
Submitted:
30 October 2025
Posted:
31 October 2025
You are already at the latest version
Abstract
Background/Objectives: In the past few decades, there have been advancements in surgical techniques, improved understanding of spinal biomechanics, and awareness of complications associated with Halo Vest (HV) use with resultant surgical treatment of various pathologies that cause acute or chronic atlanto-axial instability. The purpose of this study was to see how HV usage has changed over time.
Methods: A retrospective analysis of the North American Clinical Trials Network database. Patients with cervical spinal cord in-jury from 2006 through 2019 were identified and trend of HV use was analyzed.
Results: The mean age of patients who received HV was 37.4 years and 50 for those treated with other options, P < 0.0001. Its use consistently declined after 2009. After 2015 this decline reached nil in the database (P < 0.0001). Patients between 45 and 59 years (3.4%) and above 60 years (2.8%) group had the least treatment using HV. Fall accident (4.7%, P = 0.0295) and Central cord syndrome (4.6%, P = 0.0004) were associated with low HV use. Pulmonary complications were higher (89.4%) with HV use (vs. 65.9% with no HV), P = 0.0008. Pulmonary complications with HV decreased after 2012.
Conclusions: HV as treatment option for conditions involving the cervical Spine has decreased. This declining trend is attributable to decreased use in older individuals due to higher rates of complications and unfavorable outcomes with its use. The decreasing trend appears to coincide with published data showing better outcomes with surgical treatment and unfavorable outcomes with HV use.
Keywords:
Halo Vest
; cervical spine
; spinal cord injury
; North American clinical trials network
; NACTN
1. Introduction
Halo vest (HV) has been a widely used option of management to stabilize the cervical spine since its advent in 1959 [1]. Particularly, it is used in the stabilization of the occipital-atlantoaxial junction to treat cervical spine fractures and dislocation [1,2,3,4]. Believed to be the most effective external stabilization for the cervical spine with success rates as high as 85% [2] its reported specific success rates of fracture fusion are as high as 94.6% and overall clinical success of 89% [4]
In the past few decades, there have been advancements in surgical techniques like C1 lateral mass screw fixation, anterior screw fixation for C2 dens fracture, and posterior C2 pedicle, pars, translaminar sub/trans-facet screw fixations for various pathologies that cause acute or chronic atlanto-axial instability and would have been treated with HV in previous times [5,6,7,8,9,10,11,12]. There has also been improved understanding of spinal biomechanics showing presence of cumulative cervical motion despite HV use and better stability with surgical immobilization using screw fixation [13,14,15,16]. In addition, there is a growing awareness of HV-associated complications like non-union, pin loosening or penetration of dura, pneumonia, orbital fracture and skin irritation to name few [17,18,19,20] that may affect the use of this technique.
Therefore, it is of interest to see how actual HV usage rate has changed over time. Here, we present the trends in HV utilization among the North American Clinical Trials Network (NACTN) group using information from the NACTN database in order to inform clinicians of its use pattern in our times.
2. Materials and Methods
A retrospective analysis of the North American Clinical Trials Network (NACTN) database was performed. NACTN is a syndicate of university-affiliated clinical centers (8 centers currently) equipped with expertise and resources in SCI management with a goal to advance quality of life for people with SCI through clinical trials of promising therapies [21]. Patients who had SCI between the years 2006 and 2019 were selected. Of the patients with SCI, those with cervical level SCI were further identified. Data points consisted of age, sex, race, comorbidities, category of injury, mechanism of injury (MOI), spinal level of injury and American Spinal Injury Association (ASIA) Impairment Scale (AIS). Data points with incomplete variables were excluded from the calculation involving the specific variable. Age was assessed as a continuous as well as categorical variables. For categorical assessment of age, it was classified as Pediatric (0-18 years), Young Adult (18-25 years), Adult (26-44 years), Middle Aged (45-59 years), and Above 60 for >60 years [22]. Gender was classified as either Male or Female. Category of injury included blunt, crush, penetrating and other as labeled in the database. MOI was categorized into motor vehicle accident (MVA), fall, sport/recreation, assault (gunshot wound, stabbing, or blunt trauma), and other. Comorbidities and complications of treatment recorded in the data were also identified and described accordingly. Initially the cohort containing cervical SCI patients was described. Afterwards, patients within the cohort were stratified into those that had and had not received HV after injury. Trend for HV usage per year was analyzed for the study period. Descriptive statistics, Student’s t-test and Mann-Whitney U test were calculated for continuous variables depending on normality of distribution. Categorical variables were analyzed using proportions with 95% confidence interval and bivariate correlation studies, where Pearson’s Chi-Square and Fisher’s exact tests were used to assess statistical significance. Findings are summarized in a tabular and figure format. Statistical significance was determined for p-values < 0.05. All statistical calculations were performed using GraphPad Prism version 10.4.1 for Windows, GraphPad Software, Boston, Massachusetts, USA, www.graphpad.com.
3. Results
3.1. General Cohort
There were a total of 1,030 spine trauma patients within the NACTN registry. Of these, 516 patients (50.1%) had cervical SCI. In total 47/516 (9.1%) SCI patients were treated with an HV. Table 1 summarizes the cohort using different variables. The mean age (SD, range) of was 48.9 (17.8, 14.7–88.4) years. Middle aged individuals (45–59 yrs) comprised the highest proportion (28.5%) closely followed by the above 60 years age group (27.5%) and adults (26–44) making up 23.1% of the total cohort. Young Adults (19–25) comprised 12.4% and in 8.3% the age was not documented. Males comprised 78.9% and females 21.1%. The cohort is predominantly composed of Caucasians (70.3%) followed by blacks (19.9%). Race is recorded as “Other” in 9.7%. Fall accident was the most common cause of injury (42.5%) followed by MVA (36.6%). Sports and recreation accounted for (13.7%). Most of the injuries were categorized as blunt (89%) while the categories of crush and penetrating injuries accounted for 6.2% and 1.9%, respectively. The most common levels of injury were C5 (25.8%), C3 (23.6%), C4 (18.6%) and C6 (18.2%). C1, C2 and C7 accounted for 3.3%, 6.8% and 3.7%, respectively. AIS A and D were the most common injury grades, accounting for 36.4% and 36.2%, respectively. AIS C accounted for 15.1% and AIS B 12.3%. Table 1 shows count and proportion of variables including comorbidities within the cohort.
3.2. Figures, Tables and Schemes
3.2.1. Comparison of Patients Treated with Halo Vest to No Halo Vest
The highest number for halo vest usage was in 2008 but proportion wise 2007 had the highest percentage of HV use (Figure 1). As reflected in the figure the use of HV consistently declined after 2009, after 2015 this decline stabilized (P < 0.0001). Table 2 summarizes the cohort by differentiating it based on HV usage. The mean age (SD, range) of patients who received HV was 37.4 (17.4, 19.9–83.5), the mean for those not treated with HV was 50 (17.5, 14.7–88.4) years P < 0.0001. The highest utilization of HV was noted in the young adult age group (20.3%) followed by the adult group (16%) P < 0.0001. Another prominent finding is patients in the middle age and elderly group were the ones that had the least treatment using HV, 3.4% and 2.8%, respectively. HV was more frequently used in females (11.8%), and Blacks (12.8%) in the cohort, however with no statistical significance. Based on injury type, similar proportion of patients with penetrating (10%) and blunt (9.6%) types of injuries were treated with HV, the findings being statistically insignificant. Compared to other injuries, MVA had the highest association with HV usage (13%) followed by Sports/Recreation and assault injuries, that had similar (11.6% and 11.1%, respectively) percent of associated usage. Injury at C2 had the highest percentage (17.1%) of HV usage compared to injury at other cervical spine levels. Other levels of injury associated with higher usage of HV included C6 (12.8%) and C5 (12%). The association of vertebra level of injury to HV use is close statistical significance. It appears more severe injuries were associated with more frequent use of HV as displayed in the table, but not to a level of statistical significance. The presence of central cord syndrome was associated with 4.6% use of an HV, P = 0.0004. Pulmonary complications were present in 89.4% of patients treated with HV versus 65.9% in those not treated with HV, P = 0.0008. A post-hoc analysis regarding pulmonary complications within the cohort revealed a decreasing trend after 2012 (Figure 2). The highest occurrence of pulmonary complications was in the adult (26–44) age group (30.2%), followed by middle age and young adult groups, 25.9% and 24.6% respectively. Pulmonary complications were recorded in 16.2% of patients in the above 60 group (Table 3). Nonetheless, the finding of age group and pulmonary complications occurrence was nearly but not statistically significant (P = 0.0673). Supplementary Figures S1, S2 and S3 show Cardiac, GI/GU and Skin complication trends for the study period.
4. Discussion
The findings of this study show the declining trend of using HV as a treatment for cervical spine injuries within the NACTN institutes. C2 injuries had the highest proportion of HV use, possibly indicating odontoid fractures. Comparison of patients treated with HV and alternative treatment shows there is no significant difference except in age categories, mechanism of injury, presence of central cord syndrome, diabetes and pulmonary complications. A close look into the findings (Table 1) shows older age groups (middle age and above 60 years) and presence of variables associated with older age groups, like fall accidents, diabetes and central cord syndrome [23,24], are relatively lower in proportion for the group treated with HV. On the contrary, there is a relatively higher proportion of measures for variables associated with younger patients like motor vehicle accidents, sports injury and assaults in the HV group. Another finding is a statistically significant higher pulmonary complication in patients treated with HV. We believe the decreasing trend in HV usage has in part to do with the occurrence of pulmonary complications in older patients. This is further supported by the findings of lower pulmonary complication occurrence that coincides with the decreasing trend of HV use (Figure 2). In addition, there is a relatively lower occurrence of pulmonary complications in the above 60 years group within the cohort, although not to a statistically significant level (Table 3).
Initially HV has was used as a head stabilizing technique in patients with neck muscle paralysis due to poliomyelitis and it was described in 1959[1]. Later, it was used for early stabilizing of the neck in patients with cervical spine injury [3]. However, its use came under scrutiny and was associated with complications, hence promoting safer and more effective treatment for cervical spine injury. The works by Garfin et al. [25] and Glaser et al. [26] in the mid-80s are some of the early well-organized reviews on complications with the use of HV. Eventually, a study based on a database from the state of New York identified a decreasing trend of HV use in 2020 [27].
Literature shows that complications surrounding HV are higher in older patients, including morbidity and mortality [28,29,30,31,32,33]. Aside from the case series regarding sporadic complications that have been reported [34,35,36], there were also reviews showing more frequent complications with HV use. In their study about HV indications and complications, Lee et al. [37] , reviewed complications from thirteen studies and identified orbital roof fracture, orbital cellulitis, sub-orbital nerve injury, intracranial penetration, liquorrhea, pneumocephalus, epileptic seizure, dysphagia/aspiration, pin site infection, persistent instability, loss of subluxation reduction, halo ring dislocation, decubitus ulcer, fracture nonunion, graft subsidence, non-specific respiratory problems, pneumonia, and death as commonly reported complications. The authors noted complications ranged between 11–92% mostly within the 30–50% range.
Harrop et al. [30] in 2010, in a meta-analysis of thirty-eight papers found out non-union in elderly patients, after HV treatment of type II/III odontoid fractures (OF), reached up to 78% unlike surgical treatment that had a non-union rate of 0% to 65.5%. Their conclusion was weak recommendation of surgery for type II OF and hard collar in type III OF. Even more concerning from some studies within this meta-analysis was the issue of morbidity and mortality with the use of HV. One of the studies by Tashjian et al. [38] in 2006 found a complication rate of 66% (versus 36% for no HV) and mortality of 42% (versus 20% for no HV) in elderly patients treated with HV. Again, Taitsman et al. [39] in 2008 reported 55% complication rate with 23% having severe respiratory complication. Majercik et al. [33] in 2005 reported 40% mortality in patients >65 years old on HV compared to 2% for those <65 years old, in addition to 6% and 12% mortality for patients >65 years old had had surgery and cervical collar, respectively. This finding made the authors to liken HV use in the elderly a death sentence.
Of note, in our study the respiratory complication in the HV group is significantly higher (89.4% vs 65.9%). Such high numbers possibly indicate other underlying co-morbidity or injury, as Malnik et al. [19] reported that low GCS and high Injury Severity Score were highly associated with pneumonia. The authors also found 86% of patients with GCS < 12 had pneumonia and all patients who had pneumonia were sometime during their care on mechanical ventilation.
Vaccaro et al. [40] in 2013 published the results of a prospective study comparing surgical and non-surgical treatment of dens fractures showing significantly better outcome in neck disability index and Short-Form 36v2 as well as lower rate of non-union (5% vs 21%) for the surgically treated group. Besides these benefits, the study also showed less mortality (14% vs 26%) for the surgical group at twelve-month follow-up. These findings led them to recommend that elderly patients with type II dens fracture to be treated surgically if they are healthy enough for general anesthesia. In addition, Ivancic et al. [13] showed screw fixation was favored for Type II dens fracture after assessing motion reduction at C1/2 using HV combined with screw fixation and comparing it to an earlier report of screw and wiring in reducing C1/C2 motion reduction. The timeline of these findings matches the timeline in our finding where HV usage rate started to flatten (2013) and non-HV treatment started to trend upwards, perhaps the findings sparking a global application of surgical treatment in all age groups for cervical spine fractures/instability.
Despite these findings, recent studies from Italy still suggest that HV is a viable treatment option in younger patients but admittedly oppose its indication in older patients [4,41].
Our study is not without limitations. First, the specific diagnosis of the condition that was treated is not specified within the data, so we are not able to further define in what situations HV was used versus surgical treatment and only know level specific data. It is also not within the scope of this study to find out what the indications of HV use are but to define the trend of its use, which it clearly depicted. Second, the database is from the NACTN study group and the practice pattern in other centers outside this group are not explored to get a more general picture. However, combined with the decent number of patients and these centers being a specialized Level I trauma centers within the US and Canada the practice pattern can be representative. Future directions should aim at prospectively identifying which injuries and patient groups are most amenable to HV application., include more of institutes to get a broader idea and possibly survey physicians involved in the care of such patients to identify why they prefer or not HV use. There is also a need to further validate surgical interventions that are replacing HV use for atlanto-axial instability.
5. Conclusionห
The use of HV as treatment option for conditions involving the cervical spine has decreased. The decreasing trend is highly attributable to decreased use in older individuals. Higher rates of complications and unfavorable outcomes with HV use and better outcomes with surgical treatment appear to drive the decreasing trend from clinical and more precise perspectives. The decreasing trend appears to coincide with published data showing better outcomes with surgical treatment and unfavorable outcomes with HV use.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1. Trend of Cardiac Complications in the Cohort of Cervical Spinal Cord Injury patients. Figure S2. Trend of Gastrointestinal/Genitourinary Complications in the Cohort of Cervical Spinal Cord Injury patients. Figure S3. Trend of Skin Complications in the Cohort of Cervical Spinal Cord Injury patients.
Author Contributions
Conceptualization: Teleale F. Gebeyehu, Michael Vo, and James Harrop; Methodology: Teleale F. Gebeyehu and Michael Vo; Formal Analysis: Teleale F. Gebeyehu; Validation: James Harrop; Resources: James Harrop and Michael Vo; Data Curation: Teleale F. Gebeyehu and Michael Vo; Writing—original draft preparation: Teleale F. Gebeyehu, Michael Vo and Adam Leibold; Writing—review and editing: Teleale F. Gebeyehu, Adam Leibold, Shaan Patel; Alexander R. Vaccaro, Jack Jallo and James Harrop; Visualization: Teleale F. Gebeyehu.; Supervision: James Harrop; Project Administration: Teleale F. Gebeyehu and James Harrop. All authors have read and agreed to the published version of the manuscript.”
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to use of deidentified data.
Informed Consent Statement
Patient consent was not needed due to deidentified data.
Data Availability Statement
Data can be accessed by contacting the North American Clinical Trials Network group (https://www.christopherreeve.org/tomorrows-cure/current-research-partners-and-initiatives/nactn/).
Conflicts of Interest
Teleale F. Gebeyehu—None. Michale Vo—None. Adam Leibold—None. Shaan Patel—None. Jack Jallo—None. Alexander R. Vaccaro—Receives royalty payments from Alphatec (Atec), Atlas Spine, Curiteva, Elseviere, Globus, Jaypee, Medtronics, Spinal Elements, SpineWave, Stryker Spine, Taylor Francis/Hodder and Stoughton, Thieme, and Wheel House Medical. Stock/stock option ownership interests are held in Accellus, Advanced Spinal Intellectual Properties, Atlas Spine, AVKN Patient Driven Care, Avaz Surgical, Cytonics, Deep Health, Dimension Orthotics, LLC, Electrocore, Flagship Surgical, FlowPharma, Globus, Harvard Medtech, Innovative Surgical Design, Jushi, Orthobullets, Parvizi Surgical Innovation, Progressive Spinal Technologies, Rothman Institute and Related Properties, See All AI, Sentryx, Stout Medical, and ViewFi Health. Consulting/Independent Contractor for Accellus, Curiteva, Ferring Pharmaceutical, Globus, Medcura, Spinal Elements, Stryker Spine, and Wheel House Medical. Service on a Scientific Advisory Board/Board of Directors/ Service on Committees for Accellus, the National Spine Health Foundation (NSHF), and Sentryx. Member in good standing/independent contractor for AO Spine and Expert Testimony. James Harrop—None.
Abbreviations
The following abbreviations are used in this manuscript:
| AIS | ASIA Impairment Scale |
| ASIA | American Spinal Injury Association |
| CI | Confidence Interval |
| GI/GU | Gastrointestinal / Genito Urinary |
| HV | Halo Vest |
| MOI | Mechanism of Injury |
| MVA | Motor Vehicle Accident |
| NACTN | North American Clinical Trials Network |
| OF | Odontoid Fracture |
| SCI | Spinal Cord injury |
| SD | Standard Deviation |
| USA | United States of America |
References
- Perry, J.; Nickel, V.L. Total Cervical-Spine Fusion for Neck Paralysis. JBJS 1959, 41. [Google Scholar]
- Koutsogiannis, P.; Weisbrod, L.J.; Dowling, T.J. Halo brace. In StatPearls [Internet]; StatPearls Publishing: 2024.
- Parry, H.; Delargy, M.; Burt, A. Early mobilisation of patients with cervical cord injury using the halo brace device. Spinal Cord 1988, 26, 226–232. [Google Scholar] [CrossRef]
- Rispoli, R.; Iacopino, G.; Giorgiutti, F.; Veltri, C.; Copetti, E.; Imbrucè, P.; Cappelletto, B. Halo Vest Immobilization: Is It Still a Valid Treatment for Atlantoaxial Fractures? World Neurosurgery 2025, 193, 737–746. [Google Scholar] [CrossRef]
- Chang, D.G.; Ko, J.H.; Park, J.B.; Ju, G.I. Anterior Dens Screw Fixation for Traumatic C1-2 Lateral Subluxation With 3-Part Fractures of the C2 Axis (Dens, Lateral Mass, and Hangman Fractures): A Case Report. J Am Acad Orthop Surg Glob Res Rev 2021, 5. [Google Scholar] [CrossRef] [PubMed]
- Furuya, T.; Yamazaki, M.; Okawa, A.; Misawa, S.; Sakuma, T.; Takahashi, H.; Kato, K.; Kuwabara, S.; Takahashi, K. Cervical myelopathy in patients with athetoid cerebral palsy. Spine (Phila Pa 1976) 2013, 38, E151–E157. [Google Scholar] [CrossRef]
- Harati, A.; Oni, P. Three-point atlantoaxial fixation with C1-C2 transarticular screws and C1 lateral mass screws. J Orthop Surg (Hong Kong) 2019, 27, 2309499019854201. [Google Scholar] [CrossRef]
- Konieczny, M.R.; Gstrein, A.; Müller, E.J. Treatment of Dens Fractures with Anterior Screw Fixation. JBJS Essent Surg Tech 2014, 4, e9. [Google Scholar] [CrossRef] [PubMed]
- Oliver, J.D.; Goncalves, S.; Kerezoudis, P.; Alvi, M.A.; Freedman, B.A.; Nassr, A.; Bydon, M. Comparison of Outcomes for Anterior Cervical Discectomy and Fusion With and Without Anterior Plate Fixation: A Systematic Review and Meta-Analysis. Spine (Phila Pa 1976) 2018, 43, E413–e422. [Google Scholar] [CrossRef]
- Pommier, B.; Ollier, E.; Pelletier, J.-B.; Castel, X.; Vassal, F.; Tetard, M.-C. Conservative versus Surgical Treatment for Odontoid Fracture: Is the Surgical Treatment Harmful? Systematic Review and Meta-Analysis. World Neurosurgery 2020, 141, 490–499.e492. [Google Scholar] [CrossRef] [PubMed]
- Tao, X.; Matur, A.V.; Street, S.; Shukla, G.; Garcia-Vargas, J.; Mehta, J.; Childress, K.; Duah, H.O.; Gibson, J.; Cass, D.; et al. No Difference in Surgical Outcomes Between Stand-Alone Devices and Anterior Plating for 1-2 Level Anterior Cervical Discectomy and Fusion: A 1:1 Exact Matched Analysis. Spine (Phila Pa 1976) 2024, 49, 973–978. [Google Scholar] [CrossRef]
- Yamamoto, H.; Kurimoto, M.; Hayashi, N.; Ohmori, T.; Hirashima, Y.; Endo, S. [Atlas burst fracture (Jefferson fracture) requiring surgical treatment after conservative treatment--report of two cases]. No Shinkei Geka 2002, 30, 987–991. [Google Scholar]
- Ivancic, P.C.; Beauchman, N.N.; Mo, F.; Lawrence, B.D. Biomechanics of halo-vest and dens screw fixation for type II odontoid fracture. Spine 2009, 34, 484–490. [Google Scholar] [CrossRef]
- Koch, R.A.; Nickel, V.L. The halo vest: an evaluation of motion and forces across the neck. Spine (Phila Pa 1976) 1978, 3, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Lind, B.; Sihlbom, H.; Nordwall, A. Forces and motions across the neck in patients treated with halo-vest. Spine (Phila Pa 1976) 1988, 13, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Purvis, T.A.; Carlin, B.; Driscoll, P. The definite risks and questionable benefits of liberal pre-hospital spinal immobilisation. Am J Emerg Med 2017, 35, 860–866. [Google Scholar] [CrossRef]
- Boakye, M.; Arrigo, R.T.; Kalanithi, P.S.; Chen, Y.R. Impact of age, injury severity score, and medical comorbidities on early complications after fusion and halo-vest immobilization for C2 fractures in older adults: a propensity score matched retrospective cohort study. Spine (Phila Pa 1976) 2012, 37, 854–859. [Google Scholar] [CrossRef] [PubMed]
- Bransford, R.J.; Stevens, D.W.; Uyeji, S.; Bellabarba, C.; Chapman, J.R. Halo vest treatment of cervical spine injuries: a success and survivorship analysis. Spine (Phila Pa 1976) 2009, 34, 1561–1566. [Google Scholar] [CrossRef]
- Malnik, S.L.; Scott, K.W.; Kuhn, M.Z.; Alcindor, D.; Tavanaiepour, K.; Tavanaiepour, D.; Crandall, M.; Rahmathulla, G. Halo vest immobilization—an institutional review of safety in acute cervical spine injury from 2013 to 2017. Br J Neurosurg 2021, 35, 639–642. [Google Scholar] [CrossRef]
- van Middendorp, J.J.; Slooff, W.-B.M.; Nellestein, W.R.; Öner, F.C. Incidence of and Risk Factors for Complications Associated with Halo-Vest Immobilization: A Prospective, Descriptive Cohort Study of 239 Patients. JBJS 2009, 91. [Google Scholar] [CrossRef]
- Toups, E.G.; Ugiliweneza, B.; Howley, S.P.; Neal, C.J.; Harrop, J.S.; Guest, J.D.; Grossman, R.G.; Fehlings, M.G. North American Clinical Trials Network for Spinal Cord Injury Registry: Methodology and Analysis. J Neurotrauma 2023, 40, 1817–1822. [Google Scholar] [CrossRef]
- Peng, Y.; Zhu, Q.; Wang, B.; Ren, J. A cross-sectional study on interference control: age affects reactive control but not proactive control. PeerJ 2020, 8, e8365. [Google Scholar] [CrossRef] [PubMed]
- Carr, M.T.; Harrop, J.S.; Houten, J.K. Traumatic Central Cord Syndrome. Clin Spine Surg 2024, 37, 379–387. [Google Scholar] [CrossRef]
- Gebeyehu, T.F.; Mong, E.R.; Thalheimer, S.; Vaccaro, A.R.; Harrop, J. Epidemiology of Spinal Cord Injury and Associated Mortality, Past and Present. Is There a Difference? World Neurosurg 2024, 192, e494–e505. [Google Scholar] [CrossRef]
- Garfin, S.R.; Botte, M.J.; Waters, R.L.; Nickel, V.L. Complications in the use of the halo fixation device. JBJS 1986, 68, 320–325. [Google Scholar] [CrossRef]
- Glaser, J.A.; Whitehill, R.; Stamp, W.G.; Jane, J.A. Complications associated with the halo-vest: A review of 245 cases. Journal of Neurosurgery 1986, 65, 762–769. [Google Scholar] [CrossRef] [PubMed]
- Kurucan, E.; Sulovari, A.; Thirukumaran, C.; Greenstein, A.; Molinari, R.; Mesfin, A. Volume-outcome relationship in halo vest utilization for C2 fractures. Spine J 2020, 20, 1676–1684. [Google Scholar] [CrossRef] [PubMed]
- Delcourt, T.; Bégué, T.; Saintyves, G.; Mebtouche, N.; Cottin, P. Management of upper cervical spine fractures in elderly patients: current trends and outcomes. Injury 2015, 46 (Suppl 1), S24–27. [Google Scholar] [CrossRef]
- Harris, M.B.; Reichmann, W.M.; Bono, C.M.; Bouchard, K.; Corbett, K.L.; Warholic, N.; Simon, J.B.; Schoenfeld, A.J.; Maciolek, L.; Corsello, P.; et al. Mortality in Elderly Patients After Cervical Spine Fractures. JBJS 2010, 92. [Google Scholar] [CrossRef]
- Harrop, J.S.; Hart, R.; Anderson, P.A. Optimal Treatment for Odontoid Fractures in the Elderly. Spine 2010, 35. [Google Scholar] [CrossRef]
- Horn, E.M.; Theodore, N.; Feiz-Erfan, I.; Lekovic, G.P.; Dickman, C.A.; Sonntag, V.K.H. Complications of halo fixation in the elderly. Journal of Neurosurgery: Spine SPI 2006, 5, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Koech, F.; Ackland, H.M.; Varma, D.K.; Williamson, O.D.; Malham, G.M. Nonoperative Management of Type II Odontoid Fractures in the Elderly. Spine 2008, 33. [Google Scholar] [CrossRef]
- Majercik, S.; Tashjian, R.Z.; Biffl, W.L.; Harrington, D.T.; Cioffi, W.G. Halo Vest Immobilization in the Elderly: A Death Sentence? Journal of Trauma and Acute Care Surgery 2005, 59. [Google Scholar] [CrossRef]
- Gelalis, I.D.; Christoforou, G.; Motsis, E.; Arnaoutoglou, C.; Xenakis, T. Brain abscess and generalized seizure caused by halo pin intracranial penetration: case report and review of the literature. Eur Spine J 2009, 18 (Suppl 2), 172–175. [Google Scholar] [CrossRef] [PubMed]
- Glover, A.W.; Zakaria, R.; May, P.; Barrett, C. Overtightening of halo pins resulting in intracranial penetration, pneumocephalus, and epileptic seizure. Int J Spine Surg 2013, 7, e42–e44. [Google Scholar] [CrossRef]
- Kingma, R.; Peters, J.M.; Coene, L.N. Intracranial penetration of a halo pin causing an epileptic seizure. J Bone Joint Surg Br 2006, 88, 1654–1655. [Google Scholar] [CrossRef]
- Lee, D.; Adeoye, A.L.; Dahdaleh, N.S. Indications and complications of crown halo vest placement: A review. Journal of Clinical Neuroscience 2017, 40, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Tashjian, R.Z.; Majercik, S.; Biffl, W.L.; Palumbo, M.A.; Cioffi, W.G. Halo-Vest Immobilization Increases Early Morbidity and Mortality in Elderly Odontoid Fractures. Journal of Trauma and Acute Care Surgery 2006, 60. [Google Scholar] [CrossRef]
- Taitsman, L.A.; Altman, D.T.; Hecht, A.C.; Pedlow, F.X. Complications of cervical halo-vest orthoses in elderly patients. Orthopedics 2008, 31, 446. [Google Scholar] [CrossRef] [PubMed]
- Vaccaro, A.R.; Kepler, C.K.; Kopjar, B.; Chapman, J.; Shaffrey, C.; Arnold, P.; Gokaslan, Z.; Brodke, D.; France, J.; Dekutoski, M.; et al. Functional and quality-of-life outcomes in geriatric patients with type-II dens fracture. J Bone Joint Surg Am 2013, 95, 729–735. [Google Scholar] [CrossRef]
- Di Paolo, A.; Piccirilli, M.; Pescatori, L.; Santoro, A.; D’Elia, A. Single institute experience on 108 consecutive cases of type II odontoid fractures: surgery versus conservative treatment. Turk Neurosurg 2014, 24, 891–896. [Google Scholar] [CrossRef]
Figure 1.
Trend of Halo vest usage over the years between 2006–2019. SCI—Spinal Cord Injury.
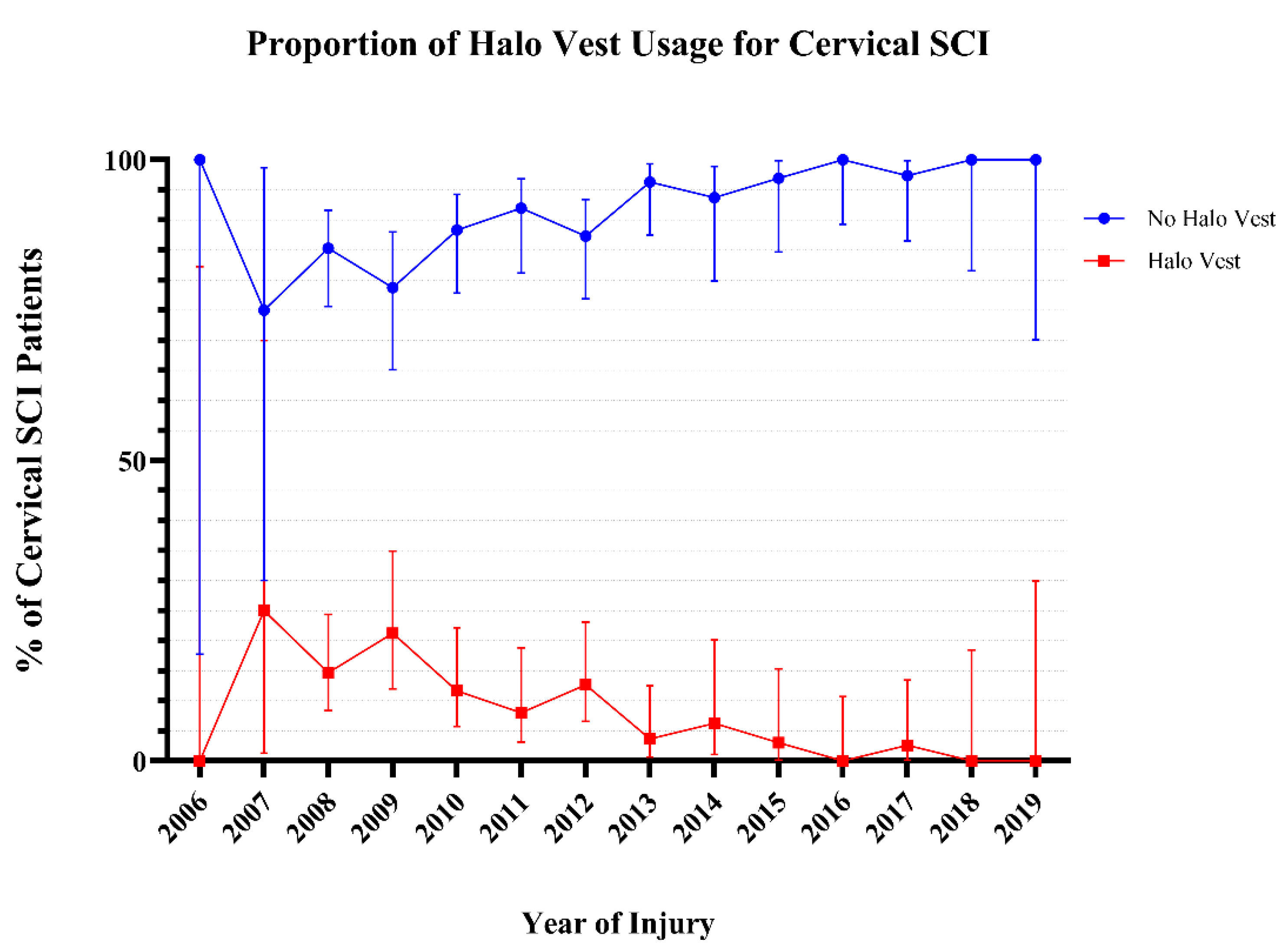
Figure 2.
Trend of proportions for occurrence of pulmonary complications in all patients.
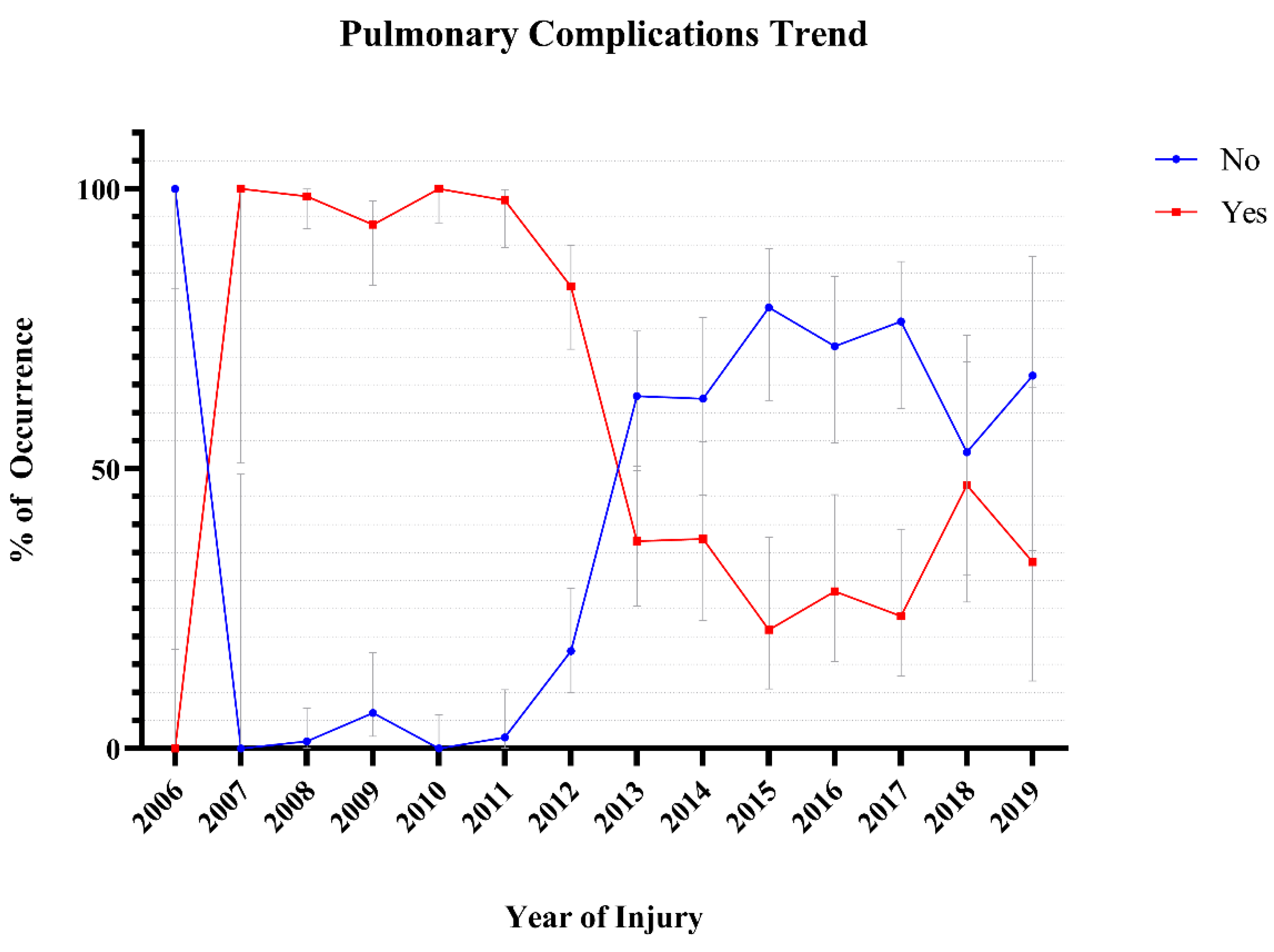

Table 1.
General Descriptive Studies of the Cohort (Cervical SCI) using different variables. ASIA- American Spinal Injury Association; GI/GU- Gastrointestinal/Genitourinary; MVA- Motor Vehicle Accident.
Table 1.
General Descriptive Studies of the Cohort (Cervical SCI) using different variables. ASIA- American Spinal Injury Association; GI/GU- Gastrointestinal/Genitourinary; MVA- Motor Vehicle Accident.
| Mean Age (SD, range) | 48.9 (17.8, 14.7–88.4) years | ||
| Count | % | 95% CI | |
| Halo Vest Use (n = 516) | |||
| Yes | 47 | 9.1 | 6.9–11.9 |
| No | 469 | 90.9 | 88.1–93.1 |
| Age Category (n = 516) | |||
| Pediatric (0–18) | 1 | 0.2 | 0–1.1 |
| Young Adult (19–25) | 64 | 12.4 | 9.8–15.5 |
| Adult (26–44) | 119 | 23.1 | 19.6–26.9 |
| Middle Age (45–59) | 147 | 28.5 | 24.8–32.5 |
| Above 60 | 142 | 27.5 | 23.8–31.5 |
| Unknown | 43 | 8.3 | 6.2–11.0 |
| Sex (n = 483) | |||
| Male | 381 | 78.9 | 75–82.3 |
| Female | 102 | 21.1 | 17.7–25 |
| Race (n = 472) | |||
| Caucasian | 332 | 70.3 | 66.1–74.3 |
| Black | 94 | 19.9 | 16.6–23.8 |
| Other | 46 | 9.7 | 7.4–12.8 |
| Type of Injury (n = 516) | |||
| Blunt | 460 | 89.1 | 86.2–91.5 |
| Crush | 32 | 6.2 | 4.4–8.6 |
| Penetrating | 10 | 1.9 | 1.1–3.5 |
| Other | 14 | 2.7 | 1.6–4.5 |
| Mechanism of Injury (n = 503) | |||
| MVA | 184 | 36.6 | 32.5–40.9 |
| Fall | 214 | 42.5 | 38.3–46.9 |
| Sport/Recreation | 69 | 13.7 | 11.0–17.0 |
| Assault | 18 | 3.6 | 2.3–5.6 |
| Other | 18 | 3.6 | 2.3–5.6 |
| Neurologic Level of Injury (n = 516) | |||
| C1 | 17 | 3.3 | 2.1–5.2 |
| C2 | 35 | 6.8 | 4.9–9.3 |
| C3 | 122 | 23.6 | 20.2–27.5 |
| C4 | 96 | 18.6 | 15.5–22.2 |
| C5 | 133 | 25.8 | 22.2–29.7 |
| C6 | 94 | 18.2 | 15.1–21.8 |
| C7 | 19 | 3.7 | 2.4–5.7 |
| ASIA Impairment Scale (n = 390) | |||
| A | 142 | 36.4 | 31.8–41.3 |
| B | 48 | 12.3 | 9.4–15.9 |
| C | 59 | 15.1 | 11.9–19.0 |
| D | 141 | 36.2 | 31.5–41 |
| Central Cord Syndrome (n = 388) | 174 | 44.8 | 40.0–49.8 |
| Comorbidities (n = 497) | |||
| Hypertension | 166 | 33.3 | 29.3–37.5 |
| Diabetes | 133 | 26.8 | 23.1–30.9 |
| Myocardial Infarction | 19 | 3.8 | 2.5–5.9 |
| Pulmonary co-morbidities | 114 | 23 | 19.5–26.9 |
| Cerebrovascular Accident | 0 | 0 | |
| Malignancy | 8 | 1.6 | 0.8–3.2 |
| Tobacco | 10 | 2 | 1.1–3.7 |
| Drug Abuse | 47 | 9.5 | 7.2–12.4 |
| Complications (n = 516) | |||
| Cardiac | 173 | 33.5 | 29.6–37.7 |
| GI/GU | 210 | 40.7 | 36.5–45.0 |
| Pulmonary | 351 | 68 | 63.9–71.9 |
| Skin | 71 | 16.2 | 11.1–17.0 |
Table 2.
Comparison of Halo Vest and No–Halo Vest Cohort. ASIA- American Spinal Injury Association; GI/GU- Gastrointestinal/Genitourinary; MVA- Motor Vehicle Accident.
Table 2.
Comparison of Halo Vest and No–Halo Vest Cohort. ASIA- American Spinal Injury Association; GI/GU- Gastrointestinal/Genitourinary; MVA- Motor Vehicle Accident.
| Halo Vest | No-Halo Vest | P-Value | |||||
| Mean Age (SD, range) | 37.4 (17.4, 19.9–83.5) | 50.0 (17.5, 14.7–88.4) | <0.0001 | ||||
| Count | % | 95% CI | Count | % | 95% CI | ||
| Age Category (n = 516) | |||||||
| Pediatric (0–18) | 0 | 0 | 0.0–94.9 | 1 | 100 | 5.1–100 | <0.0001 |
| Young Adult (19–25) | 13 | 20.3 | 12.3–31.7 | 51 | 79 | 68.3–87.7 | |
| Adult (26–44) | 19 | 16 | 10.5–23.6 | 100 | 84 | 76.4–89.5 | |
| Middle Age (45–59) | 5 | 3.4 | 1.5–7.7 | 142 | 96.6 | 92.3–98.5 | |
| Above 60 | 4 | 2.8 | 1.1–7.0 | 138 | 97.2 | 93.0–98.9 | |
| Unknown | 6 | 14 | 6.6–27.3 | 37 | 86 | 72.7–93.4 | |
| Sex (n = 483) | |||||||
| Male | 33 | 8.7 | 6.2–11.9 | 348 | 91.3 | 6.9–19.4 | 0.3402 |
| Female | 12 | 11.8 | 6.9–19.4 | 90 | 88.2 | 80.6–88.2 | |
| Race (n = 472) | |||||||
| Caucasian | 302 | 9.0 | 6.4–12.6 | 30 | 91.0 | 87.4–93.6 | 0.4236 |
| Black | 82 | 12.8 | 7.5–21 | 12 | 87.2 | 79.0–92.5 | |
| Other | 43 | 6.5 | 2.2–17.5 | 3 | 93.5 | 82.5–97.8 | |
| Type of Injury (n = 516) | |||||||
| Blunt | 44 | 9.6 | 7.2–12.6 | 416 | 90.4 | 87.4–92.8 | 0.6286 |
| Crush | 1 | 3.1 | 0.2–15.7 | 31 | 96.9 | 84.3–99.8 | |
| Penetrating | 1 | 10.0 | 0.5–40.4 | 9 | 90.0 | 59.6–99.5 | |
| Other | 1 | 7.1 | 0.4–31.5 | 13 | 92.9 | 68.5–99.6 | |
| Mechanism of Injury (n = 503) | |||||||
| MVA | 24 | 13.0 | 8.9–18.7 | 160 | 87.0 | 81.3–91.1 | 0.0295 |
| Fall | 10 | 4.7 | 2.6–8.4 | 204 | 95.3 | 91.6–97.4 | |
| Sport/Recreation | 8 | 11.6 | 6.0–21.2 | 61 | 88.4 | 78.8–94.0 | |
| Assault | 2 | 11.1 | 2.0–32.8 | 16 | 88.9 | 67.2–98.0 | |
| Other | 1 | 5.6 | 0.3–25.8 | 17 | 94.4 | 74.2–99.7 | |
| Neurologic Level of Injury (n = 516) | |||||||
| C1 | 1 | 5.9 | 0.3–27.0 | 16 | 94.1 | 73.0–99.7 | 0.078 |
| C2 | 6 | 17.1 | 8.1–32.7 | 29 | 82.9 | 67.3–91.9 | |
| C3 | 5 | 4.1 | 1.8–9.2 | 117 | 95.9 | 90.8–98.2 | |
| C4 | 6 | 6.3 | 2.9–13.0 | 90 | 93.8 | 87.0–97.1 | |
| C5 | 16 | 12.0 | 7.5–18.6 | 117 | 88.0 | 81.4–92.5 | |
| C6 | 12 | 12.8 | 7.5–21.0 | 82 | 87.2 | 79.0–92.5 | |
| C7 | 1 | 5.3 | 0.3–24.6 | 18 | 94.7 | 75.4–99.7 | |
| ASIA Impairment Scale (n = 390) | |||||||
| A | 16 | 11.3 | 7.1–17.5 | 126 | 88.7 | 82.5–92.9 | 0.2714 |
| B | 4 | 8.3 | 3.3–19.6 | 44 | 91.7 | 80.4–96.7 | |
| C | 5 | 8.5 | 3.7–18.4 | 54 | 91.5 | 81.6–96.3 | |
| D | 7 | 5.0 | 2.4–9.9 | 134 | 95.0 | 90.1–97.6 | |
| Central Cord Syndrome (n = 388) | 8 | 4.6 | 2.3–8.8 | 166 | 95.4 | 91.2–97.7 | 0.0004 |
| Comorbidities (n = 497) | |||||||
| Hypertension | 19 | 11.4 | 7.5–17.2 | 147 | 88.6 | 82.8–92.5 | 0.1878 |
| Diabetes | 6 | 4.5 | 2.1–9.5 | 127 | 95.5 | 90.5–97.9 | 0.0339 |
| Myocardial Infarction | 2 | 10.5 | 1.9–31.4 | 17 | 89.5 | 68.6–98.1 | 0.6871 |
| Pulmonary Co-morbidities | 13 | 88.6 | 81.5–93.2 | 101 | 11.4 | 6.8–18.5 | 0.3535 |
| Cerebrovascular Accident | - | - | - | - | - | - | - |
| Malignancy | 0 | 0.0 | 0.0–32.4 | 8 | 100.0 | 67.6–100 | > 0.9999 |
| Tobacco | 1 | 10.0 | 0.5–40.4 | 9 | 90.0 | 59.6–99.5 | > 0.9999 |
| Drug Abuse | 3 | 6.4 | 2.2–17.2 | 44 | 93.6 | 82.8–97.8 | 0.6043 |
| Complications (n = 516) | |||||||
| Cardiac | 18 | 38.3 | 25.8–52.6 | 155 | 33.0 | 28.9–37.4 | 0.5174 |
| GI/GU | 25 | 53.2 | 39.2–66.7 | 185 | 39.4 | 33.3–60.8 | 0.086 |
| Pulmonary | 42 | 89.4 | 77.4–95.4 | 309 | 65.9 | 61.5–70.0 | 0.0008 |
| Skin | 9 | 19.1 | 10.4–32.5 | 62 | 13.2 | 10.5–16.6 | 0.2671 |
Table 3.
Pulmonary Complication Occurrence by Age Group. Fisher’s exact test shows near but no statistical significance (P = 0.0673).
Table 3.
Pulmonary Complication Occurrence by Age Group. Fisher’s exact test shows near but no statistical significance (P = 0.0673).
| Age Group | No | % | 95% CI | Yes | % | 95% CI |
| Pediatric (0–18) | 1 | 100.0 | 5.1–100 | 0 | 0.0 | 0.0–94.9 |
| Young Adult (19–25) | 46 | 75.4 | 63.3–84.5 | 15 | 24.6 | 15.5–36.7 |
| Adult (26–44) | 81 | 69.8 | 60.9–77.4 | 35 | 30.2 | 22.6–39.1 |
| Middle Age (45–59) | 103 | 74.1 | 66.2–80.7 | 36 | 25.9 | 19.3–33.8 |
| Above 60 | 114 | 83.8 | 76.7–89.1 | 22 | 16.2 | 10.9–23.3 |
| Unknown | 36 | 85.7 | 72.2–93.3 | 6 | 14.3 | 6.7–27.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



