impairment characterising the reduced-EF phenotype.
3.2. Prognostic Discrimination for In-Hospital Mortality (ROC/AUC Analyses)
We next evaluated the discriminative ability of the Virtue Index and conventional echocardiographic parameters: RV–RA gradient, TAPSE, and LVOT VTI—for in-hospital mortality.
In the HFrEF subgroup (N = 99, 9 (9%) deaths), Virtue showed modest discrimination (AUC 0.584, 95% CI 0.36–0.79), similar to RV–RA gradient (0.532, 95% CI 0.46–0.72) and TAPSE (0.583, 95% CI 0.45–0.77). LVOT VTI performed best in this group (AUC 0.700, 95% CI 0.53–0.85).
In the HFpEF subgroup (N = 69, 8 (11.6%) deaths), Virtue achieved good discrimination (AUC 0.704, 95% CI 0.53–0.85), comparable to RV–RA gradient (0.724, 95% CI 0.54–0.90) and higher than TAPSE (0.637, 95% CI 0.45–0.89) and LVOT VTI (0.669, 95% CI 0.45–0.86).
Numerical results are shown in Table 2, while Figure 2 and Figure 3 provide graphical representations of the AUC values and ROC curves for each subgroup.
Interpretation
In the HFrEF subgroup, the Virtue Index demonstrated only modest discrimination for in-hospital mortality (AUC 0.584), similar to TAPSE and RV–RA gradient—parameters traditionally recognised as limited short-term prognostic markers in advanced systolic heart failure. LVOT VTI showed the highest predictive accuracy (AUC 0.700), underscoring the dominant role of left ventricular stroke volume and forward flow in determining outcomes when systolic function is severely reduced. Thus, in patients with reduced EF, Virtue does not appear to provide additional prognostic information beyond established systolic indices.
Conversely, in the HFpEF subgroup, Virtue achieved good discrimination (AUC 0.704), comparable to RV–RA gradient (AUC 0.724) and clearly outperforming TAPSE and LVOT VTI. Its significant correlation with NT-proBNP supports its physiological relevance as an integrative marker of right–left ventricular interaction and filling pressures. In this context, where conventional systolic indices often fail to predict outcomes, composite measures such as Virtue may more accurately capture the haemodynamic determinants of prognosis.
Overall, the prognostic performance of Virtue appears phenotype-dependent—limited in HFrEF, where LV forward flow remains the main determinant of short-term outcomes, but more informative in HFpEF, reflecting the interplay between right-sided pressures, longitudinal function, and LV outflow.
3.3. Correlation Between Virtue Index and NT-proBNP
In subgroup analyses, the Virtue Index demonstrated distinct patterns of correlation with NT-proBNP levels at admission.
In the HFrEF subgroup, the correlation was weak and not statistically significant (ρ = 0.191, 95% CI −0.006–0.39, p = 0.06; N = 96 pairs). This suggests that in patients with reduced ejection fraction, where neurohormonal activation and structural remodeling are typically advanced, Virtue may add limited prognostic information beyond NT-proBNP.
In contrast, in the HFpEF subgroup, Virtue showed a moderate and statistically significant correlation (ρ = 0.380, 95% CI 0.13–0.58, p = 0.002; N = 66 pairs). This supports the biological plausibility of Virtue as an integrated marker of congestion and ventricular interaction in patients with preserved systolic function, where conventional indices often fail to capture relevant prognostic information.
These results are summarized in Table 3. Taken together, they indicate that the relationship between Virtue and NT-proBNP may be phenotype-dependent: weak in reduced EF, but stronger and clinically relevant in preserved EF, supporting its potential role as an integrated haemodynamic marker in HFpEF.
3.4. Pairwise AUC Comparisons Between Virtue and Conventional Parameters
The discriminative ability of Virtue was directly compared with RV–RA gradient, TAPSE, and LVOT VTI using pairwise AUC differences (Hanley–McNeil approximation of the DeLong test).The results are summarized in Table 4.
In the HFrEF subgroup (n = 99, 9 deaths – 9.1%), Virtue demonstrated marginally higher AUCs than the RV–RA gradient (ΔAUC = +0.052, Z = 0.407, p = 0.684) and TAPSE (ΔAUC = +0.001, Z = 0.008, p = 0.994), but performed slightly worse than LVOT VTI (ΔAUC = −0.116, Z = −0.894, p = 0.372). None of these differences reached statistical significance.
In the HFpEF subgroup (n = 69, 8 deaths – 11.6%), Virtue showed comparable discrimination to the RV–RA gradient (ΔAUC = −0.020, Z = −0.186, p = 0.852) and modestly higher AUCs than TAPSE (ΔAUC = +0.067, Z = 0.504, p = 0.614) and LVOT VTI (ΔAUC = +0.035, Z = 0.277, p = 0.782). Again, none of these pairwise comparisons were statistically significant.
Interpretation
In HFrEF, the Virtue Index performed similarly to RV–RA gradient and TAPSE, while LVOT VTI remained the most discriminative parameter, consistent with its established role as a marker of forward stroke volume and systolic output.
In HFpEF, Virtue exhibited comparable or slightly superior discrimination relative to conventional indices. Although these differences were not statistically significant, the index appears to integrate aspects of ventricular coupling and congestion more effectively in this phenotype.
Overall, in our study cohort, Virtue demonstrated non-inferior prognostic accuracy compared to traditional echocardiographic measures in both subgroups, with a subtle tendency toward better alignment with congestion markers in HFpEF
3.5. Comparative Prognostic Performance of Virtue and NT-proBNP
We further compared the discriminative performance of the Virtue Index with NT-proBNP at admission.
In HFrEF (N = 99, 9 deaths -9,1%), Virtue achieved AUC 0.583, while NT-proBNP reached 0.744, confirming the superior prognostic accuracy of the biomarker in systolic dysfunction.
In HFpEF (N = 69, 8 deaths – 11,6%) Virtue reached AUC 0.705, whereas NT-proBNP achieved 0.838, again outperforming the echocardiographic index in short-term mortality prediction.
Numerical results are summarized in Table 5, and graphical representations of the ROC curves are shown in Figure 4 and Figure 5.
Interpretation
Across both subgroups, NT-proBNP generally provided superior prognostic discrimination compared with the Virtue Index. In HFrEF, NT-proBNP showed substantially better performance (AUC 0.744 vs. 0.583, p = 0.04), underscoring its established role as a powerful marker of neurohormonal activation and decompensation in systolic heart failure. In HFpEF, Virtue achieved reasonable discrimination (AUC 0.705), although NT-proBNP remained superior (AUC 0.838, p = 0.05).
These findings suggest that while Virtue captures relevant haemodynamic information, NT-proBNP retains higher accuracy as a standalone prognostic marker in both phenotypes. Importantly, the comparable performance of Virtue in HFpEF supports its potential complementary role, particularly when echocardiography provides immediate bedside insights and NT-proBNP results may be delayed or unavailable.
4. Discussion
In the present study, we aimed to validate the Virtue Index in a cohort of patients admitted with acute heart failure (AHF) and to assess its prognostic significance across phenotypes defined by left ventricular ejection fraction (LVEF). Our findings indicate that the Virtue Index retains prognostic value, although its performance varies with phenotype. Specifically, it provided stronger discrimination and closer alignment with NT-proBNP in HFpEF, whereas its contribution was more modest in HFrEF, where parameters of forward flow dominated outcome prediction. These results extend previous observations and emphasise the importance of integrating ventricular mechanics and congestion profiles when interpreting echocardiographic prognostic markers [32,33,34].
The heterogeneity of AHF continues to complicate risk assessment and management. While systolic dysfunction and reduced cardiac output characterise HFrEF, diastolic stiffness, abnormal relaxation, and ventriculo-arterial uncoupling define HFpEF [32,35]. These distinct mechanisms influence not only congestion patterns and filling pressures but also the prognostic interpretation of imaging and biomarker parameters. The Virtue Index—combining tricuspid regurgitation gradient with TAPSE and LVOT VTI—was conceived to capture this complex interaction between right- and left-sided function. By linking pulmonary pressure load to longitudinal contractility and stroke volume, it integrates the efficiency of biventricular coupling and the haemodynamic cost of maintaining cardiac output [13,18,36].
The clinical profile of our cohort illustrates the contrasting characteristics of heart failure phenotypes [32,35]. Patients with HFpEF were typically older, more often women, and had a greater prevalence of atrial fibrillation, hypertension, and renal dysfunction compared with those with reduced ejection fraction [32,33,34]. Despite preserved systolic function, these patients experienced higher in-hospital mortality. The combination of advanced age, multiple comorbidities, and impaired diastolic reserve likely creates a fragile physiological balance that is easily disrupted during acute decompensation [33,35]. Increased vascular stiffness, endothelial dysfunction, and altered ventricular–vascular coupling further limit cardiac adaptability to volume and pressure overload, resulting in greater vulnerability to congestion and instability [33,37].
The frequent coexistence of atrial fibrillation in HFpEF adds to this complexity by reducing atrial contribution to ventricular filling and increasing pulmonary pressures [34,37]. When combined with hypertension, renal impairment, and age-related vascular changes, these factors delineate a high-risk profile that explains the observed trend toward greater in-hospital mortality in HFpEF despite preserved systolic performance [32,33,34,35,36,37].
Within this context, the interaction between right and left ventricular function appears particularly relevant in HFpEF. In this subgroup, the Virtue Index correlated significantly with NT-proBNP and achieved comparable prognostic performance to the RV–RA gradient, outperforming TAPSE and LVOT VTI. These findings are consistent with reports highlighting the central role of ventricular interdependence and pulmonary pressure adaptation in preserved-EF syndromes [33,37]. In HFpEF, even small increases in left ventricular filling pressure can lead to disproportionate rises in pulmonary artery pressure and early right ventricular dysfunction [34,37]. Consequently, both Virtue and NT-proBNP may reflect overlapping pathophysiological domains—specifically diastolic load, wall stress, and venous congestion—rather than isolated contractile impairment. This alignment supports Virtue as a feasible echocardiographic surrogate for congestion in settings where biomarker testing is delayed or unavailable [20,38].
In contrast, Virtue showed limited predictive ability in HFrEF, where LVOT VTI emerged as the most powerful echocardiographic predictor. This observation aligns with the established pathophysiology of systolic heart failure, in which stroke volume and forward output remain the principal determinants of short-term outcomes [11,12,22]. As systolic dysfunction advances, the variability of TAPSE and tricuspid gradients narrows, diminishing the discriminative capacity of composite coupling indices. Similar attenuation has been reported for other metrics such as cardiac power output and RV/LV interaction ratios, whose incremental prognostic value declines once left ventricular contractility becomes severely impaired [36,39].
As expected, NT-proBNP outperformed all echocardiographic indices in both phenotypes. Nevertheless, Virtue offers a distinct practical advantage—it can be derived instantly at the bedside, providing an immediate imaging-based estimate of haemodynamic burden. This may be particularly valuable in acute presentations, where rapid clinical decisions precede laboratory confirmation. In HFpEF, where diagnostic uncertainty is frequent and conventional systolic indices are often preserved, early incorporation of Virtue into echocardiographic evaluation could refine prognostic assessment and support therapeutic prioritisation [35,40].
Methodologically, this study expands on the initial validation of Virtue [20] by analysing a larger, more heterogeneous population and incorporating phenotype-specific assessment with bootstrap-derived confidence intervals. The absence of significant differences in DeLong testing likely reflects the limited number of events; nevertheless, the consistent direction of results across parameters supports the comparable performance of Virtue to established echocardiographic predictors derived from routine measurements.
Several limitations should be acknowledged. The retrospective, single-centre design may introduce selection bias, and the relatively small number of in-hospital deaths per subgroup limits the power for extensive multivariable modelling. NT-proBNP values were measured only at admission, precluding assessment of dynamic changes. Prospective multicentre validation with longitudinal follow-up is warranted to confirm these findings and to determine whether serial Virtue measurements can track therapeutic response or predict post-discharge outcomes.
Despite these limitations, the present analysis provides new insight into phenotype-specific prognostication in AHF. Virtue appears to capture the integrated haemodynamic burden that drives outcomes in HFpEF, whereas in HFrEF its prognostic value is overshadowed by global systolic failure. This phenotype-dependent pattern supports a combined approach to risk stratification—one that integrates biomarkers and echocardiographic indices rather than considering them competing tools. Future research should explore whether combining Virtue with NT-proBNP or other congestion markers could enhance real-time risk assessment and optimise bedside decision-making in acute heart failure [35,37,38,39,40].
5. Conclusions
Our findings indicate that the Virtue Index, a simple, integrative, echocardiographic marker reflecting the interaction between the right and left ventricles, could offer additional prognostic insight in AHF. Its performance appears to vary according to the type of dysfunction. In patients with HFpEF, the index showed a closer link with NT-proBNP levels and a better ability to identify patients at higher short-term risk, likely mirroring the combined effects of congestion and impaired ventricular coupling [20,32,34,37]. In contrast, among those with HFrEF, where global systolic failure predominates, its contribution to prognosis was more limited, and measures of forward flow such as LVOT VTI remained stronger predictors [11,12,22].
Overall, the results suggest that the Virtue Index may enhance rather than replace established tools, providing an immediate, noninvasive view of haemodynamic burden at the bedside. Still, as this was a retrospective single-center study with a moderate sample size, the observations should be interpreted cautiously. Larger, prospective studies are needed to confirm these findings and to clarify whether changes in the Virtue Index over time could help guide therapy and refine prognosis in AHF [20,36,40].
Abbreviations
The following abbreviations are used in this manuscript:
| AUC | Area Under the Curve |
| AHF | Acute Heart Failure |
| BP | Blood Pressure |
| CAD | Coronary Artery Disease |
| CI | Confidence Interval |
| EF | Ejection Fraction |
| ESC | European Society of Cardiology |
| eGFR | Estimated Glomerular Filtration Rate |
| HFpEF | Heart Failure with Preserved Ejection Fraction |
| HFrEF | Heart Failure with Reduced Ejection Fraction |
| IQR | Interquartile Range |
| LV | Left Ventricle |
| LVEF | Left Ventricular Ejection Fraction |
| LVOT VTI | Left Ventricular Outflow Tract Velocity Time Integral |
| NT-proBNP | N-terminal pro B-type Natriuretic Peptide |
| ROC | Receiver Operating Characteristic |
| RV | Right Ventricle |
| RV- RA gradient | Right Ventricular to Right Atrial Pressure Gradient |
| SD | Standard Deviation |
| TAPSE | Tricuspid Annular Plane Systolic Excursion |
References
- Ambrosy AP, Fonarow GC, Butler J, Chioncel O, Greene SJ, Vaduganathan M, et al. The global health and economic burden of hospitalizations for heart failure: lessons learned from hospitalized heart failure registries. J Am Coll Cardiol. 2014;63(12):1123–33. [CrossRef]
- Chioncel O, Mebazaa A, Harjola VP, Coats AJ, Piepoli MF, Crespo-Leiro MG, et al.; ESC Heart Failure Long-Term Registry Investigators. Clinical phenotypes and outcome of patients hospitalized for acute heart failure: the ESC Heart Failure Long-Term Registry. Eur J Heart Fail. 2017;19(10):1242–54. [CrossRef]
- Gandhi SK, Powers JC, Nomeir AM, Fowle K, Kitzman DW, Rankin KM, et al. The pathogenesis of acute pulmonary edema associated with hypertension. N Engl J Med. 2001;344(1):17–22.
- Gheorghiade M, De Luca L, Fonarow GC, Filippatos G, Metra M, Francis GS. Pathophysiologic targets in the early phase of acute heart failure syndromes. Am J Cardiol. 2005;96(6A):11G–17G. [CrossRef]
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2016;37(27):2129–200. [CrossRef]
- Shah SJ, Katz DH, Deo RC. Phenotypic spectrum of heart failure with preserved ejection fraction. Heart Fail Clin. 2014;10(3):407–18. [CrossRef]
- Passantino A, Scrutinio D. Risk stratification in acute heart failure: we need a new agenda for clinical research. Int J Cardiol. 2019;293:179–80. [CrossRef]
- McCullough PA, Nowak RM, McCord J, Hollander JE, Herrmann HC, Steg PG, et al. B-type natriuretic peptide and clinical judgment in emergency diagnosis of heart failure: analysis from the Breathing Not Properly Multinational Study. Circulation. 2002;106(4):416–22. [CrossRef]
- Maisel AS, Krishnaswamy P, Nowak RM, McCord J, Hollander JE, Duc P, et al.; Breathing Not Properly Multinational Study Investigators. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med. 2002;347(3):161–7. [CrossRef]
- Januzzi JL Jr, Camargo CA, Anwaruddin S, Baggish AL, Chen AA, Krauser DG, et al. The N-terminal Pro-BNP investigation of dyspnea in the emergency department (PRIDE) study. Am J Cardiol. 2005;95(8):948–54. [CrossRef]
- Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, et al. Guidelines for the echocardiographic assessment of the right heart in adults. J Am Soc Echocardiogr. 2010;23(7):685–713. [CrossRef]
- Obokata M, Reddy YNV, Borlaug BA. The role of echocardiography in heart failure with preserved ejection fraction: what do we want from imaging? Heart Fail Clin. 2019;15(2):241–56. [CrossRef]
- Dini FL, Barletta V, Ballo P, Cioffi G, Pugliese NR, Rossi A, et al. Left ventricular outflow indices in chronic systolic heart failure: thresholds and prognostic value. Echocardiography. 2025;42(2):e70109. [CrossRef]
- Omote K, Nagai T, Iwano H, Tsujinaga S, Kamiya K, Aikawa T, et al. Left ventricular outflow tract velocity time integral in hospitalized heart failure with preserved ejection fraction. ESC Heart Fail. 2020;7(1):167–75. [CrossRef]
- Haddad F, Doyle R, Murphy DJ, Hunt SA. Right ventricular function in cardiovascular disease, part II: pathophysiology, clinical importance, and management of right ventricular failure. Circulation. 2008;117(13):1717–31. [CrossRef]
- Guazzi M, Naeije R, Arena R, Corrà U, Ghio S, Forfia P, et al. Echocardiography of right ventriculoarterial coupling combined with cardiopulmonary exercise testing to predict outcome in heart failure. Chest. 2015;148(1):226–34. [CrossRef]
- Grapsa J, Dawson D, Nihoyannopoulos P. Assessment of right ventricular structure and function in pulmonary hypertension. J Cardiovasc Ultrasound. 2011;19(3):115–25. [CrossRef]
- Wu VC, Takeuchi M. Echocardiographic assessment of right ventricular systolic function. Cardiovasc Diagn Ther. 2018;8(1):70–9. [CrossRef]
- Brener MI, Kanwar MK, Lander MM, Hamid NB, Raina A, Sethi SS, et al. Impact of interventricular interaction on ventricular function: insights from right ventricular pressure–volume analysis. JACC Heart Fail. 2024;12(7):1179–92. [CrossRef]
- Popescu DC, Ciobanu M, Țînț D, Nechita AC. Linking heart function to prognosis: the role of a novel echocardiographic index and NT-proBNP in acute heart failure. Medicina (Kaunas). 2025;61:1412.
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–726. [CrossRef]
- Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults. Eur Heart J Cardiovasc Imaging. 2015;16(3):233–70. [CrossRef]
- Nagueh SF, Smiseth OA, Appleton CP, Byrd BF 3rd, Dokainish H, Edvardsen T, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J Am Soc Echocardiogr. 2016;29(4):277–314. [CrossRef]
- Badano LP, Addetia K, Pontone G, Torlasco C, Lang RM, Parati G, et al. Advanced imaging of right ventricular anatomy and function. Heart. 2020;106(19):1469–76. [CrossRef]
- Pandit K, Mukhopadhyay P, Ghosh S, Chowdhury S. Natriuretic peptides: diagnostic and therapeutic use. Indian J Endocrinol Metab. 2011;15(Suppl 4):S345–53. [CrossRef]
- Tsutsui H, Albert NM, Coats AJS, Anker SD, Bayes-Genis A, Butler J, et al. Natriuretic peptides: role in the diagnosis and management of heart failure. Eur J Heart Fail. 2023;25(5):616–31. [CrossRef]
- Wettersten, N. Biomarkers in acute heart failure: diagnosis, prognosis, and treatment. Int J Heart Fail. 2021;3(2):81–105. [CrossRef]
- Kim, TK. T test as a parametric statistic. Korean J Anesthesiol. 2015;68(6):540–6. [CrossRef]
- Nachar, N. The Mann–Whitney U: a test for assessing whether two independent samples come from the same distribution. Quant Methods Psychol. 2008;4(1):13–20. [CrossRef]
- McDonald, JH. Handbook of Biological Statistics. 3rd ed. Baltimore: Sparky House Publishing; 2014.
- World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–4. [CrossRef]
- Palazzuoli A, Cartocci A, Pirrotta F, Vannuccini F, Campora A, Martini L, et al. Different right ventricular dysfunction and pulmonary coupling in acute heart failure according to left ventricular ejection fraction. Prog Cardiovasc Dis. 2023;81:89–97. [CrossRef]
- Huttin O, Fraser AG, Lund LH, Donal E, Linde C, Kobayashi M, et al.; MEDIA and KaRen investigators. Risk stratification with echocardiographic biomarkers in heart failure with preserved ejection fraction: the MEDIA Echo Score. ESC Heart Fail. 2021;8(3):1827–39. [CrossRef]
- Melenovsky V, Hwang SJ, Lin G, Redfield MM, Borlaug BA. Right heart dysfunction in heart failure with preserved ejection fraction. Eur Heart J. 2014;35(48):3452–62. [CrossRef]
- Tschöpe C, Birner C, Böhm M, Bruder O, Frantz S, Luchner A, et al. Heart failure with preserved ejection fraction: current management and future strategies. Clin Res Cardiol. 2018;107(1):1–19. [CrossRef]
- Wang J, Li X, Jiang J, Luo Z, Tan X, Ren R, et al. Right ventricular–pulmonary arterial coupling and outcome in heart failure with preserved ejection fraction. Clin Cardiol. 2024;47(7):e24308. [CrossRef]
- Tabima DM, Philip JL, Chesler NC. Right ventricular–pulmonary vascular interactions. Physiology (Bethesda). 2017;32(5):346–56. [CrossRef]
- Núñez J, de la Espriella R, Rossignol P, Voors AA, Mullens W, Metra M, et al. Congestion in heart failure: a circulating biomarker-based perspective. Eur J Heart Fail. 2022;24(10):1751–66. [CrossRef]
- Guazzi M, Villani S, Generati G, Bandera F, et al. Right ventricular contractile reserve and pulmonary circulation uncoupling during exercise challenge in heart failure: pathophysiology and clinical phenotypes. JACC Heart Fail. 2016;4(8):625–35. [CrossRef]
- Troughton RW, Richards AM. B-type natriuretic peptides and echocardiographic measures of cardiac structure and function. JACC Cardiovasc Imaging. 2009;2(2):216–25. [CrossRef]
Figure 1.
Flow diagram illustrating patient selection and subgroup allocation; Abbreviations: LVEF - left ventricular ejection fraction; HFrEF – heart failure with reduced ejection fraction; HFpEF – heart failure with preserved ejection fraction; TAPSE – tricuspid annular plane systolic excursion; LVOT VTI – left ventricular outflow tract velocity–time integral; TR - tricuspid regurgitation.
Figure 1.
Flow diagram illustrating patient selection and subgroup allocation; Abbreviations: LVEF - left ventricular ejection fraction; HFrEF – heart failure with reduced ejection fraction; HFpEF – heart failure with preserved ejection fraction; TAPSE – tricuspid annular plane systolic excursion; LVOT VTI – left ventricular outflow tract velocity–time integral; TR - tricuspid regurgitation.
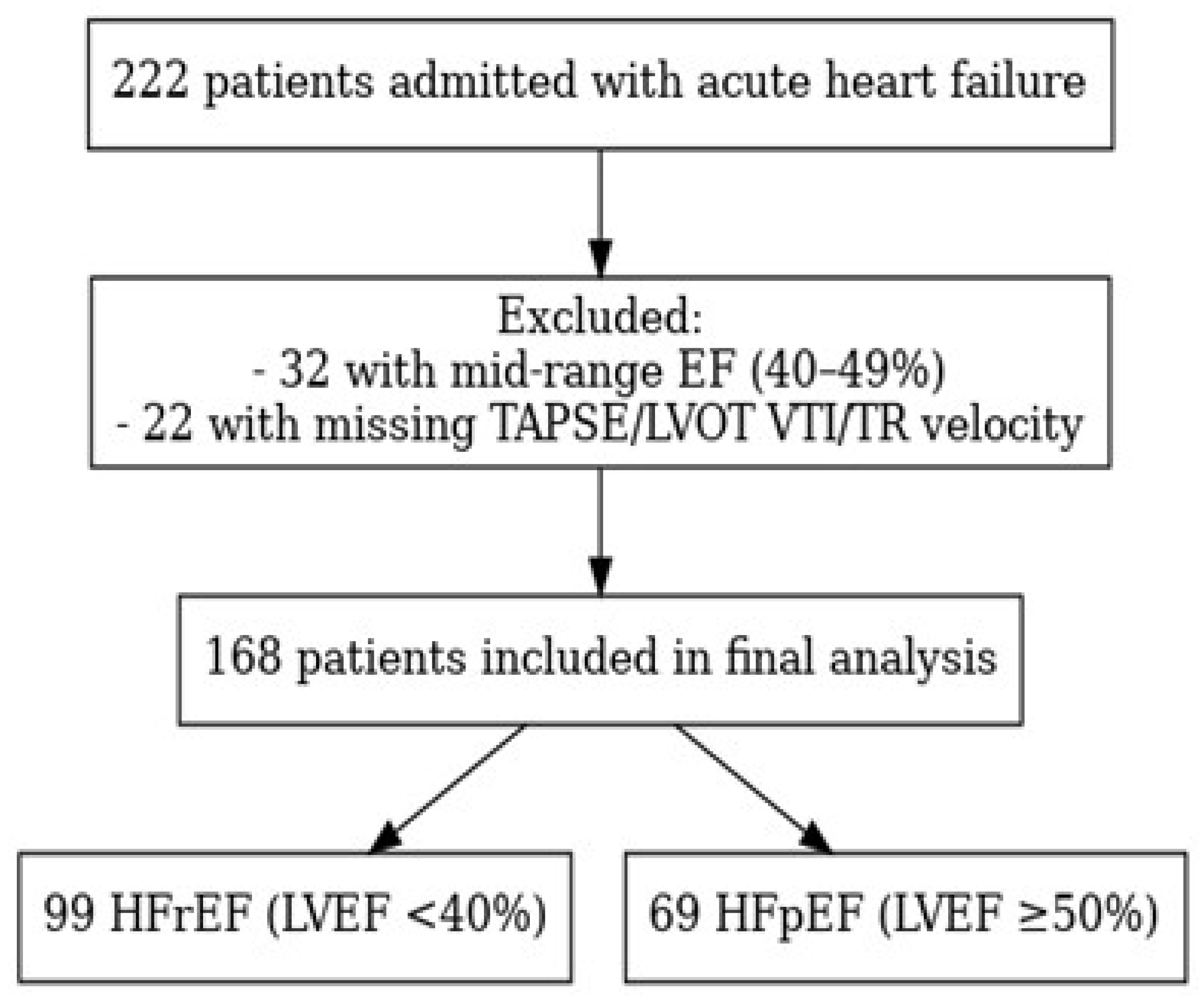
Figure 2.
Receiver operating characteristic (ROC) curves illustrating the predictive performance of the Virtue Index and conventional echocardiographic parameters for in-hospital mortality in patients with HFpEF. RV–RA gradient= right ventricular to right atrial pressure gradient; TAPSE = tricuspid annular plane systolic excursion; LVOT VTI = left ventricular outflow tract velocity–time integral.
Figure 2.
Receiver operating characteristic (ROC) curves illustrating the predictive performance of the Virtue Index and conventional echocardiographic parameters for in-hospital mortality in patients with HFpEF. RV–RA gradient= right ventricular to right atrial pressure gradient; TAPSE = tricuspid annular plane systolic excursion; LVOT VTI = left ventricular outflow tract velocity–time integral.
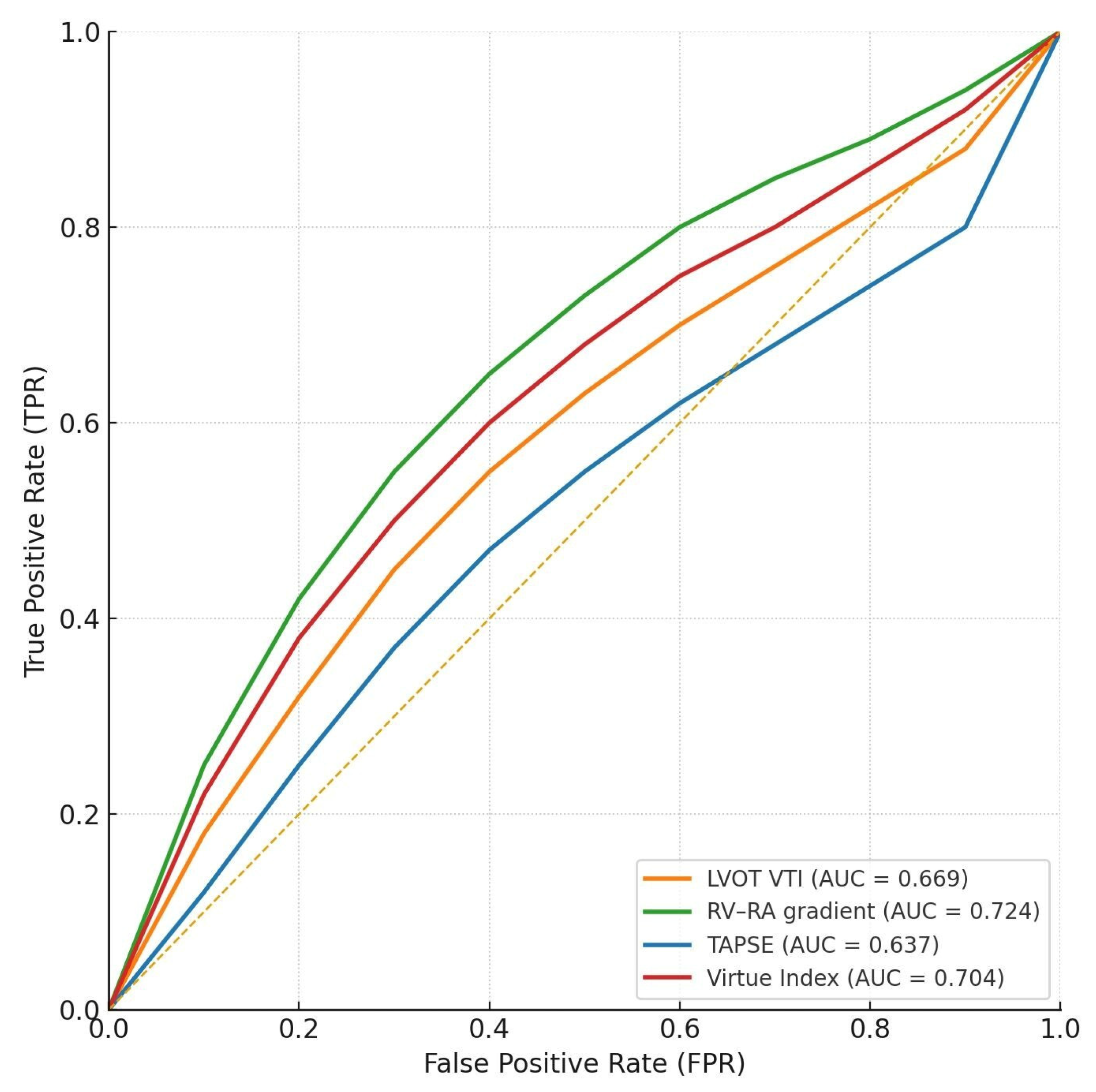
Figure 3.
Receiver operating characteristic (ROC) curves illustrating the predictive performance of the Virtue Index and conventional echocardiographic parameters for in-hospital mortality in patients with HFrEF. RV–RA gradient = right ventricular to right atrial pressure gradient; TAPSE = tricuspid annular plane systolic excursion; LVOT VTI = left ventricular outflow tract velocity–time integral.
Figure 3.
Receiver operating characteristic (ROC) curves illustrating the predictive performance of the Virtue Index and conventional echocardiographic parameters for in-hospital mortality in patients with HFrEF. RV–RA gradient = right ventricular to right atrial pressure gradient; TAPSE = tricuspid annular plane systolic excursion; LVOT VTI = left ventricular outflow tract velocity–time integral.
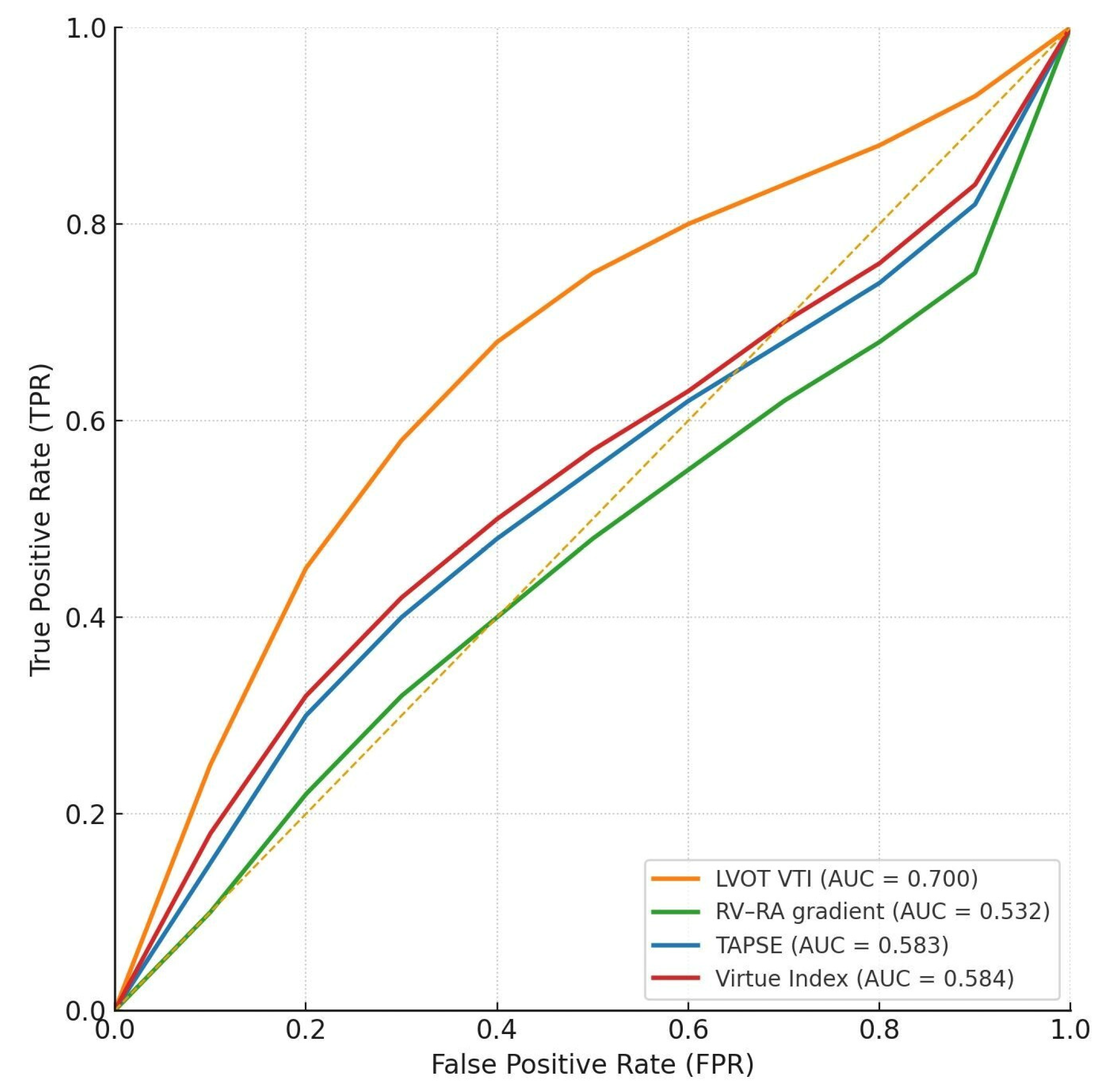
Figure 4.
Receiver operating characteristic (ROC) curves comparing the Virtue Index and NT-proBNP for in-hospital mortality prediction in patients with HFrEF.
Figure 4.
Receiver operating characteristic (ROC) curves comparing the Virtue Index and NT-proBNP for in-hospital mortality prediction in patients with HFrEF.
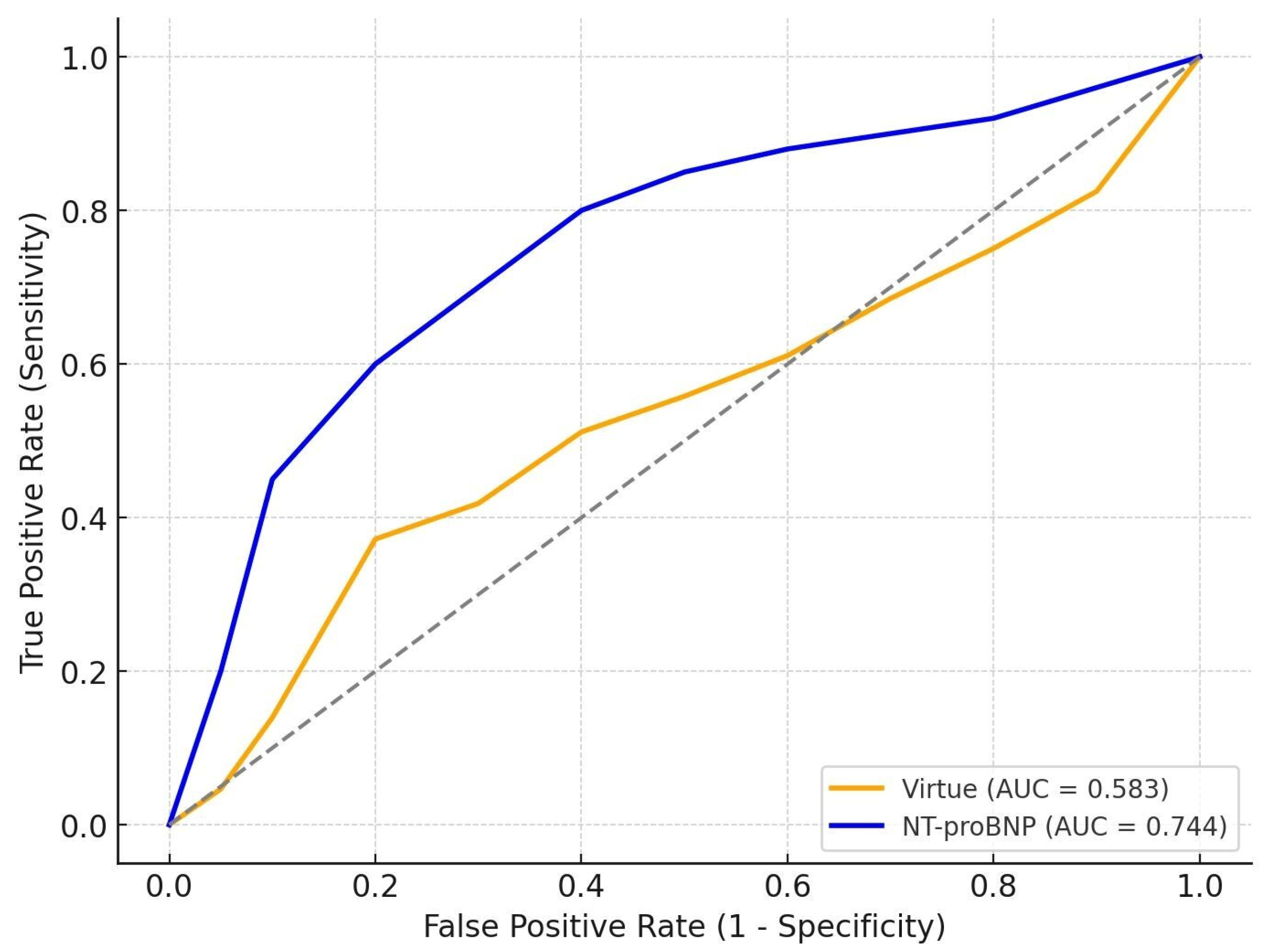
Figure 5.
Receiver operating characteristic (ROC) curves comparing the Virtue Index and NT-proBNP for in-hospital mortality prediction in patients with HFpEF.
Figure 5.
Receiver operating characteristic (ROC) curves comparing the Virtue Index and NT-proBNP for in-hospital mortality prediction in patients with HFpEF.
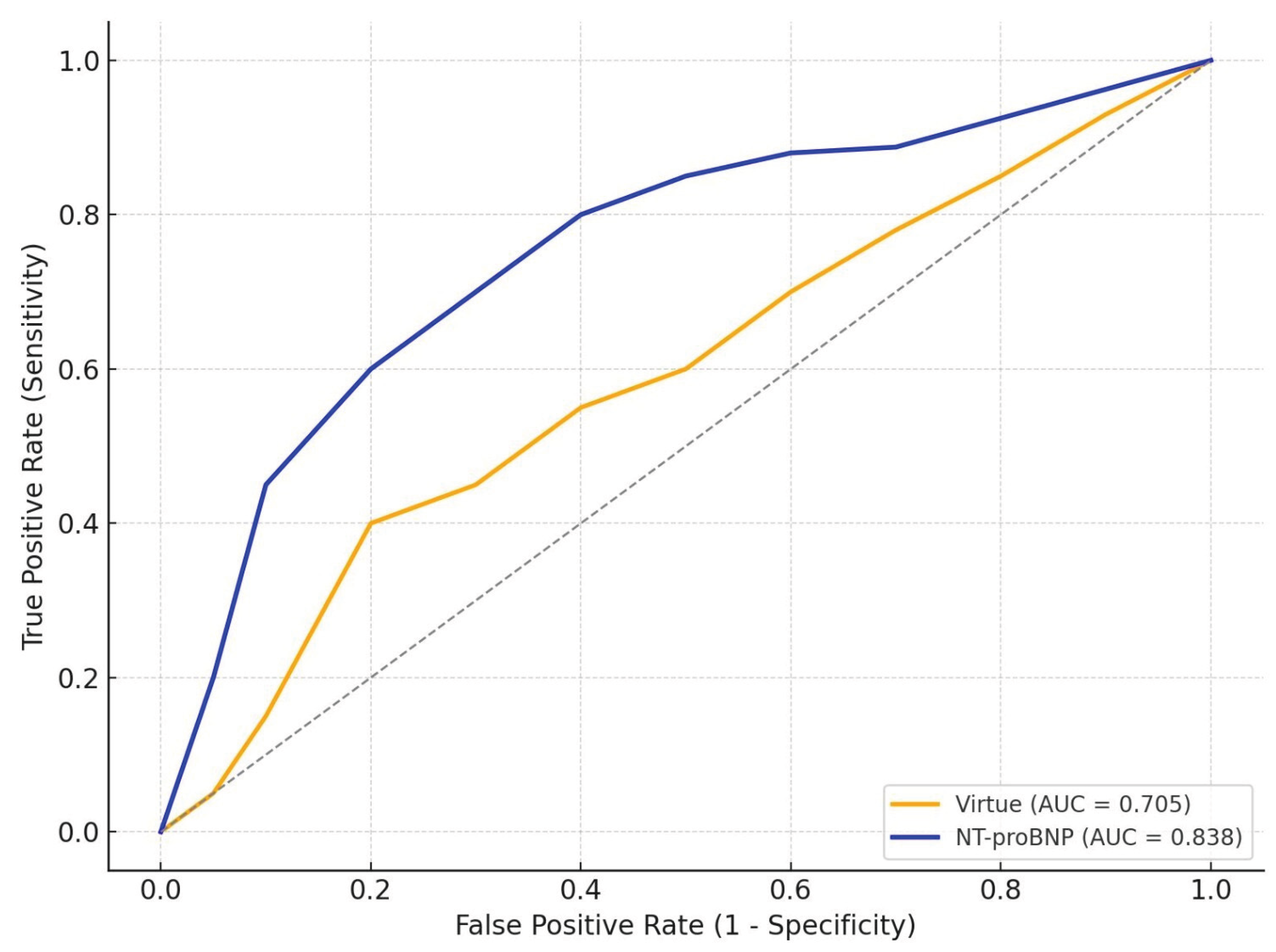

Table 1.
Baseline demographic, clinical, and echocardiographic characteristics according to ejection fraction phenotype.
Table 1.
Baseline demographic, clinical, and echocardiographic characteristics according to ejection fraction phenotype.
| Variable | Total (n = 168) | HFrEF (n = 99) | HFpEF (n = 69) | p-value |
| Age (years) | 71 ± 14 | 65,9 ± 14,9 | 77.6 ± 9.6 | < 0.001 |
| Male sex, % | 50.6% | 66.7% | 27.5% | < 0.001 |
| Smoking, % | 25.5% | 36.4% | 8.7% | < 0.001 |
| Hypertension, % | 88.1% | 82.8% | 95.7% | 0.017 |
| Dyslipidemia, % | 94.6% | 94.9% | 94.2% | 0.830 |
| Obesity, % | 28.1% | 30.3% | 24.6% | 0.460 |
| Diabetes mellitus, % | 39.9% | 41.4% | 37.7% | 0.630 |
| Valvular heart disease, % | 78.0% | 80.8% | 73.9% | 0.290 |
| Systolic BP (mmHg) | 143 ± 31 | 143 ± 31 | 142 ± 31 | 0.837 |
| Diastolic BP (mmHg) | 85 ± 17 | 87 ± 17 | 81 ± 17 | 0.026 |
| NT-proBNP (pg/mL) | 7830 [3698 – 21764] | 8453 [4957 – 21121] | 6537 [2180 – 24554] | 0.411 |
| RV-RA gradient (mmHg) | 30.0 [22.8 – 40.0] | 17.0 [14.0 – 22.0] | 21.0 [17.0 – 24.0] | < 0.001 |
| TAPSE (mm) | 21 ± 9 | 20 ± 10 | 21 ± 7 | 0.410 |
| LVOT VTI (cm) | 16 ± 5 | 14 ± 4 | 21 ± 7 | < 0.001 |
| LVEF (%) | 41 ± 18 | 28 ± 7 | 60 ± 7 | < 0.001 |
| Atrial fibrillation | 47.0% | 36.4% | 62.3% | 0.002 |
| CAD | 45.8% | 58.6% | 27.5% | < 0.001 |
| eGFR at admission | 60.0 [44.8 – 81.0] | 63.0 [46.0 – 81.5] | 54.0 [44.0 – 80.0] | 0.030 |
| In-hospital mortality | 10.1% | 9.1% | 11.6% | 0.788 |
| Virtue Index | 0.098 [0.057 – 0.190] | 0.135 [0.069 – 0.215] | 0.075 [0.049 – 0.110] | < 0.001 |
Data are presented as mean ± standard deviation (SD) for normally distributed variables or as median [interquartile range] for non-normally distributed variables. Categorical variables are expressed as percentages.Comparisons were performed between patients with reduced ejection fraction (HFrEF, LVEF < 40%) and those with preserved ejection fraction (HFpEF, LVEF ≥ 50%).p-values refer to differences between HFrEF and HFpEF. BP= blood pressure; CAD = coronary artery disease; eGFR = estimated glomerular filtration rate; HFrEF – heart failure with reduced ejection fraction; HFpEF – heart failure with preserved ejection fraction; LVOT VTI = left ventricular outflow tract velocity–time integral; LVEF = left ventricular ejection fraction; NT-proBNP = N-terminal pro–B-type natriuretic peptide; RV–RA = right ventricular to right atrial pressure gradient; TAPSE = tricuspid annular plane systolic excursion;.
Table 2.
Receiver operating characteristic (ROC) analysis of echocardiographic parameters for in-hospital mortality.
Table 2.
Receiver operating characteristic (ROC) analysis of echocardiographic parameters for in-hospital mortality.
| Group | Predictor | N | Events | AUC | CI95 LOWER | CI95 UPPER | p-value |
| HFrEF | Virtue Index | 99 | 9 | 0.584 | 0.364 | 0.791 | 0.441 |
| HFrEF | RV-RA gradient | 105 | 9 | 0.532 | 0.463 | 0.724 | 0.631 |
| HFrEF | TAPSE | 105 | 9 | 0.583 | 0.454 | 0.770 | 0.303 |
| HFrEF | LVOT VTI | 102 | 9 | 0.700 | 0.530 | 0.850 | 0.014 |
| HFpEF | Virtue Index | 69 | 8 | 0.704 | 0.536 | 0.852 | 0.011 |
| HFpEF | RV-RA gradient | 76 | 8 | 0.724 | 0.542 | 0.902 | 0.015 |
| HFpEF | TAPSE | 76 | 8 | 0.637 | 0.457 | 0.891 | 0.216 |
| HFpEF | LVOT VTI | 71 | 8 | 0.669 | 0.456 | 0.861 | 0.102 |
Area under the curve (AUC) values with 95% confidence intervals (CI) for the Virtue Index and conventional echocardiographic parameters, stratified by ejection fraction (EF); Differences in N reflect missing data for specific echocardiographic variables; AUC = area under the ROC curve; CI = confidence interval.HFrEF – heart failure with reduced ejection fraction; HFpEF – heart failure with preserved ejection fraction; RV–RA = right ventricular to right atrial pressure gradient; TAPSE = tricuspid annular plane systolic excursion; LVOT VTI = left ventricular outflow tract velocity–time integral;.
Table 3.
Spearman correlation coefficients (ρ) between the Virtue Index and NT-proBNP, stratified by ejection fraction (EF) subgroup, with 95% confidence intervals (CI).
Table 3.
Spearman correlation coefficients (ρ) between the Virtue Index and NT-proBNP, stratified by ejection fraction (EF) subgroup, with 95% confidence intervals (CI).
| Group | N_pairs | Spearman_rho | CI95_lower | CI95_upper | p-value |
| HFrEF | 96 | 0.191 | -0.006 | 0.384 | 0.061 |
| HFpEF | 66 | 0.380 | 0.134 | 0.580 | 0.002 |
Values are presented as Spearman correlation coefficients (ρ) with 95% confidence intervals (CI); HFrEF – heart failure with reduced EF; HFpEF – heart failure with preserved EF.
Table 4.
Pairwise AUC comparisons between the Virtue Index and conventional echocardiographic parameters using the DeLong test, stratified by ejection fraction (EF) subgroup.
Table 4.
Pairwise AUC comparisons between the Virtue Index and conventional echocardiographic parameters using the DeLong test, stratified by ejection fraction (EF) subgroup.
| Group | Comparison | Delta_AUC(Virtue - X) | Z | p-value | N_common |
| HFrEF | Virtue vs RV–RA gradient | 0.052 | 0.407 | 0.684 | 99 |
| HFrEF | Virtue vs TAPSE | 0.001 | 0.008 | 0.994 | 99 |
| HFrEF | Virtue vs LVOT VTI | -0.116 | -0.894 | 0.372 | 99 |
| HFpEF | Virtue vs RV–RA gradient | -0.020 | -0.186 | 0.852 | 69 |
| HFpEF | Virtue vs TAPSE | 0.067 | 0.504 | 0.614 | 69 |
| HFpEF | Virtue vs LVOT VTI | 0.035 | 0.277 | 0.782 | 69 |
AUC = area under the ROC curve; ΔAUC = difference in AUC between Virtue and comparator; HFrEF = heart failure with reduced ejection fraction; HFpEF = heart failure with preserved ejection fraction.RV–RA = right ventricular to right atrial pressure gradient; TAPSE = tricuspid annular plane systolic excursion; LVOT VTI = left ventricular outflow tract velocity–time integral; N_common = number of paired observations included in both ROC analyses; Z = standardized Z-score derived from the DeLong test.
Table 5.
Comparison of area under the ROC curve (AUC) values for the Virtue Index and NT-proBNP in predicting in-hospital mortality, stratified by ejection fraction (EF) subgroup.
Table 5.
Comparison of area under the ROC curve (AUC) values for the Virtue Index and NT-proBNP in predicting in-hospital mortality, stratified by ejection fraction (EF) subgroup.
| Group | N | AUC_Virtue | AUC_NTproBNP | p-value |
| HFrEF | 99 | 0.583 | 0.744 | 0.040 |
| HFpEF | 69 | 0.705 | 0.838 | 0.050 |
AUC = area under the ROC curve; HFrEF – heart failure with reduced ejection fraction; HFpEF – heart failure with preserved ejection fraction; NT-proBNP = N-terminal pro–B-type natriuretic peptide; N = number of patients included in each subgroup.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



